![ANNEX I SUMMARY OF PRODUCT …€¢ Liver function ( alanine aminotransferase [ALAT], aspartate aminotransferase [ASAT], albumin, bilirubin) ... • The short needle should be then](https://static.fdocuments.net/doc/165x107/5d3edcab88c993715a8c0898/annex-i-summary-of-product-liver-function-alanine-aminotransferase-alat.jpg)
PowerPoint Presentation€¦ · –Lille score: Dynamic model. Assess response to steroids at day...
29
4/12/2017 1 Alcoholism and Liver Disease Christopher Chang, MD, PhD Division of Gastroenterology/Hepatology University of New Mexico School of Medicine And New Mexico VA Health Care System April 21, 2017 National Conference for Nurse Practitioners Nashville, TN Overview • Burden of alcoholism and alcoholic liver disease • Natural history of ALD and pathogenesis • Alcoholic hepatitis (AH) – Clinical features and diagnosis – Assessing severity and prognosis – Treatment: what does the evidence show? – Ineffective and pipeline therapies – Summary and approach to the AH patient • Major complications of cirrhosis and portal hypertension: Cliff Notes version – Variceal bleeding – Ascites and SBP – Hepatorenal syndrome – Hepatic encephalopathy – Hepatopulmonary syndrome – Hepatocellular carcinoma Burden of Alcoholic Liver Disease • Nearly 6% of all deaths globally were attributable to alcohol (WHO data, 2012) • Alcoholic cirrhosis is the 8 th most common cause of all mortality in U.S. • In-hospital mortality rate of 6.8% for alcoholic hepatitis in U.S. • The “good news”: Only minority of heavy drinkers develop AH and/or cirrhosis. • The Bad News: Rising prevalence of 12-month and lifetime Alcohol Use Disorder (13.9% and 29.1%), classified in DSM-V Asrani 2010, Hepatology 52:408 Grant 2015, JAMA Psychiatry 72: 757
Transcript of PowerPoint Presentation€¦ · –Lille score: Dynamic model. Assess response to steroids at day...
4/12/2017
1
Alcoholism and Liver Disease
Christopher Chang, MD, PhDDivision of Gastroenterology/Hepatology
University of New Mexico School of Medicine
And
New Mexico VA Health Care System
April 21, 2017
National Conference for Nurse Practitioners
Nashville, TN
Overview
• Burden of alcoholism and alcoholic liver disease
• Natural history of ALD and pathogenesis
• Alcoholic hepatitis (AH)
– Clinical features and diagnosis
– Assessing severity and prognosis
– Treatment: what does the evidence show?
– Ineffective and pipeline therapies
– Summary and approach to the AH patient
• Major complications of cirrhosis and portal hypertension: Cliff
Notes version
– Variceal bleeding
– Ascites and SBP
– Hepatorenal syndrome
– Hepatic encephalopathy
– Hepatopulmonary syndrome
– Hepatocellular carcinoma
Burden of Alcoholic Liver Disease
• Nearly 6% of all deaths globally were attributable to
alcohol (WHO data, 2012)
• Alcoholic cirrhosis is the 8th most common cause of
all mortality in U.S.
• In-hospital mortality rate of 6.8% for alcoholic
hepatitis in U.S.
• The “good news”: Only minority of heavy drinkers
develop AH and/or cirrhosis.
• The Bad News: Rising prevalence of 12-month
and lifetime Alcohol Use Disorder (13.9% and
29.1%), classified in DSM-V
Asrani 2010, Hepatology 52:408
Grant 2015, JAMA Psychiatry 72: 757
4/12/2017
2
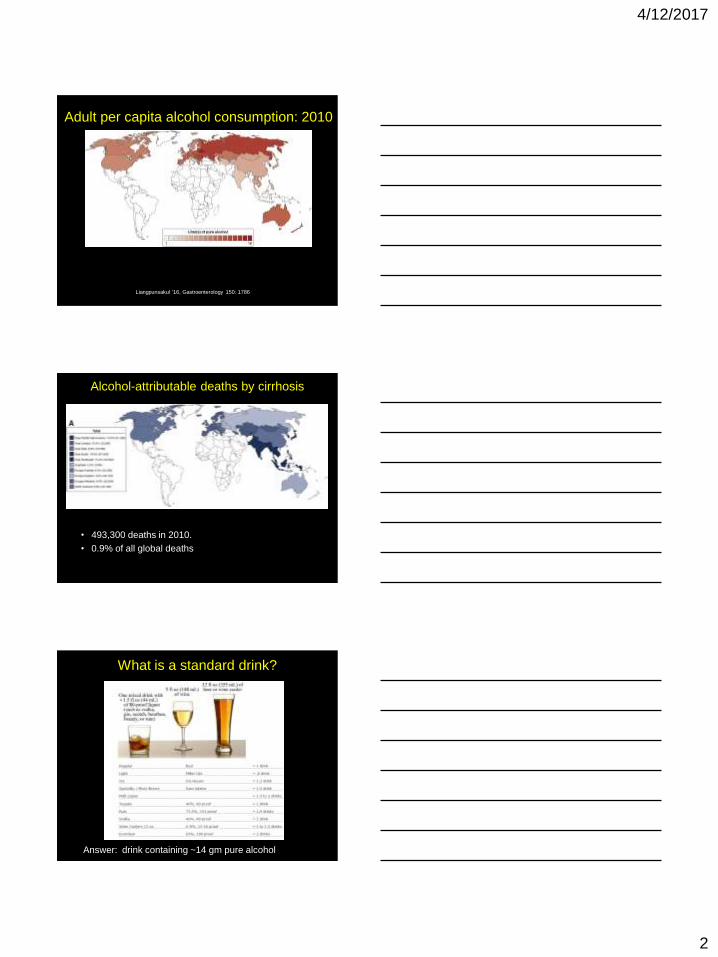
Adult per capita alcohol consumption: 2010
Liangpunsakul '16, Gastroenterology 150: 1786
Alcohol-attributable deaths by cirrhosis
• 493,300 deaths in 2010.
• 0.9% of all global deaths
What is a standard drink?
Answer: drink containing ~14 gm pure alcohol
4/12/2017
3
Risk Factors for ALD
• Female: Lower alcohol threshold for ALD
• Young age daily drinking > Binge/episodic drinking
• PNPLA3 allele GG vs. CC (Odds ratio 4.30)
• Obesity, NASH, or malnutrition
• Chronic liver disease: HCV, HBV, iron overload
• Tobacco
Long-term health risks of alcoholism
• Neurologic: dementia, stroke, neuropathy
• Cardiovascular: cardiomyopathy, a fib, Htn, MI
• Cancer: mouth, throat, esophageal, liver,
colon, breast
• GI: Alcoholic hepatitis, cirrhosis, pancreatitis,
gastritis
• Psychiatric: depression, anxiety, suicide
• Social: unemployment, lost productivity, family
problems, violence
Medications to treat alcoholism
• Pharmacotherapy with brief medical-management counseling
can reduce heavy drinking in persons with alcohol dependence
Good reference: Friedmann'13, Alcohol use in adults, NEJM 368:365
4/12/2017
4
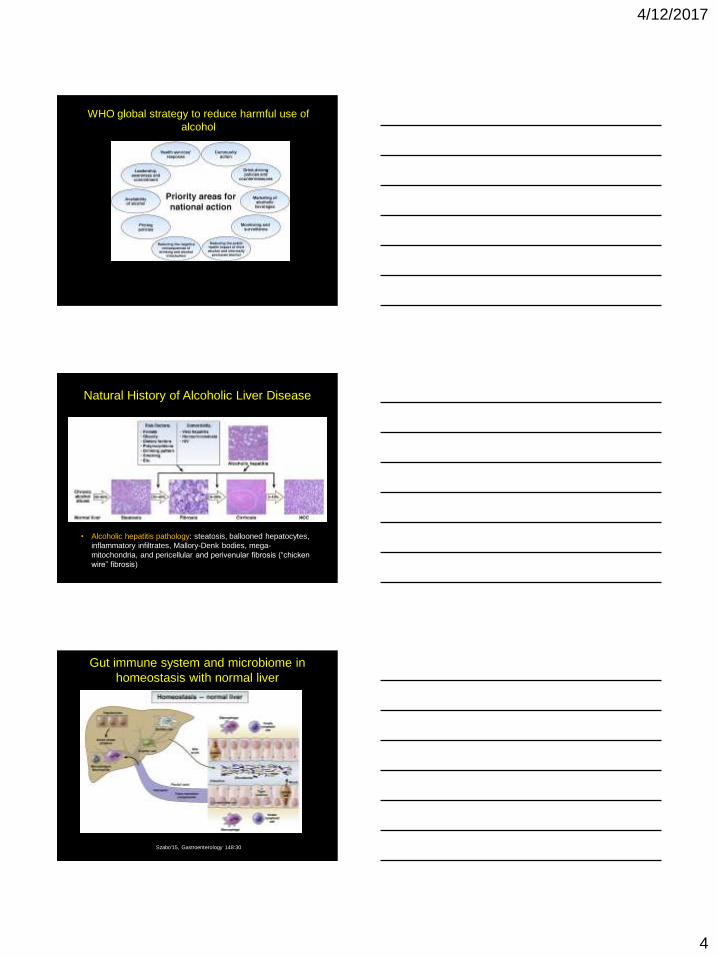
WHO global strategy to reduce harmful use of
alcohol
Natural History of Alcoholic Liver Disease
• Alcoholic hepatitis pathology: steatosis, ballooned hepatocytes,
inflammatory infiltrates, Mallory-Denk bodies, mega-
mitochondria, and pericellular and perivenular fibrosis (“chicken
wire” fibrosis)
Gut immune system and microbiome in
homeostasis with normal liver
Szabo'15, Gastroenterology 148:30

4/12/2017
5
Gut-liver axis in ALD
New understanding new Rx targets
Singal'14, Clinical Gastro and Hep 12:555
Case Presentation
• 35 year old women brought to clinic by fiancée
• Complains that he exaggerates and she only
drinks when she parties
• She noticed some “yellow skin and eyes”

4/12/2017
6
Case Presentation
• Initial eval: anxious young woman
• Has very slight tremor notable in her upper
extremities
• Mild scleral icterus
• Vitals: 160/85, HR 85, 37.5 degrees C
• She has hepatomegaly, no palpable
splenomegaly, and no notable ascites
• Lungs are clear. Skin icteric
Clinical Features of Alcholic Hepatitis
• History
– Alcohol intake: Current; usually binge; or recently
discontinued.
– New onset jaundice
– Weight loss, malnutrition
• Exam
– Toxic-appearing, fever, tachycardia
– Tender hepatomegaly +/- bruit
– Signs of chronic liver dz (ascites, spider
angiomata, muscle loss, hepatic encephalopathy)
• Similar to decompensated alcoholic cirrhosis,
aside from recent alcohol intake
Lab Features of AH
• AST, ALT elevation rarely >400
• AST/ALT ratio >2 (AST increase from
mitochondrial damage)
• T. Bili >5 mg/dl
• WBC > 10K (DDx infection)
• Decreased platelets BM suppression vs
portal HTN
• Increased INR
• Decreased Hgb nutritional deficieny vs
bleeding

4/12/2017
7
Making the diagnosis of AH
• Clinical suspicion and history
• Labs
• Rule out other etiologies
• Consider liver biopsy, when in doubt
– Not routinely done in US despite gold standard
– Thrombocytopenia and coagulopathy in many pts
– Transjugular route most common and safest
– Perform for diagnostic uncertainty that would
impact clinical managment
Assessing AH severity and prognosis
• Spontaneous encephalopathy: grave prognosis
• Steatohepatitis score
• Multi-organ Failure and Systemic Inflammation
Syndrome
• Various prediction models or scoring systems:
– Maddrey’s modified discriminant function (DF):
Bilirubin + PT
– MELD score: Bilirubin + INR + Cr
– ABIC: Age + bilirubin + INR +Cr
– Glasgow alcoholic hepatitis score: ABIC + WBC
– Lille score: Dynamic model. Assess response to
steroids at day 7. Establish threshold for steroid
treatment futility (Age, albumin, bilirubin, Cr, PT)
Discriminant function
• Most widely used prediction model.
• >32 predicts survival benefit if treated with prednisolone
• Specificity suboptimal. Static variable, calculated on adm
• Key inclusion criteria for prospective treatment trials
4/12/2017
8
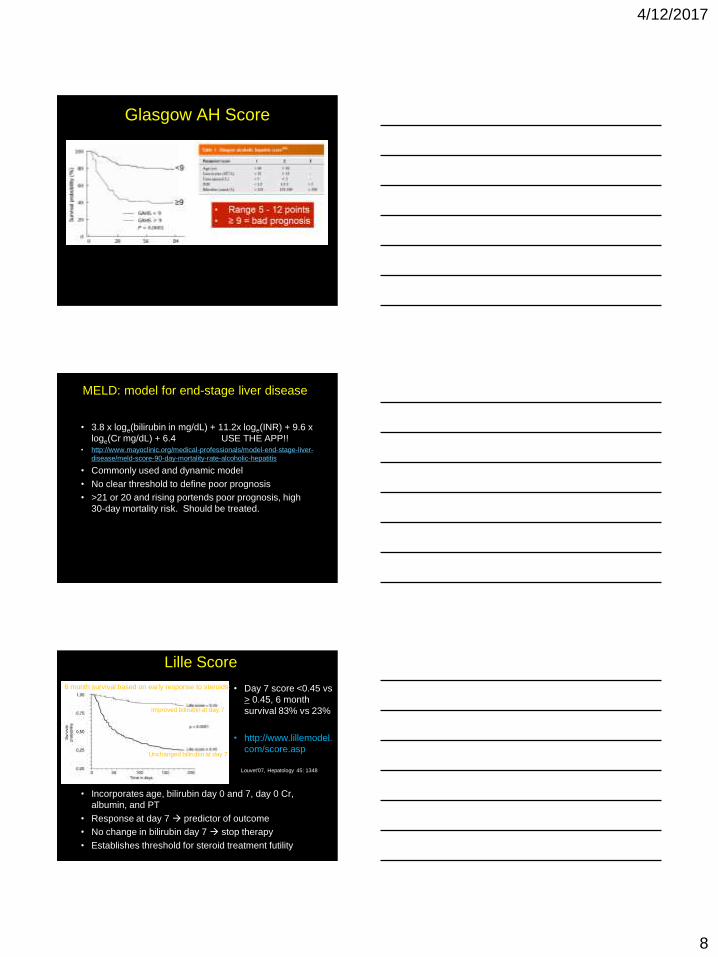
Glasgow AH Score
• a
MELD: model for end-stage liver disease
• 3.8 x loge(bilirubin in mg/dL) + 11.2x loge(INR) + 9.6 x
loge(Cr mg/dL) + 6.4 USE THE APP!!• http://www.mayoclinic.org/medical-professionals/model-end-stage-liver-
disease/meld-score-90-day-mortality-rate-alcoholic-hepatitis
• Commonly used and dynamic model
• No clear threshold to define poor prognosis
• >21 or 20 and rising portends poor prognosis, high
30-day mortality risk. Should be treated.
Lille Score
• Incorporates age, bilirubin day 0 and 7, day 0 Cr,
albumin, and PT
• Response at day 7 predictor of outcome
• No change in bilirubin day 7 stop therapy
• Establishes threshold for steroid treatment futility
• Day 7 score <0.45 vs
> 0.45, 6 month
survival 83% vs 23%
• http://www.lillemodel.
com/score.asp
6 month survival based on early response to steroids:
Improved bilirubin at day 7
Unchanged bilirubin at day 7
Louvet'07, Hepatology 45: 1348

4/12/2017
9
Back to the case
• Labs:
– WBC 12K
– Plts 90K
– Hgb 12.8
– Electrolytes, BUN, Cr are normal
– TBili 7.5, Dbili 4, AST 175, ALT 55
– INR 2.0
• Ultrasound:
– Hepatomegaly and steatosis
– Spleen is upper limit of normal
– No masses, no ascites
Assessment of this patient
• Severity by MELD and discriminant function is
high:
– MELD = 22
– DF = 35
• What do you do next?
Initial treatment for AH
• Resuscitation: Sick! 6.8% in-hospital mortality
• Rule out infection—resembles AH
– Ascites paracentesis to r/o SBP
– Low threshold for antibiotics
• Liver biopsy (transjugular route) if needed
• Renal fxn: replete fluids, no NSAIDS; albumin;
caution with diuretics, contrast dyes
• Encephalopathy: lactulose, rifaximin
• Withdrawl: benzodiazepine protocols
• Nutrition: Vit B complex (Wernicke’s), protein.
• Abstinence: critical to recovery

4/12/2017
10
Enteral nutrition vs prednisone
Cabre '00 Hepatology 32:36
71 pts randomized:
Prednisone 40 mg x 30d
Vs
Total enteral nutrition
2000 kcal/d x 30d
Surv
ival
Intention to treat analysis
• Similar 30 day mortality (9/36 vs 11/35)
• 1 year mortality higher with steroids
– 10/27 vs 2/24 p = 0.025
– 9 of 10 steroid group deaths due to infection
• Nutrition comparable to steroids
Intensive vs conventional nutrition
Moreno'16, Gastroenterology 150: 903
Multicenter RCT:
136 patients
Methylprednisolone +
Conventional EN
Vs
Intensive EN
14 days via NGT
6 month survival as primary
end point
• Per protocol analysis: 6m survival 69.8% (intensive) vs 46.8%
(conventional); p = 0.015
• Intention to treat analysis: No statistical difference ( p = 0.406)
• 48.5% withdrew feeding tube prematurely
• Low daily calories (< 21.5 kcal/kg/day) associated with death
Meta analysis of nutrition studies
• 9 enteral feeding trials; 4 parenteral trials
• 20% drop in mortality with feeding
• Nutrition associated with less HE and infections
• Better trials needed.
• Recommend 1600-2000 kcal/d; 60-100 gm protein
Fialla’15 Liver Int 35:2072
4/12/2017
11
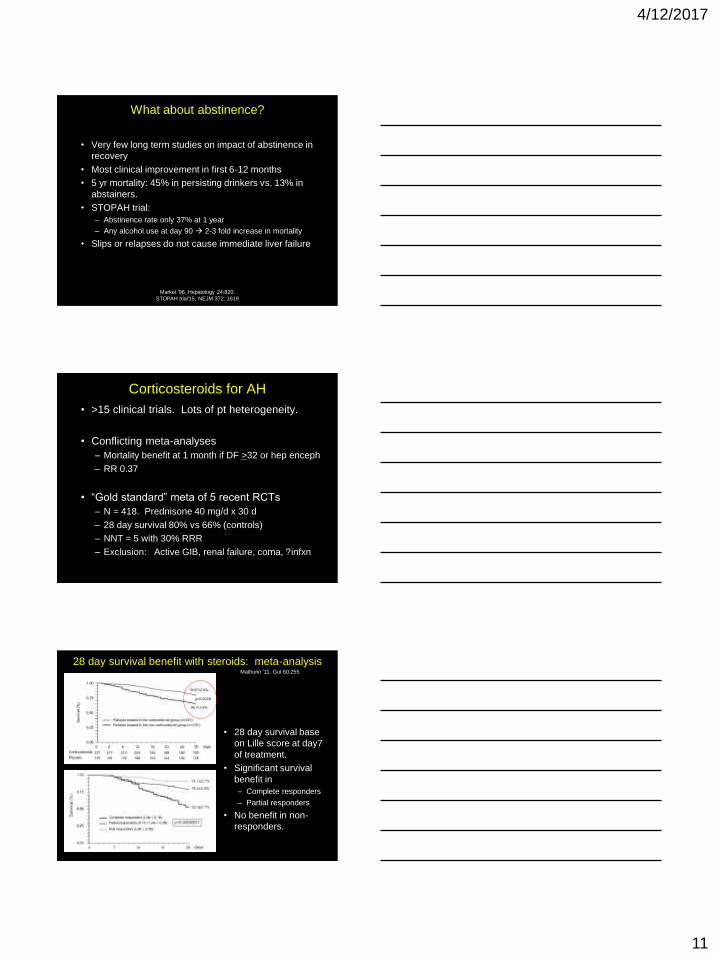
What about abstinence?
• Very few long term studies on impact of abstinence in
recovery
• Most clinical improvement in first 6-12 months
• 5 yr mortality: 45% in persisting drinkers vs. 13% in
abstainers.
• STOPAH trial:
– Abstinence rate only 37% at 1 year
– Any alcohol use at day 90 2-3 fold increase in mortality
• Slips or relapses do not cause immediate liver failure
Markel '96, Hepatology 24:820.
STOPAH trial'15, NEJM 372: 1619
Corticosteroids for AH
• >15 clinical trials. Lots of pt heterogeneity.
• Conflicting meta-analyses
– Mortality benefit at 1 month if DF >32 or hep enceph
– RR 0.37
• “Gold standard” meta of 5 recent RCTs
– N = 418. Prednisone 40 mg/d x 30 d
– 28 day survival 80% vs 66% (controls)
– NNT = 5 with 30% RRR
– Exclusion: Active GIB, renal failure, coma, ?infxn
Mathurin '11, Gut 60:255
28 day survival benefit with steroids: meta-analysis
• 28 day survival base
on Lille score at day7
of treatment.
• Significant survival
benefit in
– Complete responders
– Partial responders
• No benefit in non-
responders.
4/12/2017
12
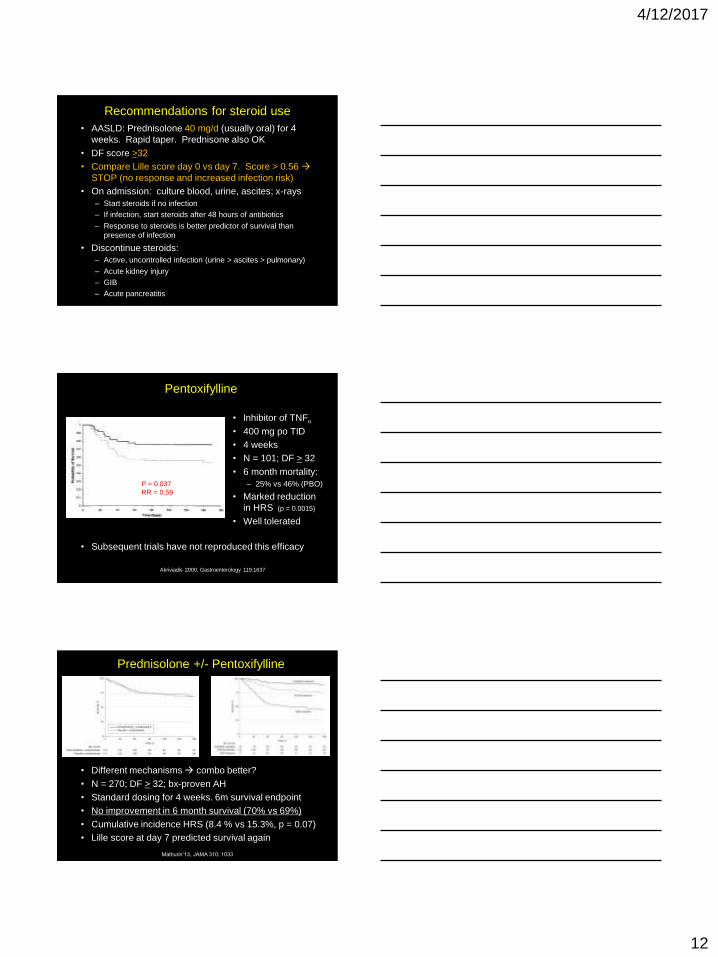
Recommendations for steroid use
• AASLD: Prednisolone 40 mg/d (usually oral) for 4
weeks. Rapid taper. Prednisone also OK
• DF score >32
• Compare Lille score day 0 vs day 7. Score > 0.56
STOP (no response and increased infection risk)
• On admission: culture blood, urine, ascites; x-rays
– Start steroids if no infection
– If infection, start steroids after 48 hours of antibiotics
– Response to steroids is better predictor of survival than
presence of infection
• Discontinue steroids:
– Active, uncontrolled infection (urine > ascites > pulmonary)
– Acute kidney injury
– GIB
– Acute pancreatitis
Pentoxifylline
Akriviadis 2000, Gastroenterology 119:1637
• Inhibitor of TNFa
• 400 mg po TID
• 4 weeks
• N = 101; DF > 32
• 6 month mortality:
– 25% vs 46% (PBO)
• Marked reduction
in HRS (p = 0.0015)
• Well tolerated
P = 0.037
RR = 0.59
• Subsequent trials have not reproduced this efficacy
Prednisolone +/- Pentoxifylline
Mathurin’13, JAMA 310: 1033
• Different mechanisms combo better?
• N = 270; DF > 32; bx-proven AH
• Standard dosing for 4 weeks. 6m survival endpoint
• No improvement in 6 month survival (70% vs 69%)
• Cumulative incidence HRS (8.4 % vs 15.3%, p = 0.07)
• Lille score at day 7 predicted survival again

4/12/2017
13
STOPAH Trial
Thursz'15, NEJM 372:1619
• Multicenter RCT in UK. N=1092. DF>32, bili>4. No GIB, infxn.
• Pred vs PTX vs Pred/PTX vs double placebo for 28 days
• Borderline reduction in mortality in prednisolone group at 28d
– Mortality at 28d OR (1.07 PTX vs 0.72 Pred, p = 0.06)
• No benefit at 90 days or 1 yr for prednisolone, PTX or combo
• Serious infxns: 13% prednisone vs 7% no pred, p = 0.002
STOPAH: 1 year survival curve
Take away messages of STOPAH:
• PTX no effective for AH
• Steroids not effective beyond 1 month to improve survival
• Abstinence is key
N-acetylcysteine
• French study; 180/430 randomized
• DF >32; bx-confirmed AH
• Prednisolone 40 mg/d +/- NAC
• NAC bolus day 1; 5 days IV total
• Primary endpoint = 6 month survival
Nguyen-Khac'11, NEJM 356:1781
• 6m survival not significantly improved (27% vs 38%)
• 1m mortality significantly lower (8% vs 24%)
• Decreased HRS and infection rates
• Overall safe. No harm to add NAC to steroid?

4/12/2017
14
Granulocyte Colony-Stimulating Factor
• G-CSF stimulates bone marrow to
produce and release neutrophils and
stem cells (CD34+)
• May stimulate liver regeneration
• Pilot RCT in India. N = 46
• “standard medical therapy” of PTX +
nutrition +/- G-CSF
• G-CSF given 5 mcg/kg SQ q12 hrs
for 5 days, then q3 days through d30
Singh'14, Am J Gastro 109:1417
• Marked improvement survival at day 90 in G-CSF arm
(78.3% vs 30.4%, p=0.001)
• Significant reduction in MELD, DF and Child-Pugh scores
• Significant increase in peripheral blood CD34+ cells
When all else fails….Liver transplant?
OLT for AH: French experience
Mathurin'11. NEJM 365: 1790
• US and most countries require 6 month abstinence
• Non-responding AH patients: >50% die within first 3 months
• Only 3% of livers transplanted into AH patients
• Many ethical issues
• Prospective study. N=26
steroid non-responders. Lille
score >0.45. Received OLT
• Matched controls w/o OLT
• 6 month survival 77% vs 23%
• 2 year survival 71%
• 3 recipients returned to drinking
Similar outcomes between AH and alcoholic cirrhosis
liver transplantation: U.S. experience
• 55 post-OLT for AH followed. Matched with 165 post-OLT for alc cirrhosis
• 5 year survival 80% vs 78%
• Causes of graft loss and pt mortality were similar in both groups. Not
alcohol-related.
Singal'12, Hepatology 55:1398

4/12/2017
15
AH Treatment
Ineffective therapy for AH
Thursz and Morgan'16, Ibid
Anti-TNFa therapy (infliximab, entanercept)
Therapeutic strategies undergoing trials

4/12/2017
16
Approach to acute AH patient
1. Resuscitate and stage
2. Nutrition
3. Treat complications of cirrhosis and infection
4. Establish diagnosis if uncertain. Biopsy?
5. Treatment options:
MELD > 20 or DF > 32
Steroids: Survival benefit only to 1 month
PTX: No proven benefit
NAC: Little harm. Need more data
G-CSF: promising. Need more data
6. Assess at day 0 and 7 with Lille model
Response Continue treatment
Refer to abstinence program
No/Slow response Clinical trials; OLT if
available; palliative care
Use steroids to get severe AH patient through
the first month so that they can abstain.
Reach out to expert and/or transplant centers
Abstinence is the key intervention
Approach to acute AH patient
Major complications of cirrhosis
and portal hypertension
• Variceal hemorrhage
• Ascites
• Spontaneous bacterial peritonitis
• Hepatic encephalopathy
• Hepatorenal syndrome
• Hepatopulmonary syndrome
• Hepatocellular carcinoma

4/12/2017
17
2.8 (1.0-7.5)
8.7 (3.3-22.6)
10.7 (2.5-45.6)
10.1 (0.6-181.4)
6.6 (2.0-22.3)
2.7 (0.2-30.2)
9.9 (3.2-30.0)
11.3 (6.3-20.1)
7.3 (4.8-11.1)
OR
0.1 0.5 1 10 50
Protective Effect Increased Risk
OR (95% Cl) Study (year/bacteria)
Ji (2005/Shigella)
Mearin (2005/Salmonella)
Wang (2004/Unspecified)
Okhuysen (2004/Unspecified)
Cumberland (2003/Unspecified)
llnyckyj (2003/Unspecified)
Parry (2003/Bacterial NOS)
Rodriguez (1999/Bacterial NOS)
Pooled estimate
4/12/2017
18

4/12/2017
19
Control of acute variceal bleeding
• Resuscitate and assess severity
– Intubate massive bleeder or agitated. MICU care.
– IVF, blood products
• Endoscopic therapy
– Variceal band ligation in majority; gastric varices less success
– Sclerotherapy—injection of sclerosant directly into varices
• Splanchnic vasoconstriction: Octreotide 50-100 mcg/hr
• Balloon tamponade: Usually if endoscopy and
octreotide fail and awaiting TIPS or urgent
transplantation. Many potential complications.
• Transjugular intrahepatic portosystemic shunt (TIPS)
– Bridge to transplant
– HE in 20-30%
– Stenosis or occlusion in 30-60%
• 30 day mortality remains high at 15-20%

4/12/2017
20
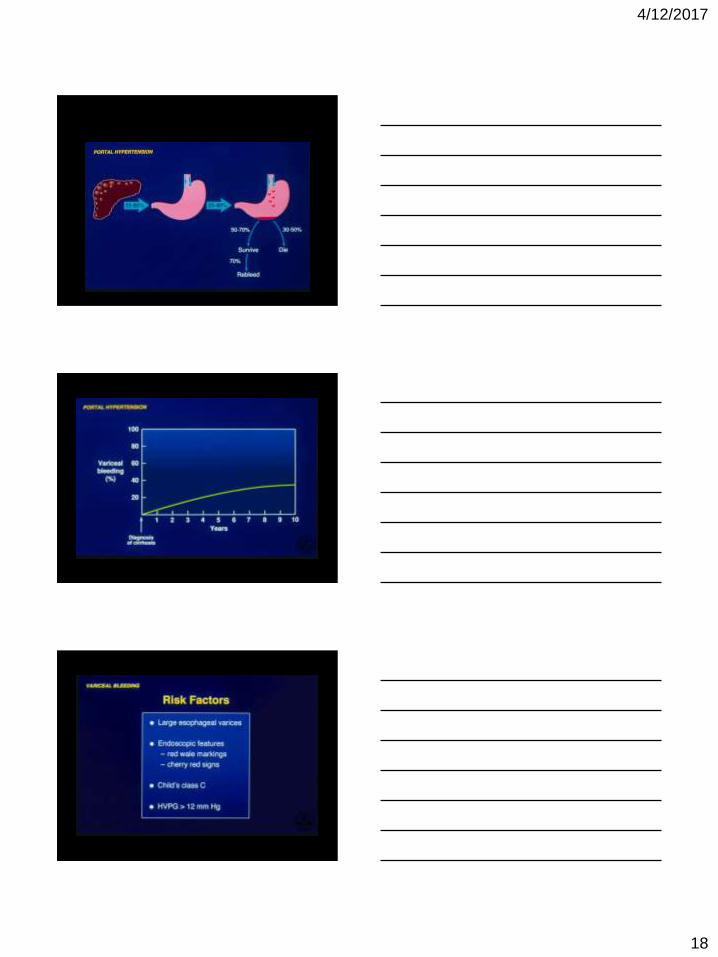
Prevention of variceal bleeding
• Variceal band ligation repeat until obliterated
• Propranolol or nadolol: Non-selective beta-blocker to decrease portal hypertension.
• TIPS: Bridge to transplant
• Portosystemic shunt: Infrequent since TIPS available
• Primary prophylaxis: Band ligation vs beta-blockers
Largely replaced by more objective MELD score,
but need to know
Ascites: accumulation of fluid in peritoneum
Most common complication
of cirrhosis

4/12/2017
21
Ascites in cirrhosis

4/12/2017
22
Think diagnostic paracentesis….
Inoculate fluid directly into blood culture bottles.
Diagnose SBP with cell count and culture.
Calculate SAAG to confirm diagnosis

4/12/2017
23
Treatment of cirrhotic ascites
• Rigid salt restriction: < 2 gm Na/day
• Diuretics: titrate to effect or complication (HE, HRS)
– spironolactone 100-200 mg/d (max 400mg) and
– furosemide 40-80 mg/d (max 160 mg)
• Monitor wt, urine Na and K, serum lytes, and Cr
• Refractory ascites: diuretic failure
– Repeated large volume paracentesis (5-10 L) with IV
albumin infusion (10 g/liter removed)
– TIPS: associated with HE; does not improve survival
• Consider OLT evaluation
Ascites prognosis poor without definitive therapy
Spontaneous bacterial peritonitis
No evidence of intra-abdominal secondary source
of infection

4/12/2017
24
Keep high index of suspicion for SBP
SBP Treatment
• Ascites fluid PNM count > 250/ul. Confirm by positive
culture
• E. coli, Klebsiella, other gut microbes most common.
Gram positive also found
• Cefotxime 2 gm IV q 8hrs for 5 days.
• Avoid aminoglycosides (nephrotoxic)
• Recommend prophylaxis abx in patients with variceal
bleeding
4/12/2017
25
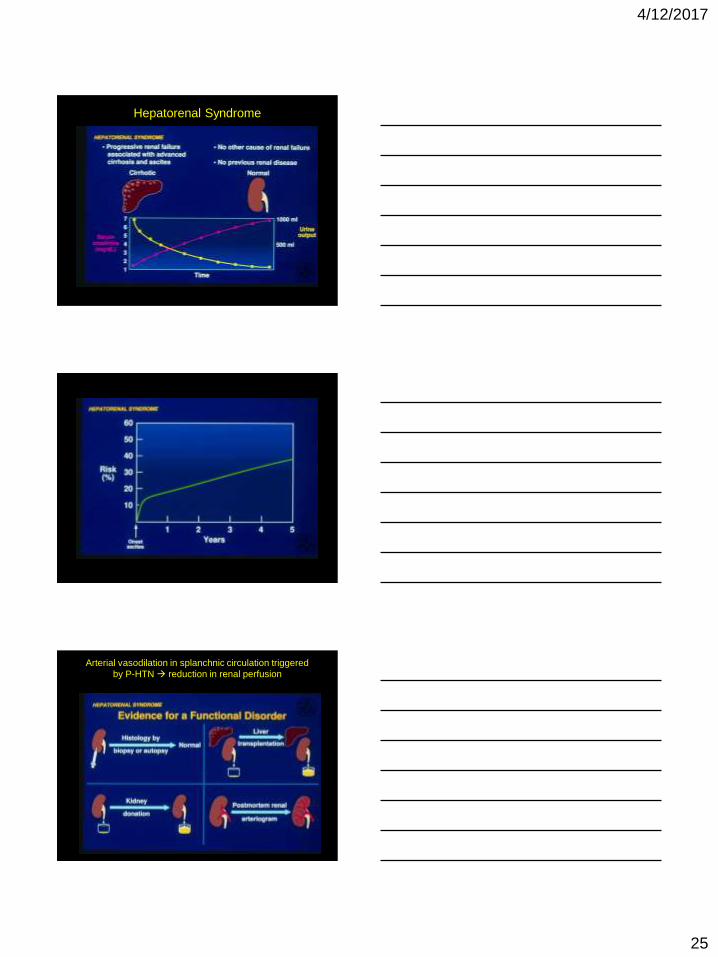
Hepatorenal Syndrome
Arterial vasodilation in splanchnic circulation triggered
by P-HTN reduction in renal perfusion
4/12/2017
26
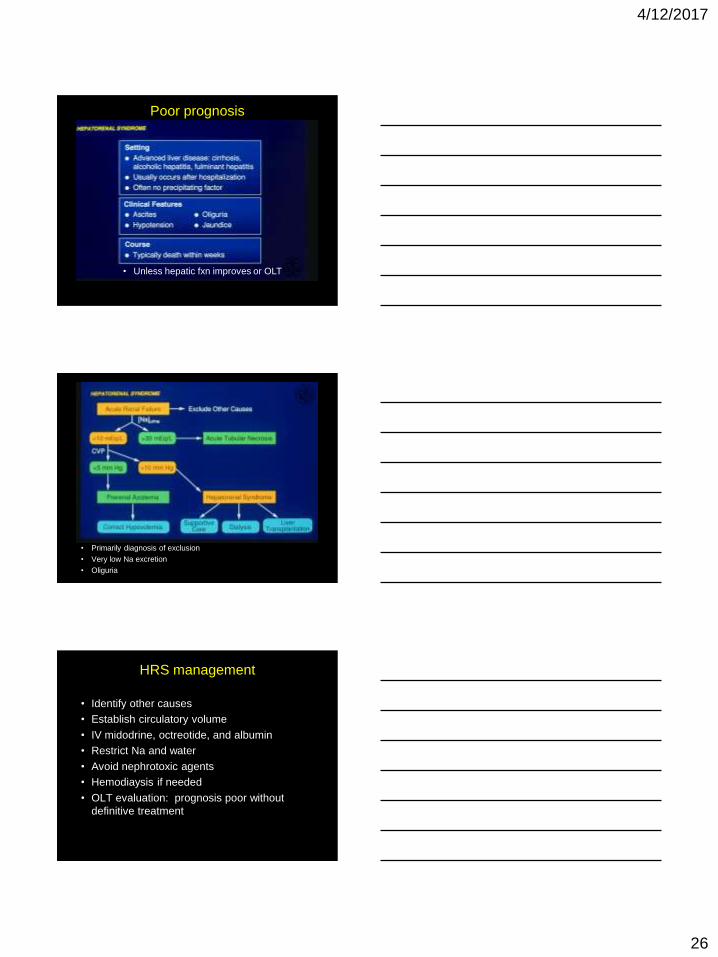
Poor prognosis
• Unless hepatic fxn improves or OLT
• Primarily diagnosis of exclusion
• Very low Na excretion
• Oliguria
HRS management
• Identify other causes
• Establish circulatory volume
• IV midodrine, octreotide, and albumin
• Restrict Na and water
• Avoid nephrotoxic agents
• Hemodiaysis if needed
• OLT evaluation: prognosis poor without
definitive treatment
4/12/2017
27
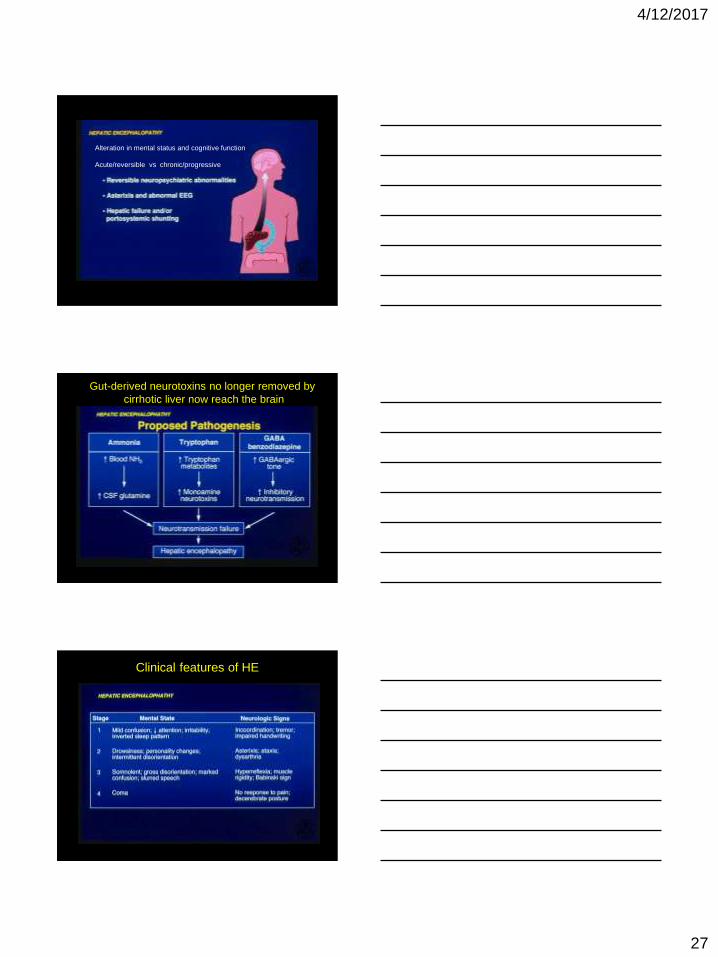
Alteration in mental status and cognitive function
Acute/reversible vs chronic/progressive
Gut-derived neurotoxins no longer removed by
cirrhotic liver now reach the brain
Clinical features of HE
4/12/2017
28
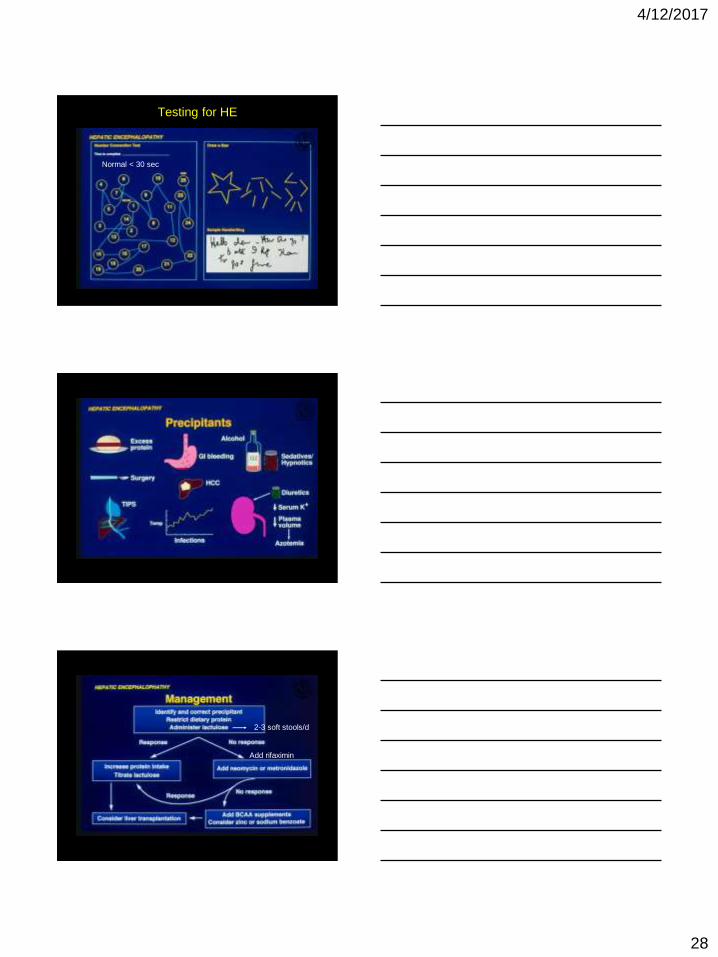
Testing for HE
Normal < 30 sec
Add rifaximin
2-3 soft stools/d
4/12/2017
29
Hepatopulmonary Syndrome
• Clinical triad:
– Liver disease
– Increased alveolar-arterial gradient while breathing room air
– Intrapulmonary vascular dilations
• Pathophysiology:
– Increased vasodilators (nitric oxide?) due to increased liver
production or decreased clearance
– Microscopic intrapulmonary A-V dilations
– Overperfusion V/Q mismatch increased alveolar-arterial
gradient
• Diagnosis:
– Dyspnea and hypoxemia, worse when standing
– Pulse ox and ABG
– Contrast echocardiography. Rapid transit of venous contrast
through lungs to left atrium
• Treatment: Liver transplantation, supplemental O2,
Hepatocellular Carcinoma
• Marked increase risk in cirrhotics, esp from HBV, HCV, NASH, and
hemochromatosis
• Frequently asymptomatic until late. Suspect in decompensated
previously doing well.
• Pain, early satiety, obstructive jaundice, and palpable mass
• Diagnosis:
– Elevated alpha fetoprotein; not specific
– Ultrasound. Recommend q 6 month surveillance
– Triple phase CT
• Treatment: OLT most definitive
– Surgical resection. Recurrence common
– Transcatheter arterial chemoembolization (TACE). High dose chemo to
feeding artery of tumor.
– Systemic chemotherapy. HCC poorly responsive. Sorafenib promising
– Brachytherapy