
PowerofoneWinn0611handout - IPAC Canada · Bonuel N, et al. Crit Care Nurs Quart, 2009;32:144-148...
26
6/10/2011 1 The Power of One: Impacting Patient Outcomes by Returning to the Basics Basics Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING [email protected] Northville Michigan www.vollman.com Disclosures • Hill-Rom • Sage Products Speaker Bureau & Consultant • E.L. Lilly • Merck Session Objectives & Content • Prevention is key: IPH model • Define key care practices based on the evidence that can reduce bacterial load and/or prevent the development of health care acquired infections B i C it ti di td t • Basic Care interventions directed at: – Reducing MDRO’s – CLA-BSI – VAP/HAP – CA-UTI Quality & Safety Drivers Institute for Medicine Evidence based practice movement Quality organizations • Safer HealthCare Now (SHN) • Canadian Patient Safety Institute Q b C i T th lt i h lth ft • Quebec Campaign: Together, lets improve healthcare safety • Patients for Patient safety Canada • IHI/VHA:100,000 lives campaign /5 million lives campaign • Clean Care is Safer Care/WHO Regulatory agencies: • Accreditation Canada • Joint Commission Public transparency Professional Nursing: Back to the Basics Economics Why Source Control? Canada 220,000 HAI’s year/Canada 8000 deaths yearly USA 2.5 million HAI’s year/USA Everyday, 247 people die in the USA as a result of a HAI 5 10% f ll ti t d itt d t 8000 deaths yearly Total cost for 1 infected MRSA pt =$12,216.00 $12,000 to $35,000 5-10% of all patients admitted to US hospital annually contract HAI’s (1 of every 10-20 patients) 6 th leading cause of death in the US Higher nurse staffing results in lower HAI’s* *Hugonnet S et al CCM 2007;35:76-81 *Pronovost PJ et al JAMA 1999;281:1310-1317 *Needleman J et al. N Engl of Med 2002;346:1715-1722 WHO 2005 Yokoe DS, et al. Infect Control Hosp Epidemiol 2008;29:S12-S21 http://www.saferhealthcarenow.ca/EN/Interventions/aro_mrsa/Pages/d efault.aspx. Health Care Acquired Infection Data Measurement CNISP-PCSIN NHSN 2006-2008 1545 hospitals in US Staph aureus/VRE Resistance MRSA 1.93-2.19 56%/33% CLA-BSI/per 1000 cath days ICU Range: 1.6-7.6 Housewide: 8.9 Range of pooled means 1.3 (PICU)-5.5 (Burn ICU) VAP/per 1000 vent days ICU: 9.4 Range of pooled means ( C) ( C) 0.5 (RICU) -10.7 (Burn ICU) HAP/per 1000 patient days - 5-15 CA-UTI/per 1000 cath days 8.5 Range of pooled means 3.1 (Med-Surg ICU)-7.4 (Burn ICU) SSI/100 patient days 1.96 0.23 (Low risk GallBladder) – 26.6 (High risk Rectal Surgery) Rosenthal VD, et al. Am J of Infect Control, 2008;36:627-37 Edwards JR, et al. Am J of Infect Control, 2008;36:609-26 Hidron Ai, et al. Infect Control Hosp Epidemiol 2008; 29:996-1011 http://www.phac-aspc.gc.ca
Transcript of PowerofoneWinn0611handout - IPAC Canada · Bonuel N, et al. Crit Care Nurs Quart, 2009;32:144-148...

6/10/2011
1
The Power of One: Impacting Patient
Outcomes by Returning to the
BasicsBasics
Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAANClinical Nurse Specialist / Educator / Consultant
ADVANCING [email protected]
Northville Michiganwww.vollman.com
Disclosures
• Hill-Rom
• Sage Products Speaker Bureau p& Consultant
• E.L. Lilly
• Merck
Session Objectives & Content
• Prevention is key: IPH model
• Define key care practices based on the evidence that can reduce bacterial load and/or prevent the development of health care acquired infections
B i C i t ti di t d t• Basic Care interventions directed at:
– Reducing MDRO’s
– CLA-BSI
– VAP/HAP
– CA-UTI
Quality & Safety Drivers
Institute for Medicine Evidence based practice movement Quality organizations
• Safer HealthCare Now (SHN)• Canadian Patient Safety Institute
Q b C i T th l t i h lth f t• Quebec Campaign: Together, lets improve healthcare safety• Patients for Patient safety Canada• IHI/VHA:100,000 lives campaign /5 million lives campaign• Clean Care is Safer Care/WHO
Regulatory agencies:• Accreditation Canada• Joint Commission
Public transparency Professional Nursing: Back to the Basics Economics
Why Source Control?
Canada
220,000 HAI’s year/Canada
8000 deaths yearly
USA
2.5 million HAI’s year/USA
Everyday, 247 people die in the USA as a result of a HAI
5 10% f ll ti t d itt d t8000 deaths yearly
Total cost for 1 infected MRSA pt =$12,216.00
$12,000 to $35,000
5-10% of all patients admitted to US hospital annually contract HAI’s (1 of every 10-20 patients)
6th leading cause of death in the US
Higher nurse staffing results in lower HAI’s*
*Hugonnet S et al CCM 2007;35:76-81*Pronovost PJ et al JAMA 1999;281:1310-1317*Needleman J et al. N Engl of Med 2002;346:1715-1722
WHO 2005Yokoe DS, et al. Infect Control Hosp Epidemiol 2008;29:S12-S21http://www.saferhealthcarenow.ca/EN/Interventions/aro_mrsa/Pages/default.aspx.
Health Care Acquired Infection Data
Measurement CNISP-PCSIN NHSN 2006-20081545 hospitals in US
Staph aureus/VREResistance
MRSA 1.93-2.19 56%/33%
CLA-BSI/per 1000 cathdays
ICU Range: 1.6-7.6Housewide: 8.9
Range of pooled means1.3 (PICU)-5.5 (Burn ICU)
VAP/per 1000 vent days ICU: 9.4 Range of pooled means( C ) ( C )0.5 (RICU) -10.7 (Burn ICU)
HAP/per 1000 patient days
- 5-15
CA-UTI/per 1000 cathdays
8.5 Range of pooled means3.1 (Med-Surg ICU)-7.4 (Burn ICU)
SSI/100 patient days 1.96 0.23 (Low risk GallBladder) – 26.6 (High risk Rectal Surgery)
Rosenthal VD, et al. Am J of Infect Control, 2008;36:627-37Edwards JR, et al. Am J of Infect Control, 2008;36:609-26 Hidron Ai, et al. Infect Control Hosp Epidemiol 2008; 29:996-1011http://www.phac-aspc.gc.ca

6/10/2011
2
Financial Burden to the Canadian Health System
• The HAI financial burden to the health care system has been estimated by measuring a number of indices including increased:– number of readmissions to hospital
l th f t– length of stay
– use of antimicrobials
– surveillance and isolation measures for AROs
– laboratory and radiological services attributable to diagnosing and managing HAIs
– overall direct or indirect costs
– cost attributable to outbreaks
http://www.phac-aspc.gc.ca/nois-sinp/guide/ps-sp/partI-eng.php[6/10/2011 3:28:32 PM]
Factors Impacting HAI’s Programs
• Factors Associated with Lower HAI’s (30% reduction)– Integrated infection control
program
– Culture change
– Leadership/Champion
– Use of proven best practices
– HAI surveillance
Rosenthal VD, et al. Am J of Infect Control, 2008;36:el-12Bonuel N, et al. Crit Care Nurs Quart, 2009;32:144-148
Safer HealthCare Now & Quebec Campaign: Together, Lets Improve Healthcare Safety!
• April 2008
– Falls in long term care
– ADE in long term care
– NACS (New approach to controlling superbugs)CS ( e app oac to co t o g supe bugs)
– VTE
• 6 Initial Intervention 2005
– RRT
– AMI
– Medication reconciliation
– Prevent central line infection
– Prevent Ventilator-Associated pneumoniahttp://www.saferhealthcarenow.ca/
Notes on Hospitals: 1859
“It may seem a strange principle to enunciate as the very first requirement in a Hospital that it should do the sickin a Hospital that it should do the sick no harm.”
Florence Nightingale
Advocacy = Safety
Patient Advocacy/Safety Related to Clinical Practice
• Nurses knowledge of the evidence based care
• Ability to deliver the care to the right patient at the right time, every time it is needed
Th bilit t i t ti t i• The ability to communicate patient concerns in a concise, data driven manner and take appropriate action
• Understanding the chain of command when faced with resistance
Advocacy Starts with Us

6/10/2011
3
Achieving the Use of the Evidence
Attitude &
Accountability
Factors Impacting theability to Achieve QualityNursing Outcomesat the Point of Care
NSOValueVollman KM.
Australian Crit Care, 2009;22(4): 152-154
Protect The Patient From Bad Things
Happening on Your Watch
Interventional Patient Hygiene
• Hygiene…the science and practice of the establishment and maintenance of health
• Interventional Patient Hygiene….nursing action plan directly focused on fortifying the patients host defense through proactive use of evidence based hygiene care strategiesIncontinence Associated Dermatitis Prevention
Program
INTERVENTIONAL PATIENT HYGIENE(IPH)
Oral Care/ Mobility
VAP/HAP
HAND
Catheter Care
CA-UTI CA-BSI
Skin Care/ Bathing/Mobility
HASISSI
HYGIENE
Patient
Vollman KM. Australian Crit Care, 2009;22(4): 152-154
Reducing Environmental Load & Preventing Infection Through Creative &
Fundamental Care Strategies
Hand Hygiene Pre-op Prep Basinless BathingHand Hygiene, Pre op Prep, Basinless Bathing, CLA-BSI, CA-UTI
Hand Hygiene is the Single Most Important Factor in Preventing the Spread of
Infection

6/10/2011
4
WHO 1st Worldwide Patient Safety Campaign: Hand Hygiene
Pittet D. Infect Control Hosp Epidemiol, 2009;30(7):611-622
Factors Impacting HAI’s Programs
• Factors Associated with Lower HAI’s (30% reduction)– Integrated infection control
program
– Culture change
– Leadership/Champion
– Use of proven best practices
– HAI surveillance
Rosenthal VD, et al. Am J of Infect Control, 2008;36:el-12Bonuel N, et al. Crit Care Nurs Quart, 2009;32:144-148
Hand Washing Compliance
Findings: 1) Healthcare workers wash hands less
than 50% of time after direct patient contact.
2) Higher workload and activities of higher risk for transmission lower hand washing compliance
1981-2007 26 Years of Data/Research
Two models were created to simulate sequential patient contact by
2010 Researchq p y
non compliant hand hygiene worker Goal: To estimate the MRSA related cost of an incident of hand
hygiene non-compliance Results:
Model 1 42 MRSA infections, mean cost $47,092, mean cost per non-compliant event $1.98
Model 2 980 MRSA infections, mean cost $53,598, mean cost per non compliant $52.53
200 bed hospital incurs $1,779,283 in annual MRSA related expenses attributable to hand hygiene non-compliance
Cummings KL, et al. Infec Contol Hosp Epidemiol, 2010;31:357-364
WHO Hand Hygiene Tools 05/09
Alcohol-based Handrub Planning & Cost Tool
http://www.who.int/gpsc/5may/tools/system_change/en/index.html
Guidelines for Hand Hygiene in Health Care Settings
• If hands are not visibly soiled, use an alcohol-based hand rub for routinely decontaminating hands in all other clinical situations (1A)
• When hands visibly soiled or exposure to potential spore forming organisms, wash with either a non-antimicrobial or antimicrobial soap & water (IB)
• Decontaminate hands after removing gloves• When washing with soap & water, wet hands first, apply
soap, rub vigorously for 15 seconds, rinse and dry. Use towel to turn of faucet. (Duration 40 seconds)
• Provide HCW with hand lotions & creams to minimize occurrence of irritant contact dermatitis (IA)
• Use multidimensional strategies to improve hand hygiene practice (IA)
• Do not wear artificial fingernails or extenders (IA)
CDC. Hand Hygiene Guidelines: MMWR 2002; 51(No. RR-16):[1-45]WHO Hand Hygiene Guidelines 2009

6/10/2011
5
Reasons for Non-Compliance
• Lack of knowledge on importance and how the hands become contaminated
• Lack of understanding of correct techniqueq
• Understaffing and overcrowding• Poor access• Irritant contact dermatitis associated with
frequent exposure• Lack of institutional commitment to good hand
hygiene
Pittet D et al. Lancet Infect Dis. 2001;1:9-20
When to Wash
Pittet D. Infect Control Hosp Epidemiol, 2009;30(7):611-622http://www.saferhealthcarenow.ca/EN/HandHygiene/Pages/HandHygieneScholarlyLiterature.aspx
Correct use can reduce colony forming units by 90%, incorrect use only 60%. 1-3mL correct amount per HH episodeLausten S, et al. Infect Control Hosp Epidemio, 2008;29:954-956
Key Components to Multimodal Strategy to Improve Adherence
• Education & motivation & strong commitment to improve hand hygiene by frontline workers & leadership
• Engage staff/Positive deviance culture• Institutional safety climate
Si l & t d di• Simply & standardize• Alcohol-based hand rub as primary method for hand
hygiene….right product• Reminders in the workplace/red line approach• Verified by competency, monitored compliance and
feedback/weekly initiallyWHO Guidelines 2009Pittet D. Infect Control & Hosp Epidemio, 2008;29:957-959Sax, H., et. al. Infection Control and Hospital Epidemiology 2009, 28, 1267-1274Erasmus, V. et. Infection Control and Hospital Epidemiology.2009 30(5), 415-419Bonuel N, et al. Critical Care Nursing Quarterly, 2009;32:144-148
Measurement: Know Your Direction
• Policies and guidelines will not increase hand hygiene compliance unless measurement and feedback are part of the process…Make it Visible
www.hhreports.comQuinn B, presented at NACNS 2011
Hand Hygiene Measurement Methods
• Direct Observation
• HCW Self-reporting
• Product Usage/Volume
• Automation monitoring can improve compliance
www.hhreports.comHaas and Larson Journal of Hospital Infection 2007;66:6-14Polgreen PM, et al. Infect Control & Hosp Epidemiol, 2010;31:1294-1297
Increase use of alcohol hand rub (measure by volume use) correlated significantly (p=0.014) with improvement in MRSA rates
Sroka S, et al. J of Hosp Infect, 2010;74:704-211

6/10/2011
6
Improved & Correctly Performed Hand Hygiene Can Lower HAI’s
Effective Hand Hygiene
33% lower antibiotic resistance over time
Reduced CLA BSI’s from 3 9 to 1 0 per Reduced CLA-BSI’s from 3.9 to 1.0 per 1000 catheter days
Trick et al. Infec Control Hosp Epidemiol, 2007;25:42-9
Zingg W, et al. Crit Care Med, 2009;37:2167-2173Webster J, et Journal of Paediatric Child Health,1994, 30:59-64.
Five Key Interventions
1. Hand hygiene2. Decontamination of the environment
and equipment…?people3 Active surveillance cultures (ASCs)3. Active surveillance cultures (ASCs)4. Contact precautions for infected and
colonized patients5. Compliance with Central Venous
Catheter and Ventilator Bundles
www.ihi.org
Environmental Contamination as a Source of Health Care Acquired Pathogens
Pathogen Survival Data Transmission Settings
C. difficile Months 3+ Healthcare facilities
MRSA d-weeks 3+ Burn units
VRE d k 3 H lth f ilitiVRE d-weeks 3+ Healthcare facilities
Acinetobacter 33 d 2/3+ ICUs
P. aeruginosa 7 h 1+ Wet environments
Hota B, Clin Inf Dis 2004; 39(8):1182-9Stiefel U et al. Infect control & Hosp Epidemiol 2011;32:185-187.
Hands equally become contaminated from commonly examined skin sites & environmental surfaces
Application of Recommendations for Environmental Cleaning
• Resources to ensure effective cleaning and decontamination– Use of a check list– Clean equipment that is transported from room to room
Dedicated equipment in isolation rooms– Dedicated equipment in isolation rooms– Reduce load– Education of healthcare workers and support staff
• Change from use of a pour bottle to bucket immersion for applying disinfectant to cleaning cloth
• Feedback method using removal of intentional applied marks visible only under UV light
Boyce JM et al Infec Control Hosp Epidemiol. 1997;18:62-627Huang SS, et al. Arch Intern Med 2006;166(18):1945-1951
• Pre-intervention rooms occupied by MRSA carrier had new acquisition increase from 2.9% to 3.9%
• Post Intervention: 1.5% (Datta R. Arch Intern Med 2011;17:491-494)
Improved Cleaning Reduces VRE Transmission
Routine cleaning reduces VRE transmission by 60%
Segers et al. JAMA, 2006;296:240-246
Improving Environmental Hygiene In 27 ICU’s Decreased MDRO Transmission
• 27 acute care hospitals ( 25 beds to 709 beds)• Fluorescent targeting method used to objectively
evaluate the thoroughness of terminal room cleaning before and after a structured educational, procedural and administrative interventionsinterventions
• Systematic covert monitoring was performedResults:• 3532 environmental surfaces were assessed
after terminal cleaning in 260 ICU unit rooms• 49.5% of services cleaned it baseline• Post-intervention with multiple cycles of
objective performance feedback resulted in 82% of environmental services cleaned (p < .0001)
Carling PC, et al. Crit Care Med, 2010;38:1054-1059

6/10/2011
7
REDUCING THE BACTERIAL LOAD ON THEBACTERIAL LOAD ON THE
PATIENT: IMPACT ON MRSA/MDRO
nurWse!
Traditional BathingWhy are there so many bugs
in here?
Spreading Microorganism
Bath Water: A Source of Health-Care Associated Microbiological Contamination
• Compared normal bath water with chlorhexidine bath water on 3 wards
• Without Chlorhexidine: All samples + for bacterial growth (14/23 > 105 cfu/ml)bacterial growth (14/23 > 105 cfu/ml)
• With Chlorhexidine: 5/32 grew bacteria with growth 240 to 1900 cfu/ml
• Gloved hands/bathing: objects touch grew significant numbers of bacteria
Shannon RJ. et.al. Journal of Health Care, Compliance & Safety Control. 1999;3(4):180-184
Bath Basins: Potential Source of Infection
• Multicenter sampling study (3 ICU’s) of 92 bath basins
• Identify & quantify bacteria in patients basins
• Sampling done on basins used > 2x in patients hospitalized > 48 hours & preformed 2 hours post bath
• Cultures sent to outside laboratory
• Qualitative vs. quantitative measures used to exclude growth that may have occurred in transport
• Bathing practices not controlled & no antiseptic soaps used to bathe
Johnson D, et al. Am J of Crit Care, 2009;18:31-40
Bath Basins: Potential Source of Infection
• Results– 98% of all cultures grew some form of
bacteria after plating or enrichment
• Enrichment ResultsEnrichment Results– 54% enterococci. 32% for gram -, 23%
for S aureus and 13% VRE (statistically significant)
– <10% growth rates for: MRSA 8%, P aeruginosa 5%, C albicans 3% & E coli 2%
Johnson D, et al. Am J of Crit Care, 2009;18:31-40
Large Multi-Center Basin Evaluation For Presence of MDRO’s
• 53 US & Canadian Hospitals
• Randomly selected basins for damp swab culture
• Central lab tested for MRSA & VRE & gram – bacilli
Methodology
• Central lab tested for MRSA & VRE & gram – bacilli
• All basins were clean & were not visibly soiled
Results:• 199 basins (34.6%) from 52 hospitals were colonized with VRE• 251 basins (43.6% from 47 hospitals had gram-negative bacilli• 24 basins (4.2%) from 19 hospitals had MRSA
Kaye, et al. Presented at SCCM January2011

6/10/2011
8
Waterborne Infections Study
• Hospital tap water is the most overlooked source for Health-care associated pathogens
29 evidenced based studies present• 29 evidenced-based studies present solid evidence of waterborne Health-care associated infections
• Transmission occurs via drinking, bathing, items rinsed with tap water and contaminated environmental surfaces
Anaissie E. et. al. Arch Int Med. 2002; 162:1483-92
Waterborne Infections Study
• Conservative estimates suggest significant morbidity and mortality from waterborne pathogens
Immunocompromised patients are at the• Immunocompromised patients are at the greatest risk
• Recommendation I: Minimize patient exposure to hospital tap water via bottled water and pre-packaged, disposable bathing sponges
Anaissie E. et. al. Arch Int Med. 2002; 162:1483-92
Bacteria Biofilm
• Organized communities of viable & non-viable microorganisms protected within a matrix of extracellular polysaccharides, nutrients & entrained particles
• Adhere to inert material (plumbing)
• Bacteria contain within Biofilm may be transmitted to at risk patients by direct contact with water used for ingestion, ice, washing
Cervia JS, et al. Arch Intern Med, 2007;167:92-93
ICU & Hospital Water Samples
• Systematic review published studies 1998-2005 (29 studies)– 9.7%-68.1% of random ICU water samples + for
Pseudomonas aeruginosag
– 14.2%-50% of patient infections were due to genotypes found in ICU water
• 9 hospital in New York city– Bacteria recovered in every hospital
– 4-14 species identified
– 1/3 organism known to be responsible for HAI’s
Trautmann M, et al. Am J of Infect Control, 2005;33(5):S41-S49, Cervia JS, et al. Arch Intern Med, 2007;167:92-93
Pre-Op Prep
• Antisepsis must demonstrate a 3.0 log 10 from baseline in groin, 2.0 10 log reduction on the abdomen and maintain effectiveness for minimum of 6 hrs.
• CHG shower/bathing versus soap & water showed no difference in SSI (Cochrane EBR: 2007:CD004985)
• 2% prep cloth more effective in reducing bacterial load• 2% prep cloth more effective in reducing bacterial load than 4% CHG solution that must be rinsed off/Inguinal sites sustained action at 10min, 30 min, 6 hrs > than 4% (Edmiston CE. Et al AJIC, 2007;35:89-96)
• CDC recommends must bathe or shower night before– Compliance issues, consistency in application, unable to
bathe self
• Chlorhexidine is absorbed onto fibers of certain fabrics, particularly cotton (Denton GW. Chlorhexidine. In Block S, ed. Disinfection, Sterilization and preservation, 4th ed. Philadelphia: Lea & Febiger, 1991:274-89)
Innovative Strategy: Study Re-examine Pre-op Prep
• Methodology– Observational study with a pre & post intervention period– Baseline: Actively part of National SCIP program– Pre-intervention pre-op prep was night before in home
showering or washing with 4% CHG solution– Post intervention: Pre-op prep preformed with a pre-
packaged 2% CHG prep product with instructions on its use
– Pre-package prep preformed at hospital prior to surgery– Measured:
• Change in baseline SSI would occur with new prep process
• Cost savings
Harris H et al Infection Control Today. March 2008: www.infecctioncontroltoday.com

6/10/2011
9
Innovative Strategy: Case Study Re-examine Pre-op Prep
• Results: – 25 SSI’s during
historical period out of 5174 procedures (rate of 2 1%)(rate of 2.1%)
– 11 SSI’s during interventional period out of 4266 procedure(rate 0 .7%)
Harris H et al Infection Control Today. March 2008: www.infecctioncontroltoday.com
72% Difference
Innovative Strategy: Case Study Re-examine Pre-op Prep
• Cost Savings Results: – Before intervention:
$648,471 for SSI’s
– After intervention: $290,827
– Cost of product: $8,721
– Readmission savings: $177,937
Harris H et al Infection Control Today. March 2008: www.infecctioncontroltoday.com
Total Savings$526,860.00
Safer Health Care Now: Pre-Op Surgical Prep
• RECOMMENDATION:– Based on the evidence, the Safer Healthcare Now! SSI faculty
recommend that:
– The skin should be cleansed before surgery with a chorhexidine–based solution,
– Preferably with no rinse disposable chlorhexidine gluconateimpregnated wash cloths.
– Chlorhexidine is well tolerated and has shown a low incidence of hypersensitivity and skin irritation
Bathing with CHG Basinless Cloths
• Prospective sequential group single arm clinical trial
• 1787 patients bathedp
– Period 1: soap & water
– Period 2: CHG basinless cloth bath
– Period 3: non-medicated basinless cloth bath
Veron MO et al. Archives Internal Med 2006;166:306-312
Veron MO et al. Archives Internal Med 2006;166:306-312
26 colonization's with VRE per 1000 patients days vs. 9 colonization's per 1000 patient days with CHG bath
Veron MO et al. Archives Internal Med 2006;166:306-312
6/10/2011
10
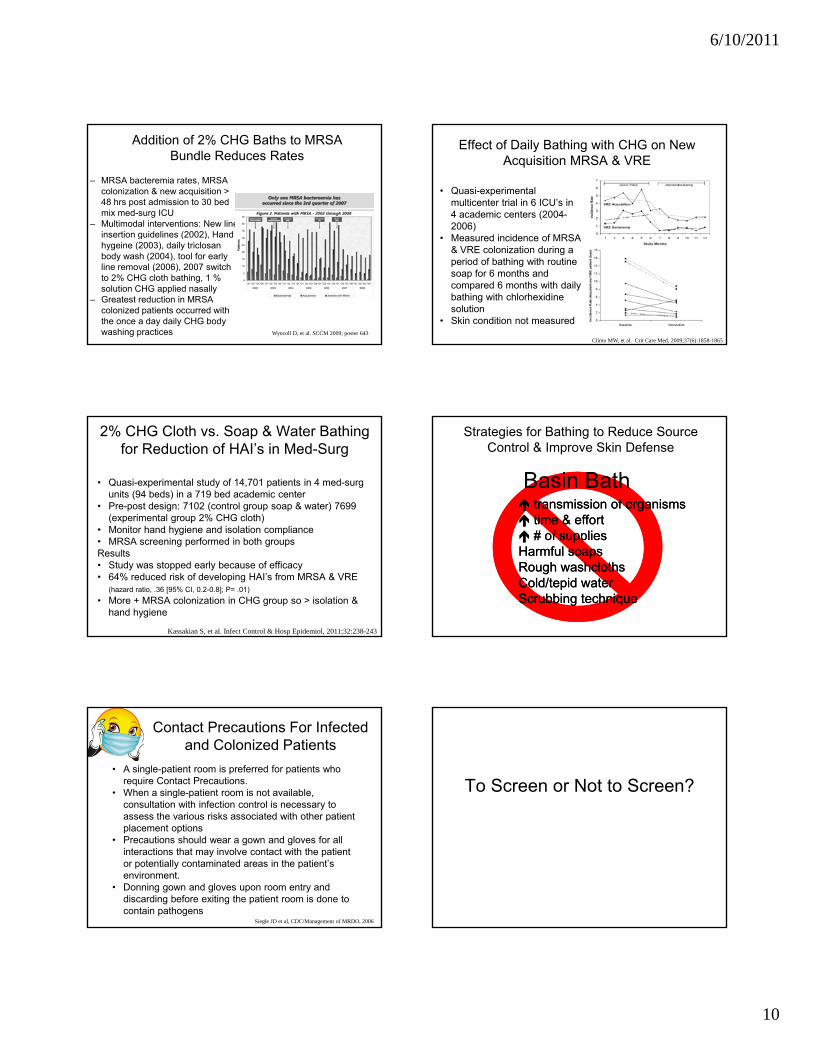
Addition of 2% CHG Baths to MRSA Bundle Reduces Rates
– MRSA bacteremia rates, MRSA colonization & new acquisition > 48 hrs post admission to 30 bed mix med-surg ICU
– Multimodal interventions: New line insertion guidelines (2002) Handinsertion guidelines (2002), Hand hygeine (2003), daily triclosan body wash (2004), tool for early line removal (2006), 2007 switch to 2% CHG cloth bathing, 1 % solution CHG applied nasally
– Greatest reduction in MRSA colonized patients occurred with the once a day daily CHG body washing practices Wyncoll D, et al. SCCM 2009; poster 643
Effect of Daily Bathing with CHG on New Acquisition MRSA & VRE
• Quasi-experimental multicenter trial in 6 ICU’s in 4 academic centers (2004-2006)M d i id f MRSA• Measured incidence of MRSA & VRE colonization during a period of bathing with routine soap for 6 months and compared 6 months with daily bathing with chlorhexidine solution
• Skin condition not measured
Climo MW, et al. Crit Care Med, 2009;37(6):1858-1865
2% CHG Cloth vs. Soap & Water Bathing for Reduction of HAI’s in Med-Surg
• Quasi-experimental study of 14,701 patients in 4 med-surg units (94 beds) in a 719 bed academic center
• Pre-post design: 7102 (control group soap & water) 7699 (experimental group 2% CHG cloth)M it h d h i d i l ti li• Monitor hand hygiene and isolation compliance
• MRSA screening performed in both groupsResults• Study was stopped early because of efficacy• 64% reduced risk of developing HAI’s from MRSA & VRE
(hazard ratio, .36 [95% CI, 0.2-0.8]; P= .01)
• More + MRSA colonization in CHG group so > isolation & hand hygiene
Kassakian S, et al. Infect Control & Hosp Epidemiol, 2011;32:238-243
Basin Bath
Strategies for Bathing to Reduce Source Control & Improve Skin Defense
transmission of organismstransmission of organisms time & efforttime & effort # of supplies# of suppliesHarmful soapsHarmful soapsRough washclothsRough washclothsCold/tepid waterCold/tepid waterScrubbing techniqueScrubbing technique
Contact Precautions For Infected and Colonized Patients
• A single-patient room is preferred for patients who require Contact Precautions.
• When a single-patient room is not available, consultation with infection control is necessary to assess the various risks associated with other patientassess the various risks associated with other patient placement options
• Precautions should wear a gown and gloves for all interactions that may involve contact with the patient or potentially contaminated areas in the patient’s environment.
• Donning gown and gloves upon room entry and discarding before exiting the patient room is done to contain pathogens
Siegle JD et al, CDC/Management of MRDO, 2006
To Screen or Not to Screen?

6/10/2011
11
Active Surveillance
• Begin with admission cultures only.– Measure compliance; add the second culture when high (>
90%).– ASCs of the anterior nares capture 80% of colonized adults– ASC’s of the anterior nares & wounds capture 92% of
colonized adultscolonized adults– Screen high risk
• Provide real-time notification of positive admission culture./PCR testing used as screening tool vs. dx
• Schedule consistent day of week for second culture.• Measure transmission.
– Number or rate of patients who convert from negative to positive
• Flag colonized patients when discharged.Yokoe DS, et al. Infect Control Hosp Epidemiol 2008;29:S12-S21www.IHI.org
To Screen or Not to Screen?
• Clustered RCT of 9000 cases between 2005 & 2006• Evaluated the effect of surveillance for MRSA & VRE
colonization & expanded used of barrier precautions compared with existing practice on incidence of MRSA & VRE infection
• Intervention group: 92% of ICU days either contact or universal, Control group: 38% of ICU days (p<0.001)
• In intervention group: When contact precautions specified; gloves used median of 82%, gown 77% and hand hygiene 69%
• No difference in colonization & infection rates between ICU’s that tested/screened patients & expanded precaution vs. those that did not
Huskins WC, et al. N Engl J Med. 2011;364(15):1407-18
To Treat or Not To Treat for Carriage
• Systematic review of clinical trials to determine effectiveness of different approaches for eradicating MRSA carriage (especially pts with elective surgery)– Uncomplicated cases, short-term nasal application of mupiricin
remains the most effective treatment for advocating MRSA carriageremains the most effective treatment for advocating MRSA carriage
– 90% success rate post one week after treatment
– 60% success rate in longer follow-up
• S aureus carriers randomized to receive Mupiricin and skin washing with CHG or placebo– Tx group demonstrated significantly lower S aureus infection rates
(RR 0.42 [95% CI, 0.23-0.75] & shorter LOS (1.8 days, p=.04)
Van Rijen M, et al. Cochrane Database Sys Rev 2008;4:CD006216Ammerlaan HS, et al. Clin Infect Dis, 2009;48922-930
All or NoneVentilator
Associated Pneumonia
The Vent Bundle…To the VAP Bundle
• Applying evidence-based practice• 5 activities that when done 100% of the time has
shown a reduction in– VAP
LOS
Nurse-intervention bundle demonstrated a 55.4% reduction in the incidence of VAP
– LOS– Time on Vent– Cost
• HOB 30°, Peptic Ulcer Disease (PUD) prophylaxis, DVT prophylaxis, Sedation vacation, Daily assessment for SBT/ & Oral Care with antisepticModification Mobility, EVAC tube, OG vs. NGT
• Maintaining ET tube cuff pressure between 20-25cm H2O• Keeping HOB elevated 30 to 45°• Providing oral care every 2-4 hours
Curtin LJ. American Nurse Today, March 2011
European VAP Bundle
• No ventilator circuit change unless specifically indicated
• Alcohol based hand h ihygiene
• Appropriately educated and trained staff
• Incorporation of sedation and weaning protocols
• Oral care with CHG Rello J, et al. Intensive Care Medicine, 2010;36:773-780

6/10/2011
12
Canada Ventilator-Associated Pneumonia(VAP)
• Incidence of VAP 10.6 cases per 1000 ventilator days• Estimated 4000 cases per year• 230 deaths (0 - 580 range)
Att ib t bl t lit 5 8%• Attributable mortality 5.8%• Accounts for 17,000 ICU days per year/2% of all ICU
days• Associated cost $30,000-$40,000 per VAP/minimiun
cost savings to system $14,000• Increase LOS 4.3 days per episode• Annual cost $46 million (10 to 82 million) per year
Muscedere JG. Et al. J of Crit Care, 2008;23:5-10
Healthcare Acquired Pneumonia
• Risk Factor Categories– Factors that increase
bacterial burden or colonization
– Factors that increase risk of aspiration
Factors that Increase Bacterial Burden or Colonization
Extreme age, severe underlying condition/ immunosuppression
Administration of
Suctioning/Saline administration
Lack of oral care Administration of
antibiotics
Agents which raise the gastric pH
Withholding gastric feeding
Mechanical ventilation
Poor infection control practices
Contaminated respiratory equipment/contaminated condensate
Immobility
Oropharyngeal Colonization
• 89 critically ill patients
• Examined microbial colonization of the oropharynx through out ICU stay
Methodology:
• Used pulse field gel electrophoresis to compare chromosomal DNA
Garrouste-Orgeas et. al. Am J Respir Crit Care Med. 1997;156:1647-1655
Results:
• Diagnosed 31 VAPs• 28 of 31 VAP’s the causative organism was
identical via DNA analysis
Dental Plaque
• 49 elderly nursing home residents admitted to the hospital
• Examined baseline dental plaque scores &
Methodology:
microorganism within dental plaque
• Used pulse field gel electrophoresis to compare chromosomal DNA
El-Solh AA. Chest. 2004;126:1575-1582
Results:
• 14/49 adults developed pneumonia• 10 of 14 pneumonias, the causative organism was identical via DNA analysis

6/10/2011
13
Role of Salivary Flow
• Provides mechanical removal of plaque and microorganisms
• Innate & specific immune components (IgA, cortisol,components (IgA, cortisol, lactoferrin)
• Patients receiving mechanical ventilation have dry mouth which in turn contributes to accumulation of plaque & reduced distribution of salivary immune factors
Munro CL & Grap MJ. AJCC. 2004;13:25-34
Endotracheal / Nasogastric Tube/ Sinusitis
• Carriage of oropharyngeal bacteria during intubation• If cuff pressure < 20 cm 4x risk VAP• Cuff pressure range btwn 25-40cm (JBI-Level A) with
maintenance at 25cm-30cm of H2O pressure.– Continuous monitoring resulted in a lower portion of out of range cuff
pressure (11% vs. 51.7% p< 0.001)
• NGT increases risk of sinusitis/gastric reflux & increases oropharyngeal colonization
• Use oral ET versus nasal (CDC-Cat IB)• Sinusitis increases the risk of nosocomial pneumonia by 3
foldCDC. 2003 Guidelines for Prevention of Healthcare Associated Pneumonia; MMWR; 2004:53(no RR-3)Davis KA. J Intensive care Med, 2006;21(4):211-226Muscedere J & Canadian Trails Group. J of Crit Care, 2008;23:126-137Carstens J. Joanna Briggs Institute, 2010Sole, ML, et al. AJCC, 2011;20:109-117
BrushCHX i lCHX rinse alone
CHX rinse in CombinationSwab/Clean/Moisturize
Suction
All of the above
BRUSH & SWAB
• 77% more clean approximal sites with brushing
• 44% more clean crevice sites with brushing
• Benefit of brushing is directly correlated with• Benefit of brushing is directly correlated with technique
• Foam swabs could not remove plaque from sheltered areas on or between teeth
Pearson LS. et. al. J of Adv Nursing. 2002;39(5):480-489
Oral Care Reduces Pneumonia In Nursing Homes
11 nursing homes in Japan over 2 year period 417 enrolled / 366 residents analyzed (death
from other causes) 184 recei ed oral care program/182 did not
Methodology
184 received oral care program/182 did not Tooth brushing after each meal (teeth or
dentures) & 1x weekly review by dentist/or hygienist
Results
No OralNo Oral Oral CareOral Care p valuep value
FebrileFebrile 29%29% 15%15% p<.01p<.01
PneumoniaPneumonia 19%19% 11%11% p<.05p<.05
DeathDeath 16%16% 7%7% p<.01p<.01
MMSEMMSE IncreaseIncrease p<.05p<.05Yoneyama et al. JAGS. 2002;50:430-433
Solutions H2 O2
EBR: CHG; grade B evidence, Sodium Bicarb; unresolved, H2O2; unresolved, Salt solutions; unresolved; Tap water; not recommended, Sterile water; unresolved. (Berry AM et al. AJCC, 2007;16:552-563)
Review of Dental Literature Not Included

6/10/2011
14
H2 O2, Cetylpyridium Chloride (CPC) & Biotene
• >3% may cause harm, <1% no benefit in plaque removal.• Must be diluted properly, not with normal saline.• 3x a day mouth rinse with 1.5% H2 02 revealed no
mucosal damage, improved plaque scores and overall
H2O2
gingival health.
West TL et. al. Journal of Peridontol. 1983; 54(6):339Tombes MA et. al. Nursing Research. 1993; 42(6):332-337Beck S. Cancer Nursing. 1979; 2:185-189.
Gunsolley JC.J Am Dent Assoc 2006;137(12):1649-57Gomes BC et.al. Clin Prev Dentistry. 1984; 6:21-25Boyd RL. et. al. J Clin Periodentol.1989; 16:557-563
CPC• Cetylpyridium chloride had significant antigingivitis
effects in several individual studies• Used in some over the counter plaque reduction rinses (Crest rins
Biotene• Contains salivary enzymes• Moisturize, Some oral care kits
Recent Trials Reduction in VAP or Colonization with CHG or Povidone-iodine
• 2004: Grap (CHG via swab) • 2005: Fourier (CHG) (negative trial)• 2006: Koeman (CHG or CHG/colistin)
2006 M (CHG i b & t thb i )• 2006: Munro (CHG via swab & toothbrusing)• 2006: Sequin (povidone-iodine)• 2006: Mori (povidone-iodine)• 2008: Tantipong (CHG)2009, Sona (CHG)2009, Panchabhai (CHG)—no decrease
Oral Decontamination for the Prevention of Pneumonia in Mechanically Ventilated Patients:
Systematic Review and Meta Analysis
Meta Analysis• 298 articles screened• 11randomized controlled
trials used• 3242 patients
Chan EY, et al. BMJ, 2007;334:889
• 4 trails (1098 pts) no significant difference with oral antibiotics
• 7 trials (2144 pts) Oral application of antiseptics significantly reduced VAP rates
• No decrease in Mortality, mechanical ventilation or LOS
Comprehensive Oral Care Program
Comprehensive Oral Care Protocol: The Good Shepherd Study
Methodology:• Retrospective study 10 bed Med-Surg• Protocol included: Covered Yankauer for
non-traumatic oral suctioning, soft-suction t thb h S ti O l S b ftoothbrush, Suction Oral Swab, use of a 1.5% H2O2 peroxide mouth rinse for cleansing, subglottic suction catheter used 4x daily, dedicated oral suction line for infection control and ease of use.
• Education provided and presence of clinical champion.
Schleder B. et al. J Advocate Health 2002;4(1):27-30
Literature Review: Oral Care Impact of VAP
Comprehensive Oral Care:• Reduction in VAP from 5.6 to 2.2 (Schleder B. et al.
J Advocate Health 2002;4(1):27-30)• Reduction in VAP from 4.10 (2005) to (2.15) in 2006
with addition of CPC & comprehensive oral carewith addition of CPC & comprehensive oral care. Vent bundle & rotational therapy already being performed
• Reduction in VAP from 12.0 to 8.0 (p=.060) with 80% compliance, vent bundle already being preformed, 1538 patients randomized to control or study group, Additional outcomes; vent days (p=.05), ICU LOS (p=.05) time to VAP (p= <.001) & reduction in mortality (p=.05) (Garcia R et alAJCC, 2009;18:523-534)

6/10/2011
15
Literature Review: Oral Care Impact of VAP
Comprehensive Oral Care & CHG:• Reduction in VAP to zero for 2 years, vent bundle, mobility, oral care
& CHG with comprehensive education preformed (Murray TM et al. AACN Advanced Critical Care. 2007;18(2):190-199)
Dickinson S et al. SCCM Critical Connections, 02/2008
Comprehensive oral care with CHG
Heck K, et al. Presented at APIC 7/15/2010
Dental Brushing for Preventing VAP
• Prospective, simple blind, randomized trial of adult patients incubated for > 48 hours
• Randomized to oral care every eight hours with .12% CHG applied by gauze after suctioning oral
ti d √ ff ( t d d)secretions and √ cuff pressures (standard) or standard oral care plus electric toothbrushing
Results• Terminated after randomizing hundred 47 patients• No difference in VAP, mortality antibiotics three days
duration mechanical ventilation or hospital ICU length of stay in the two groups
Pobo A, et al. Chest, 2009;136:433-439
Oral Suctioning with Position Change
• Prospective time sequenced non-randomized study– 237 control (observation phase 9 months)
– 227 Interventional (7 months interventional)
– Difference in nursing protocol was oral suctioning prior to position change (11 additional suctions)position change (11 additional suctions)
– All other nursing care the same
• Results: – VAP: 6.51 to 2.04 per 1000 ventilator days ( p<0.002 )
– Vent days: 28.8 + 17.2 vs. 20.2 + 4.0 (p <0.009)
– ICU LOS: 27.6 + 17 vs. 20.3 + 4.0 (p < 0.012)
– Suctioning before positional change only independent factor responsible for VAP decrease (p=0.003)
Tsai, HH, et al. Am J of Med Sci, 2008;336;397-401
Does Compliance Make A Difference?
Oral care compliance & use of the ventilator bundle resulted in a 89.7% reduction in VAP
Hutchins K, et al. Am J Infect Control 2009;37:590-7
Subglottic Secretion Drainage
Risk of VAP
Mortality
5 level 2 trials conclude that subglottic secretion drainage is associated with a reduction in VAP
Dezfulian C. et al. Am J of Med, 2005;118,11-18
Mortality
Risk of Early VAP
drainage is associated with a reduction in VAPMuscedere J & Canadian Trials Group. J of Crit Care, 2008;23:126-137
Silver Impregnated Endotracheal Tube
• Endotracheal tube cuff that prevents leakage through a re-design
• Impregnated endotracheal tube that minimize the bacteria biofilm
• A phase III multicenter, prospective, randomized, controlled t i l d t t d i ifi t d ti f i bi l i lltrial demonstrated a significant reduction of microbiologically documented– VAP (4.8% in the silver group vs. 7.5% in the control
group, p < 0.05)• Cost effective analysis: Silver coated tube yielded $9,630 to
$16,356 per case of VAP prevented.• Retrospective examination suggests that the silver-coated
ETT may be associated with a reduce mortality in pts with VAP Kollef MH, et al. JAMA, 2008;300:805-814
Shorr AF, et al. Infect Control Hosp Epidemiol, 2009;30:759-763Afessa B, et al. Chesst, 2010;137:1015-1021

6/10/2011
16
1 2
3 4
Trauma unit targeted 16 in 24 hrs for HOB > 30 degrees & VAP rates from 4.0 to 1.0Laux L, et al. Crit Care Nurs Q, 2010;33:126-131
HOB Research
• 86 patients
• Randomly assigned to supine position or HOB 45 degrees (39 semi recumbent, 47 supine)
• Monitored clinical suspected & microbiologically
Methodology:
Monitored clinical suspected & microbiologically confirmed nosocomial pneumonias
Drakulovic MB. et. al. Lancet. 1999;354:1851-1858
Results:• Microbiologically confirmed nosocomial pneumonia
lower in the semi recumbent group 2/39 (5%) vs. 11/47 (23%)
• Supine position & enteral nutrition were independent risk factors for VAP & had the greatest number of VAP’s 14/28 (50%)
HOB Research
• Methodology– Prospective multicenter trial randomly assigned to targeted
45° vs.10° HOB– 112 to targeted 45° vs. 109 patients to 10°– Continuous measurement of backrest elevation first wk of
MVMV– Dx of VAP by bronchoscopic techniques
• Results– Baseline characteristics similar– Average elevations
• 10° group day 1 & 7: 9.8 & 16.1 • 45° group day 1 & 7: 28.1 & 22.6*
– Target 45° not achieved 85% of the time– VAP: 10° = 6.5% vs. 45° = 10.7%
Van NieuwenhovenCA, et al. Crit Care Med, 2006;34:396-402*p < .001
Goldhill DR et al. Amer J Crit Care, 2007;16:50-62Xue Y. Joanna Briggs Institute 2010
CLRT to Prevent VAP
• Prospective randomized controlled trial, 3 medical ICUs at a single center
• Eligible if ventilated < 48 hours & free from pneumonia, ALI or in ARDS
• 150 patients with 75 in each group
Methodology
• 150 patients with 75 in each group• 35 CLRT patients allocated to undergo percussion before
suctioning• Measures to prevent VAP were standardized for both groups
including HOB
Results: CLRT vs. Control• VAP: 11% vs. 23% p = .048• Ventilation duration: 8 + 5 days vs. 14 + 23 days, p = .02• LOS: 25 + 22 vs. 39 + 45 days, p = .01• Mortality: no difference Staudinger t, et al. Crit Care Med, 2010;38:486-490

6/10/2011
17
Ventilator Circuit Change
Hess DR et al, Respir Care 2003;48(9):869-879
Heat-Wired Exchange
Kola A. Intensive Care Med, 2005;31(1):5-11.
Effect of CHG Cloth Bath of HAI’s in Trauma Patients
• Retrospective analysis 6 months before and after institution of CHG bathing
• 12 bed level 1 trauma center– 286 severely injured patients y j p
bathes 2% CHG cloth– 253 severely injured patients
bathed without CHG cloth• Results: CHG bathed patients less
likely to acquire a CLA BSI (2.1-vs. 8.4), MRSA VAP 1.6 vs. 5.7 & rate of colonization was significantly lowers; 23.2 vs.69.4 per 1000 patient days
Evans HL, et al. Arch Surg, 2010;145:240-246
• 112 ICU’s from 72 hospitals reported data
• Examine 550,800 ventilator days
• Implementation of the CUSP/VAP Bundle/checklist
• Results: 71% in VAP rates in MI
Intervention to Decrease VAPStatewide Collaborative-Keystone ICU
– Median rate of VAP per 1000 vent days went 5.5 cases to 0 0 at 16-18 months (p<0.001) & 0 at 28-30 months (p<.001)
– Mean rate of VAP per 1000 vent days went 6.9 to 3.4 at 16-18 month follow up (p<0.001) & 2.4 at 28 to 30 months (p<.001)
– Composite compliance measured from 32% at baseline, 75% at 18 months & 84% at 28 months
– Inclusion of oral care was not measured
Berenholtz SM, et al. Infect Control Hosp Epidemiol, 2011;32:305-314
Comprehensive Evidence-Based Clinical Practice Guidelines: Prevention
• Recommend– Oral intubation route– New vent circuit for each
patient– Circuit change if soiled or
• Consider– Rotational therapy– Oral antiseptic rinses
• Not recommended– Bacterial filtersg
damaged– Change HME q 7days– Use of closed suction,
changed each patient and clinically indicated
– Subglottic drainage if expected >72 ventilation
– HOB 45 (when impossible as near)
– Use of iseganan
• No recommendations made– Use of systematic search for
sinusitis, aerosolized antibiotics, intranasal mupirocin
– Type of airway humidification– Timing of trach– Prone positioning
Muscedere J & Canadian Trails Group. J of Crit Care, 2008;23:126-13
Central Line -Associated Blood St I f tiStream Infections

6/10/2011
18
• Remove/Avoid unnecessary lines (IA)
• Hand hygiene (IB)
• Maximal barrier (IB)
Chl h di f ki (IA)
Blood Stream Infection (BSI) Prevention Bundle (IB)
• Chlorhexadine for skin prep (IA)
• Avoid femoral lines (IA)
CDC. Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]http://www.guideline.gov/summary/summary.aspx?doc_id=13395&nbr=006806&string=CLA-BSI –Oct 2008www.ihi.orgGrady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.govhttp://www.onthecuspstophai.org/
Education & Culture of Safety
Canada CLI & CLM Bundle’s(All or None Strategy)
Central Line Insertion Bundle
Hand hygiene
Maximal barrier
Central Line Maintenance
Bundle Daily review of line
necessity & prompt removal of unnecessary Maximal barrier
precautions
Chlorhexidine skin antisepsis
Optimal catheter site selection
removal of unnecessary lines
Dedicated lumen for TPN Accessing the lumen
aseptically Checking entry site for
inflammation with every dressing change
http://www.saferhealthcarenow.ca/EN/Interventions/CLI/Pages/gsk.aspx
Updated HICPAC Categorization Scheme for Recommendations
What Does the ‘Bundle’ Evidence Tell Us?
CDC Guidelines for Insertion Site Preparation
Sterile technique; cap, mask, gown, gloves, and a large sterile drape (IA)
Recommend 2% Chlorhexidine be the cleanser of choice if available (IA)
Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
What are Maximal Barrier Precautions?
• For Provider:
– Hands hygiene
– Non-sterile cap and mask
• All hair should be under cap
• Mask should cover nose and mouth tightly
– Sterile gown and gloves
• For the Patient
– Cover patient’s head and body with a large sterile drape

6/10/2011
19
Chlorhexidine vs Povidone Iodine for Catheter Site Care
Ann Intern Med 2002:136:792-801
2011 Recommendations: Site Location
• Avoid using the femoral vein for central venous access in adult patients (1A)
• Use a subclavian site, rather than a jugular or a femoral site, in adult patients to minimize infection risk for nontunneled CVC placement (1B)
• Avoid the subclavian site in hemodialysis patients and patients with advanced kidney disease, to avoid subclavian vein stenosis (1A)
Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
2011: Additional Placement Guidelines
• Use ultrasound guidance to place central venous catheters (if this technology is available) to reduce the number of cannulation attempts and mechanical complications. Ultrasound guidance should only be used by those fully trained in its technique. (IB)
• Use a CVC with the minimum number of ports or lumens essential for the management of the patient (IB)
• Promptly remove any intravascular catheter that is no longer essential. (IA)
• Use a sutureless securement device to reduce the risk of infection for intravascular catheters. (II)
Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
CDC Recommendation for Catheter Replacement
• When adherence to aseptic technique cannot be ensured replace the catheter as soon as possible, i.e, within 48 hours. (IB)
• Do not routinely replace CVCs, PICCs, hemodialysis catheters or pulmonary artery catheters to prevent cathetercatheters, or pulmonary artery catheters to prevent catheter-related infections. (IB)
• Use a guidewire exchange to replace a malfunctioning non-tunneled catheter if no evidence of infection is present. (IB)
• Do not use guidewire exchanges to replace a non-tunneled catheter suspected of infection. (IB)
• Routine culture of the tip is not recommended.• .CDC. Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]
Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
Dressing Care
• Use a transparent or gauze dressing to cover site (IA)• Change transparent dressing and perform site care with a CHG
based antiseptic every 7 days (IB) or more frequent if the dressing is soiled, loose, or damp; (IB)
• Change gauze dressings every 2 days or more frequent if the dressing is loose, soiled or damp (II)
• Use a chlorhexidine-impregnated sponge dressing for temporary short-term catheters in patients older than 2 months of age if the CLABSI rate is not despite EBP (1B)
• No recommendation is made for other types of chlorhexidinedressings.
SHEA and IDSA, Infection Control and Hospital Epidemiology Oct 2008Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]Salgado CD, et al. Infect Control and Hosp Epidemi, 2007;28:684-688Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
Care After Insertion
• Scrubbing the access port with an appropriate antiseptic (chlorhexidine, povidone iodine, an iodophor, or 70% alcohol) and accessing the port only with sterile devices.(IA)
• 3 sec, 10 sec & 15 sec scrub showed no difference in reducing bacterial load (Simmons S, et al. Crit Care Nurs Q, 2011;34:31-35)
• When needleless system used, consider a split septum valve versus a mechanical valve.(II)
• Replace administration sets not used for blood, blood products or lipids at intervals not longer than 96 hours (IA)
• Replace tubing used to administer blood, blood products, or fat emulsions within 24 hours of initiating the infusion. (IB)
• Change the needleless components at least as frequently as the administration set. (II)
• Use a 2% chlorhexidine wash for daily skin cleansing to reduce CRBSI (II )

6/10/2011
20
Additional Strategies Used When Basic Care Has Not Achieve Zero
CHG Baths (II)
CHG Dressings (IB)
Antimicrobial impregnated CVC (IA)Antimicrobial impregnated CVC (IA)
Antimicrobial locks (II)
Appropriate nursing staff levels in ICUs. (1B)
Coffin SE, et al. Infection Control & Hosp Epid, 2008;29(1):S31-S40Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
CHG Bathing Reduces CLA-BSI’s (II)
• 52 week, 2 arm, cross-over design clinical trial• 22 bed MICU with 11 beds in 2 geographically
separate areas• 836 MICU patients
1st 28 k 1 h it l d i t b th– 1st 28 weeks: 1 hospital randomize to bathe with (Sage 2%) CHG cloths & the other unit bathe with soap & water
– 2 week wash out period– 2nd 24 weeks: methods were crossed over
• Measured: Primary outcomes: incidence of CA-BSI’s & clinical sepsis. Secondary: other infections
Bleasdale SC. et al. Arch Internal Med, 2007;167(19):2073-2079
CHG Bathing Reduces CLA-BSI’s (II)
Results: CHG arm were
significantly less likely to acquire a CA-BSI 4.1
10 4 i f ti
Bleasdale SC. et al. Arch Internal Med, 2007;167(19):2073-2079
vs. 10.4 infections per 1000 patient days
Benefit against primary CA-BSI’s by CHG cleansing after 5 days in MICU
No difference in clinical sepsis or other infections
CHG Bathing: Pre & Post Intervention
Dixon, et al. Am J Infect Control 2010;38:817-21
Corcoran et al APIC 6/2009
Additional Strategies Used When Basic Care Has Not Achieve Zero
CHG Baths (II)
CHG Dressings (B-I)
Antimicrobial impregnated CVC (A-I)Antimicrobial impregnated CVC (A I)
Antimicrobial locks (II)
Appropriate nursing staff levels in ICUs. (1B)
Coffin SE, et al. Infection Control & Hosp Epid, 2008;29(1):S31-S40Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
CHG-Impregnated Sponges for Prevention of CLA-BSI (IB)
Methodology:• Multi-center, randomized controlled trial • 7 ICUs participated• Included all patients who required arterial or central p q
venous catheter for 48 hours or longer• Use of CHG dsg vs standard dsg• Already using maximal barrier precautions, try and use
subclavian site for central line, use alcohol/povidone-iodine prep solution (not CHG)
• Looked at 3 day vs. seven day dressing change (but changed when dsg was loose, soiled or damp in all groups)
Timsit JF, et al. JAMA 2009;301:1231-1241

6/10/2011
21
CHG-Impregnated Sponges for Prevention of CLABSI (IB)
• 1636 patients (3778 catheters, 28,931 catheter days)• Median duration of catheter insertions 6 days (4-10)• Use of CHG dressing decreased the CLA-BSI rate from:
1 3 per 1000 catheter days to 0 4 per 1000 catheter days
Results:
– 1.3 per 1000 catheter days to 0.4 per 1000 catheter days
• Use of CHG dressing not associated with greater resistance of bacteria in skin samples at removal
• 8 episodes of contact dermatitis with patch ( 817 pts)• No difference in site colonization between dressing
changes at 3 days or 7 days
Timsit JF, et al. JAMA 2009;301:1231-1241
Prevented 1 Major CLA-BSI per 117 Catheters
2011: Antimicrobial CVC
CDC Recommendations:• Use a chlorhexidine/silver sulfadiazine or
minocycline/rifampin -impregnated CVC in patients whose catheter is expected to remain in p pplace >5 days if, after successful implementation of a comprehensive strategy to reduce rates of CLABSI, the CLABSI rate is not decreasing. (IA)
CDC. Prevention of Catheter Infection: MMWR 2002;51Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
01-CHSS Blue Plus-Antimicrobial Impregnated
02-Silver Impregnated-Antimicrobial Impregnated
03-Minocycline-Rifampin-Antibiotic
04-Miconazole & Rifampicin -AntibioticAl CVCs appear to be effective in reducing CLARifampicin Antibiotic
05-Benzalkonium Chloride Impregnated-Antimicrobial Impregnated
06-CHSS-Antimicrobial coated
Hockenhull JC, et al. Crit Care Med, 2009;3792): 702-712Matheos T, et al. Infect Control Hosp Epidemiol 2010;31:295-297
Al-CVCs appear to be effective in reducing CLA-BSI’s when compared to standard CVCs. It is important to establish whether this effect remains in settings where infection prevention bundles of care staff wishes routine practice
Emerging Issues: Needleless IV Access Equipment
Q-Syte
Clearlink
InVision-Plus NeutralSafesite
• Split system value designs are preferred over positive pressure mechanical valves because they
i t d ith l CLA BSI t
Clave
Posiflow
Interlink
CLC 2000
Smartsite
Ultrasite MaxPlus
SmartSite PlusPASVare associated with lower CLA-BSI rates.
• In 2008 FDA required 9 companies to conduct post market surveillance of positive displacement needless connectors
Rupp ME, et al. Clin Infect Dis. 2007;44(11):1408-1414FDA Medical Device Alert 2008
Berenholtz et al, 2004; Tsuchida et al, 2007
Interventions To Ensure Patient Receive Evidence
• Education…to all caregivers…it works*
• Ask Daily if line is needed
• Checklist, nurse
Empower nurses• Empower nurses
• Products/Processes that make it easy for the frontline caregiver to provide the care
• Measurement/Feedback**
• Simulation training of residents reduced CRBSI’s.***
* Parra AP, etal. Infect Control Hosp Epidemiol 2010;31(9):964-967**Westwall S. Nursing in Critical Care, 2008;13(4):203-207*** Barsuk JH, et al. Arch Intern Med, 2009;169:1420-1423

6/10/2011
22
• 103 ICU’s in state of Michigan reported data
• Examine 375,757 catheter days
• Implementation of the BSI Bundle/checklist
• Results
Intervention to Decrease CLA-BSIStatewide Collaborative-Keystone ICU
– Median rate of CLA-BSI per 1000 catheter days went 2.7 to 0 at 3 months ((p<0.002)
– Mean rate of CLA-BSI’s per 1000 catheter days went 7.7 to 1.4 at 18 month follow up (p<0.002)
– in mortality when compared to other mid-west states
Pronovost P et al, N Engl J Med;2006;355:2725-2732Pronovost P et al. BMJ, 2010;340:309Liptiz-Snyderman A, et al. BMJ, 2011;342:219
36 Months Post Initial Implementation: 90 of original 103 ICU’s evaluatedResults: Mean rate 1.1 per 1000 catheter days/ Median: Zero 2009: mean .88 per 1000 catheter days (personal communication)
On the CUSP: Stop BSIA National Initiative
• AHRQ government funded 3 year initiative
• HRET and American Hospital Association
• John Hopkins Quality & Safety Research Group
• MHA’s Keystone Center for Patient Safety & Quality
• Goals:– Eliminate CLA-BSI: <1/1000 catheter days, median 0
– Improve safety culture by 50%
– Learn from 1 defect a month
• Build an infrastructure for future efforts
• Baseline and monthly CLA-BSI rate, hospital survey on patient safety & monthly survey on teamwork barriers
http://www.onthecuspstophai.org/
Stop CLA-BSI: Progress Report
• Progress Report– 45 state hospital associations recruited 700 hospital & 1100
hospital teams in 2009
– 14 additional states and the District of Columbia joined in 20100 0
– Eight states, including Puerto Rico began in 2011
– 1.8 infections per 1000 days to 1.17 infections per 1000 days central line use (RR. 35%) in 22 states (350 hospitals)
– < 20% of US hospitals are participating
– CDC reported 58% drop in CLA-BSI between 2001 in 2008
• 6,000 lives saved
• 1.8 billion cost avoidance http://www.onthecuspstophai.org/http:/blogs.wsj/health/2011/04/05/progress-on-reducing-bloodstream-infections/
Canada’s Outcome
• The overall national mean for the Central Line-associated BSI rate per 1000 CLI days was reduced from a baseline of 5 to
t i d t f 0 3 t 0 8 i Ph Ia sustained rate of 0.3 to 0.8 in Phase I.
• Of the teams reporting data, 75% reached the national goal of <1.9 CLA-BSI per 1000 CLI days
http://www.saferhealthcarenow.ca/EN/Interventions/CLI/Pages/default.aspx
CA-UTI’s: Reducing Load
• Use of catheter increases risk• Daily risk of acquisition of UTI: 3% to 7% • Second common HAI & 80% attributable to indwelling
catheterization• CAUTI: associated with morbidity, mortality (2.3%), hospital cos
($589 00) & LOS($589.00) & LOS• 15%-25% of hospital patients may have a urinary catheter during
admission• Highest use; Trauma ICU units, Lowest use; Med-Surg• Pooled mean CAUTI rates 3.1 -7.5 infections per 1000 catheter
days (Burn ICU highest, Med-Surg ICU’s lowest)• Add 1 day LOS per patient
Joanna Briggs Institute EBR: 2007Saint S., et al. Infect Dis Clinics North Amer 2003; 17:411-432.Weinstein JW, et al. Infect control Hosp Epidemiol, 1999; 20:543-548Lo E, et al. Infect Contr & Hosp Epidemiol, 2008;29:S41-S50Gould, CV et al. HICPAC Guideline for Preventing Catheter-Associated UTI’s. 2009

6/10/2011
23
CA-UTI Bundle “Bladder Bundle”
• CA-UTI Bundle ( “Bladder Bundle”)– Avoid unnecessary urinary catheters– Insert urinary catheters using aseptic
t h itechnique– Maintain urinary catheters based on
recommended guidelines.– Review urinary catheter necessity daily and
remove promptly
http://www.bestcare.org.za/docs/Prevent%20Catheter%20CA-UTI.pdf
Core Recommendations
• Insert catheters only for appropriate indications (1B)• Leave catheters in only as long as needed (1B)
• Ensure that only properly trained persons insert and maintain catheters (1B)maintain catheters (1B)
• Insert catheters using aseptic technique in sterile equipment ( acute care settings) (1C)
• Maintain a close drainage system (1B)• Secure the system (1B)• Maintain unobstructed urine flow (1B)• Key the collecting bag below the level of the bladder at all
times (1B)
Core Recommendations
• Do not clean the periurethral area with antiseptics to prevent CAUTI while the catheter is in place. Routine hygiene (e.g., cleansing of the meatal surface during daily bathing) is appropriate. (IB)
• Further research is needed on the use of antisepticFurther research is needed on the use of antiseptic solutions vs. sterile water or saline for periurethral cleaning prior to catheter insertion. (No recommendation/unresolved issue)
• If the CAUTI rate is not decreasing with a comprehensive strategy, consider using antimicrobal/antiseptic impregnated catheters. (IB)
• Practice hand hygiene in standard precautions according to CDC & HICPAC guidelines
Expert Opinion
Gould, CV et al. HICPAC Guideline for Preventing Catheter-Associated UTI’s. Draft June 2009
14
16
18
20
ce
Da
ys
Impact of UTI with Basin Bathing
UTI Rate- Removal of Prepackaged Bath Product QTR 3 FY05
0
2
4
6
8
10
12
QTR 1FY05
QTR 2FY05
QTR 3FY05
QTR 4FY05
QTR 1FY06
QTR 2FY06
QTR 3FY06
Ra
te/1
00
0 D
ev
ic
50th percentile
McGuckin M, Torress-Cook A, et al APWCA Annual Meeting, Philadelphia, April 2007
The Effect of Bathing with Basin and Water and UTI Rate, LOS and Costs
Unit Census: 14
Phases Product Cost/ No. of UTI
Median4
LOS17 Days
Median4
Cost(4857.00)
I- Pre-Packaged Bathing Washcloths(9 months)
$10,5301
($3.00)25 175 $117,175
II- Basin/Water(9 months)
$3,5102
($1.00)48 336 $224,916
III- Additional Product Cost, UTI, LOS, COSTS
$7,020 233 151 $107,741
Chen Yin-Yin,Chou Yi-Chang,Chou Pesus.. Infect Control Hosp Epidemiol 2005;26:281-287
1Based on 3 packages of 8 towels each 2Based on product cost of towels, soap, and basin3 Difference between phase I pre-package/phase II basin water4

6/10/2011
24
89% Reduction
Reducing UTI’s Through Basinless Bathing
CA-UTI 7.5 per 1000 catheter days to 4.42 per 1000 catheter days, then to .46 per 1000 catheter days
Stone S, et al. 37th Annual APIC Educational Conference July 11-15, 2010
Simple Cost Effective Strategies to Reduce HAI’s
Implementation:• Utilize daily 2%
CHG cloths for cleansing at night in any patient with a central
Corcoran F. Presented at APIC 2009
with a central line or foleycatheter
• Focused on areas most prone to bacterial colonization from the neck down
Was moved from the ICU to house-wide post initial project with similar results in Med-Surg
Reducing Use…Does it Reduce CA-UTI’s
• Pre and post intervention study• Unit clinicians developed indications for continue use of catheter
(evidence-based)• 6 month intervention period evaluated appropriateness of catheter
daily337 ti t /1432 th t i ti d l t d• 337 patients/1432 catheterization days were evaluated– Duration of use significantly reduced (236.6 d/mo vs. 311.7
d/mo)– CA-UTI’s went from 4.7 per 1000 days to zero for the
intervention period– 11% inappropriate days
Elpern EH, et al. Am J of Crit Care, 2009;18(6):535-541
Cost-Benefit Ratio
CA-UTI vs. IAD & Pressure Ulcer

6/10/2011
25
Bugs Be Gone!!!!
How to Get Started
Four E’s• Engage: help staff understand the preventable harm
– Share stories about patients affected
– Estimate number of patients harmed
– Develop a business case
• Educate: ensure staff and senior leaders understand what they need yto do to prevent injury and improve teamwork and communication– Conference calls, webcasts, meetings
• Execute: how given the resources and culture they would ensure that all patients received the evidence– Share with working, what’s not
– Coaching calls
• Evaluate: project leader monitors that teens are using standardized definitions, report their data and make it transparent at the unit level
Goeschel CA, et al. Nursing in Critical Care, 2011;16:35-42
The things included in the measurement b l t th thi itt dbecomes relevant, the things omitted are
out of sight out of mindPeter F. Drucker
In God We Trust!
Potential Barriers
• Perception of lack of time or the importance
• Lack of evidence based education…just do it!!!!
• Absence of a define protocol/procedure
• Staff turnover/Replacement staff• Staff turnover/Replacement staff
• Inaccessibility of needed supplies
• No real clinical lead on the unit
• Lack of feedback on progress
• Lack of accountability/responsibility
O’keefe-McCarthy S, et al. Worldviews on Evidence Based Nursing, 2008:193-204Abott CA, et al. Worldviews on Evidence Based Nursing:2008:193-204
Interventions To Ensure Patients Receive Evidence
• Evidence based education
• Recognition of value and reinforcement
• Products/Processes that make it easy for the frontline caregiver to provide the care (make it part of the bundle)
• Bathing kits
• Placement on the med record
• Automated charting with flag reminders
• Frequent rounding/reinforcement of standard
• Multidisciplinary rounds/Checklists
Westwall S. Nursing in Critical Care, 2008;13(4):203-207Abbott CA, et al. Worldviews on Evidence Based Practice, 2006:139-152Fuchs MA, et al. J Nurs Care Qual, 2011;26:101-109

6/10/2011
26
Interventions To Ensure Patients Receive Evidence
• Setting targets/Celebrating successes
• Placement of new practice/education in orientation
• Attractive signs to outline protocol in the patient rooms near the products
• Compliance program with feedback to all caregivers
• Outcome measurement/Feedback*
• Include RN’s in Morbidity & Mortality peer review for VAP increased compliance/accountability & VAP rates
Westwall S. Nursing in Critical Care, 2008;13(4):203-207Abbott CA, et al. Worldviews on Evidence Based Practice, 2006:139-152Fuchs MA, et al. J Nurs Care Qual, 2011;26:101-109Nolan SC, et al. JONA, 2010:40(9):374-383
What Can You Do?
• Identify the challenges in your work environment• Work with your colleagues to identify solutions (don’t wait
for others to do it; if they were going to do it, it would already be done!)
• Look for tools to help youLook for tools to help you• Find evidence such as best practice guidelines to support
your plan and make your arguments more compelling• Approach her supervisor or the chief nursing officer of
your facility for support• Consult/network with experts in the field• Think globally why acting locally• Share your results so that best practices don’t just occur
in isolated pockets
CREATE A SAFE PATIENT ENVIRONMENT
Everyday hospitalcare activities increase the patients risk of INJURY & BACTERIALINJURY & BACTERIAL INVASION ……
Help reduce that risk by changing the routine ways you provide care & replace it with the evidence
Be Courageous
We all are responsible for the safety of our patients……Own the Issues
•“If not this, then what??”•“If not now, then when?”•“If not me, then who??”


















