
Data: Friend or Foe? Bob Bardwell Monson High School Monson, MA
Upload
manuel-southwickCategory
view
214download
0
Practice Modification to Embrace Multiculturalism: Balancing the Individual
and the Evidence
Samantha Pelican Monson, PsyD, Clinical Psychologist
KC Lomonaco, PsyD, Clinical Psychologist
Collaborative Family Healthcare Association 16th Annual ConferenceOctober 16-18, 2014 Washington, DC U.S.A.
Session #G3cFriday, October 17, 2014

We have not had any relevant financial relationships
during the past 12 months.
Faculty Disclosure
#1 Describe the impact of multicultural patient presentations on current integrated primary care models.
#2 Identify viable solutions to preserve efficiency and population-based care while embracing patient diversity.
#3 Cite relevant evidence to support practice innovation to incorporate multiculturalism.
Learning Objectives
At the conclusion of this session, the participant will be able to:

Bibliography / References
1. Manoleas, P. (2008). Integrated primary care and behavioral health services for Latinos: A blueprint and research agenda. Social Work in Health Care, 47, 438-454.
2. Kleinman, A., Eisenberg, L., & Good, B. (1978). Culture, illness, and care: Clinical lessons from anthropologic and cross-cultural research. Annals of Internal Medicine, 88, 251-258.
3. Bass, J.K., Annan, J., Murray, S.M., Kaysen, D., Griffiths, S., Cetinoglu, T., … Bolton, P.A. (2013). Controlled trial of psychotherapy for Congolese survivors of sexual violence. The New England Journal of Medicine, 368, 2182-2191.
4. Crosby, S.S. Primary care management of non-English-speaking refugees who have experienced trauma. The Journal of the American Medical Association, 310, 519-528.
Bibliography / References
5. Bridges, A.J., Andrews, A.R., Villalobos, et.al. (2014). Does integrated behavioral health care reduce mental health disparities for Latinos? Initial findings. Journal of Latina/o Psychology, 2, 37-53.
6. Kirmayer, L.J., Narasiah, L., Munoz, M., Rashid, M., Ryder, A.G., Guzder, J., … Pottie, K. (2011). Common mental health problems in immigrants and refugees: General approach in primary care. The Canadian Medical Association Journal, 183, E959-E967.
7. Sue, D.W., & Sue, D. (2007). Counseling the culturally diverse: Theory and practice (5th ed.). New York, NY: John Wiley & Sons, Inc.
8. Hays, P. (2013). Connecting across cultures: The helpers toolkit. Thousand Oaks, CA: Sage Publications, Inc.
A learning assessment is required for CE credit.
Questions and answers will be conducted throughout this presentation.
Learning Assessment
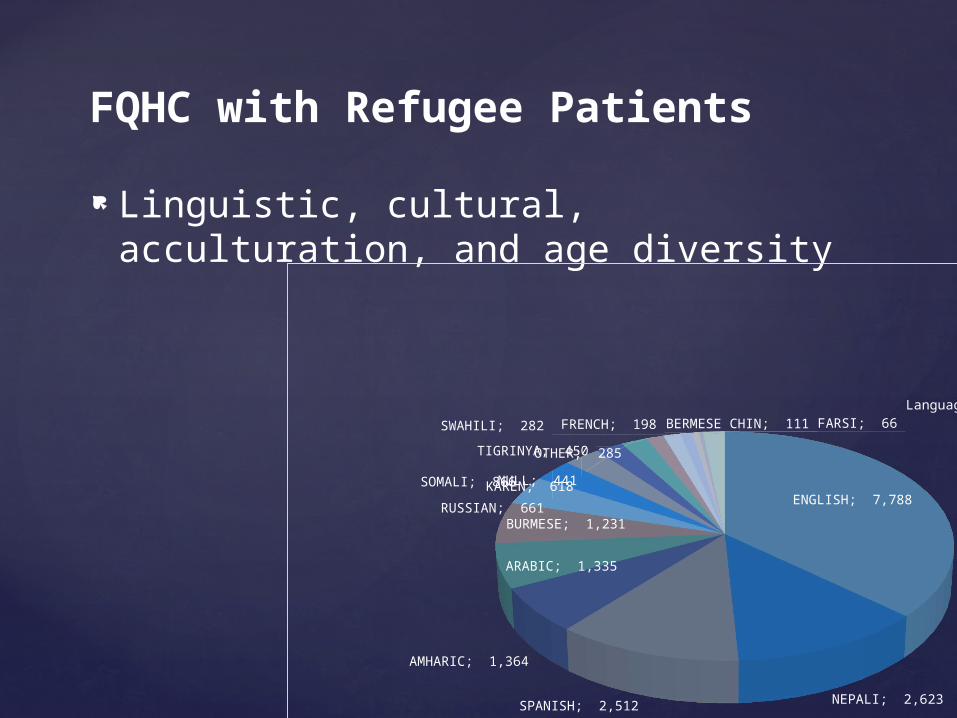
Linguistic, cultural, acculturation, and age diversity
FQHC with Refugee Patients
ENGLISH; 7,788
NEPALI; 2,623 SPANISH; 2,512
AMHARIC; 1,364
ARABIC; 1,335
BURMESE; 1,231
SOMALI; 866
RUSSIAN; 661
KAREN; 618
TIGRINYA; 450
NULL; 441
OTHER; 285
SWAHILI; 282 FRENCH; 198 BERMESE CHIN; 111 FARSI; 66 Language with less than 50 visits; 360
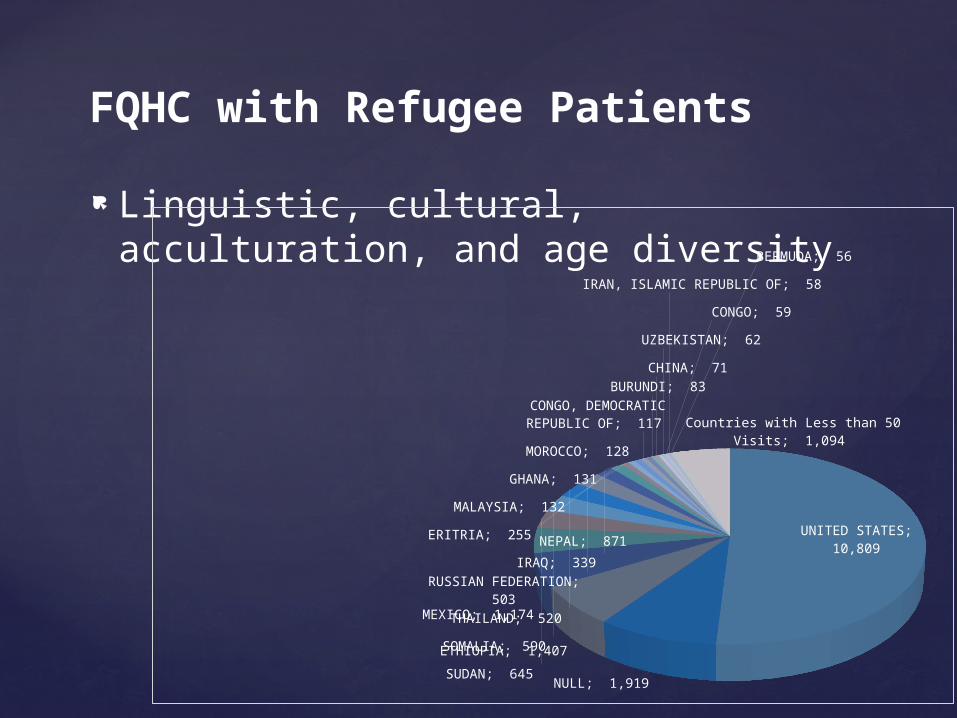
Linguistic, cultural, acculturation, and age diversity
FQHC with Refugee Patients
UNITED STATES; 10,809
NULL; 1,919
ETHIOPIA; 1,407
MEXICO; 1,174
NEPAL; 871
SUDAN; 645
SOMALIA; 590
THAILAND; 520
RUSSIAN FEDERATION; 503
IRAQ; 339 ERITRIA; 255
MALAYSIA; 132 GHANA; 131
MOROCCO; 128
CONGO, DEMOCRATIC REPUBLIC OF; 117
BURUNDI; 83
CHINA; 71
UZBEKISTAN; 62
CONGO; 59
IRAN, ISLAMIC REPUBLIC OF; 58
BERMUDA; 56
Countries with Less than 50 Visits; 1,094
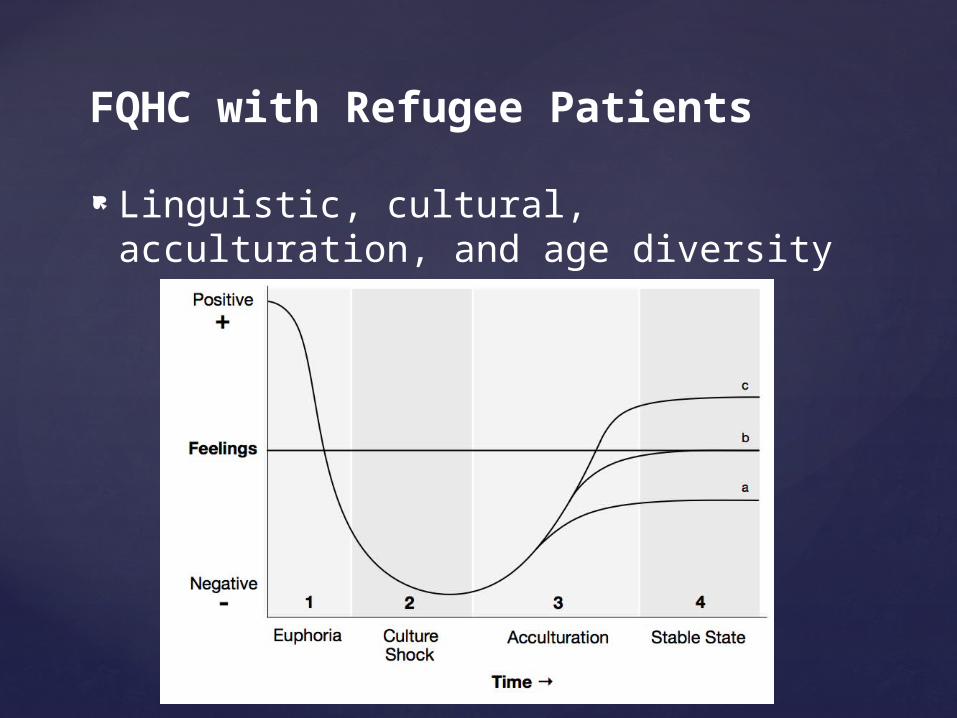
Linguistic, cultural, acculturation, and age diversity
FQHC with Refugee Patients
Linguistic, cultural, acculturation, and age diversity
FQHC with Refugee Patients
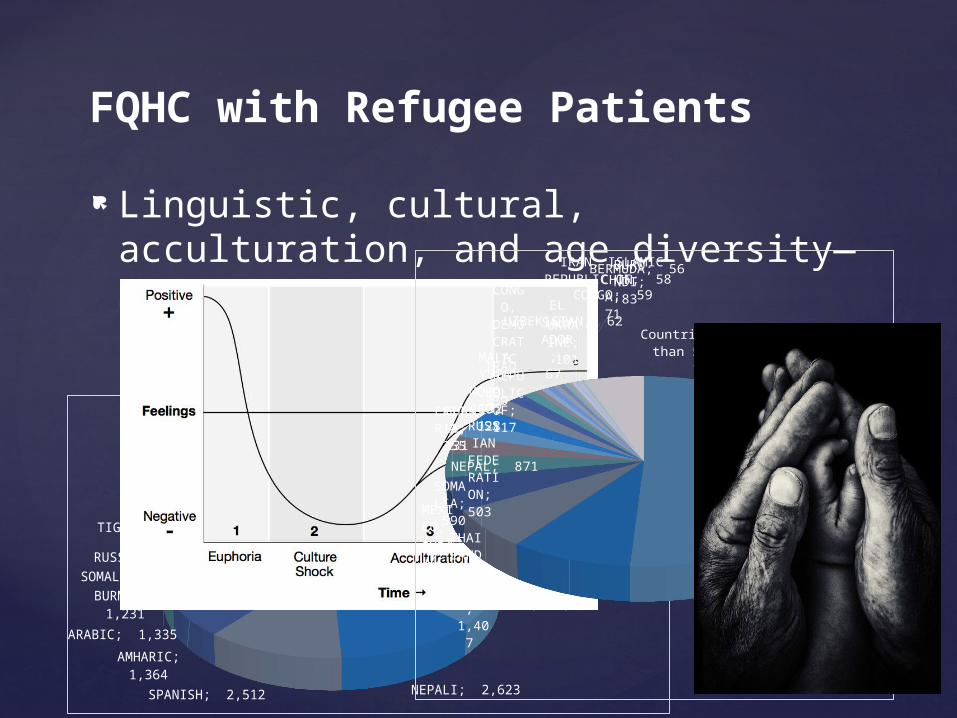
Linguistic, cultural, acculturation, and age diversity—messy!
FQHC with Refugee Patients
ENGLISH; 7,788
NEPALI; 2,623 SPANISH; 2,512
AMHARIC; 1,364
ARABIC; 1,335
BURMESE; 1,231
SOMALI; 866
RUSSIAN; 661
KAREN; 618 TIGRINYA; 450
NULL; 441
OTHER; 285
SWAHILI; 282 FRENCH; 198 BERMESE CHIN; 111 FARSI; 66 Language with less than 50
visits; 360
UNITED STATES; 10,809
NULL; 1,919
ETHIOPIA
; 1,407
MEXICO; 1,174
NEPAL; 871
SU-DAN; 645
SOMALIA; 590
THAILAND;
520
RUSSIAN FEDER-
ATION;
503
IRAQ;
339 ERI-TRIA
; 255
MALAYSIA;
132
GHANA; 131 MO
ROCCO; 128
CONGO, DEMOCRATIC RE-PUBLIC OF; 117
UKRAINE
; 101
BU-RUNDI; 83
CHINA; 71
EL SALVADOR; 67
UZBEKISTAN; 62
CONGO; 59
IRAN, ISLAMIC REPUBLIC OF; 58 BERMUDA; 56
Countries with Less than 50 Visits; 1,094
Some staff and providers are bilingual in English/Spanish, and some are not
Our organization is retrofitted to provide care to Latino patients, not built explicitly for this purpose
FQHC with Latino Patients
Issues that arise in clinic: Beliefs about heath and illness differ from
culture to culture Acculturation – Families that straddle two (or
more) different worlds Disparities in care increase stressors, health
issues
FQHC with Latino Patients

How do we look outside our Western frame of reference to offer culturally sensitive care while maintaining model fidelity?1
What do you think caused the problem? What kind of treatment do you think you
should receive? What are the most important results you
hope to get from treatment? Acknowledge the differences in the room
Is there a place for these questions in your model of integrated primary care?
Clinical Pearl #1: Add culture-based questions to standard practice.2

Validated modifications of evidence-based treatments often: Bring patients together in groups Utilize a trusted community leader Host at a non-clinical site
Is your model of integrated primary care flexible enough to incorporate alternative
modalities?
Clinical Pearl #2: De-individualize assessments and interventions.3
Micro—within the care team: Promote cultural competence through
education Mutual feedback among colleagues about
stereotyping or prejudice Macro—outside the care team:
Encourage flexibility of policies (e.g., inclusion of non-Western approaches) to align with multicultural patient populations
Is there “space” for this in your model of integrated primary care?
Clinical Pearl #3: Advocate for social justice to decrease biases in care.4,5

Prevalence of common mental health problems is lower immediately after migration and increases over time
Patients may not be prepared for the racism and discrimination they will face
Does your model of integrated primary care accommodate this?
Clinical Pearl #4: Acculturation may bring new or increased symptoms.1,6

How do ethical principles adapt to be culturally responsive? Dual relationships/conflict of interest Touch Self disclosure
How have you changed/challenged your ethical practice to work in a culturally sensitive
manner within your model of integrated primary care?
Clinical Pearl #5: When ethics are unclear, consult!7
Please complete and return theevaluation form to the classroom monitor before
leaving this session.
Thank you!
Session Evaluation


















