PowerPoint Presentation-Motivations Inc 2014s3.amazonaws.com/Osteoporosis/Osteporosis there is...
35
While waiting for webinar to begin, get a chair, preferably one with no arms for Sit-To-Stand-To-Sit Exercise OSTEOPOROSIS THERE IS SOMETHING YOU CAN DO ABOUT IT! Practical Applications for Practice THE MEEKS METHOD Sara Meeks, PT, MS, GCS that, someday in this country and, indeed, around the world, any person, no matter their age, gender, lifestyle, ethnicity, musculoskeletal condition or any other factor, can go into any environment where exercise and movement are being taught and be given a program that is Ideally, it will also be therapeutic. Although there is more awareness now than when I began teaching in 1998, there is still a lot to be done. By taking this webinar, you will help me fulfill my dream. As you learn more about movement that is you can help me take the message of safety and therapeutic intent in movement and exercise into your own life and into the lives of others.
Transcript of PowerPoint Presentation-Motivations Inc 2014s3.amazonaws.com/Osteoporosis/Osteporosis there is...
While waiting for webinar to begin,
get a chair, preferably one
with no arms for
Sit-To-Stand-To-Sit Exercise
OSTEOPOROSISTHERE
ISSOMETHINGYOU CAN DO
ABOUT IT!Practical Applications for Practice
THE MEEKS METHOD
Sara Meeks, PT, MS, GCS
that, someday in this country and, indeed, around the world, any person, no matter their age, gender, lifestyle, ethnicity,
musculoskeletal condition or any other factor, can go into any environment where exercise and movement are being taught
and be given a program that is
Ideally, it will also be therapeutic. Although there is more awareness now than when I began
teaching in 1998, there is still a lot to be done. By taking this webinar, you will help me fulfill my dream.
As you learn more about movement that is
you can help me take the message of safety and therapeutic intent in movement and exercise into your own life and into
the lives of others.
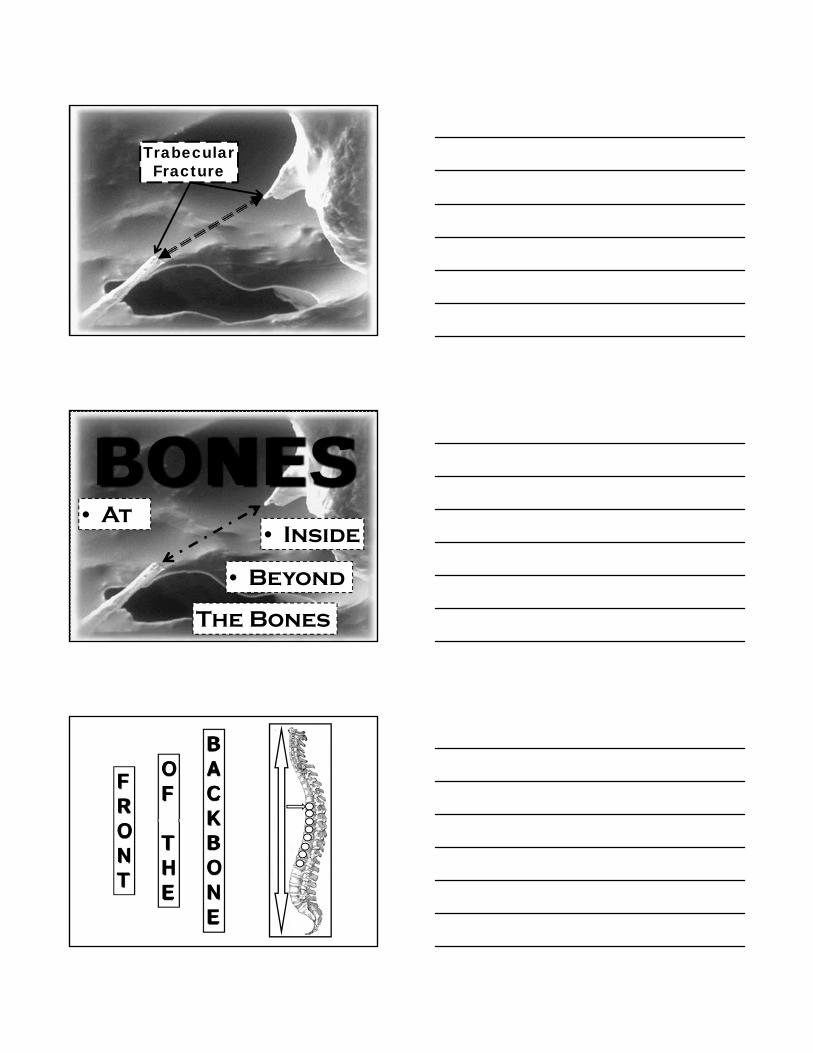
Trabecular Fracture
BONES• At
• Inside
• Beyond
The Bones
FRONT
BACKBONE
OF
THE

Spinomed Online CEU Course July 2011
INSIDETHE
BONES
6
Milner, Colin. Making Bone HealthA Priority. The Journal on Active Aging.May June 2002.
OSTEOPOROTICBONE
NORMALBONE
9
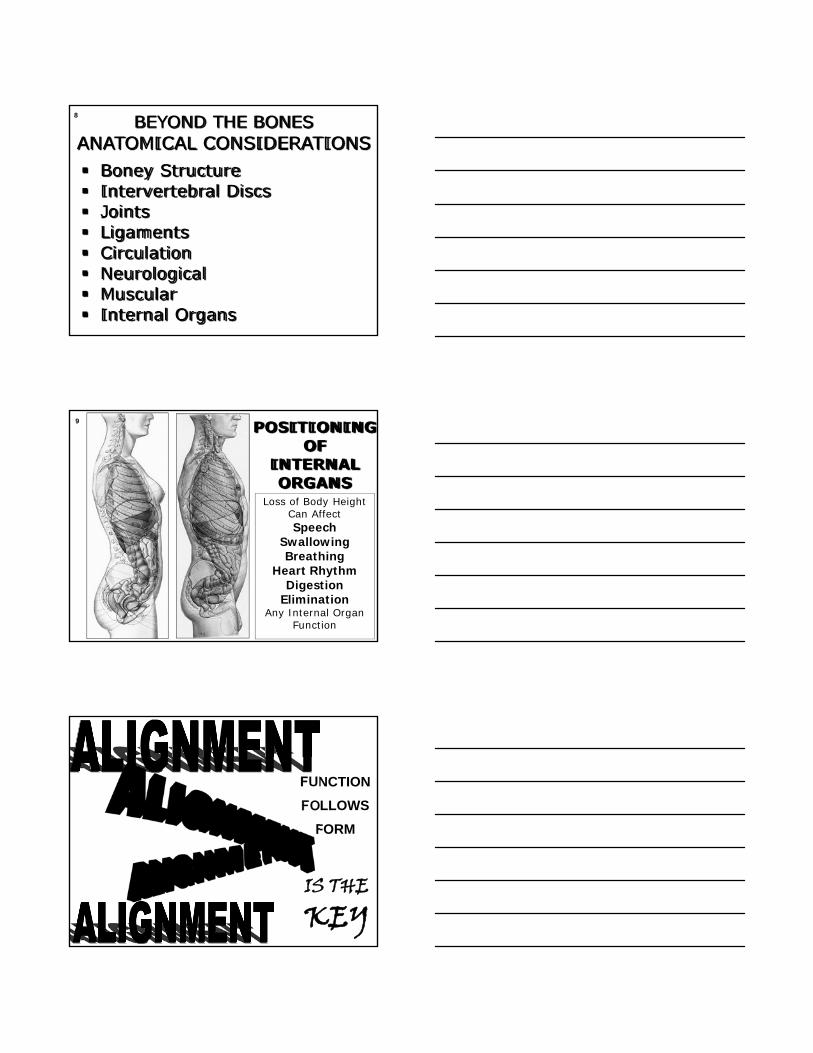
BEYOND THE BONESANATOMICAL CONSIDERATIONS Boney Structure Intervertebral Discs Joints Ligaments Circulation Neurological Muscular Internal Organs
8
POSITIONINGOF
INTERNALORGANS
9
Loss of Body Height Can AffectSpeech
SwallowingBreathing
Heart RhythmDigestion
EliminationAny Internal Organ
Function
FUNCTION
FOLLOWS
FORM
IS THEKEY
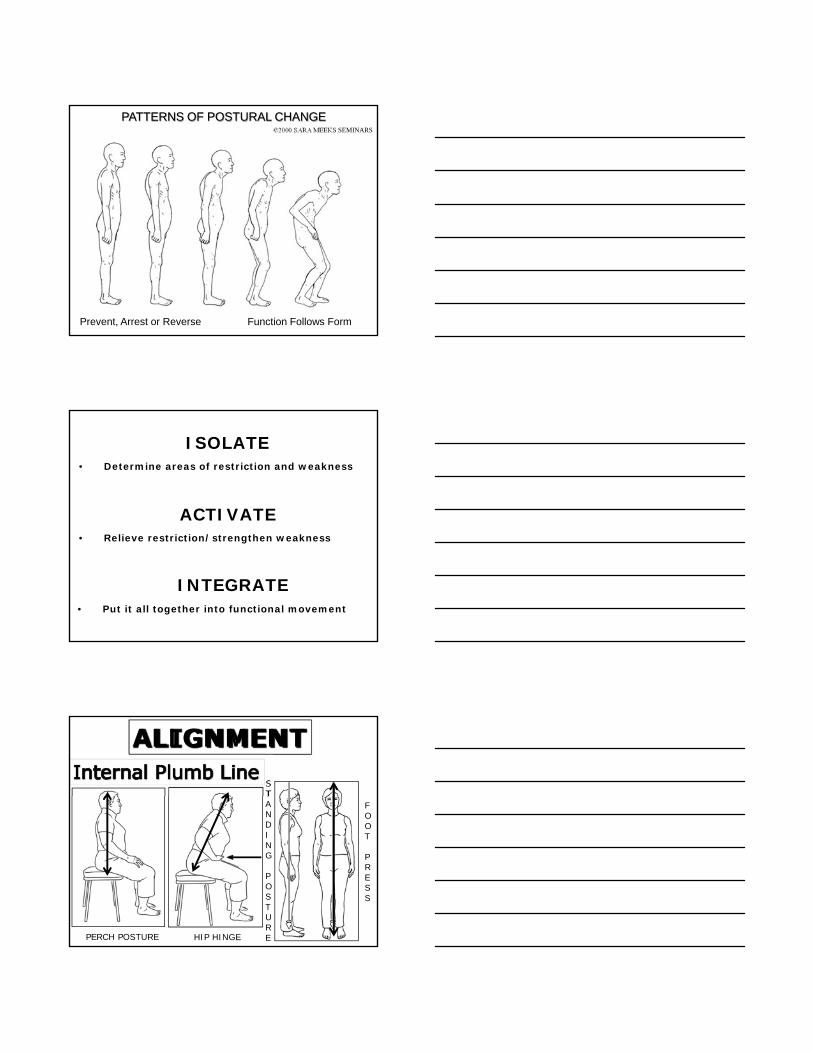
©2000 SARA MEEKS SEMINARS
PATTERNS OF POSTURAL CHANGE
Prevent, Arrest or Reverse Function Follows Form
• Determine areas of restriction and weakness
ISOLATE
ACTIVATE
INTEGRATE
• Relieve restriction/strengthen weakness
• Put it all together into functional movement
ALIGNMENT
PERCH POSTURE HIP HINGE
STANDING
POSTURE
FOOT
PRESS
SIT-TO-STAND-TO-SITFUNCTIONAL MOVEMENT
Inability to stand up out of a chair unaided is linked to a 2 fold increase in hip fracture risk Cummings et al 1995
Weakness of lower extremities linked to impending physical frailty Judge et al 1996 Guralnik et al 1995
Low femoral neck bone mineral density is significantly associated with a low sit-to-stand performance assessed by measurement of maximum rising strength in healthy adult women. Blain et al 2008
SIT-TO-STAND CHAIR
Use Lift of a Lift-Recliner Chair in Home Care
Indicated for patients who need assist with Sit-To-Stand-To-Sit movement
www.endorphin.net
17
A musculoskeletal disorder with compromised bone strength
that predisposes an individual to increased fracture risk
(broken bone)
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy.
JAMA 2001: 285:785-795
DEFINITION
•Bone Density•Bone Quality
•Architecture•Mineralization•Micro damage accumulation
BONE STRENGTH
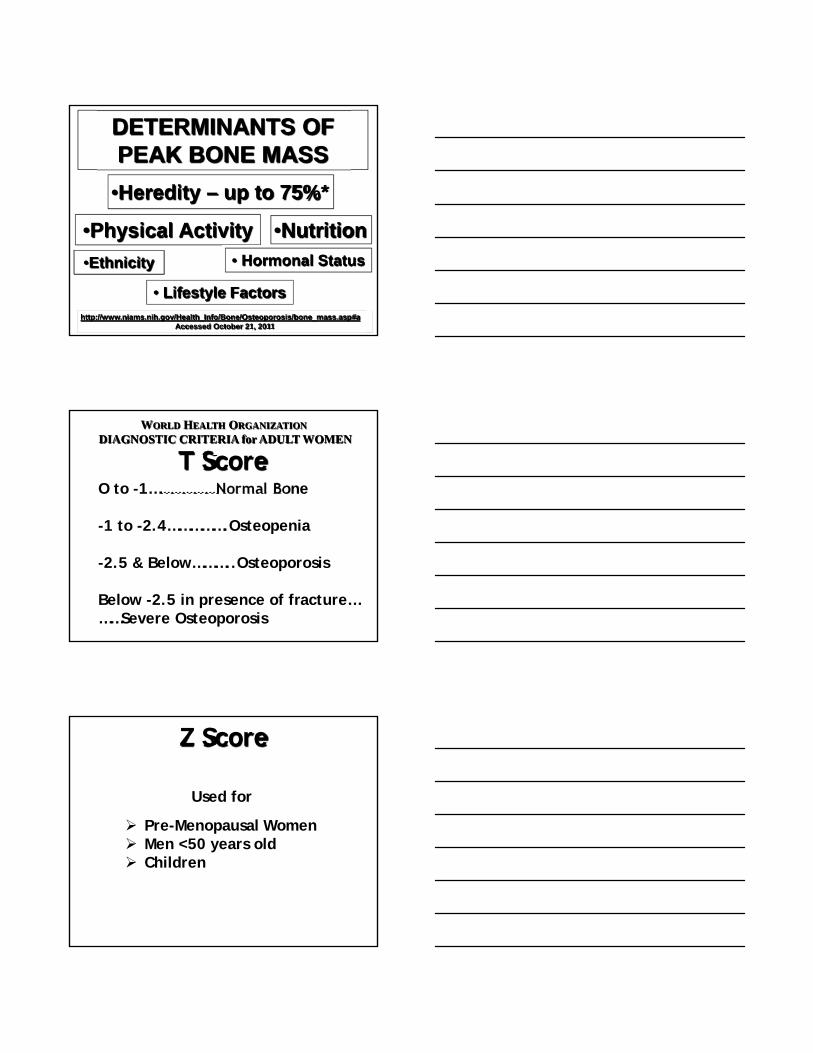
PEAK BONE MASS•The amount of bone accumulated as a young adult (generally age 30-35)
•About 90-98% is accumulated by age 18-20
Reduction of bone mass, both quantity AND quality
so that the bones become fragile and easily fracture
Bone Health and OsteoporosisA Report of the Surgeon General October 2004
DETERMINANTS OFPEAK BONE MASS
•Heredity – up to 75%*
•Physical Activity •Nutrition
•Ethnicity • Hormonal Status
• Lifestyle Factors
http://www.niams.nih.gov/Health_Info/Bone/Osteoporosis/bone_mass.asp#aAccessed October 21, 2011
O to -1………………Normal Bone
-1 to -2.4…………….Osteopenia
-2.5 & Below………..Osteoporosis
Below -2.5 in presence of fracture………Severe Osteoporosis
T Score
WORLD HEALTH ORGANIZATION
DIAGNOSTIC CRITERIA for ADULT WOMEN
Used for
Pre-Menopausal Women Men <50 years old Children
Z Score
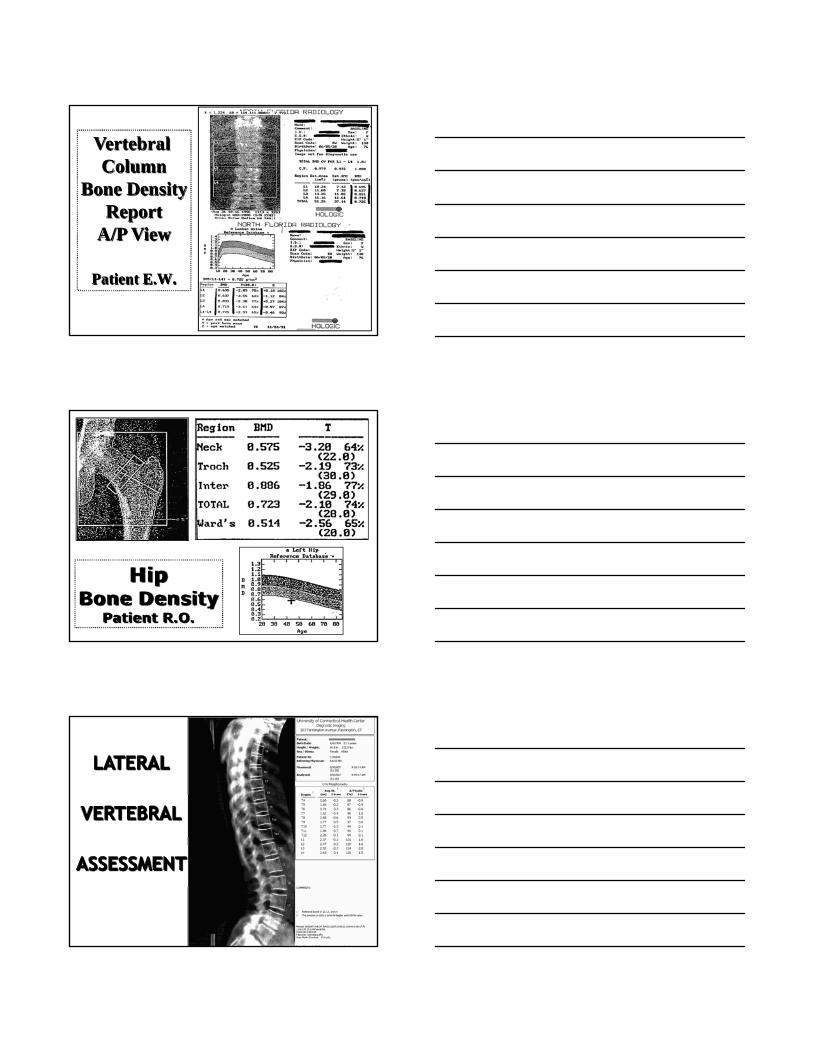
Vertebral Column
Bone DensityReport
A/P View
Patient E.W.
HipBone Density
Patient R.O.
OSTEOPOROSISIS A
PEDIATRICCONDITION
that manifests in
ADULTHOOD
• Also in childhood--babies are being born with osteoporosis• Osteoporosis affects all populations—women, men, young
adults, the elderly, patients in your clinics and classes, and anyone here in this room today
• It knows NO boundaries regarding age, gender, lifestyle, ethnicity or any other factor
• Some people are more at risk than others but no-one is totally immune
• Osteoporosis affects 60% of persons age 60+ (men and women)
• Total of 57 million age 60 + should be very concerned about their bone health
• Total # of people estimated to have low bone mass in the United States—48 million
• Osteoporosis is more prevalent than coronary heart disease (12.5 million), heart attack (1.1 million) & diabetes (17 million)
• It is more common than breast, uterine and ovarian cancer combined
PEAK BONE GROWTH
•In Utero •Adolescence
WHEN DOES
PREVENTIONBEGIN ?
BEFORE BIRTH?Evidence that fracture risk might be programmed during intrauterine life
Maternal smoking, diet (esp. Vit D deficiency) and physical activity appear to modulate bone
mineral acquisition during intrauterine lifeLow birth weight & poor childhood growth are directly
linked to later risk of hip fracture
Optimization of maternal nutrition and intrauterine growth should also be included within preventive
strategies against osteoporotic fracture
Cooper C et al. Review: developmental origins of osteoporotic fracture Osteoporosis International 2006
QUESTIONS?
?
?
??
?
?
??
?
?
?
??
?
?
?
?
?
?
? ?
?
?
?
?
?
?
?
? ?
???
??
?
?
??
?
?
?
?
?
?
?
??
?
??
??
?
?
?
??
?
?
?
?
??
?
?
??
?
??
???
? ?
??
??? ?
??
? ?
????
??
???
?
???
IN UTERO
o One of the peak times of bone growth
o Targeting healthy women to have healthy babies
o Human beings are designed to move right
from conception
o Fetal movement during pregnancy
o Skeleton formed by 7 weeks
STAGES OF BONE DEVELOPMENT
INFANCY
o Continuing with bone growth
o We are born to move
o Normal development – roll over, prone positioning,lifting head and upper body, crawling – hands/knees,walking etc.
o Prone to play/Back to sleep
STAGES OF BONE DEVELOPMENT
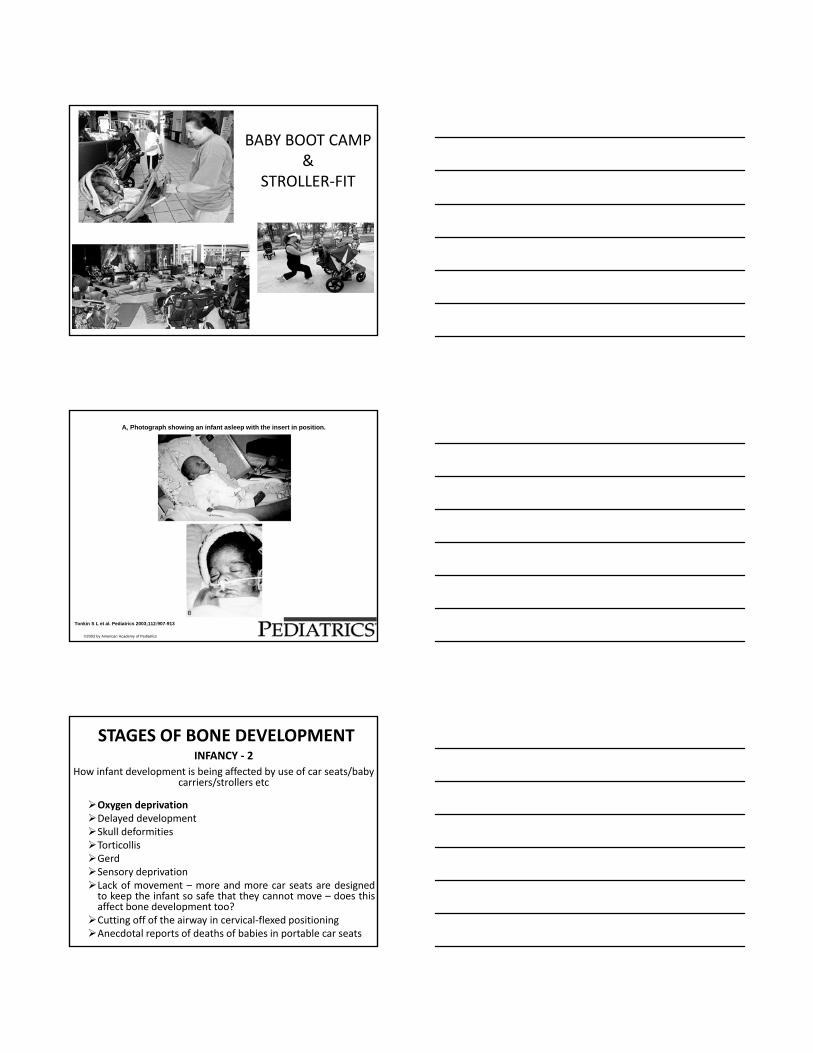
BABY BOOT CAMP&
STROLLER‐FIT
A, Photograph showing an infant asleep with the insert in position.
Tonkin S L et al. Pediatrics 2003;112:907-913
©2003 by American Academy of Pediatrics
INFANCY ‐ 2
How infant development is being affected by use of car seats/baby carriers/strollers etc
Oxygen deprivationDelayed developmentSkull deformitiesTorticollisGerdSensory deprivationLack of movement – more and more car seats are designedto keep the infant so safe that they cannot move – does thisaffect bone development too?Cutting off of the airway in cervical‐flexed positioningAnecdotal reports of deaths of babies in portable car seats
STAGES OF BONE DEVELOPMENT
CAR BED
RISK FACTORSfor
OSTEOPOROSIS
NON-MODIFIABLE RISK FACTORS
Female
Family History
Post-Menopausal – Natural or Surgical
Advanced Age
Caucasian or Asian
Delayed Puberty/Irregular Menstrual Cycles
Early Menopause
Men over age 75
Nulliparous-having had no children
Small Boned
MODIFIABLE RISK FACTORS
Smoking
High Alcohol Intake
Caffeine (more than 2-5 cups/day)
Sedentary Lifestyle/Over-Exerciser
Men-Low Testosterone
High Protein Diet (Meat)
Low Calcium Diet
Eating Disorders
AIDS/HIVAnkylosing spondylitisBlood and bone marrow disordersBreast cancerChronic obstructive pulmonary disease (COPD), including emphysemaCushing’s syndromeDepressionDiabetes Eating disorders, especially anorexia nervosaFemale athlete triad (includes loss of menstrual periods, an eating disorder and excessive exercise)GastrectomyGastrointestinal bypass proceduresHyperparathyroidismHyperthyroidismInflammatory bowel disease, including Crohn’s disease and ulcerative colitisKidney disease that is chronic and long lasting
DISEASES AND CONDITIONS
Liver disease that is severe, including biliary cirrhosisLupusLymphoma and leukemiaMalabsorption syndromes, including celiac diseaseMultiple myelomaMultiple sclerosisOrgan transplantsParkinson’s diseasePolio and post-polio syndromePoor diet, including malnutritionPremature menopauseProstate cancerRheumatoid arthritisScoliosisSpinal cord injuriesStroke ThalassemiaThyrotoxicosisWeight loss
NOTEThis list may not include all diseases and conditions that may
cause bone loss.
Aluminum-containing antacidsAntiseizure medicines (only some) such as Dilantin® or PhenobarbitalAromatase inhibitors such as Arimidex®, Aromasin® and Femara®Cancer chemotherapeutic drugsCyclosporine A and FK506 (Tacrolimus)Gonadotropin releasing hormone (GnRH) such as Lupron® and Zoladex®HeparinLithiumMedroxyprogesterone acetate for contraception (Depo-Provera®)
MEDICATIONS
Methotrexate
Proton pump inhibitors (PPIs) such as Nexium®, Prevacid® and Prilosec®
Selective serotonin reuptake inhibitors (SSRIs) such as Lexapro®, Prozac® and Zoloft®
Steroids (glucocorticoids) such as cortisone and prednisone
Tamoxifen® (premenopausal use)
Anti-rejection drugs in organ-transplant patients
Thiazolidinediones such as Actos® and Avandia®
Thyroid hormones in excess
NOTEThis list may not include all medicines that may cause bone loss.
FIRST SIGNS
• Fracture- minimal trauma(e.g., Colles Fracture, Compression Fracture, Rib Fracture. Any fall from standing body height is a fracture of minimal trauma)
• Hyper-Kyphosis • Loss of body height• Transparent skin• Periodontal disease• Back Pain• Protruding Abdomen
RISK FOR FRACTURE
History of Previous Fracture – Fracture Predicts Fracture
Vision Problems
Deconditioning/Hypokinesis
Balance Problems
Tall Slim Build
Hip Fracture Immediate Family-especially of the mother
Inability to get out of a chair unaided
Being on one’s feet less than 4 hours per day
• Occurs in 1 of 2 women; 1 of 4 men• Happens every 20 seconds• Can be immediately life-altering and life-
threatening• Annual Fracture Incidence
– Vertebral—700,000– Hip—300,000– Wrist—250,000– Other Sites—300,000
• Cost – >$46 million per day– By 2020– >$178 million per day
OSTEOPOROSIS-RELATED FRACTURE
More fragility fractures occur in women with normal bone or osteopenia than in
those with osteoporosisTherefore, when prescribing exercise,
it is important to consider bonehealth in all populations
Pasco JA, Seeman E, Henry MJ, et al. The population burden of fractures originates in women with osteopenia, not osteoporosis. Osteoporos Int (2006)17:1404Sornay-Rendu E, Munoz F, Garnero P, Duboeuf F, Delmas PD.. Identification of osteopenic women at high risk of fracture: the OFELY study. J Bone Miner Res. 2005 Oct;20(10):1813-9. Epub 2005 Jun 20.E. Siris & P. D. Delmas. Assessment of 10-year absolute fracture risk: a new paradigm with worldwide application. Osteoporosis International (2008);19:383-384
•Bones of spine usually first to show signs of osteoporosis•Primarily trabecular bone•Fractures occur during movement that includes
TRUNK FLEXION
VERTEBRAL BODY
•After one vertebral fracture, the risk for having a 2nd vertebral fracture increases 5 fold!•1 woman in 5 will sustain a 2nd vertebral fracture within 1 year•“The risk of death is 2.7 times higher than those with no fracture”1
•Only 20-30% of all compression fractures are symptomatic2
1 Too Fit To Fracture: Exercise recommendations for individuals with osteoporosis of osteoporotic vertebral fracture 2014
International Osteoporosis Foundation 2005Report of the Surgeon General on Bone Health Oct 2004
2www.nih.gov accessed November 30, 2011
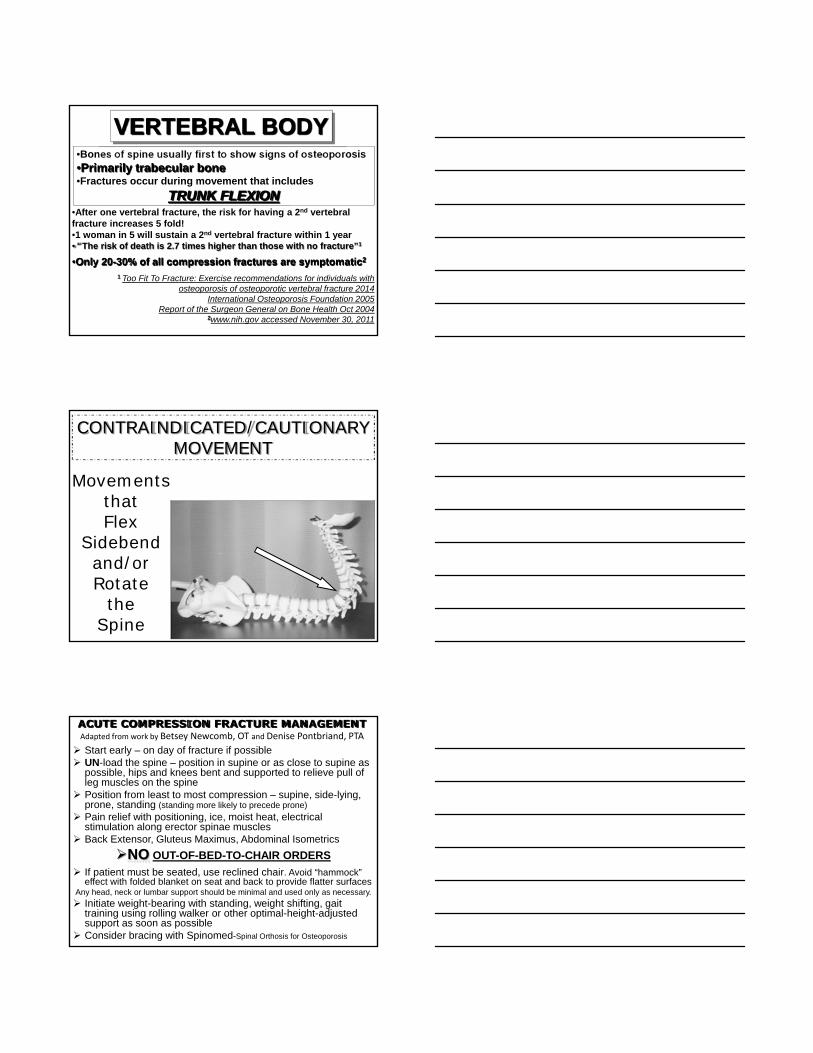
CONTRAINDICATED/CAUTIONARYMOVEMENT
Movements that Flex
Sidebend and/or Rotate
theSpine
ACUTE COMPRESSION FRACTURE MANAGEMENTAdapted from work by Betsey Newcomb, OT and Denise Pontbriand, PTA
Start early – on day of fracture if possible UN-load the spine – position in supine or as close to supine as
possible, hips and knees bent and supported to relieve pull of leg muscles on the spine
Position from least to most compression – supine, side-lying, prone, standing (standing more likely to precede prone)
Pain relief with positioning, ice, moist heat, electrical stimulation along erector spinae muscles
Back Extensor, Gluteus Maximus, Abdominal Isometrics
NO OUT-OF-BED-TO-CHAIR ORDERS
If patient must be seated, use reclined chair. Avoid “hammock” effect with folded blanket on seat and back to provide flatter surfaces
Any head, neck or lumbar support should be minimal and used only as necessary.
Initiate weight-bearing with standing, weight shifting, gait training using rolling walker or other optimal-height-adjusted support as soon as possible
Consider bracing with Spinomed-Spinal Orthosis for Osteoporosis
Initial non-weight-bearing therapy is important for preventing vertebral body collapse in elderly patients with clinical
vertebral fractures. Kishikawa Y. Int J Gen Med 2012:5 373-380.
CONVENTIONAL RELATIVE REST
• Bedrest
• Soft brace wearing
• Minimization of weight bearing to spine
INITIAL NON-WEIGHT-BEARING
• Complete bed rest (2 weeks)
• No weight bearing to spine followed by soft brace wear
• Meals and voiding in bed
• At 12 wks body union 100%
• No back pain 37%
• Mild back pain 62%
• Moderate back pain 1%
• Length of stay 49.2 days
• At 12 wks body union 97%
• No back pain 12%
• Mild back pain 75%
• Moderate back pain 13%
• Length of stay 37.9 days
55
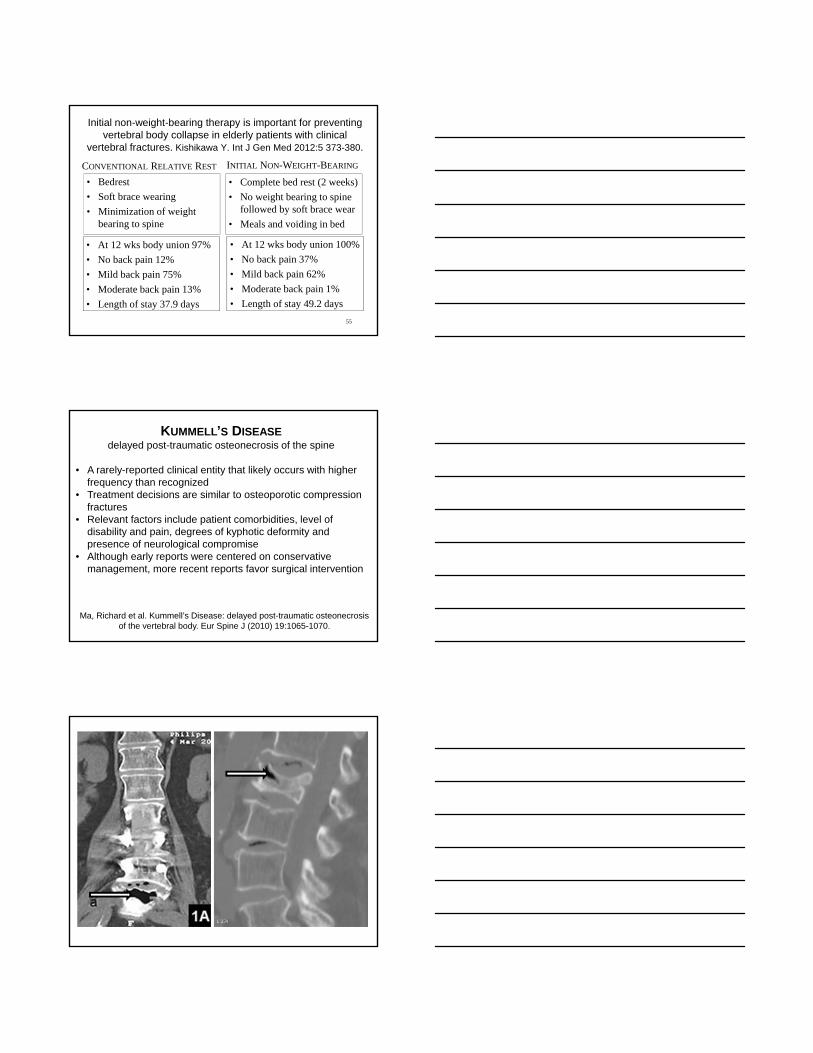
KUMMELL’S DISEASEdelayed post-traumatic osteonecrosis of the spine
• A rarely-reported clinical entity that likely occurs with higher frequency than recognized
• Treatment decisions are similar to osteoporotic compression fractures
• Relevant factors include patient comorbidities, level of disability and pain, degrees of kyphotic deformity and presence of neurological compromise
• Although early reports were centered on conservative management, more recent reports favor surgical intervention
Ma, Richard et al. Kummell’s Disease: delayed post-traumatic osteonecrosis of the vertebral body. Eur Spine J (2010) 19:1065-1070.
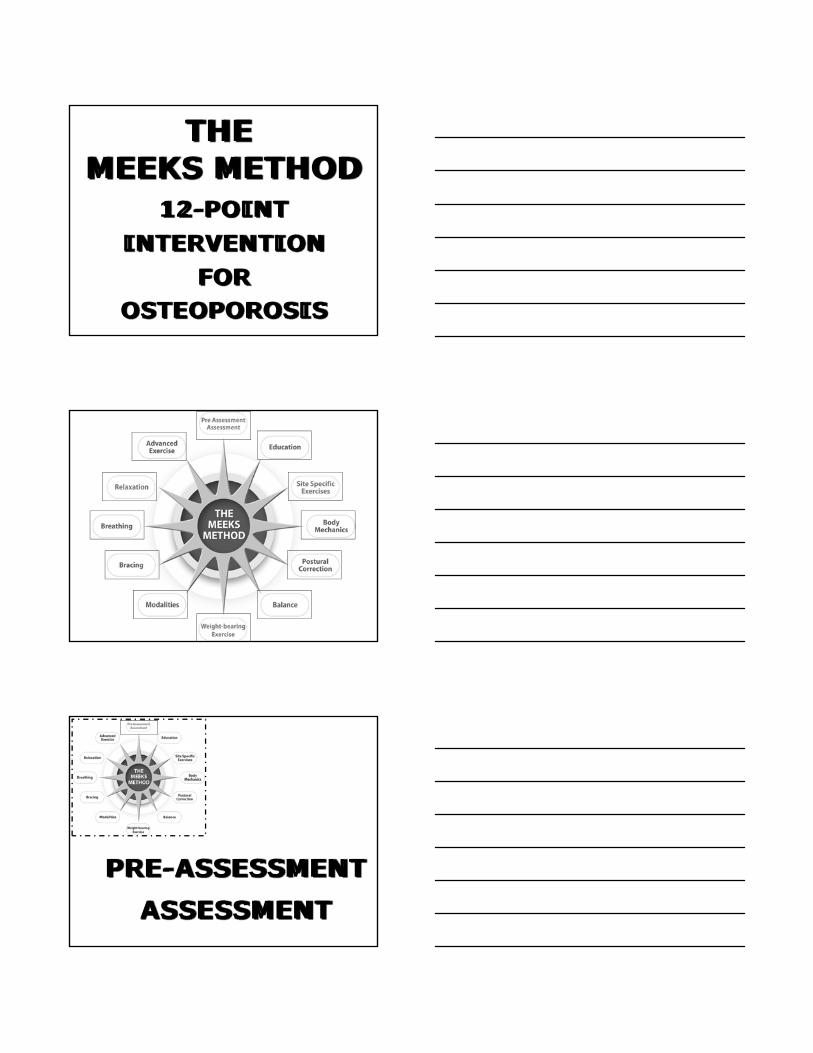
THE MEEKS METHOD
12-POINTINTERVENTION
FOROSTEOPOROSIS
PRE-ASSESSMENTASSESSMENT
EDUCATIONPatient
Advocacy****
Resources
QUESTIONS?
?
?
??
?
?
??
?
?
?
??
?
?
?
?
?
?
? ?
?
?
?
?
?
?
?
? ?
???
??
?
?
??
?
?
?
?
?
?
?
??
?
??
??
?
?
?
??
?
?
?
?
??
?
?
??
?
??
???
? ?
??
??? ?
??
? ?
????
??
???
?
???
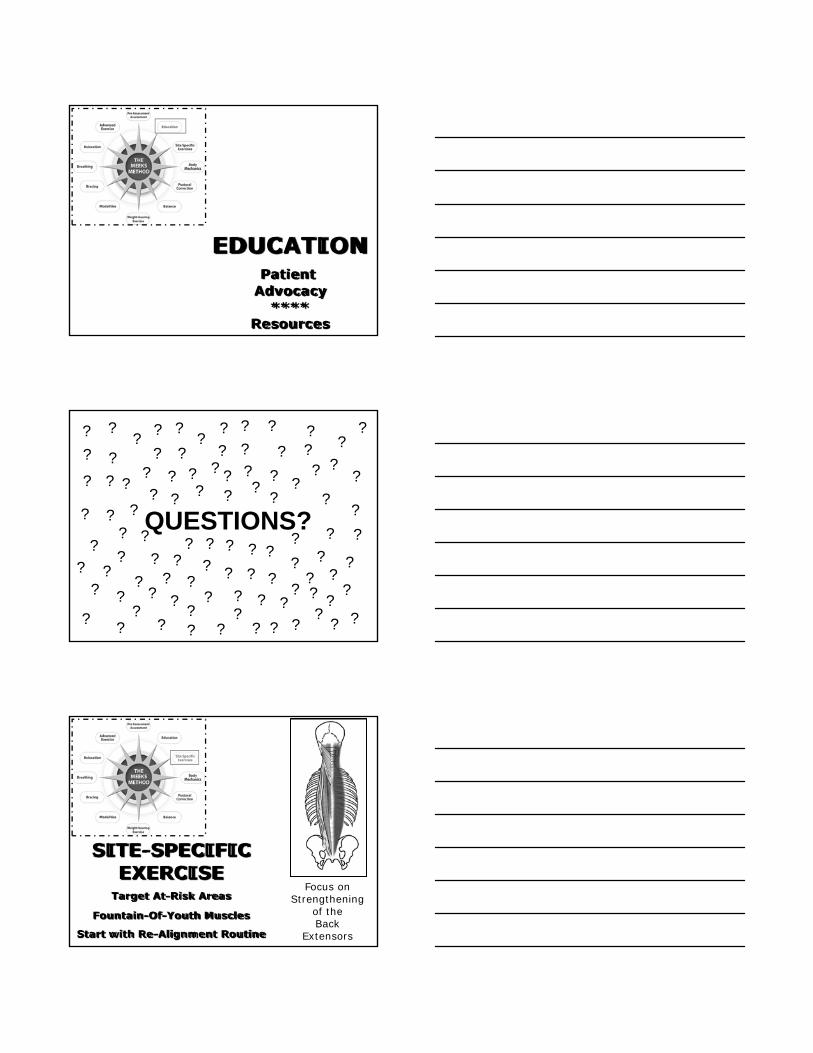
SITE-SPECIFICEXERCISE
Target At-Risk Areas
Fountain-Of-Youth Muscles
Start with Re-Alignment Routine
Focus on Strengthening
of the Back
Extensors
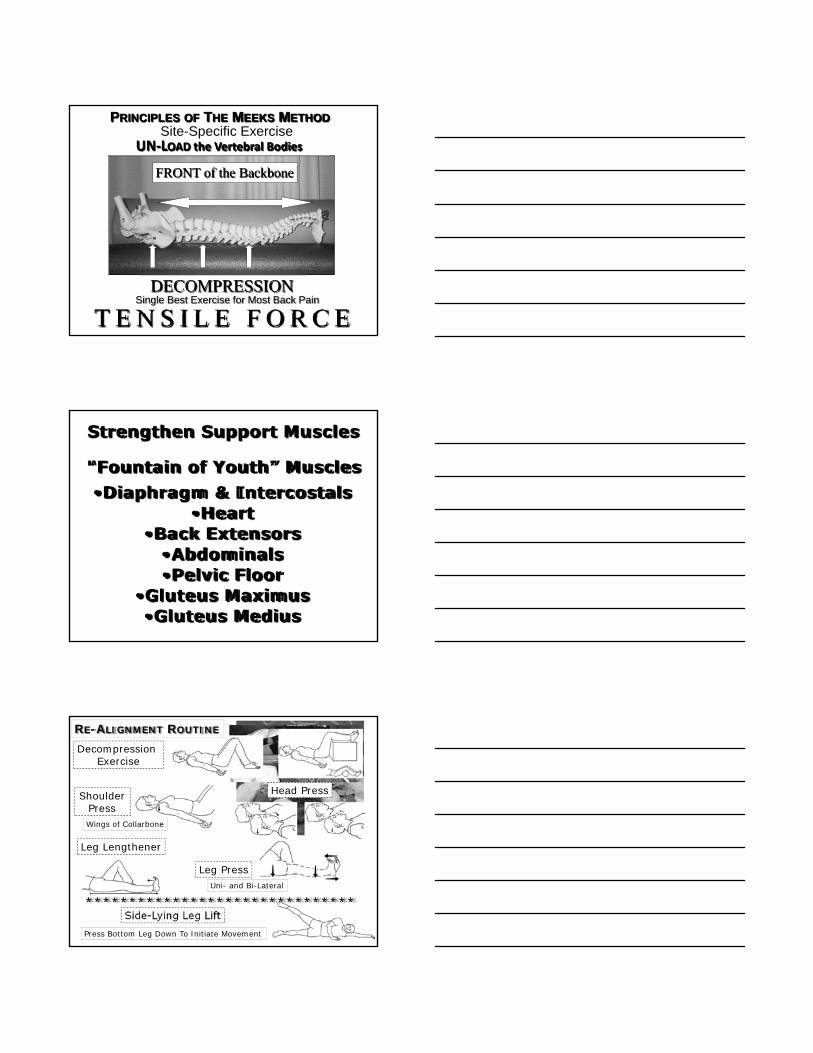
PRINCIPLES OF THE MEEKS METHOD
DECOMPRESSION
FRONT of the Backbone
T E N S I L E F O R C E Single Best Exercise for Most Back Pain
UN‐LOAD the Vertebral BodiesSite-Specific Exercise
Strengthen Support Muscles
“Fountain of Youth” Muscles•Diaphragm & Intercostals
•Heart•Back Extensors
•Abdominals•Pelvic Floor
•Gluteus Maximus •Gluteus Medius
Decompression Exercise
ShoulderPress
Head Press
Leg Lengthener
Leg Press
Side-Lying Leg Lift*******************************
RE-ALIGNMENT ROUTINE
Wings of Collarbone
Uni- and Bi-Lateral
Press Bottom Leg Down To Initiate Movement
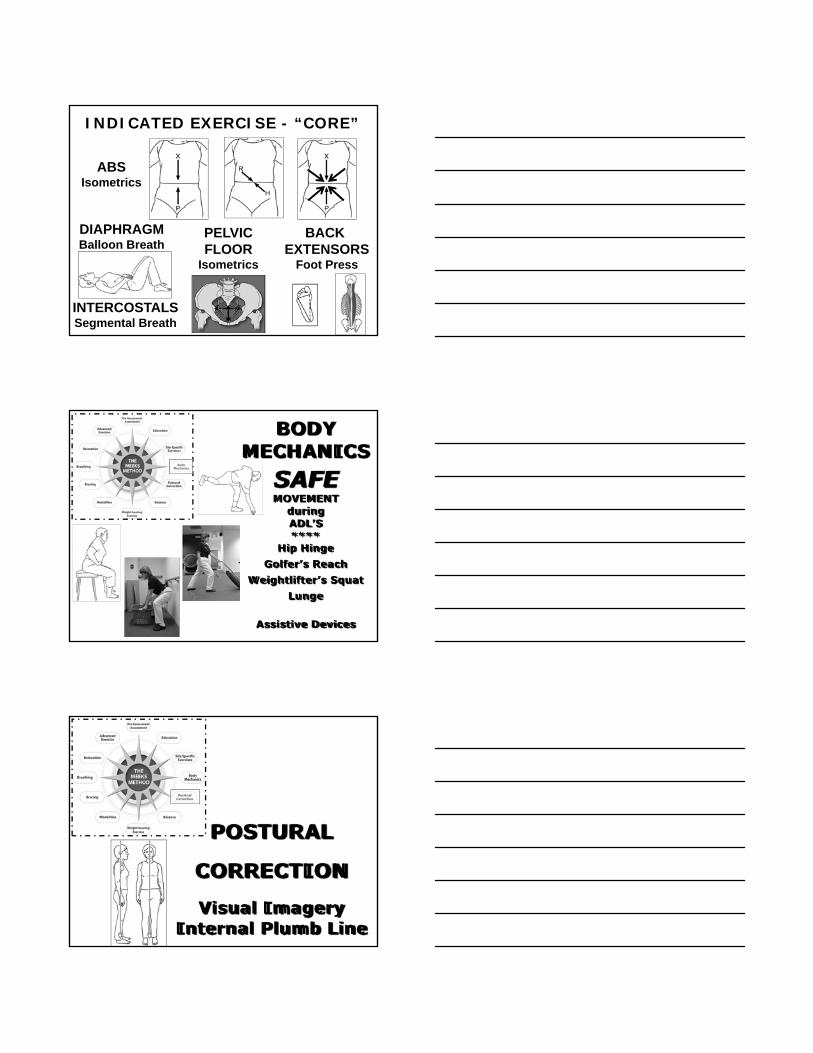
INDICATED EXERCISE - “CORE”
ABSIsometrics
PELVICFLOOR
Isometrics
DIAPHRAGMBalloon Breath
BACK EXTENSORS
Foot Press
INTERCOSTALSSegmental Breath
BODY MECHANICS
SAFEMOVEMENT
during ADL’S****
Hip HingeGolfer’s Reach
Weightlifter’s SquatLunge
Assistive Devices
POSTURAL
CORRECTION
Visual ImageryInternal Plumb Line
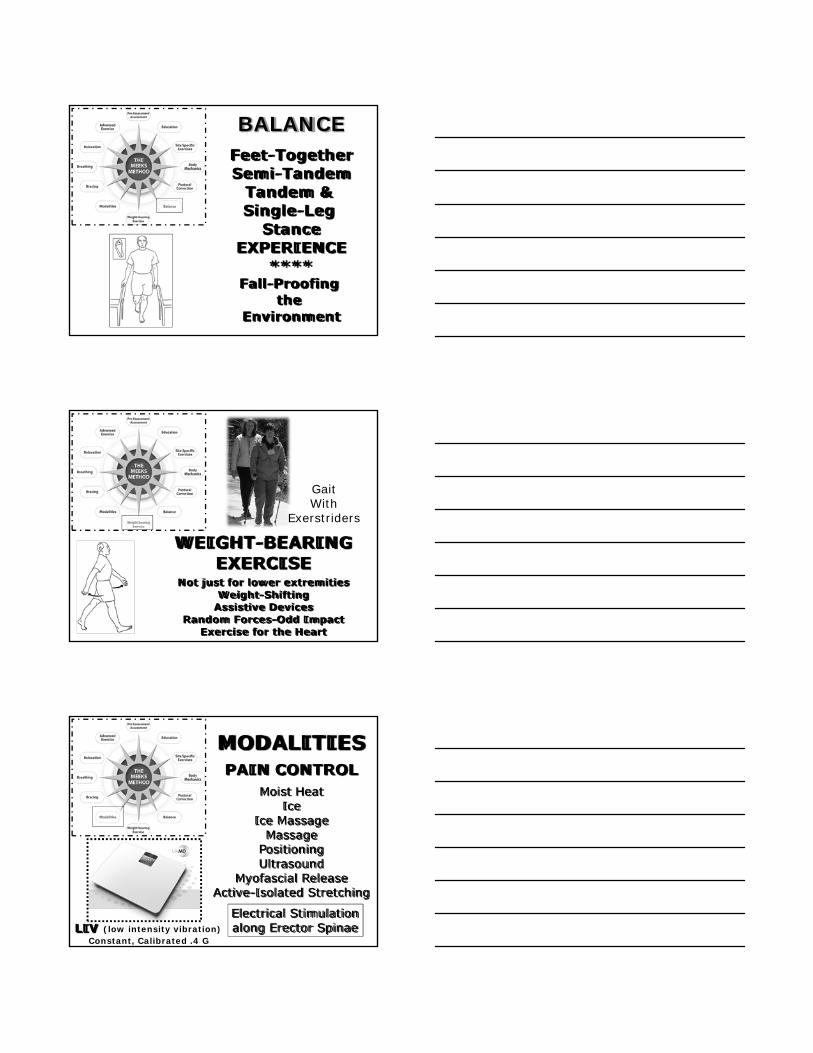
BALANCEFeet-TogetherSemi-Tandem
Tandem & Single-Leg
StanceEXPERIENCE
****Fall-Proofing
the Environment
WEIGHT-BEARINGEXERCISE
Not just for lower extremitiesWeight-Shifting
Assistive DevicesRandom Forces-Odd Impact
Exercise for the Heart
GaitWith
Exerstriders
MODALITIESPAIN CONTROL
Moist HeatIce
Ice MassageMassage
PositioningUltrasound
Myofascial ReleaseActive-Isolated Stretching
LIV (low intensity vibration)Constant, Calibrated .4 G
Electrical Stimulationalong Erector Spinae
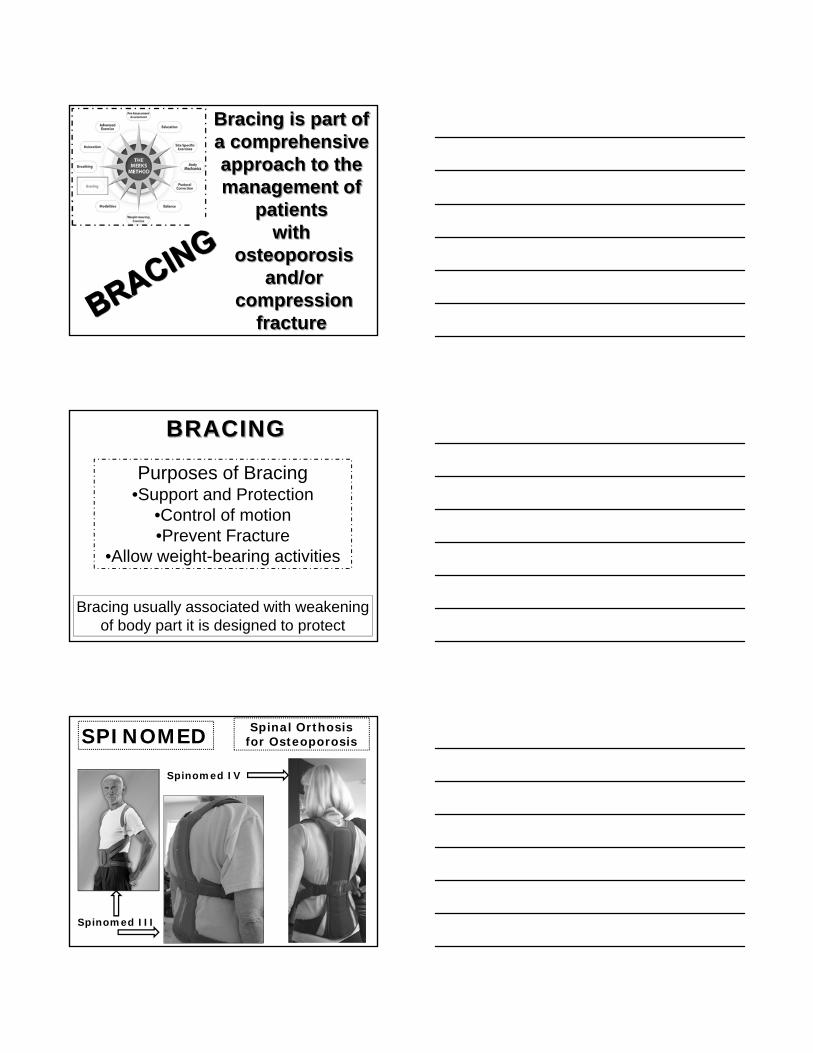
Bracing is part of a comprehensive approach to the management of
patients with
osteoporosisand/or
compressionfracture
BRACING
Purposes of Bracing•Support and Protection
•Control of motion•Prevent Fracture
•Allow weight-bearing activities
Bracing usually associated with weakeningof body part it is designed to protect
SPINOMED Spinal Orthosis for Osteoporosis
Spinomed III
Spinomed IV
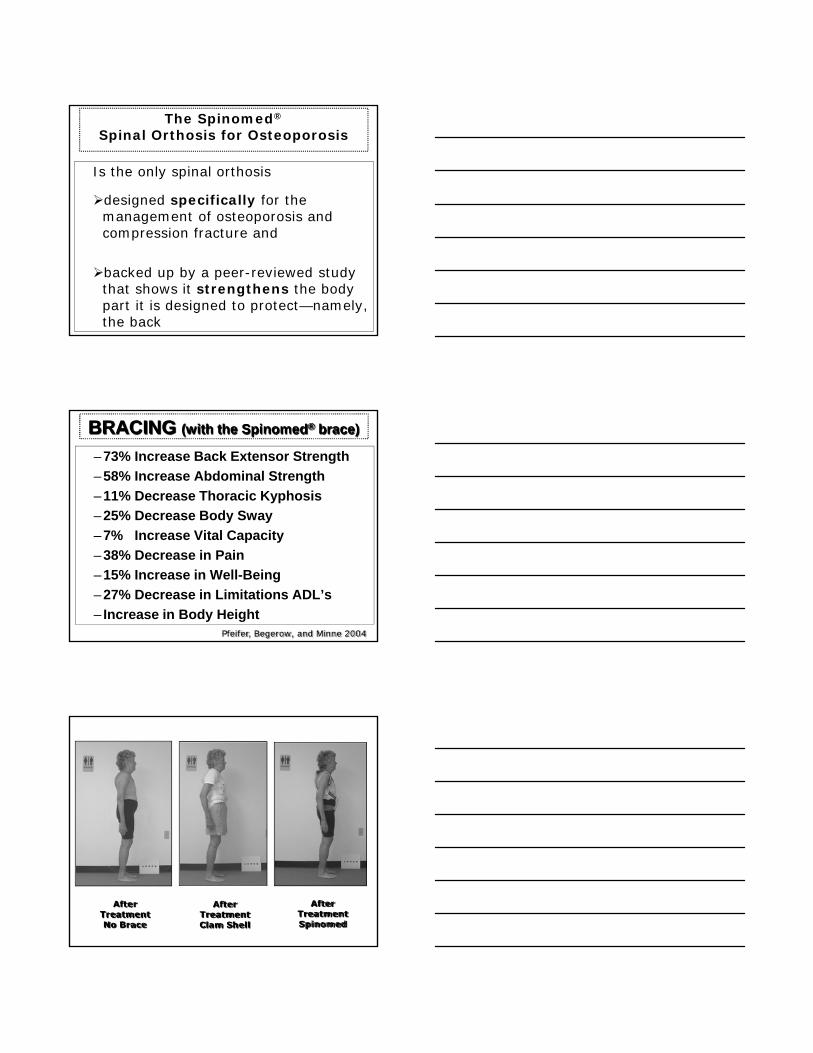
The Spinomed®
Spinal Orthosis for Osteoporosis
Is the only spinal orthosis
designed specifically for the management of osteoporosis and compression fracture and
backed up by a peer-reviewed study that shows it strengthens the body part it is designed to protect—namely, the back
BRACING (with the Spinomed® brace)
– 73% Increase Back Extensor Strength
– 58% Increase Abdominal Strength
– 11% Decrease Thoracic Kyphosis
– 25% Decrease Body Sway
– 7% Increase Vital Capacity
– 38% Decrease in Pain
– 15% Increase in Well-Being
– 27% Decrease in Limitations ADL’s
– Increase in Body HeightPfeifer, Begerow, and Minne 2004
After TreatmentNo Brace
After TreatmentClam Shell
After TreatmentSpinomed
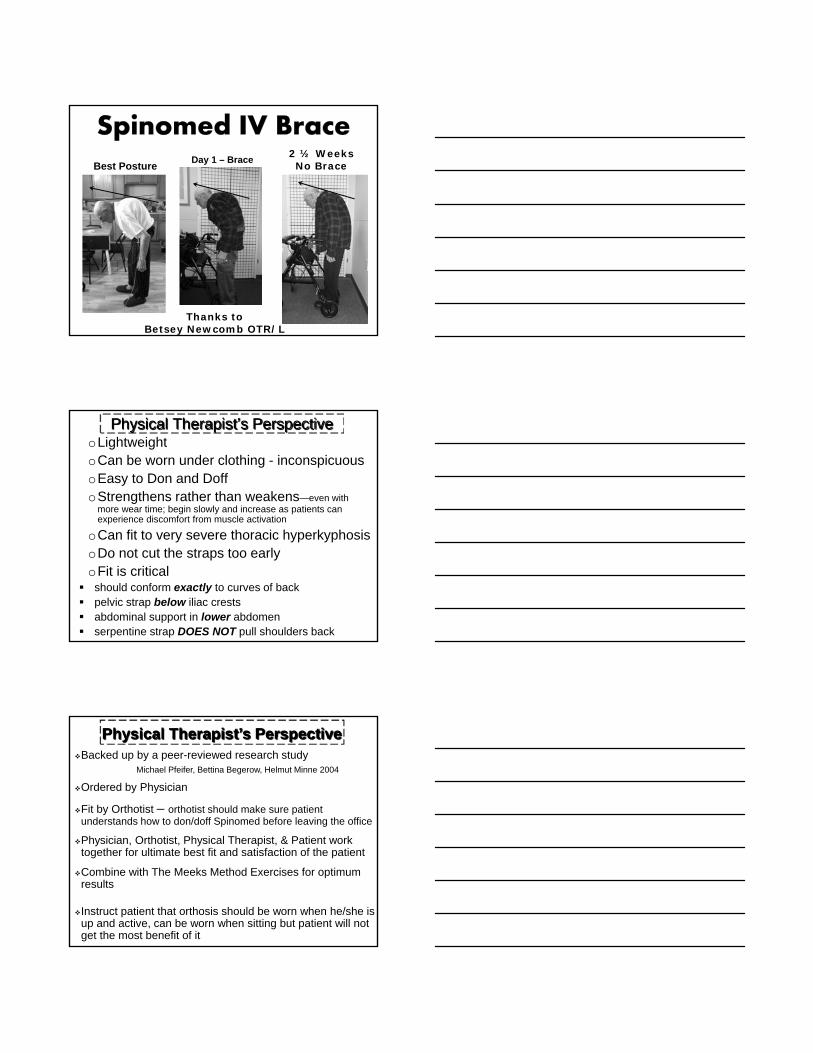
Best PostureDay 1 – Brace
2 ½ Weeks No Brace
Thanks to Betsey Newcomb OTR/L
Physical Therapist’s PerspectiveoLightweightoCan be worn under clothing - inconspicuousoEasy to Don and DoffoStrengthens rather than weakens—even with
more wear time; begin slowly and increase as patients can experience discomfort from muscle activation
oCan fit to very severe thoracic hyperkyphosisoDo not cut the straps too earlyoFit is critical should conform exactly to curves of back pelvic strap below iliac crests abdominal support in lower abdomen serpentine strap DOES NOT pull shoulders back
Physical Therapist’s PerspectiveBacked up by a peer-reviewed research study
Michael Pfeifer, Bettina Begerow, Helmut Minne 2004
Ordered by Physician
Fit by Orthotist – orthotist should make sure patient understands how to don/doff Spinomed before leaving the office
Physician, Orthotist, Physical Therapist, & Patient work together for ultimate best fit and satisfaction of the patient
Combine with The Meeks Method Exercises for optimum results
Instruct patient that orthosis should be worn when he/she is up and active, can be worn when sitting but patient will not get the most benefit of it
BRACING WITH THE SPINOMEDSpinal Orthosis for Osteoporosis
“The Spinomed orthosis is the single, most significant advancement in the conservative
management of osteoporosis and compression fracture EVER.”
Sara M. Meeks, PT, MS, GCS
Use of the Spinomed is part of thecomprehensive approach of
The Meeks MethodGoal of Management is to Minimize
the Risk of the Next Fracture
QUESTIONS?
?
?
??
?
?
??
?
?
?
??
?
?
?
?
?
?
? ?
?
?
?
?
?
?
?
? ?
???
??
?
?
??
?
?
?
?
?
?
?
??
?
??
??
?
?
?
??
?
?
?
?
??
?
?
??
?
??
???
? ?
??
??? ?
??
? ?
????
??
???
?
???
BREATHINGAwareness
DiaphragmaticSegmental
Targeted AreasUmbrella

RELAXATIONConscious “Time-Out”
Contract-RelaxDoing “Fun” Things
Breathing
ADVANCED EXERCISE
Seated ClassesFitness CenterYoga -- Pilates
&More
Yoga Bone Campwith Sara Meeks, PT, MS, GCS, KYT
SAFE Pilates for Skeletal Healthwith Sherri Betz, PT, GCS
“Non-Compliant”Patients
STAGES OF GRIEFDENIAL
"No way - can't be!" “They’ve got my report mixed up with someone else’s”ANGER
"Darn! I am so angry: I did everything right and I get OSTEOPOROSIS anyway?!??!!!“
NEGOTIATING/BARGAINING"So ... it's not so bad (osteopenia, borderline) .. and, if I elongate
A LOT, I can still do those forward bends, side bends and twists right? Maybe just breathe and move more gently?“
DEPRESSION"I am so down about this ... I have this condition for the rest of my life. I
just won't move at all cause I could break a bone“ACCEPTANCE
"Ok, I have osteoporosis. Sucks. But I'm going to find a way to do yoga and exercise because I love it ...
Just have to find a way to do it safely"
o Health care workers may benefit from an individual approach
o Face-to-Face delivery more effective o Take time to explain benefits of physical activityo Give clear & personalized adviceo Message from providers should be more consistento Educate older patients that it takes time to adapt to
new physical activity (I usually say “give it 6-8 wks”)o Involve relatives, friends and important peerso Check regularly to see that older patients
understand what you are asking them to doBaeert V et al. Motivators and barriers for physical activity in older adults with osteoporosis. J Ger Phys Ther. Vol 38. Number 3. July –Sept 2015. PP105-114.
o Personalize your approach – consider clinical condition of the patient
o LISTEN to your patiento Engage your patient as a partner in their therapyo Give your patient something they CAN do and which
will make a difference right away and they will be more likely TO do it
o Keep instructions simple & modified for each patiento Err on the side of cautiono When in doubt, don’t
In the end—minimizing risk of injury is the “bottom line”
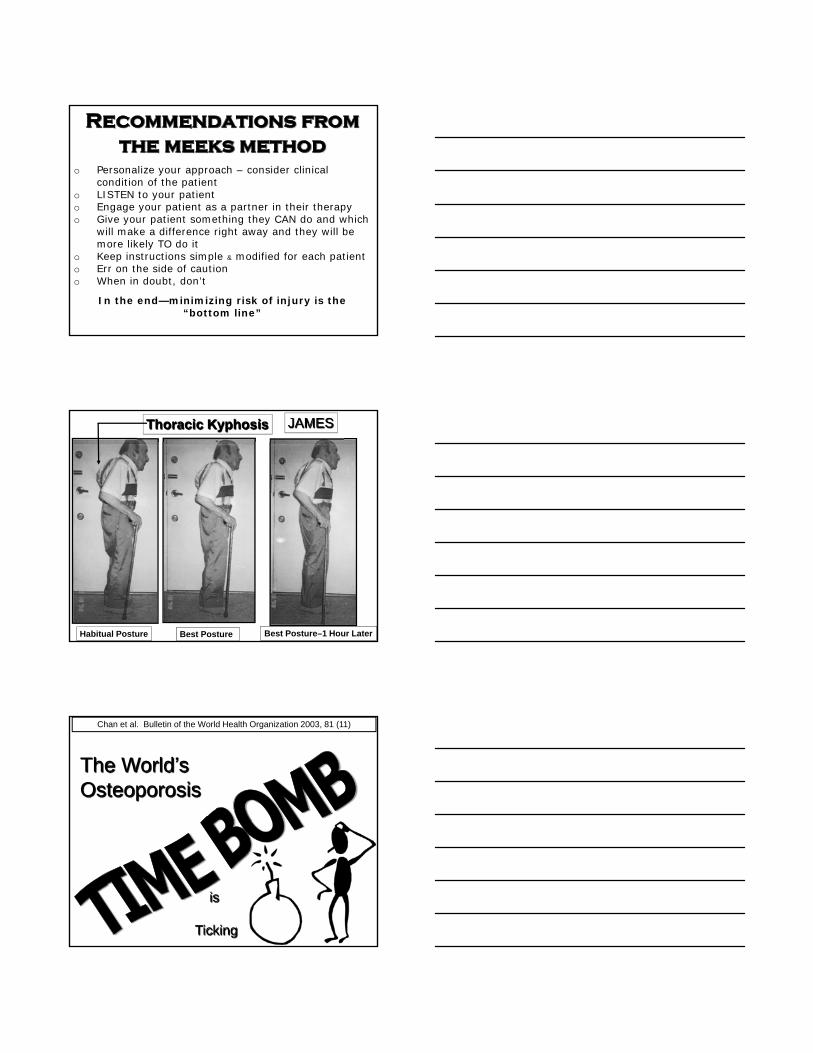
Habitual Posture Best Posture Best Posture–1 Hour Later
JAMESThoracic Kyphosis
The World’s Osteoporosis
is
Ticking
Chan et al. Bulletin of the World Health Organization 2003, 81 (11)

!! TAKE ACTION NOW !!
Best way to diffuse the world’s
OSTEOPOROSIS TIME BOMB
is to
THINK
BONEWHEN YOUR PATIENT
FIRST COMES THROUGHTHE DOOR
“BOTTOM LINE”
MINIMIZE
THE RISK OF THE
NEXT FRACTURE
WHATIS
YOURNEXTSTEP?
Rosie
Mikki
Raven
For information on the [email protected]
Sit‐To‐Stand Chairendorphin.net
Exerstrider Walking Poleswalkingpoles.com
LivMD Low Intensity Vibration Unitmarodyne.com
For PDF’s of
The Re-Alignment Routine Pre-Assessment Form
PowerPoint (color) Presentation Slide on Compression Fracture Management
Kishikawa study
send email to
Check website www.sarameekspt.com for more education by Sara Meeks, PT, MS, GCS
For seminars, webinars, books, DVDs
and other products designed to enhance practice
please visit www.sarameekspt.com
DISCLAIMER
Sara Meeks receives no commission on sales of any products presented or mentioned in this webinar
She recommends only products that enhance practice.

WAITING FOR ME TO FEED THEM
ARCHIE
MOSES
BOBBSEY
JUGHEAD
QUESTIONS?
?
?
??
?
?
??
?
?
?
??
?
?
?
?
?
?
? ?
?
?
?
?
?
?
?
? ?
???
??
?
?
??
?
?
?
?
?
?
?
??
?
??
??
?
?
?
??
?
?
?
?
??
?
?
??
?
??
???
? ?
??
??? ?
??
? ?
????
??
???
?
???