
Prediabetes: Metformin vs. Lifestyle Intervention - · PDF filePrediabetes: Metformin vs....
23
Prediabetes: Metformin vs. Lifestyle Intervention Tannaz Moin, MD, MBA, MSHS Assistant Professor, David Geffen School of Medicine at UCLA Division of Endocrinology, Diabetes and Metabolism HSR&D Center for the Study of Healthcare InnovaEon, ImplementaEon & Policy VA Greater Los Angeles Healthcare System
Transcript of Prediabetes: Metformin vs. Lifestyle Intervention - · PDF filePrediabetes: Metformin vs....
Prediabetes: Metformin vs.
Lifestyle Intervention
Tannaz Moin, MD, MBA, MSHS Assistant Professor, David Geffen School of Medicine at UCLA
Division of Endocrinology, Diabetes and Metabolism HSR&D Center for the Study of Healthcare InnovaEon, ImplementaEon & Policy
VA Greater Los Angeles Healthcare System
I have no conflicts of interest to disclose
Outline
• Prediabetes – DefiniEon, controversies and emerging data
• MeIormin and lifestyle intervenEon for type 2 diabetes prevenEon
• TranslaEon in real-‐world pracEce
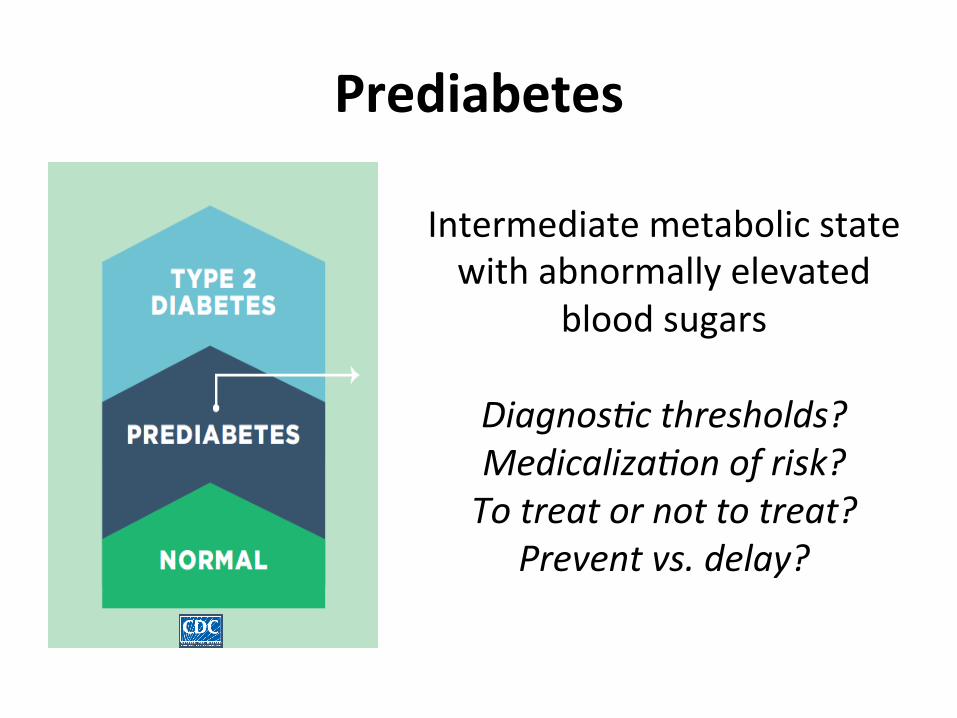
Prediabetes
Intermediate metabolic state with abnormally elevated
blood sugars
Diagnos)c thresholds? Medicaliza)on of risk? To treat or not to treat?
Prevent vs. delay?
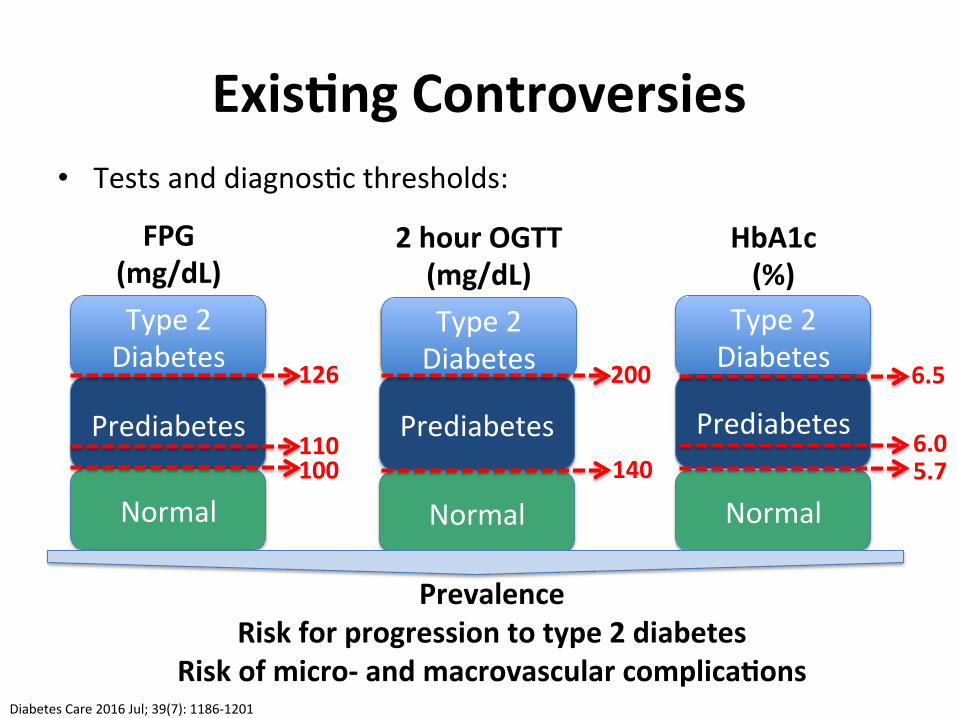
Exis8ng Controversies • Tests and diagnosEc thresholds:
Prevalence Risk for progression to type 2 diabetes
Risk of micro-‐ and macrovascular complica8ons
Type 2 Diabetes
Prediabetes
Normal
Diabetes Care 2016 Jul; 39(7): 1186-‐1201
FPG (mg/dL)
126
110 100
Type 2 Diabetes
Type 2 Diabetes
2 hour OGTT (mg/dL)
HbA1c (%)
Prediabetes Prediabetes
Normal Normal
200
140
6.5
5.7 6.0
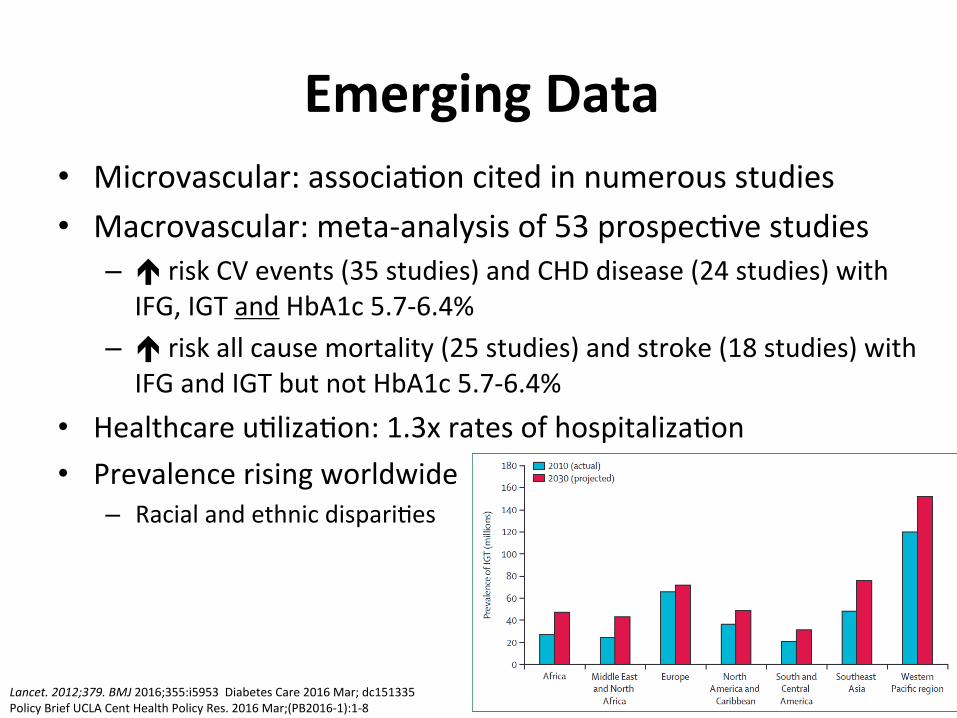
Emerging Data • Microvascular: associaEon cited in numerous studies • Macrovascular: meta-‐analysis of 53 prospecEve studies
– é risk CV events (35 studies) and CHD disease (24 studies) with IFG, IGT and HbA1c 5.7-‐6.4%
– é risk all cause mortality (25 studies) and stroke (18 studies) with IFG and IGT but not HbA1c 5.7-‐6.4%
• Healthcare uElizaEon: 1.3x rates of hospitalizaEon • Prevalence rising worldwide
– Racial and ethnic dispariEes
Lancet. 2012;379. BMJ 2016;355:i5953 Diabetes Care 2016 Mar; dc151335 Policy Brief UCLA Cent Health Policy Res. 2016 Mar;(PB2016-‐1):1-‐8
1 in 3 US adults have prediabetes
15-‐30% Percentage who will transiEon to type 2 diabetes in 5 years
Growing Public Health Concern
MeWormin vs. Lifestyle Interven8on
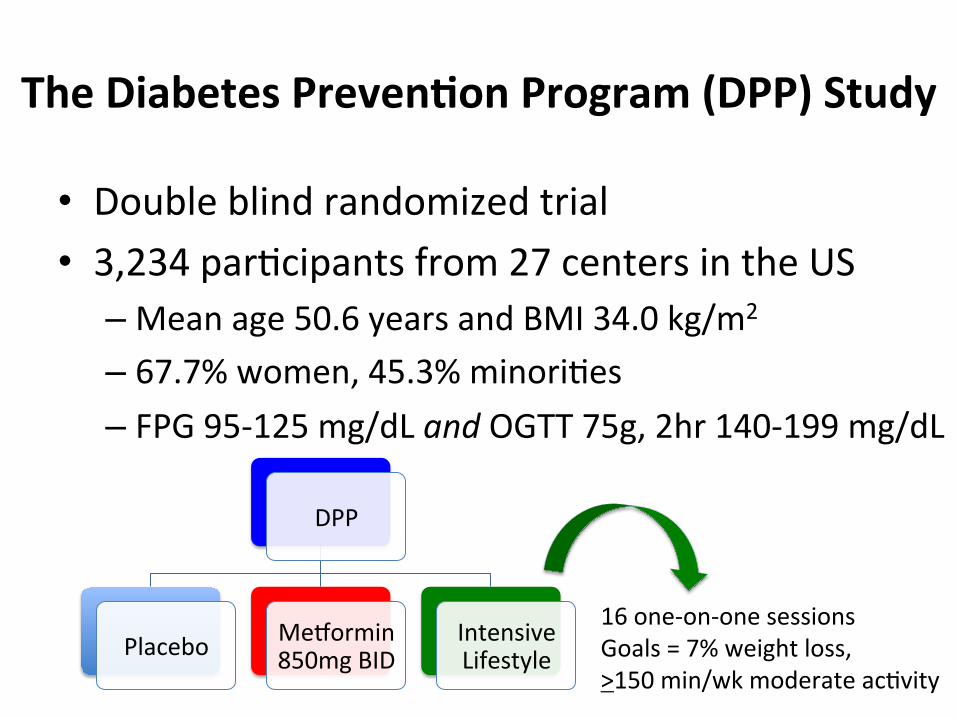
The Diabetes Preven8on Program (DPP) Study
• Double blind randomized trial • 3,234 parEcipants from 27 centers in the US
– Mean age 50.6 years and BMI 34.0 kg/m2 – 67.7% women, 45.3% minoriEes – FPG 95-‐125 mg/dL and OGTT 75g, 2hr 140-‐199 mg/dL
DPP
Placebo MeIormin 850mg BID
Intensive Lifestyle
16 one-‐on-‐one sessions Goals = 7% weight loss, >150 min/wk moderate acEvity
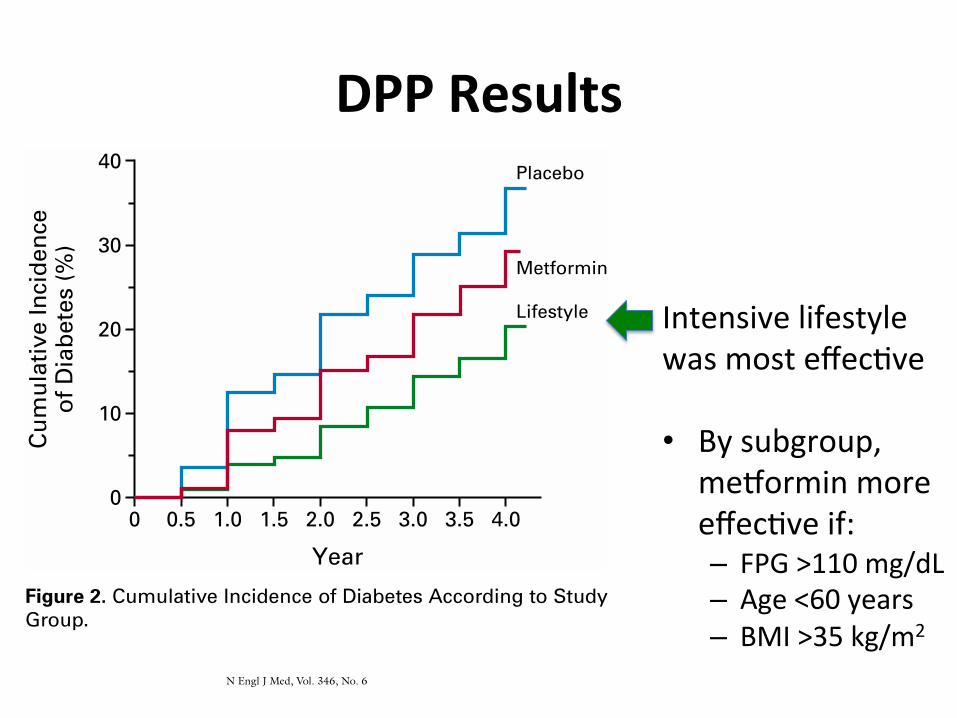
DPP Results
Intensive lifestyle was most effecEve • By subgroup,
meIormin more effecEve if: – FPG >110 mg/dL – Age <60 years – BMI >35 kg/m2
REDUCING THE INCIDENCE OF TYPE 2 DIABETES WITH LIFESTYLE INTERVENTION OR METFORMIN
N Engl J Med, Vol. 346, No. 6
·
February 7, 2002
·
www.nejm.org
·
397
er increase in leisure physical activity than did par-ticipants assigned to receive metformin or placebo.The average weight loss was 0.1, 2.1, and 5.6 kg in theplacebo, metformin, and lifestyle-intervention groups,respectively (P<0.001).
Incidence of Diabetes
The cumulative incidence of diabetes was lower inthe metformin and lifestyle-intervention groups thanin the placebo group throughout the follow-up pe-riod (Fig. 2). The crude incidence was 11.0, 7.8, and4.8 cases per 100 person-years for the placebo, met-formin, and lifestyle-intervention groups, respective-ly (Table 2). The incidence of diabetes was 58 per-cent lower (95 percent confidence interval, 48 to 66percent) in the lifestyle-intervention group and 31percent lower (95 percent confidence interval, 17 to43 percent) in the metformin group than in the pla-cebo group. The incidence of diabetes was 39 per-cent lower (95 percent confidence interval, 24 to 51percent) in the lifestyle-intervention group than inthe metformin group. The results of all three pair-wise group comparisons were statistically significantby the group-sequential log-rank test. None of theseresults were materially affected by adjustment forbase-line characteristics. The estimated cumulativeincidence of diabetes at three years was 28.9 percent,21.7 percent, and 14.4 percent in the placebo, met-formin, and lifestyle-intervention groups, respective-ly. On the basis of these rates, the estimated numberof persons who would need to be treated for threeyears to prevent one case of diabetes during this pe-riod is 6.9 (95 percent confidence interval, 5.4 to9.5) for the lifestyle intervention and 13.9 (95 per-cent confidence interval, 8.7 to 33.9) for metformin.
Treatment Effects among Subgroups
Incidence rates and risk reductions within sub-groups of participants and the results of tests of thehomogeneity of risk reduction among subgroups areshown in Table 2; 95 percent confidence intervals forthe subgroup data indicate the precision of the risk-reduction estimate for each stratum. The study hadinadequate power to assess the significance of effectswithin the subgroups, nor were such tests planned.Significant heterogeneity indicates that treatment ef-fects differed according to the values of the covariates.Treatment effects did not differ significantly accord-ing either to sex or to race or ethnic group (Table 2).The lifestyle intervention was highly effective in allsubgroups. Its effect was significantly greater amongpersons with lower base-line glucose concentrationstwo hours after a glucose load than among thosewith higher base-line glucose values. The effect of met-formin was less with a lower body-mass index or a low-er fasting glucose concentration than with higher
values for those variables. Neither interaction wasexplained by the other variable or by age. The ad-vantage of the lifestyle intervention over metforminwas greater in older persons and those with a lowerbody-mass index than in younger persons and thosewith a higher body-mass index.
Glycemic Changes
In the first year, there was a similar reduction inthe mean fasting plasma glucose values in the met-formin and lifestyle-intervention groups, whereas thevalues rose in the placebo group (Fig. 3). The valuesrose in parallel in all three groups in subsequentyears. There was a similar temporal pattern in thevalues for glycosylated hemoglobin, except that thevalues in the metformin group were in betweenthose in the lifestyle-intervention and placebo groups.Figure 4 shows the percentage of participants whohad normal glucose concentrations (fasting values,post-load values, and both) at each annual examina-tion. Metformin and the lifestyle intervention weresimilarly effective in restoring normal fasting glucosevalues, but the lifestyle intervention was more effec-tive in restoring normal post-load glucose values.
Adverse Events
The rate of gastrointestinal symptoms was highestin the metformin group, and the rate of musculo-skeletal symptoms was highest in the lifestyle-inter-vention group (Table 3). Hospitalization and mor-tality rates were unrelated to treatment. No deathswere attributed to the study intervention.
Figure 2.
Cumulative Incidence of Diabetes According to StudyGroup.The diagnosis of diabetes was based on the criteria of theAmerican Diabetes Association.
11
The incidence of diabetes dif-fered significantly among the three groups (P<0.001 for eachcomparison).
0
40
0
10
20
30
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
Year
Lifestyle
Metformin
Placebo
Cum
ulat
ive
Inci
denc
eof
Dia
bete
s (%
)
The New England Journal of Medicine Downloaded from nejm.org on August 22, 2013. For personal use only. No other uses without permission.
Copyright © 2002 Massachusetts Medical Society. All rights reserved.
The New England
Journal
of
Medicine
Copyr ight © 2002 by the Massachusett s Medical Society
VOLUME 346
F
EBRUARY
7, 2002
NUMBER 6
N Engl J Med, Vol. 346, No. 6
·
February 7, 2002
·
www.nejm.org
·
393
REDUCTION IN THE INCIDENCE OF TYPE 2 DIABETES WITH LIFESTYLE INTERVENTION OR METFORMIN
D
IABETES
P
REVENTION
P
ROGRAM
R
ESEARCH
G
ROUP
*
A
BSTRACT
Background
Type 2 diabetes affects approximate-ly 8 percent of adults in the United States. Some riskfactors — elevated plasma glucose concentrations inthe fasting state and after an oral glucose load, over-weight, and a sedentary lifestyle — are potentiallyreversible. We hypothesized that modifying thesefactors with a lifestyle-intervention program or theadministration of metformin would prevent or delaythe development of diabetes.
Methods
We randomly assigned 3234 nondiabeticpersons with elevated fasting and post-load plasmaglucose concentrations to placebo, metformin (850mg twice daily), or a lifestyle-modification programwith the goals of at least a 7 percent weight loss andat least 150 minutes of physical activity per week.The mean age of the participants was 51 years, andthe mean body-mass index (the weight in kilogramsdivided by the square of the height in meters) was34.0; 68 percent were women, and 45 percent weremembers of minority groups.
Results
The average follow-up was 2.8 years. Theincidence of diabetes was 11.0, 7.8, and 4.8 cases per100 person-years in the placebo, metformin, and life-style groups, respectively. The lifestyle interventionreduced the incidence by 58 percent (95 percent con-fidence interval, 48 to 66 percent) and metformin by31 percent (95 percent confidence interval, 17 to 43percent), as compared with placebo; the lifestyle in-tervention was significantly more effective than met-formin. To prevent one case of diabetes during aperiod of three years, 6.9 persons would have to par-ticipate in the lifestyle-intervention program, and 13.9would have to receive metformin.
Conclusions
Lifestyle changes and treatment withmetformin both reduced the incidence of diabetes inpersons at high risk. The lifestyle intervention wasmore effective than metformin. (N Engl J Med 2002;346:393-403.)
Copyright © 2002 Massachusetts Medical Society.
The writing group (William C. Knowler, M.D., Dr.P.H., Elizabeth Bar-rett-Connor, M.D., Sarah E. Fowler, Ph.D., Richard F. Hamman, M.D.,Dr.P.H., John M. Lachin, Sc.D., Elizabeth A. Walker, D.N.Sc., and DavidM. Nathan, M.D.) takes responsibility for the content of this article.
Address reprint requests to the Diabetes Prevention Program Coordinat-ing Center, Biostatistics Center, George Washington University, 6110 Ex-ecutive Blvd., Suite 750, Rockville, MD 20852.
*The members of the Diabetes Prevention Program Research Group arelisted in the Appendix.
YPE 2 diabetes mellitus, formerly callednon-insulin-dependent diabetes mellitus, isa serious, costly disease affecting approxi-mately 8 percent of adults in the United
States.
1
Treatment prevents some of its devastatingcomplications
2,3
but does not usually restore normo-glycemia or eliminate all the adverse consequences.The diagnosis is often delayed until complications arepresent.
4
Since current methods of treating diabetesremain inadequate, prevention is preferable. The hy-pothesis that type 2 diabetes is preventable
5,6
is sup-ported by observational studies and two clinical tri-als of diet, exercise, or both in persons at high riskfor the disease
7,8
but not by studies of drugs used totreat diabetes.
5
The validity of generalizing the results of previousprevention studies is uncertain.
9
Interventions thatwork in some societies may not work in others, be-cause social, economic, and cultural forces influencediet and exercise. This is a special concern in theUnited States, where there is great regional and ethnicdiversity in lifestyle patterns and where diabetes is es-pecially frequent in certain racial and ethnic groups,including American Indians, Hispanics, African Amer-icans, Asians, and Pacific Islanders.
10
The Diabetes Prevention Program Research Groupconducted a large, randomized clinical trial involv-ing adults in the United States who were at high riskfor the development of type 2 diabetes. The studywas designed to answer the following primary ques-tions: Does a lifestyle intervention or treatment with
T
The New England Journal of Medicine Downloaded from nejm.org on August 22, 2013. For personal use only. No other uses without permission.
Copyright © 2002 Massachusetts Medical Society. All rights reserved.
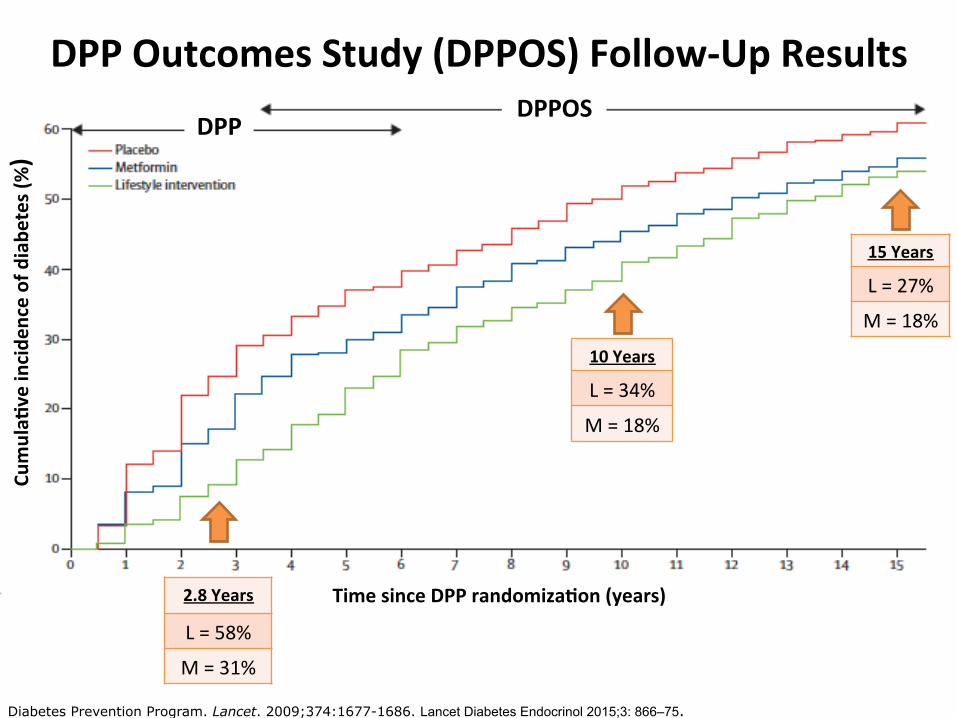
DPP Outcomes Study (DPPOS) Follow-‐Up Results
Diabetes Prevention Program. Lancet. 2009;374:1677-1686. Lancet Diabetes Endocrinol 2015;3: 866–75.
2.8 Years A\er Randomiza8on
10 Years A\er Randomiza8on
15 Years A\er Randomiza8on
Lifestyle 58% 34% 27%
MeWormin 31% 18% 18%
2.8 Years
L = 58%
M = 31%
10 Years
L = 34%
M = 18%
15 Years
L = 27%
M = 18%
DPP DPPOS
Cumula8
ve incide
nce of diabe
tes (%)
Time since DPP randomiza8on (years)
Addi8onal DPP Findings • Intensive lifestyle lost the most weight, but partly regained; meIormin maintained modest weight loss
• Heterogeneity of effect by age and subgroup • Reversion to normal glycemia was associated with lower rates of progression to type 2 diabetes
• Lifestyle and meIormin had similar effect in prevenEng HbA1c-‐defined diabetes
• Quality of life é with lifestyle but not meIormin • Lifestyle cost-‐effecEve, meIormin marginally cost-‐saving vs. placebo
Lancet. 2012 Jun 16; 379(9833):2243-‐51. Diabetes Care 2015 Jan; 38(1): 51-‐58. Ann Intern Med. 2005:142:323-‐332. Diabetes Care. 2012;35:723-‐730.
MeIormin + Lifestyle IntervenEon

Stepwise Approach: Diabetes Community Lifestyle Improvement Program (D-‐CLIP)
• Randomized, controlled, translaEonal trial • 578 Asian Indian adults
– Mean age 44.4 years and BMI 27.9 kg/m2 – IGT, IFG or IGT+IFG
D-‐CLIP
Control DPP Lifestyle + MeIormin 500mg BID
At 4 months, those with IFG+IGT and IFG and HbA1c>5.7% were prescribed meIormin
Diabetes Care 2016 Aug; dc161241.
Stepwise Approach: Diabetes Community Lifestyle Improvement Program (D-‐CLIP)
• Mean weight loss = 4% at 6 months • Over 3 years of follow-‐up, 32% relaEve risk reducEon (RRR) with lifestyle + meIormin – Diabetes incidence 34.9% control vs. 25.7% lifestyle + meIormin, p=0.014
– Heterogeneity of effect across prediabetes subtypes: IGT+IFG>IGT>IFG
• Number needed to treat (NNT) to prevent one case of diabetes = 9.8
Diabetes Care 2016 Aug; dc161241.
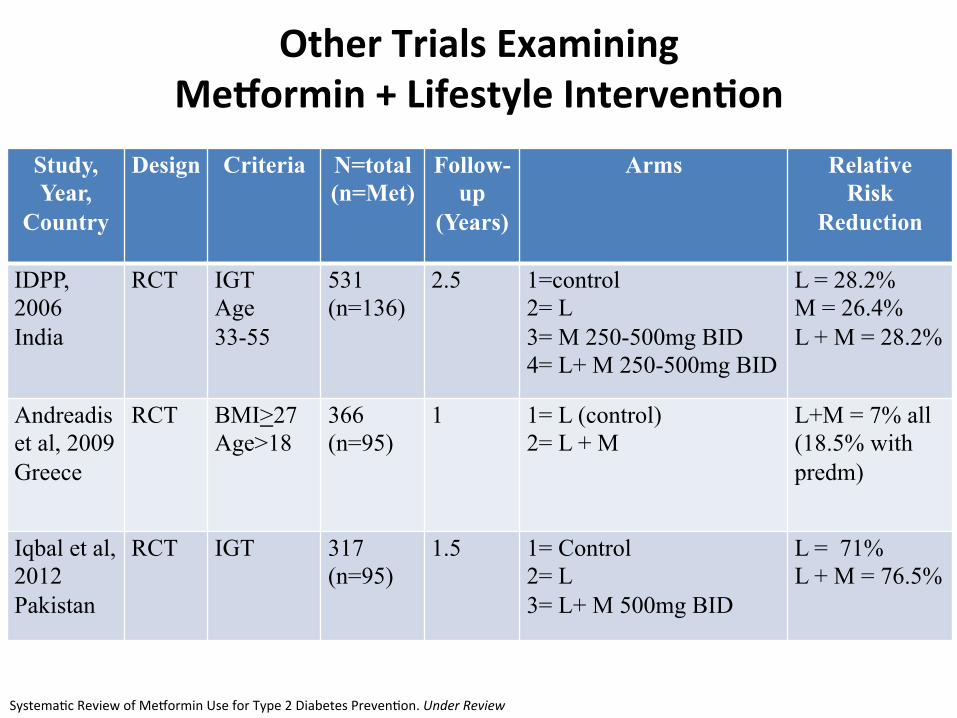
Other Trials Examining MeWormin + Lifestyle Interven8on
Study, Year,
Country
Design Criteria N=total (n=Met)
Follow-up
(Years)
Arms Relative Risk
Reduction
IDPP, 2006 India
RCT IGT Age 33-55
531 (n=136)
2.5 1=control 2= L 3= M 250-500mg BID 4= L+ M 250-500mg BID
L = 28.2% M = 26.4% L + M = 28.2%
Andreadis et al, 2009 Greece
RCT BMI>27 Age>18
366 (n=95)
1 1= L (control) 2= L + M
L+M = 7% all (18.5% with predm)
Iqbal et al, 2012 Pakistan
RCT IGT 317 (n=95)
1.5 1= Control 2= L 3= L+ M 500mg BID
L = 71% L + M = 76.5%
SystemaEc Review of MeIormin Use for Type 2 Diabetes PrevenEon. Under Review
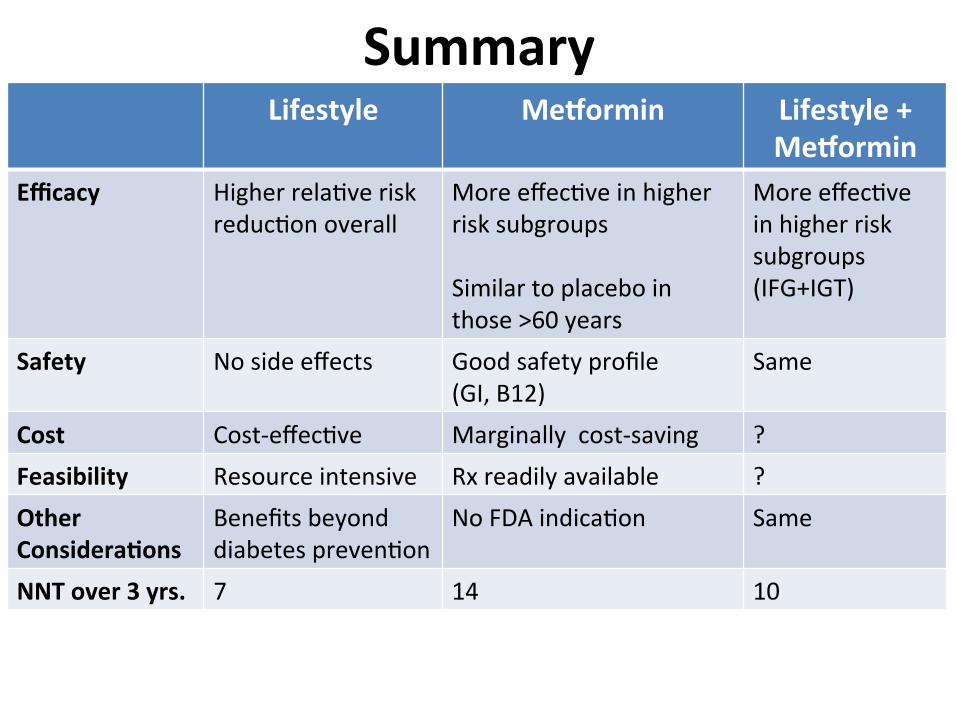
Summary Lifestyle MeWormin Lifestyle +
MeWormin Efficacy Higher relaEve risk
reducEon overall
More effecEve in higher risk subgroups Similar to placebo in those >60 years
More effecEve in higher risk subgroups (IFG+IGT)
Safety No side effects Good safety profile (GI, B12)
Same
Cost Cost-‐effecEve Marginally cost-‐saving ? Feasibility Resource intensive Rx readily available ? Other Considera8ons
Benefits beyond diabetes prevenEon
No FDA indicaEon Same
NNT over 3 yrs. 7 14 10
Are We Transla8ng Evidence into Prac8ce?
Ann Intern Med. 2015;162(8):542-‐548. CDC Prediabetes Could it Be You? 2016
• Lifestyle – Numerous real world translaEonal studies – Uptake and reach remain a criEcal challenge
• MeIormin – Efforts to translate this arm of the DPP have been limited – Extremely low rates of use à 3.7% of insured working age adults with prediabetes were prescribed meIormin 2010-‐12
Prevent Diabetes STAT
• Public health campaign launched by CDC and AMA • Healthcare Provider Toolkit
– Methods to screen and refer high-‐risk paEents to CDC-‐recognized community based or virtual DPP in their communiEes
www.PreventDiabetesSTAT.org
Changing Real World Prac8ce
• Refer paEents with prediabetes to CDC recognized DPP lifestyle intervenEons (preferred)
• Consider meIormin for diabetes prevenEon in high risk paEents: age <60 years, BMI>35 kg/m2 , and women with prior gestaEonal diabetes
• Monitor for development of diabetes annually • Screen and treat modifiable risk factors for CVD
ADA Standards of Care 2016
Changing Real World Prac8ce
• Increase prediabetes awareness – Prediabetes-‐aware adults are more likely to engage in lifestyle change intervenEons
• Help paEents make informed choices that are aligned with their preferences and values – OpportuniEes to promote paEent-‐centered dialogue about prediabetes in primary care
– PaEents may consider both intensive lifestyle and meIormin as acceptable treatment opEons
– UCLA MyMeds pharmacist consults available in EPIC
Diabetes Educ. 2016 Dec;42(6):667-‐677

Research Funding Acknowledgement:
Thank You!







![Effects of a lifestyle intervention during pregnancy to ... · sist later in life [16, 17]. Over the last decade, a variety of lifestyle intervention studies during pregnancy have](https://static.fdocuments.net/doc/165x107/5f6a106dda218f71024169ec/effects-of-a-lifestyle-intervention-during-pregnancy-to-sist-later-in-life-16.jpg)










