Prd 12059
36
Periodontal plastic surgery G IOVANNI Z UCCHELLI &I LHAM M OUNSSIF Mucogingival therapy is a general term used to describe periodontal treatment involving procedures for the correction of defects in the morphology, posi- tion and/or amount of soft tissue and underlying bone support around teeth and implants (12). At the beginning, ‘mucogingival surgery’, introduced by Friedman in 1957 (69), included surgical procedures designed to preserve gingival tissue, remove aberrant frenal or muscle attachments and increase the depth of the vestibule. Frequently, however, this term was used to describe certain pocket elimination approaches. Therefore, in 1993, Miller (132) intro- duced the term ‘periodontal plastic surgery’, accepted by the international scientific community in 1996, which was defined as ‘surgical procedures performed to prevent or correct anatomic, develop- mental, traumatic or disease-induced defects of the gingiva, alveolar mucosa or bone’ (203). This defini- tion includes various soft- and hard-tissue proce- dures aimed at gingival augmentation, root coverage, correction of mucosal defects at implants, crown lengthening, gingival preservation at ectopic tooth eruption, removal of aberrant frena, prevention of ridge collapse associated with tooth extraction and augmentation of the edentulous ridge. This paper focuses on gingival recession defects, their diagnosis and prognosis and the surgical procedures for root coverage. Etiology of gingival recessions The gingival margin is clinically represented by a scal- loped line that follows the outline of the cemento– enamel junction, 1–2 mm coronal to it. Gingival recession is an apical shift of the gingival margin with exposure of the root surface to the oral cavity (205) (Fig. 1). Gingival recession is often found in popula- tions with good oral hygiene (173, 177), when it is most commonly located at the buccal surfaces (117) and may be associated with wedge-shaped defects in the cervical area of one or more teeth (173). However, gingival recession is also found in populations with poor standards of oral hygiene in which it may affect other tooth surfaces (16, 117). Recession may exist in the presence of normal sulci and nondiseased inter- dental crestal bone levels, or it may occur as part of the pathogenesis of periodontal disease during which alveolar bone is lost. One etiological factor that may be associated with gingival recession is a pre-existing lack of alveolar buccal bone at the site (202) (Fig. 1). These deficiencies in alveolar bone may be develop- mental (anatomical) or acquired (physiological or pathological) (72). Anatomical factors Anatomical factors that have been related to gingi- val recession include fenestration and dehiscence of the alveolar bone, abnormal tooth position in the arch, an aberrant path of eruption of the tooth and the shape of the individual tooth (7). These anatom- ical factors are inter-related and may result in an alveolar osseous plate that is thinner than normal and that may be more susceptible to resorption. Anatomically, a dehiscence may be present because of the direction of tooth eruption or as a result of other developmental factors, such as buccal place- ment of the root relative to adjacent teeth, so that the cervical portion protrudes through the crestal bone (119). One surgical study found a correlation between gingival recession and bone dehiscence (21). A correlation between the pattern of eruption and gingival recession has also been suggested (134). Dehiscence may be present where the bucco- lingual thickness of a root is similar to or exceeds the crestal bone thickness (144). The same authors postulated that individuals with morphological bio- types characterized by narrow, long teeth are more prone to dehiscences than are individuals with broad, short teeth. Where gingival recession has developed, the underlying presence of dehiscences may be considered, and possibly discovered during flap procedures. 333 Periodontology 2000, Vol. 68, 2015, 333–368 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd Printed in Singapore. All rights reserved PERIODONTOLOGY 2000
-
Upload
vishwas-updesh-madaan -
Category
Documents
-
view
20 -
download
0
description
jhjj
Transcript of Prd 12059
-
Periodontal plastic surgeryGIOVANNI ZUCCHELLI & ILHAM MOUNSSIF
Mucogingival therapy is a general term used todescribe periodontal treatment involving proceduresfor the correction of defects in the morphology, posi-tion and/or amount of soft tissue and underlyingbone support around teeth and implants (12). At thebeginning, mucogingival surgery, introduced byFriedman in 1957 (69), included surgical proceduresdesigned to preserve gingival tissue, remove aberrantfrenal or muscle attachments and increase the depthof the vestibule. Frequently, however, this termwas used to describe certain pocket eliminationapproaches. Therefore, in 1993, Miller (132) intro-duced the term periodontal plastic surgery,accepted by the international scientic communityin 1996, which was dened as surgical proceduresperformed to prevent or correct anatomic, develop-mental, traumatic or disease-induced defects of thegingiva, alveolar mucosa or bone (203). This deni-tion includes various soft- and hard-tissue proce-dures aimed at gingival augmentation, root coverage,correction of mucosal defects at implants, crownlengthening, gingival preservation at ectopic tootheruption, removal of aberrant frena, prevention ofridge collapse associated with tooth extraction andaugmentation of the edentulous ridge. This paperfocuses on gingival recession defects, their diagnosisand prognosis and the surgical procedures for rootcoverage.
Etiology of gingival recessions
The gingival margin is clinically represented by a scal-loped line that follows the outline of the cementoenamel junction, 12 mm coronal to it. Gingivalrecession is an apical shift of the gingival margin withexposure of the root surface to the oral cavity (205)(Fig. 1). Gingival recession is often found in popula-tions with good oral hygiene (173, 177), when it ismost commonly located at the buccal surfaces (117)and may be associated with wedge-shaped defects inthe cervical area of one or more teeth (173). However,
gingival recession is also found in populations withpoor standards of oral hygiene in which it may affectother tooth surfaces (16, 117). Recession may exist inthe presence of normal sulci and nondiseased inter-dental crestal bone levels, or it may occur as part ofthe pathogenesis of periodontal disease during whichalveolar bone is lost. One etiological factor that maybe associated with gingival recession is a pre-existinglack of alveolar buccal bone at the site (202) (Fig. 1).These deciencies in alveolar bone may be develop-mental (anatomical) or acquired (physiological orpathological) (72).
Anatomical factors
Anatomical factors that have been related to gingi-val recession include fenestration and dehiscence ofthe alveolar bone, abnormal tooth position in thearch, an aberrant path of eruption of the tooth andthe shape of the individual tooth (7). These anatom-ical factors are inter-related and may result in analveolar osseous plate that is thinner than normaland that may be more susceptible to resorption.Anatomically, a dehiscence may be present becauseof the direction of tooth eruption or as a result ofother developmental factors, such as buccal place-ment of the root relative to adjacent teeth, so thatthe cervical portion protrudes through the crestalbone (119). One surgical study found a correlationbetween gingival recession and bone dehiscence(21). A correlation between the pattern of eruptionand gingival recession has also been suggested(134). Dehiscence may be present where the bucco-lingual thickness of a root is similar to or exceedsthe crestal bone thickness (144). The same authorspostulated that individuals with morphological bio-types characterized by narrow, long teeth are moreprone to dehiscences than are individuals withbroad, short teeth. Where gingival recession hasdeveloped, the underlying presence of dehiscencesmay be considered, and possibly discovered duringap procedures.
333
Periodontology 2000, Vol. 68, 2015, 333368 2015 John Wiley & Sons A/S. Published by John Wiley & Sons LtdPrinted in Singapore. All rights reserved PERIODONTOLOGY 2000
-
Localized gingival recession may be associated withthe position of the teeth on the arch (106, 144). Theposition in which a tooth erupts through the alveolarprocess affects the amount of gingiva that will beestablished around the tooth. If a tooth erupts closeto the mucogingival line there may be very little, orno, keratinized tissue labially and localized recessionmay occur (214). In the developing dentition of pre-teenage children, buccal displacement of the lowerincisors is common and is often associated with gingi-val recession. Follow-up studies reveal spontaneousreversal of recession as the child matures (13).
Physiological factors
Physiological factors may include the orthodonticmovement of teeth to positions outside the labial orlingual alveolar plate, leading to dehiscence forma-tion (105, 206) that may act as locus minoris resisten-tiae for gingival recession development (172, 206).The gingival recession may appear as a deep and nar-row lesion, similar to a Stillman cleft, in which domi-ciliary oral hygiene becomes very difcult to perform,and bacterial or viral infection may induce the forma-tion of a buccal probing pocket of sufcient depth toreach the periapical environment of the tooth. Some-times a delayed diagnosis is made only when an end-odontic abscess occurs.The volume of the facial soft tissue may be a factor
in predicting whether gingival recession will occurduring or after active orthodontic treatment. A thingingiva may be a greater risk factor for progression inthe presence of plaque-induced inammation ortoothbrushing trauma (206). Therefore, the activeorthodontic movement of the teeth outside the alveo-lar bone may be considered as an etiological factor.
When, during the postorthodontic retention phase,wide and deep multiple gingival recessions occur, it istoothbrushing trauma that acts as an etiological fac-tor on gingival tissue that has been thinned as a resultof tooth malposition (buccal dislocation). In such aclinical situation, orthodontic therapy acts as a pre-disposing factor for gingival recession. Sometimes,isolated deep gingival recessions occur in the lowerincisors a few years after orthodontic therapy. Com-mon characteristics associated with these gingivaldefects are the presence of a round-wire lingual-bonded retainer from canine to canine, a differentaxial (faciallingual) inclination of the affected toothwith respect to the adjacent incisors and the presenceof inammatory tissue lateral to the root exposure(Fig. 2). In such a case, the etiological factor can befound in a patients chronic habits, such as ngernailbiting, digit sucking, or sucking on objects such aspens, pencils or toothpicks, that exert continuouspressure on the biting edge of the affected tooth(Fig. 2). As any lingual-crown movement is preventedby the round-wire lingual-bonded retainer, theapplied force leads to buccal displacement of theroot, bone dehiscence and gingival recession.
Pathological factors
Toothbrushing
Toothbrushing is commonly associated with gingivalrecession and partly explains the correlation betweenlow plaque levels found at sites of recession (2).Trauma can be caused by improper toothbrushingor by a number of potentially confounding variables,such as pressure, time, bristle type and the dentifriceused (108, 164). Clinical signs of gingival recessioncaused by toothbrushing are soft-tissue ulcers (with-
A B C
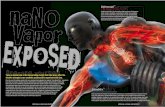
Fig. 1. Gingival recession and bonedehiscence. (A) Gingival recessionextending from the cementoenameljunction (dotted line) to the soft-tis-sue margin. (B) Gingival recession inthe lateral view: the distinctionbetween the anatomic crown andthe root (cementoenamel junction)becomes more evident. (C) Bonedehiscence (from the cementoenamel junction to the buccalbone crest) associated with gingivalrecession.
Zucchelli & Mounssif
334
-
out pain) and hard-tissue cervical abrasions (noncari-ous cervical lesions). Sometimes, soft-tissue traumamay destroy all keratinized gingival tissue. The cervi-cal abrasions are caused by continued mechanicaltrauma after recession manifestation.
Improper ossing techniques
Flossing trauma can contribute to tooth abrasion andgingival injury (1, 66, 74). These lesions often occur inhighly motivated patients who have not been prop-erly instructed in the technique of ossing. Diagnosisof these injuries can often be conrmed by askingpatients to demonstrate their oral hygiene procedures(200). The initial injury may appear as an acutelyinamed, ulcerated linear or V-shaped cleft that issymptomatic (74, 87) (Fig. 3). Chronic lesions areoften asymptomatic and may not appear to be ulcer-ated or clinically inamed. The clefts may traversethe width of the interdental space and extend into theadjacent facial and lingual gingivae. At the histologi-cal level, gingival clefts are often lined by stratiedsquamous epithelium. The base of the cleft may havea bifurcated appearance and exhibit varying degrees
of epithelialization (87). Often patients use a ossingtechnique with a sawing motion (126) while advanc-ing the oss apically into the gingival crevice (200).When ossing trauma is involved, supercial gingivaltissue clefts are red because the injury is connedwithin connective tissue. In this case the lesion isreversible: ossing procedures have to be stopped forat least 2 weeks and chemical plaque control (i.e.chlorexidine rinses) only should be performed(Fig. 3). If the cleft appears white the whole connec-tive tissue thickness is involved and the radicular sur-face becomes evident; in this case the gingival lesionis irreversible (87, 140) (Fig. 3).
Perioral and intraoral piercing
Piercing of the tongue and perioral regions is becom-ing an increasingly popular expression of so-calledbody art (79, 126). Tongue piercing has been directlyrelated to dental and gingival injuries on the lingualaspect of the anterior lower teeth (24, 37), and buccalgingival recession may occur in subjects in whom thelip stud is located such that it can traumatize the gin-giva (37, 63). Frequently, the lingual gingival lesion is
A B
Fig. 2. Postorthodontic gingival recession. (A) Buccal view:note the presence of inamed, red, highly vascularizedtissue lateral to the deep root exposure. (B) Occlusalview: note the presence of the round-wire lingual-bonded
retainer from canine to canine and the different axialbuccallingual inclination of the affected tooth withrespect to the adjacent incisors.
A B
C D Fig. 3. Gingival cleft. (A, B) Redcleft: the interruption of the soft-tis-sue margin is not full thickness. Thelesion can be reversed by interruptingthe trauma. (C, D) White cleft: theroot surface is evident at the bottomof the ssure. Re-epithelization of thelesion is complete.
Periodontal plastic surgery
335
-
narrow and thin and plaque control is difcult to per-form; when particularly deep, lingual recession canbe associated with a probing pocket depth that canreach the periapical region. Removal of the stud isdesirable to eliminate the etiological factor (175). Fur-ther therapy (such as mucogingival surgery) (179)may be necessary when keratinized tissue is lost andthe periodontal attachment compromised.
Direct trauma associated with malocclusion
Class II, division two, malocclusions have a deep over-bite and often a reduced overjet with retroclination ofthe upper anterior teeth. In some severe cases this canresult in direct trauma to the labial gingiva of thelower anterior teeth or to the palatal marginal gingivaof the upper anterior teeth (97). This may result inindentations in the gingiva and can result in recessionat the site (195). In rare cases in young people, theorthodontic/orthognatic management of malocclu-sion and appropriate toothbrushing can solve gingivalrecession without the need for surgical interaction.
Partial denture/restorative therapy
Poorly designed or maintained partial dentures andthe placement of restoration margins subgingivallymay not only result in direct trauma to the tissues(55), but may also facilitate subgingival plaque accu-mulation, with resultant inammatory alterations inthe adjacent gingiva and recession of the soft-tissuemargin (85, 111, 147). Experimental and clinical datasuggest that the thickness of the marginal gingiva(182), but not the apicocoronal width of the gingiva(64), may inuence the magnitude of recession takingplace as a result of direct mechanical trauma duringtooth preparation and bacterial plaque retention. Ifgingival recession is caused only by trauma from par-tial dentures, complete root coverage is possible bymucogingival surgery; however, if recession is causedby interdental attachment loss during tooth prepara-tion, root coverage is not achievable. In both cases anew partial denture is suggested.
Bacterial plaque
Gingival recession may be caused by localized accu-mulation of bacterial plaque on the buccal surface ofthe tooth (17, 117, 168, 195, 196). This should not beconfused with gingival recession caused/associatedwith periodontal disease. In the latter, bacterialplaque (specic periodontal pathogens) causes con-nective tissue attachment loss that may clinicallymanifest with gingival recession not only at buccalsurfaces but also at the interproximal tooth surfaces.Bacterial plaque-induced gingival recessions are
caused by plaque accumulation localized to the buc-cal surface with no severe interdental attachmentloss; thus, they can be successfully treated withroot-coverage procedures. Patients with bacterialplaque-induced recessions must be motivated on theimportance of oral hygiene, and mucogingival surgerymust not be performed until good plaque control hasbeen achieved. The presence of microbial deposits onthe exposed root surface and/or clinical signs ofinammation in the surrounding tissues are usefulfor reaching the correct diagnosis. Buccal probingpocket depths apical to the root exposure arefrequently associated with bacteria-induced gingivalrecessions.
Herpes simplex virus
Gingival recession may be associated with herpessimplex virus type 1. The lesions consist of multiplevesicles that rupture, rapidly giving rise to ulcers (62,68). They are often accompanied with pain and some-times with fever and regional lymphadenopathy. Thelesion can be found in all areas of the mouth becauseof diffusion of the infection with toothbrushing; fre-quently, associated mucocutaneous lesions can befound. In the early phase ulcers do not involve thegingival margin and it is suggested that toothbrushingis responsible for their evolution (159). In the pre-sence of virus-induced gingival lesions, toothbrushingand dental ossing should be stopped and chemicalplaque control (with chlorexidine rinsing) should beperformed. Surgical procedures are indicated only ifand when gingival recession becomes irreversible.
Classication, diagnosis andprognosis of gingival recessions
Gingival recession can be treated with various surgi-cal procedures, and root coverage can be obtainedirrespective of the surgical approach adopted. Themost important prognostic factor for root coveragefollowing surgery is the height of the interdental peri-odontal support (clinical attachment and alveolarbone levels) (131). In the case of a periodontallyhealthy tooth the papillae completely lls the inter-dental spaces and there is no clinical attachment lossor bone loss; periodontal probing and intraoral X-raymay be helpful to conrm the healthy condition. Gin-gival recessions have been classied by Miller (131)into four classes (an illustration of Millers classica-tion is reported in Fig. 4), according to the prognosisof root coverage. In Class I and Class II gingival reces-sions, there is no loss of interproximal periodontal
Zucchelli & Mounssif
336
-
attachment and bone, and complete (up to the ce-mentoenamel junction) root coverage can beachieved. The difference between the two classes liesin the height of the root exposure reaching (Class II)or not reaching (Class I) the mucogingival junction.In Class III gingival recessions, the loss of interdentalperiodontal support is mild to moderate, and partialroot coverage can be accomplished; in addition,tooth/root malposition limits the possible amount ofroot coverage. In Class IV gingival recessions, the lossof interproximal periodontal attachment (or tooth/root malposition) is so severe that no root coverage isfeasible.Some questions/doubts about the classication of
gingival recession, not claried in Millers classica-tion, have recently been highlighted (160). One ofthese doubts relates to the Millers class of gingivalrecession (Class I or Class II) extending beyond themucogingival line, but conserving a small, probableheight of keratinized tissue apical to the root expo-sure (Fig. 5). The distinction, even if not signicantfrom a prognostic point of view, could be useful for
selecting the most successful root-coverage surgicalapproach. Other criticisms of Millers classicationrelate to the unclear procedures to ascertain theamount of soft-/hard-tissue loss in the interdentalarea to differentiate Class III and Class IV (Fig. 6) andthe unclear inuence of tooth malpositioning (160)(Fig. 7). Cairo et al. (35) recently introduced a newclassication system of gingival recessions using thelevel of interproximal clinical attachment as an iden-tication criterion; they also explored the predictivevalue of the resulting classication system on nalroot coverage outcomes following surgery. Threerecession types (RT) were identied: class RT1included gingival recession with no loss of interproxi-mal attachment; class RT2 comprised recession withloss of interproximal attachment less than or equal tothe buccal site; and class RT3 showed interproximalattachment loss higher than the buccal site. Theresults of this study show that the recession type classis a strong predictor of the nal recession reductionafter different surgical procedures. The authorshypothesized that the level of interproximal clinical
A B
C D
Fig. 4. Miller classication of gingi-val recession. (A) Class I: the inter-dental periodontal support is intactand the gingival recession does notreach the mucogingival line. Com-plete root coverage can be achieved.(B) Class II: the interdental peri-odontal support is intact and thegingival recession reaches the muco-gingival line. Complete root cover-age can be achieved. (C) Class III:there is some interdental attachmentand bone loss and the gingival reces-sion reaches the mucogingival line.Partial root coverage can beachieved. (D) Class IV: bone andattachment loss are so severe that noroot coverage can be accomplished.
A B
Fig. 5. Criticisms of Millers classi-cation of gingival recession. (A, B)Distinction between Class I andClass II is not clear for gingivalrecessions extending beyond themucogingival line but a small heightof probable keratinized tissue is con-served apical to the exposed root.
Periodontal plastic surgery
337
-
attachment loss is the coronal limit of the achievableamount of root coverage at the buccal site after sur-gery. The RT1 class showed a higher mean reductionof recession compared with the RT2 class, highlight-ing the importance of baseline interproximal clinicalattachment loss for the prognosis of gingival reces-sion treatment. The same authors (34) recently pub-lished a randomized clinical trial evaluating theadjunctive benet of connective tissue grafts com-pared with coronally advanced aps for the treatmentof gingival recession associated with interdental clini-cal attachment loss the same as or smaller than buc-cal attachment loss (RT2). They concluded thatcomplete root coverage can be achieved in RT2affecting the upper anterior teeth with both coronallyadvanced ap alone and coronally advanced ap plusconnective tissue grafts; however, the additional useof a connective tissue graft resulted in a greater num-ber of sites with complete root coverage: >80% of thesites when the baseline amount of interdental clinicalattachment loss was 3 mm (34). Further longer-termstudies are advocated to evaluate root coverage inMiller Class III and Class IV gingival recessions.Another criticism of Millers classication regards thedifculty of identifying the cementoenamel junction
on teeth affected by gingival recession and noncari-ous cervical lesions (Fig. 8). Pini-Prato et al. (161)recently proposed a clinical classication of surfacedefects in teeth associated with gingival recession.Four classes of dental-surface defects in areas of gin-gival recession were identied on the basis of thepresence (Class A) or absence (Class B) of the cemen-toenamel junction and of the presence (Class+) orabsence (Class) of surface discrepancy (a step). Of1010 exposed root surfaces, 144 (14%) showed anidentiable cementoenamel junction associatedwith a root surface step (Class A+), 469 (46%) showedan identiable cementoenamel junction without anyassociated step (Class A), 244 (24%) demonstratedan unidentiable cementoenamel junction with astep (Class B+) and 153 (15%) showed an unidenti-able cementoenamel junction without any associ-ated step (Class B). According to the authors, theclassication of dental surface defects in conjunctionwith the classication of periodontal tissues is usefulfor reaching a more precise diagnosis in areas of gin-gival recession, and the condition of the exposed rootsurface may also be important for the prognosticevaluation of mucogingival surgery. In the literature(169, 203), predictability of root coverage was mea-sured in terms of the mean percentage of root cover-age (indicating the percentage of the root exposurecovered with soft tissues) and the percentage of com-plete root coverage (showing the percentage of teethwith the soft-tissue margin covering the cementoenamel junction). For the correct evaluation of bothof these parameters, it is necessary to recognize thecementoenamel junction, which anatomically sepa-rates the crown from the root, on the tooth with therecession defect. Therefore, the clinical healing pat-tern only of those gingival recessions in which the ce-mentoenamel junction is clinically detectable couldbe evaluated in terms of percentage and/or completeroot coverage. When the cementoenamel junction isnot recognizable, it is no longer possible to measurethe depth (and width) of the recession and/or toassess the efcacy of a surgical technique in terms ofroot coverage, as a result of the lack of the referenceparameter (226). Furthermore, other tooth/gingival
A B
Fig. 6. Criticisms of Millers classication of gingival reces-sion. (A, B) Distinction between Class III and Class IV: par-tial root coverage can be accomplished in supposed ClassIV gingival recessions.
A BFig. 7. Criticisms of Millers classi-cation of gingival recession. (A, B)The role of tooth malposition in pre-venting complete root coverage:complete root coverage can beaccomplished in supposed Class IIIgingival recession (caused by buccaldislocation of the root).
Zucchelli & Mounssif
338
-
local conditions that may limit complete root cover-age, even in the presence of an intact interdentalperiodontal support, have recently been suggested,such as loss of interdental papillae, tooth rotation,tooth extrusion and occlusal abrasion (226).The difculty of identifying the anatomic cemento
enamel junction at a tooth with noncarious cervicallesions, and the presence of anatomic or clinical con-ditions limiting root coverage even in Class I andClass II gingival recessions, stimulated clinicians topredetermine the level of root coverage (i.e. the levelat which the soft-tissue margin will be stable after thehealing process of a root coverage surgical proce-dure). Predetermination of root coverage was per-formed by Aichelmann-Reidy et al. (4) in acomparative study on the treatment of single-typegingival recession defects. In this study the treatingperiodontist made a clinical determination of theexpected amount of root coverage, based on clinicalexperience and clinical conditions, on the test teethand adjacent areas. Factors such as tooth position,root prominence and recessions on adjacent teethwere taken into account in making the subjectiveclinical decision. However, in this article, there wasno mention of how the expected amount of root cov-erage was calculated. More recently, a method to pre-determine the level of root coverage, based oncalculation of the ideal height of the anatomic
interdental papilla, was demonstrated to be reliablein predicting the position of the soft-tissue margin3 months after root-coverage surgery (224). This levelwas depicted as a line that should coincide with theanatomic cementoenamel junction when this wasnot clinically detectable on the tooth with Miller ClassI or Class II gingival recessions, or would be more api-cal than the anatomic cementoenamel junctionwhen the ideal anatomic conditions to obtain com-plete root coverage were not fully represented (i.e.Miller Class III gingival recession). This line wasdescribed as the line of root coverage or the clinicalcementoenamel junction. The ideal height of thepapilla in a tooth with gingival recession was denedas the apicalcoronal dimension of the interdentalpapilla capable of supporting complete root cover-age (224, 226). In a nonrotated/malpositioned tooth,the ideal height of the papilla was measured at thesame tooth with gingival recession, whereas in arotated/malpositioned tooth it was measured at thelevel of the homologous, contralateral tooth. Theideal height of the papilla was measured as the dis-tance between the point at which the cementoenamel junction crosses the facial mesialdistal lineangle of the tooth (the cementoenamel junctionangular point) and the contact point. The cementoenamel junction angular point is easily identiable,even in a tooth with noncarious cervical lesions, byelevating the interdental soft tissues (with a probe orsmall spatula) and searching for the interdental ce-mentoenamel junction. Once the ideal papilla wasmeasured, this dimension was replaced apically,starting from the tip of the mesial and distal papillaeof the tooth with the recession defect. The horizontalprojections on the recession margin of these mea-surements allowed the identication of two pointsthat were connected by a scalloped line, representingthe line of root coverage (Fig. 9). The maximal levelof root coverage was considered as the most apicalextension of the line of root coverage (221, 224, 226).Predetermination of the maximal level of root cover-age was used to select the treatment approach fornoncarious cervical lesions associated with gingivalrecessions: root coverage surgery was performedwhen the maximal level of root coverage was locatedat the level of, or coronal to, the most coronal step ofthe noncarious cervical lesions area: the need for aconnective tissue graft as an adjunct to the coronallyadvanced ap increases with increasing depth of thenoncarious cervical lesions and the proximity of themaximal level of root coverage to the coronal step ofthe abrasion defect. A restorative therapy before mu-cogingival surgery was indicated when the maximal
A B
Fig. 8. Criticisms of Millers classication of gingival reces-sion. (A, B) A noncarious cervical lesion may hide the ce-mentoenamel junction. When the cementoenameljunction is not recognizable, it is no longer possible tomeasure the depth (and width) of the recession, to assessthe prognosis and to evaluate the treatment outcome interms of root coverage.
Periodontal plastic surgery
339
-
level of root coverage was located within the abrasiondefect (using the restorativemucogingival approach).Conservative treatment (with or without access apsurgery) was performed when the maximal line ofroot coverage was located at the level or apical to themost apical extension of the abrasion area (221).
Indications for root coveragesurgical procedures
The treatment of gingival recession defects is indi-cated for esthetic reasons, to reduce root hypersensi-tivity and to create or augment keratinized tissue (36,48, 78, 136, 169, 203, 205). Indications for root cover-age procedures are root abrasion/caries and theinconsistency/disharmony of the gingival margin.
Esthetic reasons
The main indication for treatment of gingival reces-sions is patient demand. The excessive length ofthe tooth/teeth (i.e. those with recession) may beevident when smiling and sometimes duringphonation. Esthetic shortening of the tooth canonly be accomplished with root coverage surgicalprocedures.
Hypersensitivity
Sometimes the patient complains of hypersensitivityto thermal stimuli (especially to cold) at the level of
teeth affected by gingival recession. This is a cause ofdiscomfort and/or pain and can make proper oralhygiene very difcult to perform. If there is no con-comitant esthetic complaint related to the excessivetooth length, a less invasive (and patient-appreciated)treatment is the local application of chemical desen-sitizing agents. If this is not effective, a restorativetreatment (composite llings) may be performed. Ifand when dentine hypersensitivity is associated witha patient complaint about esthetics, treatment ofgingival recession should be surgical or combinedrestorativesurgical (e.g. a combined restorativemucogingival approach).
Keratinized tissue augmentation
The indication for treatment of gingival recessionmay also result from the site-specic patient dif-culty/inability to maintain adequate plaque controlbecause of the deep, narrow nature of the recessiondefect or the absence of keratinized tissue.
Root abrasion/caries
The indication for treatment of gingival recessionmay also derive from the concomitant presence ofroot demineralization/caries or deep abrasion defectsthat can cause hypersensitivity and/or may renderthe patients plaque control difcult. Treatment ofradicular caries/abrasion associated with gingivalrecession can be surgical or combined restorativesurgical, depending on the potential to cover with soft
A B C
Fig. 9. Predetermination of root coverage. (A) The idealpapilla is measured as the distance between the cementoenamel junction angular point and the contact point. Thisdistance is replaced apically starting from the tip of thepapillae. The horizontal projections of these measure-ments allow the identication of two points (blue points)that are connected by the line of root coverage. (B) This
line can be used as a guide for composite lengthening ofthe clinical crown. (C) Three months after root-coveragesurgery the soft-tissue margin is located at the level of, orslightly coronal to, the composite lling. Estheticallycomplete root coverage can be achieved, even in Class IIIgingival recessions. CAP, cemento-enamel junction angu-lar point; IP, interproximal.
Zucchelli & Mounssif
340
-
tissue, or not cover, the area affected by abrasion orcaries (see the prognosis of root coverage) (205).
Inconsistency/disharmony of gingivalmargin
Inconsistency/disharmony of the gingival marginmay be caused by the morphology of the gingivalrecession, even in the absence of dentin hypersensi-tivity, which may prevent the patient performing aneffective toothbrushing technique. This is especiallytrue when gingival recessions are isolated and deep,when they are very narrow with triangular-shape ver-tices (the so-called Stillman cleft) or when theyextend beyond the mucogingival junction. The onlyfeasible treatment is root coverage surgery.
Root coverage surgical procedures
The ultimate goal of a root coverage procedure iscomplete coverage of the recession defect with a goodappearance related to the adjacent soft tissues andminimal probing depth following healing (36, 48, 49,131, 169).Surgical procedures used in the treatment of reces-
sion defects may basically be classied as follows(115).Pedicle soft-tissue graft procedures:
Rotational ap procedures (laterally sliding ap,double papilla ap, oblique rotated ap);
Advanced ap procedures (coronally repositionedap, semilunar coronally repositioned ap);
Regenerative procedures (with barrier membraneor application of enamel matrix proteins)Free soft-tissue graft procedures:
Epithelialized graft; Subepithelial connective tissue graftThe international literature has thoroughly docu-
mented that gingival recession can be successfullytreated using several surgical procedures (205), irre-spective of the technique utilized, provided that thebiological conditions for accomplishing root coverageare satised (no loss in height of interdental soft andhard tissue) (131).The selection of one surgical technique over
another depends on several factors, some of whichare related to the defect (the size and number of therecession defects, the presence/absence, quantity/quality of keratinized tissue apical and lateral to thedefect, the width and height of the interdental soft tis-sue (papillae), the presence of frenum or muscle pulland the depth of the vestibulum), whereas others are
related to the patient (219). The esthetic request andthe need to minimize postoperative discomfort arethe most important patient-related factors to be con-sidered in the selection of the root coverage surgicalapproach. Furthermore, the clinician must considerdata from the literature in order to select the mostpredictable surgical approach, among those feasiblein a given clinical situation.In a patient with esthetic requests, pedicle ap sur-
gical techniques (coronally advanced or laterallymoved aps) are recommended if there is adequatekeratinized tissue apical or lateral to the recessiondefect (10, 32, 81, 83, 84, 187, 204). In these surgicalapproaches the soft tissue utilized to cover root expo-sure is similar to that originally present at the buccalaspect of the tooth with the recession defect and thusthe esthetic result is satisfactory. Furthermore, thepostoperative discomfort is minimal as second surgi-cal sites (palate) far from the tooth with the recessiondefect are not involved.Conversely, when the keratinized tissue apical or
lateral to the gingival defect is not adequate, free graftprocedures have to be performed (25, 96, 124, 130,133, 184, 190). The use of free gingival grafts to treatrecession defects in patients with esthetic requests isnot recommended because of the poor esthetic out-come and the low root coverage predictability (205).The use of a pedicle ap to cover the graft (i.e. the bi-laminar technique) improves the root coverage pre-dictability (by providing an additional blood supplyto the graft) and the esthetic result (through hidingthe white-scar appearance of the graft and maskingthe irregular outline of the mucogingival junction thatfrequently occurs after a free graft procedure) (8, 9,28, 29, 92, 112, 137, 163, 204). This paper will focus inparticular on those surgical procedures that havebeen reported to be more predictable in achievingroot coverage. From a clinical standpoint it can beuseful to classify them in root coverage surgical pro-cedures for single and for multiple recession-typedefects.
Pedicle soft tissue graft procedure forsingle recession defects
Coronally advanced ap
The coronally advanced ap procedure is a very com-mon approach for root coverage. This procedure isbased on the coronal shift of the soft tissues on theexposed root surface (10, 156). It is the technique ofchoice for the treatment of isolated gingival reces-sion. It is technically simple, well tolerated by thepatient [because the surgical area is limited and does
Periodontal plastic surgery
341
-
not require removal of tissue far from the tooth withthe gingival recession (palate)] and provides optimalresults from an esthetic point of view (Fig. 10). Theconditions required to perform the coronallyadvanced ap are the presence of keratinized tis-sue, apical to the root exposure, of an adequateheight (1 mm for shallow recessions and 2 mm forrecessions 5 mm) (57, 203) and thickness. The tech-nique was initially described by Norberg (138) andsubsequently reported by Allen & Miller (10).Recently, it was modied (57) using a trapezoidal apdesign and a splitfullsplit-thickness ap elevationapproach (Fig. 10). This technique resulted in a veryhigh mean percentage (99%) and complete (88%) rootcoverage at 1 year; these outcomes were similar (59,204, 217, 218), or even higher (6, 33, 155, 193), thanthose reported in the literature for other root cover-age procedures. The 3-year outcomes showed only aslight decrease compared with those at 1 year: 97% ofroot coverage and 85% of complete root coverage. Arecent systematic review (36) concluded that the cor-onally advanced ap procedure is a safe and predict-able root coverage surgical procedure for thetreatment of single type gingival recessions. Themean percentage and the percentage of completeroot coverage of the articles comprised in the system-atic review (36) are summarized in Table 1. The mod-ied coronally advanced ap (57) technique (Fig. 11)presented some clinical and biologic advantages over
the splitfullsplit-thickness ap elevation (219): thesplit-thickness elevation at the level of the wide(3 mm) surgical papilla provided anchorage andblood supply to the interproximal areas mesial anddistal to the root exposure. Furthermore, the partialthickness of the surgical papillae facilitated the nutri-tional exchanges between them and the underlyingde-epithelialized anatomical papillae and improvedthe blending (in terms of color and thickness) of thesurgically treated area with respect to the adjacentsoft tissues. The full-thickness elevation of the soft tis-sue apical to the root exposure conferred more thick-ness and some periosteum, and thus betteropportunity to achieve root coverage (18) to that por-tion of the ap residing over the exposed avascularroot surface. The more apical split-thickness ap ele-vation facilitated the coronal displacement of theap. Although the technique included vertical releas-ing incisions, these did not result in unesthetic scars.In fact, these incisions were beveled in such a waythat the bone and periosteal tissues were notincluded in the supercial cut and thus did not par-ticipate in the healing process. Another importantmodication of the present surgical technique, withrespect to the previously proposed techniques (10,150, 204), was that the coronal advancement of theap was not obtained by periosteal incisions, butrather by cutting the muscle insertions included inthe thickness of the ap. A deep incision (with the
A B C D E
Fig. 10. Predetermination of root coverage. (A) Lateralview of the same tooth shown in Fig. 9. The coronal step ofthe noncarious cervical lesion cannot be covered with thesoft tissues. (B) Enamel plastic and composite restorationnished at the level of the line of root coverage. (C) Theap is coronally advanced to cover in excess the compositeprole. Note the thickness of the coagulum that formsbetween the root surface and the coronally displaced soft
tissue. (D) The sling coronal suture anchored to the palatalcingulum permits precise adaptation of the ap marginaltissue to the convexity of the clinical crown restored incomposite. There is no space for coagulum exposure. (E)Two years after the root coverage procedure. The increasein buccal soft-tissue thickness, together with the compo-site lling, provides the treated tooth with good estheticsand a correct emergence prole.
Zucchelli & Mounssif
342
-
blade parallel to the bone) detached the lip musclefrom the periosteum and permitted the performanceof a supercial incision (with the blade parallel tothe lining mucosa) that allowed for coronal advance-ment of the ap. These incisions minimized lip ten-sion on the ap and permitted passive displacementof the ap soft-tissue margin in a coronal position. Afurther technical aspect that was considered criticalfor the success of the modied coronally advancedap procedure related to the coronal sling suture.The anchorage to the palatal cingulum permits pre-cise adaptation of the keratinized tissue of the ap tothe convexity of the crown of the treated tooth. Thisminimizes exposure of the coagulum, which formsbetween the soft tissue and the root exposure, to thedetrimental microbiological and traumatic agents ofthe oral environment. The increased stability of thecoagulum may play a role in preventing early apdehiscence and thus favor root coverage. The need
for a tight coronal adaptation of the keratinized tissueof the aps at the time of suturing (Fig. 12C,D) repre-sented another indication (221), together with theesthetic indication, for a composite reconstruction,before surgery, of the convexity of the tooth crowninterrupted by the presence of noncarious cervicallesions (Figs 9 and 12).A large increase in keratinized tissue height was
demonstrated after coronally advanced ap surgeryin the study by De Sanctis & Zucchelli (57) (Fig. 13):in fact, 3 years after the surgery, the mean increase ofkeratinized tissue was 1.78 mm, and this increase wasgreater in sites with deeper recession and a loweramount of residual keratinized tissue at baseline. Verysimilar results were obtained in a previous study eval-uating the 5-year outcomes of the coronally posi-tioned ap for multiple gingival recessions (218).Some hypotheses were made in an attempt to explainthe increase of keratinized tissue after coronally
Table 1. Mean root coverage and complete root coverage (%) with coronally advanced ap technique
Study Flap procedure Mean rootcoverage (%)
Complete rootcoverage (%)
da Silva et al. (54) Coronally advanced ap 68.8 11.0
P. Cortellini (unpublished data) Coronally advanced ap 62.0 Not available
Lins et al. (116) Coronally advanced ap 60.0 Not available
Leknes et al.(114) Coronally advanced ap 34.0 Not available
Modica et al. (135) Coronally advanced ap 80.9 58.3
Del Pizzo et al. (59) Coronally advanced ap 67.0 60.0
Spahr et al. (180) Coronally advanced ap 86.7 23.0
Castellanos et al. (41) Coronally advanced ap 62.2 36.3
Pilloni et al. (152) Coronally advanced ap 65.5 31.2
Woodyard et al. (212) Coronally advanced ap 67.0 33.3
de Queiroz Cortes et al. (56) Coronally advanced ap 55.9 23.1
Huang et al. (98) Coronally advanced ap 83.5 58.3
A B
Fig. 11. Coronally advanced ap. (A, B) Comparison of the smile before and after placement of a coronally advanced apat the level of the left upper canine. The esthetic outcome was satisfactory for the patient.
Periodontal plastic surgery
343
-
advanced ap surgery: the tendency of the mucogin-gival line, coronally displaced during the surgery, toregain its original, genetically determined position(5); or the capability of the connective tissue, derivingfrom the periodontal ligament, to participate in thehealing processes taking place at the dentogingivalinterface (107, 121, 149). The observation that theincrease in keratinized tissue height was greaterwhen, before surgery, there was a greater recessiondepth and narrower residual band of attached gingiva
apical to the defects seems to support the hypothesisof the tendency of the mucogingival junction toregain its genetically determined position. In fact,these were the clinical situations in which a greatercoronal displacement of the mucogingival line wasperformed during the surgery. The repositioning ofthe mucogingival line could also explain the great var-iability among patients (and studies) in the increaseof keratinized tissue height after coronally advancedap procedures. One can speculate that patient bio-
A B C D
Fig. 12. Coronally advanced ap surgical technique of thetooth shown in Fig. 11. (A) Baseline gingival recession. (B)Trapezoidal splitfullsplit ap elevation. Note the boneexposure apical to the bone dehiscence. The periosteumhas been left in that portion of the ap covering the avas-cular root surface. There is no bone exposure along thevertical releasing incisions to minimize keloid formation
after the healing process. (C) The ap has been coronallyadvanced and secured with interrupted sutures along thevertical releasing incisions and a coronal sling sutureanchored to the palatal cingulum. (D) At 2 years of followup, complete root coverage and an increase in keratinizedtissue height have been accomplished.
A B
C D
Fig. 13. Increase in keratinized tissue height after place-ment of a coronally advanced ap in different patient bio-types. (A) Gingival recession in a patient with an apicallocation of the mucogingival line (compare with healthytooth, i.e. the lateral incisor). (B) Three years after place-ment of a coronally advanced ap: the great increase inkeratinized tissue height could be ascribed to the tendencyof the mucogingival line to regain its genetically deter-
mined position. (C) Gingival recession in a patient with amore coronal location of the mucogingival line (see the lat-eral incisior). (D) Three years after placement of a coronal-ly advanced ap: the small increase in keratinized tissueheight could be explained with the lower excursion threatwhich the mucogingival line had to make to reach thegenetically determined position.
Zucchelli & Mounssif
344
-
type might inuence the increase in keratinized tissueafter surgery: patients with a more apical position ofthe mucogingival line will experience a greaterincrease of keratinized tissue height after coronallyadvanced ap surgery relative to patients with a morecoronal location of the mucogingival junction. Ran-domized comparative clinical trials of differentpatient biotypes are advocated to test this hypothesis.Recently, Pini Prato et al. (157) evaluated, in a long-term 14-year randomized split-mouth study, theoutcomes of two different methods of root-surfacemodications (root-surface polishing compared withroot planing) used in combination with a coronallyadvanced ap performed for the treatment of singletype gingival recessions. The authors (157) observedthat, during the 14-year follow-up period, an apicalshift of the gingival margin occurred in 39% of thepatients treated in both groups, showing a progres-sive worsening of the gingival recessions with time.The observed relapse of the soft-tissue defects couldbe ascribed to a resumption of traumatic toothbrush-ing habits in patients with high levels of oral hygiene,even if they were included in a stringent maintenanceprotocol with recall every 46 months. Regarding thekeratinized tissue width, the results of Pini Prato et al.(157) showed its tendency to decrease over time.The same authors (162) evaluated the outcomes ofcoronally advanced ap for the treatment of singlegingival recessions in another long-term 8-year caseseries study. They reported that an apical shift of thegingival margin occurred in 53% of the cases and thatthis was associated with a reduction of keratinized tis-sue; furthermore, the baseline amount of keratinizedtissue was indicated as a prognostic factor for reces-sion reduction: the greater the width of keratinizedtissue, the greater the reduction of the recession.The main contraindications for performing the cor-
onally advanced ap as a root coverage procedure arethe absence of keratinized tissue apical to the reces-sion defect, the presence of a gingival cleft (Stillmancleft) extending into the alveolar mucosa, high frenu-lum pull at the soft-tissue margin, deep root-structureloss, buccally dislocated root and a very shallow ves-tibulum depth.
Laterally repositioned (rotational) ap
The laterally repositioned ap is advocated when thelocal anatomic conditions may render the coronallyadvanced ap contraindicated. It is not the techniqueof choice in patients with high esthetic demands (asscar tissue forms in the secondary intention healingat the donor site) but it is well accepted by the patientbecause it does not involve the withdrawal of tissuefrom a distant area (the palate) and has an excellentpostoperative healing course. In the literature, mostreports on the laterally repositioned ap techniqueare quite dated. Various authors suggested severalmodications to the original laterally sliding apdescribed by Grupe & Warren in 1956 (82) in order toreduce the risk of gingival recession at the donor site:Stafleno (181), proposed the use of a partial-thick-ness ap, instead of a full-thickness ap, to cover theroot exposure. Grupe, in 1966 (81), suggested per-forming a submarginal incision at the donor site inorder to preserve the marginal integrity of the toothadjacent to the recession defect. Ruben et al., in 1976(171), introduced a mixed-thickness ap that con-sisted of a full-thickness ap, performed close to therecession defect for covering the root exposure, and asplit-thickness ap created laterally to the full-thick-ness ap, for covering the bone exposure occurring atthe donor site of the full-thickness ap. The mostrecent publication, before 2004, on the laterally repo-sitioned ap as a root coverage surgical technique,dates back to 1988 (143). The reason for the lack of amore recent interest is related to the low predictabil-ity and efcacy of the laterally repositioned ap as aroot coverage surgical procedure. In the literature,the reported mean percentage of root coverageranges between 34% and 82% (31, 33, 65, 84, 109, 142,171, 199, 215). Complete root coverage data are lack-ing, with only one study (31, 143) (Table 2) reportingdata ranging between 40% and 50%. All techniquesreported in the literature consisted of the lateral shiftof the pedicle ap only. More recently, Zucchelli et al.(217) suggested a modication of the surgicalapproach, which added coronal advancement to thelateral movement of the pedicle ap (laterally moved
Table 2. Mean root coverage and complete root coverage (%) with laterally repositioned ap technique
Study Flap procedure Mean rootcoverage (%)
Complete rootcoverage (%)
Oles et al. (143) Laterally repositioned ap Not available 40.050.0
Zucchelli et al. (217) Laterally repositioned ap 96.0 80.0
Chambrone & Chambrone (44) Laterally repositioned ap 93.8 62.5
Periodontal plastic surgery
345
-
coronally advanced ap) (Figs 14 and 15). In thisstudy, precise measurements of the keratinized tissuelateral to the root exposure were requested: themesialdistal dimension was 6 mm more than thewidth of the recession measured at the level of the ce-mentoenamel junction, whilst the apicalcoronaldimension was 3 mm more than the facial probingpocket depth of the adjacent donor tooth. The mainsurgical modications (Figs 14 and 15) consisted ofthe different thickness during ap elevation; split atthe level of the surgical papillae, full in that portion ofthe ap covering the avascular root surface and splitagain apical to the mucogingival line; the deep andsupercial cuts of the muscle insertions to permitcoronal advancement of the ap; the de-epithelializa-tion of the anatomical papillae to provide coronalanchorage to the surgical papillae of the ap; and thecoronal sling suture anchored to the palatal cingulumof the treated tooth. This technique resulted in a veryhigh mean percentage of root coverage (96%), andcomplete root coverage was accomplished in thegreat majority (80%) of patients treated. A recent
24-month study (44) assessed the clinical resultsobtained with full-thickness laterally positioned apand citric acid root conditioning for the treatment oflocalized gingival recession; the mean percentage ofroot coverage was 94% and complete root coveragewas 63%. The laterally moved coronally advanced apis mainly indicated for the treatment of deep singletype gingival recession defects affecting a lower inci-sor (Fig. 14) or the mesial root of the upper rst molar(Fig. 15). In the latter case the presence of very deepbone dehiscence must be expected. Graft techniqueswould require withdrawal of a very large (in apicalcoronal dimension and thickness) amount of tissuefrom the palate, with an unpleasant postoperativecourse for patients.
Regenerative procedures
Barrier membranes
Guided tissue regeneration with resorbable and non-resorbable membranes has been used for the treat-ment of gingival recessions. This procedure has been
A B C D
Fig. 14. Laterally moved coronally advanced ap. (A) Base-line gingival recession affecting a buccally dislocated lowerlateral incisor. The keratinized tissue mesial to the rootexposure was adequate in width and height. (B) Splitfullsplit ap elevation, de-epithelialization of the receivingbed and root treatment. (C) The ap has been coronallyadvanced and the keratinized tissue secured to the de-epi-
thelialized anatomic papillae with the sling sutureanchored to the lingual cingulum. Equine-derived collagen(gingistat) was sutured to cover the secondary intentionwound-healing donor area. (D) At 1 year of follow up.Complete root coverage and increase in keratinized tissueheight have been accomplished. Scar tissue formed in thedonor site.
A B C D
Fig. 15. Laterally moved coronally advanced ap. (A) Base-line gingival recession affecting the mesial root of an upperrst molar. The keratinized tissue distal to the root expo-sure is adequate in width and height. (B) Splitfullsplitap elevation and de-epithelization of the receiving bed.
Note the depth of the bone dehiscence. Graft techniqueswould require large withdrawal from the palate. (C) Theap has been coronally advanced and sutured. (D) At1 year of follow-up. Root coverage and a large increase inkeratinized tissue height have been accomplished.
Zucchelli & Mounssif
346
-
shown to offer a predictable modality for root cover-age (158, 188, 189), especially in deep recessions,resulting in the regeneration of new connective tissueattachment and bone. The root coverage obtained bypolytetraethylene membranes or bioresorbable mem-branes ranges from 54% to 87% (with a mean of 74%).However, the use of the membrane technique alsoresulted in several problems such as membrane expo-sure and contamination, technical difculties in plac-ing the barrier and possible damage of the newlyformed tissue as a result of membrane removal orabsorption. Furthermore, recent literature (36, 48,124) shows that the use of a barrier membrane, inconjunction with a coronally advanced ap, does notimprove the result of the coronally advanced apalone in terms of complete root coverage and reces-sion reduction. At present, the use of a barrier mem-brane for root coverage procedures appears to beinadvisable, especially considering the high incidenceof complications (i.e. membrane exposure) (11, 102,116, 187, 194).
Enamel matrix derivate
Enamel matrix derivative, in combination with a cor-onally advanced ap, was introduced to treat gingivalrecession (135) with the double objective of enhanc-ing root coverage results and inducing periodontalregeneration (59). Recent literature reviews (36, 47,169) showed that enamel matrix derivative, in con-junction with a coronally advanced ap, improvedthe percentage of complete root coverage, increasedkeratinized tissue height and provided better reduc-tion of recession. Histological studies are contradic-tory, reporting either predominant attachmentconsisting of collagen bers running parallel to theroot surface without new cementum or Sharpeysbers (39) and with new bone and new cementumforming only in the most apical portion of root sur-face, or periodontal regeneration with connective tis-sue attachment, new bone and new cementum (127,165). The true clinical rationale to choose thisapproach with respect to the coronally advanced apalone or other techniques is unclear; thus, routineuse of enamel matrix derivative associated with a cor-onally advanced ap is not recommended. One mayspeculate that the application of enamel matrix deri-vative during mucogingival surgery may be recom-mended in situations in which a wider extension ofnew attachment formation between the soft tissueand the root surface could be of clinical relevance.This may be a result of the size of root exposure (avery wide and deep recession defect), or the toothposition (buccally dislocated root) or a concomitant
buccolingual attachment and bone loss (see histo-logical healing after root coverage surgery). Clinicaland histological studies are advocated to conrmsuch a hypothesis.
Free soft-graft procedures
Epithelialized graft
The free gingival graft is the most widely used surgicaltechnique for increasing the width of attached gin-giva. Nevertheless, several authors (20, 23, 151, 166)observed a low degree of predictability of favorableresults with this technique in the coverage of exposedroot surfaces. In fact, a portion of the graft placed onthe denuded root surface does not receive an ade-quate blood supply, with consequent partial necrosisof the grafted tissue. The literature on free gingivalgrafts is contradictory and reports percentages of rootcoverage ranging from 11% to 100% (22, 27, 96, 100,101, 123125, 130, 133, 145, 176, 190). This variationmay be attributed to differences in the severity of thegingival lesion and in surgical techniques. Nowadays,free autogenous gingival grafts are the last resortwhen the main goal is root coverage or particularly tomeet the esthetic demands of patients. An unfavor-able esthetic outcome is related to incomplete rootcoverage, the white-scar appearance of the graftedtissue that contrasts with the adjacent soft tissues andthe malalignment of the mucogingival line. Free gin-gival grafts can still be used when the main goal ofthe surgical procedure is to augment keratinized tis-sue height (especially in mandibular incisors withoutattached gingiva and with aberrant frenuli), the thick-ness of gingival tissue and the vestibulum depth.When used for root coverage purposes (Fig. 16), thegraft should be sutured coronally to the cementoenamel junction (to compensate for soft-tissueshrinkage); its thickness should be >1 mm (toincrease root coverage predictability) (3, 190); and itshould be adapted to the convexity of the crown (tominimize coagulum exposure and destabilization).The free gingival graft is contraindicated in patientswith esthetic demands, in deep and wide recessiondefects and in the presence of deep facial probingpockets associated with gingival recession. Freeautogenous gingival grafts can be used as the rst sur-gical procedure in the two-stage technique describedby Bernimoulin et al. in 1975 (20). This consists of arst stage of surgery, in which a free gingival graft isperformed to increase the keratinized tissue heightapical to the gingival recession, and a second stage inwhich the grafted tissue is coronally advanced tocover the exposed root surface (Fig. 17). A mean per-
Periodontal plastic surgery
347
-
centage of root coverage ranging from 65% (31, 123)to 72% (155) was reported for the two-stagetechnique. This procedure is not well accepted by the
patient because of the two surgical stages. However,there could be a combination of unfavorableconditions at the tooth with gingival recession that
BA
C D
Fig. 16. Free gingival graft for root coverage. (A) Shallowgingival recession affecting a lower incisor with absence ofkeratinized tissue apical to the exposed root. (B) Suture ofthe graft. Two coronal interrupted sutures are used toanchor the graft to the base of the papillae. Two apicalinterrupted sutures stabilize the graft to the periosteumand adjacent soft tissue. A compressive horizontal mat-tress suture is anchored to the periosteum apical to the
graft and suspended around the lingual cingulum. (C) Thethickness of the graft must exceed 1 mm. No space shouldbe left between the graft and the convexity of the toothcrown. (D) At 1 year of follow up. Complete root coverageand a signicant increase in keratinized tissue height havebeen accomplished. Note the difference in color betweenthe grafted area and the adjacent soft tissue, and the mal-alignment of the mucogingival line.
A B
C D
Fig. 17. Two-stage surgical technique for root coverage.(A) A free gingival graft was positioned apical to a deepgingival recession defect affecting a lower central incisor;the image shows the graft after 3 months of healing. Notethat the mesialdistal length of the graft has been extendedin order to improve the quality/quantity of keratinized tis-sue of the adjacent central incisor. (B) Second-stage coro-nally advanced surgery: the grafted tissue has beenelevated; only the root of the affected tooth has been
mechanically treated and the receiving bed has been de-epithelized. (C) The grafted tissue has been coronallyadvanced and sutured with interrupted sutures along thevertical-releasing incisions and a double sling suture hasbeen anchored to the lingual cinguli of the treated teeth.(D) One year of follow up. Root coverage and an increasein keratinized tissue height have been accomplished inboth teeth. Note the difference in color between the graftedarea and the adjacent soft tissue.
Zucchelli & Mounssif
348
-
render this technique as indispensable: the lack ofkeratinized tissue apical and/or lateral to the rootexposure; gingival cleft extending beyond the muco-gingival line; and the presence of a shallow vestibu-lum depth. A recent case report (220) introduced amodied two-stage surgical procedure aiming toimprove the esthetic outcome and reduce thepatients morbidity. The main modication of therst stage of surgery consisted of harvesting a freegingival graft of the same height as the keratinizedwidth of the adjacent teeth and suturing it on theperiosteum apical to the bone dehiscence. During thesecond stage of surgery the coronal advancement ofthe grafted tissue led to root coverage and realign-ment of the mucogingival line. Zucchelli and DeSanctis (220) showed that by minimizing the apicalcoronal dimension of the free graft and standardizingthe surgical techniques, successful results (in terms ofroot coverage, increase in keratinized tissue andachieving a color similar to that of the adjacent softtissues) could be obtained in the treatment of gingivalrecessions characterized by local conditions, whichotherwise preclude, or render unpredictable, the useof one-step root coverage surgical techniques. Ran-domized controlled studies are advocated to test theefcacy and predictability of the two-stage root cov-erage surgical technique.
Subepithelial connective tissue graft (bilaminartechnique)
The recent literature indicates the bilaminar tech-niques as the most predictable root coverage surgicalprocedures (36, 4749, 51, 141, 169, 205). The biologi-cal rationale for these techniques is to provide thegraft with an increased blood supply from the cover-ing ap. This will increase the survival of the graftabove the avascular root surface (112) and improvethe esthetic outcome by hiding, partially or com-pletely, the white-scar appearance of the grated tis-sue. The mean percentage and the percentage ofcomplete root coverage in the articles of the system-atic review of Cairo et al. (36) are summarized inTable 3. During the last two decades clinicians haveintroduced several modications to the original bila-minar technique described (163), resulting in morepredictable outcomes, in terms of root coverage, andgreater esthetic satisfaction for patients. These modi-cations were related to the type of graft (partially orcompletely de-epithelialized) harvested from the pal-ate and to the design (envelope type or with a verticalreleasing incision) of the covering ap. Some authorsused an envelope ap (8, 163) or a repositioned ap(112) to partially cover epithelial connective tissue
grafts. Others utilized coronally advanced aps, with(137, 204) or without (29) vertical releasing incisions,or a laterally moved papillae ap (92) to coverconnective tissue grafts. In all surgical approachesreported, the size of the graft exceeded that of thebone dehiscence and it was positioned (and sutured)at the level of, or mainly coronal to, the cementoenamel junction. Although root coverage becameincreasingly more predictable, the esthetic appear-ance of the surgically treated area was often differentfrom that of the adjacent soft tissues. This was causedby the chromatic difference between the uncoveredepithelialized portion of the graft and the adjacentsoft tissues (8, 112, 163), the dischromy associatedwith partial exposure of the connective tissue graft asa result of early dehiscence of the covering ap (29,137, 204), or the difference in thickness between thegrafted area and adjacent soft tissues. More recently,in a comparative study by Zucchelli et al. (216), a fur-ther modied approach was proposed to improve theesthetic outcome of the bilaminar root coverage pro-cedure (Fig. 18). The main surgical modicationsrelated to the size and positioning of the connectivetissue graft: the apicocoronal dimension of the graftwas equal to the depth of the bone dehiscence (mea-sured from the cementoenamel junction to the mostapical extension of the buccal bone crest) minus thepreoperative height of keratinized tissue apical to therecession defect. The thickness of the graft was
-
crowns or implants. Contradictions for the bilaminartechniques are those anatomic situations limiting thepossibility to perform pedicle covering aps (mar-ginal frenuli, high muscle pull, gingival cleft extendingin alveolar mucosa and a very shallow vestibulumdepth), especially when these unfavorable conditions,in fact, occur more frequently in the lower incisionszone.
Connective tissue graft-harvesting procedures
Different connective tissue graft-harvesting proce-dures, with the purpose of achieving primary inten-tion palatal wound healing, have been described inthe literature: the most common are the trap-doorprocedures (60) and the envelope techniques withsingle (99, 118) or double (29) incisions. These pro-cedures have the following common characteristics:
a primary split-thickness access ap elevation; thewithdrawal of connective tissue graft; and completeclosure of the palatal wound with the access ap.The primary objective of these techniques is toreduce patient morbidity by obtaining primary clo-sure of the wound and primary intention healing;however, they need an adequate thickness of thepalatal bromucosa to avoid desquamation of theundermined supercial ap as a result of compro-mised vascularization (60, 101, 112). The free gingi-val graft surgical wound heals by secondaryintention within 24 weeks (67) and has been con-sistently associated with greater discomfort for thepatient as a result of postoperative pain and/orbleeding (58, 67, 101). However, this technique iseasy to perform and can be utilized even in thepresence of a thin palatal bromucosa.
Table 3. Mean root coverage and complete root coverage (%) with subepithelial connective tissue graft plus coronallyadvanced ap technique
Study Flap procedure Mean rootcoverage (%)
Complete rootcoverage (%)
Zucchelli et al. (216) Subepithelial connective tissue graftplus coronally advanced ap
80.0 97.0
da Silva et al. (54) Subepithelial connective tissue graftplus coronally advanced ap
75.3 18.1
P. Cortellini (unpublished data) Subepithelial connective tissue graftplus coronally advanced ap
76.0 Not available
Jepsen et al. (102) Subepithelial connective tissue graftplus coronally advanced ap
86.9 Not available
Trombelli et al. (194) Subepithelial connective tissue graftplus coronally advanced ap
81.0 Not available
Borghetti et al. (26) Subepithelial connective tissue graftplus coronally advanced ap
76.0 28.6
Tatakis & Trombelli (186) Subepithelial connective tissue graftplus coronally advanced ap
96.0 83.0
Romagna-Genon (170) Subepithelial connective tissue graftplus coronally advanced ap
84.8 Not available
Wang et al. (201) Subepithelial connective tissue graftplus coronally advanced ap
84.0 43.7
McGuire & Nunn (128) Subepithelial connective tissue graftplus coronally advanced ap
93.8 79.0
Aichelmann-Reidy et al. (4) Subepithelial connective tissue graftplus coronally advanced ap
74.1 Not available
Paolantonio et al. (146) Subepithelial connective tissue graftplus coronally advanced ap
88.8 46.6
Tal et al. (185) Subepithelial connective tissue graftplus coronally advanced ap
88.7 42.8
Joly et al. (104) Subepithelial connective tissue graftplus coronally advanced ap
79.5 Not available
Wilson et al. (210) Subepithelial connective tissue graftplus coronally advanced ap
64.4 Not available
Zucchelli & Mounssif
350
-
The evidence in the literature evaluating differ-ences in patient outcomes and morbidity followinguse of the connective tissue graft and free gingivalgraft for root coverage procedures, is minimal. A fewprospective comparative studies (58, 80, 207) reportedpoorer patient outcomes, specically a greater inci-dence of postoperative pain, for free gingival graftscompared with connective tissue graft procedures.Recently, a clinical randomized controlled study (223)was performed to compare the postoperative morbid-ity and root coverage outcomes in patients treatedwith trap-door connective tissue (control group) andepithelialized (test group) graft-harvesting techniquesfor the treatment of gingival recession using the bila-minar procedure. In the test group the connective tis-sue graft was obtained after de-epithelialization ofthe epithelialized graft with a scalpel blade. No statis-tically signicant differences in painkiller consump-tion, postoperative discomfort and bleeding(recorded using the visual analog scale) were foundbetween the two groups. By contrast, necrosis of theprimary ap in the control patients resulted in a six-fold increase of the intake of anti-inammatorydrugs. The reasons for the lack of differences betweenthe two patient groups are open to speculation; how-ever, a possible explanation may be found in the sur-gical techniques and, in particular, in the reduceddimensions of the graft or in the protection of thewound area with equine-derived collagen in the testgroup. At present, study data demonstrate that theheight (the apicalcoronal dimension) and depth ofthe harvesting graft, but not the type (primarycompared with secondary) of palatal wound healing
inuence postoperative analgesic consumption. Theresults of the study also indicate that both types ofconnective tissue graft can be successfully used undera coronally advanced ap to cover gingival recession,with no statistically signicant difference in rootcoverage outcomes between the grafts. One yearpost-treatment, 92% of the control gingival defectsand 97% of the test gingival recessions were coveredwith the soft tissue. Furthermore, complete rootcoverage was achieved in 70% of the controls and in85% of the test subjects. The only statistically signi-cant difference in the clinical outcomes between thetwo treatment groups was the greater increase ingingival thickness in the patients treated with thede-epithelialized graft. Any attempt to explain thisdifference is speculative in nature, but it may berelated to the better quality (greater stability and lessshrinkage) of the more supercial connective tissueresulting from the de-epithelialization of a free gingi-val graft with respect to the deeper connective tissueharvested using the trap-door approach (223).
Surgical procedures for multiplerecession defects
Gingival recession is rarely localized to a single tooth,and no reports are available on the prevalence of sin-gle recession defects compared with multiple reces-sion defects; nevertheless, clinical experienceindicates a greater incidence of multiple gingivalrecessions (219). In the presence of multiple defects,the attempt to reduce the number of surgeries andintraoral surgical sites, together with the need to sat-
A B C D E F
Fig. 18. Bilaminar technique for root coverage. (A) Gingi-val recession affecting a buccally prominent upper canine(lateral view). (B) A small (
-
isfy the patients esthetic demands, must always betaken into consideration. Thus, when multiple reces-sions affect adjacent teeth they should be treated atthe same time and, if possible, the removal of soft tis-sue from distant areas of the mouth (palate) shouldbe minimized to reduce patient discomfort (46).To date, extensive evidence reports positive out-
comes following the use of root coverage proceduresin the treatment of localized gingival recessions (36,48), whilst few studies are currently available report-ing the outcomes for the treatment of multiple gingi-val recessions (46, 154, 218, 222). The coronallyadvanced ap for multiple recessions was introducedby Zucchelli & De Sanctis (219) as a novel approachto treat more than two adjacent teeth with gingivalrecession. This technique (Fig. 19) comprises anenvelope type of ap (with no vertical releasing inci-sions); an innovative ap design that anticipates therotational movement of the surgical papillae duringthe coronal advancement of the ap; a split (at thelevel of the surgical papillae) full (at the soft tissueapical to the root exposure) split (apical to boneexposure) approach during ap elevation; a doubleincision (one to dissect muscle insertions from theperiosteum and the other to cut muscle from theinner connective tissue lining the mucosa of the ap)to permit coronal advancement of the ap; thede-epithelization of the anatomic papillae; and a vari-ous number of sling sutures anchored to the palatal
cingulum of the treated teeth. This case series reported97.1 5.1% mean root coverage and 88.6 20.3%complete root coverage (219). A long-term study(5 years) (218) conducted by the same authorsreported stability of the successful outcomes obtainedat 1 year of evaluation: 94% of the root surfaces ini-tially exposed by gingival recession were still coveredwith soft tissue and 85% of the treated recessiondefects showed complete coverage (218).A recent systematic review (46) evaluated the
results obtained with different root-coverage proce-dures in the treatment of multiple recession typedefects; only four studies were included in this paper:coronally advanced ap (218); coronally advancedap plus subepithelial connective tissue (42, 45); andsubepithelial connective ap with a modied coro-nally advanced ap (40). A mean percentage of rootcoverage of 96% was reported, with 73% of completeroot coverage. The authors concluded that all theperiodontal plastic surgery procedures evaluated (i.e.a coronally advanced ap, either alone or in combi-nation with a subepithelial connective tissue graft)led to improvements in recession depth, clinicalattachment level and width of keratinized tissue; fur-ther multicenter studies may be required to increasethe number of patients and to achieve adequatestatistical power.A recent randomized clinical trial comparing coro-
nally advanced ap, with or without vertical releasing
A B C
D E F
Fig. 19. Coronally advanced ap for multiple gingivalrecessions. (A) Multiple gingival recessions affecting theanterior teeth in a patient with esthetic demands. Coron-ally advanced ap surgeries, in the right and left uppersides, were performed. (B) Baseline clinical situation in therst quadrant. (C) An envelope ap from the central inci-sor to the rst molar was elevated using a splitfullsplitapproach. The papillae are de-epithelialized. (D) The apwas anchored coronal to the cementoenamel junctions of
all teeth present in the ap design using sling suturesanchored to the palatal cinguli. (E) One year of follow up.Complete root coverage has been achieved in all treatedteeth. An increase in the height of the buccal keratinizedtissue can be observed. (F) One year after the same coro-nally advanced ap treatment of the gingival recessionsaffecting teeth of the second quadrant. Complete rootcoverage and good esthetic outcome were achieved in alltreated teeth.
Zucchelli & Mounssif
352
-
incisions, for the treatment of multiple recession, didnot report differences in terms of the mean percent-age of root coverage between both approaches (222).However, the envelope type of coronally advancedap was associated with an increased probability ofachieving complete root coverage and with a greaterincrease of buccal keratinized tissue height. Patientsatisfaction with esthetics (overall satisfaction, colormatch and amount of root coverage) was very highfor both treatments, with no signicant differenceobserved between them; better results, in terms ofpostoperative healing and esthetic evaluation, asjudged by an independent expert periodontist, wereobtained for patients treated with the envelope typeof coronally advanced ap. Keloids, which may formalong the vertical releasing incisions, were responsi-ble for the worst esthetic evaluation made by theexpert periodontist (222).The coronally advanced ap for multiple gingival
recessions should not be considered only as a rootcoverage surgical procedure but also as a coveringap for connective tissue grafts (subepithelial con-nective tissue graft) should the keratinized band oftissue apical to the root exposure for root coveragebe absent or inadequate (Fig. 20). This inadequacymay be a result of the small height and/or thicknessof the keratinized tissue itself or the presence ofdeep root abrasion (221) or root prominence. Verylittle data are available on the effectiveness of sub-epithelial connective tissue grafts in the treatment
of multiple recessions (40, 45) and only two long-term studies have been published (155, 225). Thistrial compared the clinical outcomes of coronallyadvanced ap alone with those of coronallyadvanced ap plus connective tissue graft in thetreatment of multiple gingival recessions with5 years of follow-up. Six months after surgery, nostatistically signicant difference between coronallyadvanced aps plus connective tissue grafts andcoronally advanced aps alone was reported interms of recession reduction and complete root cov-erage. A different trend was noted over time at the6-month and 5-year follow-up time points. A slightcoronal shift of the gingival margin occurred in thecoronally advanced ap plus connective tissue graft,whilst a slight apical shrinkage of the margin wasobserved in the coronally advanced ap group(154). The progressive coronal improvement of thegingival margin level and the increased percentageof sites with complete root coverage observed at5 years in the sites treated with coronally advancedap plus connective tissue graft were explained withthe creeping attachment effect over time (124).According to the authors, this effect was facilitatedby the thick gingival tissue obtained after healing ofthe connective tissue graft (154). Conversely, theapical shift of the gingival margin of the coronallyadvanced ap-treated sites at 5 years was ascribedto the lower thickness/amount of keratinized tissueachieved (36), leading to possible apical relapse of
A B
C D
Fig. 20. Coronally advanced ap plus connective tissuegraft for multiple gingival recessions. (A) Multiple gingivalrecessions in a patient with esthetic demands. (B) An enve-lope ap from the central incisor to the rst molar was ele-vated using a splitfullsplit approach. A de-epithelizedconnective tissue graft was sutured at the level of thecanine and rst premolar, teeth with smaller amounts ofresidual buccal keratinized tissue. (C) The ap wasanchored coronal to the cementoenamel junctions of all
teeth present in the ap design using sling suturesanchored to the palatal cinguli. (D) One year of follow up.Complete root coverage has been achieved in all treatedteeth. An increase in the height of the buccal keratinizedtissue can be observed in all treated teeth. The increase insoft-tissue thickess was greater for the teeth treated withthe adjunct of connective tissue graft. There was no sign ofgraft exposure.
Periodontal plastic surgery
353
-
the gingival margin during the maintenance phase.These data underline, to an even greater extent, theimportance of renewing (refreshing) patient motiva-tion for plaque control and an atraumatic tooth-brushing technique in the rst year(s) postsurgery.Data of the study carried out by Pini Prato et al.(154) could be interpreted as showing that theadjunct use of connective tissue does not reallyimprove the surgical outcomes (until 6 months)compared with the coronally advanced ap proce-dure alone, but facilitates long-term patient mainte-nance. A recent randomized controlled trial (225)compared short-term (6 months and 1 year) andlong-term (5 years) clinical and esthetic outcomesof the coronally advanced ap, with and withoutconnective tissue grafts, in the treatment of multiplegingival recessions. The authors (225) showed that,in patients with high standards of oral hygiene andundergoing a very strict regimen of postsurgicalcontrol visits, both techniques were effective inreducing recession depth and achieving completeroot coverage at 6 months and 1 year, with no sta-tistically signicant differences between these timepoints. Better results, in terms of postoperativecourse and color-match evaluation made by anindependent expert periodontist, were obtained inpatients treated with the coronally advanced approcedure. Conversely, the coronally advanced applus connective tissue graft procedure was associ-ated with an increased probability of obtainingcomplete root coverage at 5 years. Further investi-gations are advocated.
Tunnel technique
The tunnel procedure for root coverage was intro-duced in 1994 and termed the supraperiosteal enve-lope technique (8, 9). The unique characteristic ofthis procedure is that the interdental papillae are leftintact. A connective tissue graft is placed in the tunneland it does not need to be completely covered as longas the dimension of the graft is sufcient to ensuregraft survival. An advantage of not covering the graftcompletely is that additional keratinized tissue isgained, whereas a disadvantage is that the exposedtissue might not be an exact color match. Conversely,the absence of vertical incisions has a tendency toproduce better esthetics. Probably the main advan-tage of the technique is the minimally invasive natureof the surgery, which results in negligible postopera-tive discomfort at the recipient site. Recently, the tun-nel technique was modied to include coronalpositioning of the marginal tissue, which allows com-plete coverage of the graft (E. P. Allen, Center forAdvanced Dental Education, Dallas, Texas; coursemanual) (Fig. 21). This was accomplished by dissect-ing more deeply to free up the facial tissue and by lift-ing the papillae off the interproximal septum fromthe facial and lingual aspects. These two featuresallow greater coronal mobilization of the tissue mar-gin. Successful execution of the technique requiresalmost a microsurgical approach, using smaller, spe-cially designed instruments, small sutures and aunique suturing technique. Aroca et al. (14) tested, ina controlled randomized split-mouth study, the ef-
A B C
D E F
Fig. 21. (A) Baseline. Multiple Miller Class 1 recessions.(B) Use of the tunnel instrument to completely mobilizethe ap. (C) The ap was completely mobilized. Notethat a tension-free ap was obtained. (D) The palatalconnective tissue graft was placed in the tunnel and xedwith mattress and sling sutures. (E) The tunnel was
sutured coronally to the cementoenamel junction insuch a way that the connective tissue graft and the reces-sion defects were completely covered. (F) At 12 monthsfollowing surgery, complete coverage of the recessionswas achieved. Courtesy of Anton Sculean (University ofBern).
Zucchelli & Mounssif
354
-
cacy of a modied tunnel plus connective tissue grafttechnique in the treatment of multiple Class III gingi-val recessions. The data showed predictable results at1 year (14). Recently, the same author (15), in asplit-mouth randomized controlled trial, showed thendings of treatment of Miller Class I and II multipleadjacent gingival recessions with a modied coronallyadvanced tunnel technique in conjunction with aconnective tissue graft. At 12 months this techniqueresulted in statistically signicant improvements incomplete root coverage (85%), mean root coverage(90 18%) and mean keratinized tissue width(2.7 0.8 mm) compared with baseline (P < 0.05).The favorable root coverage results of the tunnel pro-cedure and its modication are summarized inTable 4.
Allograft
The subepithelial connective tissue graft is a predict-able and versatile technique in which a bilaminar vas-cular environment is created to nourish the graft.However, harvesting the palatal area increases post-operative morbidity and is time consuming (104). Theneed for a second surgical procedure to harvest donortissue is a disadvantage of the connective tissue graftprocedure because only a limited amount of donortissue is available for multiple recession defects. Thus,there has been a desire to nd a substitute for theautogenous donor tissue (19). As a response, acellulardermal matrix graft has been used as a substitute forconnective tissue grafts in root coverage procedures(Fig. 22). The acellular dermal matrix graft is a dermalallograft processed to extract cell components andthe epidermis, whilst maintaining the collagenous
scaffolding (43). The remaining dermal layer iswashed in detergent solutions to inactivate virusesand to reduce rejection and then is cryoprotected andrapidly freeze dried in a proprietary process topreserve its biochemical and structural integrity. Theallograft acts as a scaffold for the vascular endothelialcells and broblasts to repopulate the connective tis-sue matrix and encourage the epithelial cells tomigrate from the adjacent tissue margins (211). Thehealing process observed in the allograft is similar tothat seen in autogenous grafts (178, 183, 184). Similarroot coverage outcomes have been reported in sev-eral studies (4, 36, 48, 52, 56, 70, 95, 104, 139, 141, 146,212) that compared coronally advanced aps plusacellular dermal matrix grafts with coronallyadvanced aps plus connective tissue grafts.Recent systematic reviews (36, 48) did not show a
statistically signicant difference between the coro-nally advanced ap plus the acellular dermal matrixgraft compared with the coronally advanced apalone in terms of complete root coverage, recessionreduction and keratinized tissue gain, suggesting noadditional benet with the use of the acellular der-mal matrix graft. Surprisingly, even the comparisonbetween coronally advanced ap plus acellular der-mal matrix graft and coronally advanced ap plusconnective tissue graft showed no statistically signi-cant differences for complete root coverage andrecession reduction, even though a tendency favor-ing connective tissue grafts was observed for bothvariables. A statistically signicant difference in gainof keratinized tissue was detected with use of theconnective tissue graft. Furthermore, a meta-analy-ses of two studies (52, 212) showed large heterogene-ity in recession reduction for both comparisons
Table 4. Mean root coverage and complete root coverage (%) with subepithelial connective tissue graft plus tunneltechnique
Study Flap procedure Mean percentageroot coverage
Mean percentagecomplete root coverage
Allen (8) Subepithelial connective tissue graft plustunnel technique
84.0 Not available
Zabalegui et al. (213) Subepithelial connective tissue graft plustunnel technique
91.6 66.7
Tozum & Dini (191) Subepithelial connective tissue graft plustunnel technique
95.0 Not available
Tozum et al. (192) Subepithelial connective tissue graft plustunnel technique
96.0 Not available
Georges et al. (73) Subepithelial connective tissue graft plustunnel technique
85.0 Not available
Aroca et al. (15) Connective tissue graft plus modiedcoronally advanced tunnel technique
90.0 85
Periodontal plastic surgery
355
-
(coronally advanced ap plus acellular dermal matrixgraft vs. coronally advanced ap alone), thus indicat-ing the possible inuence of patient-related factors,operator skill and severity of recession on the clinicaloutcomes. However, the coronally advanced applus acellular dermal matrix graft gave better overallesthetic outcomes, as reported by both cliniciansand patients, when compared blind with the coron-ally advanced ap plus connective tissue graft, eventhough it showed less complete root coverage (4).This nding may be related to different colormatches with adjacent tissues for the acellular der-mal matrix graft and connective tissue graft, orpoorer healing for the connective tissue graft, inwhich size exceeds the bone dehiscence (216). Thedata from the literature on the use of acellular der-mal matr