
PowerPoint Presentation Trial: Number Needed to Treat (NNT) to prevent a primary outcome in one...
33
Transcript of PowerPoint Presentation Trial: Number Needed to Treat (NNT) to prevent a primary outcome in one...



IHD mortality (floating absolute risk and 95% CI)
Usual SBP (mm Hg)
IHD, ischemic heart disease. Prospective Studies Collaboration. Lancet. 2002;360:1903-1913.
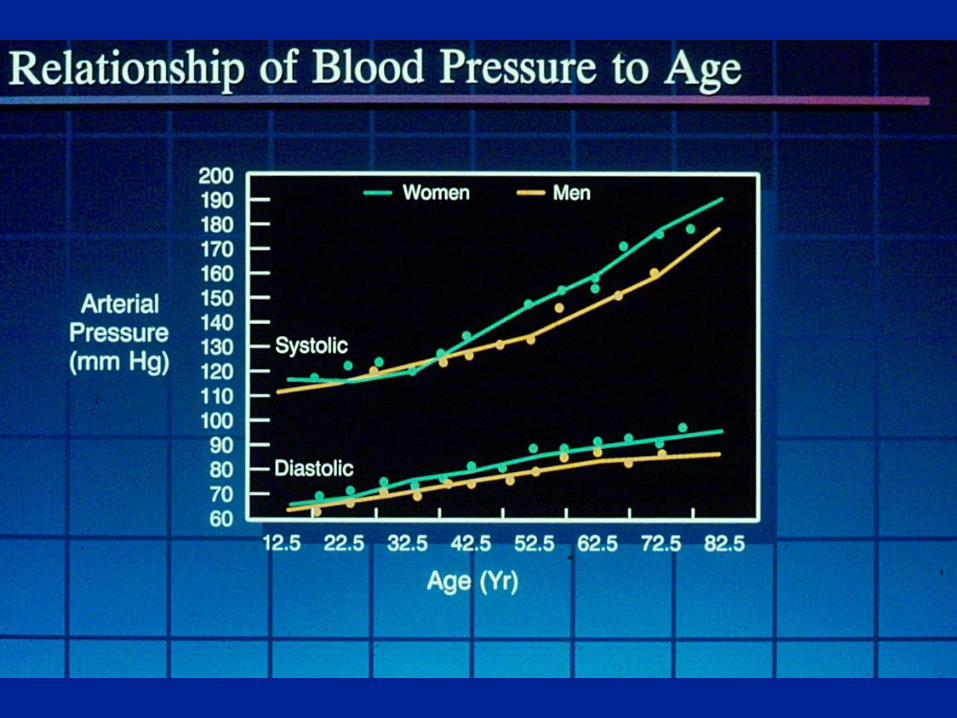
Ischemic Heart Disease Mortality Rate in Each Decade of Age
120 140 160 180
256
128
64
32
16
8
4
2
1
SBP
40-49 y
Age at risk:
70-79 y
60-69 y
50-59 y
80-89 y
Usual DBP (mm Hg)
70 80 90 110 100
256
128
64
32
16
8
4
2
1
DBP
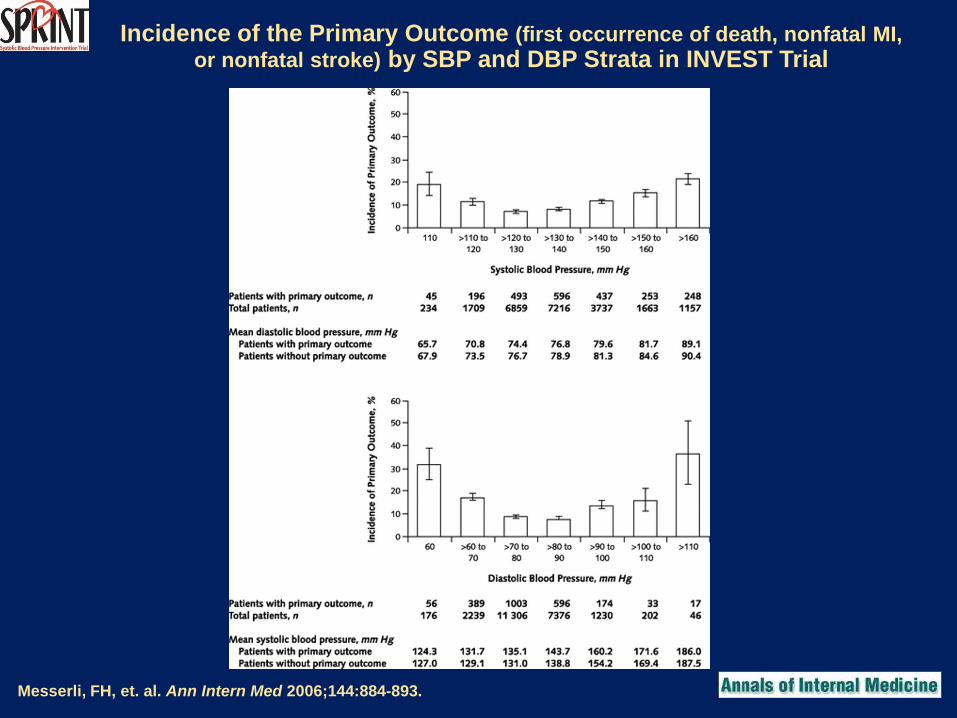
Incidence of the Primary Outcome (first occurrence of death, nonfatal MI,
or nonfatal stroke) by SBP and DBP Strata in INVEST Trial
Messerli, FH, et. al. Ann Intern Med 2006;144:884-893.

Blo
od
pressu
re (
mm
Hg
)
0 12 36 60 Months of follow-
up
SHEP Average Blood Pressure During Follow-up
24 48
50
65
80
95
110
125
140
155
170
185
200
0
SHEP=Systolic Hypertension in the Elderly Program SHEP Research Group. JAMA. 1991;265:3255-3264. Copyright ©1991, American Medical Association.
0
1
2
3
4
5
6
7
8
9
10
Cu
mu
lati
ve s
tro
ke r
ate
p
er 1
00
perso
ns
0 12 36 60
Months of follow-up
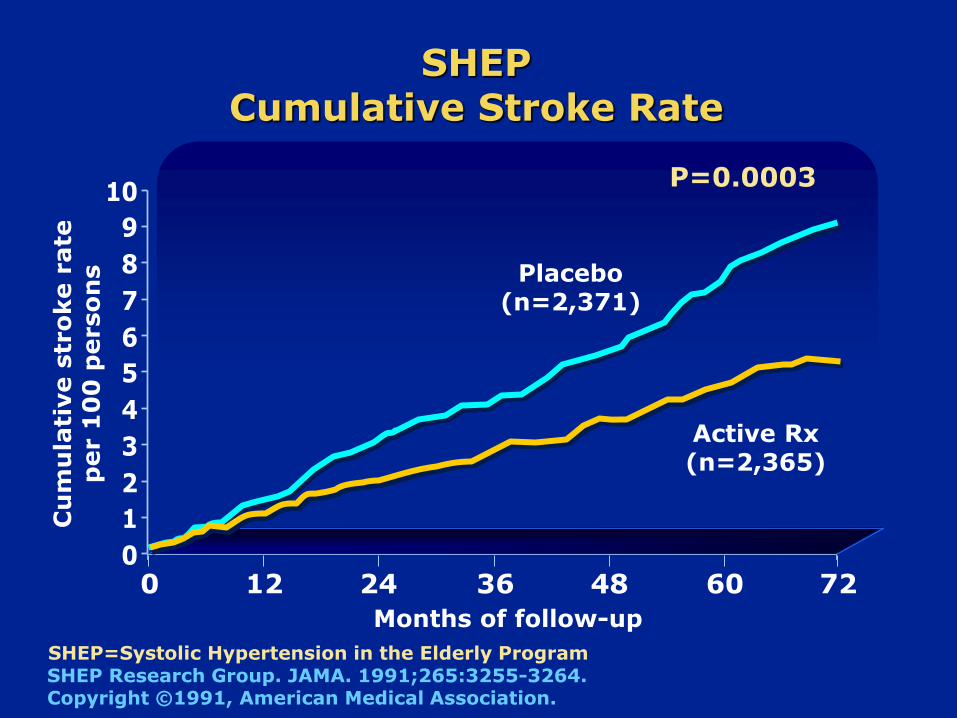
SHEP Cumulative Stroke Rate
24 48 72
P=0.0003
Placebo (n=2,371)
Active Rx (n=2,365)
SHEP=Systolic Hypertension in the Elderly Program SHEP Research Group. JAMA. 1991;265:3255-3264. Copyright ©1991, American Medical Association.

0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
Rela
tive r
isk (
95
% C
I)
Stroke CHD
Active Therapy vs. Placebo
CHF Death
0.63
0.46
0.68
0.87
CVD
0.75
SHEP Cardiovascular Disease Endpoints
SHEP Research Group. JAMA. 1991;265:3255-3264.
SHEP=Systolic Hypertension in the Elderly Program
CHD=coronary heart disease; CHF=congestive heart failure; CVD=cardiovascular disease
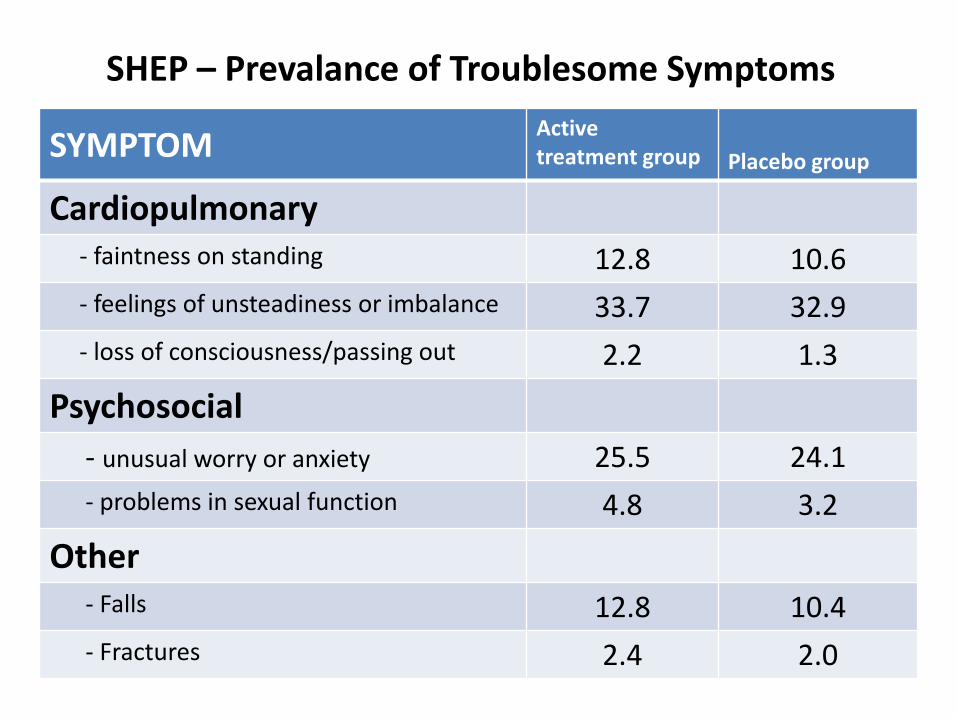
SYMPTOM Active treatment group Placebo group
Cardiopulmonary - faintness on standing 12.8 10.6
- feelings of unsteadiness or imbalance 33.7 32.9
- loss of consciousness/passing out 2.2 1.3
Psychosocial
- unusual worry or anxiety 25.5 24.1
- problems in sexual function 4.8 3.2
Other - Falls 12.8 10.4
- Fractures 2.4 2.0
SHEP – Prevalance of Troublesome Symptoms
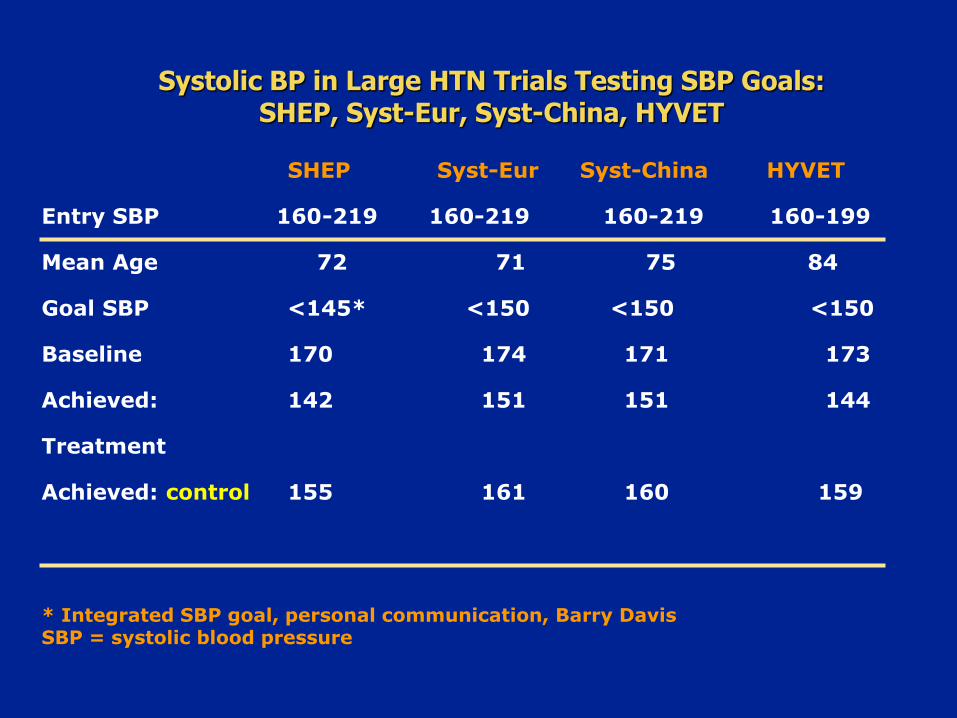
SHEP Syst-Eur Syst-China HYVET
Entry SBP 160-219 160-219 160-219 160-199
Mean Age 72 71 75 84
Goal SBP <145* <150 <150 <150
Baseline 170 174 171 173
Achieved: 142 151 151 144
Treatment
Achieved: control 155 161 160 159
Systolic BP in Large HTN Trials Testing SBP Goals: SHEP, Syst-Eur, Syst-China, HYVET
* Integrated SBP goal, personal communication, Barry Davis SBP = systolic blood pressure

All stroke (30% reduction)
Placebo
IndapamideSR ±perindopril
Indapamide
SR
±perindopril
Placebo
P=0.055
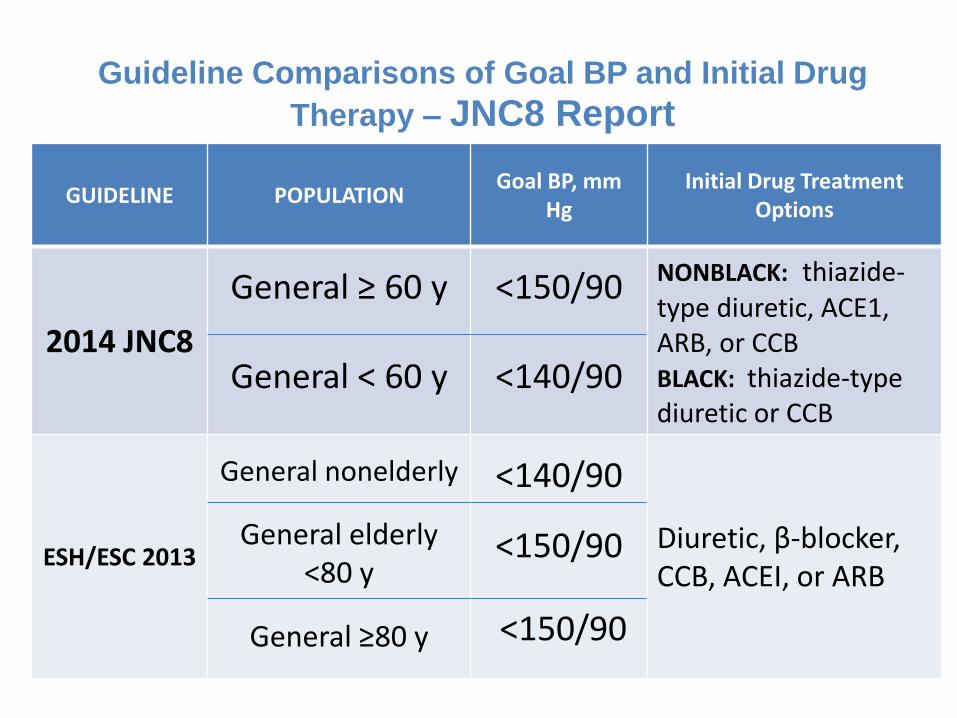
GUIDELINE POPULATION Goal BP, mm
Hg Initial Drug Treatment
Options
2014 JNC8
General ≥ 60 y
General < 60 y
<150/90
<140/90
NONBLACK: thiazide-type diuretic, ACE1, ARB, or CCB BLACK: thiazide‐type diuretic or CCB
ESH/ESC 2013
General nonelderly
General elderly <80 y
General ≥80 y
<140/90
<150/90
<150/90
Diuretic, β‐blocker, CCB, ACEI, or ARB
Guideline Comparisons of Goal BP and Initial Drug
Therapy – JNC8 Report

ACCORD Double 2 x 2 Factorial Design
Intensive
Glycemic
Control 5128
Standard
Glycemic
Control 5123
Lipid BP
Placebo Fibrate Intensive
<120 mm
Standard
<140 mm
2371 2362 2753 2765
1383 1374
1391 1370
1193
1178 1184
1178
10,251
4733* 5518 * 94% power for 20% reduction in event rate, assuming
standard group rate of 4% / yr and 5.6 yrs follow-up
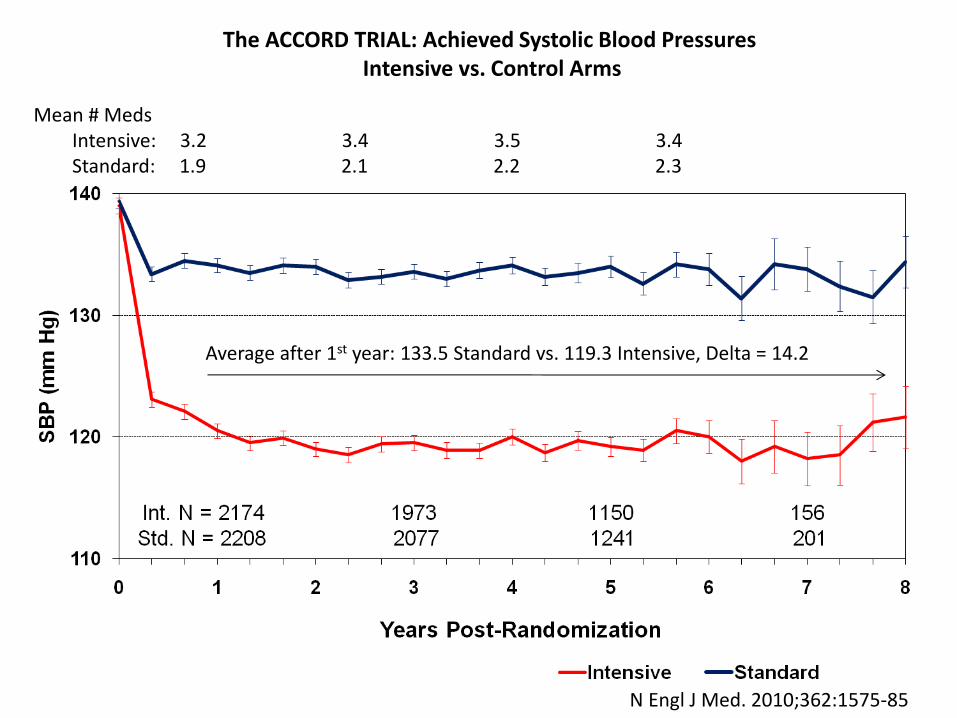
Average after 1st year: 133.5 Standard vs. 119.3 Intensive, Delta = 14.2
Mean # Meds Intensive: 3.2 3.4 3.5 3.4 Standard: 1.9 2.1 2.2 2.3
N Engl J Med. 2010;362:1575-85
The ACCORD TRIAL: Achieved Systolic Blood Pressures Intensive vs. Control Arms
Pa
tie
nts
wit
h E
ve
nts
(%
)
0
5
10
15
20
Years Post-Randomization
0 1 2 3 4 5 6 7 8
Pati
en
ts w
ith
Even
ts (
%)
0
5
10
15
20
Years Post-Randomization
0 1 2 3 4 5 6 7 8
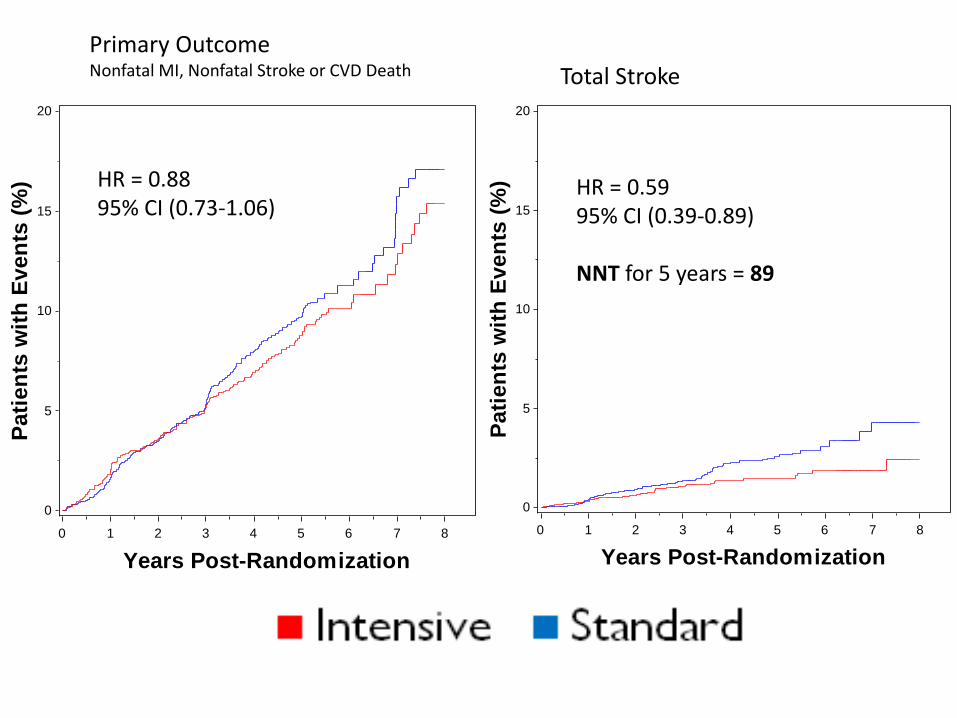
Primary Outcome Nonfatal MI, Nonfatal Stroke or CVD Death Total Stroke
HR = 0.88 95% CI (0.73-1.06)
HR = 0.59 95% CI (0.39-0.89) NNT for 5 years = 89

Background – SPRINT Senior
• Prevalence of hypertension is > 75% among those 75 years of age or older
• Optimal SBP target especially controversial in older, frail patients
• Observational evidence of inverse relationship between SBP and mortality
• Concerns regarding falls and fall-related injury due to antihypertensive therapy
• Cognitive and quality of life outcomes not certain
17
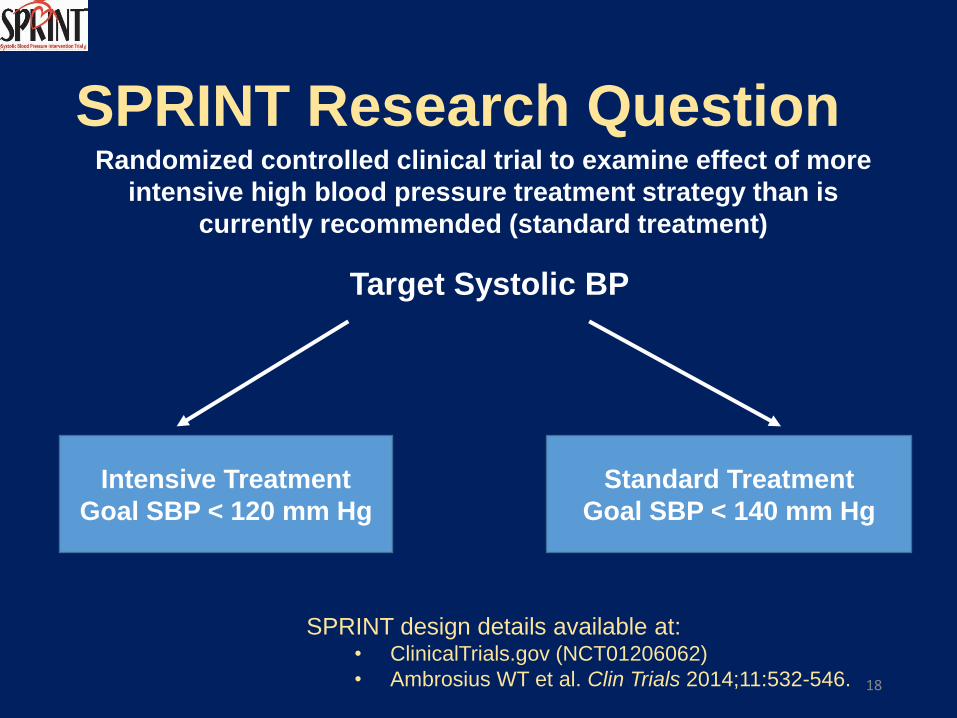
SPRINT Research Question Randomized controlled clinical trial to examine effect of more
intensive high blood pressure treatment strategy than is
currently recommended (standard treatment)
Target Systolic BP
Intensive Treatment
Goal SBP < 120 mm Hg
Standard Treatment
Goal SBP < 140 mm Hg
SPRINT design details available at: • ClinicalTrials.gov (NCT01206062)
• Ambrosius WT et al. Clin Trials 2014;11:532-546. 18
Major Inclusion Criteria
• ≥50 years old
• Systolic blood pressure: 130 – 180 mm Hg, allowed to be on up to 4 antihypertensive medications depending on SBP
• Additional cardiovascular disease (CVD) risk
• Clinical or subclinical CVD (excluding stroke)
• Chronic kidney disease (CKD), defined as eGFR
20 – <60 ml/min/1.73m2 based on MDRD equation
• Framingham Risk Score for 10-year CVD risk ≥ 15%
• Age ≥ 75 years
At least one of these risk factors
19

BP Interventions • BP monitored monthly for 3 months and every 3
months thereafter (additional visits could be scheduled)
• Antihypertensive medication titration decisions based on mean BP (3 readings at each visit), using a structured stepped-care approach
• Agents from major antihypertensive drug classes available free of charge
• Periodic assessment for orthostatic hypotension and related symptoms
• Intensive participants started on 2 drugs, with option of starting with 1 drug in those 75+ years. 2nd drug then added at second visit if not at goal
• Standard group participants were down-titrated if BP too low.
20
Major Exclusion Criteria
• Stroke
• Diabetes mellitus
• Polycystic kidney disease
• Congestive heart failure (symptoms or EF < 35%)
• Proteinuria >1g/d
• CKD with eGFR < 20 mL/min/1.73m2 (MDRD)
• Adherence concerns
21

Baseline Characteristics
Total N=9361
Intensive N=4678
Standard N=4683
Mean (SD) age, years 67.9 (9.4) 67.9 (9.4) 67.9 (9.5) % ≥75 years 28.2% 28.2% 28.2% Female, % 35.6% 36.0% 35.2% White, % 57.7% 57.7% 57.7% African-American, % 29.9% 29.5% 30.4% Hispanic, % 10.5% 10.8% 10.3% Prior CVD, % 20.1% 20.1% 20.0% Mean 10-yr Framingham CVD risk, % 20.1% 20.1% 20.1%
Not taking antihypertensive meds, % 9.4% 9.2% 9.6%
Mean (SD) number of antihypertensive meds
1.8 (1.0) 1.8 (1.0) 1.8 (1.0)
Mean (SD) Baseline BP, mm Hg
Systolic 139.7 (15.6) 139.7 (15.8) 139.7 (15.4)
Diastolic 78.1 (11.9) 78.2 (11.9) 78.0 (12.0) 22
The SPRINT Research Group. N Engl J Med 2015. DOI: 10.1056/NEJMoa1511939
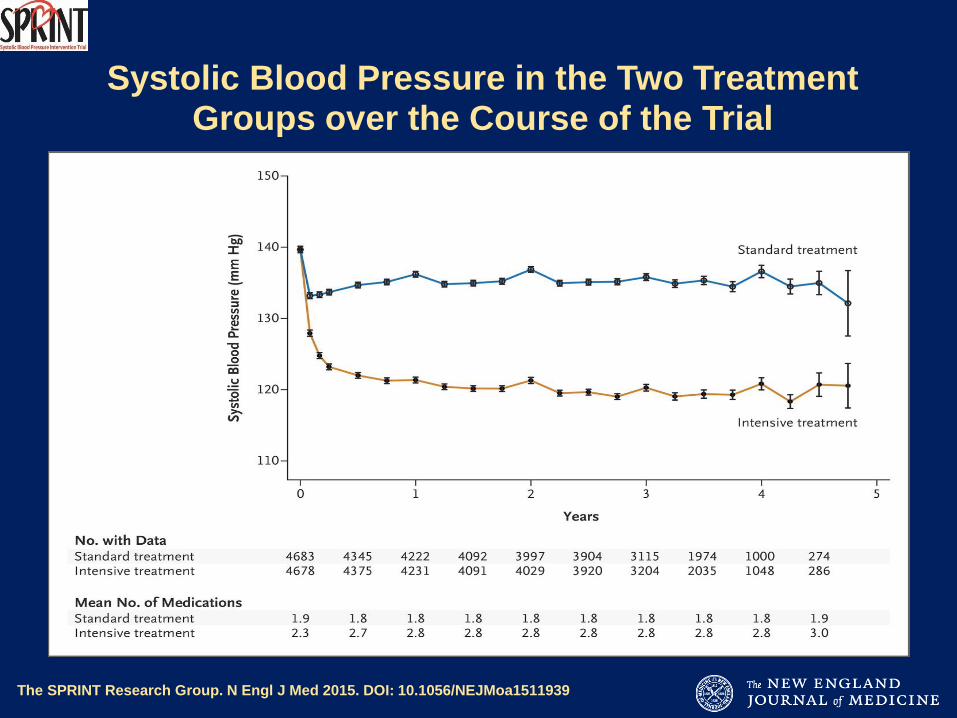
Systolic Blood Pressure in the Two Treatment Groups over the Course of the Trial

Decision to Stop BP Intervention
• On August 20, 2015, NHLBI Director (Dr. Gary Gibbons) accepted the DSMB recommendation to inform SPRINT investigators and participants of CVD results
• Concurrently, decision made to stop BP intervention
• Blinded data for secondary non-CVD outcomes (e.g., dementia and cognitive impairment) being collected at final close-out visit and this process will be completed in 2016
24

The SPRINT Research Group. N Engl J Med 2015. DOI: 10.1056/NEJMoa1511939
Primary Outcome and Death from Any Cause
During Trial: Number Needed to Treat (NNT) to prevent a primary outcome in one participant = 61
During Trial: Number Needed to Treat (NNT) to prevent death in one participant = 90
The SPRINT Research Group. N Engl J Med 2015. DOI: 10.1056/NEJMoa1511939
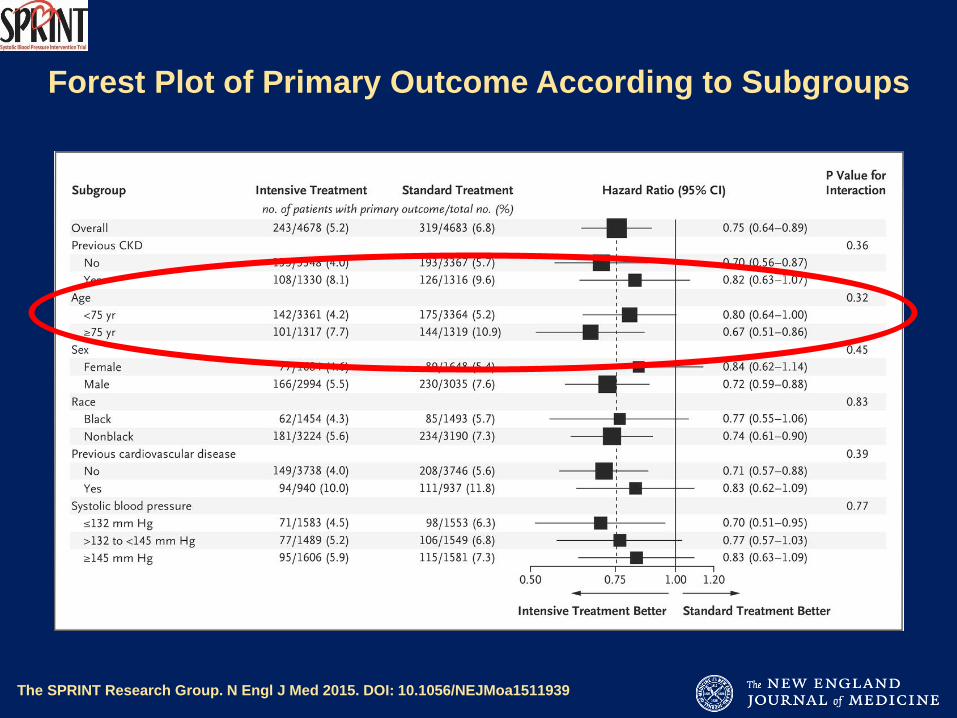
Forest Plot of Primary Outcome According to Subgroups

Hypertension in the Very Elderly Trial (HYVET)
“We found no evidence of an interaction between baseline FI and treatment with antihypertensives on risk of stroke, death from all causes, or cardiovascular events in very elderly people. Furthermore, the burden of frailty was similar to that seen in population studies.”
Warwick et al. BMC Medicine 2015;13(1):1-8.
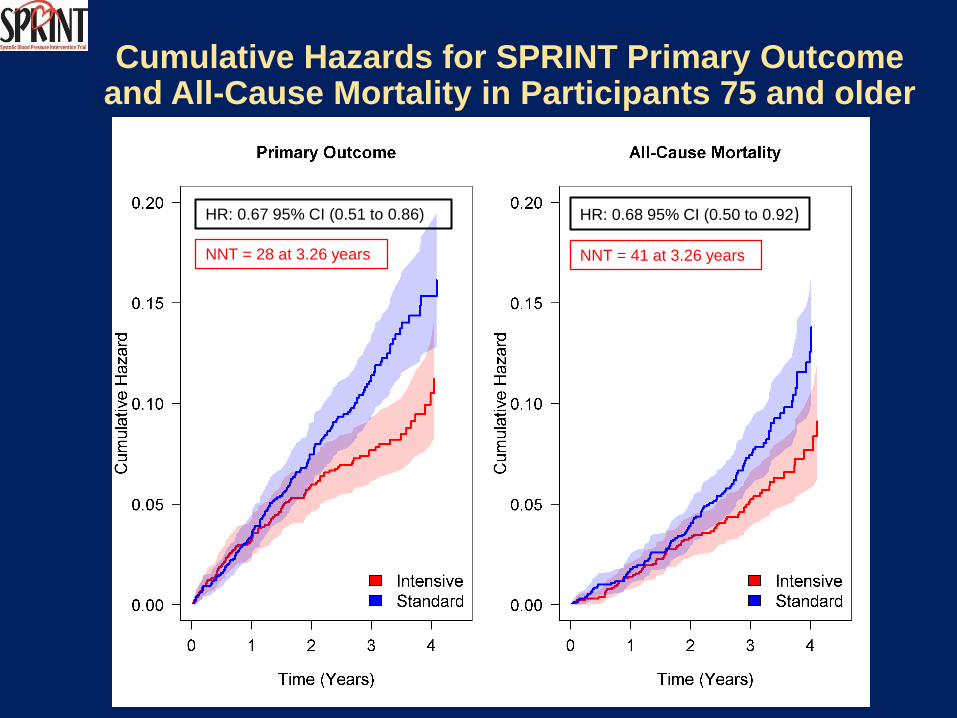
Cumulative Hazards for SPRINT Primary Outcome and All-Cause Mortality in Participants 75 and older
HR: 0.67 95% CI (0.51 to 0.86)
NNT = 28 at 3.26 years
HR: 0.68 95% CI (0.50 to 0.92)
NNT = 41 at 3.26 years
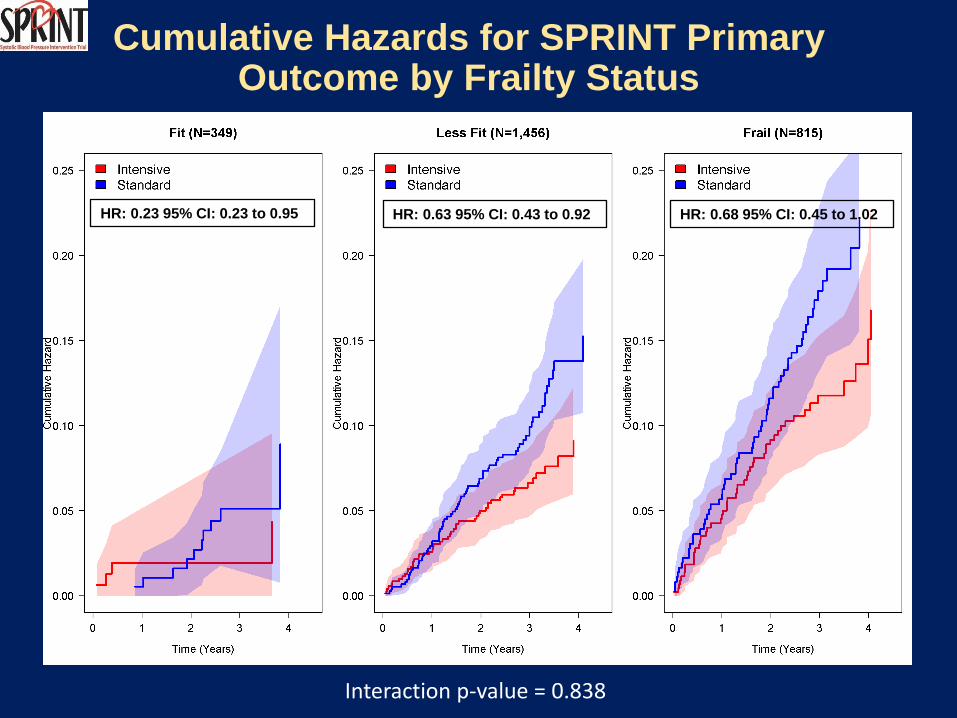
Cumulative Hazards for SPRINT Primary Outcome by Frailty Status
HR: 0.23 95% CI: 0.23 to 0.95 HR: 0.63 95% CI: 0.43 to 0.92 HR: 0.68 95% CI: 0.45 to 1.02
Interaction p-value = 0.838

Cumulative Hazards for SPRINT Primary Outcome by Gait Speed
HR: 0.65 95% CI: 0.41 to 1.02 HR: 0.68 95% CI: 0.48 to 0.95
Interaction p-value = 0.732
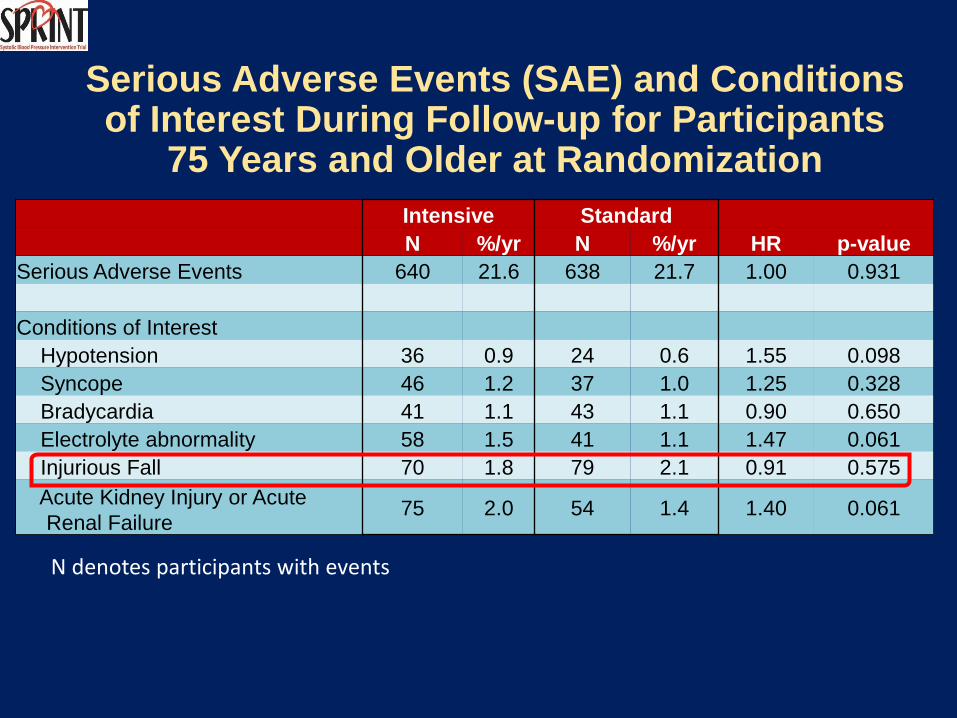
Serious Adverse Events (SAE) and Conditions of Interest During Follow-up for Participants
75 Years and Older at Randomization
Intensive Standard
N %/yr N %/yr HR p-value
Serious Adverse Events 640 21.6 638 21.7 1.00 0.931
Conditions of Interest
Hypotension 36 0.9 24 0.6 1.55 0.098
Syncope 46 1.2 37 1.0 1.25 0.328
Bradycardia 41 1.1 43 1.1 0.90 0.650
Electrolyte abnormality 58 1.5 41 1.1 1.47 0.061
Injurious Fall 70 1.8 79 2.1 0.91 0.575
Acute Kidney Injury or Acute
Renal Failure 75 2.0 54 1.4 1.40 0.061
N denotes participants with events

Summary and Conclusions
• SPRINT was designed to examine effects of more intensive
antihypertensive therapy than currently recommended
• Rapid and sustained difference in SBP achieved between the 2
treatment arms regardless of age or frailty status
• Trial stopped early, due to CVD & mortality benefit, after a
median follow-up of 3.3 years
• For persons age 75+, incidence of primary outcome (composite
of CVD events) 33% lower in Intensive compared to Standard
Group and all-cause mortality reduced by 32%
• The “number needed to treat” for age 75+ to prevent a primary
outcome event or death during a median follow-up of 3.26 years
was 28 and 41, respectively
Relevance of Frailty to SPRINT
• Translation of clinical trial results into clinical practice
• Concerns about selection biases and generalizability of trial cohorts, especially for geriatric populations
• For example, recruitment for the Hypertension in the Very Elderly Trial (HYVET) mainly from Eastern Europe and China, may not generalize well to Western, developed countries1
• Concern is that trial cohorts are healthier, have less co-morbidity, are less frail, which perhaps limits external validity to clinical practice
1Morley JE. J Am Geriatr Soc 2013;61:1197-8.


















