Practical Diabetes Management - Welcome to CCEHS · PDF file · 2017-03-24Practical...
56
1 Mary Korytkowski M.D. Professor of Medicine University of Pittsburgh Practical Diabetes Management Choosing the Right Medication
Transcript of Practical Diabetes Management - Welcome to CCEHS · PDF file · 2017-03-24Practical...

1
Mary Korytkowski M.D.
Professor of Medicine
University of Pittsburgh
Practical Diabetes Management
Choosing the Right Medication

Mary Korytkowski MD
Honoraria
British Medical Journal Diabetes Research and Care
Advisory Board Member Novo Nordisk
Other
ABIM Endocrinology & Metabolism Test-Writing Committee
No exam content will be disclosed
Disclosure of Financial Relationships
2

Biguanides: Metformin
Insulin secretogogues: Sulfonylureas, meglitinides
Sodium glucose cotransporter 2 (SGLT2) inhibitors
Thiazolidinediones (TZD)
Incretins — Dipeptidyl peptidase IV inhibitors (DPP-IV)
— Glucagon like peptide agonists
_________________________________
Alpha glucosidase inhibitors
Other agents — Bile acid sequestrants
— Bromocriptine
Amylin agonists
Non-insulin therapy for treatment of diabetes

Pharmacologic Approaches to Glycemic Treatment
4 Diabetes Care 2017;40(Suppl. 1):S64–S74
Efficacy
Risk for hypoglycemia
Weight
Side effects
Cost
Factors to consider in choosing the right medication
5

Metformin
6
Efficacy Reduces A1c by 1.5-2.0%
Risk for hypoglycemia Low
Weight Neutral / Mild weight loss
Side effects B12 Deficiency (monitor B12 levels periodically)
Gastrointestinal (5% of patients)*
Lactic acidosis (rare)
Cost Low
*Can be minimized by using extended release formulations and taking after a meal

Insulin secretogogues:
7
Efficacy
Reduces A1c by 1.5-2.0%
Risk for hypoglycemia
Moderate
Weight
Neutral / gain
Side effects
Hypoglycemia
Cost
Low
Sulfonylureas: glipizide and glimepiride
Glinides: repaglinide and meglitinide

Thiazolidinediones: Pioglitazone, Rosiglitazone
9
Efficacy
High
Risk for hypoglycemia
Low
Weight
Weight gain
Side effects
Edema
CHF
Bone loss and fractures
Cost
Low

Sodium Glucose Transporter (SGLT) 2 Inhibitors
10
Efficacy
Intermediate (Reduce A1C by ~ 0.8-1.0%)
Risk for hypoglycemia
Low
Weight
Weight loss
Side effects
Genito-urinary infections
Dehydration
Fracture risk (canagliflozin)
Cost
High
dapagliflozin , canagliflozin, empagliflozin

Dipeptidyl Peptidase Inhibitors
11
Efficacy
Intermediate (Reduce A1C by ~ 0.8-1.0%)
Risk for hypoglycemia
Low
Weight
Weight neutral
Side effects
Infrequent
Increase in nasopharyngitis/URI/UTI
Headache, myalgias / arthralgias
Rarely LFT elevations
Case reports of acute pancreatitis
Rare case reports severe hypersensitivity reactions with
anaphylaxis, angioedema, exfoliative skin conditions
Cost
High
Sitagliptin / Saxagliptin / Alogliptin / Linagliptin

Glucagon Like Peptide 1 (GLP1) Receptor Agonists
12
Efficacy
High
Risk for hypoglycemia
Low
Weight
Weight loss
Side effects
Gastrointestinal (nausea, vomiting) Post-marketing reports of pancreatitis and acute renal failure
Cost
High
exenatide, liraglutide, albiglutide, dulaglutide
The reported low risk for hypoglycemia reported with
TZDs, , GLP1 agents, DPP4 and SGLT2 inhibitors
increases when these agents are used in combination
with insulin secretogogues or insulin
13

14
82 year old male with 20 year history type 2 diabetes and osteopenia
Microvascular complications: Background DR, Neuropathy, CKD
Macrovascular complications: CAD s/p CABG
Home glucose: FBG 110-218 mg/dl
Hypoglycemia: none reported
Medications
Glipizide 5 mg BID
Metformin 500 mg bid
Pravastatin 20 mg
Ramipril 10 mg qd
Atenolol 12.5 mg
Vitamin D 1000 IU
PE: Wt 210 lbs HT 5”9” BMI 312 kg/m
BP 146/80 HR 70
Extremities 1+ pitting edema
Absent KJ / AJ DTRs
Vibration decreased 50% MF testing normal
Laboratory Studies
HA1c 8.4% (increased from 7.8%)
Creatinine 1.6 mg/dl eGFR 46 ml/min
LFTs normal
LDL 89
25 Vitamin D 35 ng/ml
Patient Case

Management of Atherosclerotic Cardiovascular Disease Risk Factors in the Older Adult Patient With Diabetes
15
Korytkowski M and Forman DE Diabetes Care April 2017.

Consensus Development Conference on
Diabetes in Older Adults A Framework for Considering Treatment Goals
Kirkman et al. JAGS. Special Report-Diabetes in Older Adults: A Consensus Report 2012, 1-15.

American Geriatric Society:
A1c Recommendations 2013 for 65+
• 7.5 - 8% in general for the older adults
• 7% - 7.5% may be appropriate if it can be safely achieved in healthy older adults with few comorbidities and good functional status
• 8% - 9% is appropriate for older adults with multiple comorbidities, poor health, and limited life expectancy (IIA)
• Potential harm in lowering A1C to < 6.5% in older adults with type 2 DM (IIA)
American Geriatrics Society (AGS) Panel . Guidelines for Improving the Care of the Older Person with Diabetes Mellitus. J Am Geri Soc 2013; 51:S265-S280

? Increase dose of metformin
? Stop metformin
? Increase dose of glipizede
? Stop glipizide
? Add an SGLT2 inhibitor
? Add pioglitazone
? Add a DPP-IV inhibitor
? Add a GLP1 receptor agonist
? Add a basal insulin
_________________________________
What is the correct medication for this patient?
18


Updated Metformin–CKD Prescribing Guidelines (April 2016)
• Obtain eGFR before starting metformin and annually, more
frequently in those at risk for renal impairment (e.g., elderly).
• Metformin contraindicated in patients with an eGFR <30.
• Starting metformin in patients with an eGFR between 30-45 not
recommended.
• If eGFR falls <45, assess the benefits and risks of continuing
treatment. D/C if eGFR falls <30.
• Hold metformin at the time of / before iodinated contrast
procedure if eGFR 30-60; if h/o liver disease, alcoholism, or heart
failure; or if intra-arterial contrast. Recheck eGFR 48 hrs after
procedure and restart if renal function stable. http://www.fda.gov/Drugs/DrugSafety/ucm493244.htm (accessed 4-8-16)
0
1
2
3
4
5
6
7
8
9
SU only SU + eGFR<30ml/min
SU +eGFR 30-59ml/min
SU +eGFR >60ml/min
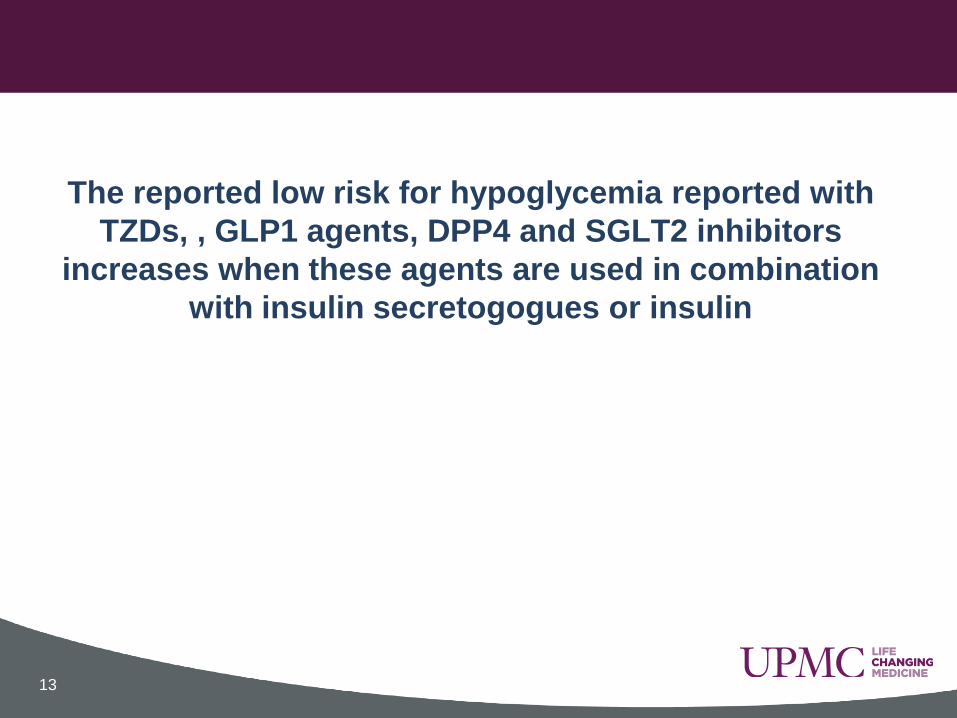
Hazard Ratio (HR) for hypoglycemia with current SU therapy according to eGFR
Risk of Hypoglycemia with Sulfonylureas compared with metformin in relation to renal function
21 Van Dalem J et al BMJ 2016;354:i3625
Results adjusted for age and sex

? Increase dose of metformin
? Stop metformin
? Increase dose of glipizide
? Stop glipizide
? Add an SGLT2 inhibitor
? Add pioglitazone
? Add a DPP-IV inhibitor
? Add a GLP1 receptor agonist
? Add a basal insulin
_________________________________
What is the correct medication for this patient?
22

SGLT2-Inhibitors: Mechanism of action

24
Sodium-Glucose Cotransporter 2 Inhibitors
Advantages
• Effective
• Do not cause hypoglycemia when used alone or in combination with metformin
• Associated with weight loss, reductions in BP, and CVD events
Disadvantages: Expensive
May offer unique cardiovascular benefit
Empagliflozin recently approved for use

25

Original Article Empagliflozin, Cardiovascular Outcomes, and
Mortality in Type 2 Diabetes
Bernard Zinman, M.D., Christoph Wanner, M.D., John M. Lachin, Sc.D., David Fitchett, M.D., Erich Bluhmki, Ph.D., Stefan Hantel, Ph.D., Michaela Mattheus, Dipl.
Biomath., Theresa Devins, Dr.P.H., Odd Erik Johansen, M.D., Ph.D., Hans J.
Woerle, M.D., Uli C. Broedl, M.D., Silvio E. Inzucchi, M.D., for the EMPA-REG OUTCOME Investigators
N Engl J Med Volume 373(22):2117-2128
November 26, 2015
7070 subject with T2D at high risk for CVD randomized to Placebo,
Study Drug 10 or 25 mg for ~ 3.1 years
Mean age of subjects ~63 ± 9 years
Mean BMI ~30 ± 5 kg/m2

Emplagliflozin Study: HbA1c Levels
Zinman B et al. N Engl J Med 2015;373:2117-2128
Subject treated with study drug had
decreases in SBP of 4 mm Hg, DPB 1.5 mm
Hg, weight 2 kg, and waist circumference
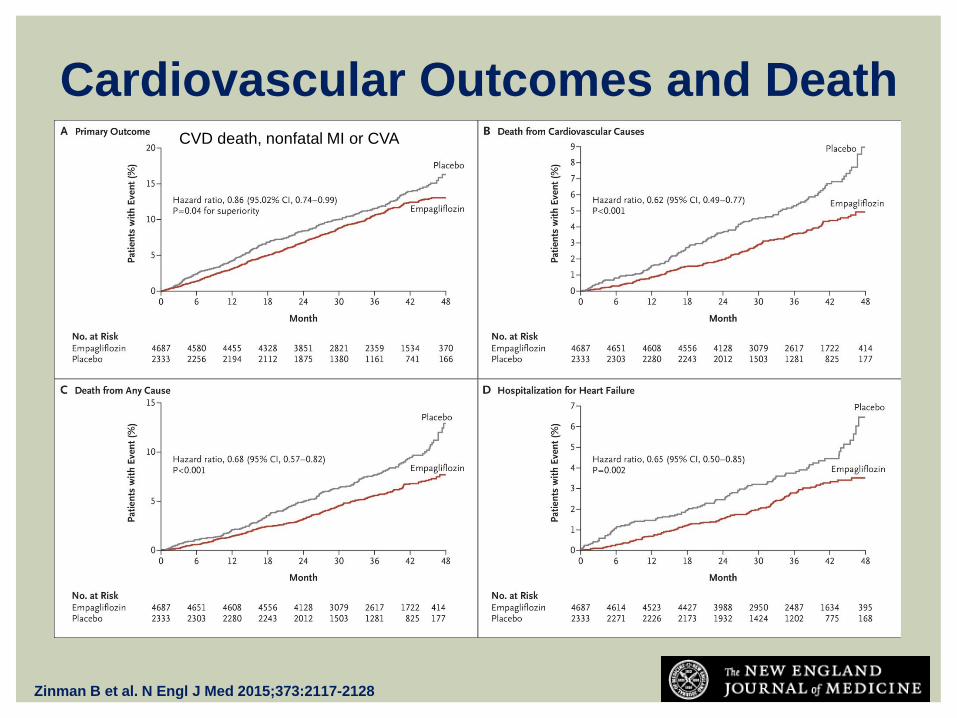
Cardiovascular Outcomes and Death
Zinman B et al. N Engl J Med 2015;373:2117-2128
CVD death, nonfatal MI or CVA

Sodium-Glucose Cotransporter 2 Inhibitors Disadvantages:
• Increase in risk for “euglycemic DKA”
• High risk for volume depletion, hypotension and dehydration
Use carefully, if at all, in the elderly or those receiving diuretics
• Contraindicated in patients with advanced kidney disease
Effect declines as eGFR declines
Minimal effect with eGFR < 50 ml/min
• These are very new drugs for which long term safety has yet
to be established
Concern for an increase in bladder and breast neoplasms raised in
preclinical trials
• (I would not use this in any male suspected of having
prostatic hyperplasia)

Efficacy of SGLT-2 inhibitors (dapagliflozin) is reduced with declining eGFR.
van Bommel EJM et al. Clin J Am Soc Neph March 2017 doi:10.2215/CJN.06080616 ©2017 by American Society of Nephrology

Effect of the SGLT2i Canagliflozin on Fracture Risk
31
Watts NB et al J Clin Endocrinol Metab 2016;101:157
Pooled analysis of data from 3 large preclinical trials
CANagliflozin cardioVascular Assessment Study (CANVAS) was primary
contributor to observed increase in fracture risk
4330 patients with T2D with elevated CVD risk Mean age 62±8 years

? Increase dose of metformin
? Stop metformin
? Increase dose of glipizide
? Stop glipizide
? Add an SGLT2 inhibitor
? Add pioglitazone
? Add a DPP-IV inhibitor
? Add a GLP1 receptor agonist
? Add a basal insulin
_________________________________
What is the correct medication for this patient?
32

• Weight gain (up to 10 kg in some patients)
• Reductions in bone density with increase risk of fractures
• Exacerbation of CHF
– Use with caution in patients with pre-existing CHF
• Significant questions raised regarding CV safety of
rosiglitazone (2011)
• Increased bladder cancer risk with pioglitazone
demonstrated in some but not all studies
TZDS: Considerations for Use

Kernan WN et al. N Engl J Med 2016;374:1321

U.S. National Institute of Neurological Disorders and Stroke
(Grant # U01NS044976)
February 17, 2016DOI: 10.1056/NEJMoa1506930

IRIS Secondary Outcomes Pioglitazone
(N=1939)
Placebo
(N=1937)
Outcome* % (No.) % (No.)
Hazard Ratio
(95% CI) P
ACS 5.0 (96) 6.6 (128) 0.75 0.11
Stroke/MI/HF 10.6 (206) 12.9 (249) 0.82 0.11
DM 3.8 (73) 7.7 (149) 0.48 <.0001
Death 7.0 (136) 7.5 (146) 0.93 0.52
*ACS=Acute coronary syndrome (unstable angina or MI).
*HF=heart failure

IRIS Serious Adverse Events
# Participants
Pioglitazone
(N=1939)
Placebo
(N=1937)
Event % (N) P
Bone fracture† 5.1 (99) 3.2 (66) <0.01
Heart failure† 2.6 (51) 2.2 (42) 0.35
Incident cancer 6.9 (133) 7.7 (150) 0.29
†Previously reported to be associated with pioglitazone or drugs in its class.

IRIS Non-Serious Adverse Events
Pioglitazone
(N=1939)
Placebo
(N=1937)
Event % (No. Participants) P
Weight Gain†
at Year 4, mean 2.6 kg -0.5 kg <0.01
New or worse edema†
691 (36%)
483 (25%)
<0.01
New or worse SOB†
342 (18%)
292 (15%)
0.03
†Previously reported to be associated with pioglitazone or drugs in its class.

? Increase dose of metformin
? Stop metformin
? Increase dose of glipizide
? Stop glipizide
? Add an SGLT2 inhibitor
? Add pioglitazone
? Add a DPP-IV inhibitor
? Add a GLP1 receptor agonist
? Add a basal insulin
_________________________________
What is the correct medication for this patient?
39

• Can be taken with or without food
• Once-daily dosing
• Side effects are infrequent
Increase in upper respiratory infections/UTI
Headache
Case reports of acute pancreatitis
Rare case reports severe hypersensitivity reactions with anaphylaxis, angioedema, and exfoliative skin conditions
• No evidence of macrovascular risk reduction
• Increased CHF exacerbations with saxagliptin
Dipeptidyl Peptidase-IV Inhibitors
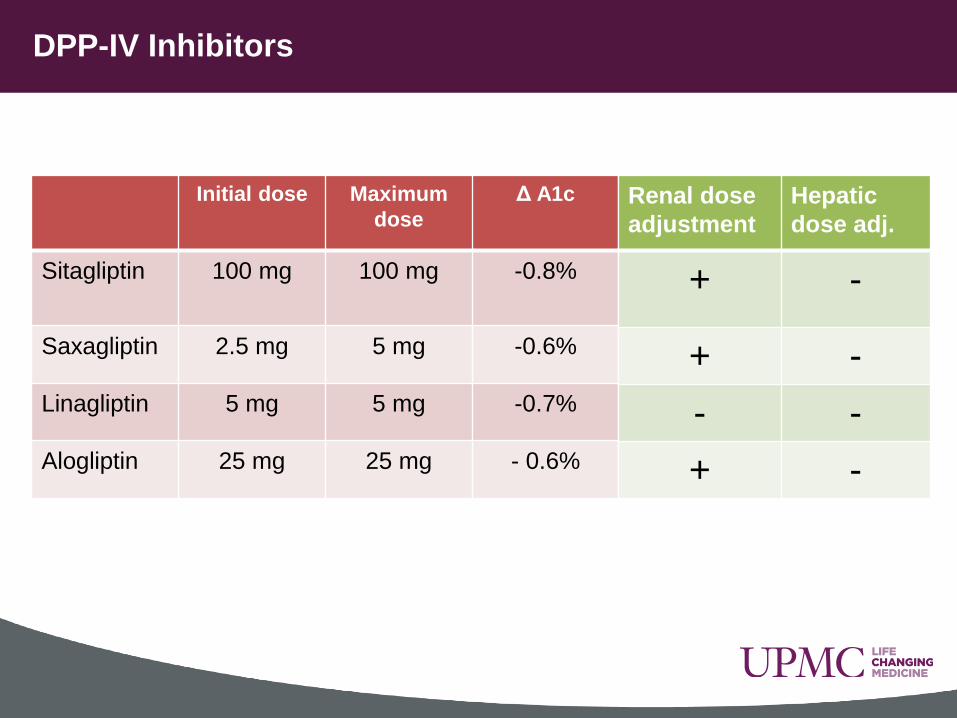
DPP-IV Inhibitors
Initial dose Maximum
dose
Δ A1c Half life (hr) Duration
(hr)
Sitagliptin 100 mg 100 mg -0.8% 12
~16
Saxagliptin 2.5 mg 5 mg -0.6% 2.5 24
Linagliptin 5 mg 5 mg -0.7% 12 ~ 100 *
Alogliptin 25 mg 25 mg - 0.6% 21
Renal dose
adjustment
Hepatic
dose adj.
+ -
+ -
- -
+ -
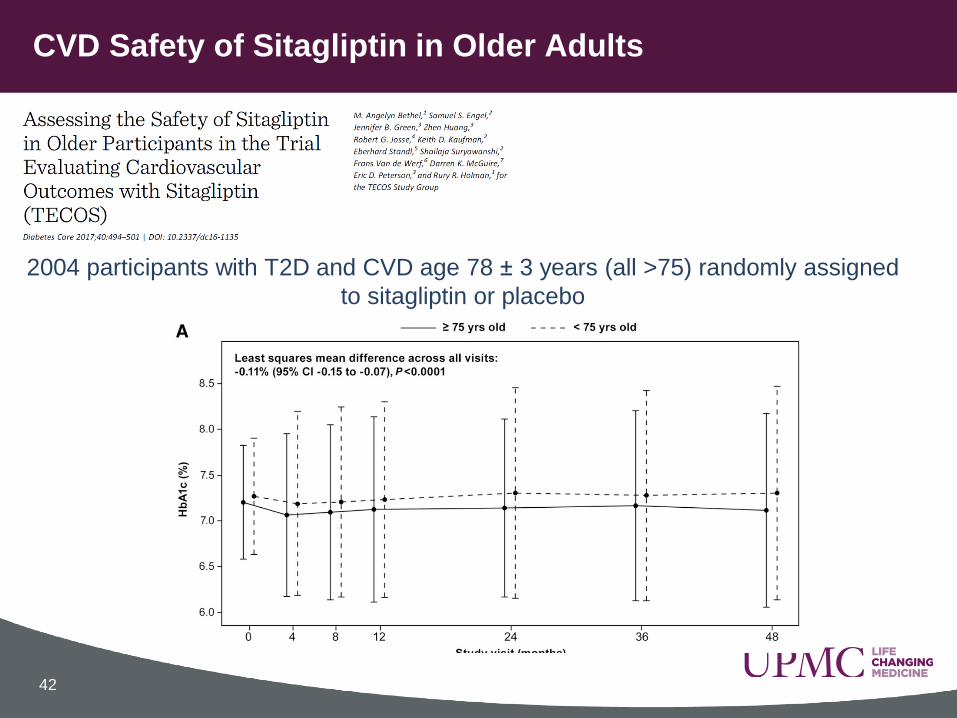
CVD Safety of Sitagliptin in Older Adults
42
2004 participants with T2D and CVD age 78 ± 3 years (all >75) randomly assigned
to sitagliptin or placebo

Study outcomes : Sitagliptin vs. Placebo (TECOS)
43 Bethel MA et al. Diabetes Care 2017;40:494
? Increase dose of metformin
? Stop metformin
? Increase dose of glipizide
? Stop glipizide
? Add an SGLT2 inhibitor
? Add pioglitazone
Add a DPP-IV inhibitor: Reasonable Choice Sitagliptin 50 mg or Linagliptin 5 mg
Biggest concern: Cost
? Add a GLP1 receptor agonist
? Add a basal insulin
_________________________________
What is the correct medication for this patient?
44
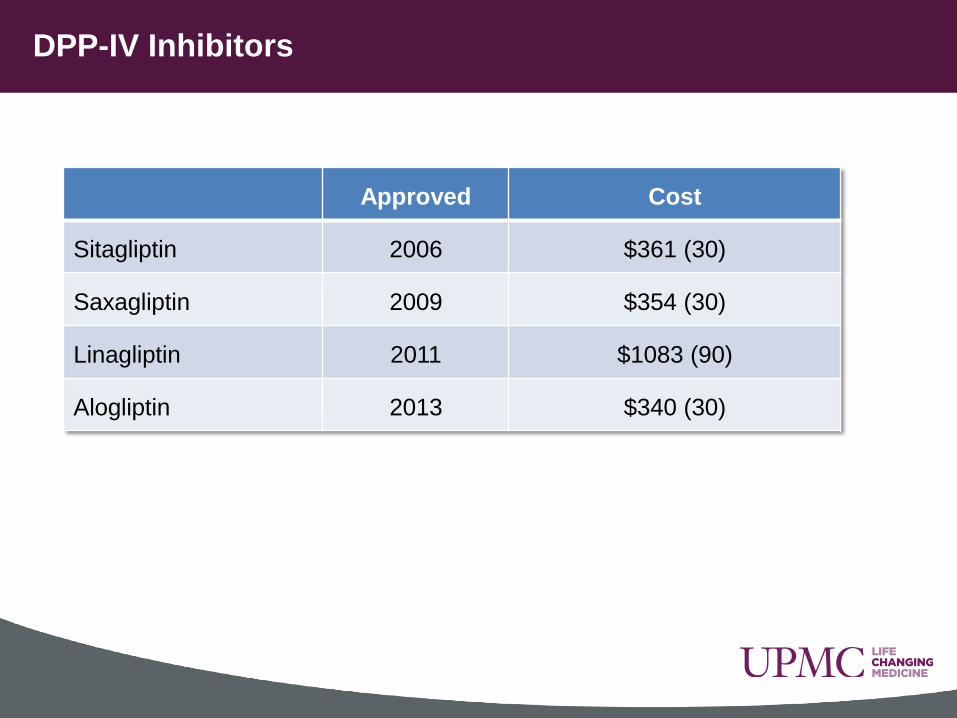
DPP-IV Inhibitors
Approved Cost
Sitagliptin 2006 $361 (30)
Saxagliptin 2009 $354 (30)
Linagliptin 2011 $1083 (90)
Alogliptin 2013 $340 (30)

Initial
Dose Max Dose ΔA1c Weight
Loss (kg)*
Half Life
Exenatide 5 mcg 10 mcg BID -0.9% -2.9 ~ 2.4 hr
Exenatide ER 2 mg 2 mg Qwk -1.5% -2.0 ~ 2 week
Liraglutide 0.6 mg 1.8 mg QD -1.1% -2.5 ~ 13 hr
Albiglutide 30 mg 50 mg Qwk -0.9% -0.9 ~ 5 days
Dulaglutide 0.75 mg 1.5 mg Qwk -0.8% -2.3 ~ 5 days
Lixisenatide 10 mcg 20 mcg QD -0.8% -- --
Renal dose
adjustment
Hepatic dose
adj.
- -
- -
- -
- -
- -
Glucagon-Like Peptide 1 Agonists

Incretin therapy improves first phase insulin secretion in type 2 diabetes
Time (min) -180 -90 0 30 60 90 120
Intravenous glucose
Insu
lin (
pM
/kg/
min
) Exenatide
Placebo

The GLP1 analog exenatide reduces glucose and glucagon levels following a meal
Kolterman J Clin Endocrinol Metab. 2003;88:3082-3089
0 120 180 60 50
100
150
200
Glucagon (pg/mL)
Placebo Exenatide
Standardized Breakfast
Time (min)
Plasma Glucose (mg/dL)
90
180
270
360
Standardized Breakfast
0 60 120 180 240 300
Placebo Exenatide

GLP-1RA in Older Adults: GetGoal-O
49
350 participants with T2D and CVD age 74 ± 4 years of age (37% > 75 and 11% >
80) (28% with eGFR 30-60 ml/min) randomly assigned to a GLP-1RA
(lixesenatide) or placebo
30% on insulin / 30% on SU + metformin / 30% on other oral DM medications
HbA1c Glucose profile
Meneilly GS et al. Diabetes Care 2017;40:485

Frequency of Nausea in GetGoal-O
50 Meneilly GS et al. Diabetes Care 2017;40:485
Lixisenatide
Placebo

51
Placebo Lixisenatide
< 59 mg/dl
Adverse Events : GetGoal-O
Meneilly GS et al. Diabetes Care 2017;40:485
Hypoglycemia was more frequent in lixisenatide group receiving SU (11.9% vs.
3.9% in placebo group) and less frequent in those receiving basal insulin in
combination with the GLP-1RA (5.4 vs. 12.7% of patients)

? Increase dose of metformin
? Stop metformin
? Increase dose of glipizide
? Stop glipizide
? Add an SGLT2 inhibitor
? Add pioglitazone
Add a DPP-IV inhibitor: Reasonable Choice Sitagliptin 50 mg or Linagliptin 5 mg
Biggest concern: Cost
Add a GLP1 receptor agonist Biggest concern: Cost (but would want to stop or lower dose SU)
? Add a basal insulin
_________________________________
What is the correct medication for this patient?
52

Progression to insulin therapy in type 2 diabetes
53 Diabetes Care 2017;40(Suppl 1):S64

? Increase dose of metformin
? Stop metformin
? Increase dose of glipizide
? Stop glipizide
? Add an SGLT2 inhibitor
? Add pioglitazone
Add a DPP-IV inhibitor: Reasonable Choice Sitagliptin 50 mg or Linagliptin 5 mg
Biggest concern: Cost
Add a GLP1 receptor agonist Biggest concern: Cost
Add a basal insulin: Starting dose 0.1 unit/kg or 6-10 units/day
_________________________________
What is the correct medication for this patient?
54

55
82 year old male with 20 year history type 2 diabetes and osteopenia
Microvascular complications: Background DR, Neuropathy, CKD
Macrovascular complications: CAD s/p CABG
Home glucose: 110-218 mg/dl
Hypoglycemia: none reported
Medications
Glipizide 5 mg BID
Metformin 500 mg bid
Pravastatin 20 mg
Ramipril 10 mg qd
Atenolol 12.5 mg
Vitamin D 1000 IU
PE: Wt 210 lbs HT 5”9” BMI 312 kg/m
BP 146/80 HR 70
Extremities 1+ pitting edema
Absent KJ / AJ DTRs
Vibration decreased 50% MF testing normal
Laboratory Studies
HA1c 8.4% (increased from 7.8%)
Creatinine 1.6 mg/dl eGFR 46 ml/min
LFTs normal
LDL 89
25 Vitamin D 35 ng/ml
Patient Case Summary

• Metformin:
– No need to DC therapy based on current guidelines
– Would not increase dose further with eGFR < 50 ml/min
• Sulfonylurea
– No need to lower dose or DC as no evidence hypoglycemia unless
additional medication started that could increase risk
• TZDS
– Raise risk for worsening of LE edema, CHF, and fractures
• SGTL2 inhibitors
– While he may benefit from CVD risk reduction, low eGFR may limit efficacy
• DPP4 inhibitor or GLP-1RA
– Demonstrated efficacy and safety in elderly population
• Add basal insulin with progression of dosing according to home
BG monitoring
Summary
56