Powerpoint: colorectal surgical diseases
74
COLORECTAL SURGICAL COLORECTAL SURGICAL DISEASES DISEASES GROSS ANATOMY GROSS ANATOMY
Transcript of Powerpoint: colorectal surgical diseases

COLORECTAL SURGICAL COLORECTAL SURGICAL DISEASESDISEASES
GROSS ANATOMYGROSS ANATOMY

LARGE INTESTINELARGE INTESTINE5 parts: ascending, transverse, 5 parts: ascending, transverse, descending, sigmoid colon and rectumdescending, sigmoid colon and rectumBegins at the cecum - ileocecal valveBegins at the cecum - ileocecal valveAppendix projects from the Appendix projects from the convergence of the teniae at the convergence of the teniae at the lowest part of the cecumlowest part of the cecumAscending colon is retroperitoneal, Ascending colon is retroperitoneal, suspended from above at the hepatic suspended from above at the hepatic flexure by hepatocolic ligamentflexure by hepatocolic ligament

LARGE INTESTINELARGE INTESTINEANATOMYANATOMY
Transverse colon is intraperitoneal, from Transverse colon is intraperitoneal, from hepatic flexure to the splenic flexure, hepatic flexure to the splenic flexure, suspended by splenocolic and gastrocolic suspended by splenocolic and gastrocolic ligamentsligamentsDescending colon is retroperitoneal, Descending colon is retroperitoneal, continued by sigmoid coloncontinued by sigmoid colonSigmoid colon is intraperitonealSigmoid colon is intraperitonealRectum begins at the level of S3, 12-15 Rectum begins at the level of S3, 12-15 cm. in length, passes the pelvic cm. in length, passes the pelvic diaphragm, ends in the anal canal diaphragm, ends in the anal canal

LARGE INTESTINELARGE INTESTINEANATOMYANATOMY
Rectum describes 3 lateral curvesRectum describes 3 lateral curvesRectal ampulla is the most distal portion of Rectal ampulla is the most distal portion of the rectumthe rectumRectum ends at the anorectal junctionRectum ends at the anorectal junctionAnal canal, 4 cm. in length, ends at the Anal canal, 4 cm. in length, ends at the anal vergeanal vergeInternal sphincter- smooth inner muscle Internal sphincter- smooth inner muscle with involuntary controlwith involuntary controlStriated external sphincter- under Striated external sphincter- under voluntary controlvoluntary control





LARGE COLONLARGE COLONHISTOLOGYHISTOLOGY
Colonic wall- 4 layers: mucosa, Colonic wall- 4 layers: mucosa, submucosa, muscularis propria, serosasubmucosa, muscularis propria, serosaMucosa is lined by columnar epithelium, Mucosa is lined by columnar epithelium, malignant cells confind to this are reffered malignant cells confind to this are reffered to as carcinoma in situto as carcinoma in situ1-2 cm. above the dentate line is a zone of 1-2 cm. above the dentate line is a zone of transitional epithelium having both transitional epithelium having both columnar and squamous cellscolumnar and squamous cellsBelow the dentate line, the anal canal is Below the dentate line, the anal canal is lined by modified skin- no hair follicle, no lined by modified skin- no hair follicle, no seb. glandsseb. glands

LARGE COLONLARGE COLONHISTOLOGYHISTOLOGY
Submucosa contains blood vessels and Submucosa contains blood vessels and lymphaticslymphaticsTumor cells must penetrate this layer to Tumor cells must penetrate this layer to gain access to the lymphatic system, gain access to the lymphatic system, enabling metastatic spreadenabling metastatic spreadSubmucosa is the strongest layer of the Submucosa is the strongest layer of the bowel wallbowel wallMuscularis propria is made up of circular Muscularis propria is made up of circular and longitudinal smooth musclesand longitudinal smooth musclesRectum lacks a serosal layerRectum lacks a serosal layerAccording to the depth invasion- Duke’s According to the depth invasion- Duke’s stagingstaging


LARGE BOWELLARGE BOWELARTERIAL SUPPLYARTERIAL SUPPLY
1.- Ileocolic art.- terminal branch of SMA1.- Ileocolic art.- terminal branch of SMA2.- Right colic art.- from SMA or ileocolic2.- Right colic art.- from SMA or ileocolic3.- Middle colic art.- from SMA3.- Middle colic art.- from SMA4.- Left colic art- from IMA4.- Left colic art- from IMA5.- Rectosigmoid art.- from IMA5.- Rectosigmoid art.- from IMA6.- Superior rectal art.- from IMA6.- Superior rectal art.- from IMA7.- Middle rectal art.- from internal ileal7.- Middle rectal art.- from internal ileal8.- Inferior rectal art.- from internal 8.- Inferior rectal art.- from internal pudental art.pudental art.


LARGE BOWELLARGE BOWELVENOUS RETURNVENOUS RETURN
Colorectal veins parallel the arteries Colorectal veins parallel the arteries similarly namedsimilarly named
Colon veins drain into the portal Colon veins drain into the portal systemsystem
Rectal veins drain into the portal and Rectal veins drain into the portal and systemic venous systemsystemic venous system

LARGE BOWELLARGE BOWELPHYSIOLOGYPHYSIOLOGY
Storage, transport, concentration of Storage, transport, concentration of intestinal waste productsintestinal waste productsNa, chloride, water are actively absorbedNa, chloride, water are actively absorbedThe absorbative capacity of the colon is The absorbative capacity of the colon is about 2 l/ dayabout 2 l/ dayColonic mucosa secretes K and bicarbonate- Colonic mucosa secretes K and bicarbonate- excessive diarrhea may result in potassium excessive diarrhea may result in potassium and bicarbonate losses and metabolic and bicarbonate losses and metabolic acidosisacidosisColonic gas originates from both swallowed Colonic gas originates from both swallowed air and the by-products of bacterial reactionsair and the by-products of bacterial reactions

EVALUATION OF THEEVALUATION OF THECOLON, RECTUM AND ANUSCOLON, RECTUM AND ANUS
History:History:
– Recent and past bowel habitRecent and past bowel habit– Pattern of rectal bleedingPattern of rectal bleeding– Consistency of stoolConsistency of stool– Family history of IBD, colonic polyps, Family history of IBD, colonic polyps,
cancercancer– Nature of painNature of pain

PHYSICAL EXAMINATIONPHYSICAL EXAMINATION
Anorectal examination in the left Anorectal examination in the left lateral decubitus:lateral decubitus:– Inspection of the perianal regionInspection of the perianal region– Digital rectal examinationDigital rectal examination– AnoscopyAnoscopy– SigmoidocopySigmoidocopy– Examination of stoolsExamination of stools

INVESTIGATIONS INVESTIGATIONS
1. Plain abdominal X ray1. Plain abdominal X ray
2. Barium enema2. Barium enema
3. Endoscopy +/- biopsy3. Endoscopy +/- biopsy
4. Abdominopelvic CT4. Abdominopelvic CT
5. Endoscopic ultrasonography5. Endoscopic ultrasonography

PLAIN ABDO X RAYPLAIN ABDO X RAY
Assess the pattern of air and fluidAssess the pattern of air and fluid– PneumoperitoneumPneumoperitoneum– Gaseous distention of small or large Gaseous distention of small or large
bowelbowel– Fluid level- topographyFluid level- topography
Routine examination of an acute Routine examination of an acute abdomenabdomen
Patient in stand up position during Patient in stand up position during exam.exam.

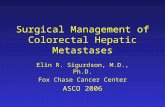
This upright abdominal x-ray shows multiple air-This upright abdominal x-ray shows multiple air-fluid levels, which are indicative of a bowel fluid levels, which are indicative of a bowel
obstruction.obstruction.
Dilation of the large intestine, Dilation of the large intestine, indicated by the larger caliber indicated by the larger caliber of the air-filled segments and of the air-filled segments and the transverse lines called the transverse lines called haustra. .
The air extends into the left The air extends into the left lower quadrant and pelvis, lower quadrant and pelvis, indicating that the obstructive indicating that the obstructive lesion is quite distal, in the lesion is quite distal, in the recto-sigmoid region. recto-sigmoid region.
Therefore this is a distal large Therefore this is a distal large bowel obstructionbowel obstruction

A 50 year old man underwent an above-knee amputation to remove his A 50 year old man underwent an above-knee amputation to remove his gangrenous leg. He developed nausea and dyspneoa on the 4th gangrenous leg. He developed nausea and dyspneoa on the 4th
postoperative day. On examination he had tachypnoea and postoperative day. On examination he had tachypnoea and tachycardia, but was apyrexic. On chest auscultation air entry was tachycardia, but was apyrexic. On chest auscultation air entry was
reduced bilaterally at the lung bases. The abdomen, though distended, reduced bilaterally at the lung bases. The abdomen, though distended, was not tender and the bowel sounds were audible. Digital rectal was not tender and the bowel sounds were audible. Digital rectal
examination was unremarkable. examination was unremarkable.

Acute colonic pseudo-obstruction or Acute colonic pseudo-obstruction or Ogilvie syndromeOgilvie syndrome
The chest radiograph shows dilated loops of large bowel. This The chest radiograph shows dilated loops of large bowel. This finding is confirmed on the plain abdominal film which shows a finding is confirmed on the plain abdominal film which shows a picture of large bowel obstruction. There is no evidence of free gas picture of large bowel obstruction. There is no evidence of free gas under the diaphragm.under the diaphragm.
A subsequent CT scan of the abdomen did not reveal a mechanical A subsequent CT scan of the abdomen did not reveal a mechanical cause of the condition and colonoscopic decompression was cause of the condition and colonoscopic decompression was theraputic.theraputic.
DifferentialDifferential
Mechanical colonic obstruction Mechanical colonic obstruction
Toxic megacolon Toxic megacolon
Mesenteric ischaemia Mesenteric ischaemia

Acute colonic pseudo-obstruction or Ogilvie syndrome is a Acute colonic pseudo-obstruction or Ogilvie syndrome is a condition with clinical and radiological features of colonic condition with clinical and radiological features of colonic obstruction without any evidence of a mechanical cause.obstruction without any evidence of a mechanical cause.
Abdominal distension in this patient accounted for the Abdominal distension in this patient accounted for the respiratory distressrespiratory distress
Pathophysiology of Ogilvie syndrome is not clearly understood, Pathophysiology of Ogilvie syndrome is not clearly understood, though it is thought to be due to an imbalance in the though it is thought to be due to an imbalance in the autonomic innervation leading to a functional bowel autonomic innervation leading to a functional bowel obstruction. obstruction.
Ogilvie syndrome typically occurs in patients hospitalized with Ogilvie syndrome typically occurs in patients hospitalized with a significant illness e.g. severe cardio-respiratory disorders, a significant illness e.g. severe cardio-respiratory disorders, sepsis, electrolyte imbalance and postoperatively. sepsis, electrolyte imbalance and postoperatively.
Left untreated it can progress to colonic perforation and Left untreated it can progress to colonic perforation and peritonitis. peritonitis.

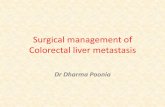
Complete colonic obstruction from an obstructing Complete colonic obstruction from an obstructing carcinoma in the descending left colon with proximal air-carcinoma in the descending left colon with proximal air-
fluid levels. fluid levels. The absence of air distally in the rectum or the sigmoid is The absence of air distally in the rectum or the sigmoid is
suggestive of complete obstruction. suggestive of complete obstruction. The ileocecal valve is competent, and thus, there is no The ileocecal valve is competent, and thus, there is no
small bowel air.small bowel air.

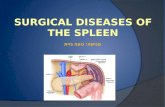
Upright radiograph: complete small bowel Upright radiograph: complete small bowel obstructionobstruction
Upright radiograph shows Upright radiograph shows multiple air-fluid levels of multiple air-fluid levels of varying size arranged in varying size arranged in inverted Us.inverted Us.
In the right lower pelvis, a In the right lower pelvis, a loop of small bowel is seen loop of small bowel is seen a finding suggestive of a finding suggestive of adhesive obstruction.adhesive obstruction.

CONTRAST ENEMACONTRAST ENEMA
It is not an emergent investigationIt is not an emergent investigation
Requires bowel preparationRequires bowel preparation
Instant enema in rare occasionsInstant enema in rare occasions
Indicated in assessing colon polyps, Indicated in assessing colon polyps, tumors or diverticulosis.tumors or diverticulosis.
If perforation is suspected- contrast If perforation is suspected- contrast substance used-gastrografinsubstance used-gastrografin

SINGLE CONTRASTSINGLE CONTRAST BARIUM ENEMA BARIUM ENEMA

DOUBLE CONTRASTDOUBLE CONTRAST BARIUM ENEMA BARIUM ENEMA

ENDOSCOPIC STUDIESENDOSCOPIC STUDIES
Rigid proctorectoscopy- can examine Rigid proctorectoscopy- can examine 25 cm. from the anal verge25 cm. from the anal verge
Position of the patient-lateral Position of the patient-lateral decubitus or prone jacknife positiondecubitus or prone jacknife position
Bowel preparation- 2 enemas onlyBowel preparation- 2 enemas only

COLONOSCOPYCOLONOSCOPY
Can assess the entire length of the Can assess the entire length of the coloncolon
Concurrent biopsy and polypectomy Concurrent biopsy and polypectomy is possibleis possible
Inssuflation of air induces some Inssuflation of air induces some discomfort for the patientdiscomfort for the patient
Bowel preparation mandatoryBowel preparation mandatory

COLONOSCOPYCOLONOSCOPYINDICATIONS:INDICATIONS:– The treatment of polypsThe treatment of polyps– Suspicious colon cancerSuspicious colon cancer– Evaluation of a positive fecal occult blood testEvaluation of a positive fecal occult blood test– Follow-up in pts. with IBDFollow-up in pts. with IBD
Bowel preparation:Bowel preparation:
- Nil by mouth for 8 h. prior to the procedure- Nil by mouth for 8 h. prior to the procedure
- Laxatives- Laxatives
- Enemas- Enemas

COLONOSCOPYCOLONOSCOPY



NORMAL COLONIC SURFACENORMAL COLONIC SURFACE


IRRITABLE BOWEL SYNDROMEIRRITABLE BOWEL SYNDROMENamed in the past “spastic colon”Named in the past “spastic colon”Clinical features:Clinical features:– Episodic cramping abdo pain at any time of the Episodic cramping abdo pain at any time of the
dayday– Episodes can last from 15 min.- several hoursEpisodes can last from 15 min.- several hours– The pain is unrelated to mealsThe pain is unrelated to meals– It may occur anywhere in the abdomenIt may occur anywhere in the abdomen– Symptoms occur daily for weeks at a time Symptoms occur daily for weeks at a time – Worse at times of sressWorse at times of sress– Eratic bowel habit- loose stools/constipationEratic bowel habit- loose stools/constipation– Abdominal distention/excess flatusAbdominal distention/excess flatus

IRRITABLE BOWEL SYNDROMEIRRITABLE BOWEL SYNDROME
Pathophysiology- low fiber diet Pathophysiology- low fiber diet seems to play a partseems to play a partColonic motility studiesColonic motility studies– abnormal rises in intraluminal pressure, abnormal rises in intraluminal pressure, – disordered peristalsisdisordered peristalsisThe small volume of feces-dehydrated, The small volume of feces-dehydrated,
fragmented- rabbit palletsfragmented- rabbit palletsImbalance in gut hormonal and autonomic Imbalance in gut hormonal and autonomic
control systemscontrol systems

IRRITABLE BOWEL SYNDROMEIRRITABLE BOWEL SYNDROME
ManagementManagement– Carcinoma and diverticulosis must be excluded Carcinoma and diverticulosis must be excluded
by colonoscopy/barium enemaby colonoscopy/barium enema
Treatment:Treatment:
- reasurence- reasurence
- adjusting the diet to include adequate fibre- adjusting the diet to include adequate fibre
- bulking agents, antispasmodic drugs- bulking agents, antispasmodic drugs
- codeine phosphate-analgesic for occasional use- codeine phosphate-analgesic for occasional use
- relaxation therapy- relaxation therapy

SIGMOID VOLVULUSSIGMOID VOLVULUS
PathophysiologyPathophysiology
Chronic constipation- enlarged, Chronic constipation- enlarged, elongated, atonic sigmoid colon= elongated, atonic sigmoid colon= dolicomegacolondolicomegacolon
Occasionally, the huge sygmoid loop, Occasionally, the huge sygmoid loop, heavy with feces becomes twisted on heavy with feces becomes twisted on its mesenteric pedicle- closed loop its mesenteric pedicle- closed loop obstructionobstruction
Venous infarction- perforation-peritonitisVenous infarction- perforation-peritonitis

SIGMOID VOLVULUSSIGMOID VOLVULUS
Clinical features:Clinical features:– Elderly, mentally handicapedElderly, mentally handicaped– Abdominal distension, abdominal painAbdominal distension, abdominal pain– Assymetrical distension, tympanismAssymetrical distension, tympanism– Variable degree of tendernessVariable degree of tenderness– Absolute constipation for at least 24 Absolute constipation for at least 24
hourshours– Perforation- peritonitisPerforation- peritonitis– PR- the rectum is emptyPR- the rectum is empty

SIGMOID VOLVULUSSIGMOID VOLVULUSManagement:Management:– Plain abdominal x ray- single grossly dilated Plain abdominal x ray- single grossly dilated
sigmoid loop often reaching the xiphisternumsigmoid loop often reaching the xiphisternum– An erect film- a characteristic” inverted U” of An erect film- a characteristic” inverted U” of
bowel gas in the upper abdomen with fluid bowel gas in the upper abdomen with fluid level at the same height in the two bowel limbs level at the same height in the two bowel limbs in the lower abdomenin the lower abdomen
– An abdominal lateral decubitus x ray may An abdominal lateral decubitus x ray may reveal two parallel fluid levels running the full reveal two parallel fluid levels running the full length of the abdomenlength of the abdomen




SIGMOID VOLVULUSSIGMOID VOLVULUS
ManagementManagement– Rectoscope is passed as far as possible Rectoscope is passed as far as possible
into the rectum and a flatus tube inserted into the rectum and a flatus tube inserted through itthrough it
– The end of the flatus tube is then gently The end of the flatus tube is then gently manipulated through the twisted bowel manipulated through the twisted bowel into the obstructed loopinto the obstructed loop
– If this is successful there is a gush of liquid If this is successful there is a gush of liquid feces and flatus relieving the obstructionfeces and flatus relieving the obstruction
– The flatus tube left in-situ for 24 hoursThe flatus tube left in-situ for 24 hours







SIGMOID VOLVULUSSIGMOID VOLVULUS
Acute large bowel obstruction- Acute large bowel obstruction- instant enema may define the lesioninstant enema may define the lesion
Persistent volvulus- urgent operationPersistent volvulus- urgent operation
Sigmoidectomy with colorectal Sigmoidectomy with colorectal anastomosis / Hartmann procedureanastomosis / Hartmann procedure
After a period of recovery following After a period of recovery following Hartmann op.- redo colorectal Hartmann op.- redo colorectal anastomosisanastomosis

DIVERTICULAR DISEASEDIVERTICULAR DISEASE
Common condition- chronic lack of Common condition- chronic lack of dietary fiberdietary fiber
Patients over 60 years of agePatients over 60 years of age
Female are more affectedFemale are more affected

DIVERTICULAR DISEASEDIVERTICULAR DISEASE
PathophysiologyPathophysiology– Chronic constipation- hypertrophy of the Chronic constipation- hypertrophy of the
colonic wall musclecolonic wall muscle– Increased intestinal pressure- pockets of Increased intestinal pressure- pockets of
mucosa herniating through weak points mucosa herniating through weak points in the bowel wallin the bowel wall
– Potential defects are where mucosal Potential defects are where mucosal blood vessels penetrate the wall from blood vessels penetrate the wall from outsideoutside




DIVERTICULAR DISEASEDIVERTICULAR DISEASESigmoid colon is most affectedSigmoid colon is most affected
Isolated diverticula- congenitalIsolated diverticula- congenital
Asymptomatic condition- diverticulosisAsymptomatic condition- diverticulosis
Complications:Complications:– Acute diverticulitisAcute diverticulitis– Pericolic abscessPericolic abscess– Fistula formationFistula formation– HematochesisHematochesis– Bowel obstruction: strictures, adhesionsBowel obstruction: strictures, adhesions

DIVERTICULAR PERFORATIONDIVERTICULAR PERFORATION
Diverticular abscess ruptures within Diverticular abscess ruptures within peritoneal cavity- fecal peritonitisperitoneal cavity- fecal peritonitisAcute abdomenAcute abdomenAbdominal X ray- pneumoperitoneumAbdominal X ray- pneumoperitoneumTreatmentTreatment– i.v.antibioticsi.v.antibiotics– Laparotomy, diversion of fecal stream Laparotomy, diversion of fecal stream
with resection of the affected bowel, with resection of the affected bowel, after 3 months, re-do anastomosisafter 3 months, re-do anastomosis



ACUTE INFLAMMATIONACUTE INFLAMMATIONMECKEL DIVERTICULUMMECKEL DIVERTICULUM

MECKEL’S DIVERTICULUMMECKEL’S DIVERTICULUMCommon congenital diverticulum on Common congenital diverticulum on the wall of the terminal small bowelthe wall of the terminal small bowelMay contain stomach or pancreatic May contain stomach or pancreatic tissuetissueComplications:Complications:– Diverticulitis, perforation, peritonitisDiverticulitis, perforation, peritonitis– GI bleeding- melenaGI bleeding- melena– Intussusception- bowel obstructionIntussusception- bowel obstructionSurgery- removal, enteroraphySurgery- removal, enteroraphy

MECKEL DIVERTICULUMMECKEL DIVERTICULUM

FISTULA FORMATIONFISTULA FORMATIONOccurs when an inflammed diverticulum Occurs when an inflammed diverticulum lies in close proximity to another hollow lies in close proximity to another hollow viscusviscusFistula formation:Fistula formation:– Colo- intestinal fistula- diarrheaColo- intestinal fistula- diarrhea– Colo-vesical fistula- pneumaturiaColo-vesical fistula- pneumaturia– Colo-vaginal fistula- fecal vaginal dischargeColo-vaginal fistula- fecal vaginal dischargeDifferential diagnosis- Crohn’s or tumoral fistulaDifferential diagnosis- Crohn’s or tumoral fistulaDiagnosis: endoscopy, barium enemaDiagnosis: endoscopy, barium enemaTreatment- excision of the affected segment of Treatment- excision of the affected segment of
bowelbowel

ACUTE RECTAL BLEEDINGACUTE RECTAL BLEEDING
HematocheziaHematochezia
Bleeding always stops spontaneouslyBleeding always stops spontaneously
Differential diagnosis- ischemic colitis, Differential diagnosis- ischemic colitis, carcinoma, pilescarcinoma, piles
Management- rarely surgicalManagement- rarely surgical
The patient is kept under observation, The patient is kept under observation, on conservative treatmenton conservative treatment
Check barium enemaCheck barium enema


BOWEL OBSTRUCTIONBOWEL OBSTRUCTION
Due to: acute inflamm. wall thickening Due to: acute inflamm. wall thickening muscle hypertrophy, bowel spasmmuscle hypertrophy, bowel spasm
Incomplete obstruction- more commonIncomplete obstruction- more common
Chronic diverticular inflammation- Chronic diverticular inflammation- fibrous bands, adhesionsfibrous bands, adhesions
Barium enema, colonoscopyBarium enema, colonoscopy
Treatment-segmental colectomyTreatment-segmental colectomy

CLINICAL PRESENTATIONCLINICAL PRESENTATIONDIVERTICULAR DISEASEDIVERTICULAR DISEASE
Chronic grumbling diverticular painChronic grumbling diverticular pain– Chronic pain and low-gradeChronic pain and low-grade– Erratic bowel habitErratic bowel habit– Mild iliac fossa tendernessMild iliac fossa tenderness– Abdo x ray- fecal loadingAbdo x ray- fecal loading– Barium enema- excludes malignancyBarium enema- excludes malignancy– Symptoms relieved by high fiber diet Symptoms relieved by high fiber diet
and bulking agentsand bulking agents

ACUTE DIVERTICULITISACUTE DIVERTICULITIS
Acute inflammation with local Acute inflammation with local extension to pericolic tissue and extension to pericolic tissue and parietal peritoneumparietal peritoneum
Continuous LIF painContinuous LIF pain
Fever, tachycardia, malaiseFever, tachycardia, malaise
Tenderness LIFTenderness LIF
Antibiotics against colonic flora: Antibiotics against colonic flora: cefalosporins, gentamycine, cefalosporins, gentamycine, metronidazolmetronidazol

PERICOLIC ABSCESSPERICOLIC ABSCESSPus formation following further extension Pus formation following further extension of acute inflammationof acute inflammationAntibiotics fail to resolve the problemAntibiotics fail to resolve the problemSwinging pyrexiaSwinging pyrexiaPersistent pain and tendernessPersistent pain and tendernessAbdominal distension- partial bowel Abdominal distension- partial bowel obstructionobstructionDiagnosis: USS, barium enemaDiagnosis: USS, barium enemaTreatment: bowel resection, Hartmann-Treatment: bowel resection, Hartmann-redo anastomosis laterredo anastomosis later

COMPLICATIONS OF COMPLICATIONS OF ILEOSTOMY AND COLOSTOMYILEOSTOMY AND COLOSTOMY
Early complicationsEarly complications– Mucosal necrosis due to ischemia- refashionMucosal necrosis due to ischemia- refashion– Obstruction of stoma due to edema of fecal Obstruction of stoma due to edema of fecal
impactionimpaction– Persistent leakage between skin and Persistent leakage between skin and
appliance- skin erosion and patient distressappliance- skin erosion and patient distress
Late complicationsLate complications– Prolapse of bowel-refashioning of stomaProlapse of bowel-refashioning of stoma– Parastomal hernia-resiting of stomaParastomal hernia-resiting of stoma– Retraction- refashioning of stomaRetraction- refashioning of stoma