Ppt Copd 2011 Dr Ana Rima
31
COPD – The Silent Killer
-
Upload
yeni-belawati -
Category
Documents
-
view
89 -
download
4
description
pulmonologu
Transcript of Ppt Copd 2011 Dr Ana Rima

COPD – The Silent Killer

Chronic Respiratory Disease is a Leading Cause of Chronic Disease Deaths Worldwide
Adapted from: World Health Organization. Preventing chronic diseases: a vital investment. (2005) Available at: http://www.who.int/chp/chronic_disease_report/contents/en/index.html (accessed June 2009).
The World Health Organization (WHO) projected that, in 2005, chronic respiratory disease would be the third-leading cause of deaths from chronic disease
worldwide
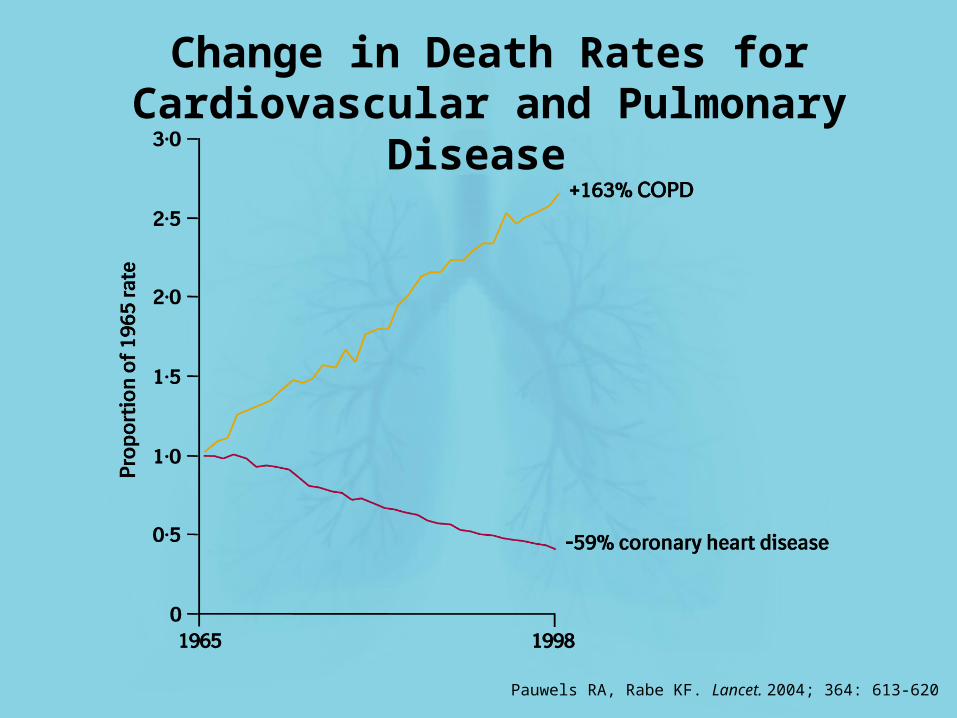
Pauwels RA, Rabe KF. Lancet. 2004; 364: 613-620
Change in Death Rates for Cardiovascular and Pulmonary Disease

Tan and NG Chest 2008; 133:517
Prevalence COPD in Asia-Pacific Region

Definition
GOLD. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Revised 2011. Available from: http://www.goldcopd.org
• COPD, a common preventable and
treatable disease, is characterized
by persistent airflow limitation that
is usually progressive and associated
with an enhanced chronic
inflammatory response in the
airways and the lung to noxious
particles or gases
• Exacerbations and comorbidities
contribute to the overall severity in
individual patients
REVISED 2011

General considerations for FEV1 decline
FEV1 decline in healthy subjects
FEV1 decline in COPD patients
FE
V1 d
ecl
ine (
mL
)
“normal decline”
“additional decline”
Annual
PotentialRoom for
Improvement
1. Celli BR, MacNee W. Eur Respir J. 2004; 23: 932–946;2. GOLD. Global Initiative for Chronic Obstructive Lung Disease. Updated 2010. Available: www.goldcopd.com

Mechanisms of Airflow Limitation in COPD
(Peripheral Airways)
Adapted from: Barnes P. NEJM 2000; 343; 269

FEV1 decline in COPD:Potentially reversible
mechanisms
Mucus hypersecretion
Smooth musclecontraction
Cholinergic tone
Loss of alveolar attachmentPeribronchial fibrosis
1. Celli BR, et al. Am J Respir Crit Care Med 2008; 178: 332–38;2. Beaucage F, Decramer M, et al. Am J Respir Crit Care Med .2008; 177: A401.

Adapted from: Hansel T/Barnes P. An Atlas of COPD. 2004
Central nervous system
Vagus nerve
Airway epithelium
Parasympatheticganglion
ACh
ACh
AChInflammatory
cell mediators
SubmucosalglandCholinergic
receptors
Irritants(e.g. cigarette smoke, bacteria, viruses)
Airway smooth muscleconstriction
MucusHypersecretion
Pathophysiology of COPD:Vagal Nerve System

Pre-ganglionicnerve
Parasympatheticganglion
Post-ganglionicnerve
Airway smoothmuscle
Nicotinic receptors (+)
M1 receptors (+)
M2 receptors (–)
M3 receptors (+)ACh
Hansel T / Barnes P. An Atlas of COPD. 2004
Cholinergic Receptor Subtypes in Airways
Ideal anti cholinergi
c

FEV1 Model of Disease Progression in COPD
100%
75%
50%
25%
0%25 50 75
Age (years)
FE
V1
(% o
f v
alu
e at
ag
e 2
5)
Moderate
Severe
Very Severe
COPDStages
Treatment
Adapted from Fletcher C and Peto R, BMJ 1977; 1:1645-1648. Imagery courtesy O’Donnell D
Diagnosis

Severe COPD
The Progression of COPD
Mild COPD

What can we do ???What can we do ???

Key Indicators for Considering a Diagnosis of COPD
Buku Lengkap Diagnosis dan Penatalaksanaan PPOK PDPI, Juli 2011

Stable COPD Treatment Goals
Buku Lengkap Diagnosis dan Penatalaksanaan PPOK PDPI, Juli 2011

UPLIFT : FEV1 Over 4-Year Trial Duration
*P<0.05 vs control. †Difference, tiotropium – control. BD, bronchodilator.
Total cohort2Asian cohort1
Δ rate of decline:†
0 mL/yr pre-BD (P=0.95)2 mL/yr post-BD (P=0.21)
Δ rate of decline:†
-2 mL/yr pre-BD (P=0.83)
5 mL/yr post-BD (P=0.54)
Japanese cohort1
Day 30
Post-BDTiotropium (n=2516)Control (n=2374)
*
*********
48
Month
423630241812601
Pre-BDTiotropium (n=2494)Control (n=2363)
* * * * * * * *
Tiotropium Control
48423630241812601
Day 30
**
Month
0.00
0.80
0.90
1.00
1.10
1.20
1.30
1.40
1.50
FE
V1 (L
)
Tiotropium Control
** * * * *
*********Pre-BDTiotropium (n=152)Control (n=145)
Post-BDTiotropium (n=156)Control (n=147)
Δ rate of decline:†
11 mL/yr pre-BD (P=0.24)13 mL/yr post-BD (P=0.16)
48423630241812601
Day 30Month
0.00
0.80
0.90
1.00
1.10
1.20
1.30
1.40
1.50 Tiotropium Control
Pre-BDTiotropium (n=45)Control (n=43)
** * * * * * *
*
*******
0.00
0.80
0.90
1.00
1.10
1.20
1.30
1.40
1.50
Post-BDTiotropium (n=46)Control (n=43)
1Fukuchi Y, et al. Respirology 2011; 16: 825-835; 2Adapted from Tashkin DP, et al. N Engl J Med 2008;359:1543-1554.
Significant lung function improvement with tiotropium in total, Asian and
Japanese cohort

*P<0.05 vs. control. Repeated measure ANOVA was used to estimate means. Estimated means are adjusted for baseline measurements. Patients with ≥2 acceptable SGRQ Total Scores after Month 6 were included in the analysis.
UPLIFT : SGRQ Total Score
= 2.3-3.3 units
Asian Cohort1 Total Cohort2
= 1.5-6.1 units
6 12 18 24 30 36 42 480
Month
* * * * * * * *
6 12 18 24 30 36 42 480
Month
Imp
rove
men
t
* * * *
= 1.1-6.2 units
Japanese Cohort1
6 12 18 24 30 36 42 480
Month
** *
35
40
45
50
SG
RQ
To
tal
Sco
re (
Un
its)
Tiotropium (n=184)
35
40
45
50
Control (n=178)Tiotropium (n=48)Control (n=43)
Tiotropium (n=2478)Control (n=2337)
35
40
45
50
1Fukuchi Y, et al. Respirology 2011; 16: 825-835; 2Adapted from Tashkin DP, et al. N Engl J Med 2008;359:1543-1554.
Significant SGRQ improvement with tiotropium in total, Asian and Japanese
cohort

The UPLIFT Lesson
Similar to the overall cohort, 4 years treatment with tiotropium provided the following benefits in the subgroup of COPD patients from Asia (Improved lung function, Improved HRQoL, Reduced exacerbations)
These data indicate that tiotropium may be used in patients from Asia in accordance with current international treatment guidelines
Tiotropium is beneficial to COPD patients of various severities (GOLD stages II to IV) and has clearly demonstrated benefit to GOLD stage II patients
1Fukuchi Y, et al. Respirology 2011; 16: 825-835

Exacerbations
Increased mortality with exacerbation
hospitalizations
Increased health resource
utilization and direct costs
Reduced health-relatedquality of life
Accelerateddeclinein FEV1
The Clinical Course of COPD:Consequences of Exacerbations

Systemic inflammation increases during ECOPD potential mechanism to explain the increased risk of vascular events
Plasma levels of the cardiac biomarkers NT-proBNP and troponin T were abnormal in a significant number of ECOPD patients hospitalized both markers predicted mortality
Patients with COPD had increased circulating platelete-monocyte aggregates further increased during ECOPD
Fabbri LM, et al. Thorax. 2011; 66(9): 745-747

POET-COPD®: Tiotropium Significantly Delayed Time to First
ExacerbationP
rob
abili
ty o
f C
OP
D e
xace
rbat
ion
(%
)
Time to event (days)0
50
030 60 90 120 150 180 210 240 270 300 330 360
Hazard ratio = 0.83*(95% CI, 0.77, 0.90)P<0.001 (log-rank test)
Tiotropium 3707 3369 3136 2955 2787 2647 2561 2455 2343 2242 2169 2107 1869
Salmeterol 3669 3328 3028 2802 2605 2457 2351 2251 2137 2050 1982 1915 1657
No. of patients at risk:
45
40
35
30
25
20
15
10
5
TiotropiumSalmeterol
*Cox regression adjusted for (pooled) centre and treatment.
17%Risk
difference
Vogelmeier C et al. N Engl J Med 2011;364:1093-1103.

Pro
bab
ility
of
ho
spit
aliz
ed
CO
PD
exa
cerb
atio
n (
%)
Time to event (days)0
0
5
10
15
20
30 60 90 120 150 180 210 240 270 300 330 360
POET-COPD®: Tiotropium Significantly Delayed Time to First
Severe ExacerbationTiotropiumSalmeterol
Hazard ratio = 0.72*(95% CI, 0.61, 0.85)P<0.001 (log-rank test)
Tiotropium 3707 3564 3453 3359 3285 3217 3177 3125 3066 3017 2977 2984 2663
Salmeterol 3669 3502 3362 3244 3172 3080 3032 2982 2921 2870 2834 2806 2489
No. of patients at risk:
28%Risk
difference
*Cox regression adjusted for (pooled) centre and treatment. Vogelmeier C et al. N Engl J Med 2011;364:1093-1103.

Tiotropium Reduced Number of Exacerbations
0.64
0.54
0.09
0.72
0.59
0.13
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
All exacerbations Moderateexacerbations
Severeexacerbations
Ad
jus
ted
ye
arl
y r
ate
RR 0.89*
(95% CI 0.83, 0.96)P=0.002 RR 0.93*
(95% CI 0.86, 1.00)P=0.048
RR 0.73*
(95% CI 0.66, 0.82)P<0.001
Tiotropium
Salmeterol
RR=rate ratio.
*Poisson regression correcting for overdispersion and adjusted for treatment exposure.
Vogelmeier C et al. N Engl J Med 2011;364:1093-1103.

POET-COPD®: Time to First Exacerbation by Subgroup Consistent with Overall Cohort
Hazard ratio for at least one COPD exacerbation
0.4 0.6 0.8 1 1.2 1.4Favours tiotropium Favours salmeterol
Stage II 561/1781 635/1833 0.88 (0.79, 0.99)
455/1230≥20 to <25 501/1254 0.89 (0.79, 1.02)
Age group
Characteristic Tiotropiumn/N
Salmeteroln/N
Hazard Ratio(95% CI)
Sex
GOLD stage
Smoking status
BMI group
ICS use at baseline
237/655<55 y 258/665 0.88 (0.74, 1.05)484/1462≥55 to <65 y 522/1426 0.87 (0.77, 0.98)556/1590≥65 y 634/1578 0.83 (0.74, 0.93)
913/2759Male 1016/2747 0.86 (0.78, 0.94)364/948Female 398/922 0.84 (0.73, 0.97)
Stage III 589/1597 627/1545 0.86 (0.77, 0.97)Stage IV 127/329 152/291 0.64 (0.50, 0.81)
678/1929Noncurrent 746/1896 0.84 (0.75, 0.93)599/1778Current 668/1773 0.87 (0.78, 0.97)
105/286<20 134/271 0.66 (0.51, 0.85)
424/1276≥25 to <30 468/1284 0.87 (0.76, 0.99)293/915≥30 311/860 0.85 (0.72, 1.00)
Yes 785/1986 839/1955 0.87 (0.79, 0.96)No 492/1721 575/1714 0.82 (0.73, 0.92)
*Subgroup by treatment interaction. GOLD=Global Initiative for Chronic Obstructive Lung Disease; BMI=body-mass index; ICS=inhaled corticosteroid.
*n=no. patients with event; N=total no. patients.
0.76
P-value*
0.83
0.05
0.64
0.17
0.41
Vogelmeier C et al. N Engl J Med 2011;364:1093-1103.
Tiotropium was significantly more effective across almost all subgroup compared to
salmeterol

POET-COPD®: Discontinuing ICS did not Increase Rate of Exacerbations*
Tiotropium Salmeterol
n Exacerbation rate
(95% CI)
n Exacerbation rate
(95% CI)
Continued ICS during trial
1452
0.78(0.73, 0.85)
1401
0.81(0.75, 0.88)
Discontinued ICS during trial 395 0.67
(0.57, 0.79) 416 0.86 (0.74, 0.99)
*Analysis in subset of patients who were receiving ICS at baseline. ICS=inhaled corticosteroid.
Vogelmeier C et al. N Engl J Med 2011;364:1093-1103.

POET-COPD®: More Patients Receiving Concomitant ICS Experienced Pneumonia
• 180 reported pneumonia cases
– 158 (87.8%) radiologically confirmed 70 in the tiotropium group
88 in the salmeterol group
– Higher numbers of patients with ≥1
radiologically confirmed pneumonia were
receiving concomitant ICS for ≥1 day on
treatment n=89, 2.7% (n=72 hospitalized) – concomitant ICS
n=59, 1.5% (n=46 hospitalized) – no concomitant ICSVogelmeier C et al. N Engl J Med 2011;364:1093-1103.

The POET-COPD Lesson
Tiotropium was significantly more effective than salmeterol in almost all assessed exacerbation endpoints and across all major patient subgroups
Addition of ICS did not affect the outcome of exacerbation; prevention of exacerbations by tiotropium alone appears to be efficient
Adverse events seen in the POET-COPD® trial were consistent with the well-established, long-term safety profile of tiotropium

Stable COPD Treatment Goals
Buku Lengkap Diagnosis dan Penatalaksanaan PPOK PDPI, Juli 2011
UPLIFT 4 years study
UPLIFT 4 years study
UPLIFT 4 years study and POET-COPD 1 year
study

Management of COPD in Indonesia
Buku Lengkap Diagnosis dan Penatalaksanaan PPOK PDPI, Juli 2011
Spiriva ®
early treatment start from
stage II COPD
Spiriva ®
early treatment start from
stage II COPD
Berotec®
Combivent UDV ®

Take Home Messages
Cholinergic tone is the basic of COPD patophysiology
Early intervention – impact disease progression
The UPLIFT and POET – COPD trials of support initiating tiotropium (Spiriva®) as the preferred foundation maintenance therapy as it improves lung function, improves quality of life as well as reduces the risk of COPD exacerbations
In case of exacerbations, fenoterol (Berotec®) or combination of ipratropium/salbutamol (Combivent UDV®) can be used as reliever in every stage of COPD

Thank You