PowerPoint Presentation...Title PowerPoint Presentation Author Sharon Baudry Created Date 5/17/2016...
35
International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected] Medical management of advanced PD Raja Mehanna MD
Transcript of PowerPoint Presentation...Title PowerPoint Presentation Author Sharon Baudry Created Date 5/17/2016...

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Medical management of
advanced PD Raja Mehanna MD

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
What is advanced PD?
• Levodopa is the most effective symptomatic treatment for PD
• All PD patients eventually require levodopa.
• Chronic levodopa treatment -> motor complications – ELLDOPA: 9 months on levodopa 200 mg tid: 16%
developed dyskinesia and 20% had motor fluctuations
– Higher risk with younger age at onset and high dose of levodopa
• Motor complications (MF and /or LID) = advanced PD
Olanow et al.,2001; Agid et al., 2002; Miyasaki et al., 2002; Rascol et al., 2002; Korczyn et al., 2002

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
OFF

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
ON

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Why does it happen?
• Motor effects of levodopa
– Presynaptic mechanisms (synthesis and
storage of dopamine in remaining nigral
neurons)
– Postsynaptic mechanisms (activation of
postsynaptic dopamine receptors on striatal
neurons)
Fabbrini et al., 1988

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
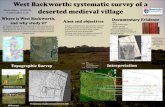
L Dopa central pharmacodynamic
Early PD Late PD
Mouradian et al., 1988

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
THERAPEUTIC
WINDOW
0 5 10 15
Change in therapeutic window with PD progression
Years from symptom
onset
ON
OFF
ON
OFF
BRADYKINESIA
DYSKINESIA
THERAPEUTIC WINDOW

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Dyskinesia Threshold “on”
“off”
Levodopa 2 4 6 hours
Early Parkinson’s disease

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
“on”
Dyskinesia Threshold
“off”
Levodopa 2 4 6 hours
Moderate Parkinson’s disease

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
“on”
Dyskinesia Threshold
off”
Levodopa 2 4 6 hours
Late Parkinson’s disease

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
OFF

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
ON w LID

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
How can we manage it?
• Medical management.
• Deep Brain Stimulation
• Infusion therapies.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
How can we manage it?
• Medical management.
• Deep Brain Stimulation
• Infusion therapies.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Medical management
• MF
– Manipulate C/L
– Dopamine agonists
– MAO-I
– COMT-I
• LID
– Fractionating
– Amantadine
– Namenda?Clozapine? Levetiracetam?

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Manipulate C/L
• Dropped dose or delayed latency: Take far
form high protein meals (1 hour b/a)
• Unpredictable effects of dose : Switch CR
to IR
• Delayed latency: Dissolvable C/L
(Madopar, parcopa) or diluting IR in
ascorbic acid drink
Nutt JG et al., 1984; Leenders et al., 1986; Stocchi et al., 1996;Stocchi et al., 2008

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
COMT-I
• Entacapone , Tolcapone
• Addition to C/L
• Increases ON time by 1.3 to 1.8 hours/day
and increases UPDRS.
• Increases risk of LID if used in early PD
Rinne et al., 1998; The Parkinson Study Group 1997; Deane et al., 2004, Stocchi et al., 2010

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
MAOB-I
• Rasagiline
• PRESTO – n= 472, RCT, add on Rasagiline 0.5 mg vs 1 mg vs
placebo, f/u 26 weeks.
– Decreased OFF time by 1.85h (1mg), 1.41h (0.5mg) and 0.91h (P)
• LARGO – n= 687, RCT, add on Rasagiline 1 mg (R) vs
Entacapone (E) vs placebo (P) , 18 weeks f/u.
– Decreased OFF time by 1.2h with R or E , 0.4 h with P
– Increased ON w/o troublesome LID: 0.85h with R or E, 0.03 with P

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
MAOB-I
• Selegiline
– Usually in early PD as dopamin paring
– Showed to decreased OFF time when added
to C/L
• Selegiline ODT
– Bypasses first-pass hepatic metabolism
– Add on to C/L decreases OFF time by 1.6
hours v/s placebo
Golbe et al., 1988.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Dopamine agonists
• Pergolide, cabergoline: valvular fibrotic disease/ pulmonary fibrosis.
• Pramipexole, ropinirole, rotigotine.
• Added to C/L, decrease OFF time by 1.1 to 1.5 hours/day
• More so with ER tablets and patch
• Useful for nighttime symptoms
• Can decrease LID indirectly by decreasing C/L dose by up to 30%
• SE: EDS, ICD, leg edema, cognitive impairment, hallucinations
Olanow et al., 1994; Lieberman et al., 1998; Pinter et al., 1999; Clarke et al.,2001

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Apomorphine
• SubQ only
• Very short latency and half-life
• Dropped dose, unexpected OFF
• First dose always in clinic wih EKG and
BP monitoring
• Individualized dose 2-5mg
Frankel et al., 1990; Hughes et al.,1993; Attanasio A, et al., 1990.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
LID
Peak dose LID vs DID

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Peak dose LID
• Fractionation of C/L
– Give smaller doses at smaller interval: try to
avoid peak effect
• Decrease C/L and start/increase DA
Facca and Sanchez-Ramos , 1996; Cristina et al., 2003; Storch et al., 2005.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Amantadine
• Amantadine
– Decreases LID scores by 45-60% w/o
worsening OFF Sustained effect
– SE: hallucination and cognitive issues
• Some concern that this effect does not last
Verhagen et al.,1998; Luginger et al., 2000.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Amantadine
• AMANDYSK trial , 2014
– Multicenter RCT placebo-controlled, parallel-group, wash-out study , n=57 PD with LID, on amantadine ≥200 mg/d for ≥6 months, 3 months f/u.
– Mean duration of therapy: 2.7 y (placebo), 4.3y (treatment), p=0.16
– In discontinuing group: • LID worsened in duration and severity.
• Drop out 2/2 LID
• Apathy and fatigue worsened.
– No difference in UPDRS III between the groups.
Ory-Magne et al., 2014

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Antipsychotics
• Clozapine
– Atypical antipsychotic
– In 1 RTC, decreased LID by 1.5 hour/day
– SE: sedation, agranulocytosis
• Other antipsychotics: not proven and likely
to worsen motor symptoms of PD
Durif et al., 2004

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Levetiracetam
• Zesiewicz et al., 2005
– Open-label, n= 9 PD with LID, increased ON
w/o LID from 43% to 61% of the day
– Decreased ON with troublesome LID from
23% to 11%
– 50% drop out (somnolence)

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Leviteracetam
• Wong et al., 2011 – RCT, cross over, n=16, 6 weeks x 2 + 4 week
wash out. Titration of Leviteracetam 500mg weekly up to 200 mg/day.
– Hourly videotaped dyskinesia assessments and UPDRS on 1 day at the end of each treatment period.
– Direct observation: LID slightly less on placebo (P = .26).
– Patient diary: LID less on placebo (P = .10).
– Parkinsonism a little worse on levetiracetam (P = .05).

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Memantine
• Wictorin and Widner, 2016
– RCT , n=15, 3 weeks, memantine 20 mg v/s
placebo
– No change in LID ratings, but
• 7/15 reduced LID score by 32%
• 5/15 no change
• 3/15 worsened by 33%
• 35% reduction of LID in self administered diaries
(25%-> 16%)
• No side effects

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
DA vs MAOB-I vs COMT
• Stowe et al., 2010, Cochrane Database review.
– Metanalysis: 44 trials, n=8436.
– Compared to placebo, adjuvant therapy
significantly
• Reduced off-time ,
• Reduced levodopa dose
• Improved UPDRS scores
– However, dyskinesia and SE increased:,
constipation, dizziness, dry mouth , hallucinations,
hypotension, insomnia , nausea , somnolence and
vomiting .

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
DA vs MAOB-I vs COMT
• Indirect comparisons of the three drug classes : – Impact on OFF time :DA: -1.54 hours/day;
COMTI: -0.83 hours/day; MAOBI: -0.93 hours/day;
– Decrease in L-dopa dose : DA: -116 mg/day; COMTI: -52 mg/day; MAOBI: -29 mg/day;
– Change in total UPDRS scores : DA: -10.01 point COMTI: -1.46 ; MAOBI: -2.20 points;
– LID : DA :OR 2.70;COMTI :OR 2.50: than with MAOBI :OR 0.94.
– Other side effects: DA : OR 1.52 ;COMTI :OR 2.0; MAOBI :OR 1.32

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
Non Motor Symptoms in PD
• Depression – Paroxetine and venlafaxine
• Dementia – Donepezil and rivastigmine
• Hallucinations – Quetiapine, clozapine and pimavanserine
• Constipation – Lubiprostone and polyethylene glycol
• Urinary urgency
• Orthostatic hypotension – droxidopa
• REM Sleep Behavior disorder
• EDS
• Dysphagia – ST
• Dysarthria – ST
• Falls/gait disorders – PT

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
References
• Agid Y, Olanow C, Mizuno Y. Levodopa: why the controversy? Lancet 2002;360:575.
• Attanasio A, Capria C, Leggiardro G, et al. Transient cardiac arrest during continuous intravenous infusion of
apomorphine. Lancet 1990;336:1321.
• Clarke CE, Deane KH. Cabergoline for levodopa-induced complications in Parkinson’s disease. Cochrane
Database Syst Rev 2001;1:CD001518.
• Cristina S, Zangaglia R, Mancini F, Martignoni E, Nappi G, Pacchetti C. High-dose ropinirole in advanced
Parkinson’s disease with severe dyskinesias. Clin Neuropharmacol 2003;26: 146–150.
• Deane KH, Spieker S, Clarke CE. Catechol-O-methyltransferase inhibitors for levodopa-induced complications in
Parkinson’s disease. Cochrane Database Syst Rev 2004;4: CD004554.
• Durif F, Debilly B, Galitzky M, Morand D, Viallet F, Borg M, Thobois S, Broussolle E, Rascol O. Clozapine improves
dyskinesias in Parkinson disease: a double-blind, placebo-controlled study. Neurology 2004;62:381–388.
• Fabbrini G, Mouradian MM, Juncos J, et al. Motor fluctuations in Parkinson’s disease: central pathophysiological
mechanisms, Part I. Ann Neurol 1988;24:366–371.
• Facca A, Sanchez-Ramos J. High-dose pergolide monotherapy in the treatment of severe levodopa-induced
dyskinesias. Mov Disord 1996;11:327–329.
• Frankel JP, Lees AJ, Kempster PA, Stern GM. Subcutaneous apomorphine in the treatment of Parkinson’s
disease. J Neurol. Neurosurg Psychiatry 1990;53:96–101.
• Golbe LI, Lieberman AN, Muenter MD, et al. Deprenyl in the treatment of symptom fluctuations in advanced
Parkinson’s disease. Clin Neuropharmacol 1988;11:45–55.
• Hughes AJ, Bishop S, Kleedorfer B, et al. Subcutaneous apomorphine in Parkinson’s disease: response to chronic
administration for up to five years. Mov Disord 1993;8:165–170.
• Korczyn AD, Nussbaum M. Emerging therapies in the pharmacological treatment of Parkinson’s disease. Drugs
2002;62: 775–786.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
• Leenders Kl, Poewe WH, Palmer AJ, et al. Inhibition of L- (19F)-fluorodopa uptake into human brain by amino acids demonstrated by positron emission tomography. Ann Neurol 1986;20:258–262.
• Lieberman A, Olanow CW, Sethi K, et al. A multi-center double blind placebo-controlled trial of ropinirole as an adjunct to L-dopa in the treatment of Parkinson’s disease patients with motor fluctuations. Neurology 1998;51:1057–1062.
• Luginger E, Wenning GK, Bosch S, Poewe W. Beneficial effects of amantadine on L-dopa-induced dyskinesias in Parkinson’s disease. Mov Disord 2000;15:873–878.
• Miyasaki JM, Martin W, Suchowersky O, Weiner WJ, Lang AE. Practice parameter: initiation of treatment for Parkinson’s disease: an evidence-based review. Report of the quality standards
• Mouradian MM, Juncos JL, Fabbrini G, Schlegel J, Bartko JJ, Chase TN. Wearing-off fluctuations in Parkinson’s disease: central pathophysiology mechanisms, Part II. Ann Neurol 1988; 24:372–378.
• Nutt JG, Woodward WR, Hammerstad JP, et al. The ‘on-off’ phenomenon in Parkinson’s disease: relation to levodopa absorption and transport. N. Engl J Med 1984;310:483–488.
• Olanow CW, Fahn S, Muenter M, et al. A multi-center, double- blind, placebo-controlled trial of pergolide as an adjunct to Sinemet in Parkinson’s disease. Mov Disord 1994;9:40–47.
• Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson’s disease: treatment guidelines. Neurology 2001;56(Suppl 5):S1–S86.
• Ory-Magne F1, Corvol JC, Azulay JP, Bonnet AM, Brefel-Courbon C, Damier P, Dellapina E, Destée A, Durif F, Galitzky M, Lebouvier T, Meissner W, Thalamas C, Tison F, Salis A, Sommet A, Viallet F, Vidailhet M, Rascol O; NS-Park CIC Network. Withdrawing amantadine in dyskinetic patients with Parkinson disease : the AMANDYSK trial. Neurology. 2014 Jan 28;82(4):300-7.
• Parkinson Study Group. A randomized placebo-controlled trial of rasagiline in levodopa-treated patients with Parkinson disease and motor fluctuations. The PRESTO study. Arch Neurol 2005;62:241–248.
• Pinter MM, Pogarell O, Oertel WH. Efficacy, safety, and tolerance of the non-ergoline dopamine agonist pramipexole in the treatment of advanced Parkinson’s disease: a double blind, placebo controlled, randomised, multicentre study. J Neurol Neurosurg Psychiatry 1999;66:436–441.
• Rascol O, Goetz C, Koller W, Poewe W, Sampaio C. Treatment interventions for Parkinson’s disease: an evidence-based assessment. Lancet 2002;359:1589–1598.

International Parkinson and Movement Disorder Society | 555 East Wells Street, Suite 1100, Milwaukee WI 53202-3823 USA
Tel: +1 414-276-2145 | www.movementdisorders.org | [email protected]
• Rascol O1, Brooks DJ, Melamed E, Oertel W, Poewe W, Stocchi F, Tolosa E; LARGO study group.Rasagiline as an adjunct to levodopa in patients with Parkinson's disease and motor fluctuations (LARGO, Lasting effect in Adjunct therapy with Rasagiline Given Once daily, study): a randomised, double-blind, parallel-group trial. Lancet. 2005 Mar 12-18;365(9463):947-54.
• Rinne UK, Larsen JP, Siden A, Worm-Petersen J. Entacapone enhances the response to levodopa in parkinsonian patients with motor fluctuations. Nomecomt Study Group. Neurology 1998;51:1309–1314.
• Stocchi F, Barbato L, Bramante L, Nordera G, Vacca L, Ruggieri S. Fluctuating parkinsonism: a pilot study of single afternoon dose of levodopa methyl ester. J Neurol 1996;243:377– 380.
• Stocchi F, Rascol O, Kieburtz K, Poewe W, Jankovic J, Tolosa E, Barone P, Lang AE, Olanow CW. Initiating levodopa/carbidopa therapy with and without entacapone in early Parkinson disease: the STRIDE-PD study. Ann Neurol. 2010 Jul;68(1):18-27.
• Storch A, Trenkwalder C, Oehlwein C, Winkelmann J, Polzer U, Hundemer HP, Schwarz J. High-dose treatment with pergolide in Parkinson’s disease patients with motor fluctuations and dyskinesias. Parkinsonism Relat Disord 2005;11:393–398.
• Stowe R, Ives N, Clarke CE, Deane K; van Hilten, Wheatley K, Gray R, Handley K, Furmston A. Evaluation of the efficacy and safety of adjuvant treatment to levodopa therapy in Parkinson s disease patients with motor complications. Cochrane Database Syst Rev. 2010 Jul 7;(7):CD007166. doi: 10.1002/14651858.CD007166.pub2
• subcommittee of the American academy of neurology. Neurology 2002;58:11–17.
• The Parkinson Study Group. Entacapone improves motor fluctuations in levodopa treated Parkinson’s disease patients. Ann Neurol 1997;42:747–755.
• Verhagen Metman L, Del Dotto P, et al. Amantadine as treatment for dyskinesias and motor fluctuations in Parkinson’s disease. Neurology 1998;50:1323–1326.
• Wictorin K, Widner H. Memantine and reduced time with dyskinesia in Parkinson's Disease. Acta Neurol Scand. 2016 May;133(5):355-60.
• Wong KK, Alty JE, Goy AG, Raghav S, Reutens DC, Kempster PA. A randomized, double-blind, placebo-controlled trial of levetiracetam for dyskinesia in Parkinson's disease. Mov Disord. 2011 Jul;26(8):1552-5. doi: 10.1002/mds.23687. Epub 2011 Apr 29.
• Zesiewicz TA, Sullivan KL, Maldonado JL, et al. Open-label pilot study of levetiracetam (Keppra) for the treatment of levodopa- induced dyskinesias in Parkinson’s disease. Mov Disord 2005;20:1205–1209.