PRC Form.pdf

of 4
-
Upload
shariff-bernardo-sarikin -
Category
Documents
-
view
212 -
download
0
Transcript of PRC Form.pdf
-
7/29/2019 PRC Form.pdf
1/4
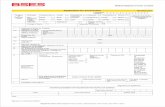
WESTERN MINDANAO STATE UNIVERSITYNormal Road, Baliwasan, Zamboanga City, Philippines
Telephone No. (062) 992-0315 / Fax No. (062) 992-4238 / E-mail: [email protected]/ Web-Site: www.wmsu.edu.ph
Accredited by: Accrediting Agency of Chartered Colleges and Universities in the Philippines (AACCUP)/Level II Re-accredited / February 2009
SURGICAL SCRUB inHospital, Municipality / City / Province
Prepared by:
Printed Name with Signature of Student:
Date Performed
and
Time Started
Patients INITIALS (only)
SURGICAL PROCEDURE
PERFORMED
O.R. Nurse On Duty
(Name and Signature)
SUPERVISED BY:
Clinical Instructor
Name and SignatureCase Number
Noted by: SARAH S. TAUPAN, R.N., M.N., D.P.A Approved by: LEILA D. BENITO, R.N., M.N.
Clinical Coordinator,PRC I.D. No. 0150766 Valid Until: January 17, 2015 OIC - Dean,PRC I.D. No.0106758Valid Until: October 9, 2012Date document is signed: Time: Date document is signed: Time:
Please specify Highest Nursing Degree Earned: Master in Nursing Specify Highest Nursing Degree Earned: Master in Nursing
O.R Form 1AO.R. SCRUB FORM M
mailto:[email protected]://www.wmsu.edu.ph/http://www.wmsu.edu.ph/mailto:[email protected] -
7/29/2019 PRC Form.pdf
2/4
WESTERN MINDANAO STATE UNIVERSITYNormal Road, Baliwasan, Zamboanga City, Philippines
Telephone No. (062) 992-0315 / Fax No. (062) 992-4238 / E-mail: [email protected]/ Web-Site: www.wmsu.edu.ph
Accredited by: Accrediting Agency of Chartered Colleges and Universities in the Philippines (AACCUP)/Level II Re-accredited / February 2009
SURGICAL SCRUB inHospital, Municipality / City / Province
Prepared by:
Printed Name with Signature of Student:
Date Performed
and
Time Started
Patients INITIALS (only) SURGICAL PROCEDURE
PERFORMED
O.R. Nurse On Duty
(Name and Signature)
SUPERVISED BY:
Clinical Instructor
Name and SignatureCase Number
Noted by: SARAH S. TAUPAN, R.N., M.N., D.P.A Approved by: LEILA D. BENITO, R.N., M.N.
Clinical Coordinator,PRC I.D. No. 0150766 Valid Until: January 17, 2015 OIC - Dean,PRC I.D. No.0106758Valid Until: October 9, 2012Date document is signed: Time: Date document is signed: Time:
Please specify Highest Nursing Degree Earned: Master in Nursing Specify Highest Nursing Degree Earned: Master in Nursing
O.R Form 1BO.R. CIRCULATING FORM MA
mailto:[email protected]://www.wmsu.edu.ph/http://www.wmsu.edu.ph/mailto:[email protected] -
7/29/2019 PRC Form.pdf
3/4
WESTERN MINDANAO STATE UNIVERSITYNormal Road, Baliwasan, Zamboanga City, Philippines
Telephone No. (062) 992-0315 / Fax No. (062) 992-4238 / E-mail: [email protected]/ Web-Site: www.wmsu.edu.ph
Accredited by: Accrediting Agency of Chartered Colleges and Universities in the Philippines (AACCUP)/Level II Re-accredited / February 2009
ACTUAL DELIVERY inHospital, Municipality / City / Province
Prepared by:
Printed Name with Signature of Student:
Date Performed
and
Time Started
Patients INITIALS (only)
PROCEDURE PERFORMED
D.R. Nurse On Duty
(Name and Signature)(If Midwife on Duty,
Signature is not Required)
SUPERVISED BY:
Clinical Instructor
Name and SignatureCase Number
(not applicable for Birthing /Lying In Clinics /
Homes)
Noted by: SARAH S. TAUPAN, R.N., M.N., D.P.A Approved by: LEILA D. BENITO, R.N., M.N.
Clinical Coordinator,PRC I.D. No. 0150766 Valid Until: January 17, 2015 OIC - Dean,PRC I.D. No.0106758Valid Until: October 9, 2012Date document is signed: Time: Date document is signed: Time:
Please specify Highest Nursing Degree Earned: Master in Nursing Specify Highest Nursing Degree Earned: Master in Nursing
D.R FormACTUAL DELIVERY
mailto:[email protected]://www.wmsu.edu.ph/http://www.wmsu.edu.ph/mailto:[email protected] -
7/29/2019 PRC Form.pdf
4/4
WESTERN MINDANAO STATE UNIVERSITYNormal Road, Baliwasan, Zamboanga City, Philippines
Telephone No. (062) 992-0315 / Fax No. (062) 992-4238 / E-mail: [email protected]/ Web-Site: www.wmsu.edu.ph
Accredited by: Accrediting Agency of Chartered Colleges and Universities in the Philippines (AACCUP)/Level II Re-accredited / February 2009
ACTUAL DELIVERY inHospital, Municipality / City / Province
Prepared by:
Printed Name with Signature of Student:
Date Performed
and
Time Started
Patients INITIALS (only) Immediate Newborn Cord CarePERFORMED
Indicate where performed e.g. D.R., Nursery,
NICU, or Home
D.R. Nurse On Duty
(Name and Signature)(If Midwife on Duty,
Signature is not Required)
SUPERVISED BY:
Clinical Instructor
Name and SignatureCase Number
(not applicable for Birthing /Lying In Clinics /
Homes)
Noted by: SARAH S. TAUPAN, R.N., M.N., D.P.A Approved by: LEILA D. BENITO, R.N., M.N.
Clinical Coordinator,PRC I.D. No. 0150766 Valid Until: January 17, 2015 OIC - Dean,PRC I.D. No.0106758Valid Until: October 9, 2012Date document is signed: Time: Date document is signed: Time:
Please specify Highest Nursing Degree Earned: Master in Nursing Specify Highest Nursing Degree Earned: Master in Nursing
ICBN FormIMMEDIATE CARE O
NEWBORN
mailto:[email protected]://www.wmsu.edu.ph/http://www.wmsu.edu.ph/mailto:[email protected]