[email protected] Department of Surgical Sciences and Integrated Diagnostics (DISC) University of...
52
[email protected] Department of Surgical Sciences and Integrated Diagnostics (DISC) University of Genoa – IRCCS AOU San Martino IST – Genoa , Italy The Role of Intensive Care to Improve Perioperative Mortality Pelosi Paolo Dubai Anaesthesia 2013
-
Upload
diane-carter -
Category
Documents
-
view
217 -
download
0
Transcript of [email protected] Department of Surgical Sciences and Integrated Diagnostics (DISC) University of...

Department of Surgical Sciences and Integrated Diagnostics (DISC)
University of Genoa – IRCCS AOU San Martino IST – Genoa , Italy
The Role of Intensive Care to Improve
Perioperative Mortality
Pelosi Paolo
Dubai Anaesthesia 2013





Annual figures for the European
high-risk surgical population
• 21 million in-patient general procedures
• 2.6 million high-risk procedures
• 1.3 million patients develop complications
• 315,000 deaths in hospital
Ghaferi A. N Engl J Med 2009; 361: 1368-75
Weiser T Lancet 2008; 372: 139-144; Pearse R Crit Care 2006; 10: R81

Perioperative and anaesthetic-related mortality indeveloped and developing countries:
a systematic review and meta-analysisBainbridge et al Lancet 2012; 380: 1075–81
Perioperative mortality per year

Country Patients (n) and Mortality (%)
UK (Findlay G. 2011)
13.513 - 1.60
Netherlands(Noordzij PG. 2010)
3.667.875 - 1.84
Brasil(Yu PC. 2010)
32.659.515 - 1.77
USA(Glance LG. 2012)
322.398 - 1.34
Spain(Canet J. 2010)
2.464 - 1.44
Post-op mortality at 30 days in different countries

80% of surgical deaths are from the high-risk population
Overall Standard High-risk0
1
2
3
4
5
0
5
10
15
Size Mortality
Po
pu
lati
on
siz
e (
mil
lio
ns
)P
os
t-op
era
tive
mo
rtality
(%)
Pearse et al. Crit Care 2006; 10: R81.
Surgical deaths: Size, Risk and Mortality
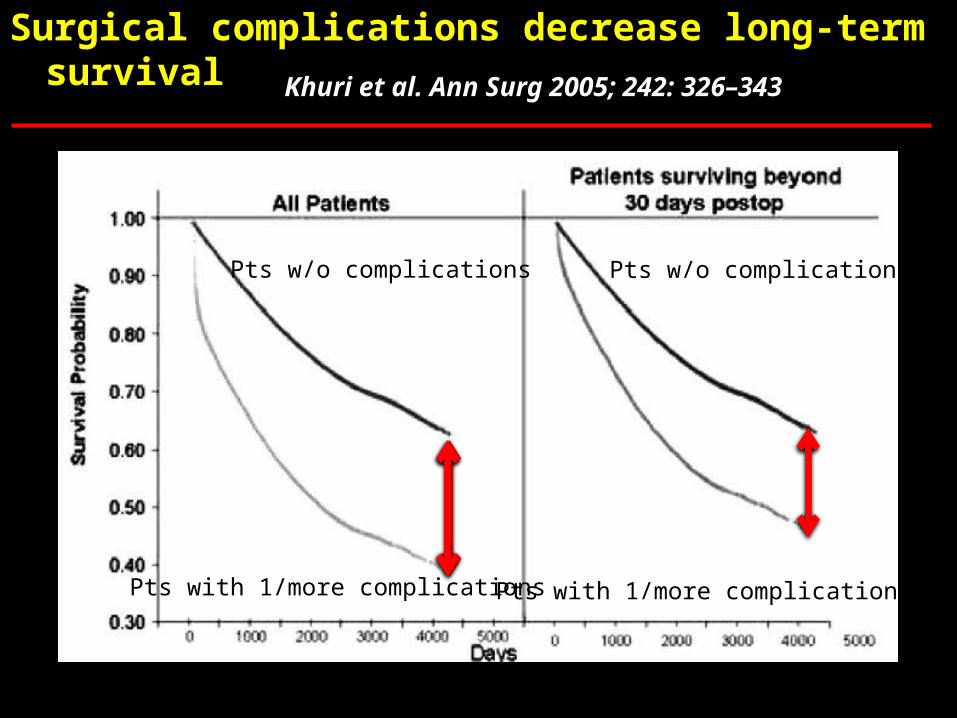
Surgical complications decrease long-term survival
Khuri et al. Ann Surg 2005; 242: 326–343
Pts w/o complications Pts w/o complications
Pts with 1/more complications Pts with 1/more complications

Variation in hospital mortality associatedwith in patient surgery
Ghaferi AA et al N Engl J Med 2009;361:1368-75.
ComplicationsPneumonia 1.8-2.4 %MV>48hr 6.3-8.1 %
Mortality Pneumonia 17-25.5%MV>48hr 20.6-30.1%

Euroanaesthesia 2010, Sunday, 13 June 2010
Eur J Anaesthesiol 2010;27:592–597

ESA Clinical Trials Network (ESA CTN)
Research Committee
Did you know that the most importantand challenging clinical questions
are more likely to be solved if severalcentres join forces ?



Poor quality of surgical outcome data
• Inaccurate healthcare systems data
• Specialty society data on limited subsets
• Mostly retrospective analyses
• Too much focus on elective surgery
• No comparative data across Europe

International seven day cohort study of
standards of care and clinical outcomes
for non-cardiac surgery
European Surgical Outcomes Study
EuSOS

European Surgical Outcomes StudyEuSOS
Lancet 2012; 380:1059-1065
Lancet 2012; 380:1059-1065

EuSOS: Inclusion criteria
All adult patients undergoing
in-patient non-cardiac surgery during the
seven day study period
Start: 09:00 4th April 2011
Finish: 08:59 11th April 2011
EuSOSEuropean Surgical Outcomes Study
Lancet 2012; 380:1059-1065

EuSOS: Exclusion criteria
• No planned overnight hospital stay
• Neurosurgery
• Obstetrics
• Cardiac surgery (thoracic surgery is included)
EuSOSEuropean Surgical Outcomes Study
Lancet 2012; 380:1059-1065

97
16
13
1
2
13
4
12
21
35
28
7
3
16
29
23
14
8
5
17 56
173
8
44
61923 Investigators !

EuSOS Cohort46539
Patients admitted in ICU
3612 (8%)
Patients admitted in ward
42927 (92%)
Died in ICU 287 (8%)
Died in ward1358 (3%)
Died in ward after ICU discharge
217 (6,5%)
Total Mortality 1682 (4%)

EuSOS Cohort46539 patients
1864 (4%) deaths
Elective surgery35040 (75%)
1132 (3%)
Urgent surgery8919 (19%)483 (5%)
Emergency surgery2557 (5%)249 (10%)
Planned admission
to ICU1864 (5%)
32 (2%)
Discharged to ward alive
2088 (97,5%)104 (5%)
Unplanned admission
to ICU278 (1%)22 (8%)
Unplanned admission
to ICU391 (4%)63 (16%)
Unplanned admission
to ICU356 (14%)79 (22%)
Planned admission
to ICU490 (5%)54 (11%)
Planned admission
to ICU201 (8%)37 (18%)
Discharged to ward alive764 (87%)
63 (8%)
Discharged to ward alive441 (79%)49 (11%)

Mortality Risk Factors
Variable Odds Ratio
Age (per year) 1
ASA IV-V 4.75-18.03
Metastatic Cancer 1.39
Cirrhosis 2.13
Urgent-Emergency surgery 1.78-3.23
Upper gastro-intestinal surgery 1.57
EuSOSEuropean Surgical Outcomes Study
Lancet 2012; 380:1059-1065

EuSOSEuropean Surgical Outcomes Study
Lancet 2012; 380:1059-1065
Which are the “safer” types of surgery ?
Laparoscopic surgery 0.75 – 0.25
Plastic/Cutaneous 0.71 – 0.66
Kidney/Urology 0.23 – 0.82
Head and Neck 0.66 - 0.81
Odds Ratio

European Surgical Outcomes StudyEuSOS
• Large numbers of patients die following in-patient non-cardiac surgery
• Large variations in mortality between countries suggest the need for national and international strategies to improve care for this patient group
• Patterns of critical care admission suggest process failure in the allocation of these resources
Lancet 2012; 380:1059-1065
EuSOS: Conclusions

European Surgical Outcomes Study

Message to be delivered:
Dear Colleagues funding medical care, ……care.
“We suggest that even use of expensiveresources, such as additional ICU beds, could rapidly become cost effective by reducing complications”.
Vonlanthen R and Clavien PA. Lancet. 2012 Sep 22;380(9847):1034-6
What factors affect mortality after surgery?

Lancet 2012; 380:1059-1065; Intensive Care Med 2012; 38:1647-1653
Peri-op Mortality and GDP/inhabitant
R = 0.55P < 0.01
MORTALITY (%)

The definition of ICU beds (recovery room vs post-op ICU vs General ICU) and resources might differ between countries
Other factors are important:- Use of surgical safety checklists- Clinical pathways- Enhanced recovery strategy (fast track surgery)- Volume of cases- Presence of general versus specialised surgeons- Ability to recognise and manage complications- Quality of care and Economic resources
What factors affect mortality after surgery?
Vonlanthen R and Clavien PA. Lancet. 2012 Sep 22;380(9847):1034-6

Need of Surgery
Comorbidity- Age (per year)- ASA IV-V- Metastatic cancer- Cirrhosis
High risk surgery- Urgent/emergency- Upper gastro-intestinal
No comorbidityNo high risk
surgery
High risk surgeryand
No comorbidity
Comorbidityand
No High risk surgery
High risk surgery
and comorbidity
Surgical ward Surgical ward/ monitoring
Surgical ward/monitoring
orPost-op ICU
Post-op ICUand
monitoring in ward after discharge

PPCs: are they a problem?
• Variable incidence (2%-40%), depending on definition, kind of surgery and patients
• Prevalence: as cardiac complications
• Leading cause of long hospital stay and mortality
• Etiology: anesthesia and surgery induce changes

Post-operative pulmonary complications:EFFECTS ON SURVIVAL
Fernandez-Perez et al Thorax 2009;64;121-127

PPCs

Anesthesiology 2011: 115: 10-11
Pelosi P and Gama de Abreu M

How to evaluate the risk of PPCs ?
11
13 % (score 26-44) – 54 % (score >45) risk to develop PPCs
Canet J et al for ARISCAT, Anesthesiology. 2010; 113(6):1338-50.

Steering Committee:
Jaume Canet (S)Sergi Sabaté (S)Valentín Mazo (S)Lluis Gallart (S)Marcelo Gama de Abreu (G)Javier Belda (S)Olivier Langeron (F)Andreas Hoeft (G)Paolo Pelosi (I)Brigitte Leva (ESA Secretariat) (B)
Prospective Evaluation of a RISk Score for
postoperative pulmonary COmPlications
in Europe

Methods 1/5
Design
– Prospective, multicenter, observational, cohort study
Geographic scope
– ARISCAT: 51 Anesthesiology Departments (Catalonia, Spain)
– PERISCOPE: 63 Anesthesiology Departments (21 European countries)

Methods 2/5
Data collection
– 7 days
• ARISCAT: January 2006 – January 2007
– Randomized days (one for each day of the week) for each center.
• PERISCOPE: May 2011 – August 2011
– Continuous days (a full week)

Methods 3/5
• Inclusion criteria
– Undergoing a surgical procedure under regional or general anesthesia (epidural, spinal or saddle block) ...
– ... on the selected days at a participating center
– Informed consent

Methods 4/5
• Exclusion criteria– Age < 18 years– Obstetric/childbirth procedures– Local or peripheral nerve anesthesia with or without
sedation– Diagnostic and therapeutic procedures outside the
operating room– Intubated on arrival at the operating room– Re-operation due to an in-hospital postoperative
complication – Transplantss and brain-dead patients

Primary outcome (composite) Respiratory insufficiency Bronchospasm Pleural effusion Respiratory infection Atelectasis Aspiration pneumonitis Pneumothorax
Methods 5/5
Unified definitions of variables

PPCs Incidence
ARISCAT development subsample
ARISCAT validation subsample
PERISCOPE sample0
1
2
3
4
5
6
7
8
9
PPC (%)
7.92%
4.37%
6.21%5384 patients

PPCs or CHF ?

PPCs & Surgical Speciality

Lenght of Hospital Stay
Periscope Ariscat
Patients without PPCs
Patients with PPCs
3(1-10.9)
3(1-11.0)
9(4-33)
12(4-36.8)
Median (10th -90th percentile)
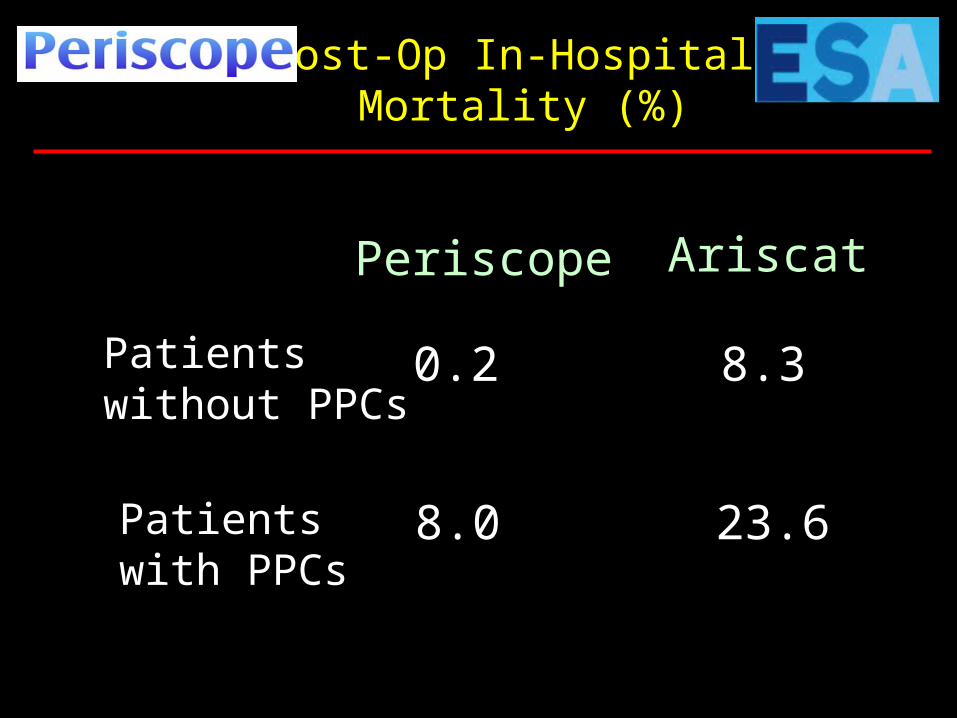
Periscope Ariscat
Patients without PPCs
Patients with PPCs
0.2 8.3
8.0 23.6
Post-Op In-Hospital Mortality (%)

PLOS and In–Hospital Mortality & PPCs

Conclusions
• Postoperative pulmonary complications are frequent, expensive and associated with increased mortality
• There is increased national focus on the need for higher quality, safer and more appropriate care.
• Readmission of surgical patients with pneumonia is a significant source of increased healthcare costs.

Conclusions
• Strongest risk factors for PPCs are age, preoperative SpO2, previous respiratory infection, anemia, kind of surgery and surgical aggressiveness
• More than 50% of the risk is related to patient factors
• A risk index based on 7 objective factors discriminates well across a wide range of patients, surgeries and geographic areas.
• Stratifying risk for PPCs can be calculated preoperatively and, in case, recalibrated.

The ICUs & Hospital activities
GeneralICU
In HospitalEmergencies
In HospitalPlanned
Critical Care
Step-Down ICU
Ward
SpecializedICUs
Out of HospitalEmergencies

Thanks