
POTENTIAL SHAPES - qums.ac.irfile.qums.ac.ir/repository/sd/pazhohesh/Library/E-book/...the curved...
120
movement with NiTi instruments with noncutting tips creates shapes with little or no incidence of preparation errors. 120 POTENTIAL SHAPES Figure 49 illustrates basic requirements for a radicu- lar shape, with adequate WL and working width as well as a homogenous taper that attempts to recreate the original main canal shape in an enlarged form. Cases present clinicians with a variety of anatomical and other challenges but the principles for root canal shaping remain the same for straight and curved canals (see Figure 49). However, specific cases, such as wide apices found in incompletely formed roots or after apical root resorption, call for modified approaches due to thin dentin walls and difficulties in controlling the apical extent of the fill. Special procedures such as apexogenesis and apexification may be required to provide adequate obturation (see Chapter 30, Obturation of the Radicular Space). Variations in apical shape have received special attention and varying recommendations. Names were given for the desired configuration (lower panel in Figure 49): ‘‘apical stop,’’ 265 ‘‘apical box,’’ 242 ‘‘apical capture or control zone.’’ 266,267 The intent of all the described techniques is two-fold: (1) allow irrigant access to the apical root canal system and (2) prevent filling material from being extruded into the periapi- cal space. As stated earlier, no conclusive evidence favors one apical shape over another regarding clinical outcomes; however, Kast’akova et al. 268 demonstrated that an apical stop, prepared to follow the recommen- dation to prepare three sizes larger than the first file to bind at WL, did not prevent sealer or gutta-percha extrusion. Finally, the argument has been made that a tapered apical preparation would reduce the incidence of overpreparation that may occur following a length determination error and an apical stop preparation. 269 This idea derived its attraction from the well-sup- ported notion that preparation errors should be avoided as they are associated with inferior out- comes. 270–275 Preparation errors and their develop- ment are discussed further below. Several systems to prepare canal with hand or engine- driven instruments have been described, beginning with Ingle’s standardized technique 276 (Table 11). There are two principally different approaches: the ‘‘apex first’’ and the ‘‘coronal first’’ techniques. The former approach advocates that WL is reached and the apical area is prepared first with increasingly larger instrument Figure 48 Clinical examples of root canal filled teeth that do not follow principles for an optimized shape. A, Very narrow shape that is not conducive to cleaning and irrigant access. B, Overenlargement that may predispose to vertical root fracture (arrowhead). C, The so-called ‘‘coke bottle’’ shape produced by overzealous action of Gates Glidden drills. Chapter 27 / Preparation of Coronal and Radicular Spaces / 935
Transcript of POTENTIAL SHAPES - qums.ac.irfile.qums.ac.ir/repository/sd/pazhohesh/Library/E-book/...the curved...

movement with NiTi instruments with noncutting tipscreates shapes with little or no incidence of preparationerrors.120
POTENTIAL SHAPESFigure 49 illustrates basic requirements for a radicu-
lar shape, with adequate WL and working width aswell as a homogenous taper that attempts to recreatethe original main canal shape in an enlarged form.Cases present clinicians with a variety of anatomicaland other challenges but the principles for root canalshaping remain the same for straight and curvedcanals (see Figure 49). However, specific cases, suchas wide apices found in incompletely formed roots orafter apical root resorption, call for modifiedapproaches due to thin dentin walls and difficultiesin controlling the apical extent of the fill. Specialprocedures such as apexogenesis and apexificationmay be required to provide adequate obturation (seeChapter 30, Obturation of the Radicular Space).
Variations in apical shape have received specialattention and varying recommendations. Names weregiven for the desired configuration (lower panel inFigure 49): ‘‘apical stop,’’265 ‘‘apical box,’’242 ‘‘apicalcapture or control zone.’’266,267 The intent of all thedescribed techniques is two-fold: (1) allow irrigantaccess to the apical root canal system and (2) preventfilling material from being extruded into the periapi-cal space. As stated earlier, no conclusive evidencefavors one apical shape over another regarding clinicaloutcomes; however, Kast’akova et al.268 demonstratedthat an apical stop, prepared to follow the recommen-dation to prepare three sizes larger than the first file tobind at WL, did not prevent sealer or gutta-perchaextrusion.
Finally, the argument has been made that a taperedapical preparation would reduce the incidence ofoverpreparation that may occur following a lengthdetermination error and an apical stop preparation.269
This idea derived its attraction from the well-sup-ported notion that preparation errors should beavoided as they are associated with inferior out-comes.270–275 Preparation errors and their develop-ment are discussed further below.
Several systems to prepare canal with hand or engine-driven instruments have been described, beginning withIngle’s standardized technique276 (Table 11). There aretwo principally different approaches: the ‘‘apex first’’and the ‘‘coronal first’’ techniques. The former approachadvocates that WL is reached and the apical areais prepared first with increasingly larger instrument
Figure 48 Clinical examples of root canal filled teeth that do notfollow principles for an optimized shape. A, Very narrow shape thatis not conducive to cleaning and irrigant access. B, Overenlargementthat may predispose to vertical root fracture (arrowhead). C, Theso-called ‘‘coke bottle’’ shape produced by overzealous action of GatesGlidden drills.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 935

sizes, whereas the latter uses descending instrument sizesto prepare coronal canal areas first and apical ones last.The following section will describe the basic techniquesand some subaspects of them in more detail. As these
techniques are generally independent of the instrumentswith which they are performed, the reader is referred toChapter 26C, ‘‘Instruments for Cleaning and Shaping’’for a detailed review of design and properties ofhandheld and engine-driven endodontic instruments.However, it needs to be kept in mind that the literatureis replete with references to the superiority of oneinstrument or one method of preparation over allothers.288–290 The following statement may put expec-tations on any particular file type into perspective:‘‘Regardless of the instrument type, none was able toreproduce ideal results; however, clinically acceptableresults could be obtained with all of them.’’291
Preparation Techniques
STANDARDIZEDThe standardized technique uses the same WL defini-tion for all instruments introduced into a root canal
Figure 49 Schematic diagrams of potential root canal shapes after preparation. Depending on the instrument and the sequence used, the canal isenlarged into a tapered shape (A, for example, rotary instrumentation), a taper with incremental size increase (B, step-back preparation), or a slight taperwith defined apical stop C. The bottom panel shows magnified apical shapes produced.
Table 11 Summary of Preparation Techniques Suggestedfor Hand and Rotary Instruments
Reference Year Technique
Ingle276 1961 Standardized instrumentation
Clem277, Weine278
Schilder31969–1974 Step-back, serial preparation
Abou-Rass279 1980 Anticurvature filing
Marshall280,281 1980 Crown-down pressureless
Goerig262 1982 Step-down
Fava282,283 1983/1992 Double flare, with modifications
Roane284 1985 Balanced force
Torabinejad285,286 1994 Passive step back
Siqueira287 2002 Alternate rotary motion
936 / Endodontics

and therefore relies on the inherent shape of theinstruments to impart the final shape to the canal. Itcan therefore also be called a ‘‘single-length techni-que,’’ an approach that has recently gained popularitywith the ProTaper (Dentsply Maillefer) and MTwo(Sweden and Martina, Padova, Italy) NiTi rotaryinstruments.
Negotiation of fine canals is initiated with fine filesthat are then advanced to WL and worked until a nextlarger instrument may be used. Conceptually, the finalshape is predicted by the last-used instrument (alsonamed MAF, see Box 1). A single matching gutta-percha point may then be used for root canal filling.In reality, this concept suffers from two factors ofvariation: first, canals (in particular those with curva-tures), shaped with the standardized technique, endup wider than the instrument size would sug-gest,292,293 and second, production quality is insuffi-cient, both for instruments and for gutta-perchacones, leading to size variations.294,295
STEP-BACKRealizing the importance of a shape larger than thatproduced with the standardized approach, Clem277
and Weine278 introduced the step-back technique,sometimes also called telescopic technique.296 Thisparadigm relies on stepwise reduction of WL for lar-ger files, typically in 1- or 0.5-mm steps, resulting inflared shapes with 0.05 and 0.10 taper, respectively.Incrementally reducing WL for larger and stifferinstruments in turn lessened the forces associated withaberrant preparations, in particular in curved canals(Figure 50).
Clem277 originally described the step-back techniquefor curved canals in teeth of adolescents, as the creationof a single step, at the transition from the straight tothe curved portion of the root. The resulting shape issomewhat similar to the ‘‘coke bottle’’ configurationsthat occur when inflexible engine-driven instrumentssuch as GG or Peeso drills are advanced past the mid-dle root canal third (see Figure 48). Taking GG andPeeso drills deep into canals carries the risk of fractureas they are not very resistant to fatigue occurring incurved canals.297 Furthermore, overpreparation andsubsequent strip perforations may occur,263,264,298 andtherefore these shapes are generally not desirable.
Subsequently, Schilder3 suggested a ‘‘serial prepara-tion’’ that included enlarging to a file size #30 or #35and then serially reducing WL for the followinginstruments. Initially, he did not advocate a metricallydefined step but rather a tactile feedback and cuttingof dentin when initial wall contact was made. Thus,
larger instruments would be used with decreasing WLand finally a smoothly tapered canal shape wouldresult. The developed shape, however, may be verysimilar to what had been described as the outcome ofa step-back procedure and in fact later, Schilder-typepreparation was illustrated as involving regular pre-determined steps.258 Coffae and Brilliant,299 for exam-ple, described a serial procedure that entailed the useof a #35 file to WL, stepwise reduction of WL forsubsequent files up to size #60, and then the use ofGG drills Nos. 2 and 3 approximately 16 and 14,respectively, into the canal (Figure 51). They describesuperior debridement with serial preparation com-pared to standardized shapes.299 Walton et al.300 cor-roborated these results by histological evaluations.Clearly, coronal enlargement (flaring) appeared ben-eficial for cleaning and obturation.248 However, there
Figure 50 Principles of radicular dentin removal. In a curved canal,apical pressure leads to transportation toward the outer curvature. Atthe same time, the reactionary force builds up in the straighteninginstrument against the dentin coronal of the curvature and leads totransportation toward the inner curvature (e.g., furcation).
Chapter 27 / Preparation of Coronal and Radicular Spaces / 937

was concern about the potential for overinstrumen-tation and potential perforation. Development con-tinued to modify shaping procedures.
Mullaney301 described the step-back technique asparticularly effective in fine canals. He divided thestep-back preparation into two phases. Phase I is theapical preparation starting at the apical constriction.Phase II is the preparation of the remainder of thecanal, gradually stepping back while increasing theinstrument size. The completion of the preparationis the Refining Phase IIa and IIb to produce thecontinuing taper from the apex to the cervical (seeFigure 51). To start Phase I instrumentation, the canalshould have been explored with a fine instrument andthe WL established. It is important that a lubricant isused at this point since fibrous pulp stumps may becompacted against the apical constriction and causeapical blockage.302 In very fine canals, the irrigant thatwill reach this area may be insufficient to dissolvetissue. Lubrication is believed to emulsify tissue,allowing instrument tips to macerate and remove thistissue. It is only later, in canal filing, that dentin chipspack apically blocking the constriction. When theMAF size has been used to full WL, Phase I is con-sidered complete and the 1.0- to 2.0-mm space backfrom the apical constriction should be clean of debris.
It must be emphasized here that irrigation betweeneach instrument use as well as recapitulation with theprevious smaller instrument carried to full depth is
crucial. Then the step-back process (Phase II) beginswith a file one size larger than the MAF. Its WL is set1 mm short of the full WL, and it is carried down thecanal to the new shortened depth. The same process isrepeated with subsequent instruments again shortenedby 1.0 or 0.5 mm from the MAF. Thus, the preparationsteps back up the canal with either 1 or 0.5 mm andone larger instrument at a time. It has been recom-mended to end this step-back phase at size #603 orwhen the instrument has reached the wider straightportion of the root canal. In any case, frequent turn-over of the irrigant and recapitulation with the MAFare necessary to promote canal disinfection and preventblockage. The most coronal canal portion may then becarefully flared with GG drills or Hedstrom files. Therefining Phase IIb is a return to the MAF, smoothing allaround the walls to perfect the taper from the apicalconstriction to the cervical canal orifice, which wouldthen be a larger replica of the original canal.303
Although the step-back technique was primarilydesigned to avoid preparation errors in curved canals,it applies to straight canal preparation as well. In fact,all root canals have some curvature.14,304,305 Apparentlystraight canals are usually curved to some degree andcanals that appear to curve in one direction often curvein other directions as well.14 While it has been main-tained that only curved instruments should be intro-duced into curved canals,302 it seems in fact unlikelythat one can successfully match canals’ curvature with
Figure 51 Sequence of instruments in the step-back procedure. After coronal preenlargement with Gates Glidden burs A, apical preparation to thedesired master apical file (MAF) size commences with K-Files to determine working length (WL) B and then files of ascending size to the desired apicaldimension (also called Phase I, C). Then, the WL is progressively decreased (‘‘stepped-back’’) by 1 or 0.5 mm to create a more tapered shape (Phase IIa,D). Recapitulation with a small K-file is done to smooth canal walls and to ensure that the canal lumen is not blocked (Phase IIb, E). Frequent irrigationpromotes disinfection and removal of soft tissue.
938 / Endodontics

a precurved file. Moreover, rotary instruments arestraight and should be introduced only into canal areasthat a straight hand instrument, size #15 or #20, hasexplored (‘‘glide path,’’ see below).
A modification of the step-down approach usinghand instruments has been described by Torabine-jad.285,286 He advocated insertion of progressively lar-ger hand instruments as deep as they would passivelygo in order to gain insight into the canal anatomy andto provide some enlargement prior to reaching the WL.Subsequent use of GG drills or Peeso reamers willprovide additional coronal enlargement and improvetactile feedback from the apical region as well as betteraccess for irrigants.306,307 The use of an ultrasonicallyactivated size #15 K-file has been advocated to furtherblend canal irregularities.286 A second, probably evenmore important, benefit is the ultrasonic or sonic acti-vation of the irrigant placed in the root canal for 1 to2 minutes, and is turned over every 30 seconds.222,286
ANTICURVATURE FILINGIn this context, Abou Rass, Glick, and Frank308
described a method called ‘‘anticurvature filing’’ toprevent excessive removal of dentin from thinner rootsections in curved canals. The underlying observationwas that the furcation side (danger zone) of crosssections of mesial roots of mandibular molars has lessdentin thickness than the mesial side (safety zone).34,309
The technique included the use of precurved hand filesthat were purposefully manipulated to file the canalaway from the danger zone. It also incorporates cor-onal flaring with rotary instruments after the use ofhand instruments, but it is stated that such instrumentsshould not be introduced more than 3 mm into rootcanals.308 The final use of a manual instrument toblend the apical and coronal segments was advocated.
Kessler et al.310 as well as Lim and Stock260 demon-strated that ‘‘anticurvature’’ filing in fact helped toreduce the risk of perforation. Later, Safety Hedstromfiles (Kerr/Sybron, Romulus, MI) followed a similarconcept, namely filing away from the danger zone.These files had cutting edges that were flattened andthus dulled at one side and were therefore believed toremove less material in one direction.311 However,subsequent research showed that Safety Hedstrom fileswhen used as engine-driven versions are in fact not safebut tend to create preparation errors.312
STEP-DOWNA different approach was taken by Goerig et al.,262 whoadvocated shaping the coronal aspect of a root canal firstbefore apical instrumentation commenced. The authors
list the following advantages: the technique permitsstraighter access to the apical region, it eliminates cor-onal interferences, it removes the bulk of tissue andmicroorganisms before apical shaping, it allows deeperpenetration of irrigants, and the WL is less likely tochange. Subsequently, several of these claims were inves-tigated; it was found that shaping was subjectively easierbut had no measurable effect on canal transportation.313
Furthermore, there was a small but significant beneficialeffect on WL retention.186,314 The removal of coronalobstructions does allow a better determination of apicalcanal sizes;233,234 however, it is not clear if better irrigantpenetration occurs and if that has clinically measurablebenefits.
Another primary purpose of this technique is tominimize or eliminate the amount of necrotic debristhat could be extruded through the apical foramenduring instrumentation. This would help prevent post-treatment discomfort, incomplete cleansing, and diffi-culty in achieving a biocompatible seal at the apicalconstriction.280 One of the major advantages of step-down preparation is the freedom from the constraintof the apical enlarging instruments. By first flaring thecoronal two-thirds of the canal, the final apical instru-ments are unimpeded through most of their length.This increased access allows greater control and lesschance of zipping near the apical constriction.315 Inaddition, it ‘‘provides a coronal escape way thatreduces the piston in a cylinder effect’’204 responsiblefor debris extrusion from the apex. This is one possiblereason for the finding that coronal preflaring reducedthe amount of apically extruded debris.316
The procedure itself involves the preparation of twocoronal root canal thirds using Hedstrom files of size#15, #20, and #25 to 16 to 18 mm or where they bind.Thereafter, GG drills Nos. 2 and 3, and then poten-tially No. 4, are used sequentially shorter, thus flaringthe coronal segment of the main root canal. Then,apical instrumentation is initiated; it consists of nego-tiating the remainder of the canal with a small K-file,shaping an apical ‘‘seat,’’ and combining the twoparts, step-down and apical shape, by stepwisedecreasing of WL of incrementally larger files. Fre-quent recapitulation with a #25 K-file to WL isadvised to prevent blockage.
Numerous modifications of the original step-downtechnique have been used clinically but most include theuse of a small initial penetrating instrument, mostly astainless steel K-file exploring the apical constriction andestablishing the WL. To ensure this penetration, one mayhave to enlarge the coronal third of the canal withprogressively smaller GG drills or with other rotary instru-ments. At this point, and in the presence of NaOCl,
Chapter 27 / Preparation of Coronal and Radicular Spaces / 939

step-down cleaning and shaping may begin with a varietyof instruments. For example, starting with a size #50 K-fileand working down the canal, the instruments are useduntil the apical constriction (or WL) is reached. Whenresistance is met for further penetration, the next smallestsize is used. Irrigation should follow the use of each instru-ment and recapitulation after every other instrument. Toproperly enlarge the apical third and to round out ovoidshape and lateral canal orifices, a reverse order of instru-ments may be used starting with a size #20 (for example)and enlarging this region to a size #40 or #50 (for example).The tapered shape can be improved by stepping back upthe canal with larger instruments, bearing in mind all thetime the importance of irrigation and recapitulation.
BALANCED FORCEAfter many years of experimentation, Roane et al.284 intro-duced the ‘‘Balanced Force’’ concept of canal preparationin 1985. The concept came to fruition, they claimed, withthe development and introduction of a new K-type filedesign, the Flex-R File284,317 (originally manufactured byMoyco Union Broach, now Miltex, York, PA). The tech-nique can be described as ‘‘positioning and preloading
an instrument through a clockwise rotation andthen shaping the canal with a counterclockwiserotation.’’284 The authors evaluated the damagedinstruments produced by the use of this techniqueand discovered that a greater risk of instrumentdamage was associated with clockwise movement.318
For the best results with the ‘‘Balanced Force’’ techni-que, preparation is completed in a step-downapproach. The coronal and mid-thirds of a canal areflared with GG drills, beginning with small sizes, andthen shaping with hand instrument is carried out inthe apical areas. Similar to techniques described above,increasing the diameter of the coronal and mid-thirdsof a canal removes most of the contamination andprovides access for a more passive movement of handinstruments into the apical third. Shaping becomesless difficult: the radius of curvature is increased asthe arc is decreased. In other words, the canal becomesstraighter and the apex is accessible with less flexing ofthe shaping instruments (see Figure 50).
After mechanical shaping with GG drills, BalancedForce hand instrumentation begins with the typicaltriad of movements: placing, cutting, and removinginstruments using only rotary motions (Figure 52).
Figure 52 Principles of the Balanced Force technique. Instruments with a symmetrical triangular cross section and pilot tips (e.g., Flex-R files, MoycoUnion Broach, Montgomeryville, PA) were originally suggested to be used in three steps in a rotational movement. A file may be advanced into the canalwith a one-quarter clockwise rotation. The second movement involves adequate apical pressure to keep the instrument at this level of the canal whilerotate counterclockwise for a half- to three-quarter turn. Currently, it is recommended to use the first two movements repeatedly, progressing moreapically. Then the third movement pulls the instrument gently out of the canal with clockwise rotation.
940 / Endodontics

Insertion is done by a quarter-turn clockwise rotationwhile slight or no apical pressure is applied. Cutting isthen accomplished by counterclockwise rotationapplying sufficient apical pressure to the instrument.
The amount of apical pressure must be adjusted tomatch the file size (i.e., very light for fine instru-ments to fairly heavy for large instruments).284 Pres-sure should maintain the instrument at or near itsclockwise insertion depth. Then counterclockwiserotation and apical pressure act together to enlargeand shape the canal to the diameter of the instru-ment. Counterclockwise motion should be 120� orgreater. It must rotate the instrument sufficiently tomove the next larger cutting edge into the location ofthe blade that preceded it in order to shape the fullcircumference of a canal. A greater degree of rotationis preferred and will more completely shape the canalto provide a diameter equal to or greater than thatestablished by the counterclockwise instrumenttwisting during its manufacture. It is important tounderstand that clockwise rotation allows the instru-ment to engage dentin, and this motion should notexceed 90�. If excess clockwise rotation is used, theinstrument tip can become locked into place and thefile may unwind.284 If continued, when twistedcounterclockwise, the file may fail unexpectedly.The process is repeated (clockwise insertion andcounterclockwise cutting) as the instrument isadvanced toward the apex in shallow steps. Afterthe working depth is obtained, the instrument isfreed by one or more counterclockwise rotationsmade, while the depth is held constant. The file isthen removed from the canal by a slow clockwiserotation that loads debris into the flutes and elevatesit away from the apical foramen.284 A more or lessflared final shape may be obtained by stepping backin 0.5 or 1 mm increments.
Generous irrigation follows each shaping instru-ment, since residual debris will cause transportationof the shape. Debris applies supplemental pressuresagainst the next shaping instrument and tends to causestraightening of the curvature. By repeating the pre-viously described steps, the clinician gradually enlargesthe apical third of the canal by advancing to larger andlarger instruments. Working depths are changedbetween instruments to produce an apical taper. Theworking loads can and should be kept very light bylimiting the clockwise motion and thereby reducing theamount of tooth structure removed by each counter-clockwise shaping movement. This technique can andshould be used with minimal force.
The Balanced Force technique may be used withany file with symmetrical cross section;319 however,
shaping and transportation control are consideredoptimal when a Flex-R file is used.320 The Flex-Rfile design removes the transition angles inherentto the tip of standard K-files (see Chapter 26C,Instruments for Cleaning and Shaping). Theseangles may cut a ledge into the canal wall.321–324
The specific tip design prevents Flex-R files fromtransporting the canal into the external wall of acurve.325
Balanced Force instrumentation initiated fromthe belief that the apical area should be shaped tosizes larger than were generally practiced (see Table10). The original Balanced Force concept then refersto apical control zones by, for example, first usingsizes #15 and #20 files to the periodontal ligament(i.e., through the apical foramen) and then redu-cing the working depth by 0.5 mm for subsequentsizes #25, #30, and #35. The apical shape is thencompleted 1 mm short using sizes #40 and #45under continuing irrigation with NaOCl. Single-appointment preparation and obturation played animportant role in the formation of these shapingconcepts.
The success of this shaping technique and enlargingscheme has been closely evaluated in both clinicalpractice and student clinics, and it can be said thatfiles used in ‘‘Balanced Force’’ motion generally leadto comparatively little canal transportation. However,subsequent research has indicated that the underlyingmechanisms are different from what was originallyenvisaged.326,327 Specifically, there is evidence thatthe force required to hold the instrument close tothe position during counterclockwise rotation closelymatches the amount of force required to bend aninstrument into a curve similar to the main curve ofthe canal that is prepared.326 Nevertheless, in vitroreports indicate that shapes created with the BalancedForce technique are of excellent quality328 and arecomparable to those with NiTi rotary instru-ments.245,329,330 Furthermore, extrusion of materialwas less than with other techniques, such as thestep-back filing technique and the CaviEndo ultraso-nic method.331 More recently, Siqueira et al.287 testeda modification of the Balanced Forces technique theyhad earlier called alternated rotary movements. Thisapproach did not recommend withdrawal of theinstrument after each set of rotations but emphasizedincremental apically directed movement and withdra-wal only when the file, for example, a size #25 NitiFlex(Dentsply Maillefer) has reached the WL. Canalsshaped to an apical size #40 had in vitro bacterialreduction similar to canals prepared with GT rotariesto size #20 0.12 taper.287
Chapter 27 / Preparation of Coronal and Radicular Spaces / 941

CROWN-DOWN PRESSURELESSThe first description of a crown-down preparation, inwhich larger files are first used in the coronal two-thirds of the canals and then progressively smaller files
are used more apically, can be found in a Master’sThesis by John Pappin332 and the endodontic techniquemanual of the Oregon Health & Science University.281
They described the approach as follows (Figure 53):
Figure 53 Sequence of instruments in the crown-down approach. Coronal preenlargement was originally suggested to commence after determination ofa provisional working length (WL) with a size #35 hand file A, Then, Gates Glidden burs were used B, followed by hand files starting with a large file(e.g., size #60) and progressing apically with smaller sizes C, The definitive WL was determined as soon as the progress was made beyond theprovisional WL D, Apical enlargement E, and recapitulation F, created a homogenous shape that may be similar to the one created with the step-backapproach, provided that both techniques were performed with little or no procedural errors. Both step-back and crown-down techniques may be used inconjunction with hand and rotary instruments but in vitro evidence suggests that a crown-down approach is preferred for tapered rotary instruments.335
942 / Endodontics

After completion of coronal access, a provisional WL isdetermined and a size #35 K-file is introduced into theroot canal with no apically directed pressure. Then, aGG No. 2 is used, short of or to the length explored bythe size #35 file. The GG No. 2 flares the coronal rootcanal and is followed by GG Nos. 3 and 4 with pro-gressively shorter WLs. The next step is the core ofwhat is now known as crown-down technique: a size#60 hand file is used with no apical force, and reamingis employed to enlarge the canal, followed by incremen-tally smaller instruments progressing deeper into thecanal. A radiograph is taken when an instrument pene-trates deeper than the provisional WL; after that, theapically directed procedure continues until an instru-ment reached the definitive WL.
The final step is to enlarge the apical area to threesizes larger than the first file that bound at WL. This isaccomplished by going through the sequence of des-cending instrument sizes starting with a file one sizelarger than the starting size in the preceding series.Copious irrigation and recapitulation at the end of theprocedure is advocated. Marshall in 1984 and 1987amended the manual to include ‘‘Balanced Force’’movements (Tinkle J, personal communication).
Morgan and Montgomery333 described a slightlydifferent method where both GG Nos. 2 and 3 wereintroduced to a straight portion of the canal and the‘‘crown-down’’ process was started with a size #30 K-file.They showed superior ratings by experts judging canalshapes, but similar occurrence of preparation errors,compared to the step-back preparation.333 However, asubsequent study found no differences in canal transpor-tation when comparing ‘‘crown-down,’’ ‘‘step-back,’’sonic instrumentation, and a NiTi rotary system.334
Nevertheless, a crown-down approach is currently advo-cated for the majority of engine-driven rotary systems dueto reduced contact areas and forces on the instruments.335
DOUBLE FLAREFava282 presented a preparation technique that con-sisted of an exploratory action with a small file, acrown-down portion with K-files of descending sizes,and an apical enlargement to size #40 or similar. Herecommended stepping back in 1 mm incrementswith ascending files sizes and frequent recapitulationswith the MAF. Copious irrigation is considered man-datory. It is further emphasized that significant wallcontact should be avoided in the crown-down phaseto reduce hydrostatic pressure and the possibility ofblockage. At this time, the double-flare technique wasfelt to be indicated for straight canals treated in onevisit.282 Later studies demonstrated better prepara-
tions in teeth with curved root canals shaped with amodified double-flare technique and Flex-R files com-pared to shapes prepared with K-files and step-backtechnique. A double-flare technique was also sug-gested for ProFile rotary instruments.336
Rotary Instrumentation
The introduction of NiTi alloy337 for manufacturinghand files,338 and later engine-driven instruments,339
has altered canal shaping procedures drastically overthe past two decades.340 The endodontic literature isreplete with accounts of shaping outcomes in vitroand descriptions of forces to which NiTi instrumentsare subjected (for review see references 120 and 122).NiTi rotary instruments and their design specifics aredescribed in detail in Chapter 26B, ‘‘Introduction ofNickel-titanium Alloy to Endodontics’’ and Chapter26C, ‘‘Instruments for Cleaning and Shaping’’. Thefollowing section is dedicated to their clinical use.
A major benefit of NiTi rotaries is their potential toavoid preparation errors.341 This in turn may result inbetter clinical outcomes.228,273 Moreover, throughchanges in instrument geometries, the creation of opti-mized canal shapes has been simplified. There is anongoing debate over which shape is the most useful. Inany event, shapes that are apically narrow and have asmooth taper can be safely prepared to become moreparallel and apically larger. In achieving these designs,most manufacturers of rotary files recommend a strictcrown-down sequence, with the exception of the LSinstrument.342 Several strategies have been recommendedfor this instrument, most of which represent a double-flare technique. Recently, other instruments (ProTaper,MTwo) have appeared on the market that are to be usedin a single-length technique, somewhat similar to thestandardized technique for hand instruments.
A main reason for recommending a crown-downapproach is to avoid overloading rotating instrumentswith large frictional wall contact; this is believed toreduce the incidence of file fracture, in particulartorsional fracture (Box 2).343,344 One possible
Box 2 Fracture Mechanisms for Endodontic Instrumentsand Possible MechanismsTorsional failure Forcing the instrument into a narrow canal
space and rotating it
Fatigue failure Overusing an instrument by prolonged rotation
in a curved canal
Corrosive failure Combination of torsional and fatigue failure
of an instrument with signs of corrosion
Chapter 27 / Preparation of Coronal and Radicular Spaces / 943

mechanism for this type of fracture is an event knownas ‘‘taper lock,’’ illustrated in Figure 54.345,346 Taperlock occurs when the shape of the tapered root canalbeing prepared becomes similar to the instrument inuse. Instruments may then become locked into thecanal, and the tip may fracture.343 In a crown-downpattern, the next smaller instrument should beselected before taper lock can occur. Blum et al.335
were convinced that ProFiles used this way experi-enced much less torque than when a step-back patternwas followed. This finding can be extended to most ofthe other rotaries that have a similar longitudinaldesign, for example, K3 (SybronEndo), EndoSequence(BrasselerUSA), HERO 642 (MicroMega, BesanOon,France), and several others.
The distinctive design of LightSpeed instruments(Discus Dental) maximizes flexibility and allows lar-ger apical preparations without unnecessary removalof dentin. The LightSpeed (LSX) has a noncuttingshaft and a very short blade. After making SLA toabout the mid-root, the coronal third is flared withthe instrument of choice (not with the LSX). Afterflaring, at least #15 K-file is used to obtain patency toWL. A #20 LSX and sequentially larger sizes are usedto prepare the apical third. The Final Apical instru-ment Size (FAS) is the blade size that encounters
4 mm or more of cutting resistance apically. A4-mm step back with the next larger instrument (thanthe FAS) completes the apical preparation. The mid-root is then cleaned and tapered with the next two orthree sequentially larger LSX sizes, blending mid-rootinstrumentation with the previously prepared coronalthird. Recapitulation is usually necessary only once,with the FAS, at the end of canal preparation. Thenew LSX is to be used at 2500 rpm, and irrigation isrequired throughout the procedure.
Apical enlargement is sometimes done after crown-down has been accomplished. At this stage, differentstrategies are possible, that is, switching tapers or tipsizes, changing to different instruments. Torsionalstresses that files are subjected to depend on thesequence employed.347 Little is known of the inci-dence of fractures with single-length techniques,348
particularly when the recommendations of the man-ufacturers are followed. In addition, it is not certainhow important overall NiTi instrument fracturesare for clinical outcomes.349 Nevertheless, strict mon-itoring of instrument use should be instituted sothat NiTi files can be periodically disposed of priorto failure.350,351 In fact, single use in severely curvedor calcified canals may be preferable due to pro-blems of decontamination352–355 and corrosion356–358
Figure 54 Rotary instruments may be subject to taper lock as soon as the canal taper approaches their dimension. Then, a large proportion of theinstrument surface engages the canal wall (indicated by red bars), frictional resistance and hence torque increases, with a high risk of instrumentfracture. This risk may be minimized by sequentially A to C using instruments with smaller tip sizes or taper, thus reducing contact areas and torque.336
944 / Endodontics

in addition to the greater amount of stress that theinstruments are subjected to in such situations.
Three different main handling paradigms havebeen described for the use of rotary instruments.Buchanan359 recommends feeding the rotating fileinto a root canal with very slight apical force, untilthe instrument stalls, and then to immediately with-draw the file. At this point the file has done its cuttingaction and the flutes are loaded with debris that mustbe removed. The file is then reinserted. A similarmovement has been recommended for RaCe files(FKG, La Chaux-de-Fonds, Switzerland), designed toavoid threading into the canal.
In contrast, the second recommendation for mostother instruments is to use them in an up-and-downmovement342,360 with a very light touch to avoid taperlock and to distribute forces throughout the canal. Thismovement is continued until a certain resistance is metor WL is reached. Rotation in a curved canal leads toaccumulation of cyclic fatigue, another potential reasonfor instrument fracture (see Box 2).343,361–363 Fatigueoccurs through cyclic compression and elongation ofmetal. The compounded amount of strain leads tofracture after a typical lifespan of up to 1,500 rotationsin the most commonly used experimental configura-tion.364,365 While the lifespan, calculated as rotations tofracture, is independent of the rotational speed,366 theinstrument undergoing fatigue will fracture in a shortertime period with higher rotations per minute.
Regarding hand movements, there is mixed evi-dence regarding the protective effect of up-and-downmovements on the accumulation of cyclic fati-gue,360,363 but it does not appear to be harmful forthe instrument brands tested.
The third instrument usage recommendation is spe-cifically for ProTaper instruments and is termed ‘‘brush-ing’’.367 Instead of feeding the file axially into the rootcanal, it is moved distinctly laterally in order to avoidthreading in. Such lateral cutting occurs most effectivelywith a positive rake angle and a stiffer instrument.Regarding operational safety, it was recently establishedfor MTwo instruments that the ‘‘brushing’’ motionextended fatigue life for larger size instruments.368 Thisfinding may be extended to other instruments usinglateral cutting (Peters OA, Paque F, Boessler C, unpub-lished data). However, GG drills, used in this manner inthe coronal third of the canal,308,310 occasionally separatethrough fatigue. In this case, the GG shaft may be readilyremoved since fracture usually occurs on the transitionfrom shaft to shank.
A guideline emphasized for ProTaper367 that maybe extended to other currently available instruments
suggests determination of a ‘‘glide path.’’ Specifically,prior to the use of any rotary instrument, root canalsshould be explored with #10, #15, or even #20 K-filesto avoid overloading NiTi instrument tips with unex-pected canal curves or excessive wall contact.369 Spe-cial pathfinding files with specially designed geometryare available for this task (e.g., ProFinder, DentsplyMaillefer). Regardless of the design, it is important touse straight, not precurved, files to allow the subse-quent rotary files to reach the same depth, withoutencountering acute bends or very narrow canal areas.
Finally, it has been recommended by manufacturersto use gel-based lubricants in conjunction with NiTirotary files, or to fill the access cavity with NaOCl priorto instrument insertion.232,359 The use of gel-based lubri-cants could potentially reduce frictional resistance andhence torsional load.370 However, experimental evi-dence, using a dentin disk model, suggests otherwise.371
In fact, the use of ethylenediaminetetraacetic acid(EDTA)-containing gels such as RC-Prep (PremierDental Products, Norristown, PA) or Glyde (DentsplyMaillefer) may be detrimental, due to increased torquescores371,372 and, more importantly, due to chemicalinteraction with its EDTA moiety and NaOCl action.373
Therefore, and despite reports of its corrosivepotential,374,375 frequently replenishing a reservoir ofNaOCl376 is presently advocated, providing lubrica-tion and disinfection during canal shaping. Afterrotary instrumentation is complete, irrigation withEDTA and/or NaOCl may be done377, with and with-out ultrasonic activation.147,222,378
The following ten principles apply to the successfuluse of currently available NiTi rotary files:
1. As with any type of instrument, poor accesspreparation will lead to procedural errors. Whilegenerally important in root canal preparation, it iscrucial for the use of NiTi rotaries.
2. Files should never be forced, as NiTi instru-ments require a passive technique. If resistance isencountered, stop immediately and before conti-nuing, increase the coronal taper and verify the‘‘glide path’’ using small stainless steel hand files.
3. Canals representing difficult anatomy should bedetected, analyzed, and carefully instrumentedfollowing specific rules (Figure 55, see below formore details).
4. Files should not be overused. Once only is thesafest number but the actual stress level dependsupon the case. Hence files may be used for morethan one canal, but may have to be replaced whenshaping a particularly difficult canal.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 945

5. Instrument breakage occurs more often during theinitial stages of the learning curve. The clinicianchanging from stainless steel to NiTi should take
continuing education courses with experiencedclinicians and educators, followed by in vitropractice on plastic blocks and extracted teeth.
Figure 55 Example of a sequence of instruments to safely enlarge and shape the coronal part of the root canal system. This enables a complete shape of theapical third also. Shown are magnified buccal views into the access cavity of a maxillary molar and respective radiographs. After pathfinding with a lubricated(arrowhead) K-file, straight-line access (SLA) is created with ultrasonically powered and rotary instruments. This is often difficult but equally important in thesecond mesiobuccal canal (shown accessed here). Then working lengths (WLs) in all four canals are determined; subsequently canals are enlarged and filled.
946 / Endodontics

6. NiTi rotaries should not be used to bypass ledges.Confirmation of a glide path with a straight K-file isrequired prior to the use of any NiTi rotary.
7. Cutting with the entire length of the file bladeshould be avoided. This total or frictional fit ofthe file in the canal will cause the instrument tolock.
8. Sudden changes in the direction of an instrumentcaused by the operator (i.e., stopping and startingwhile inside the canal) must be avoided. A smoothgentle reaming or rotary motion is most efficient.
9. Inspection of instruments, particularly usedinstruments, by staff and doctor is essential. Itshould be remembered that NiTi has an excellentmemory. The file should be straight. If any bend ispresent, the instrument is fatigued and should bereplaced.
10. WL should be well established and controlled, asshould the actual length of the file. If a file breakswithout the clinician taking notice, a very sharptipped instrument, upon the next insertion, willcreate procedural errors.
It is extremely important, for successful root canalpreparation with rotary instruments, to carefully reviewthe specific anatomy of each case (see earlier in thischapter and Chapter 6, Morphology of teeth and theirroot canal systems). Straight access into the root canalmiddle third should be created, with extended accesscavities and early coronal flaring. When using rotaryinstruments, canals that curve, recurve, dilacerate,divide, or merge should be approached with extracare.232 Figure 56 illustrates other problematic canalconfigurations. For example, very long narrow canalsdo not allow early coronal enlargement to the sameextent as regular canals. The consequence is anincreased frictional contact area and the potential fortorsional overloading. There is no ideal solution to thisproblem except for extra careful flaring and potentiallyusing hand instruments.
Acute bends, that is, those with a small radius ofcurvature, more coronally (see Figure 56B), puts alarger instrument cross section under cyclic fatigueand may cause breakage.362 Here coronal flaring tothe point of curvature and the use of rotary files withless taper to the WL are indicated. Ovoid canals thatare wide buccolingually, such as distal canals of man-dibular molars or some premolars, present a differentproblem. Instrument fracture is not very likely, butthey can rarely be prepared to be round; hence deb-ridement may be incomplete. It may be appropriate toapproach these cases as if two canals existed buccallyand lingually, and then merge the preparations by
filing action with ultrasonic files or hand files. Formerging canals, it is suggested to prepare the straigh-ter canal to WL and the other canal to the merging
A B
C
D
EF
G H
Figure 56 Schematic diagram of typical root canal anatomy withincreasing degrees of difficulty for root canal preparation. Shown arebasic canal shapes and cross sections at the middle root canal third (seetext for more details). A, Short straight canal. B, Longer canal withmoderate curvature. C, Very long canal. D, Canal that is wide buccolin-gually and may have multiple apical ramifications. E, Canal that splitsapically in two main canals. F, Canals merging at the transition of middleand apical thirds. G, Acute curvature in coronal root canal third. H,Extreme curve in the apical 2 to 3 mm.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 947

point. This avoids forcing a rotary instrumentthrough a sharp S-curve. Many procedures have beensuggested for very acute curves and narrow canals (seeFigure 56C), although none is certain to be universallysuccessful.
By extending the strategies detailed earlier in thischapter, the following recommendations representcurrent thinking379 for such a procedure. In part,
these are different from earlier descriptions forhand instruments.256,257 Coronal enlargement andcreation of SLA are important to allow rotaryinstrument to work without undue stress. More-over, this procedure reduces the danger of ledgingand blocking. Figure 57 illustrates how this may beaccomplished for a curved canal in a maxillarymolar.
Figure 57 Example of a clinical sequence of instruments to safely enlarge and shape the apical two-thirds of curved root canal systems (palatal canal in A)using hand and rotary instruments. After pathfinding with small hand instruments B, and coronal preenlargement C, working length (WL) is determined. Fora safe use of rotary instruments, a glide path is established with a series of hand instruments D, which rotary instruments can then follow E, Sufficientapical enlargement F, allows small irrigation needles to be passively inserted deep into the main canal G, and facilitates fitting of master cones H .
948 / Endodontics

Calcifications occur nearest to the irritant to whichthe pulp is reacting. Since most irritants are in thecoronal region of the pulp, the farther apical one goesinto the canal, the more unlikely it is to be calcified.When files bind in these canals, it may be from smallconstrictions in the coronal part of the canal.
Obviously, before the canals can be entered, theirorifices must be found. Knowledge of pulp anatomy isof first importance. Perseverance is the secondrequirement, followed by a calm determination notto become desperate and decimate the internal toothwhen the expected orifice does not appear. The endo-dontic explorer is the greatest aid in finding a minutecanal entrance (see Figures 18 and 55), feeling alongthe walls and into the floor of the chamber in the areawhere the orifices are expected to be.
A valuable aid in finding and enlarging canal ori-fices, particularly with magnification, is the Micro-Opener (Dentsply Maillefer) or the EndoHandle(Logan Dental, Logan, UT), with K-type flutes in0.04 and 0.06 tapers.
Radiographs are indispensable in determiningwhere and in which direction canals enter into thepulp chamber. The initial radiograph is one of themost important aids available to the clinician; a bite-wing radiograph is helpful in providing an undis-torted and metrically accurate view of the pulp cham-ber. The handpiece and the bur may be held up to theradiograph to estimate the correct depth of penetra-tion and direction to the orifices. Color is anotherimportant aid in finding a canal orifice. The floor ofthe pulp chamber and the continuous anatomical linethat connects the orifices (the so-called molar trian-gle) are dark gray or sometimes brown in contrast tothe white or light yellow of the walls of the chamber(see Figure 55). Various ultrasonically powered tips
are very helpful in relocating and enlarging orificesonce their position has been determined (see Figure55).
Current rotary instruments have noncutting tipsand, with correct handling, pose relatively little riskof ledging the canal, certainly not in the coronal two-thirds. Provided that copious irrigation is used, api-cally directed transport of debris is less than withhand instruments and filing actions.162,380,381 Verify-ing a glide path, as illustrated earlier, is particularlyimportant when shaping narrow canals. This may beaccomplished with a small (size #6, #8, or #10) K- orC-file (Dentsply Maillefer), lubricated and used in awatch-winding motion (see Figures 55 and 57).
An argument against using a straight instrument isthat it tends to engage the wall at the curve or thepivot on a catch on the wall. Rotary instruments,however, are also straight. Therefore, the presence ofa glide path has to be verified with a straight hand file.When the presence of sharp curves, debris, or verynarrow canal areas is expected, precurving an explora-tory file is indeed indicated (Figure 58). Most often,the pathfinding file can be advanced to WL withadequate hand movements, in particular gentlewatch-winding. If this cannot be accomplished, cor-onal interferences must be removed by increasing thetaper of the already explored coronal canal segment(see Figure 55).
When tentative WL is reached with a pathfinderfile, the clinician may determine the direction of amajor curvature by noting the direction of the tip ofthe file when it is withdrawn. This is a valuable clue,since the clinician understands the direction in whichthe canal curves and may guide the instrumentaccordingly. Valuable time may be saved whenexploration is eliminated each time the instrument is
Figure 58 Flexible endodontic files may be used straight A, to initially scout and pathfind a root canal, since a subsequent rotary instrument can moresafely be used in a canal area that a straight hand file negotiated (‘‘glide path’’). If an intracanal obstruction is encountered, an adequately precurvedmanual instrument should be used to conform more to overall canal anatomy B, A more acutely curved instrument can be utilized to bypass ledges orblockages C, Inset shows bacterial growth on blood agar after a K-file was bent using ‘‘clean’’ gloved fingertips.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 949

placed in the canal. A pointed silicone stop will clearlyshow the direction of the file curvature. The WL maythen be confirmed with a radiograph using a size #15K-file. After determining the WL, a curved pathfind-ing file should be used if additional canals are sus-pected, for example, in mandibular incisors, mandib-ular premolars, the distal root of mandibular molars,or the mesiobuccal root of maxillary molars.
While ultrasonically powered inserts are routinelyused under magnification to explore and refine accessinto canals, rarely do they need to be used into middleand even apical third of canals. However, when severecalcification is present, there is the option to locate acanal cross section that needs further shaping withhand or rotary files to WL (Figure 59).
Others have recommended the use of EDTA buf-fered to a pH of 7.3 to ‘‘dissolve’’ a pathway forexploring instruments.382,383 When the mineral saltshave been removed from the obstructing dentin bychelation, only the softened matrix remains.384 How-ever, this action has been disputed by others, sincechelation does not readily occur in narrow parts of thecanal, although softening can occur in the cervical andmiddle portions.385,386 EDTA must be concentratedenough in an area to be effective.
Like in many other situations in root canal therapy,it is the obligation of an astute clinician to execute acost-benefit evaluation, in order to determine iffurther progress without clear evidence of a canalcross section is indicated. Magnification and
Figure 59 Occasionally, calcification may occur more apically than usual. In this case, ultrasonic instruments were used to remove the obstruction(arrowhead in A); both mesial and distal canals were shaped and filled to the desired working length (WL). A, View through the operating microscopebefore using ultrasonic tips and preoperative radiographs. B, Canal lumen exposed as seen in the operating microscope and postoperative radiograph.Images courtesy of Dr. Peter Velvart.
950 / Endodontics

illumination are keys to this task and experience willhelp to guide the clinician here more than textbooks.
In conclusion, it needs to be emphasized that thesuggested methods are by no means the only way toapproach difficult root canals. Again, it is in thehands of an artful clinician to master all aspects ofsuch a case.
Devices for Powered Canal Preparation
Engine-driven instruments have been used in rootcanal preparation for more than 100 years beginningwith GG drills in 1885. These drills were mostly usedin handpieces connected to belt drives and werepedal-powered, even though the first electric dentalhandpiece had been patented in 1875. Subsequently,many modifications, and specifically handpieces withvarious oscillating movements, were brought to themarket, none of which provided superior preparationquality.122 Currently, the newest major energy sourcesfor root canal preparation are again electric motorsfor continuous rotary motion and ultrasonic/sonicunits for vibration.
MOTORS FOR ROTARYINSTRUMENTATIONEngine-driven instruments can be used in three typesof contra-angle handpieces: a full rotary handpiece,mostly latch grip, a reciprocating/quarter-turn hand-piece, or a special handpiece that imparts a verticalstroke but with an added reciprocating quarter turnthat ‘‘cuts in’’ when the instrument is stressed. Theseall are powered by electric or air-driven motors.While electric motors are more popular in Europe,air-powered motors are in much use in the UnitedStates. It is not clear if there are relevant differencesbetween these two motor types regarding file break-age.387 In addition to these two motors, there arebattery-powered, slow-speed handpieces that may be
combined with an apex locator, designed to simplify WL-control as well as torque-control motors (Figure 60).
As stated above, traditional handpieces with non-continuous movement such as the Giromatic (Micro-Mega) and M4 Safety handpiece (Kerr/Sybron) (seereference 122 for review) have been shown to lead toaberrant canal preparations. Some reports for thesesystems were favorable388–390 while most othersdemonstrated problems, most notably a high inci-dence of preparation errors.391–397 Consequently,these handpieces have lost popularity in the last yearswith the increased market share of NiTi rotaries.
An exception may be the Canal Finder systemdeveloped by Levy (currently marketed by SET,Olching, Germany) that uses a handpiece, either air-powered or electrically driven, that delivers a verticalstroke ranging from 0.3 to 1 mm. The more freely theinstrument moves in the canal, the longer is thestroke. The handpiece also has a quarter-turn recipro-cating motion that starts along with the vertical strokewhen the canal instrument is under bind in a tightcanal. If it is too tight, the motion ceases and theclinician switches to a smaller file.
More recently another handpiece with oscillatingaction was introduced (EndoEZE AET, Ultradent,South Jordan, UT) to more adequately prepare canalswith oval cross sections. Unfortunately, this techniquein its original configuration did not perform well incurved canals,398 but with updates, in file type andalloy as well as instrument sequence, it may serve asan adjunct to address cases not suitable for rotarypreparation alone.399
Recommended speeds for currently available NiTirotaries are in the range of 150 to 600 rpm, with theexception of LS that works predominantly above1,500 rpm. This range of speeds is typically reachedwith reduction gear handpieces (1:8 or 1:10). Higherspeed is occasionally advocated for better efficacyand safety,400 but the majority of authors maintainthat lower speeds are beneficial, offering a better
Chapter 27 / Preparation of Coronal and Radicular Spaces / 951

compromise regarding fatigue lifespan387,401,402 andoccurrence of taper lock.345,346,403,404
For continuous rotary movement, electric motorsoffer several benefits over air-powered ones, such asstable preset rotations per minute. However, the mostattention has been focused on the potential to pre-select maximum torque in order to protect instru-ment tips from fracturing.405 This is accomplishedby setting a maximum current (DC motors) exceptfor the so-called stepper motor that is software-con-trolled (EndoStepper, SET). There is some evidencethat the use a of a torque-limiting motor reduces the
overall load on NiTi files and hence increases theirfatigue lifespan.406,407 Moreover, these motors areseen as useful for beginners, to avoid forcing aninstrument.404 Various settings are possible for sometorque-limited motors; for example, the motor canstop, go into reverse or into oscillations.
On the other hand, electronics inside motors andhence their torque limits are not very precise;408–410
wear and friction inside the handpiece must also befurther taken into account. Moreover, these motorsdepend on correct presets for the expected fracturelimit. The limits are determined according to the
Figure 60 Selection of cable-bound A, and cordless B, motors intended for use with nickel–titanium (NiTi) rotary instruments.
952 / Endodontics

pertinent norms at D3, 3 mm from the tip of thefile.411 Hence, a short and less resistant segment ofthe file can still break even when the presets arecorrect.
A minimum torque is required for a rotaryinstrument to work against friction to prepare a canal(Figure 61). This torque level depends on instrumentcross sections and hand movements employed. Therelationship between fracture load at D3 and workingtorque has been referred to by J.T. McSpadden as the‘‘safety quotient’’; it is calculated by dividing fractureload by working torque.
If working torque is high and the fracture limit is asmall torque value, the instrument’s safety quotient isbelow 1. This indicates that the instruments mayoperate with imminent danger of fracturing. In con-trast, if there is very little working torque and a hightorque is required to fracture the instrument, thequotient is well above 1, and hence safety is consid-ered high (see Figure 61). However, Blum et al.412
have correctly pointed out that the quotient shouldrefer to a specific instrument cross section rather thanD3 alone to be more meaningful.
ULTRASONIC CANAL INSTRUMENTATIONThe use of ultrasonic in endodontics is based onsound as an energy source (at 20 to 25 kHz) thatactivates an endodontic file. As a result, three-dimen-sional file movement in the surrounding medium ofroot canals may be enlarged.413 The main debride-ment action of ultrasonics was initially thought to beby cavitation, a process by which bubbles formedfrom the action of the file become unstable, collapse,and cause an implosion. A combined shock, shear,and vacuum action resulted.413 Ultrasonic handpiecestypically use K-files as instruments for canal shaping.Before a size #15 file can fully function, however, thecanal must be enlarged with hand instruments to atleast a size #20 to allow the file to oscillate withoutconstraint. Although Richman must be credited withthe first report (1957) of the use of ultrasonics inendodontics,414 Martin and Cunningham415–420 werethe first to develop a device, test it, and see it mar-keted in 1976. It was named the Cavitron EndodonticSystem by Dentsply Caulk and was followed by manyother devices on the market. These instruments alldeliver an irrigant/coolant, usually NaOCl, into the
Figure 61 Relationship of torque during canal preparation and fracture load: The McSpadden Factor. A, Working torque (in blue), apically directed force (ingreen), and insertion depth (in red) into an extracted tooth simultaneously recorded during preparation with a ProFile 0.04 60 rotary using a testing platform.Note that total length of the instrument use was about 16 seconds. B, Determination of fracture load according to ISO 3630-1 at 2 rpm, determined at D3. C,Mean working torques (means SD, n = 10 each) in straight and curved plastic blocks or in extracted teeth (indicated by various shades of dark blue) andstatic fracture load (bright blue bar, n = 8). Modified with permission from Peters OA and Barbakow F.363 D, Values of the McSpadden factors for ProFile0.04 60 are above 1 in all tested conditions, indicating a very fracture-resistant instrument (bar shades correspond to panel C).
Chapter 27 / Preparation of Coronal and Radicular Spaces / 953

canal space while canal preparation is carried out bya vibrating K-file. The canal shapes and surfacesachieved, by preparation with ultrasonic units,have ranged from outstanding419–424 to disappoint-ing,166,425–428 in particular regarding canal shapes,289,429,430
and the use of ultrasonics to shape canals has fallen intodisregard over the last decade.
Research into the potential mechanisms of ultraso-nic action has continued and has revealed that it isnot cavitation, but a different physical phenomenon,acoustic streaming, that is responsible for the debri-dement.431–433 Clearly, acoustic streaming depends onthe free displacement amplitude of the file, and if thevibrating file is at least partially constrained and dam-pened in its action, it will become ineffective.434
SONIC CANAL INSTRUMENTATIONSonic endodontic handpieces attach to the regularairline at a pressure of 0.4 MPa. Air pressure may bevaried with an adjustable ring on the handpiece togive an oscillatory range of 1.5 to 3 kHz. Tap waterirrigant/coolant is delivered into the preparation fromthe handpiece. Walmsley et al.434,435 studied the oscil-latory pattern of sonically powered files. They foundthat out in the air, the sonic file oscillated in a largeelliptical motion at the tip. However, when loaded, asin a canal, they found that the oscillatory motionchanged to a longitudinal motion, up and down,‘‘. . . a particularly efficient form of vibration for thepreparation of root canals. . . .’’435
Similar to ultrasonic instrumentation, there is cur-rently little support for the use of sonic vibration toprepare root canals, with the only exception of retro-grade canal preparation during endodontic surgery(see Chapter 32, Endodontic treatment outcome: thepotential for healing and retained function).
Today ultrasonically activated instruments are usedfor final canal debridement rather than canal prepara-tion.436 Passive sonic and ultrasonic irrigation is dis-tinct from active irrigation; in the former, irrigantdeposited in the canal is activated, whereas in thelatter, a stream of solution is continuously deliveredfrom the ultrasonic or sonic unit. Passive irrigation
(after smear layer removal) with a size #15 file for 3minutes in the presence of 5.25% NaOCl producedcleaner canals when compared to hand instrumenta-tion alone.437 Improvement in irrigation efficacy wasalso reported by authors using 5.25% NaOCl for 30 to60 seconds,438 2% NaOCl for 3 minutes,222 or 2%chlorhexidine for 1 minute.439
There has been concern that cutting instrumentswould in fact negatively impact canal surface andshape and therefore blunt noncutting inserts havebeen advocated. Figure 62 shows canal segments afterpassive ultrasonic irrigation, demonstrating nodamage with either cutting or noncutting instru-ments.378,440 It has also been of interest to see ifNaOCl may be extruded out of the apical foramenfrom ultrasonic filing and cause harmful effects.Alacam441 intentionally overinstrumented beyondthe apex in a monkey study and then evaluated thetissue response when NaOCl was used with conven-tional filing versus ultrasonic filing/irrigation. He didnot find any difference between the two methods andnoted a low to moderate inflammatory response peri-apically.
Ultrasonically and sonically activated passive irriga-tion exerts its effects via acoustic streaming andincrease in temperature442,443 (Figure 63) rather thancavitations as previously thought. Using bothmechanisms, 3 minutes of ultrasonic instrumentationwith a size #15 file and 5.25% NaOCl improved canalcleanliness.444 It is presently not clear which combina-tion of file size and canal shape produces the bestresults. In one study, smaller files generated greateracoustic streaming and hence much cleaner canals.432
As it had been shown that constraint of the activatedinsert in the apical canal third was an importantfactor,434,445 a freely oscillating size #15 K-file wasused for 5 minutes with a free flow of 1% NaOCl.The same authors found that root canals had to beenlarged to the size of a size #40 file to permit enoughclearance for the free vibration of the size #15 file atfull amplitude.446 Others have also recommended asize #15 file;378,427,447 however, van der Sluis et al.440
recently speculated that the shape of the insert in
954 / Endodontics

relation to the canal shape may play a role for its efficacy.Indeed, temperature changes during activation of irri-gants vary with the geometry and the material of theinsert, indicative of energy transfer (Paque F and PetersOA, unpublished data) (see Figure 63). While the major-ity of in vitro studies support improved debridementwith the use of passive ultrasonic irrigation, potentialclinical benefit is as yet unproven. In fact, ultrasonicinserts may fracture, representing an iatrogenic problemduring canal shaping (Figure 64).
Evaluation of Canal Preparation
Techniques
A variety of techniques have been used over the yearsto assess preparation quality (see references 120, 122for review), and most of these investigations weredone in vitro. Previously, two main parameters wereaddressed, mostly from a mechanistic viewpoint:canal shapes and appearance of canal surfaces, thelatter also termed cleanliness.
Figure 62 Varying effect of ultrasonic activation of deposited irrigation solution on apical canal wall morphology. In this experiment, both 5.25% sodiumhypochlorite (NaOCl) and 17% ethylenediaminetetraacetic acid (EDTA) irrigation were activated with either K-file-type or prototype noncutting insertsafter enlargement of single-rooted teeth to an apical size #45. A, Scanning electron micrographs of ultrasonic inserts, black bars are 300 �m. B, Canalsurface with smear layer without the use of EDTA (control). C, Apical segments after irrigation with NaOCl and EDTA with ultrasonic activation,demonstrating thin continuous (left) or no smear layer with open dentinal tubules (right, white bars are 50 �m).
Chapter 27 / Preparation of Coronal and Radicular Spaces / 955

The ability of an instrument or a technique to allowthe prepared canal to stay centered in root cross sec-tions is seen as beneficial (Figure 65). Conversely,canal transportation, or any deviation from the origi-nal canal path, is seen as negative and in particular theend points of transportation, namely preparation
errors (Figure 66). The term ‘‘zip’’ was coined byWeine,278 who described the appearance of a ‘‘zipped’’apex when viewed directly in vitro. The formation ofpreparation errors is believed to be due to the interac-tion of canal curvature, file design, and file handling(see Figure 50). The tendency of a file to straighten
Figure 63 Effect of ultrasonic activation on intracanal temperature in vitro. Thermocouples were attached to single-rooted teeth and the assembly wasplaced in a water bath at 37�C. Irrigation solution was either added and activated or continuously deposited concurrent with ultrasonic activation usingvarious inserts. A, Three thermocouples fitted into holes drilled in radicular dentin close to the intracanal surface. B, Bar diagrams showing maximumand minimum temperatures at the coronal, middle, and apical levels. Measurement duration 2.5 minutes, n=15. C, Original records of temperature overtime with no ultrasonic activation (control, left), using an agitator at sonic frequency (prototype, middle) and a blunt nickel–titanium (NiTi) wire forpassive ultrasonic agitation (right, EndoSoft, EMS, Nyon, Switzerland). Beginning of irrigation indicated by arrows.
956 / Endodontics

itself cannot be completely overcome by precurvingand leads to uneven distribution of forces and hencematerial removal.284,448
Moreover, the cutting action of instruments in theapical region, particularly when extended beyond thecanal space, may create an apical zip with perfora-tion.449 The occurrence of such apical preparationerrors has previously been linked to hand and rotaryinstruments with sharp tips.450–452 Zip-and-elbow for-mation and other well-described preparation outcomessuch as ledges, strip perforations, or excessive thinningof canal walls453 may have clinical consequences such asincomplete debridement, problems with root canal fill-
ing, or eventual vertical root fracture (Figure 67). Pre-paration errors may decrease outcomes, most likely viareduced antimicrobial efficacy, but their clinical con-sequences are still a matter of debate.270–274,454,455
Generally, apical canal areas tend to be overpreparedtoward the outer curve or the convexity of the canal,while more coronal areas are transported toward theconcavity or the furcation in multirooted teeth (seeFigure 50). This results in an uneven preparationdemonstrated in canal cross sections with large areasleft unprepared.456–460 This finding was validated bythree-dimensional analyses (see Figure 66) using micro-computed tomography.245,263,461–464 While the amount
Figure 64 Use of activated irrigation in the clinical setting. A size #15 K-file was attached to an ultrasonic unit (middle power setting) and activated for30 s. During cone fit, it was noted that a segment of the instrument had fractured. The fragment was removed and the root canal system filled withthermoplasticized gutta-percha.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 957

of prepared canal surface seems to be independentof the instrument type, it was significantly affectedby preoperative canal anatomy.245,463,464 Sequentialmechanical enlargement, as shown in Figure 68, maybe indicated in order to increase prepared surface
areas, in particular to remove tenacious biofilms pre-sent in retreatment cases.465
While the use of microcomputed tomographyrepresents the latest available technology, there arenumerous other ways to evaluate canal shapes, for
Figure 65 Canal cross sections before and after preparation can be assessed using a specially designed mold that allows sectioning of root, removal,and precise reposition of the resulting root disks A, Photographs can be taken and the effect of canal preparation numerically determined, for example,in the coronal, middle, and apical root thirds before B, and after preparation C, In this case shown, rotary preparation (left canals) resulted in round andcentered shapes, while hand instrumentation produced canal transportation and thinning of root structure (arrowhead, C ). Gradation of bar is 0.5 mm.
958 / Endodontics

example, superimposing radiographs before and aftershaping.334,466–468 Bramante et al.469 and laterothers470–474 embedded teeth with their roots in a
muffle system (see Figure 65). They were then cutand the cross sections evaluated before and after canalpreparation. Center points of the canals were deter-mined and movements of the canals’ centers calcu-lated.472,474–480 Numerous studies evaluated shapingcapabilities of specific instruments using canals ofvarying geometry in plastic blocks and extracted teeth.Various factors for canal transportation have been
Figure 66 Root canal preparation errors develop more readily withincreasing instrument size and hence stiffness. This panel of microcom-puted tomography data shows canal straightening and perforation aftershaping to size #25 in an experiment where quarter-turn pull motion wasemployed with stainless steel hand files. A, Unprepared root canalsystem of a maxillary molar. B, Accessed and coronal scouting with asize #15 file. C, Enlargement to size #15 (buccal canals) and #25 (palatalcanal) to working length (WL), note fractured instrument in secondmesiobuccal canal (arrowhead). D, Enlargement to size #30 (buccalcanals) and #35 (palatal canal), note perforation in main mesiobuccalcanal. E, Enlargement to size #50 and #55 in buccal and palatal canals,respectively. F, Enlargement to size #60 and #70 in buccal and palatalcanals, respectively.
Figure 67 Relationship between vertical root fracture location, clinical,and radiographic appearance. A buccal swelling but not appreciableprobing was present in this case. Only after the removal of the crownand the buildup material, a fracture line extending to the mesial wasapparent (arrowhead in A). A periodontal defect (probing depth 11 mm)was detected that corresponded to radiographically visible bone destruc-tion B, Images courtesy of Dr. Tri Huynh.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 959

Figure 68 Dependence of instrumented canal surface on file geometry and usage. A, Bar diagram showing overall and apical fractions of instrumentedcanal surface. Data recalculated from Peters OA, et al.245 B, Bar diagram showing increase of instrumented surface with increased apical sizes (Paque F,Peters OA, unpublished data). C, Microcomputed tomography reconstructions of canals shaped with cutting and noncutting instruments usedsubsequently.
960 / Endodontics

identified, such as canal anatomy, instrument type,cross-sectional and tip design, instrument taper,sequence, operator experience, rpm, and the use ofirrigants or lubricants.120
The effect of canal anatomy on shaping outcome iswell documented for LS, ProFile 0.4 and 0.06, Quan-tec LX and SC (Analytic Endodontics, Glendora, CA,USA), and HERO 642, in particular by experimentsfrom Dummer’s group452,481–488 using plastic blocks.Taken together, these studies demonstrated animpact of canal geometry on outcome: the moresevere the angle and radius of the curve, the moresevere the canal transportation. On the other hand,there was no significant effect of canal shape onpreparation times.
Furthermore, file design was crucial to avoid pre-paration errors: actively cutting tips such as withQuantec SC and LX452,488 produced more aberrationsthan instruments with noncutting tips.450,451,488–492
The direction of apical canal transportation varied,but occurred mainly outward in relation to the canals’curve; the total amount of canal transportation variedsignificantly, again in relation to canal geometry, andranged in most cases between 0.01 and0.150 mm.452,481–488
Compared to stainless steel hand files, NiTiinstruments were superior in their shaping abil-ity.493,494 Schafer et al. reported that HERO 642,495
FlexMaster (VDW, Munich, Germany),496 and K3instruments497 maintained the original canal path incurved plastic blocks better compared to stainless steelhand instruments. They found little incidence of canalaberrations and material removal in excess of0.15 mm in less than 50% of the levels analyzed forHERO, FlexMaster, and K3,495–497 while hand instru-mentation resulted in significantly greater materialremoval (up to 0.69 mm).497
ProTaper instruments prepared curved canals inplastic blocks in less time and with no definite canalaberrations, but with a larger amount of materialremoved, compared to GT Rotary, Quantec, and Pro-File 0.04 and 0.06 instruments.498 In a study usinganother brand of plastic blocks, Hata et al. foundoverly long preparation times (>250s) for ProFile0.04 and 0.06, GT Rotary, and in particular for‘‘Balanced Force’’ instrumentation.330
Instrument shaft design did not significantly mod-ify shapes of similar apical sizes in one series ofstudies,461,462 while it is generally held that a thinflexible shaft will allow larger apical shapes with lessaberrations.9,472 In contrast, ProFile 0.04 instrumentsalone removed more material compared to a combi-nation of ProFile 0.04 and 0.06.330
Cutting blade design was modified lately from pas-sive, so-called U-file designs to more actively cuttingtriangular ones in instruments such as ProTaper, Flex-Master, K3, HERO 642, and RaCe. However, whilethere is only limited evidence for each individualfile,462–464,495,496,499,500 the introduction of activelycutting cross sections does not appear to negativelyaffect centering abilities.
K-files used in most techniques, with the exceptionof ‘‘Balance forces,’’ performed inferior to NiTi rotaryin vitro.290,292,501–503 Clearly, reaming producedrounder canal shapes in cross section,504–506 whichmay be desirable as long as a canal may be reasonablyprepared round.
Handpieces with noncontinuous rotation have alsobeen extensively tested, and some are better in cuttingefficiency, some in following narrow curved canals,some in producing smooth canals, and some in allow-ing irrigation and smear layer removal.398,423,507–514
While all of the automated devices may be occasion-ally useful, none has proved to be outstanding; cur-rently NiTi rotary instrumentation is widely believedto be a better choice for root canal preparation.
As stated earlier, rotary instrumentation is poten-tially associated with an increased risk of instrumentbreakage.349,515–518 Substantial work has been donein vitro to elucidate the fracture mechanismsinvolved (see Box 2); however, the clinical impactof instrument fractures is less well documented anddoes not lend itself to assessment in prospectiveclinical studies.
Currently available evidence for outcome studiesregarding the impact of file breakage, as recentlyreviewed by Parashos and Messer,349 relates mainlyto the pre-NiTi era, with few exceptions.518,519 Forexample, Strindberg131 using very stringent criteriain his comprehensive outcome study found a 19%higher incidence of failure when a file fragment wasretained. He speculated that infection of the rootcanal apically of the retained fragment would renderthe prognosis poorer. On the other hand, a retrospec-tive analysis by Crump and Natkin454 of the outcomesof root canal treatments done by dental studentsrevealed instrument fractures in 178 out of approxi-mately 8,500 cases. Matched control cases of the samecohort without instrument fracture had statisticallysimilar outcomes when cases were evaluated as ‘‘suc-cess,’’ ‘‘failure,’’ or ‘‘uncertain,’’ based on clinical andradiographic criteria. In fact, the success rate wasslightly higher in the cases with retained fragments(81.2% versus 73.6%, p>0.05).
In a retrospective assessment of 66 cases with bro-ken instruments, Grossman520 found over a recall
Chapter 27 / Preparation of Coronal and Radicular Spaces / 961

period of up to 5 years, that out of cases without pre-existing apical periodontitis (47/66) about 90% stayedhealthy and only 2 showed signs of a lesion. Of the 19cases with a diagnosis of apical periodontitis, how-ever, healing occurred only in 9 cases. Similar resultswere reported by Fox et al.521 referring to 204 caseswith accidentally broken files, out of which only 12were scored as failures.
In a recent study on 8,460 cases, Spili et al.518 foundoverall a 3.3% prevalence of instrument fractures but aprevalence of 5.1% after the introduction of NiTirotaries (4.4% NiTi versus 0.7% stainless steel). How-ever, success rates were similar for teeth with andwithout a retained instrument fragment (91.8% versus94.5%). Moreover, if an instrument fractured in atooth with existing apical periodontitis, the healingrate would be lower (86.7% versus 92.9%), but thisdifference was not significant. Similarly, Wolcottet al.519 in an analysis of 4,652 cases found an overallfracture incidence of 2.4% using ProTaper instru-ments; however, they did not report on clinical out-comes of these cases.
From the described outcome studies, fractures thatdeveloped early compared to late during cleaning andshaping may be viewed differently, regarding thepotential to remove microbes from the root canalspace. Irrigant efficacy is affected by the amount ofcanal enlargement;9,10,222 therefore, a fragment lodgedin the canal before sufficient enlargement has takenplace may render canal disinfection ineffective. In caseof corrosion356,358,522 of the retained fragment, chan-ged ion concentrations in the microenvironment mayinhibit microorganism growth.523 At least this par-tially explains acceptable outcomes, even in the pre-sence of retained instrument fragments.349
Opinions vary over the risk and incidence of rotaryinstrument fractures, but even without solid clinicaldata it is generally thought that NiTi rotary fractureincidence is higher when compared to stainless steelhand instruments. The impact of these fractures onhealing probabilities524 is not clear.349 In fact, conse-quences of a retained or removed instrument fragmentare part of a complex array of impact factors governingthe spectrum of clinical outcomes. Therefore, animmediate attempt to remove a fractured root canalinstrument is mainly indicated if the coronal aspect ofthe fragment is visible, aided by magnification, and ifthere is microbial contamination apical to the frag-ment. A fragment position apical to a major curvesignificantly decreases the potential of successfulremoval.525,526
In summary, available evidence from recall studieswould suggest to take a conservative approach after a
fracture of a root canal instrument: (1) when a pre-operative diagnosis of irreversible pulpitis and hence anoncontaminated root canal system had been made;(2) if the instrument fractured very late in the proce-dure, after a sufficient attempt for canal disinfectionhad been done; and (3) if the instrument fracturedapical to a significant curve. For a detailed account oftechniques for instrument removal, the reader isreferred to Chapter 31, ‘‘Retreatment of non-healingendodontic therapy and management of mishaps’’.
Nontraditional Techniques
Besides hand and rotary instruments, lasers have beenproposed for root canal preparation for some timeand is still contemplated by some authors today.527
On the other hand, if no enlargement of the rootcanal system was required for disinfection and rootcanal filling, no preparation errors could be made;this may be possible with the so-called noninstrumen-tation technique.528 Finally, ongoing research is aimedat changing the paradigm of root canal preparationfor disinfection and filling altogether, with the poten-tial of seeding stem cells or at least allowing local cellpopulation to recolonize endodontic spaces.529
LASER-ASSISTED CANAL PREPARATIONEarly studies of the effects of lasers on hard dentaltissues were based simply on the empirical use ofavailable lasers and an examination of the tissue mod-ified by various techniques. Lasers emitting in theultraviolet, visible (i.e., argon laser, wavelengths of488 and 514 nm), and near infrared (i.e., neodymiu-m:yttrium–aluminum-garnet laser, 1.064 �m) areweakly absorbed by dental hard tissues, such as enameland dentin.530,531 Nd:YAG laser energy, on the otherhand, interacts well with dark tissues and is trans-mitted by water. Excimer lasers (193, 248, and308 nm) and erbium lasers (~3.0 �m) are stronglyabsorbed by dental hard tissues.530,531 Studies havebeen conducted evaluating the effects of laser irradia-tion inside root canals. The authors have discussedlaser endodontic therapy, some as supplementary andothers as a purely laser-assisted method.532
Applications of lasers in endodontic therapy havebeen aggressively investigated over the last two dec-ades, and this is discussed in more detail in Chapter26E, ‘‘Lasers’’. Briefly, there are three main areas inendodontics for the use of lasers: (1) hard tissue, (2)root canal surface, and (3) the periapex. Obviously,laser light travels straight; therefore, specific light-
962 / Endodontics

emitting probes have been developed to direct laserenergy not only into straight but also into curved rootcanals. Enlargement and cleaning of straight canalswith an Er:YAG laser was found to be effective andin fact faster than with step-back preparation withK-files.527 However, shaping curved root canals, inde-pendent of the probes used, has not been satisfactory(Figure 69).
Several authors have reported better removal ofdebris, for example, using an erbium:YAGlaser,533,534 although areas covered by residual debriscould be found where the laser light did not get intocontact with the root canal surface.535 An erbium:YAGlaser was more effective in debris removal (Figure 70),producing a cleaner surface with a greater num-ber of open tubules when compared with a Nd:YAGlaser and an unlased control without laser treat-ment.
Nd:YAG laser-irradiated samples presented notonly with melted and recrystallized dentin and smear
layer removal but also with charring in light micro-scopic images.536 However, SEM evaluation showedspecific patterns for erbium:YAG and Nd:YAG irra-diation as a result of different mechanisms of laser–-tissue interaction by these two wavelengths.533–535,537
Dederich et al.532 used a Nd:YAG laser to irradiatethe root canal walls and showed melted, recrystallized,and glazed surfaces. The process of melting and recrys-tallizing root canal surfaces was hoped to create a cleanand less penetrable canal.538 Laser energy transferredinto canal surfaces, when sufficient to melt dentin,may overheat the periodontal ligament also. Bahcallet al.,539 for example, investigated the use of the pulsedNd:YAG laser to clean root canals. Their resultsshowed that the Nd:YAG laser may cause harm tothe bone and periodontal tissues by overheating,which was also suggested by others.536,540,541 Accord-ing to Hibst et al.,542 the use of a highly absorbed laserlight tends to localize heating to a thin layer at thesample surface, thus minimizing the absorption depth.
Figure 69 Shaping of single-rooted teeth in vitro using an Er:YAG laser. A, Canal diameters compared using standardized radiographs. B, Bar diagramshowing mean (˘ SD) canal diameters before and after shaping. C, Scanning electron micrographs of lased apical canal surface (left) and control afterrotary instrumentation (right). D, Er:YAG laser used in the study. Images courtesy of Dr. Mark Roper.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 963

Consequently, the risk of subsurface thermal damagemay decrease since less energy is necessary to heat thesurface.543
One of the limitations of the laser treatment wasdemonstrated in a study by Harashima et al.544
Where the (argon) laser optic fiber had not touchedor reached the canal walls, areas with clean root canalsurfaces were interspersed with areas covered by resi-dual debris. Access into severely curved roots and thecost of the equipment are other limitations. Finally,operator and patient safety are of concern in theapplication of lasers in endodontics; safety precau-tions include safety glasses specific for each wave-length, warning signs, and high-volume evacuationclose to the treated area.
NONINSTRUMENTATION TECHNIQUEBased on the premise that optimal cleansing of theroot canal system is a prime prerequisite for long-
term success in endodontics, Lussi et al.246 introduceda minimally invasive approach for removing canalcontents and accomplishing disinfection that did notinvolve the use of a file (the noninstrumentationtechnique or NIT). This system consists of a pump,a hose, a special valve, and a connector that needs tobe cemented into the access cavity (Figure 71). Clean-ing action is then provided by oscillations of theirrigation solution (1% to 3% NaOCl) at a reducedpressure. Cavitation likely loosens the debris andNaOCl dissolves viable and necrotic tissue compo-nents that are then removed by suction from the lowpressure. It needs to be stressed that this system isdifferent from other recently proposed active irriga-tion systems,545–547 since the latter techniques still relyon mechanical shaping prior to the use of irrigationwhile a canal undergoing NIT is not enlarged.
The evolution of the technique over theyears548,549 has resulted in good cleaning ability invitro. However, clinical moisture control and filling
Figure 70 Intracanal dentin surfaces (apical third) under scanning electron microscope (SEM) (orig. mag. x1500) after laser treatment. A, Dentin treatedwith erbium:YAG laser (100 mJ, 15 Hz). Note effective debris removal. B, Control, unlased dentin surface. C, Dentin surface treated with Nd:YAG laser(80 mJ, 10 Hz). Note melted and recrystallized dentin surface. Reproduced with permission from Cecchini SCM et al.537
964 / Endodontics

root canal system, while possible,550,551 is notstraightforward. Moreover, preliminary in vivoresults are mixed and the technique is currently notcommercially available.247
Canal Surface Modification
It has been established that mechanical canal prepara-tion142 alone cannot predictably remove microbialcanal contaminants and therefore irrigation with anti-microbial solutions is recommended. The effect ofvarious irrigants and medicaments is described inChapter 28, ‘‘Irrigants and Intracanal Medicaments’’but some issues pertinent to canal preparation will bedetailed below.
In addition to the removal of soft tissue and micro-organisms, the canal surface is modified by irrigation
solutions.552 Canal surface after shaping with mechan-ical instruments is characterized by an irregularly dis-tributed layer of soft and hard tissue debris that issmeared onto dentin surfaces (Figure 72).553–555 This1- to 5-�m-thin superficial structure consists of twoseparate layers: a loose superficial layer and anattached layer that also extends into dentinal tubulesto form occluding plugs.421 A smear layer consists ofseveral components: dentin ‘‘mud,’’ remnants ofodontoblastic processes, pulp tissue, and microorgan-isms.554 Its appearance and structure differs depend-ing on the contacting instrument’s cutting action:more actively cutting blades shear off dentin leavingthinner smear layer, while U-blade designs tend toburnish a thicker smear layer deeper into dentinaltubuli.556,557
The question as whether to leave the smear layer insitu on the canal walls or to remove it has been a
Figure 71 Application of the noninstrumentation technique for root canal cleaning and filling. A, Principle and clinical placement of the tubing system.The pump is connected to a tubing system and via a three-way valve to a cannula. This cannula is sealed into the access cavity with impression materialto provide an air-tight system. B, After removal of the soft tissue with oscillating pressure waves of sodium hypochlorite (NaOCl), highly viscous sealer isdelivered into the canal system at low pressure. Micrographs show adaptation of sealer at canal walls and also diffusion of sealer stained with red dyeinto the dentinal tubules. Images courtesy of Prof. Adrian Lussi.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 965

matter of debate for more than 50 years. For example,some authors reported that the presence of a smearlayer delays but does not eliminate disinfection;558 itmay also increase microleakage after canal obtura-tion.554 In contrast, other researchers suggested thatthe presence of a smear layer, while acting as a barrier,might block irrigation solutions from entering thedentinal tubules.555,559 Others reported that a smearlayer might act as a beneficial barrier preventingmicroorganisms from entering dentinal tubules whena root canal is contaminated between appointments.Their microbiological analyses of split root halvesshowed that the early removal of the smear layermay lead to significantly higher bacteria counts.560
Smear layer removal may be accomplished by var-ious chemicals, as suggested over the last 50 years(Table 12), ranging from EDTA382 to bisphospho-nates.552 Earlier studies had suggested a synergisticmechanism with EDTA removing the organic smearlayer and then subsequently allowing NaOCl betteraccess to deeper calcified layers;145 recent work hasdemonstrated that EDTA and NaOCl show chemicalinteractions;373 similar interactions were demon-strated between citric acid and NaOCl.552 These inter-actions greatly reduce NaOCl efficacy and suggestattention to irrigation sequencing. In fact, the oftencited ‘‘bubbling’’ that occurs between EDTA andNaOCl suggests that the active component of NaOCl,chlorine, is released from the solution and hence doesnot actively kill microorganisms.
Salvizol is another root canal chelating irrigant thathas a broad spectrum of bactericidal activity. This
gives the product a cleansing potency while beingbiologically compatible.570 Kaufman567 reported thesuccess of several cases using bis-dequalinium acetateas a disinfectant and chemotherapeutic agent. Hecited its low toxicity, lubrication action, disinfectingability, and low surface tension, as well as its chelatingproperties and low incidence of posttreatment pain.
Figure 72 Appearance of root canal walls in a scanning electron micrograph. The smear layer was partially removed; there is a thin smear layer presentin the area that was touched by an instrument (left half). Hard tissue debris and predentin calcospherites (arrowhead) were present in the area that wasnot instrumented but had soft tissue removed by sodium hypochlorite (right half).
Table 12 Available and Potential Solutions and Pastes forSmear Layer Removal.
Reference Year Chemical
Baumgartner561 1984 Citric acid 10%
Wayman562 1979 Citric acid 20%
Tidmarsh563 1978 Citric acid 40%
Nygaard-Østby382 1957 EDTA (15%, ethylenediamineacetate)
Fehr383 1963 EDTAC (15% EDTA plus cetrimide)
Stewart564 1969 RC Prep (Premier Dental, Philadelphia, PA)
(10% urea peroxide, 15% EDTA)*
Koskinen565 1975 Tubulicid (38% benzalkonium chloride, EDTA,
50% citric acid)
Koskinen566 1980 Largal Ultra (Septodont, Paris, France), 15%
EDTA, cetrimide, NaOH)
Kaufman567 1981 Salvizol (Ravensberg, Konstanz, Germany),
5% aminoquinaldinium diacetate,
propylene glycol
Berry568 1987 40% polyacrylic acid
Torabinejad569 2003 MTAD (Densply Tulsa Dental) (4.25% citric
acid, 3% doxycycline, 0.5% Tween 80)
Zehnder552 2005 HEBP (7% 1-hydroxyethylidene-1,
1-bisphosphonate)
*Other preparations are similar, for example, Glyde (Dentsply Maillefer), File
Care (VDW), FileEze (Ultradent), except for the base that could be carbowax or
glycerine.
966 / Endodontics
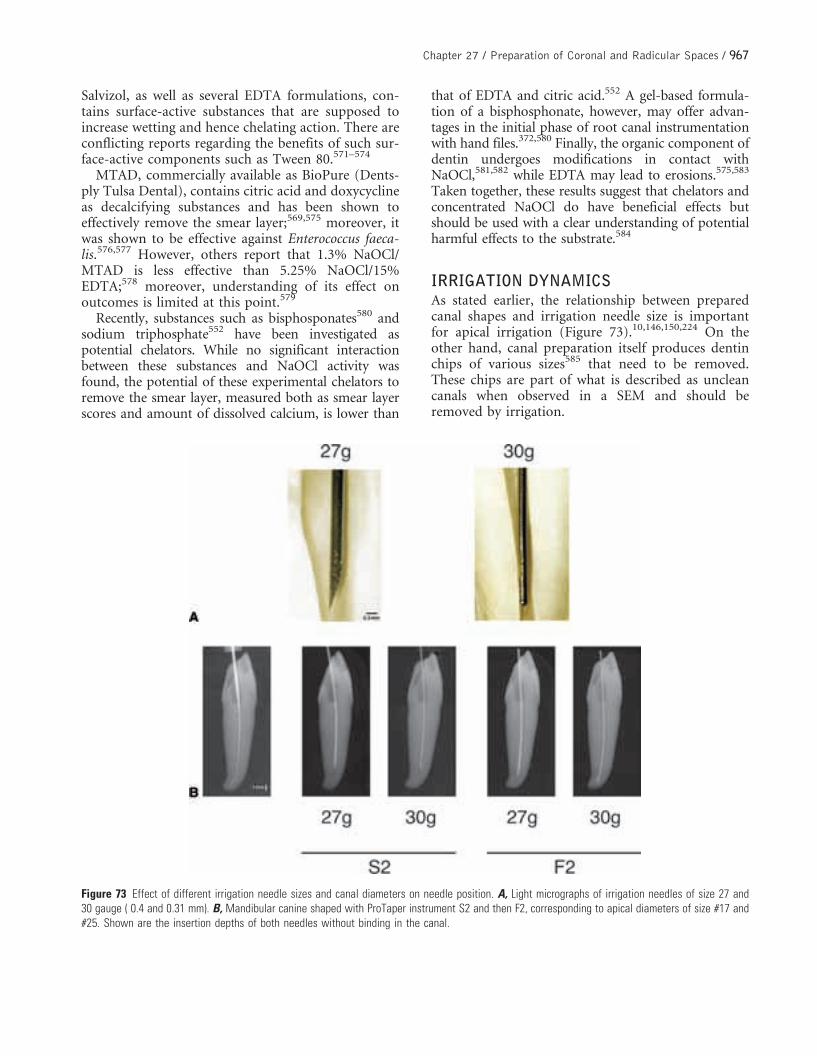
Salvizol, as well as several EDTA formulations, con-tains surface-active substances that are supposed toincrease wetting and hence chelating action. There areconflicting reports regarding the benefits of such sur-face-active components such as Tween 80.571–574
MTAD, commercially available as BioPure (Dents-ply Tulsa Dental), contains citric acid and doxycyclineas decalcifying substances and has been shown toeffectively remove the smear layer;569,575 moreover, itwas shown to be effective against Enterococcus faeca-lis.576,577 However, others report that 1.3% NaOCl/MTAD is less effective than 5.25% NaOCl/15%EDTA;578 moreover, understanding of its effect onoutcomes is limited at this point.579
Recently, substances such as bisphosponates580 andsodium triphosphate552 have been investigated aspotential chelators. While no significant interactionbetween these substances and NaOCl activity wasfound, the potential of these experimental chelators toremove the smear layer, measured both as smear layerscores and amount of dissolved calcium, is lower than
that of EDTA and citric acid.552 A gel-based formula-tion of a bisphosphonate, however, may offer advan-tages in the initial phase of root canal instrumentationwith hand files.372,580 Finally, the organic component ofdentin undergoes modifications in contact withNaOCl,581,582 while EDTA may lead to erosions.575,583
Taken together, these results suggest that chelators andconcentrated NaOCl do have beneficial effects butshould be used with a clear understanding of potentialharmful effects to the substrate.584
IRRIGATION DYNAMICSAs stated earlier, the relationship between preparedcanal shapes and irrigation needle size is importantfor apical irrigation (Figure 73).10,146,150,224 On theother hand, canal preparation itself produces dentinchips of various sizes585 that need to be removed.These chips are part of what is described as uncleancanals when observed in a SEM and should beremoved by irrigation.
Figure 73 Effect of different irrigation needle sizes and canal diameters on needle position. A, Light micrographs of irrigation needles of size 27 and30 gauge ( 0.4 and 0.31 mm). B, Mandibular canine shaped with ProTaper instrument S2 and then F2, corresponding to apical diameters of size #17 and#25. Shown are the insertion depths of both needles without binding in the canal.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 967

Irrigation is commonly applied by a syringe and aneedle, with needle sizes varying typically between 27and 30 gauge (see Figure 73), 0.635 and 0.305 mm,respectively. With such a system, irrigation solutionswill not travel apically more than 1 mm beyond thetip of the needle.307,586 While it is therefore desirableto place the irrigation needle into the shaped rootcanals, the needle must not be locked in to avoidexpressing the irrigation solution into periapical tis-sues. Serious incidents have been reported followingNaOCl expressed into maxillary sinus or close tonerves.587–590
With careful use, the benefits of deep intracanalirrigation clearly seem to outweigh the risks.591 In factthe proximity of the irrigation needle to the apex playsan important role in removing root canal debris.592
Druttman and Stock593 found that irrigation perfor-mance varied with the size of the needle and thevolume of the irrigant, while Walton and Torabine-jad594 stated in their textbook that perhaps the mostimportant factor is the delivery system and not theirrigating solution per se.
Canal size and shape are crucial to the penetration ofthe irrigant. The apical 5 mm are not flushed until theyhave been enlarged to size #30 and more often size #40file.146,595–597 Small-diameter needles were found to bemore effective in reaching adequate depth but were moreprone to problems of possible breakage and difficulty inexpressing the irrigant from the narrow needles.591
Recently, Hsieh et al.224 compared a shaped rootcanal to a ‘‘wind tunnel’’ and evaluated the behaviorof irrigation solutions deposited into various depths offlared canals from irrigation needles measuring from23 to 27 gauge. They showed that an undisturbedlaminar flow of irrigants occurred with a combinationof sufficiently enlarged canals, deep needle insertion,and small needle diameter, for example, a 27-gaugeneedle placed 3 mm from the apex in a canal preparedto size #30. Similar observations had been made earlierin experiments using radiopaque irrigation solutions(Machtou P, personal communication).
Several methods have been devised to increase irri-gant turnover and overall efficacy. As mentioned
earlier, the use of ultrasonic or sonic irrigation toremove dentin filings, debris, and bacteria from rootcanals has been well documented (Figure 62 andFigure 74).123,147,222,351,417,598,599
However, there are doubts that passive ultrasoni-cally or sonically assisted irrigation can in fact removeall contaminants.600,601 While the time frames andsequence of irrigation solutions is still a matter ofdebate,149,602 the cleanest canals were produced byirrigating with ultrasonics and NaOCl after the canalhas been fully prepared. Ultrasonics was shown to besuperior to syringe irrigation alone when the canalwas prepared to 0.3 mm (size #30 instrument).603
Several novel strategies have been proposed toincrease irrigation efficacy. Gutarts et al.546 evaluatedthe use of a 25-gauge irrigation needle, connected toan ultrasonic unit, through which 6% NaOCl wasdelivered for 1 minute at the conclusion of canalshaping. They reported significantly cleaner canalscompared to a control group that did not receiveultrasonic irrigation.
Irrigation with positive pressure has also been tried,for example, with the system RinsEndo (Duerr,Bietigheim-Bissingen, Germany). However, reportsfor this particular device are sparse;604 moreover,there is a potential for apical extrusion of NaOCl,and the necessary precautions should be taken.
More recently, Fukumoto et al.547 described anexperimental system that consisted of a washing nee-dle, placed just into the root canal, and a 27-gaugeaspiration needle, ground flat at the tip and placeddeep into the shaped root canal. Irrigants, 14% EDTAand 6% NaOCl, were aspirated at ~20 kPa; theirresults showed superior smear layer removal com-pared to a control group that received conventionalirrigation with a needle of the same diameter.
This system is similar to a patent submitted bySchoeffel545 with the exception that his system doesnot include a constantly operating washing line(Figure 75). Irrigant is deposited into the access cav-ity; then, two sequentially operated and speciallydesigned aspiration needles are placed into the shapedroot canal. Preliminary data suggest good cleaning
968 / Endodontics

capacity;605 however, currently no published resultsare available regarding clinical outcomes using thesenew irrigation techniques.
Currently, ultrasonically activated passive irrigationseems to be the standard until more experimentaltechniques are scientifically evaluated and brought tothe market. However, as mentioned earlier, using anultrasonically activated insert deep in a root canal
carries some risk (see Figure 63). Furthermore, morework is needed to clarify insert shapes and materialsas well as activation times and power settings.
PHOTODYNAMIC THERAPYWhile lasers are probably not a good alternative formechanical root canal preparation, they have been
Figure 74 Canal surfaces as seen in scanning electron micrographs. A, Typical appearance after cleaning and shaping with wall areas that hasinstrument contact and some smear layer removal as well as uninstrumented areas with calcospherites as part of the mineralization front in predentin(arrow). B, Uninstrumented canal that was washed with 5.25% sodium hypochlorite (NaOCl). C, Canal wall segment presenting with all dentinal tubulesopen. D, Completely shaped canal wall area with a thin remaining smear layer. Bars are 30 �m.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 969

shown to be effective for canal disinfection and canalsurface modification, as reviewed in detail in Chapter26E, ‘‘Lasers’’. In this context, the use of lasers for photo-activated disinfection, also known as photodynamictherapy, has been promoted.606–608 This technique doesnot provide canal enlargement but assists in the eradica-tion of intracanal microorganisms. Photodynamic ther-apy is well known as a treatment for cancer and otherdiseases609 and is based on the concept that a nontoxicphotosensitizing agent can be preferentially localized intarget tissues. The agent is then activated by light ofappropriate wavelength to generate reactive moleculesthat in turn are toxic to cells of the target tissue.609 Visiblelight can also kill bacteria in root canal systems aftertreatment with an appropriate agent (Kishen A, personalcommunication).
Such photoactivated disinfection has only recentlybeen explored to treat bacterial infections inhumans.606 A wide range of oral bacteria could bekilled by red light after sensitization with toluidine blueand methylene blue.610 More than 400 photoactivesubstances are known that can be combined with laserstailored to their specific wavelengths of absorption.Potentially one of these substances will be able topenetrate into the root canal system better than cur-rently available irrigants. In fact, partial inactivation ofStreptococcus intermedius biofilms in root canals ofextracted teeth using toluidine blue and light appliedat the orifice level has been recently reported.611
Clinically, the photoactivated agent is used as anirrigant after mechanical canal enlargement (Figure76) and activation; root canal filling is accomplished
Figure 75 The EndoVac system (Discus Dental) for apical negative pressure irrigation. Recent in vitro results demonstrate better debridement comparedto conventional syringe irrigation.605 A, Overview of the micro cannula demonstrating a closed rounded tip and an array of 12 openings in the apical end(inset, bar is 250 �m). B, Light microscopic images of canals irrigated with conventional syringe (left) and with the EndoVac system (right). Orig. mag. x100.Images courtesy of Dr. John Schoeffel.
970 / Endodontics

conventionally. This technique is experimental and itsimpact on clinical outcomes needs to be evaluated.
Conclusion
The past decade has brought significant changes toroot canal preparation, for example, the use of rotary
NiTi instruments and magnification. These techni-ques have allowed more complicated root canal treat-ment to be undertaken safely and successfully (Figure77). The way educational content is delivered is alsochanging: private educational institutions are takingthe lead in presenting information to clinicians.Moreover, electronic media and web-based contenthave gained more widespread acceptance. Using these
Figure 76 Use of photoactivated disinfection in a case of post-endodontic disease. The existing root canal filling was removed (Arrowhead) and thecanals reshaped with ProFile instruments (upper panel). Then, tolonium chloride (also known as toluidine blue O) was placed in the root canal system andirradiated with a diode laser (lower panel, also showing root canal filling after retreatment). Images courtesy of Prof. Paul Lambrechts.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 971

avenues, evidence-based information will reach clin-icians who at present have limited access to book,journals, or hands-on teaching.
Aseptic techniques are a prerequisite for successfulendodontic therapy as they are in the goal of eradicat-ing the causative microbial flora (Figure 78). Askedfor any particular direction for development in thenext decade, disinfection and systems to increase itsefficacy are the most likely candidates. Seemingly exo-tic applications such as the use of ozone (e.g., Healo-zone, KaVo, Biberach, Germany) or high-frequency
current (Endox, Lysis, Nova Milanese, Italy)612 orphotoactivated disinfection may be utilized more;however, it will be difficult to prove with statisticalmethods that any individual device will have signifi-cant and clinically relevant impact.
Regarding instrument and strategies, new materialsmay appear, such as more durable and flexible alloysor plastic materials, but the basic strategy will likelyremain the same in the next decade: enlargement forsubsequent disinfection and filling. The long-termgoal is certainly to replace root canal therapy, as part
Figure 77 Routine cases of second maxillary and mandibular molars that had coronal and radicular preparation done adhering to the principles laid outin this chapter. Radiographs represent situation immediately after root canal filling.
972 / Endodontics

of current repair methods, with tissue-engineeringstrategies that provide healing in the sense of a resti-tutio ad integrum.
ACKNOWLEDGMENT
The authors would like to express their specialgratitude to Vickie Leow, Master Graphic Designerat the UCSF School of Dentistry, as well as Anjan Lallfor their expert help with the schematic drawings usedin this chapter.
References
1. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgi-cal exposures of dental pulps in germ-free and conventionallaboratory rats. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1965;20:340.
2. Moller AJ, Fabricius L, Dahlen G, et al. Influence on peria-pical tissues of indigenous oral bacteria and necrotic pulptissue in monkeys. Scand J Dent Res 1981;89:475.
3. Schilder H. Cleaning and shaping the root canal. Dent ClinNorth Am 1974;18:269.
4. Abbott PV. Assessing restored teeth with pulp and periapicaldiseases for the presence of cracks, caries and marginalbreakdown. Aust Dent J 2004;49:33.
5. Mannan G, Smallwood ER, Gulabivala K. Effects of accesscavity location and design on degree and distribution ofinstrumented root canal surface in maxillary anterior teeth.Int Endod J 2001;34:176.
6. Sonntag D, Mollaakbari K, Kock K, Stachniss V. Einfluss derZugangskavitat auf Hartsubstanzverlust und Kanaldetektionbei humanen Frontzahnen. Dtsch Zahnarztl Z 2006;61:612.
7. Green D. A stereomicroscopic investigation of the rootapices of 400 maxillary and mandibular anterior teeth. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1956;9:1224.
8. Wu M-K, Barkis D, Roris A, Wesselink PR. Does the first fileto bind correspond to the diameter of the canal in the apicalregion. Int Endod J 2002;35:264.
9. Card SJ, Sigurdsson A, Ørstavik D, Trope M. The effective-ness of increased apical enlargement in reducing intracanalbacteria. J Endod 2002;28:779.
10. Usman N, Baumgartner JC, Marshall JG. Influence of instru-ment size on root canal debridement. J Endod 2004;30:110.
11. Nguy D, Sedgley C. The influence of canal curvature on themechanical efficacy of root canal irrigation in vitro usingreal-time imaging of bioluminescent bacteria. J Endod2006;32:1077.
12. Mickel AK, Chogle S, Liddle J, et al. The role of apical sizedetermination and enlargement in the reduction of intraca-nal bacteria. J Endod 2007;33:21.
Figure 78 Aseptic techniques and disinfection of the root canal system.A, Swabbing of the operation site, for example, with sodium hypochlorite(arrow), while marginal imperfections of the rubber dam seal are correctedwith a caulking material (e.g., Oraseal, Ultradent). B, Reservoir of sodiumhypochlorite (NaOCl) is always present in the access cavity during handand rotary instrumentation to promote disinfection and lubrication.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 973

13. Coldero LG, McHugh S, MacKenzie D, Saunders WP.Reduction in intracanal bacteria during root canal prepara-tion with and without apical enlargement. Int Endod J2002;35:437.
14. Cunningham CJ, Senia ES. A three-dimensional study ofcanal curvatures in the mesial roots of mandibular molars.J Endod 1992;18:294.
15. Peters OA, Laib A, Gohring TN, Barbakow F. Changes inroot canal geometry after preparation assessed by high-reso-lution computed tomography. J Endod 2001;27:1.
16. Peters OA, Peters CI, Schonenberger K, Barbakow F. ProTa-per rotary root canal preparation: effects of canal anatomyon final shape analysed by micro CT. Int Endod J2003;36:86.
17. Zillich RM, Jerome JK. Endodontic access to maxillary lat-eral incisors. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1981;52:443.
18. LaTurno SA, Zillich RM. Straight-line endodontic access toanterior teeth. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1985;59:418.
19. Dempster WT, Adams WJ, Duddles RA. Arrangement in thejaws of the roots of the teeth. J Am Dent Assoc 1963;67:779.
20. Acosta Vigouroux SA, Trugeda Bosaans SA. Anatomy of thepulp chamber floor of the permanent maxillary first molar. JEndod 1978;4:214.
21. Bjørndal L, Carlsen O, Thuesen G, Darvann T, KreiborgS. External and internal macromorphology in 3D-reconstructed maxillary molars using computerizedX-ray microtomography. Int Endod J 1999;32:3.
22. Krasner P, Rankow HJ. Anatomy of the pulp-chamber Floor.J Endod 2004;30:5.
23. Hess W, Zurcher E. The anatomy of root canals of the teethof the permanent and deciduous dentitions.New York: Wil-liam Wood; 1925.
24. Peters OA, Gohring TN, Lutz F. Effect of a eugenol-contain-ing sealer on marginal adaptation of dentine-bonded resinfillings. Int Endod J 2000;33:53.
25. Janik JM. Access cavity preparation. Dent Clin North Am1984;28:809.
26. Sorensen JA, Engelman MJ. Ferrule design and fractureresistance of endodontically treated teeth. J Prosthet Dent1990;63:529.
27. Libman WJ, Nicholls JI. Load fatigue of teeth restored withcast posts and cores and complete crowns. Int J Prosthodont1995;8:155.
28. Creugers NH. 5-year follow-up of a prospective clinicalstudy on various types of core restorations. Int J Prostho-dont 2005;18:34.
29. Tan PL, Aquilino SA, Gratton DG, Stanford CM, et al. Invitro fracture resistance of endodontically treated centralincisors with varying ferrule heights and configurations.J Prosthet Dent 2005;93:331.
30. Stokes AN, Tidmarsh BG. A comparison of diamond andtungsten carbide burs for preparing endodontic access cav-ities through crowns. J Endod 1988;14:550.
31. Teplitsky PE, Sutherland JK. Endodontic access of Cerestorecrowns. J Endod 1985;11:555.
32. Cohen BD, Wallace JA. Castable glass ceramic crowns andtheir reaction to endodontic therapy. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1991;72:108.
33. Ash MM, Nelson SJ. Wheeler’s dental anatomy, physiologyand occlusion. 8th ed. Philadelphia, PA: WB Saunders; 2003.
34. Pineda F, Kuttler Y. Mesiodistal and buccolingual roent-genographic investigation of 7,275 root canals. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1972;33:101.
35. Vertucci FJ. Root canal anatomy of the human permanentteeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1984;58:589.
36. Hamasa AA, Al-Khateeb T, Darwazeh A. Prevalence of dila-ceration in Jordanian adults. Int Endod J 2002;35:910.
37. Kasahara E, Yasuda E, Yamamoto A, Anzai M. Root canalsystem of the maxillary central incisor. J Endod 1990;16:158.
38. Genovese FR, Marsico EM. Maxillary central incisor withtwo roots: a case report. J Endod 2003;29:220.
39. Lin WC, Yan SF, Pai SF. Non-surgical endodontic treatmentof a two rooted maxillary central incisor. J Endod2006;32:478.
40. Khademi J. Endodontic Access. In: Johnson WT, editor.Color atlas of endodontics. Philadelphia, PA: WB Saunders;2002. p. 21.
41. Christie WH, Peikoff MD, Acheson DW. Endodontic treat-ment of two maxillary lateral incisors with anomalous rootformation. J Endod 1981;7:528.
42. Fried IL, Winter AA. Diagnosis and treatment of a two-rooted maxillary lateral incisor. Periodont Case Rep1984;6:40.
43. Yoshikawa M, Hosomi T, Sakiyama Y, Toda T. Endodontictherapy for a permanent maxillary lateral incisor having tworoots. J Osaka Dent Univ 1987;21:87.
44. Hatton JF, Ferrillo PJ Jr. Successful treatment of a two-canaled maxillary lateral incisor. J Endod 1989;15:216.
45. Caliskan MK, Pehlivan Y, Sepetcioglu F, et al. Root canalmorphology of human permanent teeth in a Turkish popu-lation. J Endod 1995;21:200.
46. Carns EJ, Skidmore AE. Configurations and deviations ofroot canals of maxillary first premolars. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1973;36:880.
47. Vertucci FJ, Gegauff A. Root canal morphology of the max-illary first premolar. J Am Dent Assoc 1979;99:194.
48. Walker RT. Root form and canal anatomy of maxillary firstpremolars in a southern Chinese population. Endod DentTraumatol 1987;3:130.
974 / Endodontics

49. Pecora JD, Saquy PC, Sousa Neto MD, Woelfel JB. Rootform and canal anatomy of maxillary first premolars. BrazDent J 1991;2:87.
50. Kartal N, Ozcelilk B, Cimilli H. Root canal morphology ofmaxillary premolars. J Endod 1998;24:417.
51. Kerekes K, Tronstad L. Morphometric observations on rootcanals of human premolars. J Endod 1977;3:74.
52. Bellizzi R, Hartwell G. Radiographic evaluation of root canalanatomy of in vivo endodontically treated maxillary premo-lars. J Endod 1985;11:37.
53. Green D. Double canals in single roots. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1973;35:689.
54. Sert S, Bayirli GS. Evaluation of the root canal configura-tions of the mandibular and maxillary permanent teeth bygender in the Turkish population. J Endod 2004;30:391.
55. Gilles J, Reader A. An SEM investigation of the mesiolingualcanal in human maxillary first and second molars. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1990;70:638.
56. Buhrley LJ, Barrows MJ, BeGole E, Wenckus CS. Effect ofmagnification on locating the mb2 canal in maxillarymolars. J Endod 2002;28:324.
57. Fogel HM, Peikoff MD, Christie WH. Canal configuration inthe mesiobuccal root of the maxillary first molar: a clinicalstudy. J Endod 1994;20:135.
58. Pomeranz HH, Fishelberg G. The secondary mesiobuccalcanal of maxillary molars. J Am Dent Assoc 1974;88:119.
59. Seidberg BH, Altman M, Guttuso J, Suson M. Frequency oftwo mesiobuccal root canals in maxillary permanent firstmolars. J Am Dent Assoc 1973;87:852.
60. Thomas RP, Moule AJ, Bryant R. Root canal morphology ofmaxillary permanent first molar teeth at various ages. IntEndod J 1993;26:257.
61. Kulild JC, Peters DD. Incidence and configuration of canalsystems in the mesiobuccal root of maxillary first and secondmolars. J Endod 1990;16:311.
62. Al-Shalabi RM, Omer OE, Glennon J, et al. Root canalanatomy of maxillary first and second permanent molars.Int Endod J 2000;33.
63. Weine FS, Hayami S, Hata G, Toda T. Canal configurationof the mesiobuccal root of the maxillary first molar of aJapanese sub-population. Int Endod J 1999;32:79.
64. Alavi AM, Opasanon A, Ng Y-L, Gulabivala K. Root andcanal morphology of Thai maxillary molars. Int Endod J2002;35:478.
65. Imura N, Hata GI, Toda T, et al. Two canals in mesiobuccalroots of maxillary molars. Int Endod J 1998;31:410.
66. Weine FS, Healey HJ, Gerstein H, Evanson L. Canal config-uration in the mesiobuccal root of the maxillary first molarand its endodontic significance. Oral Surg Oral Med OralPathol Oral Radiol Endod 1969;28:419.
67. Stropko J. Canal Morphology of maxillary molars:clinical observations on canal configurations. J Endod1999;25:446.
68. Wasti F, Shearer AC, Wilson NH. Root canal systems of themandibular and maxillary first permanent molar teeth ofsouth Asian Pakistanis. Int Endod J 2001;34:263.
69. Ng YL, Aung TH, Alavi A, Gulabivala K. Root and canalmorphology of Burmese maxillary molars. Int Endod J2001;34:620.
70. Baldassari-Cruz LA, Lilly JP, Rivera EM. The influence ofdental operating microscope in locating the mesiolingualcanal orifice. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2002;93:190.
71. Eskoz N, Weine FS. Canal configuration of the mesiobuccalroot of the maxillary second molar. J Endod 1995;21:38.
72. Peikoff MD, Christie WH, Fogel HM. The maxillary secondmolar: variations in the number of roots and canals. IntEndod J 1996;29:365.
73. Rankine-Wilson RW, Henry PJ. The bifurcated root canal inlower anterior teeth. J Am Dent Assoc 1965;70:1162.
74. Madeira MC, Hetem S. Incidence of bifurcations in man-dibular incisors. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1973;36:589.
75. Benjamin KA, Dowson J. Incidence of two root canals inhuman mandibular incisor teeth. Oral Surg Oral Med OralPathol Oral Radiol Endod 1974;38:122.
76. Kartal N, Yanikoglu FC. Root canal morphology of mandib-ular incisors. J Endod 1992;18:562.
77. Miyashita M, Kasahara E, Yasuda E, et al. Root canal systemof the mandibular incisor. J Endod 1997;23:479.
78. Bellizzi R, Hartwell G. Clinical investigation of in vivoendodontically treated mandibular anterior teeth. J Endod1983;9:246.
79. Walker RT. The root canal anatomy of mandibular incisorsin a southern Chinese population. Int Endod J 1988;21:218.
80. Al-Qudah AA, Awawdeh LA. Root canal morphology ofmandibular incisors in a Jordanian population. Int EndodJ 2006;39:873.
81. Mauger MJ, Waite RM, Alexander JB, Schindler WG. Idealendodontic access in mandibular incisors. J Endod1999;25:206.
82. Heling I, Gottlieb-Dadon I, Chandler NP. Mandibularcanine with two roots and three root canals. Endod DentTraumatol 1995;11:301.
83. Orguneser A, Kartal N. Mandibular canine with two rootsand three canals. Endod Dent Traumatol 1998;11:301.
84. Vertucci FJ. Root canal morphology of mandibular premo-lars. J Am Dent Assoc 1978;97:47.
85. Baisden MK, Kulild JC, Weller RN. Root canal configurationof the mandibular first premolar. J Endod 1992;18:505.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 975

86. Zillich R, Dowson J. Root canal morphology of mandibularfirst and second premolars. Oral Surg Oral Med Oral PatholOral Radiol Endod 1973;36:738.
87. Yoshioka TV, Villegas JC, Kobayashi C, Suda H. Radio-graphic evaluation of root canal multiplicity in mandibularfirst premolars. J Endod 2004;30:73.
88. Nallapati S. Three canal mandibular first and second pre-molars: a treatment approach. A case report. J Endod2005;31:474.
89. Bram SM, Fleisher R. Endodontic therapy in a mandibularsecond bicuspid with four canals. J Endod 1991;17:513.
90. Holtzman L. Root canal treatment of mandibular secondpremolar with four root canals: a case report. Int Endod J1998;31:364.
91. Rhodes JS. A case of unusual anatomy: a mandibular secondpremolar with four canals. Int Endod J 2001;34:645.
92. Macri E, Zmener O. Five canals in a mandibular secondpremolar. J Endod 2000;26:304.
93. Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canalmorphology of Thai mandibular molars. Int Endod J2002;35:56.
94. Zaatar EI, Anizi SA, Al-Duwairi Y. A study of the dentalpulp cavity of mandibular first permanent molars in theKuwaiti population. J Endod 1998;24:125.
95. Skidmore AE, Bjorndal AM. Root canal morphology of thehuman mandibular first molar. Oral Surg Oral Med OralPathol Oral Radiol Endod 1971;32:778.
96. Walker RT. Root form and canal anatomy of mandibularfirst molars in a southern Chinese population. Endod DentTraumatol 1988;4:19.
97. Pomeranz HH, Eidelman DL, Goldberg MG. Treatmentconsiderations of the middle mesial canal of mandibularfirst and second molars. J Endod 1981;7:565.
98. Fabra-Campos H. Unusual root anatomy of mandibular firstmolars. J Endod 1985;11:568.
99. da Costa LF, Sousa Neto MD, Fidel SR, et al. External andinternal anatomy of mandibular molars. Braz Dent J1996;7:33.
100. Mannocci F, Peru M, Sheriff M, et al. The isthmuses of themesial root of mandibular molars: a micro-computed tomo-graphic study. Int Endod J 2005;38:558.
101. Fabra-Campos H. Three canals in the mesial root of man-dibular first permanent molars: a clinical study. Int Endod J1989;22:39.
102. Vertucci FJ, Williams RG. Furcation canals in the humanmandibular first molar. Oral Surg Oral Med Oral PatholOral Radiol Endod 1974;38:308.
103. Vertucci FJ, Anthony RL. A scanning electron microscopicinvestigation of accessory foramina in the furcation and pulpchamber floor of molar teeth. Oral Surg Oral Med OralPathol Oral Radiol Endod 1986;62:319.
104. Rice RT, Gilbert BO Jr. An unusual canal configuration in amandibular first molar. J Endod 1987;13:515.
105. Bolger WL, Schindler WG. A mandibular first molar with aC-shaped root configuration. J Endod 1988;14:515.
106. Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canalmorphology of Burmese mandibular molars. Int Endod J2001;34:359.
107. Cooke HG III, Cox FL. C-shaped canal configurations inmandibular molars. J Am Dent Assoc 1979;99:836.
108. Weine FS. The C-shaped mandibular second molar: inci-dence and other considerations (with members ofthe Arizona Endodontic Association). J Endod 1998;24:372.
109. Melton DC, Krell KV, Fuller MW. Anatomical and histolo-gical features of C-shaped canals in mandibular secondmolars. J Endod 1991;17:384.
110. Sorensen JA, Martinoff JT. Intracoronal reinforcement andcoronal coverage: a study of endodontically treated teeth. JProsthet Dent 1984;51:780.
111. Rosen H. Operative procedures on mutilated endodonticallytreated teeth. J Prosthet Dent 1961;11:972.
112. Johnson JK, Schwartz NL, Blackwell RT. Evaluation andrestoration of endodontically treated posterior teeth. J AmDent Assoc 1976;93:597.
113. Greenfeld RS, Marshall FJ. Factors affecting dowel (post)selection and use in endodontically treated teeth. J Can DentAssoc 1983;49:777.
114. Radke RA, Eissmann HF. Postendodontic restoration. In:Cohen S, Burns RC, editors. Pathways of the pulp. 5th ed.St. Louis, MO: CV Mosby; 1991.
115. Helfer AR, Melnick S, Schilder H. Determination of themoisture content of vital and pulpless teeth. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1972;34:661.
116. Reeh ES, Messer HH, Douglas WH. Reduction in toothstiffness as a result of endodontic and restorative procedures.J Endod 1989;15:512.
117. Howe CA, McKendry DJ. Effect of endodontic access pre-paration on resistance to crown–root fracture. J Am DentAssoc 1990;121:712.
118. Sedgley CM, Messer HH. Are endodontically treated teethmore brittle? J Endod 1992;18:332.
119. Panitvisai P, Messer HH. Cuspal deflection in molars inrelation to endodontic and restorative procedures. J Endod1995;21:57.
120. Peters OA. Current challenges and concepts in the prepara-tion of root canal systems: a review. J Endod 2004;30:559.
121. Peters OA, Dummer PM. Infection control through rootcanal preparation: a review of cleaning and shaping proce-dures. In: Peters OA, Dummer PM, editors. EndodonticTopics. Copenhagen, Denmark: Blackwell Munksgaard;2005.
976 / Endodontics

122. Hulsmann M, Peters OA, Dummer PMH. Mechanical pre-paration of root canals: shaping goals, techniques andmeans. Endod Top 2005;10:30.
123. Sjogren U, Sundqvist G. Bacteriologic evaluation of ultra-sonic root canal instrumentation. Oral Surg Oral Med OralPathol Oral Radiol Endod 1987;63:366.
124. Yared GM, Bou Dagher FE. Influence of apical enlargementon bacterial infection during treatment of apical periodonti-tis. J Endod 1994;20:535.
125. Dalton BC, Ørstavik D, Phillips C, et al. Bacterial reductionwith nickel-titanium rotary instrumentation. J Endod1998;24:763.
126. Peters LB, Wesselink PR. Periapical healing of endodonti-cally treated teeth in one and two visits obturated in thepresence or absence of detectable microorganisms. IntEndod J 2002;35:660.
127. McGurkin-Smith R, Trope M, Caplan D, Sigurdsson A. Reduc-tion of intracanal bacteria using GT rotary instrumentation,5.25% NaOCl, EDTA, and Ca(OH)2. J Endod 2005;31:359.
128. Brynolf I. A histological and roentgenological study of theperiapical region of human incisors. Odontol Revy1967;18(Suppl 11).
129. Green TL, Walton RE, Taylor JK, Merrell P. Radiographicand histologic periapical findings of root canal treated teethin cadaver. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1997;83:707.
130. Barthel CR, Zimmer S, Trope M. Relationship of radiologicand histologic signs of inflammation in human root-filledteeth. J Endod 2004;30:75.
131. Strindberg L. The dependence of the results of pulp therapyon certain factors. Acta Odontol Scand 1956;14(Suppl 21).
132. Nair PN, Henry S, Cano V, Vera J. Microbial status of apicalroot canal system of human mandibular first molars withprimary apical periodontitis after ‘‘one-visit’’ endodontictreatment. Oral Surg Oral Med Oral Path Oral Radiol Endod2005;99:231.
133. Peters LB, Wesselink PR, Moorer WR. The fate and the roleof bacteria left in root dentinal tubules. Int Endod J1995;28:95.
134. Saleh IM, Ruyter IE, Haapasalo M, Ørstavik D. Survival ofEnterococcus faecalis in infected dentinal tubules after rootcanal filling with different root canal sealers in vitro. IntEndod J 2004;37:193.
135. Wu MK, Dummer PM, Wesselink PR. Consequences of andstrategies to deal with residual post-treatment root canalinfection. Int Endod J 2006;39:343.
136. Fabricius L, Dahlen G, Sundqvist G, et al. Influence ofresidual bacteria on periapical tissue healing afterchemomechanical treatment and root filling of experimen-tally infected monkey teeth. Eur J Oral Sci 2006;114:278.
137. Siqueira JF. The etiology of root canal treatment failure: whywell-treated teeth can fail. Int Endod J 2001;34:1.
138. Nair PN. On the causes of persistent apical periodontitis: areview. Int Endod J 2006;39:249.
139. Iwaya SI, Ikawa M, Kubota M. Revascularization of animmature permanent tooth with apical periodontitis andsinus tract. Endod Dent Traumatol 2001;17:185.
140. Banchs F, Trope M. Revascularization of immature perma-nent teeth with apical periodontitis: new treatment protocol?J Endod 2004;30:196.
141. Love RM. Clinical management of infected root canal den-tin. Pract Periodont Aesthet Dent 1996;8:581.
142. Bystrom A, Sundqvist G. Bacteriologic evaluation of theefficacy of mechanical root canal instrumentation in endo-dontic therapy. Scand J Dent Res 1981;89:321.
143. Siqueira J, Lima K, Magalhaes F, et al. Mechanical reductionof the bacterial population in the root canal by three instru-mentation techniques. J Endod 1999;25:332.
144. Bystrom A, Sundqvist G. Bacteriologic evaluation of theeffect of 0.5 percent sodium hypochlorite in endodontictherapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1983;55:307.
145. Bystrom A, Sundqvist G. The antibacterial action of sodiumhypochlorite and EDTA in 60 cases of endodontic therapy.Int Endod J 1985;18:35.
146. Falk KW, Sedgley CM. The influence of preparation size onthe mechanical efficacy of root canal irrigation in vitro. JEndod 2005;31:742.
147. van der Sluis LW, Gambarini G, Wu MK, Wesselink PR. Theinfluence of volume, type of irrigant and flushing method onremoving artificially placed dentine debris from the apical rootcanal during passive ultrasonic irrigation. Int Endod J 2006;39:472.
148. Haapasalo M, Endal U, Zandi H, Coil JM. Eradication ofendodontic infection by instrumentation and irrigationsolutions. Endod Top 2005;10:77.
149. Zehnder M. Root canal irrigants. J Endod 2006;32:389.
150. Albrecht L, Baumgartner J, Marshall J. Evaluation of apicaldebris removal using various sizes and tapers of ProFile GTfiles. J Endod 2004;30:425.
151. Jou Y-T, Karabuchak B, Levin J, Liu D. Endodontic workingwidth: current concepts and techniques. Dent Clin NorthAm 2004;48:323.
152. Nair PMR. Apical periodontitis: a dynamic encounterbetween root canal infection and host response. Periodon-tology 2000 2000;13:121.
153. Ricucci D. Apical limit of root canal instrumentation andobturation, part1. Literature review. Int Endod J 1998;31:384.
154. Certosimo FJ, Milos MF, Walker T. Endodontic workinglength determination—where does it end? Gen Dent1999;47:281.
155. Wu MK, Wesselink PR, Walton RE. Apical terminus loca-tion of root canal treatment procedures. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2000;89:99.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 977

156. Davis WJ. Pulpectomy vs pulp-extirpation. Dent ItemsInterest 1922;44:81.
157. Kerekes K, Tronstad L. Long-term results of endodontictreatment performed with a standardized technique. J Endod1979;5:83.
158. Cailleteau JG, Mullaney TP. Prevalence of teaching apicalpatency and various instrumentation and obturation techni-ques in United States dental schools. J Endod 1997;23:394.
159. Holland R, Sant’Anna Junior A, Souza V, et al. Influence ofapical patency and filling material on healing process ofdog’s teeth with vital pulp after root canal therapy. BrazDent J 2005;19:9.
160. Sjogren U, Hagglund B, Sundqvist G, Wing K. Factorsaffecting the long-term results of endodontic treatment.J Endod 1990;16:498.
161. Izu KH, Thomas SJ, Zhang P, et al. Effectiveness of sodiumhypochlorite in preventing inoculation of periapical tissuewith contaminated patency files. J Endod 2004;30:92.
162. Beeson TJ, Hartwell GR, Thornton JD, Gunsolley JC. Com-parison of debris extruded apically in straight canals: con-ventional filing versus ProFile .04 taper series 29. J Endod1998;24:18.
163. Tinaz AC, Alacam T, Uzun O, et al. The effect of disruptionof the apical constriction on periapical extrusion. J Endod2005;31:533.
164. Souza RA. The importance of apical patency and cleaningthe apical foramen on root canal preparation. Braz DentJ 2006;17:6.
165. Parris J, Wilcox L, Walton R. Effectiveness of apical clearing:histological and radiographical evaluation. J Endod 1994;20:219.
166. Heard F, Walton RE. Scanning electron microscope studycomparing four root canal preparation techniques in smallcurved canals. Int Endod J 1997;30:323.
167. Goldberg F, Massone EJ. Patency file and apical transporta-tion: an in vitro study. J Endod 2002;28:510.
168. Kuttler Y. Microscopic investigation of root apexes. J AmDent Assoc 1955;50:544.
169. Dummer PMH, McGinn JH, Rees DG. The position andtopography of the apical canal constriction and apical fora-men. Int Endod J 1984;17:192.
170. Tidmarsh BG, Sherson W, Stalker NL. Establishing endo-dontic working length: a comparison of radiographic andelectronic methods. N Z Dent J 1985;81:93.
171. Stein TJ, Corcoran JF. Radiographic ‘‘working length’’ revis-ited. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1992;74:796.
172. Gutmann JL, Leonard JE. Problem solving in endodonticworking-length determination. Compend Contin Educ Dent1995;16:288.
173. El Ayouti A, Weiger R, Lost C. Frequency of overinstrumen-tation with an acceptable radiographic working length.J Endod 2001;27:49.
174. Glossary of endodontic terms. 7th ed. Chicago, IL: AmericanAssociation of Endodontists; 2003.
175. Palmer MJ, Weine FS, Healey HJ. Position of the apicalforamen in relation to endodontic therapy. J Can Dent Assoc1971;37:305.
176. Olson AK, Goerig AC, Cavataio RE, Luciano J. The ability ofthe radiograph to determine the location of the apical fora-men. Int Endod J 1991;24:28.
177. Green EN. Microscopic investigation of root canal dia-meters. J Am Dent Assoc 1958;57:636.
178. Green D. Stereomicroscopic study of 700 root apices ofmaxillary and mandibular posterior teeth. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1960;13:728.
179. Chapman CE. A microscopic study of the apical region ofhuman anterior teeth. J Br Endod Soc 1969;3:52.
180. Morfis A, Sylaras SN, Georgopoulou M, et al. Study of theapices of human permanent teeth with the use of a scanningelectron microscope. Oral Surg Oral Med Oral Path OralRadiol Endod 1994;77:172.
181. Guiterrez JH, Aguayo P. Apical foraminal openings inhuman teeth. Number and location. Oral Surg Oral MedOral Path Oral Radiol Endod 1995;79:769.
182. Wu MK, R’Oris A, Barkis D, Wesselink PR. Prevalence andextent of long oval canals in the apical third. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2000;89:739.
183. Briseno Marroquin B, El-Sayed MAA, Willershausen-Zonnchen B. Morphology of the physiological foramen: I.Maxillary and mandibular molars. J Endod 2004;30:321.
184. Langeland K. The histopathologic basis in endodontic treat-ment. Dent Clin North Am 1967;Nov:491.
185. Caldwell JL. Change in working length following instrumen-tation of molar canals. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1976;41:114.
186. Davis RD, Marshall JG, Baumgartner JC. Effect of earlycoronal flaring on working length change in curved canalsusing rotary nickel–titanium versus stainless steel instru-ments. J Endod 2002;28:438.
187. Sonntag D, Stachniss-Carp S, Stachniss V. Determination ofroot canal curvatures before and after canal preparation (part1): a literature review. Aust Endod J 2005;31:89.
188. Oguntebi B, Slee AM, Tanker JM, Langeland K. Predomi-nant microflora associated with human dental periapicalabscesses. J Clin Microbiol 1982;15:964.
189. Pascon EA, Introcaso JH, Langeland K. Development ofpredictable periapical lesion monitored by subtractionradiography. Endod Dent Traumatol 1987;3:192.
978 / Endodontics

190. Ricucci D, Langeland K. Apical limit of root canal instru-mentation and obturation, part 2. A histological study. IntEndod J 1998;31:394.
191. Katz A, Szajkis S, Tamse A, Tagger M. Standardization ofendodontic instruments and materials: expectations and rea-lity. Part 1: Development of the system. Refuat Ha-Shinayim1984;2:18.
192. Steffen H, Splieth CH, Behr K. Comparison of measure-ments obtained with hand files or the Canal Leader attachedto electronic apex locators: an in vitro study. Int EndodJ 1999;32:103.
193. Simon JH. The apex: how critical is it? Gen Dent1994;42:330.
194. Seidberg BH, Alibrandi BV, Fine H, Logue B. Clinical inves-tigation of measuring working lengths of root canals with anelectronic device and with digital-tactile sense. J Am DentAssoc 1975;90:379.
195. Balto KA. Modern electronic apex locators are reliable fordetermining root canal working length. Evid Based Dent2006;7:31.
196. Bramante CM, Berbert A. A critical evaluation of somemethods of determining tooth length. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1974;37:463.
197. Dummer PM, Lewis JM. An evaluation of the EndometricProbe in root canal length estimation. Int EndodJ 1987;20:25.
198. Ingle JI. Endodontics. 1st ed. Philadelphia, PA: Lea & Febi-ger; 1965.
199. Vande Voorde HE, Bjorndahl AM. Estimating endodontic‘‘working length’’ with paralleling radiographs. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1969;27:106.
200. Hoer D, Attin T. The accuracy of electronic working lengthdetermination. Int Endod J 2004;37:125.
201. El Ayouti A, Weiger R, Lost C. The ability of root ZX apexlocator to reduce the frequency of overestimated radio-graphic working length. J Endod 2002;28:116.
202. Nguyen HQ, Kaufman AY, Komorowski RC, Friedman S.Electronic length measurement using small and large files inenlarged canals. Int Endod J 1996;29:359.
203. El Ayouti A, Kimionis I, Chu AL, Lost C. Determining theapical terminus of root-end resected teeth using three mod-ern apex locators: a comparative ex vivo study. Int EndodJ 2005;38:827.
204. Weine FS. Endodontic therapy. 4th ed. St. Louis, MO: CVMosby; 1989.
205. Von der Lehr WN, Marsh RA. A radiographic study of thepoint of endodontic egress. Oral Surg Oral Med Oral PatholOral Radiol Endod 1973;35:705.
206. Cox VS, Brown CE Jr, Bricker SL, Newton CW. Radio-graphic interpretation of endodontic file length. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1991;72:340.
207. Nair MK, Nair UP. Digital and advanced imaging in endo-dontics: a review. J Endod 2007;33:1.
208. Friedlander LT, Love RM, Chandler NP. A comparison ofphosphor-plate digital images with conventional radio-graphs for the perceived clarity of fine endodontic files andapical lesions. Oral Surg Oral Med Oral Path Oral RadiolEndod 2002;93:321.
209. Borg E, Grondahl HG. Endodontic measurements in digitalradiographs acquired by a photostimulable, storage phosphorsystem. Endod Dent Traumatol 1996;12:20.
210. Cederberg RA, Tidwell E, Frederiksen NL, Benson BW.Endodontic working length assessment. Comparison of sto-rage phosphor digital imaging and radiographic film. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1998;85:325.
211. Leddy BJ, Miles DA, Newton CW, Brown CE Jr. Interpreta-tion of endodontic file lengths using RadioVisiography. JEndod 1994;20:542.
212. Sanderink GC, Huiskens R, van der Stelt PF, et al. Imagequality of direct digital intraoral X-ray sensors in assessingroot canal length. The RadioVisioGraphy, Visualix/VIXA,Sens-A-Ray, and Flash Dent systems compared with Ektas-peed films. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1994;78:125.
213. Woolhiser GA, Brand JW, Hoen MM, et al. Accuracy offilm-based, digital, and enhanced digital images for endo-dontic length determination. Oral Surg Oral Med Oral PathOral Radiol Endod 2005;99:499.
214. Radel RT, Goodell GG, McClanahan SB, Cohen ME. In vitroradiographic determination of distances from workinglength files to root ends comparing Kodak RVG 6000, SchickCDR, and Kodak insight film. J Endod 2006;32:566.
215. Stabholz A, Rotstein I, Torabinejad M. Effect of preflaringon tactile detection of the apical constriction. J Endod1995;21:92.
216. Ounsi HF, Haddad G. In vitro evaluation of the reliability ofthe Endex electronic apex locator. J Endod 1998;24:120.
217. Clouse HR. Electronic methods of root canal measurement.Gen Dent 1991;39:432.
218. Lin L, Shovlin F, Skribner J, Langeland K. Pulp biopsies fromthe teeth associated with periapical radiolucency. J Endod1984;10:436.
219. Yusuf H. The significance of the presence of foreign materialperiapically as a cause of failure of root treatment. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1982;54:566.
220. Walton RE. Current concepts of canal preparation. DentClin North Am 1992;36:309.
221. Baugh D, Wallace J. The role of apical instrumentation inroot canal treatment: a review of the literature. J Endod2005;31:333.
222. van der Sluis LW, Wu MK, Wesselink PR. The efficacy ofultrasonic irrigation to remove artificially placed dentine
Chapter 27 / Preparation of Coronal and Radicular Spaces / 979

debris from human root canals prepared using instrumentsof varying taper. Int Endod J 2005;38:764.
223. Khademi A, Yazdizadeh M, Feizianfard M. Determination ofminimum instrumentation size for the penetration of irri-gants to the apical third of root canal systems. J Endod2006;32:417.
224. Hsieh YD, Gau CH, Kung Wu SF, et al. Dynamic recordingof irrigation fluid distribution in root canals using thermalimage analysis. Int Endod J 2007;40:11.
225. Peters CI, Koka RS, Highsmith S, Peters OA. Calciumhydroxide dressings using different preparation and applica-tion modes: density and dissolution by simulated tissuepressure. Int Endod J 2005;38:889.
226. Pekruhn RB. The incidence of failure following single-visitendodontic therapy. J Endod 1986;12:68.
227. Hoskinson SE, Ng YL, Hoskinson AE, et al. A retrospectivecomparison of outcome of root canal treatment using twodifferent protocols. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2002;93:705.
228. Peters OA, Barbakow F, Peters CI. An analysis of endodontictreatment with three nickel–titanium rotary root canal pre-paration techniques. Int Endod J 2004;37:849.
229. Kirkevang LL, Hørsted-Bindslev P. Technical aspects oftreatment in relation to treatment outcome. Endod Top2002;2:89.
230. Farzaneh M, Abitbol S, Lawrence HP, Friedman S. Treat-ment outcome in endodontics-the Toronto study. Pahse II:initial treatment. J Endod 2004;30:302.
231. Ørstavik D, Qvist V, Stoltze K. A multivariate analysis of theoutcome of endodontic treatment. Eur J Oral Sci 2004;112:224.
232. Ruddle C. Cleaning and shaping the root canal system. In:Cohen S, Burns RC, editors. Pathways of the pulp. 8th ed. St.Louis, MO: Mosby; 2002. p. 231.
233. Tan BT, Messer HH: The effect of instrument type andpreflaring on apical file size determination. Int Endod J2002;35:752.
234. Pecora JD, Capelli A, Guersoli DM, et al. Influence of cervi-cal preflaring on apical file size determination. Int Endod J2005;38.
235. Gutmann JL, Witherspoon DE. Obturation of the cleanedand shaped root canal system. In: Cohen S, Burns RC,editors. Pathways of the pulp. 8th ed. St. Louis, MO: Mosby;2002. p. 293.
236. Guide to clinical endodontics. 4th ed. Chicago, IL: AmericanAssociation of Endodontists; 2004.
237. European Society of Endodontology. Quality guidelines ofendodontic treatment: consensus report of the EuropeanSociety of Endodontology. Int Endod J 2006.
238. Kerekes K, Tronstad L. Morphometric observations on rootcanals of human anterior teeth. J Endod 1977;3:24.
239. Kerekes K, Tronstad L. Morphometric observations on theroot canals of human molars. J Endod 1977;3:114.
240. Grossman L. Endodontic practice. 10th ed. Philadelphia, PA:Lea & Febiger; 1986.
241. Sabala CL, Biggs JT. A standard predetermined endodonticpreparation concept. Compend Contin Educ Dent 1991;12:656.
242. Tronstad L. Endodontic techniques. In: Clinical endodon-tics. 1st ed. Stuttgart, New York: Thieme; 1991. p. 167.
243. Glickman GN, Dumsha TC. Problems in cleaning and shap-ing. In: Gutman J, Dumsha TC, Lovdahl PE, Hovland E,editors, Problem solving in endodontics. 3rd ed. St. Louis,MO: Mosby; 1997;
244. Spangberg L. The wonderful world of rotary root canalpreparation. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2001;92:479.
245. Peters OA, Schonenberger K, Laib A. Effects of four NiTipreparation techniques on root canal geometry assessed bymicro computed tomography. Int Endod J 2001;34:221.
246. Lussi A, Nussbacher U, Grosrey J. A novel noninstrumentedtechnique for cleansing the root canal system. J Endod1993;19:549.
247. Attin T, Buchalla W, Zirkel C, Lussi A. Clinical evaluation ofthe cleansing properties of the noninstrumental techniquefor cleaning root canals. Int Endod J 2002;35:929.
248. Allison DA, Weber CR, Walton RE. The influence of themethod of canal preparation on the quality of apical andcoronal obturation. J Endod 1979;5:298.
249. Grossman LI. Endodontics 1776–1976: a bicentennial historyagainst the background of general dentistry. J Am DentAssoc 1976;93:78.
250. Cruse WP, Bellizzi R. A historic review of endodontics,1689–1963, part 1. J Endod 1980;6:495.
251. Lilley JD. Endodontic instrumentation before 1800. J BrEndod Soc 1976;9:67.
252. Hulsmann M. Zur Geschichte der Wurzelkanalaufbereitung.Endodontie 1996:97.
253. Bellizzi R, Cruse WP. A historic review of endodontics,1689–1963, part III. J Endod 1980;6:576.
254. Anthony LP, Grossman LI. A brief history of root-canaltherapy in the United States. J Am Med Assoc 1945;32:43.
255. Ehrmann EH. Wanted: a standard for the recognition ofrotary instruments. Int Endod J 2002;35:215.
256. Mullaney TP. Instrumentation of finely curved canals. DentClin North Am 1979;23:575.
257. Taylor GN. Advanced techniques for intracanal preparationand filling in routine endodontic therapy. Dent Clin NorthAm 1984;28:819.
258. Ingle JI, Himel VT, Hawrish CE, et al. Endodontic cavitypreparation. In: Ingle JI, Bakland LK, editors. Endodontics.5th ed. Hamilton, ON: B.C. Decker; 2002.
980 / Endodontics

259. Barbakow F. The status of root canal therapy in Switzerlandin 1993. J Dent Assoc S Afr 1996;51:819.
260. Lim SS, Stock CJ. The risk of perforation in the curved canal:anticurvature filing compared with the stepback technique.Int Endod J 1987;20:33.
261. Wu M-K, van der Sluis LW, Wesselink PR. The capability oftwo hand instrumentation techniques to remove the innerlayer of dentine in oval canals. Int Endod J 2003;36:218.
262. Goerig AC, Michelich RJ, Schultz HH. Instrumentation ofroot canals in molar using the step-down technique. J Endod1982;8:550.
263. Gluskin AH, Brown DC, Buchanan LS. A reconstructedcomputerized tomographic comparison of Ni–Ti rotary GTfiles versus traditional instruments in canals shaped bynovice operators. Int Endod J 2001;34:476.
264. Wu M-K, van der Sluis LW, Wesselink PR. The risk of furcalperforation in mandibular molars using Gates-Glidden drillswith anticurvature pressure. Oral Surg Oral Med Oral PatholOral Radiol Endod 2005;99:378.
265. Guldener PH. [The filling technic in endodontics]. SchweizMonatsschr Zahnmed 1971;81:311.
266. Roane JB. Balanced force, crown-down preparation, andinject-R Fill obturation. Compend Contin Educ Dent1998;19:1137.
267. Serota KS, Nahmias Y, Barnett F, et al. Predictable endo-dontic success. The apical control zone. Dentistry Today2003;22:90.
268. Kast’akova A, Wu MK, Wesselink PR. An in vitro experi-ment on the effect of an attempt to create an apical matrixduring root canal preparation on coronal leakage and mate-rial extrusion. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2001;91:462.
269. Buchanan LS. The standardized-taper root canal prepara-tion—Part 1. Concepts for variably tapered shaping instru-ments. Int Endod J 2000;33:516.
270. Stadler LE, Wennberg A, Olgart L. Instrumentation of thecurved root canal using filing or reaming technique—a clin-ical study of technical complications. Swed Dent J 1986;10:37.
271. Greene KJ, Krell KV. Clinical factors associated with ledgedcanals in maxillary and mandibular molars. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1990;70:490.
272. Kapalas A, Lambrianidis T. Factors associated with rootcanal ledging during instrumentation. Endod Dent Trauma-tol 2000;16:229.
273. Pettiette MT, Delano EO, Trope M. Evaluation of successrate of endodontic treatment performed by students withstainless-steel K-files and nickel-titanium hand files. J Endod2001;27:124.
274. Eleftheriades G, Lambrianidis T. Technical quality of rootcanal treatment and detection of iatrogenic errors in anundergraduate dental clinic. Int Endod J 2005;38:725.
275. Lin LM, Rosenberg PA, Lin J. Do procedural errors causeendodontic treatment failure? J Am Dent Assoc2005;136:187.
276. Ingle JI. A standardized endodontic technique using newlydevelopment instruments and filling materials. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1961;14:83.
277. Clem WH. Endodontics: the adolescent patient. Dent ClinNorth Am 1969;13:482.
278. Weine FS, Healey HJ, Gerstein H, Evanson L. Pre-curvedfiles and incremental instrumentation for root canal enlarge-ment. J Can Dent Assoc 1970;36:155.
279. Abou-Rass M, Frank AL, Glick DH. The anticurvature filingmethod to prepare the curved root canal. J Am Dent Assoc1980;101:792.
280. Marshall FJ, Pappin JB. A crown-down pressureless prepara-tion root canal enlargement technique. Technique Manual.ed. Portland OR: Oregon Health Sciences University; 1980.
281. Froese WJ, Schechter DS. Sophomore Laboratory Manual.ed. Portland OR: Oregon Health Sciences University; 1981.
282. Fava LR. The double-flared technique: an alternative forbiomechanical preparation. J Endod 1983;9:76.
283. Saunders WP, Saunders EM. Effect of noncutting tippedinstruments on the quality of root canal preparation usinga modified double-flared technique. J Endod 1992;18:32.
284. Roane JB, Sabala CL, Duncanson MG Jr. The ‘‘balancedforce’’ concept for instrumentation of curved canals.J Endod 1985;11:203.
285. Torabinejad M. Passive step-back technique. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1994;77:398.
286. Torabinejad M. Passive step-back technique. A sequentialuse of ultrasonic and hand instruments. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1994;77:402.
287. Siqueira JF Jr, Rjcas IN, Santos SR, et al. Efficacy of instru-mentation techniques and irrigation regimens in reducingthe bacterial population within root canals. J Endod2002;28:181.
288. Cimis GM, Boyer TJ, Pelleu GB Jr. Effect of three file typeson the apical preparations of moderately curved canals.J Endod 1988;14:441.
289. Calhoun G, Montgomery S. The effects of four instrumenta-tion techniques on root canal shape. J Endod 1988;14:273.
290. Alodeh MHA, Dummer PMH. A comparison of the abilityof K-files and Hedstrom files to shape simulated root canalsin resin blocks. Int Endod J 1989;22:226.
291. Briseno BM, Sonnabend E. The influence of different rootcanal instruments on root canal preparation: an in vitrostudy. Int Endod J 1991;24:15.
292. Alodeh MH, Doller R, Dummer PM. Shaping of simulatedroot canals in resin blocks using the step-back techniquewith K-files manipulated in a simple in/out filling motion.Int Endod J 1989;22:107.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 981

293. Schafer E, Tepel J, Hoppe W. Properties of endodontic handinstruments used in rotary motion. Part 2. Instrumentationof curved canals. J Endod 1995;21:493.
294. Stenman E, Spangberg LS. Root canal instruments are poorlystandardized. J Endod 1993;19:327.
295. Moule AJ, Kellaway R, Clarkson R, et al. Variability ofmaster gutta-percha cones. Aus Endod J 2002;28:38.
296. Martin H. A telescopic technique for endodontics. J DistColumbia Dent Soc 1974;49:12.
297. Brantley WA, Luebke NH, Luebke FL, Mitchell JC. Perfor-mance of engine-driven rotary endodontic instruments witha superimposed bending deflection: V. Gates Glidden andPeeso drills. J Endod 1994;20:241.
298. Kuttler S, MacLean A, Dorn S, Fischzang A. The impact ofpost space preparation with Gates-Glidden drills on residualdentin thickness in distal roots of mandibular molars. J AmDent Assoc 2004;135:903.
299. Coffae KP, Brilliant JD. The effect of serial preparationversus nonserial preparation on tissue removal in the rootcanals of extracted mandibular human molars. J Endod1975;14:527.
300. Walton RE. Histologic evaluation of different methods ofenlarging the pulp canal space. J Endod 1976;2:304.
301. Mullaney TP. Instrumentation of finely curved canals. DentClin North Am 1979;4:575.
302. Buchanan LS. Paradigm shifts in cleaning and shaping.J Calif Dent Assoc 1991;19:23.
303. Gutmann JL, Rakusin H. Perspectives on root canal obtura-tion with thermoplasticized injectable gutta-percha. IntEndod J 1987;20:261.
304. Kartal N, Cimilli HK. The degrees and configurations ofmesial canal curvatures of mandibular first molars. J Endod1997;23:358.
305. Schafer E, Diey C, Hoppe W, Tepel J. Roentgenographicinvestigation of frequency and degree of canal curvaturesin human permanent teeth. J Endod 2002;28:211.
306. Baker NA, Eleazer PD, Averbach RE, Seltzer S. Scanningelectron microscopic study of the efficacy of various irrigat-ing solutions. J Endod 1975;1:127.
307. Ram Z. Effectiveness of root canal irrigation. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1977;44:306.
308. Abou Rass M, Jastrab RJ. The use of rotary instruments asauxiliary aids to root canal preparation of molars. J Endod1982;8:78.
309. Vertucci F. Root canal morphology and its relationship toendodontic procedures. Endod Top 2005;10:3.
310. Kessler JR, Peters DD, Lorton L. Comparison of the relativerisk of molar root perforations using various endodonticinstrumentation techniques. J Endod 1983;9:439.
311. Lumley PJ. A comparison of dentine removal using safety orconventional Hedstrom files. Endod Dent Traumatol1997;13:65.
312. Lloyd A, Jaunberzins A, Dhopatkar A, et al. Shaping ofsimulated root canals by the M4 handpiece and Safety Hed-strom files when oriented incorrectly. Braz Endod J 1997;2:7.
313. Swindle RB, Neaverth EJ, Pantera EA Jr, Ringle RD. Effect ofcoronal–radicular flaring on apical transportation. J Endod1991;17:147.
314. Schroeder KP, Walton RE, Rivera EM. Straight line accessand coronal flaring: effect on canal length. J Endod2002;28:474.
315. Leeb J. Canal orifice enlargement as related to biomechanicalpreparation. J Endod 1983;9:463.
316. Fairbourn DR, McWalter GM, Montgomery S. The effect offour preparation techniques on the amount of apicallyextruded debris. J Endod 1987;13:102.
317. Roane JB, Powell SE. The optimal instrument design forcanal preparation. J Am Dent Assoc 1986;113:596.
318. Roane JB, Sabala C. Clockwise or counterclockwise. J Endod1984;10:349.
319. Southard DW, Oswald RJ, Natkin E. Instrumentation ofcurved molar root canals with the Roane technique. J Endod1987;13:479.
320. Backman CA, Oswald RJ, Pitts DL. A radiographic compar-ison of two root canal instrumentation techniques. J Endod1992;18:19.
321. Al-Omari MA, Dummer PM, Newcombe RG, Doller R.Comparison of six files to prepare simulated root canals.Part 2. Int Endod J 1992;25:67.
322. Al-Omari MA, Dummer PM, Newcombe RG. Comparisonof six files to prepare simulated root canals. Part 1. IntEndod J 1992;25:57.
323. Dummer PMH, Al-Omari MAO, Bryant S. Comparison ofthe performance of four files with rounded tips dur-ing shaping of simulated root canals. J Endod 1998;24:364.
324. Ponce de Leon Del Bello T, Wang N, Roane JB. Crown-down tip design and shaping. J Endod 2003;29:513.
325. Sabala CL, Roane JB, Southard LZ. Instrumentation ofcurved canals using a modified tipped instrument: a com-parison study. J Endod 1988;14:59.
326. Kyomen SM, Caputo AA, White SN. Critical analysis of thebalanced force technique in endodontics. J Endod1994;20:332.
327. Charles TJ, Charles JE. The ‘balanced force’ concept forinstrumentation of curved canals revisited. Int EndodJ 1998;31:166.
328. Schafer E. Effects of four instrumentation techniqueson curved canals: a comparison study. J Endod 1996;22:685.
982 / Endodontics

329. Imura N, Kato AS, Novo NF, et al. A comparison of mesialmolar root canal preparations using two engine-driveninstruments and the balanced-force technique. J Endod2001;27:627.
330. Hata G, Uemura M, Kato AS, et al. A comparison of shapingability using ProFile, GT file, and Flex-R endodontic instru-ments in simulated canals. J Endod 2002;28:316.
331. McKendry DJ. Comparison of balanced forces, endosonic,and step-back filing instrumentation techniques: quantifica-tion of extruded apical debris. J Endod 1990;16:24.
332. Pappin JB. Biologic sealing of the apex in endodonticallytreated human teeth [Masters Thesis]. Portland OR: OregonHealth & Sciences University; 1982.
333. Morgan LF, Montgomery S: An evaluation of the crown-down pressureless technique. J Endod 1984;10:491.
334. Luiten DJ, Morgan LA, Baumgartner JC, Marshall JG. Acomparison of four instrumentation techniques on apicalcanal transportation. J Endod 1995;1995:26.
335. Blum JY, Machtou P, Micallef JP. Location of contact areason rotary Profile instruments in relationship to the forcesdeveloped during mechanical preparation on extracted teeth.Int Endod J 1999;32:108.
336. Schrader C, Ackermann M, Barbakow F. Step-by-stepdescription of a rotary root canal preparation technique.Int Endod J 1999;32:312.
337. Thompson SA. An overview of nickel–titanium alloys usedin dentistry. Int Endod J 2000;33:297.
338. Walia HM, Brantley WA, Gerstein H. An initial investigationof the bending and torsional properties of Nitinol root canalfiles. J Endod 1988;14:346.
339. Serene TP, Adams JD, Saxena A. Nickel–titanium instru-ments: applications in endodontics.St. Louis, MO: IshiakuEuroAmerica; 1995.
340. Parashos P, Messer HH. The diffusion of innovation indentistry: a review using rotary nickel–titanium technologyas an example. Oral Surg Oral Med Oral Path Oral RadiolEndod 2006;101:395.
341. Pettiette MT, Metzger Z, Phillips C, Trope M. Endodonticcomplications of root canal therapy performed by dentalstudents with stainless-steel K-files and nickel-titanium handfiles. J Endod 1999;25:230.
342. Barbakow. The LightSpeed system. Dent Clin North Am2004;48:113.
343. Sattapan B, Nervo GJ, Palamara JEA, Messer HH. Defects inrotary nickel–titanium files after clinical use. J Endod2000;26:161.
344. Roland DD, Andelin WE, Browning DF, et al. The effect ofpreflaring on the rates of separation for 0.04 taper nickeltitanium rotary instruments. J Endod 2002;28:543.
345. Yared GM, Bou Dagher FE, Machtou P, Kulkarni GK.Influence of rotational speed, torque and operator profi-
ciency on failure of Greater Taper files. Int EndodJ 2002;35:7.
346. Yared GM, Bou Dagher FE, Machtou P. Influence of rota-tional speed, torque and operator’s proficiency on ProFilefailures. Int Endod J 2001;34:47.
347. Schrader C, Peters OA. Analysis of torque and force duringstep-back with differently tapered rotary endodontic instru-ments in vitro. J Endod 2005;31:120.
348. Peng B, Shen Y, Cheung GS, Xia TJ. Defects in ProTaper S1instruments after clinical use: longitudinal examination. IntEndod J 2005;38:550.
349. Parashos P, Messer HH. Rotary NiTi instrument fractureand its consequences. J Endod 2006;32:1031.
350. Zuolo ML, Walton RE. Instrument deterioration with usage:nickel–titanium versus stainless steel. Quintessence Int1997;28:397.
351. Herold KS, Johnson BR, Wenckus CS. A scanning electronmicroscopy evaluation of microfractures, deformation andseparation in EndoSequence and Profile Nickel-Titaniumrotary files using an extracted molar tooth model. J Endod2007;33:712.
352. Lemmer K, Mielke M, Pauli G, Beekes M. Decontaminationof surgical instruments from prion proteins. in vitro studieson the detachment, destabilization and degradation of PrPScbound to steel surfaces. J Gen Virol 2004;85:3805.
353. Aasim SA, Mellor AC, Qualtrough AJ. The effect of pre-soaking and time in the ultrasonic cleaner on the cleanlinessof sterilized endodontic files. Int Endod J 2006;39:143.
354. Peretz D, Supattapone S, Giles K, et al. Inactivation of prionsby acidic sodium dodecyl sulfate. J Virol 2006;80:322.
355. Sonntag D, Peters OA. Effect of prion decontamination pro-tocols on nickel–titanium rotary surfaces. J Endod 2007;33.
356. O’Hoy PY, Messer HH, Palamara JE. The effect of cleaningprocedures on fracture properties and corrosion of NiTifiles. Int Endod J 2003;36:724.
357. Darabara M, Bourithis L, Zinelis S, Papadimitriou GD. Sus-ceptibility to localized corrosion of stainless steel and NiTiendodontic instruments in irrigating solutions. Int Endod J2004;37:705.
358. Peters OA, Roelicke JO, Baumann MA. Effect of immersion insodium hypochlorite on torque and fatigue resistance of nickel–titanium instruments. J Endod 2007;33:589.
359. Buchanan LS. The standardized-taper root canal prepara-tion—Part 1. Concepts for variably tapered shaping instru-ments. Int Endod J 2000;33:516.
360. Li UM, Lee BS, Shih CT, et al. Cyclic fatigue of endodonticnickel titanium rotary instruments: static and dynamic tests.J Endod 2002;28:448.
361. Rowan MB, Nicholls JI, Steiner J. Torsional properties ofstainless steel and nickel–titanium endodontic files. J Endod1996;22:341.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 983

362. Pruett JP, Clement DJ, Carnes DL. Cyclic fatigue testing ofnickel–titanium endodontic instruments. J Endod1997;23:77.
363. Peters OA, Barbakow F. Dynamic torque and apical forces ofProFile .04 rotary instruments during preparation of curvedcanals. Int Endod J 2002;35:379.
364. Haikel Y, Serfaty R, Bateman G, et al. Dynamic and cyclicfatigue of engine-driven rotary nickel–titanium endodonticinstruments. J Endod 1999;25:434.
365. Ullmann C, Peters OA. Effect of cyclic fatigue on staticfracture loads in ProTaper nickel–titanium rotary instru-ments. J Endod 2005;31:183.
366. Kitchens GG, Liewehr FR, Moon PC. The effect of opera-tional speed on the fracture of nickel–titanium rotary instru-ments. J Endod 2007;33:52.
367. Ruddle C. The Protaper technique. Endod Top 2005;10:187.
368. Plotino G, Grande NM, Sorci E, et al. Influence of a brushingworking motion on the fatigue life of NiTi rotary instru-ments. Int Endod J 2007;40:45.
369. Patino PV, Biedma BM, Liebana CR, et al. The influence of amanual glide path on the separation of NiTi rotary instru-ments. J Endod 2005;31:114.
370. Anderson DN, Joyce AP, Roberts S, Runner R. A compara-tive photoelastic stress analysis of internal root stressesbetween RC Prep and saline when applied to the Profile/GT rotary instrumentation system. J Endod 2006;32:224.
371. Peters OA, Boessler C, Zehnder M. Effect of liquid and paste-type lubricants on torque values during simulated rotary rootcanal instrumentation. Int Endod J 2005;38:223.
372. Boessler C, Peters OA, Zehnder M. Impact of lubricantparameter on rotary instrument torque and force. J Endod2007;33:280.
373. Grawehr M, Sener B, Waltimo T, Zehnder M. Interactions ofethylenediaminetetraacetic acid with sodium hypochlorite inaqueous solutions. Int Endod J 2003;36:411.
374. Berutti E, Angelini E, Rigolone M, et al. Influence of sodiumhypochlorite on fracture properties and corrosion of ProTa-per rotary instruments. Int Endod J 2006;39:693.
375. Castro Martins R, Bahia MGA, Buono VTL. The effect ofsodium hypochlorite on the surface characteristics and fati-gue resistance of ProFile nickel-titanium instruments. OralSurg Oral Med Oral Path Oral Radiol Endod 2006;102:99.
376. Baumgartner JC, Cuenin PR. Efficacy of several concentra-tions of sodium hypochlorite for root canal irrigation. JEndod 1992;18:605.
377. Grandini S, Balleri P, Ferrari M. Evaluation of Glyde FilePrep in combination with sodium hypochlorite as a rootcanal irrigant. J Endod 2002;28:300.
378. Mayer BE, Peters OA, Barbakow F. Effects of rotary instru-ments and ultrasonic irrigation on debris and smear layerscores: a scanning electron microscopic study. Int Endod J2002;35:582.
379. Regan JD, Gutmann JL. Preparation of the root canal sys-tem. In: Pitt Ford TR, editors. Endodontics in clinical prac-tice, 5th ed. Oxford: Elsevier; 2003. p. 77.
380. Al-Omari MA, Dummer PM. Canal blockage and debrisextrusion with eight preparation techniques. J Endod1995;21:154.
381. Reddy SA, Hicks ML. Apical extrusion of debris using twohand and two rotary instrumentation techniques. J Endod1998;24:180.
382. Nygaard-Østby B. Chelation in endodontic therapy: ethyle-nediamineacetate acid for cleansing and widening of rootcanals. Odontologisk Tidskrift 1957;65:3.
383. Fehr F, Nygaard-Østby B. Effect of EDTAC and sulfuric acidon root canal dentin. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1963;12:99.
384. Goldberg F, Spielberg C. The effect of EDTAC and thevariation of its working time analyzed with scanning electronmicroscopy. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1982;53:74.
385. Fraser JG. Chelating agents: their softening effect on rootcanal dentin. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1974;37:803.
386. Fraser JG, Laws AJ. Chelating agents: their effect on thepermeability of root canal dentin. Oral Surg Oral Med OralPathol Oral Radiol Endod 1976;41:534.
387. Bortnick KL, Steiman HR, Ruskin A. Comparison of nick-el–titanium file distortion using electric and air-drivenhandpieces. J Endod 2001;27:57.
388. Molven O. A comparison of the dentin-removing ability offive root canal instruments. Scand J Dent Res 1970;78:500.
389. O’Connell DT, Brayton SM. Evaluation of root canal pre-paration with two automated endodontic handpieces. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1975;39:298.
390. Klayman SM, Brilliant JD. A comparison of the efficacy ofserial preparation versus Giromatic preparation. J Endod1975;1:334.
391. Harty FJ, Stock C. The Giromatic system compared withhand instrumentation in endodontics. Br Dent J1974;137:239.
392. Weine FS, Kelly RF, Bray KE. Effect of preparation withendodontic handpieces on original canal shape. J Endod1976;2:298.
393. Felt RA, Moser JB, Heuer MA. Flute design of endodonticinstruments: its influence on cutting efficiency. J Endod1982;8:253.
394. Spyropoulos S, Eldeeb ME, Messer HH. The effect of Giro-matic files on the preparation shape of severely curvedcanals. Int Endod J 1987;20:133.
395. Hulsmann M, Stryga F. Comparison of root canal prepara-tion using different automated devices and hand instrumen-tation. J Endod 1993;19:141.
984 / Endodontics

396. Schafer E, Zapke K. A comparative scanning electron micro-scopic investigation of the efficacy of manual and automatedinstrumentation of root canals. J Endod 2000;26:660.
397. Tepel J. Experimentelle Untersuchungen uber die maschi-nelle Wurzelkanalaufbereitung.Berlin, Germany: Quintes-senz Verlags-GmbH; 2000.
398. Paque F, Barbakow F, Peters OA. Root canal preparationwith Endo-Eze AET: changes in root canal shape assessed bymicro-computed tomography. Int Endod J 2005;38:456.
399. Zmener O, Pamaijer CH, Banegas G. Effectiveness in clean-ing oval-shaped root canals using Anatomic EndodonticTechnology, ProFile and manual instrumentation: a scan-ning electron microscopic study. Int Endod J 2005;38:356.
400. Daugherty DW, Gound TG, Comer TL. Comparison offracture rate, deformation rate, and efficiency between rotaryendodontic instruments driven at 150 rpm and 350 rpm. JEndod 2001;27:93.
401. Gabel WP, Hoen M, Steiman HR, et al. Effect of rotationalspeed on nickel–titanium file distortion. J Endod1999;25:752.
402. Dietz DB, Di Fiore PM, Bahcall JK, Lautenschlager EP.Effect of rotational speed on the breakage of nickel-titaniumrotary files. J Endod 2000;26:68.
403. Yared GM. Behaviour of Hero NiTi instruments used by anexperienced operator under access limitations. Aust Endod J2002;28:64.
404. Yared G, Bou Dagher F, Kulkarni K. Influence of torquecontrol motors and the operator’s proficiency on ProTaperfailures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;96:229.
405. Gambarini G. Rationale for the use of low-torque endodon-tic motors in root canal instrumentation. Endod Dent Trau-matol 2000;16:95.
406. Gambarini G. Cyclic fatigue of nickel–titanium rotaryinstruments after clinical use with low- and high-torqueendodontic motors. J Endod 2001;27:772.
407. Gambarini G. Advantages and disadvantages of new torque-controlled endodontic motors and low-torque NiTi rotaryinstrumentation. Aust Endod J 2001;27:99.
408. Yared G, Kulkarni GK. Accuracy of the DTC torque controlmotor for nickel–titanium rotary instruments. Int Endod J2004;37:399.
409. Yared G, Kuklarni GK. Accuracy of the TCM Endo IIItorque-control motor for nickel–titanium rotary instru-ments. J Endod 2004;30:644.
410. Yared G, Kulkarni GK. Accuracy of the Nouvag torquecontrol motor for nickel-titanium rotary instruments. OralSurg Oral Med Oral Path Oral Radiol Endod 2004;97:499.
411. Dental root-canal instruments—Part 1: Files, reamers,barbed broaches, rasps, paste carriers, explorers and cottonbroaches. Geneva: International Organization for Standardi-zation; 1992.
412. Blum JY, Machtou P, Ruddle C, Micallef JP. Analysis ofmechanical preparations in extracted teeth using ProTaperrotary instruments: value of the safety quotient. J Endod2003;29:567.
413. Johnson TA, Zelikow R. Ultrasonic endodontics: a clinicalreview. J Am Dent Assoc 1987;114:655.
414. Richman MJ. The use of ultrasonics in root canal therapyand root resection. J Dent Med 1957;12:12.
415. Martin H. Ultrasonic disinfection of the root canal. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1976;42:92.
416. Cunningham WT, Martin H. A scanning electron micro-scope evaluation of root canal debridement with the endo-sonic ultrasonic synergistic system. Oral Surg Oral Med OralPathol Oral Radiol Endod 1982;53:527.
417. Cunningham WT, Martin H, Forrest WR. Evaluation of rootcanal debridement by the endosonic ultrasonic synergistic system.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1982;53:401.
418. Cunningham WT, Martin H, Pelleu GB Jr, Stoops DE. Acomparison of antimicrobial effectiveness of endosonic andhand root canal therapy. Oral Surg Oral Med Oral PatholOral Radiol Endod 1982;54:238.
419. Martin H, Cunningham W. Endosonic endodontics:the ultrasonic synergistic system. Int Dent J 1984;34:198.
420. Martin H, Cunningham W. Endosonics—the ultrasonicsynergistic system of endodontics. Endod Dent Traumatol1985;1:201.
421. Cameron JA. The use of ultrasonics in the removal of thesmear layer: a scanning electron microscope study. J Endod1983;9:289.
422. Barnett F, Trope M, Khoja M, Tronstad L. Bacteriologicstatus of the root canal after sonic, ultrasonic and handinstrumentation. Endod Dent Traumatol 1985;1:228.
423. Reynolds MA, Madison S, Walton RE, et al. An in vitrohistological comparison of the step-back, sonic, and ultra-sonic instrumentation techniques in small, curved rootcanals. J Endod 1987;13:307.
424. Yamaguchi M, Matsumori M, Ishikawa H, et al. The use ofultrasonic instrumentation in the cleansing and enlargementof the root canal. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1988;65:349.
425. Pedicord D, elDeeb ME, Messer HH. Hand versus ultrasonicinstrumentation: its effect on canal shape and instrumenta-tion time. J Endod 1986;12:375.
426. Baker MC, Ashrafi SH, Van Cura JE, Remeikis NA. Ultra-sonic compared with hand instrumentation: a scanning elec-tron microscopic study. J Endod 1988;14:435.
427. Chenail BL, Teplitsky PE. Endosonics in curved root canals.Part II. J Endod 1988;14:214.
428. Krell KV, Johnson RJ. Irrigation patterns of ultrasonic endo-dontic files. Part II. Diamond coated files. J Endod 1988;14:535.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 985

429. Loushine RJ, Weller RN, Hartwell GR. Stereomicroscopicevaluation of canal shape following hand, sonic, and ultra-sonic instrumentation. J Endod 1989;15:417.
430. Schulz-Bongert U, Weine FS, Schulz-Bongert J. Preparationof curved canals using a combined hand-filing, ultrasonictechnique. Comp Cont Ed Dent 1995;16:270.
431. Ahmad M, Pitt Ford TR, Crum LA. Ultrasonic debridementof root canals: an insight into the mechanisms involved. JEndod 1987;13:93.
432. Ahmad M, Pitt Ford TR, Crum LA. Ultrasonic debridementof root canals: acoustic streaming and its possible role. JEndod 1987;13:490.
433. Ahmad M, Pitt Ford TR, Crum LA, Walton AJ. Ultrasonicdebridement of root canals: acoustic cavitation and its rele-vance. J Endod 1988;14:486.
434. Walmsley AD, Williams AR. Effects of constraint on the oscilla-tory pattern of endosonic files. J Endod 1989;15:189.
435. Walmsley AD, Lumley PJ, Laird WRE. The oscillatory pat-tern of sonically powered endodontic files. Int Endod J1989;22:125.
436. Burleson A, Nusstein J, Reader A, Beck M. The in vivo evalua-tion of hand/rotary/ultrasound instrumentation in necrotic,human mandibular molars. J Endod 2007;33:782.
437. Jensen SA, Walker TL, Hutter JW, Nicoll BK. Comparison ofthe cleaning efficacy of passive sonic activation and passiveultrasonic activation after hand instrumentation in molarroot canals. J Endod 1999;25:735.
438. Sabins RA, Johnson JD, Hellstein JW. A comparison of thecleaning ability of short-term sonic and ultrasonic passiveirrigation after hand instrumentation in molar root canals. JEndod 2003;29:674.
439. Weber CD, McClanahan SB, Miller GA, et al. The effect ofpassive ultrasonic activation of 2% chlorhexidine and of5.25% sodium hypochlorite irrigant on residual microbialactivity in root canals. J Endod 2003;29:562.
440. van der Sluis LW, Wu MK, Wesselink PR. A comparisonbetween a smooth wire and a K-file in removing artificiallyplaced dentine debris from root canals in resin blocks duringultrasonic irrigation. Int Endod J 2005;38:593.
441. Alacam T. Scanning electron microscope study comparingthe efficacy of endodontic irrigating systems. Int Endod J1987;20:287.
442. Cunningham WT, Balekjian AY. Effect of temperature oncollagen-dissolving ability of sodium hypochlorite endodon-tic irrigant. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1980;49:175.
443. Cameron JA. The effect of ultrasonic endodontics onthe temperature of the root canal wall. J Endod 1988;14:554.
444. Archer R, Reader A, Nist R, et al. An in vivo evaluation ofthe efficacy of ultrasound after step-back preparation inmandibular molars. J Endod 1992;18:549.
445. Krell KV, Johnson RJ, Madison S. Irrigation patterns duringultrasonic canal instrumentation. Part I. K-type files. JEndod 1988;14:65.
446. Ahmad M, Ford TR, Crum LA, Walton AJ. Ultrasonic deb-ridement of root canals: acoustic cavitation and its relevance.J Endod 1988;14:486.
447. Martin H, Cunningham WT, Norris JP, Cotton WR. Ultra-sonic versus hand filing of dentin: a quantitative study. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1980;49:79.
448. Wildey WL, Senia ES, Montgomery S. Another look at rootcanal instrumentation. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1992;74:499.
449. Lam TV, Lewis DJ. Changes in root canal morphology insimulated curved canals over-instrumented with a variety ofstainless steel and nickel titanium files. Aust Dent J1999;44(1):12.
450. Powell SE, Simon JH, Maze BB. A comparison of the effectof modified and nonmodified instrument tips on apicalcanal configuration. J Endod 1986;12:293.
451. Dummer PM, Al-Omari MA, Bryant S. Comparison of theperformance of four files with rounded tips during shapingof simulated root canals. J Endod 1998;24:364.
452. Griffiths IT, Bryant ST, Dummer PMH. Canal shapes pro-duced sequentially during instrumentation with Quantec LXrotary nickel–titanium instruments: a study in simulatedcanals. Int Endod J 2000;33:346.
453. Garala M, Kuttler S, Hardigan P, et al. A comparison of theminimum canal wall thickness remaining following prepara-tion using two nickel–titanium rotary systems. Int Endod J2003;36:636.
454. Crump MC, Natkin E. Relationship of broken root canalinstruments to endodontic case prognosis: a clinical investi-gation. J Am Dent Assoc 1970;80:1341.
455. Weine FS, Kelly RF, Lio PJ. The effect of preparation proce-dures on original shape and on apical foramen shape. JEndod 1975;1:255.
456. Tucker DM, Wenckus CS, Bentkover SK. Canal wall plan-ning by engine-driven nickel–titanium instruments, com-pared with stainless-steel hand instrumentation. J Endod1997;23:170.
457. Wu MK, Wesselink PR. A primary observation on the pre-paration and obturation of oval canals. Int Endod J2001;34:137.
458. Tan BT, Messer HH. The quality of apical canal preparationusing hand and rotary instruments with specific criteria forenlargement based on initial apical file size. J Endod2002;28:658.
459. Rodig T, Hulsmann M, Muhge M, Schafers F. Quality ofpreparation of oval distal root canals in mandibular molarsusing nickel–titanium instruments. Int Endod J 2002;35:919.
460. Weiger R, El Ayouti A, Lost C. Efficiency of hand and rotaryinstruments in shaping oval root canals. J Endod 2002;28:580.
986 / Endodontics

461. Bergmans L, Van Cleynenbreugel J, Beullens M, et al.Smooth flexible versus active tapered shaft design using NiTirotary instruments. Int Endod J 2002;35:820.
462. Bergmans L, Van Cleynenbreugel J, Beullens M, et al. Pro-gressive versus constant tapered shaft design using NiTirotary instruments. Int Endod J 2003;36:288.
463. Peters OA, Peters CI, Schonenberger K, Barbakow F. Pro-Taper rotary root canal preparation: assessment of torqueand force in relation to canal anatomy. Int Endod J2003;36:93.
464. Hubscher W, Barbakow F, Peters OA. Root canal prepara-tion with FlexMaster: canal shapes analysed by micro-computed tomography. Int Endod J 2003;36:740.
465. Stuart CH, Schwartz SA, Beeson TJ, Owatz CB. Enterococcusfaecalis: its role in root canal treatment failure and currentconcepts in retreatment. J Endod 2006;32:93.
466. Pertot WJ, Camps J, Damiani MG. Transportation of curvedcanals prepared with Canal Master-U, Canal Master-U-NiTi,and stainless steel K-type files. Oral Surg Oral Med Oral PathOral Radiol Endod 1995;79:504.
467. Jardine SJ, Gulabivala K. An in vitro comparison of canalpreparation using two automated rotary nickel–titaniuminstrumentation techniques. Int Endod J 2000;33:381.
468. Iqbal MK, Maggiore F, Suh B, et al. Comparison of apicaltransportation in four Ni–Ti rotary instrumentation techni-ques. J Endod 2003;29:587.
469. Bramante CM, Berbert A, Borges RP. A methodology forevaluation of root canal instrumentation. J Endod1987;13:243.
470. McCann JT, Keller DL, LaBounty GL. A modification of themuffle model system to study root canal morphology. JEndod 1990;16:114.
471. Tamse A, Pilo R. A new muffle model system to study rootcanal morphology and instrumentation techniques. J Endod1998;24:540.
472. Portenier I, Lutz F, Barbakow F. Preparation of the apicalpart of the root canal by the Lightspeed and step-backtechniques. Int Endod J 1998;31:103.
473. Kuttler S, Garala M, Perez R, Dorn SO. The endodonticcube: a system designed for evaluation of root canal anatomyand canal preparation. J Endod 2001;27:533.
474. Deplazes P, Peters O, Barbakow F. Comparing apical pre-parations of root canals shaped by nickel titanium rotaryand nickel titanium hand instruments. J Endod 2001;27:196.
475. Leseberg DA, Montgomery S. The effects of Canal Master,Flex-R, and K-Flex instrumentation on root canal configura-tion. J Endod 1991;17:59.
476. Coleman CL, Svec TA. Analysis of Ni-Ti versus stainless steelinstrumentation in resin simulated canals. J Endod 1997;23:232.
477. Short JA, Morgan LA, Baumgartner JC. A comparison ofcanal centering ability of four instrumentation techniques.J Endod 1997;23:503.
478. Shadid DB, Nicholls JI, Steiner JC. A comparison of curvedcanal transportation with balanced force versus lightspeed.J Endod 1998;24:651.
479. Kosa D, Marshall G, Baumgartner J. An analysis of canalcentering using mechanical instrumentation techniques.J Endod 1999;25:441.
480. Porto Carvalho LA, Bonetti I, Gagliardi Borges MA. A com-parison of molar root canal preparation using stainless steeland nickel–titanium instruments. J Endod 1999;25:807.
481. Thompson SA, Dummer PM. Shaping ability of Lightspeedrotary nickel–titanium instruments in simulated root canals.Part 1. J Endod 1997;23:698.
482. Thompson SA, Dummer PM. Shaping ability of Lightspeedrotary nickel–titanium instruments in simulated root canals.Part 2. J Endod 1997;23:742.
483. Bryant ST, Thompson SA, Al-Omari MAO, Dummer PMH.Shaping ability of ProFile rotary nickel–titanium instru-ments with ISO sized tips in simulated root canals: Part 1.Int Endod J 1998;31:275.
484. Bryant ST, Thompson SA, Al-Omari MAO, Dummer PMH.Shaping ability of ProFile rotary nickel–titanium instru-ments with ISO sized tips in simulated root canals: Part 2.Int Endod J 1998;31:282.
485. Bryant ST, Dummer PM, Pitoni C, et al. Shaping ability of.04 and .06 taper ProFile rotary nickel–titanium instrumentsin simulated root canals. Int Endod J 1999;32:155.
486. Thompson SA, Dummer PM. Shaping ability of Hero 642rotary nickel–titanium instruments in simulated root canals:Part 2. Int Endod J 2000;33:255.
487. Thompson SA, Dummer PM. Shaping ability of Hero 642rotary nickel–titanium instruments in simulated root canals:Part 1. Int Endod J 2000;33:248.
488. Griffiths IT, Chassot AL, Nascimento MF, et al. Canal shapesproduced sequentially during instrumentation with QuantecSC rotary nickel–titanium instruments: a study in simulatedcanals. Int Endod J 2001;34:107.
489. Powell SE, Wong PD, Simon JH. A comparison of the effectof modified and nonmodified instrument tips on apicalcanal configuration. Part II. J Endod 1988;14:224.
490. Kuhn WG, Carnes DL Jr, Clement DJ, Walker WA III. Effectof tip design of nickel–titanium and stainless steel files onroot canal preparation. J Endod 1997;23:735.
491. Hulsmann M, Schade M, Schafers F. A comparative study ofroot canal preparation with HERO 642 and Quantec SCrotary Ni–Ti instruments. Int Endod J 2001;34:538.
492. Hulsmann M, Herbst U, Schafers F. Comparative study ofroot-canal preparation using Lightspeed and Quantec SCrotary NiTi instruments. Int Endod J 2003;36:748.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 987

493. Al-Omari MA, Bryant S, Dummer PM. Comparison of twostainless steel files to shape simulated root canals. Int EndodJ 1997;30:35.
494. Bishop K, Dummer PM. A comparison of stainless steelFlexofiles and nickel-titanium NiTiFlex files duringthe shaping of simulated canals. Int Endod J 1997;30:25.
495. Schafer E. Shaping ability of Hero 642 rotary nickel-titaniuminstruments and stainless steel hand K-Flexofiles in simu-lated curved root canals. Oral Surg Oral Med Oral PatholOral Radiol Endod 2001;92:215.
496. Schafer E, Lohmann D. Efficiency of rotary nickel–titaniumFlexMaster instruments compared with stainless steel handK-Flexofile—Part 1. Shaping ability in simulated curvedcanals. Int Endod J 2002;35:505.
497. Schafer E, Florek H. Efficiency of rotary nickel–titanium K3instruments compared with stainless steel hand K-flexofile.Part 1. Shaping ability in simulated curved canals. Int EndodJ 2003;36:199.
498. Yun HH, Kim SK. A comparison of the shaping abilities of 4nickel–titanium rotary instruments in simulated root canals.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;95:228.
499. Hulsmann M, Gressmann G, Schafers F. A comparativestudy of root canal preparation using FlexMaster and HERO642 rotary Ni–Ti instruments. Int Endod J 2003;36:358.
500. Schafer E, Schlingemann R. Efficiency of rotary nickel–titaniumK3 instruments compared with stainless steel hand K-Flexofile. Part 2. Cleaning effectiveness and shaping ability inseverely curved root canals of extracted teeth. Int Endod J 2003;36:208.
501. Lim KC, Webber J. The validity of simulated root canals forthe investigation of the prepared root canal shape. Int EndodJ 1985;18:240.
502. Lim KC, Webber J. The effect of root canal preparationon the shape of the curved root canal. Int Endod J1985;18:233.
503. Ciucchi B, Cergneux M, Holz J. Comparison of curved canalshape using filing and rotational instrumentation techni-ques. Int Endod J 1990;23:139.
504. Haga CS. Microscopic measurements of root canal prepara-tions following instrumentation. J Br Endod Soc 1968;2:41.
505. Vessey R. The effect of filing versus reaming on the shape ofthe prepared root canal. Oral Surg Oral Med Oral PatholOral Radiol Endod 1969;27:544.
506. Jungmann CL, Uchin RA, Bucher JF. Effect of instrumenta-tion on the shape of the root canal. J Endod 1975;1:66.
507. Tronstad L, Niemczyk SP. Efficacy and safety tests of sixautomated devices for root canal instrumentation. EndodDent Traumatol 1986;2:270.
508. Kielt LW, Montgomery S. The effect of endosonic instru-mentation in simulated curved root canals. J Endod1987;13:215.
509. Lev R, Reader A, Beck M, Meyers W. An in vitro comparisonof the step-back technique versus a step-back/ultrasonictechnique for 1 and 3 minutes. J Endod 1987;13:523.
510. Bolanos OR, Sinai IH, Gonsky R, Srinivasan R. A compar-ison of engine and air-driven instrumentation methods withhand instrumentation. J Endod 1988;14:392.
511. Miserendino LJ, Miserendino CA, Moser JB, et al. Cuttingefficiency of endodontic instruments. Part III. Comparisonof sonic and ultrasonic instrument systems. J Endod1988;14:24.
512. Walker TL, del Rio CE. Histological evaluation of ultrasonicand sonic instrumentation of curved root canals. J Endod1989;15:49.
513. Yahya AS, ElDeeb ME. Effect of sonic versus ultrasonicinstrumentation on canal preparation. J Endod 1989;15:235.
514. Lloyd A, Jaunberzins A, Dhopatkar A, et al. Shaping abilityof the M4 handpiece and Safety Hedstrom files in simulatedroot canals. Int Endod J 1997;30:16.
515. Barbakow F, Lutz F. The ‘Lightspeed’ preparation techniqueevaluated by Swiss clinicians after attending continuing edu-cation courses. Int Endod J 1997;30:46.
516. Mandel E, Adib-Yazdi M, Benhamou L-M, et al. RotaryNi–Ti ProFile systems for preparing curved canals in resinblocks: influence of operator on instrument breakage. IntEndod J 1999;32:436.
517. Al-Fouzan KS. Incidence of rotary ProFile instrument frac-ture and the potential for bypassing in vivo. Int Endod J2003;36:864.
518. Spili P, Parahos P, Messer HH. The impact of instrumentfracture on outcome of endodontic treatment. J Endod2005;31:845.
519. Wolcott S, Wolcott J, Ishley D, et al. Separation incidence ofProTaper rotary instruments: a large cohort clinical investi-gation. J Endod 2006;12:1139.
520. Grossman LI. Fate of endodontically treated teeth with frac-tured root canal instruments. J Br Endod Soc 1968;2:35.
521. Fox J, Moodnik RM, Greenfield E, Atkinson JS. Filing rootcanals with files radiographic evaluation of 304 cases. N YState Dent J 1972;38:154.
522. Sonntag D, Heithecker K. Korrosion von Nickel-Titan-Instrumenten. Endodontie 2006;15:23.
523. Borkow G, Gabbay J. Copper as biocidal tool. Curr MedChem 2004;12:2163.
524. Thoden van Velzen SK, Duivenvoorden HJ, Schuurs AH.Probabilities of success and failure in endodontic treatment:a Bayesian approach. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1981;52:85.
525. Ward JR, Parashos P, Messer HH. Evaluation of an ultra-sonic technique to remove fractured rotary nickel–titaniumendodontic instruments from root canals: an experimentalstudy. J Endod 2003;29:756.
988 / Endodontics

526. Ward JR, Parashos P, Messer HH. Evaluation of an ultra-sonic technique to remove fractured rotary nickel–titaniumendodontic instruments from root canals: clinical cases. JEndod 2003;29:764.
527. Kesler G, Gal R, Kesler A, Koren R. Histological and scan-ning electron microscope examination of root canal afterpreparation with Er:YAG laser microprobe: a preliminaryin vitro study. J Clin Laser Med Surg 2002;20:269.
528. Lussi A, Messerli L, Hotz P, Grosrey J. A new non-instru-mental technique for cleaning and filling root canals. IntEndod J 1995;28:1.
529. Nakashima M, Akamine A. The application of tissue engi-neering to regeneration of pulp and dentin in endodontics. JEndod 2005;31:711.
530. Matsumoto K. Lasers in endodontics. Dent Clin North Am1990;44:889.
531. Stabholz A, Sahar-Helft S, Moshonov J. Lasers in endodon-tics. Dent Clin North Am 2004;48:809.
532. Dederich DN, Zakariasen KL, Tulip J. Scanning electronmicroscopic analysis of canal wall dentin following neody-mium–yttrium–aluminum–garnet laser irradiation. J Endod1984;10:428.
533. Takeda FH, Harashima T, Eto JN, et al. Effect of Er:YAGlaser treatment on the root canal walls of human teeth: anSEM study. Endod Dent Traumatol 1998;14:270.
534. Takeda FH, Harashima T, Kimura Y, Matsumoto K. Efficacyof Er:YAG laser irradiation in removing debris and smearlayer on root canal walls. J Endod 1998;24:548.
535. Harashima T, Takeda FH, Kimura Y, Matsumoto K. Effectof Nd:YAG laser irradiation for removal of intracanal debrisand smear layer in extracted human teeth. J Clin Laser MedSurg 1997;15:131.
536. Barbakow F, Peters O, Havranek L. Effects of Nd: YAG laserson root canal walls: A light and scanning electron micro-scopic study. Quintessence Int 1999;30:837.
537. Cecchini SCM, Zezell DM, Bachmann L. Evaluation of twolaser systems for intracanal irradiation. In: Featherstone JDB,Rechmann P, Fried D, editors, Lasers in dentistry V. ProcSPIEE; 1999. p. 31.
538. Liu HC, Lin CP, Lan WH. Sealing depth of Nd:YAG laser onhuman dentinal tubules. J Endod 1997;23:691.
539. Bahcall JK, Miserendino CA, Walia H, Belardi DW. Scan-ning electron microscopic comparison of canal preparationwith Nd:YAG laser and hand instrumentation: a preliminarystudy. Gen Dent 1993;41:45.
540. Anic I, Dzubur A, Vidovic D, Tudja M. Temperature andsurface changes of dentine and cementum induced by CO2
laser exposure. Int Endod J 1993;26:284.
541. Ramskold LO, Fong CD, Stromberg T. Thermal effects andantibacterial properties of energy levels required to sterilizestained root canals with an Nd:YAG laser. J Endod1997;23:96.
542. Hibst R, Stock K, Gall R, Keller U. ErYAG laser for endo-dontics efficiency and safety. In: Altshuler GB, Bringruber R,Dal Fante M, et al., editors, Medical applications of lasers indermatology, ophthalmology, dentistry, and endoscopy.Proc SPIEE, Vol 3192; 1997. p. 14.
543. da Costa Ribeiro A, Nogueira GEC, Antoniazzi JH, et al.Effects of a diode laser (810 nm) irradiation on root canalwalls: thermographic and morphological studies. J Endod2006;33:252.
544. Harashima T, Takeda FH, Zhang C, et al. Effect of argonlaser irradiation on instrumented root canal walls. EndodDent Traumatol 1998;14:26.
545. Schoeffel GJ. Apparatus for evacuation of root canal; 2004.
546. Gutarts R, Nusstein J, Reader A, Beck M. In vivo debride-ment efficacy of ultrasonic irrigation following hand-rotaryinstrumentation in human mandibular molars. J Endod2005;31:166.
547. Fukumoto Y, Kikuchi I, Yoshioka T, et al. An ex vivoevaluation of a new root canal irrigation technique withintracanal aspiration. Int Endod J 2006;39:93.
548. Lussi A, Portmann P, Nussbacher U, et al. Comparison oftwo devices for root canal cleansing by the noninstrumenta-tion technology. J Endod 1999;25:9.
549. Lussi A. Die Reinigung und Obturation des Wurzelkanalsys-tems ohne konventionelle Instrumente-eine Standortbestim-mung. Schweizerische Monatsschrift fur Zahnmedizin2000;110:249.
550. Lussi A, Suter B, Grosrey J. Obturation of root canals in vivowith a new vacuum technique. J Endod 1997;23:629.
551. Lussi A, Imwinkelried S, Stich H. Obturation of root canalswith different sealers using non-instrumentation technology.Int Endod J 1999;32:17.
552. Zehnder M, Schmidlin P, Sener B, Waltimo T. Chelation inroot canal therapy reconsidered. J Endod 2005;31:817.
553. Mader CL, Baumgartner JC, Peters DD. Scanning electronmicroscopic investigation of the smeared layer on root canalwalls. J Endod 1984;10:477.
554. Sen BH, Wesselink PR, Turkun M. The smear layer: a phe-nomenon in root canal therapy. Int Endod J 1995;28:141.
555. Torabinejad M, Handysides R, Khademi AA, Bakland LK.Clinical implications of the smear layer in endodontics: areview. Oral Surg Oral Med Oral Path Oral Radiol Endod2002;94:658.
556. Jeon IS, Spangberg LS, Yoon TC, et al. Smear layer produc-tion by 3 rotary reamers with different cutting blade designsin straight root canals: a scanning electron microscopicstudy. Oral Surg Oral Med Oral Path Oral Radiol Endod2003;96:601.
557. Kum K-Y, Kazemi RB, Cha BY, Zhu Q. Smear layer produc-tion of K3 and ProFile Ni–Ti rotary instruments in curvedroot canals: a comparative SEM study. Oral Surg Oral MedOral Path Oral Radiol Endod 2006;101:536.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 989

558. Ørstavik D, Haapasalo M. Disinfection by endodontic irri-gants and dressings of experimentally infected dentinaltubules. Endod Dent Traumatol 1990;6:142.
559. Kokkas AB, Boutsioukis A, Vassiliades LP, Stavrianos CK.The influence of the smear layer on dentinal tubule penetra-tion depth by three different root canal sealers: an in vitrostudy. J Endod 2004;30:100.
560. Drake DR, Wiemann AH. Bacterial retention in canal wallsin vitro: effect of smear layer. J Endod 1994;20, 2:78.
561. Baumgartner JC, Brown CM, Mader CL, et al. A scanningelectron microscopic evaluation of root canal debridementusing saline, sodium hypochlorite, and citric acid. J Endod1984;10:525.
562. Wayman BE, Kopp WM, Pinero GJ, Lazzari EP. Citric andlactic acids as root canal irrigants in vitro. J Endod 1979;5:258.
563. Tidmarsh BG. Acid-cleansed and resin-sealed root canals. JEndod 1978;4:117.
564. Stewart GG, Kapsimalas P, Rappaport H. EDTA and urea per-oxide for root canal preparation. J Am Dent Assoc 1969;78:335.
565. Koskinen KP, Rahkamo A, Hakala PE. Antimicrobial effectof some endodontic medicaments in vitro. Proc Finn DentSoc 1975;71:132.
566. Koskinen KP, Meurman JH, Stenvall H. Appearance of che-mically treated root canal walls in the scanning electronmicroscope. Scand J Dent Res 1980;88:505.
567. Kaufman AY. The use of dequalinium acetate as a disinfec-tant and chemotherapeutic agent in endodontics. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1981;51:434.
568. Berry EA, von der Lehr WN, Herrin HK. Dentin surfacetreatments for the removal of the smear layer: an SEM study.J Am Dent Assoc 1987;115:65.
569. Torabinejad M, Khademi AA, Babagoli J, et al. A new solu-tion for the removal of the smear layer. J Endod 2003;29:170.
570. Kaufman AY. Accidental ingestion of an endodontic instru-ment. Quintessence Int 1978;9:83.
571. Abou-Rass M, Patonai FJ Jr. The effects of decreasing surfacetension on the flow of irrigating solutions in narrow rootcanals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1982;53:524.
572. Cameron JA. The effect of a fluorocarbon surfactant on thesurface tension of the endodontic irrigant, sodium hypo-chlorite. A preliminary report. Aust Dent J 1986;31:364.
573. Tasman F, Cehreli ZC, Ogan C, Etikan I. Surface tension ofroot canal irrigants. J Endod 2000;26:586.
574. Zehnder M, Schicht O, Sener B, Schmidlin P. Reducingsurface tension in endodontic chelator solutions has noeffect on their ability to remove calcium from instrumentedroot canals. J Endod 2005;31:590.
575. Torabinejad M, Cho Y, Khademi AA, et al. The effect ofvarious concentrations of sodium hypochlorite on the abilityof MTAD to remove the smear layer. J Endod 2003;29:233.
576. Portenier I, Waltimo T, Ørstavik D, Haapasalo H. Killing ofEnterococcus faecalis by MTAD and chlorhexidine digluco-nate with or without cetrimide in the presence or absence ofdentine powder or BSA. J Endod 2006;32:138.
577. Krause TA, Liewehr FR, Hahn CL. The antimicrobial effectof MTAD, sodium hypochlorite, doxycycline, and citric acidon Enterococcus faecalis. J Endod 2007;33:28.
578. Baumgartner CJ, Johal S, Marshall JG. Comparison of theantimicrobial efficacy of 1.3% NaOCl/BioPure MTAD to5.25% NaOCl/15% EDTA for root canal irrigation. J Endod2007;33:48.
579. Torabinejad M, Shabahang S, Bahjri K. Effect of MTAD onpostoperative discomfort: a randomized clinical trial. JEndod 2005;31:171.
580. Girard S, Paque F, Badertscher M, et al. Assessment of a gel-type chelating preparation containing 1-hydroxyethylidene-1,1-bisphosphonate. Int Endod J 2005;38:810.
581. Sim TP, Knowles JC, Ng YL, et al. Effect of sodium hypo-chlorite on mechanical properties of dentine and tooth sur-face strain. Int Endod J 2001;34:120.
582. Grigoratos D, Knowles J, Ng YL, Gulabivala K. Effect ofexposing dentine to sodium hypochlorite and calciumhydroxide on its flexural strength and elastic modulus. IntEndod J 2001;34:113.
583. Calt S, Serper A. Time-dependent effects of EDTA on dentinstructures. J Endod 2002;28:17.
584. Sum CP, Neo J, Kishen A. What we leave behind in rootcanals after endodontic treatment: some issues and concerns.Aus Endod J 2005;31:94.
585. Guppy DR, Curtis RV, Ford TR. Dentine chips produced bynickel–titanium rotary instruments. Endod Dent Traumatol2000;16:258.
586. Chow TW. Mechanical effectiveness of root canal irrigation.J Endod 1983;9:475.
587. Kaufman AY. Facial emphysema caused by hydro-gen peroxide irrigation: report of a case. J Endod 1981;7:470.
588. Hulsmann M, Hahn W. Complications during root canalirrigation—literature review and case reports. Int Endod J2000;33:186.
589. Witton R, Brennan PA. Severe tissue damage and neurolo-gical deficit following extravasation of sodium hypochloritesolution during routine endodontic treatment. Br Dent J2005;198:749.
590. Bowden JR, Ethunanadan M, Brennan PA. Life-threateningairway obstruction secondary to hypochlorite extrusion dur-ing root canal treatment. Oral Surg Oral Med Oral Path OralRadiol Endod 2006;101:402.
591. Abou-Rass M, Piccinino MV. The effectiveness of four clin-ical irrigation methods on the removal of root canal debris.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1982;54:323.
990 / Endodontics

592. Moser JB, Heuer MA. Forces and efficacy in endodonticirrigation systems. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1982;53:425.
593. Druttman AC, Stock CJ. An in vitro comparison of ultra-sonic and conventional methods of irrigant replacement. IntEndod J 1989;22:174.
594. Walton RE, Torabinejad M. Principles and practice of endo-dontics. Philadelphia, PA: WB Saunders; 2001.
595. Senia ES, Marshall FJ, Rosen S. The solvent action of sodiumhypochlorite on pulp tissue of extracted teeth. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1971;31:96.
596. Salzgeber RM, Brilliant JD. An in vivo evaluation of the penetra-tion of an irrigating solution in root canals. J Endod 1977;3:394.
597. Sedgley C, Applegate B, Agel A, Hall D. Real-time imagingand quantification of bioluminescent bacteria in root canalsin vitro. J Endod 2004;30:893.
598. Cameron JA. The synergistic relationship between ultra-sound and sodium hypochlorite: a scanning electron micro-scope evaluation. J Endod 1987;13:541.
599. Griffiths BM, Stock CJ. The efficiency of irrigants in remov-ing root canal debris when used with ultrasonic preparationtechnique. Int Endod J 1986;19:277.
600. Cameron JA. The use of sodium hypochlorite activated byultrasound for the debridement of infected, immature rootcanals. J Endod 1986;12:550.
601. Walker TL, del Rio CE. Histological evaluation of ultrasonicdebridement comparing sodium hypochlorite and water. JEndod 1991;17:66.
602. Hulsmann M, Heckendorff M, Lennon A. Chelating agentsin root canal treatment: mode of action and indications fortheir use. Int Endod J 2003;36:810.
603. Teplitsky PE, Chenail BL, Mack B, Machnee CH. Endodon-tic irrigation—a comparison of endosonic and syringe deliv-ery systems. Int Endod J 1987;20:233.
604. Braun A, Kappes D, Kruse F, Jepsen S. Efficiency of a novelrinsing device for the removal of pulp tissue in vitro. IntEndod J 2005;38:8.
605. Nielsen BA, Baumgartner JC. Comparison of the EndoVacsystem to needle irrigation of root canals. J Endod2007;33:611.
606. Lee MT, Bird PS, Walsh LJ. Photo-activated disinfection ofthe root canal: a new role for lasers in endodontics. AusEndod J 2004;30:93.
607. Bonsor SJ, Nichol R, Reid TM, Pearson GJ. An alternativeregimen for root canal disinfection. Br Dent J2006;22:101.
608. Soukos NS, Chen PS, Morris JT, et al. Photodynamic therapyfor endodontic disinfection. J Endod 2006;32:979.
609. Dougherty TJ, Gomer CJ, Henderson BW, et al. Photo-dynamic therapy. J Nat Canc Inst 1998;90:889.
610. Soukos NS, Mulholland SE, Socransky SS, Doukas AG.Photodestruction of human dental plaque bacteria:enhancement of the photodynamic effect by photomecha-nical waves in an oral biofilm model. Lasers Surg Med2003;33:161.
611. Seal GJ, Ng Y-L, Spratt DA, et al. An in vitro comparisonof the bactericidal efficacy of lethal photosensitization orsodium hyphochlorite irrigation on Streptococcus inter-medius biofilms in root canals. Int Endod J 2002;35:268.
612. Lendini M, Alamano E, Migliaretti G, Berutti E. The effect ofhigh-frequency electrical pulses on organic tissue in rootcanals. Int Endod J 2005;38:531.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 991

CHAPTER 28
IRRIGANTS AND INTRACANAL MEDICAMENTS
MARKUS HAAPASALO, WEI QIAN
Infection Control in the Human Body
Successful elimination of opportunistic infections inmost parts of the human body usually requires onlyinvolvement of normal host defense mechanisms.Occasionally, a systemic antibiotic therapy or manip-ulative treatment (such as drainage of pus) is appliedin addition in order to resolve the infection. Elimina-tion of endodontic infection, however, follows a dif-ferent pathway. Host measures that are sufficient toeliminate the infective microorganisms in other sitesare unable to completely eliminate endodontic infec-tions. Because of the special anatomical challenges,control of an endodontic infection must be built ona joint effort by a number of host and treatmentfactors.1–3 Success in all parts of treatment will beneeded for elimination of infection and healing ofperiapical pathosis. The sequence of events and pro-cedures in the control of endodontic infections arehost defense system, systemic antibiotic therapy(rarely used with specific indications only), instru-mentation and irrigation (‘‘cleaning and shaping’’),intracanal medicaments used between appointments,permanent root filling, and coronal restoration.1–3
Host defense is responsible for the prevention ofspreading canal infections to the bone and to otherparts of the body. The body defense is usually success-ful in stabilizing the lesion size and preventing itsexpansion after the initial growth period. However,because of the lack of circulation, host defensemechanisms cannot effectively reach the microbesresiding inside the tooth in the necrotic root canalsystem. Mechanical instrumentation removes a por-tion of the microbes from the main root canal space,but its main purpose is to enhance irrigation and theplacement of medication and the root filling. Irriga-tion supports mechanical instrumentation, by redu-cing friction and removing dead and living microbesfrom the root canal. In addition, many irrigatingsolutions have antimicrobial activity that effectively
kill residual microbes in the canal. Intracanal antimi-crobial medicaments, on the other hand, are used inmulti-appointment endodontic treatments to com-plete the work started by instrumentation and irriga-tion and, optimally, to render the root canal systembacteria-free.
The classical study by Sjogren and his colleagues4
and by others indicated that a bacteria-free canal at thetime of filling is a prerequisite for high success rate andthat calcium hydroxide [Ca(OH)2] as an intracanalmedicament will predictably help reach this goal.5–7
A number of other studies, however, have chall-enged these results, and at present, there is no clearconsensus regarding the use of intracanal medica-ments, or the microbiological and other advantagesfrom their use.8–10
In this chapter, the focus is on the role of irrigationand intracanal medication in killing and reducing thenumber of bacteria in the root canal system. It is impor-tant, however, to understand that irrigation and localantibacterial dressings in the root canal are part of aconcerted effort to control endodontic infections. Alonethey cannot guarantee success if there are problems inquality of some other parts of the treatment.
Complete Elimination of Microbes
in the Root Canal System
Pulpitis is caused by microbial antigens entering thepulp from a carious lesion or a leaking filling throughdentinal tubules. As long as the pulp remains vital, thenumber of bacteria in the pulp is considered minimaland of no clinical significance. However, with proceed-ing infection, necrosis and apical periodontitis, theentire root canal system becomes invaded by bacteria.It has been shown beyond doubt that microorgan-isms are the etiological factor of apical periodontitis(Figure 1).11–13 It has been suggested that, in a small
992

number of cases, non-microbial factors are responsiblefor the persistence of the lesion after treatment.14,15
Nevertheless, there is general consensus that, in anoptimal situation, the goal of endodontic treatment isto remove and kill all microorganisms in the root canaland to neutralize any antigens that may be left in thecanal after killing the microbes. Reaching this goal isexpected to guarantee healing of periapical lesions. Ithas become obvious that complete destruction of rootcanal microbes is a particularly difficult challenge. Onthe other hand, in a high number of cases, high qualitytreatment is followed by complete healing.16–18 It hasalso been shown that a majority of cases harboringliving bacteria at the time of filling healed completely.4
It is clear, therefore, that although destroying 100% ofthe infective flora is the optimal goal, complete clinicaland radiographic healing can also occur when themicrobiological goal of treatment has not been fullyrealized. The situation may be compared to marginalperiodontitis and gingivitis, where it is not possible togain a totally bacteria-free environment in the gingival
crevice area. Periodontal treatment of good quality,however, results in healing of the periodontal disease.
The Goal of Endodontic Treatment
The goal, with the great majority of teeth requiringroot canal treatment, is either the prevention or treat-ment of apical periodontitis.19 In other words, the goalis prevention or elimination of a microbial infection inthe root canal system. In some special situations, suchas resorptions and endodontic complications, theremay be a variety of intermediate goals of a more‘‘technical’’ nature. Even then, the final success isdependent on successful infection control. There is awidely accepted view that cleaning and shaping of theroot canal system is the most important step toward asterile canal free from a microbial presence.
Instrumentation of the Root Canal
The goal of hand and rotary instrumentation andirrigation is to remove all necrotic and vital organictissue, as well as some hard tissue including dentinchips created by instrumentation, from the root canalsystem and give the canal system a shape that facil-itates optimal irrigation, debridement and placementof local medicaments, and permanent root filling.From a biological point of view, the goal of instru-mentation and irrigation is to remove and eradicatethe microorganisms residing in the necrotic root canalsystem. Furthermore, the goal is to neutralize anyresidual antigenic material remaining in the canalafter instrumentation and irrigation.
The Effect of Instrumentation
on the Root Canal Microbes
Instrumentation has a key role in the cascade oftreatment procedures to eradicate microbes in theroot canal system. Instrumentation removes a greatnumber of microbes from the accessible parts of themain root canal by direct mechanical cleaning action.Moreover, instrumentation shapes the root canal insuch a way that effective irrigation becomes possible.In other words, instrumentation is a way of mechani-cally removing microbes from the root canal. In addi-tion, it supports and facilitates mechanical removaland chemical eradication of the infection by irrigationduring and following instrumentation.
Figure 1 Bacteria are the etiological factor of apical periodontitis. Six-week-old biofilm on the main root canal wall created by a mixed cultureof oral bacteria under anaerobic conditions. Notice that several cellshave died (hollow cells) because of limited availability of nutrients.
Chapter 28 / Irrigants and Intracanal Medicaments / 993

The classical studies from Umea, Sweden havegreatly influenced our understanding of the effects ofinstrumentation and irrigation of the intracanalmicroflora.20 In a series of studies on teeth with apicalperiodontitis, the authors demonstrated that thor-ough mechanical instrumentation with hand stainlesssteel instruments, together with irrigation with eitherphysiological saline, ethylenediamine-tetra-acetic acid(EDTA), or EDTA and sodium hypochlorite(NaOCl), they were unable to predictably producesterile root canals. Fifteen root canals were instrumen-ted at five sequential appointments and sampled atthe beginning and end of each appointment. Theaccess cavity was sealed with a bacteria-tight tempor-ary filling, but the canals were left empty between theappointments. This procedure resulted in a 100- to1000-fold reduction in bacterial numbers, but it wasdifficult to obtain completely bacteria-free rootcanals. Corresponding results were also reported byØrstavik et al.21 and Cvek et al.22 in teeth with closedand immature apices. The antibacterial effect ofmechanical cleansing with sterile saline was reportedto be very low and limited to the teeth with fullydeveloped roots. NaOCl increased the antibacterialeffect as compared with saline irrigation. Interestingly,no statistical difference was found in the antibacterialeffect between 0.5% and 5.0% NaOCl solutions.22
The effects of instrumentation and irrigation wereinvestigated in an excellent series of studies by Dal-ton et al.23 They measured reduction in microbialcounts in 48 patients, on teeth instrumented with0.04 taper nickel–titanium (NiTi) rotary instrumentsor with stainless steel K-files using the step backtechnique with saline for irrigation. Bacteriologicalsamples were obtained before, during, and afterinstrumentation. All teeth with apical periodontitisyielded positive growth at the beginning, whereascontrol teeth with vital pulp and irreversible pulpitiswere sterile. A reduction in bacterial counts wasdetected with progressive enlargement of the rootcanals with both techniques. However, only 28%of the teeth became bacteria-free following instru-mentation.
Similar observations were reported by Siqueiraet al.24 when saline was used in irrigation. Interest-ingly, this study showed that increasing the size ofapical preparation from #30 to #40 resulted in a sig-nificant reduction in microbial counts. Ex vivo studiesby Pataky et al.,25 using 40 human first maxillarypremolars extracted for orthodontic reasons, also ver-ified the difficulty of obtained sterility of the infectedcanal space by instrumentation and saline irrigation.Although a considerable reduction in bacterial counts
was detected after instrumentation, none of the teethbecame bacteria-free. It should be mentioned, how-ever, that the size of the master apical file in some ofthe studies was quite small, #25, and that may increasethe possibility of positive cultures.25 It can be con-cluded that instrumentation and irrigation with salinealone cannot predictably eliminate all bacteria frominfected root canals. Therefore, it is not surprisingthat the focus of activity in root canal disinfection isplaced on the development and use of irrigating solu-tions and other intracanal disinfecting agents withstrong antibacterial activity. In addition, there isgrowing interest in the combined effect of ultrasonicenergy and irrigating solutions as well as other newways of mechanical irrigation.
Root Canal Disinfection
by Chemical Means
THE CHALLENGES AND PITFALLSIN STUDYING THE ANTIMICROBIALEFFECTIVENESS OF ENDODONTICIRRIGATING SOLUTIONS ANDINTRACANAL MEDICAMENTS
In Vitro ModelsThe testing of the antimicrobial activity of variouschemical compounds may appear to be straightforwardand simple procedure. In theory, this may be true—themicrobes of interest are exposed to the antimicrobialagent to be examined. At certain time intervals, micro-biological samples are collected and cultured on suit-able media. The results are then expressed as the lengthof time required to kill all microbes. In reality, regard-ing endodontic disinfecting agents, it is, however, quitedifferent. Research focusing on the antimicrobial effec-tiveness of irrigating solutions and temporarily usedintracanal medicaments has in many occasions adoptedtechniques originally designed for some other context,for example, antibiotic susceptibility using agar plates.Testing of systemically used antibiotics is based on tensof years of international standardization.26–30 The che-mical composition of both the antibiotic discs and theculture media used in testing are defined in detail inorder to secure predictable diffusion of the active ingre-dient of the antibiotic and the absence of chemicalreactions between the agar plate ingredients and theantibiotic. Zones of inhibition of growth around theantibiotic disc have been compared through clinicalstudies to the serum and tissue concentrations that
994 / Endodontics

are possible to reach with safe dosages of low toxicity,as well as the clinical effectiveness of the antibiotics. Inaddition, reference strains from culture collections withknown antibiotic susceptibilities are used as internalstandards for quality testing of each new batch ofplates. Most aerobic and facultative bacteria can bereliably tested using the disc diffusion method. How-ever, despite years of extensive research, there is still nogenerally accepted standard for susceptibility testinganaerobic bacteria using the disc diffusion method.31
The use of agar diffusion method in endodontics,despite good intentions, is not based on any kind ofstandardization of the media or the tested materials.Chemical interactions between the media and thedisinfecting agents are largely unknown. Further-more, there are no true comparative studies helpingto draw conclusions from the zones of inhibition tothe performance of the disinfectants in vivo. Theantimicrobial effect of some endodontic medica-ments is based on the pH effect; therefore, the buf-fering capacity of the agar plate is in key position indetermining the diameter of the growth inhibitionzone. Another example is EDTA, that causes a zoneof inhibition on an agar plate, but fails to reduce thenumber of viable microbes even after 24-hour incu-bation in a test tube. The growth inhibition on agarplates is based on removal of important ingredientsfrom the media by EDTA, that makes the mediumunsuitable for growth of many species. Such bac-teria, even if alive, cannot multiply on the platewhich has been nutritionally altered by EDTA. Inconclusion, the information obtained from agar dif-fusion studies is at best of limited value and shouldnot be used to compare and select disinfectingagents for clinical use.
Another matter of importance in susceptibilitytesting is understanding the difference between bac-teriostatic and bactericidal activities. Bacteriostaticmeans prevention of growth of the microbial cells.However, they are not killed, unlike when the med-icament has bactericidal activity. In endodontic stu-dies, this difference is not always clearly addressed,and the results are often reported as ‘‘antibacterialactivity.’’ The agar diffusion test, when properlyused, is an example of measuring bacteriostaticactivity. In endodontics, a bactericidal effect of adisinfecting agent is more important than a bacter-iostatic effect. In the necrotic root canal system, atemporary prevention of bacterial growth (as long asthe disinfecting agent remains in the canal) is oflimited value, because the microbes may still growin numbers afterwards causing a new challenge tothe host defense.
Testing endodontic disinfecting agents in vitro canbe done in test tubes using a mixture of the microbes(suspended in sterile water) and the medicament. Thepresence of a culture medium in the mixture is com-monly seen in endodontic literature. However, culturemedium or other organic material is a confoundingfactor: the disinfecting agents vary in their suscept-ibility to the inactivating effect of the various organicsubstances.32 Experiments done under such condi-tions do not give a reliable picture of the character-istics and activity of the medicament/disinfectantagainst the tested microbe.
‘‘Carry-over effect’’ means that the medicament,in active form, follows along with the sample into thedilution series and even to the culture plate (orliquid culture), where surviving microbes are calcu-lated [e.g., ‘‘percentage of colony forming units(CFU) surviving’’]. A high enough concentration ofthe disinfectant, in such a situation, can cause a false-negative result: the microbes are not killed, but resi-dual medicament in the culture media prevents theirgrowth by a bacteriostatic effect. Thus, carry-over, ifundetected, gives a too positive picture of the anti-bacterial effectiveness of the medicament. Endodon-tic irrigants and disinfecting agents, containing localantibiotics, are at particularly high risk of causingfalse-negative results. Effective inactivators are notavailable for many antibiotics. If they are used inhigh concentration, carry-over effect is possible evenafter several 10-fold dilutions.32
Various inactivating agents are used to prevent theeffects of carry-over. Citric acid has been used in theroot canal to neutralize Ca(OH)2, sodium thiosulfateneutralizes NaOCl,33 and a mixture of Tween 80 andalpha-lecithin inactivates chlorhexidine (CHX).34
Inactivation, however, is dependent on the concentra-tion of the medicaments. When they are used in highconcentration, inactivation may not be complete. Agood example of this is CHX that cannot be effectivelyinactivated with Tween and alpha-lecithin if CHXconcentrations of 1% or more are used (Figure 2A).The importance of the careful design of the experi-ments and proper controls cannot be overestimated, inorder to avoid the possibility of false negative results.
Ex Vivo and In Vivo ModelsIn vitro models give valuable information about thespectrum and antimicrobial potential of endodontic dis-infecting agents. However, information from suchexperiments alone is not enough to predict their perfor-mance in a clinical situation in the root canal. The effec-tiveness of the medicament in vivo can be reduced by avariety of factors. These include problems in delivery, low
Chapter 28 / Irrigants and Intracanal Medicaments / 995

overall volume, poor/incomplete penetration in the mainroot canal system, poor penetration into dentin, shortcontact time, or inactivation of the activity of the disin-fecting agent by one or more of the chemical compoundspresent in the necrotic root canal. Therefore, a number ofex vivo and in vivo models have been developed in orderto meet the challenge by the various confounding factorsof the root canal and to improve the correlation betweenthe test results and clinical performance. The ex vivo andin vivo models include the dentin block model,35,36 den-tin powder model,37–39 and several modifications usingroots/root canals from extracted teeth.40,41 More studiesare also made in vivo during the treatment of endodonticinfections.42,43
The dentin powder model, with its modifications,makes it possible to obtain information about theinhibition of the medicament activity by dentin andother compounds (biomolecules, microbial biomass,etc.) in various concentrations.37 It also allows stan-dardization of the experimental conditions for largeseries of tests. Prolonged incubation time to createdentin infection is not required because the dentin ispowdered. The downsides of the powder modelinclude partial loss of the microanatomical structureof the tooth and the difficulty to use/create microbialbiofilms. In short, the dentin powder model is aneffort to simulate the chemical environment of thetooth.
The dentin block model has been widely used fortesting endodontic medicaments.35 The benefits ofthe model include simulation of the chemical andmicroanatomical environment of the tooth and theroot canal system. The root canal is usually stan-dardized in size, making it easier to obtain compar-
able samples of dentin in different blocks. It alsoallows the use of microbial biofilms in the experi-ments. On the other hand, the dentin block modelis quite laborious in use; it cannot be fully standar-dized as different blocks may vary in thickness anddentin microstructure. Handling of the block pre-sents some challenges which may increase the riskfor false-positive results (contaminations from out-side the sampling area). Despite its limitations, thedentin block model has greatly contributed to ourunderstanding of dentin disinfection, and it is stillfrequently used in endodontic research.
Newer ex vivo and in vivo models use ‘‘natural’’root canals either in extracted teeth or directly in vivo.The obvious benefit of these experiments is the morecomplete simulation of the clinical situation; theresults obtained with the various materials may bestreflect their true activity clinically. However, in addi-tion to the well-known difficulty to organize con-trolled clinical studies, and to gather patients for suchstudies, there are also other potential pitfalls that mayweaken the usefulness of the results. These include thedifficulty to standardize the size of the apical prepara-tion because of the great natural variation in canalsizes, different total volume of the canals, variations inthe microanatomy of the root canals, and differencesin the quality and quantity of the microbial infection.In addition to this kind of natural variation, theredoes not seem to be any standard way of dealing withthe smear layer or taking the microbiological samples.According to the treatment protocols, the smear layerhas not been removed in a great number of thestudies. This is likely to have an effect on the abilityof several sampling methods to collect viable
A B
Figure 2 A, Samples of Enterococcus faecalis from 10-fold dilution series after a brief contact with 2% chlorhexidine. Because of short contact time (2seconds), no killing has taken place. Chlorhexidine (CHX) ‘‘carry-over’’ has prevented growth of the first two samples (arrows) on the plate (upper row,left) despite the presence of Tween-lecithin inactivator in the dilution series. Lower row: control sample with no CHX. If only the first two dilutions hadbeen made, the result would have indicated complete killing of the microbes in just 2 seconds. B, The size of the initial inoculum and the length of thedilution series determine the depth of measurement of the colony forming units. In this example, killing effectiveness can by calculated to a level ofabout 99.99%. Upper row: medicament; lower row: control.
996 / Endodontics

microorganisms left in the dentinal tubules or lateralcanals behind the smear layer. In quantitative studieswhere dentin is sampled, it is difficult to collect equalamounts of dentin (sample) because of the naturalvariations in canal sizes and shapes and different typesof instruments used.
QUALITATIVE OR QUANTITATIVERESULTS; DETECTION LEVEL:MORE CHALLENGES?Optimally, the goal of endodontic disinfection is com-plete eradication of the microbes from the root canalsystem of the affected tooth. Although difficult toachieve, this noble goal may have affected the studydesign of several studies as the results are oftenexpressed qualitatively, only as ‘‘growth’’ or ‘‘nogrowth.’’ This approach may in some cases hide differ-ences in the effectiveness of different treatment proto-cols and chemicals used for disinfection. For example,two different treatments that cause 10% and 99.95%reduction in bacterial counts per canal, respectively,are reported as equal (‘‘growth’’), unless the overallnumber of ‘‘no growth’’ cases is higher with one of themethods. It is possible that some of the recent poorresults with Ca(OH)2 as a disinfecting agent can bepartly explained by the fact that qualitative rather thanquantitative approach has been used to measure theeffectiveness of the disinfection. Quantitative measure-ment of the effect by endodontic disinfecting agentsshould therefore be preferred over qualitative approach.Accordingly, quantitative reporting has been used insome studies.32,44
However, there are a number of factors that createchallenges for accurate and comparable counting ofmicrobes in the samples. Residual medicament indentin may result in a very low number of CFU persample unless neutralizing agents are properly used.Dispersing the sample effectively may be required todetach the viable cells from the dentin chips, toincrease the CFU numbers to correctly reflect the truenumber of microbes in the sample. Collection of smalldentin samples is technically demanding and requiresgreat care to secure a standardized yield from allsamples. When the overall number of CFU in thesample is low, which is often the situation in infectedand medicated dentin, it is also important not to losethe microbes during too vigorous dilution process.
Success in both qualitative and quantitative mea-surement of (surviving) microbes is dependent,among other factors mentioned above, on the designof the microbiological procedures that determine thedetection level of the method. Detection level dic-
tates whether the most effective killing can beannounced, for example, on the level of 99%,99.9% or 99.99% (see Figure 2B). In other words,detection level tells how many cells in the test mix-ture must be alive so that growth can be detected bythe culturing. Detection level is mainly dependent onthe total number of cells in the initial reaction mix-ture/sample, proportion of the initial sample trans-ferred into the dilution series, and the proportion ofthe mixture plated from each dilution. Theoretically,the detection limit can be easily calculated from theabove numbers. In practice, detection limit is oftenreduced by carry-over of strong medicaments such asCHX or MTAD that may cause false-negative resultsat the beginning of the dilution series. Detectionlimit gives important information about the designand quality of the methods in studies of endodonticdisinfecting agents. Unfortunately, detection limitsare only rarely reported, making it more difficult tocompare the results from different studies. Onewould hope that in the future, reporting the detec-tion limit will be a routine requirement for studieson endodontic disinfection.
ANTIBACTERIAL IRRIGATING SOLUTIONSThe use of irrigating solutions is an important part ofendodontic treatment. The irrigants facilitate removalof necrotic tissue, microorganisms and dentin chipsfrom the root canal by a flushing action. Irrigants canalso help prevent packing infected hard and soft tissueapically in the root canal and into the periapical area.Some irrigating solutions dissolve either organic orinorganic tissue. Finally, several irrigating solut-ions exhibit antimicrobial activity by actively killingbacteria and yeasts when in direct contact with themicroorganisms. On the negative side, many irrigatingsolutions have shown cytotoxic activity and may causesevere pain reaction if they gain access into the peria-pical tissues.45
An optimal irrigant should have all or most of thepositive characteristics listed above, but none ofthe negative or harmful properties. Presently, none ofthe available irrigating solutions can be regarded asoptimal. However, with a combined use of selectedproducts, irrigation will greatly contribute to successfuloutcome of treatment.
NaOClNaOCl is the most widely used irrigating solution. Inwater, NaOCl ionizes to produce Na+ and the hypo-chlorite ion, OCl–, that establishes an equilibriumwith hypochlorous acid, HOCl. Between pH 4 and 7,
Chapter 28 / Irrigants and Intracanal Medicaments / 997

chlorine exists predominantly as HClO, the active moi-ety, whereas above pH 9, OCl– predominates.46 It is thehypochlorous acid that is responsible for bacteria inac-tivation, the OCl– ion being less effective than theundissolved HOCl. Hypochlorous acid disrupts oxida-tive phosphorylation and other membrane-associatedactivities as well as DNA synthesis.47,48
NaOCl is used in concentrations varying from 0.5to 7%. It is a very potent antimicrobial agent andeffectively dissolves pulpal remnants and organiccomponents of dentin (Figure 3). It is used both asan unbuffered solution at pH 11 in concentrationsmentioned above and buffered with a bicarbonatebuffer (pH 9.0) usually as a 0.5% (Dakin’s solution)or 1% solution.46 Contradicting earlier statements,Zehnder et al.49 reported that buffering had littleeffect on tissue dissolution, and Dakin’s solutionwas equally effective on decayed (necrotic) and freshtissues. In addition, no differences were recorded forthe antibacterial properties of Dakin’s solution withan equivalent unbuffered hypochlorite solution.49
NaOCl is best known for its strong antibacterialactivity; it kills bacteria very rapidly even at low con-centrations. Waltimo et al.50 showed that the resistantmicroorganism, Candida albicans, was killed in vitro in30 seconds by both 5% and 0.5% NaOCl, whereasconcentrations 0.05% and 0.005% were too weak to
kill the yeast even after 24 hours of incubation. Thehigh susceptibility of C. albicans to NaOCl was recentlyalso verified by Radcliffe et al.33 Later, Vianna et al.51
contrasted these results partly, as 0.5% NaOCl required30 minutes to kill C. albicans, whereas 5.25% solutionkilled all yeast cells in 15 seconds. In the latter study,however, organic material from the broth culture med-ium may have been present during the incubation withNaOCl which would explain delayed killing. Gomeset al.52 tested in vitro the effect of various concentra-tions of NaOCl against enterococcus. Enterococcusfaecalis (Figure 4) was killed within 30 seconds by the5.25% solution, while 10 and 30 minutes was requiredfor killing all bacteria by 2.5 and 0.5% solutions,respectively. The higher resistance of E. faecalis tohypochlorite as compared with the yeast C. albicanswas suggested also by Radcliffe et al.33 However, bothof these studies are in contrast to the results reportedby Haapasalo et al.37 who demonstrated rapid killing ofE. faecalis by 0.3% NaOCl and by Portenier et al.53 whowere able to show rapid killing of E. faecalis strains inlogarithmic and stationary growth phase by even0.001% NaOCl.
Experiments with Gram-negative anaerobic rodsPorphyromonas gingivalis, Porphyromonas endodonta-lis, and Prevotella intermedia, often isolated from api-cal periodontitis, demonstrated high susceptibility to
A B
Figure 3 A, Instrumented (upper part of the picture) and uninstrumented (lower part) root canal wall after irrigation with 5% sodium hypochlorite(NaOCl) for 10 minutes. Pulpal remnants and predentin have been effectively removed with NaOCl while the instrumented part (smear layer) seemsrelatively unaffected. Notice the typical calcospherites at the lower part of the image. B, Calcospherites on the uninstrumented canal wall after irrigationfor 10 minutes with 2.6% NaOCl.
998 / Endodontics

NaOCl, and all three species were killed within 15seconds with 0.5 to 5% concentrations of NaOCl.51
The differences between in vitro and in vivo studiesinclude the volume of the medicament available for kill-ing, access to all microbes, and absence of other materialsin the in vitro experiments that potentially protect bac-teria in vivo. Many of the in vivo studies have failed toshow a better antibacterial effect in the root canal by highconcentrations of NaOCl as compared to low concentra-tions. Bystrom and Sundqvist54,55 studied root canalsnaturally infected, mainly with a mixture of anaerobicbacteria, and showed that although 0.5% NaOCl, withor without EDTA, improved the antibacterial efficiency ofpreparations compared with saline irrigation, all canalswere not bacteria free even after several appointments. Nosignificant difference in antibacterial efficiency in vivobetween 0.5 and 5% NaOCl solutions was found in thestudy. Siqueira et al.56 using E. faecalis-infected root canalsdemonstrated the superior antibacterial affect against rootcanal bacteria of hypochlorite in comparison with phy-siological saline. However, no difference was detectedbetween 1, 2.5, and 5% NaOCl solutions.
Many of the studies about the antibacterial effect ofNaOCl against root canal bacteria are in vitro studies,in either ‘‘neutral’’ test tube conditions, in the rootcanals of extracted teeth, or in dentin blocks infectedwith a pure culture of one organism at a time. The invivo studies, on the other hand, have focused on theeradication of bacteria from the root canals of teethwith primary apical periodontitis.
Peciuliene et al.57 studied the effect of instrumenta-tion and NaOCl irrigation in failed, previously root-filled teeth with apical periodontitis. Old root fillingswere removed with hand instruments, and the firstsample was taken. No chloroform was used to avoidfalse-negative cultures. Bacteria were isolated in 33 ofthe 40 teeth before further instrumentation. E. faecaliswas found in 21 teeth (in 11 as a pure culture), theyeast C. albicans in 6 teeth, Gram-negative entericrods in 3 teeth, and other microbes in 17 teeth. Thecanals were then hand instrumented to size #40 orlarger and irrigated with 2.5% NaOCl (10 mL percanal) and 17% buffered EDTA (pH 7 and 5 mL percanal). After instrumentation and irrigation, E. faeca-lis was still detected in six canals. Other microbespersisted in five canals after preparation. EntericGram-negative rods were no longer present in thesecond sample.
The disappearance of yeasts but not E. faecalis in theroot canals may reflect their different susceptibilities tothe described chemomechanical instrumentation or itmay be a result of different biofilm characteristics anddentin penetration by these species.
The weaknesses of NaOCl include unpleasant taste,toxicity, and its inability to remove smear layerbecause of its lack of effect on inorganic material.58,59
The poorer antimicrobial effectiveness of NaOCl invivo than in vitro is also somewhat disappointing.There are several possible reasons for the reduced invivo performance. Root canal anatomy, particularlythe difficulty to effectively irrigate the most apicalregion of the canal, is generally acknowledged as oneof the main challenges. In addition, the chemicalmilieu in the canal is different from a test tube.Haapasalo et al.37 showed that the presence of dentincaused marked delays in the killing of E. faecalis by1% NaOCl. The effect of other materials present inthe necrotic or previously treated root canal, to theantimicrobial potential of NaOCl, has not been stu-died.
Studies measuring NaOCl cytotoxicity have indi-cated greater cytotoxicity and caustic effects onhealthy tissue with 5.25% NaOCl than with 1.0 and0.5% solutions.60,61 The fear of toxic and chemicalcomplications is the main reason for that low concen-trations 0.5 to 1% NaOCl solutions are used for canalirrigation instead of the 5.25% solution in manycountries.45 However, more in vivo studies on persis-tent endodontic infections and retreatment are neces-sary for a deeper understanding of the relationshipbetween NaOCl concentration and its antimicrobialactivity against specific microorganisms, before final
Figure 4 A scanning electron micrograph of growing Enterococcusfaecalis cells.
Chapter 28 / Irrigants and Intracanal Medicaments / 999

conclusions can be drawn regarding the optimalNaOCl concentration.
EDTA, Citric Acid and Other AcidsEDTA (17%, disodium salt, pH 7) has little if anyantibacterial activity. On direct exposure forextended time, EDTA releases some of the bacteria’ssurface proteins by combining with metal ions fromthe cell envelope. This can cause even bacterialdeath. More importantly, EDTA is an effective che-lating agent in the root canal.62,63 It removes smearlayer (Figure 5) when used together (but not simul-
taneously) with NaOCl by acting on the inorganiccomponent of the dentin (Figure 6). Therefore, byfacilitating cleaning and removal of infected tissue,EDTA contributes to the elimination of bacteria inthe root canal. It has also been shown that removalof the smear layer by EDTA (or citric acid) improvesthe antibacterial effect of locally used disinfectingagents in deeper layers of dentin.35,36 Niu et al.64
studied the ultrastructure on canal walls after EDTAand EDTA plus NaOCl irrigation by scanning elec-tron microscopy (SEM): more debris was removedby irrigation with EDTA followed by NaOCl thanwith EDTA alone (Figure 7).
A B
Figure 5 A, Smear layer on the surface of the root canal wall after hand instrumentation with H-files. B, Smear layer after instrumentation of the rootcanal before ethylenediamine-tetra-acetic acid irrigation.
A B
Figure 6 A, Instrumented root canal wall after irrigation with 5% sodium hypochlorite (NaOCl) and 17% ethylenediamine-tetra-acetic acid (EDTA), eachfor 5 minutes. Smear layer has been completely removed. B, Close-up scanning electron micrograph of the root canal wall after removal of smear layerwith NaOCl and EDTA.
1000 / Endodontics

Citric acid can also be used for irrigation of the rootcanal and for removal of the smear layer.62,65,66 Similarto EDTA, complete removal of smear layer requires alsoirrigation with NaOCl before or after citric acid irriga-tion (Figure 8). Concentrations ranging from 1 to 50%have been used.65 In comparison with ultrasound, 10%citric acid has been shown to remove the smear layermore effectively from apical root-end cavities thanultrasound.67 In another study, powdered dentin–resinmixture was more soluble in a 0.5, 1, and 2 M citric acid
than in 0.5 M EDTA.68 Contrary to this, Liolios et al.69
reported better removal of smear layer by commercialEDTA preparations than with 50% citric acid, whileother studies have found only small or no differencebetween citric acid and 15% EDTA in their capacity toremove the smear layer.70,71 A comparative studyshowed that 10% citric acid was more effective than1% citric acid, which was more effective than EDTAin demineralizing dentin.72 Takeda et al.73 reportedthat irrigation with 17% EDTA, 6% phosphoric acid,and 6% citric acid did not remove the entire smearlayer from the root canal system. This is not unex-pected, however, as it is known that NaOCl is alsorequired for complete removal of the smear layer. Theacids demineralized the intertubular dentin makingthe tubular openings larger than by EDTA. Theauthors also showed that CO2 laser was useful inremoving the smear layer and that the Er:YAG laserwas even more effective than the CO2 laser in smearlayer removal.
Smear layer removal facilitates penetration of sealersinto the dentinal tubules. It also enhances disinfectionof the root canal wall and deeper layers of dentin. BothEDTA and citric acid can effectively remove the smearlayer when used together with NaOCl. Citric acid andEDTA may have weak antimicrobial activity as stand-alone products. However, their antimicrobial effective-ness has not been extensively documented and appearsto be of minor importance.
A B
Figure 8 A, Instrumented root canal wall after irrigation for 10 minutes with 50% citric acid only. Similar to ethylenediamine-tetra-acetic acid, sodiumhypochlorite irrigation is needed in addition for complete removal of the smear layer. B, Uninstrumented part of the root canal wall after irrigation for 10minutes with 50% citric acid. Citric acid alone cannot dissolve the organic tissue within a reasonable time.
Figure 7 Partial removal of smear layer by irrigation for 10 minutes with17% ethylenediamine-tetra-acetic acid only. Mainly organic material hasbeen left covering the surface.
Chapter 28 / Irrigants and Intracanal Medicaments / 1001

Hydrogen PeroxideHydrogen peroxide (H2O2) is a biocide that has beenwidely used for disinfection and sterilization.46 How-ever, in endodontics, H2O2 has not been very popular,and presently its use is generally in decline. H2O2 is aclear and colorless liquid. Concentrations from 1 to30% have been used. H2O2 produces hydroxyl-freeradicals (HO.) that attack microbial components suchas proteins and DNA.46 H2O2 is nonproblematic froman environmental point of view because it degradesinto water and oxygen. H2O2 is relatively stable insolution, but many products contain stabilizers toprevent decomposition. H2O2 has antimicrobial activ-ity against various microorganisms including viruses,bacteria, yeasts, and even bacterial spores.74 It is moreeffective against Gram-positive than Gram-negativebacteria. Catalase or superoxide dismutase producedby several bacteria can provide them partial protec-tion against H2O2.
Use of H2O2 in endodontics has been based on itsantimicrobial and cleansing properties. Thirty per-cent H2O2 (Superoxol) has been recommended asthe first step in tooth surface disinfection aftermechanical cleaning.75 H2O2 acts on the organicmatter on the tooth making other disinfectants, suchas iodine, more effective. It has been widely usedearlier for cleaning the pulp chamber from bloodand tissue remnants. It has also been used in canalirrigation, but evidence supporting the effectivenessof H2O2 as a root canal irrigant is scarce. On thecontrary, Siqueira et al.76 reported that a combina-tion of NaOCl and H2O2 gave no advantage overNaOCl alone against E. faecalis in contaminated rootcanals ex vivo. Heling and Chandler77 found strongsynergism between H2O2 and Chlorhexidine (CHX)in disinfection of infected dentin: a combination ofthe two medicaments at low concentration was farmore effective in sterilizing dentin than these or anyother medicament alone. The synergistic mode ofaction between CHX and H2O2 was later documen-ted also by Steinberg et al.78 In a recent study, 10%H2O2 was used as part of the irrigating protocol inmonkey teeth.79 A total of 186 root canals in 176teeth were inoculated with a known mixture of bac-teria for several months. One group consisted ofanaerobic bacteria and streptococci; the secondgroup was identical to group one except with addedE. faecalis. The root canals were sampled and instru-mented manually to size #40 to #60 and irrigatedwith buffered 1% NaOCl, followed by 10% H2O2.Final irrigation was with NaOCl. Sodium thiosulp-fate was used to inactivate hypochlorite before sam-
pling, and a second bacteriological sample was taken.In group 1 (160 canals), bacteria were found in 98%and 68% of the canals in samples 1 and 2, respec-tively. In group 2, with E. faecalis, the correspondingfrequencies were 100% and 88%. Although the bac-terial counts were greatly reduced, the study indi-cated the difficulty to completely eradicate bacteriafrom infected root canals in monkey teeth.79
Despite the long history of use of H2O2 in endo-dontics, evidence supporting its use is at best weak.However, it still has a role as part of the tooth surfacedisinfection protocol. Furthermore, the potentialbenefit of the suggested synergistic effect with CHXin deep dentin disinfection remains to be evaluatedclinically.
CHXChlorhexidine digluconate (CHX) is widely used in dis-infection because of its excellent antimicrobial activity.80–82
It has gained increased popularity in endodontics as anirrigating solution and as an intracanal medicament.Unlike NaOCl, CHX does not have bad smell, it is notequally irritating to periapical tissues, and neither does itcause dramatic spot bleaching of the patients clothes. Itsantimicrobial effectiveness is well documented in endo-dontics. However, it completely lacks tissue dissolvingcapability, an important reason for the popularity ofNaOCl (Figure 9).
CHX is perhaps the most widely used antimicrobialagent in antiseptic products. It permeates the cell wall orouter membrane (Gram-negative cells) and attacks thebacterial cytoplasmic or inner membrane of the yeastplasma membrane. In high concentrations, CHX causescoagulation of intracellular components.46 CHX gluco-nate has been in use for some time in dentistry becauseof its antimicrobial properties, its substantivity (long-term continued effect), and its relatively low toxicitycompared to some other agents. However, the activityof CHX is dependent on the pH and is greatly reducedalso in the presence of organic matter.82
CHX is effective against both Gram-positive andGram-negative bacteria as well as yeasts, althoughactivity against Gram-negative bacteria is not as goodas against Gram-positive bacteria.83–85 Mycobacteriaand bacterial spores are resistant to CHX.80,81 There-fore, CHX is not as suited to chairside sterilization ofgutta-percha cones as NaOCl.86,87 Studies indicatingequally good performance by CHX and NaOCl ingutta-percha disinfection have not used bacterialspores in testing.88 CHX is not very effective againstviruses, its activity being limited to viruses with a lipidenvelope.89 CHX is cytotoxic in direct contact with
1002 / Endodontics

human cells. A study using fluorescence assay onhuman periodontal ligament (PDL) cells showed nodifference in cytotoxicity by 0.4% NaOCl and 0.1%CHX.61 The potential benefits of using CHX in endo-dontics have been under active research over the lastseveral years. Several studies have compared the anti-bacterial effect of NaOCl and CHX against intracanalinfection.
While many studies show little or no differencebetween their antimicrobial effectiveness,77,90–92 theirmode of action may indicate important differences.The effects of 15 minutes of irrigation of experimentalbiofilms by mixtures of endodontic bacteria on dentinblocks have been evaluated by SEM and by cultur-ing.93 Six percent NaOCl was the only irrigant thatcompletely eliminated (removed) the biofilm as ver-ified by SEM observations and killed all bacteria. Twopercent CHX was equally effective in bacterial killing,and no growth was detected in any of the samplesafter the CHX treatment. However, an importantdifference was observed in how the biofilm was struc-turally affected by irrigation with these two solutions:6% hypochlorite completely removed the biofilmwhile the CHX solution had no effect on the biofilmstructure.93 Although the bacteria were killed, theresult indicates that as the biofilm remains in thecanal after CHX irrigation, it may continue to expressits antigenic potential if allowed the possibility to
communicate with living periapical tissue. Moreover,such residual organic tissue may have a negativeimpact on the quality of the seal of the permanentroot filling. Different types of biofilm are shown inFigure 10.
Some studies have indicated differences in thekilling of certain endodontic microbes by hypochlor-ite and CHX. An in vitro study demonstrated differ-ences in the killing of enterococci by CHX andNaOCl. While 5.25% NaOCl killed E. faecalis within30 seconds, lower concentration (4.0 to 0.5%) ofhypochlorite required 5 to 30 minutes for completekilling of the bacteria.52 In the same study, 0.2 to2% CHX killed the E. faecalis cells in 30 seconds orless in all concentrations tested. The result was latersupported by two other studies using E. faecalis andStaphylococcus aureus as test organisms.51,94 How-ever, the results of these studies have been contra-dicted by some other studies with regard to theeffectiveness of NaOCl.37,53
The antifungal effectiveness of CHX has been shownin several studies.50,95–97 In a study of the effectiveness ofvarious endodontic disinfecting agents, it was found thatcombinations of disinfectants were equally or less effec-tive against fungi than the more effective componentalone.50
An interesting, but not yet fully understood syner-gism has been reported between CHX and H2O2.77 In
A B
Figure 9 A, Instrumentation smear layer seems intact after irrigation for 10 minutes with 2% chlorhexidine. B, Uninstrumented area in the root canalafter irrigation with 2% chlorhexidine only. Chlorhexidine has no tissue dissolving capability.
Chapter 28 / Irrigants and Intracanal Medicaments / 1003

A B
C D
E
Figure 10 A, Densely packed natural biofilm (in vivo) on the root canal wall of a tooth with apical periodontitis. The film consists of bacteria of differenttypes and shapes and remnants of necrotic pulp tissue. B, Cocci and rod-shaped bacteria in necrotic pulp tissue of a tooth with apical periodontitis. C,Early stages of biofilm formation in vitro on root dentin by a mixture of oral bacteria. Binding of coccoid cells on long rod-shaped bacteria can be seen. D,More advanced stage of biofilm formation in vitro on root dentin by a mixture of oral bacteria. Many of the bacterial cells in the larger aggregate areembedded in extracellular matrix. E, Biofilm by a mixture of oral bacteria grown under increased CO2 atmosphere in vitro on root dentin.
1004 / Endodontics

vitro studies using the dentin block model indicatedstrong synergism between these two agents againstE. faecalis infection in dentinal tubules. Complemen-tary in vitro experiments by Steinberg et al.78 demon-strated that the combination of CHX and H2O2
completely eradicated E. faecalis in concentrationsclearly lower than required when the compounds wereused alone. It is possible that CHX, as a membraneactive agent, makes the bacterial membranes morepermeable to H2O2, that can more easily penetratethe cells and cause damage to the intracellular orga-nelles.78 Although NaOCl and H2O2 are occasionallyused together in root canal irrigation, such synergisticeffect has not been detected between them in thedentin block model.77 The CHX–H2O2 synergismhas been demonstrated also in a study of antiplaquemouth rinse.98 Surprisingly, so far there are no pub-lished studies of the clinical performance of the com-binations of CHX and H2O2. Combinations of CHXand carbamide peroxide have been shown to be addi-tive in their cytotoxicity,99 but corresponding experi-ments with CHX and H2O2 are lacking.
Inhibition of the antimicrobial activity of endodonticirrigants, by substances present in the root canal, hasrecently been discussed in a number of studies.37–39
Haapasalo et al.37 showed in an in vitro study that theeffect of CHX is reduced or delayed, by the presence ofdentin. In following studies by the same group, Portenieret al.38 detected loss of CHX antimicrobial activity byhigh concentration (18%, v/w) of bovine serum albu-min. In a clinical situation, inflammatory exudate rich inproteins may thus have a negative impact on the effec-tiveness of CHX. A subsequent study showed thatorganic dentin matrix and heat-killed microbial cellswere effective inhibitors of CHX activity.39 In a studyby Sassone et al.,100 CHX was incubated together withlow concentration (0.5%, v/w) albumin, and no inhibi-tion of the CHX activity could be detected. Albuminconcentration in human serum is approximately 2 to 3%and the total protein concentration is approximately7%.101
During the last few years, several studies have mea-sured the activity of CHX gel against root canal bac-teria. Vianna et al.51 found that CHX in a gel formrequired a longer time to kill E. faecalis than the corre-sponding concentration in a liquid. Oliveira et al.102
reported that 2% CHX gel and 5.25% NaOCl showedexcellent activity against E. faecalis. When diluted to1.5% solution, NaOCl reduced the E. faecalis countsinitially, but the bacterial counts increased during the7-day follow-up period to the level comparable to thecontrol group.
Because CHX lacks the tissue dissolving activity ofNaOCl, there have been efforts to simplify the clinicalwork by combining the two solutions to obtain com-bined benefits from both. However, CHX and NaOClare not soluble in each other and a brownish-orangeprecipitate is formed (Figure 11). Although the anti-microbial and other characteristics of the precipitateand the liquid phase have not been thoroughly exam-ined, the precipitate prevents clinical use of the mix-ture. Marchesan et al.103 showed that the precipitatewas soluble to 0.1 mol/L acetic acid, but the brown/orange color of the solution remained. Atomic absorp-tion spectrophotometry indicated that the precipitatecontained iron which may be the reason for the color.
Despite of some shortcomings, there is increasingevidence that CHX gluconate, as a 2% solution (liquidor gel), may offer a good alternative for root canal
Figure 11 Mixing sodium hypochlorite with chlorhexidine causes abrown/orange precipitate. The color may be due to iron impurities inhypochlorite. The mixture should not be used for irrigation of the rootcanals.
Chapter 28 / Irrigants and Intracanal Medicaments / 1005

irrigation. However, one should bear in mind that themajority of the research on the use of CHX in endo-dontics is done using in vitro and ex vivo models andGram-positive test organisms, mostly E. faecalis. Thepossibility cannot be excluded that the experimentaldesigns give a biased (too positive) picture of theusefulness of CHX as an antimicrobial agent in endo-dontics. More research is needed to identify the opti-mal irrigation regimen for various types of endodontictreatments. CHX is presently marketed as a water-based solution, as a gel (with Natrosol), and as a liquidmixture with surface active agents. Future studies ofthe various CHX preparations will establish the com-parative effectiveness of the various CHX combina-tions in vivo.
Iodine Potassium Iodide (IPI)Iodine compounds are among the oldest disinfectantsstill actively used. They are best known for their use onsurfaces, skin, and operation fields. Iodine is less reactivethan the chlorine in hypochlorite. However, it killsrapidly and has bactericidal, fungicidal, tuberculocidal,virucidal, and even sporicidal activity.101 Molecularform, I2, is the active antimicrobial component.104
Poor stability of iodine in aqueous solutions motivatedthe development of iodophors (‘‘iodine carriers’’):povidone–iodine and poloxamer–iodine. Iodophorsare complexes of iodine and a solubilizing agent thatgradually releases the iodine.104 Iodophors are less activeagainst some yeasts and bacterial spores than are thealcoholic iodine solutions (tinctures). Iodine penetratesrapidly into the microorganisms and causes cell deathby attacking the proteins, nucleotides, and other keymolecules of the cell.104,105
Iodine potassium iodide (IPI) has been successfullyused in tooth surface disinfection.75 Potassium iodideis used to dissolve iodine in water, but the antimicro-bial activity is carried by the iodine, while potassiumiodide has no activity against the microbes.
The effectiveness of 2.5% NaOCl and 10% iodinefor disinfection of the operation field (tooth, rubberdam, and the clamp) has been compared by bacterialculturing and polymerase chain reaction.106 Theoperation field was treated with 30% H2O2 andeither by 10% iodine or 2.5% NaOCl. No significantdifference in the recovery of cultivable bacteria fromvarious sites in either group was detected. However,bacterial DNA was detected significantly morefrequently from the tooth surfaces after iodine treat-ment (45%) than after NaOCl (13%) treatment.106
Molander et al.107 suggested that irrigation with 5%IPI before Ca(OH)2 medication did not have an effecton the overall antimicrobial power. However, it is
possible that IPI reduces the frequency of persistingstrains of E. faecalis. Peciuliene et al.57 studied theeffect of iodine irrigation in 20 teeth with previouslyroot-filled canals and apical periodontitis. The resultsshowed that when used after normal chemomechani-cal preparation, IPI increased the number of culturenegative canals.
In the root canal, iodine compounds come in con-tact with a variety of substances such as dentin andvarious proteins. Studies of the interaction of IPI withthe chemical environment of the necrotic root canalhave shown that dentin can reduce or even abolish theeffect of 0.2/0.4% IPI against E. faecalis.37,38 However,pure hydroxyl apatite or bovine serum albumin hadlittle or no effect on the antibacterial activity of IPI.Portenier et al.39 have shown that dentin matrix(mostly dentin collagen) and heat-killed cells of E.faecalis and C. albicans inhibit the antibacterial activ-ity of IPI. These studies indicate that inactivation ofiodine compounds is one factor explaining the diffi-culty in obtaining sterile root canals.
ANTIBIOTIC-CONTAINING IRRIGATIONSOLUTIONS
MTAD and TetracleanMTAD [a mixture of tetracycline isomer, acid, anddetergent (Biopure, Dentsply, Tulsa, OK)] is a newgeneration combination product for root canal irri-gation.105,106 Tetraclean (Ogna Laboratori Farmaceu-tici, Muggio, Italy) is another combination productsimilar or close to MTAD.108 MTAD has a low pH(2.15) because it contains citric acid, it removessmear layer after NaOCl irrigation, and it has anti-bacterial activity against endodontic microbes. Themain potential benefits of MTAD are that it makesirrigation simpler by combining smear layer removalactivity with antimicrobial effect and that it may be‘‘gentler’’ with dentin than EDTA.109 The authorswho introduced MTAD have recommended the useof 1.3% NaOCl during instrumentation, followed byMTAD to remove the smear layer.110 However, 1.3%NaOCl may not be strong enough to completelyclean the uninstrumented parts of the root canal(Figure 12). Beltz et al.111 found that MTAD solu-bilizes dentin, whereas organic pulp tissue is unaf-fected by it. Zhang et al.112 showed that MTAD isless cytotoxic than eugenol, 3% H2O2, Ca(OH)2
paste, 5.25% NaOCl and EDTA, but more cytotoxicthan 2.63% NaOCl.
The antibacterial activity of MTAD is of particularinterest as it contains doxycycline (tetracycline) in
1006 / Endodontics

high concentration. Shabahang et al.113 and Shabahangand Torabinejad114 investigated the effect of MTAD onroot canals contaminated with either whole saliva or E.faecalis of extracted human teeth and reported goodantibacterial activity. Portenier et al.32 showed thatMTAD killed E. faecalis in vitro in less than 5 minutes.In an ex vivo study, Kho and Baumgartner115 com-pared the antimicrobial effectiveness of NaOCl/EDTAand NaOCl/MTAD in extracted roots infected for 4weeks with E. faecalis. After chemomechanical prepara-tion and irrigation, the roots were pulverized in liquidnitrogen and viable bacteria were counted. No differ-ence was measured between the two irrigation regi-mens. Another ex vivo study using roots of 26 matchedpairs of teeth compared the same irrigation regimenswith a different type of sampling procedure.116 In thisstudy, NaOCl/EDTA (5.25%/15%) irrigation resultedin 0/20 culture positive samples in both sample 1(directly after irrigation) and sample 2 (after instru-menting the canals 2 instrument sizes wider) using asensitive sampling protocol. However, in the otherexperimental group of 1.3% NaOCl/MTAD, the corre-sponding number of culture positive samples was 8 and10 out of the total of 20 samples in each group. Itshould be noted that in the absence of negative control(e.g. water irrigation), it is not possible to know whatmay have been the reduction of bacterial CFU in the
NaOCl/MTAD group. Nevertheless, the result indicatesbetter performance by NaOCl/EDTA than by NaOCl/MTAD irrigation. The result is interesting becauseEDTA alone lacks antimicrobial activity against E. fae-calis. The mechanisms of action of sequential use ofNaOCl and EDTA on bacterial viability have not beenthoroughly studied. There are no reports so far on theantibacterial effectiveness of Tetraclean.
The antibacterial effect of MTAD may be based notonly on the antibiotic component (doxycycline) butalso on the combined effect of doxycycline and theother ingredients (Tween 80, citric acid) on the integ-rity and stability of the microbial cell wall. However,there is no specific information available on sucheffects regarding MTAD.
Physical Means of Canal Cleaning
and Disinfection
ULTRASONIC CLEANINGEndodontic ultrasound has become an importanttool in modern endodontic work. Ultrasound is usedin a variety of tasks including finishing access cavitypreparation, removing pulp stones, locating canalorifices, opening calcified canals, fractured instru-ment removal, placing cements and root filling mate-rials, and retro canal preparation during surgicalprocedures.117 The use of ultrasonic energy for clean-ing of the root canal and to facilitate disinfection hasa long history in endodontics. The comparative effec-tiveness of ultrasonics and hand instrumentationtechniques has been evaluated in a number of earlierstudies.117–121 The majority of these studies con-cluded that the ultrasonics, together with an irrigant,contributed to a better cleaning of the root canalsystem than irrigation and hand instrumentationalone. Cavitation and acoustic streaming of the irri-gant contribute to the biological chemical activity formaximum effectiveness.122 Analysis of the physicalmechanisms of the hydrodynamic response of anoscillating ultrasonic file suggested that stable andtransient cavitation of a file, steady streaming, andcavitation microstreaming all contribute to the clean-ing of the root canal.123
Several different methods have been used to studythe effect of ultrasound on the cleanliness of the canal.These include bacteriological, histological, and micro-scopic techniques.124–128 Studies focusing on the abil-ity of ultrasound to remove smear layer have showncontradictory results. This is not, in fact, surprising
Figure 12 Uninstrumented root canal wall irrigated for 5 minutes with1.3% sodium hypochlorite (NaOCl) followed by 5-minute irrigation withMTAD (a mixture of tetracycline isomer, acid, and detergent). Althoughthis combination produces excellently clean canal walls in the instru-mented areas (smear layer), the low concentration NaOCl may be toomild to thoroughly clean the uninstrumented areas if the irrigation timeis not long enough. In this figure, some of the predentin is still left tocover the mineralized dentin and the calcospherites.
Chapter 28 / Irrigants and Intracanal Medicaments / 1007

because it is generally known that smear layer can beremoved primarily by chemical means only, or byappropriate laser treatment.129,130 It has also beenshown that to work effectively, ultrasonic files mustbe free in the canal without contact with the canalwalls.131
Among the areas that are particularly difficult toclean are anastomoses between double canals, isth-muses and fins. Several studies have indicated theimportance of ultrasonic preparation for optimal deb-ridement of the root canals and isthmuses.130,132–134
Ultrasonics also eliminated bacteria from canals moreeffectively than hand instrumentation.134–136 How-ever, not all studies have supported this finding.137 Ithas been proposed that canal anatomy is more impor-tant than ultrasound for effectiveness of the cleaningprocedures.138
The direct bactericidal effect by ultrasonic energyseems to be very limited at best.139,140 Ultrasonicsseems to exert its antimicrobial effect when usedtogether with irrigants, perhaps via the physicalmechanisms of cavitation and acoustic streaming. It isalso possible that ultrasonics helps irrigants penetrateinto areas, in complex canal systems, not easily reachedby normal irrigation.
In a series of studies on the effect of canal shape(taper) and instrument design, Lee et al.141 demon-strated in simulated plastic root canals that thediameter and taper of root canal influenced the effec-tiveness of ultrasonic irrigation to remove artificiallyplaced dentin debris. After ultrasonic irrigation, theamount of debris in the #20/04 taper group was sig-nificantly higher than that for the size #20/06 groupand the size #20/08 group. Van der Sluis et al.142 usingroots from human teeth ex vivo reported that therewas a tendency for ultrasonic irrigation to be moreeffective in removing artificially placed dentin debrisfrom simulated canal extensions from canals withgreater tapers.
A study using a split tooth technique found thatultrasonic irrigation ex vivo was more effective thansyringe irrigation in removing artificially created den-tin debris placed in simulated uninstrumented exten-sions and irregularities in straight, wide root canals.141
In another study, passive ultrasonic irrigation with2% NaOCl was more effective in removing Ca(OH)2
paste from artificial root canal grooves than syringedelivery of 2% NaOCl or water as an irrigant.143
Ultrasonic instrumentation can also have an impacton canal dimensions and in some cases can causeunwanted complications such as straightening of thecanal (transportation), perforations, and extrusion ofinfectious material beyond the apex.131,144–147 A his-
tobacteriological study of teeth with non-vital pulpsshowed compacted debris and bacteria in the apicalregion and in the dentinal tubules after ultrasonicinstrumentation.148 In one study, the step preparationtechnique was shown to cause more extrusion thanthe standard technique, whereas the least extrusionwas detected with the crown down and ultrasoundtechniques.149 Interestingly, Van der Sluis et al.142
suggested that a smooth wire during ultrasonic irriga-tion is as effective as a size 15 K-file in removal ofartificially placed dentin debris in grooves in simu-lated root canals in resin blocks. It is possible thatusing an ultrasonic tip with a smooth, inactive sur-face, preparation complications are less likely tooccur.
Recently, serious damage to paradental tissues wasreported in a case where dental cement, used forcementing a post, was removed by ultrasound from amaxillary incisor.150 After ‘‘several minutes’’ of ultra-sound treatment, the patient complained of discom-fort. During the following days and weeks, a largenecrotic zone developed, affecting the bone and softtissue around the tooth, resulting in the loss of thetooth. In controlled use, ultrasound together with irri-gation, however, is not likely to cause harmful tem-perature rise.151
LASERSLasers in endodontics are dealt with in Chapter 26E,‘‘Laser in Endodontics’’. However, their role in endo-dontic disinfection will be summarized briefly in thefollowing sections. The potential of different endodon-tic lasers in eradicating root canal microbes has been afocus of interest for many years. Early comparativestudies indicated, however, that the antibacterial effec-tiveness of lasers in the root canal was inferior toNaOCl irrigation.152–154 Excellent antibacterial effi-ciency against E. faecalis was reported by Gutknechtet al.;155 using a holmium:yttrium–aluminum–garnet(Ho:YAG) laser on root canals infected with this spe-cies in vitro, 99.98% of the bacteria were eliminated.However, Le Goff et al.156 obtained only an 85%decrease in the bacterial counts by a CO2 laser, clearlyless than by irrigation with 3% NaOCl. Contrary tothe main stream of results with laser treatment, Kesleret al.157 indicated that complete sterility of the rootcanal can be obtained with a CO2 laser microprobecoupled onto a special hand piece attached to thedelivery fiber. Schoop et al.158 in subsequent studiesindicated that the effect of laser is dependent on theapplied output power and specific for different bac-teria. Complete sterility still seems to remain a
1008 / Endodontics

challenge with laser treatment.159,160 Another impor-tant aspect of laser radiation in endodontics is theeffect of lasers on the smear layer, which may alsofacilitate effective disinfection of the canal.
New Developments in Root Canal
Disinfection
Several new technologies have been introduced duringthe last few years to improve the effectiveness of rootcanal disinfection. Increasing attention has been focusedon the use of ozone, photoactivated disinfection withlow-energy laser, electrochemically activated water, andelectric current.161–165 In a comparative study, 3%NaOCl was more effective than electrochemically acti-vated water in eradicating E. faecalis in an ex vivomodel.162 Nagayoshi et al.164 reported relatively equaleffectiveness in killing E. faecalis with ozonated waterand 2.5% NaOCl, when the specimen was irrigated withsonication. However, NaOCl was superior to ozonatedwater in killing E. faecalis in broth culture and in bio-films.166 Estrela et al.167 studied root blocks infected for60 days with a strain of E. faecalis and were unable toeradicate all bacteria with any of the methods used,including ozonated water, gaseous ozone, 2.5% NaOCl,and 2% CHX. Many of the new methods offer a biolo-gical approach to canal disinfection. However, availableevidence so far has failed to show that these methodswould be superior or sometimes even equal to existingones with regard to their antimicrobial effectiveness inthe infected root canal.
One of the latest new developments for canal disin-fection are bioactive materials such as bio(active)glass.168 In vitro studies have shown that bioglass hasantimicrobial activity against a range of microbes andthat this activity is, surprisingly, potentiated by den-tin.169,170 However, studies demonstrating better anti-microbial effect when compared to Ca(OH)2 in vivo sofar are lacking. Recent experiments with nanometricbioactive glass indicated excellent antimicrobial effectin a human dentin model.171 More research will beneeded to evaluate the value of bioglass in root canaldisinfection.
Intracanal Interappointment
Medicaments
In the treatment of teeth with a vital pulp, there is noneed for intracanal medication. However, if time doesnot allow completion of the treatment in one
appointment, it is generally recommended that theroot canal should be filled between appointments withan antibacterial dressing, for example, Ca(OH)2, toprovide sterility in the canal space until a permanentroot filling is placed. However, there are no studiescomparing the bacteriological status of the root canalsfollowing pulpectomy, when the canals have been leftempty or filled with an antibacterial dressing.
The question of the role of intracanal medicamentsbecomes more relevant, and complex, in the treatmentof pulpal necrosis and apical periodontitis. There isoverwhelming evidence in the literature that many ifnot most root canals contain viable microorganismsafter the completion of the chemomechanical prepara-tion at the end of the first appointment.8–10,54,55,57,172–
175 Therefore, a variety of intracanal medicaments havebeen used between appointments to complete disinfec-tion of the root canal. In addition to killing bacteria,intracanal medicaments may have other beneficialfunctions. Ca(OH)2 neutralizes the biological activityof bacterial lipopolysaccharide176,177 and makes necro-tic tissue more susceptible to the solubilizing action ofNaOCl at the next appointment. Another aspect inusing intracanal medicaments may be that a morethorough instrumentation is achieved because of thelonger overall time used for the treatment. On theother hand, several appointments can also increasethe risk for aseptic complications, for instance, througha leaking temporary filling and poor patient compli-ance.178
Several studies have indicated a poorer prognosis ofthe treatment of apical periodontitis if viable bacteriaare residing in the root canal system at the time offilling.5–7 Other studies, however, have contradictedthese results and reported no significant differences inhealing between teeth filled after positive or negativecultures from the root canal,8 or between treatmentsperformed in one or two appointments.8,9 It has alsobeen suggested that ‘‘intracanal sampling techniquessuffer from deficiencies that limit their predictivevalue.’’179 A permanent root filling of high qualityusing endodontic cements with antibacterial activitycan effectively seal and entomb residual microorgan-isms in the canal and prevent communication withperiradicular tissues. Continued killing of the micro-organisms could take place due to the antibacterialactivity of the root-filling materials44,180 and unavail-ability of nutrients.
CA(OH)2
Ca(OH)2 has a special position in endodontics. Indi-cations for the use of Ca(OH)2 in the prevention and
Chapter 28 / Irrigants and Intracanal Medicaments / 1009

treatment of various pulpal and periapical conditionshave been numerous. In addition to endodonticinfections, use of Ca(OH)2 has been widely advo-cated in dental traumatology and in the treatmentof resorptions. The classical studies in the 1970s and1980s at the university of Umea, Sweden, were astrong stimulus for the wide spread use of Ca(OH)2
as a local disinfecting medicament in the root canalfor the treatment of apical periodontitis. Bystromet al.6 reported that Ca(OH)2 was an effective intra-canal medicament, rendering 34 out of 35 canalsbacteria free after a 4-week period. The effectivenessof interappointment Ca(OH)2 was also reported bySjogren et al.,181 who demonstrated that a 7-daydressing with Ca(OH)2 eliminated all bacteria inthe root canal. However, these pioneer studies havebeen challenged by others who reported a residualflora in 7 to 35% of teeth after 1 or more weekswith Ca(OH)2 in the canal.21,182–184 Kvist et al.185
reported the antimicrobial efficacy of endod-ontic procedures performed in a single visit (with10-minute iodine irrigation), compared with a two-visit procedure, including an interappointment dres-sing with a Ca(OH)2 paste. Residual microorganismswere detected in 29% of the one-visit teeth and in36% of the two-visit-treated teeth, with no statisti-cally significant differences between the groups.
Zerella et al.42 compared the antibacterial activity ofCa(OH)2 mixed either with water or with 2% CHX invivo. Pure Ca(OH)2 completely disinfected 12 out of20 teeth, while the Ca(OH)2–CHX paste disinfected16 of 20 teeth. The difference, however, was notstatistically significant because of small sample size.Siqueira et al.186 examined bacterial reduction in teethwith apical periodontitis, after instrumentation andirrigation with 0.12% CHX solution and after 7 daysof intracanal medicament with a Ca(OH)2–CHX(0.12%) mixture. After finishing the chemomechani-cal preparation, 7 of the 13 cases still showed growth,while after the Ca(OH)2–CHX treatment only one of13 teeth was culture positive.
Vivacqua-Gomes et al.40 examined the benefit ofinterappointment Ca(OH)2 medicament in rootcanals in an ex vivo model. The premolar teeth wereinfected with E. faecalis for 60 days, and the canalswere instrumented using rotary instruments. Irriga-tion, interappointment medication, and root fillingwere performed following five different protocols,either in single visit or in multiple visits. A secondbacteriological sample was obtained 60 days after theroot filling (the root fillings were removed and sam-ples taken). Bacteria were found in 3 of 15 teeth
(20%) irrigated with 2% CHX gel and filled in singlevisit and in 4 of 15 teeth (25%) irrigated with CHXand filled with Ca(OH)2 for 14 days before thegutta-percha/sealer root filling was placed. Teeth thatwere left empty for 1 week after irrigation andbefore root filling, or irrigated with saline onlyinstead of CHX, or filled without sealer showedbacteria in 40 to 100% of the teeth 60 days afterthe root filling was placed. Because of the small sizeof the experimental groups, far-reaching conclusionscannot be made. However, the result supports thefinding of other studies indicating that interappoint-ment Ca(OH)2 may not add to the antibacterialeffectiveness of the treatment. Moreover, the resultsemphasize the importance of not leaving the rootcanal empty (no medicament, no root filling) as wellthe role of sealer in the joined effort to combatinfection.
CHLORHEXIDINE DIGLUCONATECHX is used as an irrigating solution during or at theend of instrumentation. However, CHX has also beenused as an intracanal medicament between theappointments. Recently, interest has been focused onthe effectiveness of CHX in gel form or as a mixturewith Ca(OH)2 as an intracanal interappointment dres-sing.187,188 The information available is based mostlyon in vitro and ex vivo experiments in which severalintracanal medicaments have been compared for theiractivity against induced dentin infection. Siren et al.188
using a bovine dentin block model reported thatCa(OH)2 mixed with CHX was much more effectivein disinfecting dentin infected with E. faecalis that pureCa(OH)2. Ercan et al.187 reported 2% CHX gel wassignificantly more effective than Ca(OH)2 combinedwith 2% CHX, or Ca(OH)2 alone, against root dentininfected with E. faecalis and the yeast C. albicans after 7,15, and 30 days of incubation. Similarly, it has beenreported that 2% CHX gel alone completely inhibitedthe growth of E. faecalis after 1, 2, 7, and 15 days in theroot canal whereas Ca(OH)2 allowed some microbialgrowth at all experimental times.41 Interestingly, inthis study, the combination of the CHX gel andCa(OH)2 had killed all bacteria in the 1- and 2-daysamples, but failed to secure sterility in the 7- and 15-day samples. The antibacterial efficacy of intracanalmedication with Ca(OH)2, 2% CHX gel, and a com-bination of both was assessed in a clinical study inteeth with chronic apical periodontitis.43 Bacterialsamples were taken before and 7 days after filling thecanals temporarily with the medicaments. CHX and
1010 / Endodontics

Ca(OH)2, alone as well as their mixture, all performedequally well, and no statistically significant differencescould be detected in their antibacterial effectiveness.
OTHER ALTERNATIVES FORINTERAPPOINTMENT MEDICAMENTS
Intracanal Medicaments ContainingAntibioticsThroughout the history of endodontics, there havebeen time periods with increased interest in the useof local antibiotics as temporary canal dressings forroot canal disinfection.189–196 Locally used antibioticshave not, however, become an established part of rootcanal disinfection and eradication of the infection.The reasons for the failure of antibiotics to overtakeendodontic infection control are many. Many of theantibiotics tested are bacteriostatic, which may not bea good strategy for treating endodontic infections.Generally, bacteriostatic antibiotics prevent thegrowth of the microorganisms without killing them,giving the host defense a possibility to deal with theinfection. In the necrotic root canal, however, there isno host defense because of the lack of the circulation.Therefore, the antibacterial effect of such antibioticsin the root canal may be only temporary. On the otherhand, it is possible that some bacteriostatic antibioticscan have a bactericidal effect when used in high con-centrations, usually the case with locally used antibio-tics. However, information about this is scarce andpresently there is no direct evidence of bacteriostaticantibiotics used in the root canal, although one studyindicated that mixing erythromycin with Ca(OH)2
improved the effectiveness against E. faecalis as com-pared to Ca(OH)2 alone.197
With bactericidal antibiotics, the potential problemin the root canal may be the metabolic and physiolo-gical state of the microorganisms. Many bactericidalantibiotics are most effective when the microbial cellsare in active growth phase, which may not be the casein the necrotic root canal with only limited nutrientsavailable. In general, specific information about theeffectiveness of intracanal antibiotics in infection con-trol in endodontics is limited. Recently, an interestingnew development has taken place with the use ofantibiotic cocktails in the treatment of teeth withimmature apex and apical periodontitis.198,199 It ispossible that better circulation and survival of somepulpal cells in the apical root canal are among the keyfactors for the promising results reported so far.Future research will show whether this approach can
be extended to the treatment of teeth with closed apexand apical periodontitis.
Phenol Compounds.Chemicals of the phenol group such as phenol, formo-creosol, cresatin, parachlorophenol (monoparachloro-phenol), camphorated phenol, and camphoratedparachlorophenol have a long history in endodonticsas locally used root canal disinfecting agents. They havebeen applied into the pulp chamber in a moist cottonpellet (vapor effect), or the whole canal has been filledwith liquid with various concentrations of the phenolcompound.200–208 The rationale of using phenol com-pounds for root canal disinfection has its roots in theirrole as general disinfecting agents in the past. However,emphasis of safety in addition to effectiveness hasresulted in dramatic decline in their use generally. Alsoin endodontics, concerns have been raised regarding thetoxicity and possible mutagenicity of the disinfectingagents of the phenol group.209–213 There are severaldemonstrations of their cytotoxicity,209,214,215 however,recent studies indicate that the risk of genotoxicity bythe various phenol compounds used in endodontics issmall.211–213 Comparative studies of the antimicrobialeffectiveness of the phenol compounds have not beenable to show superiority of the substances over the other.On the contrary,200,203,205,208,209 Bystrom et al.203
reported that Ca(OH)2 was superior to camphoratedparachlorophenol (CMCP) by its antibacterial potentialwhen used for 4 weeks as the local intracanal medica-ment. Several studies have indicated relatively rapid lossof activity of CMCP in the canal, although the resultsshow variation.206,216 In the balance of the benefits andthe demonstrated and potential weaknesses of phenolcompounds, it can be predicted that they will be increas-ingly replaced by other, more biological disinfectingagents.
References
1. Spangberg LZ, Haapasalo M. Rationale and efficacy of rootcanal medicaments and filling materials with emphasis ontreatment outcome. Endod Topics 2002;2:35–58.
2. Haapasalo M, Udnæs T, Endal U. Persistent, recurrent andacquired infection of the root canal system post-treatment.Endod Topics 2003;6:29–56.
3. Haapasalo M, Endal U, Zandi H, Coil J. Eradication ofendodontic infection by instrumentation and irrigationsolutions. Endod Topics 2005;10:72–102.
4. Sjogren U, Figdor D, Persson S, Sundqvist G. Influenceof infection at the time of root filling on the outcome of
Chapter 28 / Irrigants and Intracanal Medicaments / 1011

endodontic treatment of teeth with apical periodontitis. IntEndod J 1997;30:297–306.
5. Engstrom B. The significance of enterococci in root canaltreatment. Odontol Revy 1964;15:87–106.
6. Bystrom A, Claesson R, Sundqvist G. The antibacterial effectof camphorated paramonochlorophenol, camphorated phe-nol and calcium hydroxide in the treatment of infected rootcanals. Endod Dent Traumatol 1985;1:170–5.
7. Katebzadeh N, Sigurdsson A, Trope M. Radiographic eva-luation of periapical healing after obturation of infected rootcanals: an in vivo study. Int Endod J 2000;33:60–6.
8. Peters LB, Wesselink PR. Periapical healing of endodonti-cally treated teeth in one and two visits obturated in thepresence or absence of detectable microorganisms. IntEndod J 2002;35:660–7.
9. Weiger R, Rosendahl R, Lost C. Influence of calcium hydro-xide intracanal dressings on the prognosis of teeth withendodontically induced periapical lesions. Int Endod J2000;33:219–26.
10. Sathorn C, Parashos P, Messer H. Antibacterial efficacy ofcalcium hydroxide intracanal dressing: a systematic reviewand meta-analysis. Int Endod J 2007;40:2–10.
11. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgicalexposures of dental pulps in germfree and conventionallaboratory rats. J Southern Calif Dent Assoc 1966: 34: 449–51.
12. Bergenholtz G. Micro-organisms from necrotic pulp of trau-matized teeth. Odontol Revy 1974;25:347–58.
13. Sundqvist G. Bacteriological studies of necrotic dental pulps.[Umea University Odontological Dissertation No. 7]. Umea,Sweden: University of Umea; 1976.
14. Nair PN. On the causes of persistent apical periodontitis: areview. Int Endod J 2006;39:249–81.
15. Nair PN. Pathogenesis of apical periodontitis and the causesof endodontic failures. Crit Rev Oral Biol Med 2004 Nov1;15:348–81.
16. Friedman S. Treatment outcome and prognosis of endodon-tic therapy. In: Ørstavik D, Pitt Ford TR, editors. Essentialendodontics. Osney Mead, Oxford: Blackwell Science Ltd;1998, pp. 367–91.
17. Shetty K, Garcia J, Leigh J. Success of root canal therapy inHIV-positive patients. Gen Dent 2006;54:397–402.
18. Taschieri S, Del Fabbro M, Testori T, et al. Endodonticsurgery with ultrasonic retrotips: one-year follow-up. OralSurg Oral Med Oral Pathol Oral Radiol Endod2005;100:380–7.
19. Ørstavik D, Pitt Ford TR. Essential endodontology: preven-tion and treatment of apical periodontitis. Oxford: BlackwellScience; 1998.
20. Bystrom A, Sundqvist G. Bacteriologic evaluation of theefficacy of mechanical root canal instrumentation in endo-dontic therapy. Scand J Dent Res 1981;89:321–8.
21. Ørstavik D, Kerekes K, Molven O. Effects of extensive apicalreaming and calcium hydroxide dressing on bacterial infec-tion during treatment of apical periodontitis: a pilot study.Int Endod J 1991;24:1–7.
22. Cvek M, Nord CE, Hollender L. Antimicrobial effect of rootcanal debridement in teeth with immature root. A clinical andmicrobiologic study. Odontol Revy 1976;27:1–10.
23. Dalton BC, Ørstavik D, Phillips C, et al. Bacterial reductionwith nickel-titanium rotary instrumentation. J Endod1998;24:763–7.
24. Siqueira JF Jr, Lima KC, Magalhaes FA, et al. Mechanicalreduction of the bacterial population in the root canal bythree instrumentation techniques. J Endod 1999;25:332–5.
25. Pataky L, Ivanyi I, Grigar A, Fazekas A. Antimicrobial effi-cacy of various root canal preparation techniques: an in vitrocomparative study. J Endod 2002;28:603–5.
26. Baquero F. European standards for antibiotic susceptibilitytesting: towards a theoretical consensus. Eur J Clin Micro-biol Infect Dis 1990;9:492–5.
27. Kronvall G, Ringertz S. Antibiotic disk diffusion testingrevisited. Single strain regression analysis. Review article.APMIS 1991;99:295–306.
28. Oakes AR, Badger R, Grove DI. Comparison of direct andstandardized testing of infected urine for antimicrobialsusceptibilities by disk diffusion. J Clin Microbiol1994;32:40–5.
29. Dowzicky MJ, Nadler HL, Sheikh W. Comparison of sensi-titre broth microdilution and agar dilution susceptibilitytesting techniques for meropenem to determine accuracy,reproducibility, and predictive values. J Clin Microbiol1994;32:2204–7.
30. Espinel-Ingroff A, Chaturvedi V, Fothergill A, Rinaldi MG.Optimal testing conditions for determining MICs and mini-mum fungicidal concentrations of new and established anti-fungal agents for uncommon molds: NCCLS collaborativestudy. J Clin Microbiol 2002;40(10):3776–81.
31. Dubreuil L, Houcke I, Singer E. Susceptibility testing ofanaerobic bacteria: evaluation of the redesigned (Version96) bioMerieux ATB ANA device. J Clin Microbiol1999;37:1824–8.
32. Portenier I, Waltimo T, Ørstavik D, Haapasalo M. Killing ofEnterococcus faecalis by MTAD and chlorhexidine digluconatewith or without cetrimide in the presence or absence of dentinepowder or BSA. J Endod 2006;32:138–41.
33. Radcliffe CE, Potouridou L, Qureshi R, et al. Antimicrobialactivity of varying concentrations of sodium hypochlorite onthe endodontic microorganisms Actinomyces israelii,A. naeslundii, Candida albicans and Enterococcus faecalis.Int Endod J 2004;37:438–46.
34. Zamany A, Spangberg LS. An effective method of inactivat-ing chlorhexidine. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2002;93:617–20.
1012 / Endodontics

35. Haapasalo M, Ørstavik D. In vitro infection and disinfectionof dentinal tubules. J Dent Res 1987;66:1375–9.
36. Ørstavik D, Haapasalo M. Disinfection by endodontic irri-gants and dressings of experimentally infected dentinaltubules. Endod Dent Traumatol 1990;6:142–9.
37. Haapasalo HK, Siren EK, Waltimo TM, et al. Inactivation oflocal root canal medicaments by dentine: an in vitro study.Int Endod J 2000;33:126–31.
38. Portenier I, Haapasalo H, Rye A, et al. Inactivation of rootcanal medicaments by dentine, hydroxylapatite and bovineserum albumin. Int Endod J 2001;34:184–8.
39. Portenier I, Haapasalo H, Ørstavik D, et al. Inactivation ofthe antibacterial activity of iodine potassium iodide andchlorhexidine digluconate against Enterococcus faecalis bydentin, dentin matrix, type-I collagen, and heat-killedmicrobial whole cells. J Endod 2002;28:634–7.
40. Vivacqua-Gomes N, Gurgel-Filho ED, Gomes BP, et al.Recovery of Enterococcus faecalis after single- or multiple-visit root canal treatments carried out in infected teeth exvivo. Int Endod J 2005;38:697–704.
41. Gomes BP, Souza SF, Ferraz CC, et al. Effectiveness of 2%chlorhexidine gel and calcium hydroxide against Enterococ-cus faecalis in bovine root dentine in vitro. Int Endod J2003;36:267–75.
42. Zerella JA, Fouad AF, Spangberg LS. Effectiveness of a cal-cium hydroxide and chlorhexidine digluconate mixture asdisinfectant during retreatment of failed endodontic cases.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2005;100:756–61.
43. Manzur A, Gonzalez AM, Pozos A, et al. Bacterial quantifica-tion in teeth with apical periodontitis related to instrumen-tation and different intracanal medications: a randomizedclinical trial. J Endod 2007;33:114–18.
44. Saleh IM, Ruyter IE, Haapasalo M, Ørstavik D. Survival ofEnterococcus faecalis in infected dentinal tubules after rootcanal filling with different root canal sealers in vitro. IntEndod J 2004;37:193–8.
45. Hulsmann M, Hahn W. Complications during root canalirrigation: literature review and case reports. Int Endod J2000;33:186–93.
46. Mcdonnell G, Russell D. Antiseptics and disinfectants: activity,action, and resistance. Clin Microbiol Rev 1999;12:147–79.
47. Barrette WC Jr, Hannum DM, Wheeler WD, Hurst JK. Generalmechanism for the bacterial toxicity of hypochlorous acid:abolition of ATP production. Biochemistry 1989;28:9172–8.
48. McKenna SM, Davies KJA. The inhibition of bacterialgrowth by hypochlorous acid. Biochem J 1988;254:685–92.
49. Zehnder M, Kosicki D, Luder H, et al. Tissue-dissolvingcapacity and antibacterial effect of buffered and unbufferedhypochlorite solutions. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2002;94:756–62.
50. Waltimo TM, Ørstavik D, Siren EK, Haapasalo MP. In vitrosusceptibility of Candida albicans to four disinfectants andtheir combinations. Int Endod J 1999;32:421–9.
51. Vianna ME, Gomes BP, Berber VB, et al. In vitro evaluationof the antimicrobial activity of chlorhexidine and sodiumhypochlorite. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2004;97:79–84.
52. Gomes BP, Ferraz CC, Vianna ME, et al. In vitro antimicrobialactivity of several concentrations of sodium hypochlorite andchlorhexidine gluconate in the elimination of Enterococcusfaecalis. Int Endod J 2001;34:424–8.
53. Portenier I, Waltimo T, Ørstavik D, Haapasalo M. Thesusceptibility of starved, stationary phase, and growing cellsof Enterococcus faecalis to endodontic medicaments. J Endod2005;31:380–6.
54. Bystrom A, Sundqvist G. Bacteriologic evaluation of theeffect of 0.5 percent sodium hypochlorite in endodontictherapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1983;55:307–12.
55. Bystrom A, Sundqvist G. The antibacterial action of sodiumhypochlorite and EDTA in 60 cases of endodontic therapy.Int Endod J 1985;18: 35–40.
56. Siqueira JF Jr, Rocas IN, Santos SR, et al. Efficacy of instru-mentation techniques and irrigation regimens in reducingthe bacterial population within root canals. J Endod2002;28:181–4.
57. Peciuliene V, Reynaud A, Balciuniene I, Haapasalo M. Iso-lation of yeasts and enteric bacteria in root-filled teeth withchronic apical periodontitis. Int Endod J 2001;34:429–34.
58. Spangberg L, Engstrom B, Langeland K. Biologic effects ofdental materials. 3. Toxicity and antimicrobial effect ofendodontic antiseptics in vitro. Oral Surg Oral Med OralPathol Oral Radiol Endod 1973;36:856–71.
59. McComb D, Smith DC, Beagrie GS. The results of in vivoendodontic chemomechanical instrumentation: a scanningelectron microscopic study. J Br Endod Soc 1976;9:11–18.
60. Pashley EL, Birdsong NL, Bowman K, Pashley DH. Cytotoxiceffects of NaOCl on vital tissue. J Endod 1985;11:525–8.
61. Chang YC, Huang FM, Tai KW, Chou MY. The effect ofsodium hypochlorite and chlorhexidine on cultured humanperiodontal ligament cells. Oral Surg Oral Med Oral PatholOral Radiol Endod 2001;92:446–50.
62. Czonstkowsky M, Wilson EG, Holstein FA. The smear layer inendodontics. Dent Clin North Am 1990;34:13–25.
63. Baumgartner JC, Mader CL. A scanning electron micro-scopic evaluation of four root canal irrigation regimens.J Endod 1987;13:147–57.
64. Niu W, Yoshioka T, Kobayashi C, Suda H. A scanningelectron microscopic study of dentinal erosion by final irri-gation with EDTA and NaOCl solutions. Int Endod J2002;35:934–9.
Chapter 28 / Irrigants and Intracanal Medicaments / 1013

65. Loel DA. Use of acid cleanser in endodontic therapy. J AmDent Assoc 1975;90:148–51.
66. Baumgartner JC, Brown CM, Mader CL, et al. A scanningelectron microscopic evaluation of root canal debridementusing saline, sodium hypochlorite, and citric acid. J Endod1984;10:525–31.
67. Gutmann JL, Saunders WP, Nguyen L, et al. Ultrasonic root-end preparation. Part 1. SEM analysis. Int Endod J1994;27:318–24.
68. Yamaguchi M, Yoshida K, Suzuki R, Nakamura H. Rootcanal irrigation with citric acid solution. J Endod1996;22:27–9.
69. Liolios E, Economides N, Parissis-Messimeris S, BoutsioukisA. The effectiveness of three irrigating solutions on rootcanal cleaning after hand and mechanical preparation. IntEndod J 1997;30:51–7.
70. Di Lenarda R, Cadenaro M, Sbaizero O. Effectiveness of1 mol L-1 citric acid and 15% EDTA irrigation on smearlayer removal. Int Endod J 2000;33:46–52.
71. Scelza MF, Teixeira AM, Scelza P. Decalcifying effect ofEDTA-T, 10% citric acid, and 17% EDTA on root canaldentin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;95:234–6.
72. Machado-Silveiro LF, Gonzalez-Lopez S, Gonzalez-Rodri-guez MP. Decalcification of root canal dentine by citric acid,EDTA and sodium citrate. Int Endod J 2004;37:365–9.
73. Takeda FH, Harashima T, Kimura Y, Matsumoto K. Acomparative study of the removal of smear layer by threeendodontic irrigants and two types of laser. Int Endod J1999;32:32–9.
74. Block SS. Peroxygen compounds. In: Block SS, editor. Dis-infection, sterilization, and preservation. 4th ed.Philadelphia, PA: Lea & Febiger; 1991, pp. 167–81.
75. Moller AJ. Microbiological examination of root canals andperiapical tissues of human teeth Methodological studies (the-sis). Odontol Tidskr 1966;74:1–380.
76. Siqueira JF Jr, Machado AG, Silveira RM, et al. Evaluation ofthe effectiveness of sodium hypochlorite used with threeirrigation methods in the elimination of Enterococcus faecalisfrom the root canal, in vitro. Int Endod J 1997;30:279–82.
77. Heling I, Chandler NP. Antimicrobial effect of irrigant com-binations within dentinal tubules. Int Endod J 1998;31:8–14.
78. Steinberg D, Heling I, Daniel I, Ginsburg I. Antibacterialsynergistic effect of chlorhexidine and hydrogen peroxideagainst Streptococcus sobrinus, Streptococcus faecalis and Sta-phylococcus aureus. J Oral Rehabil 1999;26:151–6.
79. Moller AJ, Fabricius L, Dahlen G, et al. Apical periodontitisdevelopment and bacterial response to endodontic treat-ment. Experimental root canal infections in monkeys withselected bacterial strains. Eur J Oral Sci 2004;112:207–15.
80. Russell AD. Activity of biocides against mycobacteria. J ApplBacteriol Symp 1996;81(Suppl):87S–101S.
81. Shaker LA, Dancer BN, Russell AD, Furr JR. Emergenceand development of chlorhexidine resistance during spor-ulation of Bacillus subtilis 168. FEMS Microbiol Lett1988;51:73–6.
82. Russell AD, Day MJ. Antibacterial activity of chlorhexidine.J Hosp Infect 1993;25:229–38.
83. Davies GE, Francis J, Martin AR, et al. 1:6-Di-4’-chlorophenyl-diguanidohexane (hibitane); laboratory investigation of a newantibacterial agent of high potency. Br J Pharmacol Chemother1954;9:192–6.
84. Hennessey TS. Some antibacterial properties of chlorhexi-dine. J Periodontal Res Suppl 1973;12:61–7.
85. Emilson CG. Susceptibility of various microorganisms tochlorhexidine. Scand J Dent Res 1977;85:255–65.
86. Siqueira JF Jr, da Silva CH, Cerqueira M das D, et al.Effectiveness of four chemical solutions in eliminating Bacil-lus subtilis spores on gutta-percha cones. Endod Dent Trau-matol 1998;14:124–6.
87. Gomes BP, Vianna ME, Matsumoto CU, et al. Disinfectionof gutta-percha cones with chlorhexidine and sodium hypo-chlorite. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2005;100:512–17.
88. Royal MJ, Williamson AE, Drake DR. Comparison of 5.25%sodium hypochlorite, MTAD, and 2% chlorhexidine in therapid disinfection of polycaprolactone-based root canal fill-ing material. J Endod. 2007;33:42–4.
89. Park JB, Park NH. Effect of chlorhexidine on the in vitro andin vivo herpes simplex virus infection. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1989;67:149–53.
90. Vahdaty A, Pitt Ford TR, Wilson RF. Efficacy of chlorhex-idine in disinfecting dentinal tubules in vitro. Endod DentTraumatol 1993;9:243–8.
91. Buck RA, Eleazer PD, Staat RH, Scheetz JP. Effectiveness ofthree endodontic irrigants at various tubular depths inhuman dentin. J Endod 2001;27:206–8.
92. Jeansonne MJ, White RR. A comparison of 2.0% chlorhexidinegluconate and 5.25% sodium hypochlorite as antimicrobialendodontic irrigants. J Endod 1994;20:276–8.
93. Clegg MS, Vertucci FJ, Walker C, et al. The effect of expo-sure to irrigant solutions on apical dentin biofilms in vitro.J Endod 2006;32:434–7.
94. Oncag O, Hosgor M, Hilmioglu S, et al. Comparison ofantibacterial and toxic effects of various root canal irrigants.Int Endod J 2003;36:423–32.
95. Barkvoll P, Attramadal A. Effect of nystatin and chlorhex-idine digluconate on Candida albicans. Oral Surg Oral MedOral Pathol 1989;67:279–81.
96. Hamers AD, Shay K, Hahn BL, Sohnle PG. Use of a micro-titer plate assay to detect the rate of killing of adherentCandida albicans by antifungal agents. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1996;81:44–9.
1014 / Endodontics

97. Hiom SJ, Furr JR, Russell AD, Dickinson JR. Effects of chlor-hexidine diacetate on Candida albicans, C. glabrata and Sac-charomyces cerevisiae. J Appl Bacteriol 1992; 72:335–40.
98. Dona BL, Grundemann LJ, Steinfort J, et al. The inhibitoryeffect of combining chlorhexidine and hydrogen peroxide on3-day plaque accumulation. J Clin Periodontol 1998;25:879–83.
99. Babich H, Wurzburger BJ, Rubin YL, et al. An in vitro studyon the cytotoxicity of chlorhexidine digluconate to humangingival cells. Cell Biol Toxicol 1995;11:79–88.
100. Sassone LM, Fidel R, Fidel S, et al. The influence of organicload on the antimicrobial activity of different concentrationsof NaOCl and chlorhexidine in vitro. Int Endod J2003;36(12):848–52.
101. Hoefs JC. Serum protein concentration and portal pressuredetermine the ascitic fluid protein concentration in patientswith chronic liver disease. J Lab Clin Med 1983;102:260–73.
102. Oliveira DP, Barbizam JV, Trope M, Teixeira FB. In vitroantibacterial efficacy of endodontic irrigants against Enter-ococcus faecalis. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2007;103:702–6.
103. Marchesan MA, Pasternak B Jr, Afonso MM, et al. Chemicalanalysis of the flocculate formed by the association of sodiumhypochlorite and chlorhexidine. Oral Surg Oral Med OralPathol Oral Radiol Endod 2007;103:103–5.
104. Gottardi W. Iodine and iodine compounds. In: Block SS,editor. Disinfection, sterilization, and preservation. 4th ed.Philadelphia, PA: Lea & Febiger; 1991, pp. 152–66.
105. Chang SL. Modern concept of disinfection. J Sanit Eng DivProc ASCE 1971;97:689.
106. Ng YL, Spratt D, Sriskantharajah S, Gulabivala K. Evaluationof protocols for field decontamination before bacterial sam-pling of root canals for contemporary microbiology techni-ques. J Endod 2003;29:317–20.
107. Molander A, Reit C, Dahlen G. The antimicrobial effect ofcalcium hydroxide in root canals pretreated with 5% iodinepotassium iodide. Endod Dent Traumatol 1999;15:205–9.
108. Giardino L, Ambu E, Becce C, et al. Surface tension compar-ison of four common root canal irrigants and two newirrigants containing antibiotic. J Endod 2006;32:1091–3.
109. Torabinejad M, Khademi AA, Babagoli J, et al. A new solu-tion for the removal of the smear layer. J Endod2003;29:170–5.
110. Torabinejad M, Cho Y, Khademi AA, et al. The effect ofvarious concentrations of sodium hypochlorite on the abilityof MTAD to remove the smear layer. J Endod 2003;29:233–9.
111. Beltz RE, Torabinejad M, Pouresmail M. Quantitative ana-lysis of the solubilizing action of MTAD, sodium hypochlor-ite, and EDTA on bovine pulp and dentin. J Endod2003;29:334–7.
112. Zhang W, Torabinejad M, Li Y. Evaluation of cytotoxicity ofMTAD using the MTT-tetrazolium method. J Endod2003;29:654–7.
113. Shabahang S, Pouresmail M, Torabinejad M. In vitro anti-microbial efficacy of MTAD and sodium. J Endod2003;29:450–2.
114. Shabahang S, Torabinejad M. Effect of MTAD on Enterococ-cus faecalis-contaminated root canals of extracted humanteeth. J Endod 2003;29:576–9.
115. Kho P, Baumgartner JC. A comparison of the antimicrobialefficacy of NaOCl/Biopure MTAD versus NaOCl/EDTA againstEnterococcus faecalis. J Endod 2006;32:652–5.
116. Baumgartner JC, Johal S, Marshall JG. Comparison of theantimicrobial efficacy of 1.3% NaOCl/BioPure MTAD to5.25% NaOCl/15% EDTA for root canal irrigation. J Endod2007;33:48–51.
117. Plotino G, Pameijer CH, Grande NM, Somma F. Ultrasonicsin endodontics: a review of the literature. J Endod2007;33:81–95.
118. Martin H. Ultrasonic disinfection of the root canal. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1976:42:92–9.
119. Cunningham W, Martin H, Forrest W. Evaluation of rootcanal debridement by the endosonic ultrasonic synergisticsystem. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1982;53:401–4.
120. Cunningham W, Martin H. A scanning electron microscopeevaluation of root canal debridement with the endosonicultrasonic synergistic system. Oral Surg Oral Med OralPathol Oral Radiol Endod 1982;53:527–31.
121. Cunningham W, Martin H, Pelleu G, Stoops D. A conmpar-ison of antimicrobial effectiveness of endosonic and handroot canal therapy. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1982;54:238–41.
122. Martin H, CunninghamW. Endosonics – the ultrasonicsynergistic system of endodontics. Endod Dent Traumatol1985;1:201–6.
123. Roy RA, Ahmad M, Crum LA. Physical mechanisms govern-ing the hydrodynamic response of an oscillating ultrasonicfile. Int Endod J 1994;27:197–207.
124. Reynolds MA, Madison S, Walton RE, et al. An in vitrohistological comparison of the step-back, sonic, and ultra-sonic instrumentation techniques in small, curved rootcanals. J Endod 1987;13:307–14.
125. Heard F, Walton RE. Scanning electron microscope studycomparing four root canal pereparation techniques in smallcurved canals. Int Endod J 1997;30:323–31.
126. Lumley PJ, Walmsley AD, Walton RE, Rippin JW. Cleaningof oval canals using ultrasonic or sonic instrumentation.J Endod 1993;19:453–7.
127. Cheung GS, Stock CJ. In vitro cleaning ability of root canalirrigants with and without endosonics. Int Endod J1993;26:334–43.
128. Hulsmann M, Rummelin C, Schafers F. Root canal cleanli-ness after preparation with different endodontic handpieces
Chapter 28 / Irrigants and Intracanal Medicaments / 1015

and hand instruments: a comparative SEM investigation.J Endod 1997;23:301–6.
129. Cameron JA. Factors affecting the clinical efficiency of ultra-sonic endodontics: a scanning electron microscopy study.Int Endod J 1995;28:47–53.
130. Cameron JA. The choice of irrigant during hand instrumen-tation and ultrasonic irrigation of the root canal: a scanningelectron microscope study. Aust Dent J 1995;40:85–90.
131. Lumley PJ, Walmsley AD, Walton RE, Rippin JW. Effect ofpre-curving endosonic files on the amount of debris andsmear layer remaining in curved root canals. J Endod1992;18:616–19.
132. Goodman A, Reader A, Beck M, et al. An in vitro compar-ison of the efficacy of the step-back technique versus a step-back ultrasonic technique in humanmandibularmolars.J Endod 1985;11:249–56.
133. Archer R, Reader A, Nist R, et al. An in vivo evaluation ofthe efficacy of ultrasound after stepback preparation inmandibular molars. J Endod 1992;18:549–52.
134. Sjogren U, Sundqvist G. Bacteriologic evaluation of ultra-sonic root canal instrumentation. Oral Surg Oral Med OralPathol Oral Radiol Endod 1987;63:366–70.
135. Spoleti P, Siragusa M, Spoleti MJ. Bacteriological evaluation ofpassive ultrasonic activation. J Endod 2002;29:12–14.
136. Sabins RA, Johnson JD, Hellstein JW. A comparison of thecleaning efficacy of short term sonic and ultrasonic passiveirrigation after hand instrumentation in molar root canals.J Endod 2003;29:674–8.
137. DeNunzio MS, Hicks ML, Pelleu GB Jr, et al. Bacteriologicalcomparison of ultrasonic and hand instrumentation of rootcanals in dogs. J Endod 1989;15:290–3.
138. Biffi JC, Rodrigues HH. Ultrasound in endodontics: a quan-titative and histological assessment using human teeth.Endod Dent Traumatol 1989;5:55–62.
139. Ahmad M. Effect of ultrasonic instrumentation on Bacter-iodes intermedius. Endod Dent Traumatol 1989;5:83–6.
140. Ahmad M, Pitt Ford TR, Crum LA, Wilson RF. Effectivenessof ultrasonic files in the disruption of root canal bacteria.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1990;70:328–32.
141. Lee SJ, Wu MK, Wesselink PR. The effectiveness of syringeirrigation and ultrasonics to remove debris from simulatedirregularities within prepared root canal walls. Int EndodJ 2004;37:672–8.
142. Van der Sluis LW, Wu MK, Wesselink PR. A comparisonbetween a smooth wire and a K-file in removing artificiallyplaced dentine debris from root canals in resin blocks duringultrasonic irrigation. Int Endod J. 2005;38:593–6.
143. Van der Sluis LW, Wu MK, Wesselink PR. The evaluation ofremoval of calcium hydroxide paste from an artificial stan-dardized groove in the apical root canal using differentirrigation methodologies. Int Endod J 2007;40:52–7.
144. Calhoun G, Montgomery S. The effects of four instrumenta-tion techniques on root canal shape. J Endod 1988;14:273–7.
145. Schulz-Bongert U, Weine FS, Schulz-Bongert J. Preparationof curved canals using a combined hand-filing, ultrasonictechnique. Compend Contin Educ Dent 1995;16:272–4.
146. McCann JT, Keller DL, LaBounty GL. Remaining dentin/cementum thickness after hand or ultrasonic instrumenta-tion. J Endod 1990;16:109–13.
147. McKendry DJ. Comparison of balanced forces, endosonic,and step-back filing instrumentation techniqaues: quantifi-cation of extruded apical debris. J Endod 1990;16:24–7.
148. Rodrigues HH, Biffi JC. A histobacteriological assessment ofnonvitgal teeth after ultrasonic root canal instrumentation.Endod Dent Traumatol 1989;5:182–7.
149. Vansan LP, Pecora JD, Costa WF, et al. Effects of variousirrigating solutions on the cleaning of the root canal withultrasonic instrumentation. Braz Dent J 1990;1:37–44.
150. Walters JD, Rawal SY. Severe periodontal damage by anultrasonic endodontic device: a case report. Dent Traumatol2007;23:123–7.
151. Ahmad M. Measurements of temperature generated by ultra-sonic file in vitro. Endod Dent Traumatol 1990;6:230–1.
152. Fegan SE, Steiman HR. Comparative evaluation of the anti-bacterial effects of intracanal Nd:YAG laser irradiation: an invitro study. J Endod 1995;21:415–17.
153. Moshonov J, Ørstavik D, Yamauchi S, et al. Nd:YAG laserirradiation in root canal disinfection. Endod Dent Trauma-tol 1995;11:220–4.
154. Blum JY, Michailesco P, Abadie MJ. An evaluation of thebactericidal effect of the Nd:YAP laser. J Endod 1997;23:583–5.
155. Gutknecht N, Nuebler-Moritz M, Burghardt SF, Lampert F.The efficiency of root canal disinfection using a holmium:yt-trium–aluminum–garnet laser in vitro. J Clin Laser MedSurg 1997;15:75–8.
156. Le Goff A, Dautel-Morazin A, Guigand M, et al. An evalua-tion of the CO2 laser for endodontic disinfection. J Endod1999;25:105–8.
157. Kesler G, Koren R, Kesler A, et al. Histological changesinduced by CO2 laser microprobe specially designed for rootcanal sterilization: in vivo study. J Clin Laser Med Surg1998;16:263–7.
158. Schoop U, Moritz A, Kluger W, et al. The Er:YAG laser inendodontics: results of an in vitro study. Lasers Surg Med2002;30:360–4.
159. Piccolomini R, D’Arcangelo C, D’Ercole S, et al. Bacteriolo-gic evaluation of the effect of Nd:YAG laser irradiation inexperimental infected root canals. J Endod 2002;28:276–8.
160. Mehl A, Folwaczny M, Haffner C, Hickel R. Bactericidaleffects of 2.94 microns Er:YAG-laser radiation in dental rootcanals. J Endod 1999;25:490–3.
1016 / Endodontics

161. Lee MT, Bird PS, Walsh LJ. Photo-activated disinfection ofthe root canal: a new role for lasers in endodontics. AustEndod J 2004;30:93–8.
162. Gulabivala K, Stock CJ, Lewsey JD, et al. Effectiveness ofelectrochemically activated water as an irrigant in an infectedtooth model. Int Endod J 2004;37:624–31.
163. Solovyeva AM, Dummer PM. Cleaning effectiveness of rootcanal irrigation with electrochemically activated anolyte andcatholyte solutions: a pilot study. Int Endod J 2000;33:494–504.
164. Nagayoshi M, Kitamura C, Fukuizumi T, et al. Antimicro-bial effect of ozonated water on bacteria invading dentinaltubules. J Endod 2004;30:778–81.
165. Millar BJ, Hodson N. Assessment of the safety of two ozonedelivery devices. J Dent 2007;35:195–200.
166. Hems RS, Gulabivala K, Ng YL, et al. An in vitro evaluationof the ability of ozone to kill a strain of Enterococcus faecalis.Int Endod J 2005;38:22–9.
167. Estrela C, Estrela CR, Decurcio DA, et al. Antimicrobialefficacy of ozonated water, gaseous ozone, sodium hypo-chlorite and chlorhexidine in infected human root canals.Int Endod J 2007;40:85–93.
168. Stoor P, Soderling E, Salonen JI. Antibacterial effects of abioactive glass paste on oral microorganisms. Acta OdontolScand 1998;56:161–5.
169. Zehnder M, Soderling E, Salonen J, Waltimo T. Preliminaryevaluation of bioactive glass S53P4 as an endodontic medi-cation in vitro. J Endod 2004;30:220–4.
170. Zehnder M, Waltimo T, Sener B, Soderling E. Dentinenhances the effectiveness of bioactive glass S53P4 against astrain of Enterococcus faecalis. Oral Surg Oral Med OralPathol Oral Radiol Endod 2006;101:530–5.
171. Waltimo T, Brunner T, Wendelin A, Zehnder M. Antimi-crobial effect of nanometric bioactive glass 45S5. J Dent Res,2007;86:754–7.
172. Chugal NM, Clive JM, Spangberg LS. A prognostic modelfor assessment of the outcome of endodontic treatment:effect of biologic and diagnostic variables. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2001;91:342–52.
173. Coldero LG, McHugh S, Mackenzie D, Saunders WP.Reduction in intracanal bacteria during root canal prepara-tion with and without apical enlargement. Int Endod J2002;35:437–46.
174. Rollison S, Barnett F, Stevens RH. Efficacy of bacterialremoval from instrumented root canals in vitro related toinstrumentation technique and size. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2002;94:366–71.
175. Card SJ, Sigurdsson A, Ørstavik D, Trope M. The effective-ness of increased apical enlargement in reducing intracanalbacteria. J Endod 2002;28:779–83.
176. Safavi KE, Nichols FC. Effect of calcium hydroxide on bac-terial lipopolysaccharide. J Endod 1993;19:76–8.
177. Tanomaru JM, Leonardo MR, Tanomaru Filho M, et al.Effect of different irrigation solutions and calcium hydroxideon bacterial LPS. Int Endod J 2003;36:733–9.
178. Siren EK, Haapasalo MP, Ranta K, et al. Microbiologicalfindings and clinical treatment procedures in endodonticcases selected for microbiological investigation. Int Endod J1997;30:91–5.
179. Sathorn C, Parashos P, Messer HH. How useful is root canalculturing in predicting treatment outcome? J Endod2007;33:220–5.
180. Ørstavik D. Antibacterial properties of endodontic materials.Int Endod J 1988;21:161–9.
181. Sjogren U, Figdor D, Spangberg L, Sundqvist G. The anti-microbial effect of calcium hydroxide as a short term intra-canal dressing. Int Endod J 1991;24:119–25.
182. Reit C, Molander A, Dahlen G. The diagnostic accuracy ofmicrobiologic root canal sampling and the influence of antimi-crobial dressings. Endod Dent Traumatol 1999;15:278–83.
183. Shuping GB, Ørstavik D, Sigurdsson A, Trope M. Reductionof intracanal bacteria using nickel-titanium rotary instru-mentation and various medications. J Endod 2000;26:751–5.
184. Peters LB, Van Winkelhoff AJ, Buijs JF, Wesselink PR.Effects of instrumentation, irrigation and dressing with cal-cium hydroxide on infection in pulpless teeth with periapicalbone lesions. Int Endod J 2002;35:13–21.
185. Kvist T, Molander A, Dahlen G, Reit C. Microbiologicalevaluation of one- and two-visit endodontic treatment ofteeth with apical periodontitis: a randomized, clinical trial. JEndod 2004;30:572–6.
186. Siqueira JF Jr, Paiva SS, Rocas IN. Reduction in the cultivablebacterial populations in infected root canals by a chlorhexidine-based antimicrobial protocol. J Endod 2007;33:541–7.
187. Ercan E, Dalli M, Dulgergil CT. In vitro assessment of theeffectiveness of chlorhexidine gel and calcium hydroxidepaste with chlorhexidine against Enterococcus faecalis andCandida albicans. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2006;102:27–31.
188. Siren EK, Haapasalo MP, Waltimo TM, Ørstavik D. In vitroantibacterial effect of calcium hydroxide combined withchlorhexidine or iodine potassium iodide on Enterococcusfaecalis. Eur J Oral Sci 2004;112:326–31.
189. Grossman LI. Polyantibiotic treatment of pulpless teeth. JAm Dent Assoc 1951;43:265–78.
190. Bender IB, Seltzer S. Combination of antibiotics and fungi-cides used in treatment of the infected pulpless tooth. J AmDent Assoc 1952;45:293–300.
191. Rubbo SD, Reich J, Dixson S. The use of a combination ofneomycin, bacitracin, and polymyxin in endodontia. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1958;11:878–96.
192. Baker GR, Mitchell DF. Topical antibiotic treatment ofinfected dental pulps of monkeys. J Dent Res 1969 May–June;48:351–5.
Chapter 28 / Irrigants and Intracanal Medicaments / 1017

193. Hoshino E, Iwaku M, Sato M, et al. Bactericidal efficacy ofmetronidazole against bacteria of human carious dentin invivo. Caries Res 1989;23:78–80.
194. Hoshino E, Kurihara-Ando N, Sato I, et al. In-vitro antibac-terial susceptibility of bacteria taken from infected rootdentine to a mixture of ciprofloxacin, metronidazole andminocycline. Int Endod J 1996 Mar;29:125–30.
195. Sato I, Ando-Kurihara N, Kota K, et al. Sterilization ofinfected root-canal dentine by topical application of a mix-ture of ciprofloxacin, metronidazole and minocycline in situ.Int Endod J 1996;29:118–24.
196. Molander A, Reit C, Dahlen G. Microbiological evaluation ofclindamycin as a root canal dressing in teeth with apicalperiodontitis. Int Endod J 1990;23:113–18.
197. Molander A, Dahlen G. Evaluation of the antibacterialpotential of tetracycline or erythromycin mixed with calciumhydroxide as intracanal dressing against Enterococcus faeca-lis in vivo. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;96:744–50.
198. Banchs F, Trope M. Revascularization of immature perma-nent teeth with apical periodontitis: new treatment protocol?J Endod 2004;30:196–200.
199. Windley W III, Teixeira F, Levin L, et al. Disinfection ofimmature teeth with a triple antibiotic paste. J Endod2005;31:439–43.
200. Harrison JW, Madonia JV. Antimicrobial effectiveness ofparachlorophenol. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1970;30:267–75.
201. Harrison JW, Madonia JV. The toxicity of parachlorophenol.Oral Surg Oral Med Oral Patho Oral Radiol Endod1971;32:90–9.
202. Taylor GN, Madonia JV, Wood NK, Heuer MA. In vivoautoradiographic study of relative penetrating abilities ofaqueous 2% parachlorophenol and cambhorated 35% para-chlorophenol. J Endod 1976;2:81–6.
203. Bystrom A, Claesson R, Sundqvist G. The antibacterial effect ofcamphorated paramonochlorophenol, camphorated phenoland calcium hydroxide in the treatment of infected root canals.Endod Dent Traumatol 1985;1:170–5.
204. Fager FK, Messer HH. Systemic distribution of camphoratedmonochlorophenol from cotton pellets sealed in pulp cham-bers. J Endod 1986;12:225–30.
205. Koontongkaew S, Silapichit R, Thaweboon B. Clinical andlaboratory assessments of camphorated monochlorophenolin endodontic therapy. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1988;65:757–62.
206. Alencar AH, Leonardo MR, Silva LA, et al. Determination ofthe p-monochlorophenol residue in the calcium hydroxide +P-monochlorophenol combination used as an intracanaldressing in pulpless teeth of dogs with induced chronicperiapical lesion. J Endod 1997;23:522–4.
207. Siqueira JF Jr, Rocas IN, Favieri A, et al. Incidence of post-operative pain after intracanal procedures based on an anti-microbial strategy. J Endod 2002;28:457–60.
208. Ferrari PH, Cai S, Bombana AC. Effect of endodontic proce-dures on enterococci, enteric bacteria and yeasts in primaryendodontic infections. Int Endod J 2005;38:372–80.
209. Messer HH, Feigal RJ. A comparison of the antibacterialand cytotoxic effects of parachlorophenol. J Dent Res1985;64:818–21.
210. Fager FK, Messer HH. Systemic distribution of camphoratedmonochlorophenol from cotton pellets sealed in pulp cham-bers. J Endod 1986;12:225–30.
211. Ribeiro DA, Marques ME, Salvadori DM. Antimicrobial endo-dontic compounds do not modulate alkylation-induced geno-toxicity and oxidative stress in vitro. Oral Surg Oral Med OralPathol Oral Radiol Endod 2006;102:32–6.
212. Hagiwara M, Watanabe E, Barrett JC, Tsutsui T. Assessmentof genotoxicity of 14 chemical agents used in dental practice:ability to induce chromosome aberrations in Syrian hamsterembryo cells. Mutat Res 2006;603:111–20.
213. Ribeiro DA, Scolastici C, De Lima PL, et al. Genotoxicity ofantimicrobial endodontic compounds by single cell gel (comet)assay in Chinese hamster ovary (CHO) cells. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2005;99:637–40.
214. Breault LG, Schuster GS, Billman MA, et al. The effectsof intracanal medicaments, fillers, and sealers on the attach-ment of human gingival fibroblasts to an exposed dentinsurface free of a smear layer. J Periodontol 1995;66:545–51.
215. Chang YC, Tai KW, Chou LS, Chou MY. Effects of campho-rated parachlorophenol on human periodontal ligamentcells in vitro. J Endod 1999;25:779–81.
216. Messer HH, Chen RS. The duration of effectiveness of rootcanal medicaments. J Endod 1984;10:240–5.
1018 / Endodontics

CHAPTER 29
ROOT CANAL FILLING MATERIALS
JAMES DAVID JOHNSON
Historically, many materials have been used to fill rootcanals. In the 1800s and before, materials ranging fromtin foil, lead foil, gold foil, cotton pellets with variousmedicaments, wood, spunk, plaster of Paris, oxychlor-ide of zinc, oxyphosphate of zinc, zinc oxide, paraffin,copper points, and various other concoctions wereused to fill root canals. Sometimes canals were notfilled at all, and only a mixture of Hill’s stopping wasplaced over canals.1 With Asa Hill’s development ofHill’s stopping in 1847, which consisted of bleachedgutta-percha and carbonate of lime and quartz, theadvent of gutta-percha as a root canal filling material inendodontics began.2 In 1867, G. A. Bowman of St. Louiswas credited with using gutta-percha points to obturateroot canals.1 The S. S. White Company began to marketgutta-percha points to the profession in 1887.3 Gutta-percha, as an obturating material, has survived, and todayexists in many forms, and is still the most widely usedmaterial to obturate root canals.
Requirements for an Ideal Root Canal
Filling Material
Grossman4 modified Brownlee’s5 criteria for the idealroot canal filling material and listed the followingcriteria for an ideal root canal filling material:
1. It should be easily introduced into the root canal.2. It should seal the canal laterally as well as apically.3. It should not shrink after being inserted.4. It should be impervious to moisture.5. It should be bacteriostatic or at least not encou-
rage bacterial growth.6. It should be radiopaque.7. It should not stain tooth structure.8. It should not irritate periradicular tissues.9. It should be sterile, or easily and quickly steri-
lized, immediately before insertion.10. It should be removed easily from the root canal, if
necessary.
Root canal filling materials have been classified assolid-core filling materials, semisolid-core fillingmaterials, and paste filling materials. Silver pointsare an example of solid-core filling materials. Gutta-percha is the most widely used semisolid-core mate-rial. Various paste systems have been used over theyears, such as zinc oxide-containing pastes.
Solid-Core Filling Materials
HISTORICAL ROOT CANAL FILLINGMATERIALS (SILVER POINTS)Silver points, having the same diameter and taper asfiles and reamers, were introduced by Jasper in1933.2 Silver points were widely used in the 1930sto the 1960s, particularly in smaller canals. Theywere fabricated to the same size as instruments usedin the preparation of the canal. Silver points had theadvantages of being easy to insert, and length con-trol was easier. Although silver points fulfilled manyof Grossman’s requirements, the main drawback ofsilver points is that they do not seal well laterally orapically because of their lack of plasticity. Silverpoints cannot adequately fill all the canal space andcannot be compacted into spaces or voids within theroot canal system. They maintain their round shapeand no canal is perfectly round in shape, even afterinstrumentation. This leaves too much space to befilled by sealer or cement, thus leading to leakage.The leakage allows corrosion of the silver points andthe formation of silver salts. These products werefound to be cytotoxic. Seltzer et al.6 found suchproducts as silver amine sulfate amide hydrate, silversulfides, and silver sulfates from silver pointsremoved from canals that were obturated with silverpoints. Brady and Del Rio7 found corrosion pro-ducts of sulfur and chlorides by microanalysis of
1019

failed silver points. Goldberg8 found that corrosionwas present microscopically in cases obturated withsilver points that were deemed successful clinicallyand radiographically. Gutierrez et al.9 reported thatcanal irrigants could corrode silver points. Kehoe10
reported a case of localized argyria leading to ‘‘tat-tooing’’ of the alveolar mucosa associated with cor-roding of a silver point in a maxillary premolar.
Silver points used in smaller canals were very suc-cessful in their era. The inappropriate use of silverpoints in larger canals helped to give rise to theirreputation as an inferior obturation method. Withthe advent of different instrumentation techniquesthat allowed for successful obturation of smallercanals with gutta-percha, the use of silver points hasdeclined because of their inherent disadvantages. Theuse of silver points in modern endodontic therapy isextremely limited, and there seems to be no indica-tions or justification for their use today.
Semisolid-Core Filling Materials
Gutta-percha is by far the most popular and com-monly used root canal filling material. Although itdoes not meet all the criteria for an ideal filling mate-rial, it satisfies most of them. The major disadvantageof gutta-percha as a root canal filling material is itslack of rigidity. Gutta-percha, particularly the smallersizes, will bend easily under lateral pressure.
Gutta-percha, known as ‘‘mazer wood,’’ was intro-duced to England from Asia in the 1600s and existedas little more than a curiosity of the East for nearly200 years.11 It was not until 1848 that Ernst Wernervon Siemans used gutta-percha as insulation forunderwater cable. With its many desirable proper-ties, gutta-percha soon was being used in many dif-ferent ways and in many different products. Patentswere applied for new products using gutta-percha,which included ‘‘corks, cements, thread, surgicalinstruments, garments, pipes, musical instruments,candelabras, gaiters, garters, suspenders, windowshades, carpets, gloves, mattresses, pillows, tents,umbrellas, and sheathing for ships.’’11 Perhaps thebest known use of gutta-percha was in golf balls,introduced in the later part of the nineteenth centuryand used until 1920. These golf balls were called‘‘gutties.’’11
Natural gutta-percha has been described as theproduct of various species of rubber trees fromMalaysia, Borneo, Indonesia, and South America,mainly Brazil. Some of the species mentioned assources of natural gutta-percha are Palaquium gutta,
Mimusops globsa, and Manilkara bidentata, and are ofthe same botanical family as the natural rubber treeHevea brasiliensis. Raw gutta-percha is the flexiblehardened juice of these tropical trees.
Gutta-balata is identical in chemical structure andphysical properties to gutta-percha and has long been usedas gutta-percha, or added to gutta-percha in commercialbrands. Additionally, synthetic trans-polyisoprene maybe added to commercial gutta-percha. Raw gutta-perchafrom the tree undergoes a rigorous process to convert itinto commercial grade gutta-percha. This process involvespurification, dissolving of resins, and denaturing ofproteins.12
Friedman et al.13 investigated the ingredients of fivecommercial brands of gutta-percha points. Theyfound the composition of these commercially avail-able gutta-percha points, as seen in Table 1, to consistof 18 to 22% gutta-percha, 59 to 76% zinc oxide, 1 to4% waxes and resins, and 1 to 18% metal sulfates.Although gutta-percha is not the major ingredient, itserves as the matrix. Zinc oxide acts as the filler,whereas the waxes and resins serve as plasticizers.Metal sulfates, such as barium sulfate, provide theradiopacity to identify the material radiographically.
Evidence of slight antibacterial activity from gutta-percha points exists, presumably from the zinc oxidein commercially available gutta-percha14; however, itis too weak to be an effective microbiocide. As thedestruction of bacteria is key to endodontic success, anew formulation of gutta-percha that contains iodo-form, medicated gutta-percha (MGP) (MedidentaInternational, Inc., Woodside, NY), has been devel-oped by Martin and Martin.15 Within the filled rootcanal, the iodine/iodoform depot in the MGP point isa biologically active source for inhibiting microbialgrowth. The iodoform is centrally located within thegutta-percha and takes about 24 hours to leach to thesurface. ‘‘The iodoform remains inert until it comes in
Table 1 Composition of Gutta-Percha Endodontic FillingMaterials (Mean Percentage ± SD)
SampleGutta-Percha
Wax and/or Resin
Heavy MetalSulfates Zinc Oxide
Premier 18.9 ± 0.1 4.1 ± 0.2 14.5 ± 0.4 61.5 ± 0.5
Mynol 19.9 ± 0.1 3.9 ± 0.02 16.2 ± 1.8 59.1 ± 2.0
Union Broach 21.8 ± 0.2 1.0 ± 0.02 17.3 ± 0.3 59.6 ± 0.1
Schwed 19.9 ± 0.2 2.8 ± 0.2 1.5 ± 0.3 75.3 ± 0.5
Star Dental 20.6 ± 1.4 2.9 ± 0.2 3.4 ± 2.1 73.4 ± 2.0
Adapted and reproduced with permission from Friedman et al (1975).13
Composition of commercially available gutta-percha by quantitative analysis
as performed by Friedman, Sandrik, Heuer, and Rapp.
1020 / Endodontics

contact with tissue fluids that activate the freeiodine.’’15 A canal filled with MGP gutta-percha couldserve as a protection against bacterial contaminationfrom coronal microleakage reaching the apical tissue.The use of heat during obturation does not affecteither the release of iodoform or its chemical compo-sition.16 Presumably, the use of iodine containinggutta-percha points would be contraindicated in apatient with a history of allergy to iodine.
An in vitro assessment of iodoform containinggutta-percha tested the ability of the iodoform con-taining gutta-percha to delay the infiltration of Enter-ococcus faecalis using a bacterial microleakagemodel.17 The results showed no difference betweenregular gutta-percha points and iodoform-containinggutta-percha points, both with Roth’s 801 sealer, intheir ability to delay microleakage of E. faecalis.
Gutta-percha points have also been introduced thatcontain a high percentage of calcium hydroxide(40–60%) (Roeko/Coltene/Whaledent, Langenau,Germany). This permits a simple placement of themedicament within the canal space between appoint-ments. Calcium hydroxide points combine the efficacyof calcium hydroxide in a matrix of 42% bio-inertgutta-percha. Once the calcium hydroxide has leachedout, the point is no longer useful as a filling materialand must be removed. Holland et al.18 have reportedon the use of an experimental calcium hydroxide con-taining gutta-percha point that can be used for rootcanal filling. Their results indicate that these pointsproduced an improvement in the apical sealing qualityof the root canal filling.
There are also gutta-percha points available thatcontain chlorhexidine (Activ Point) (Roeko/Coltene/Whaledent) that have a slow release of the chlorhex-idine, and are used in a similar manner as the calciumhydroxide-containing gutta-percha. Some studieshave shown that the points containing chlorhexidinehad a better antibacterial effect than the calciumhydroxide containing gutta-percha points.19
Podbielski et al.20 tested gutta-percha points con-taining calcium hydroxide and zinc oxide, points con-
taining zinc oxide and chlorhexidine, points contain-ing iodine–polyvinylpyrrolidone, and gutta-perchapoints containing a mixture of chlorhexidine andiodine–polyvinylpyrrolidone for their ability to inhi-bit growth of pure cultures of bacterial species comm-only involved in endodontic infections. The calciumhydroxide-containing gutta-percha points proved topossess the strongest antibacterial activity, comparedwith the other three of the four types, for all bacteriatested, with the exception Peptostreptococcus micros.
One study investigated the antimicrobial efficacy ofmedicated filling materials, including standard gutta-percha, iodoform gutta-percha (MGP), and gutta-percha with tetracycline.21 These medicated fillingmaterials were tested against several strains of bacteriaincluding Actinomyces israelii, Actinomyces naeslundii,E. faecalis, and Fusobacterium nucleatum. Standardgutta-percha and the iodoform-containing gutta-perchaweakly inhibited F. nucleatum and A. naeslundii. Inaddition, the iodoform gutta-percha also inhibited A.israelii. Only the tetracycline-containing gutta-perchainhibited all bacterial strains, including E. faecalis.
In 1942, Bunn22 discovered that natural gutta-perchaexisted in a 1,4-trans-polyisoprene stereochemicalstructure. Natural rubber has a 1,4-cis-polyisoprenestereochemical structure. Both gutta-percha andnatural rubber are high-molecular-weight stereo-isomers of polyisoprene. In the cis form of naturalrubber, the CH2 group is on the same side of thedouble bond, whereas in the trans form of polyisoprene(gutta-percha) the CH2 groups are on the opposite sideof the double bond as shown in Figure 1. The cisconfiguration of natural rubber allows for mobility ofone chain past another and gives rise to the elasticnature of rubber, whereas the trans configuration ofgutta-percha is more linear and crystallizes more read-ily making gutta-percha harder, more brittle, and lesselastic than natural rubber.11,23 The scientific methodsavailable to Bunn in 1942 did not allow for 100%identification of the 1,4-polyisoprene configuration, ashe could not rule out the presence of a minoritycis form.24 In 1993, Marciano et al.,24 using nuclear
Figure 1 Stereochemical structure of gutta-percha, 1,4-trans-polyisoprene isomer (natural gutta-percha). CH2 groups are on opposite sides of the doublebond for each successive monomer. Adapted and reproduced with permission from Marciano J et al (1993).24
Chapter 29 / Root Canal Filling Materials / 1021

magnetic resonance, were able to confirm that bothnatural and commercial gutta-percha mainly have a1,4 trans stereochemical structure and that the coloringagent in commercial gutta-percha is erythrosine. Lessthan 1% of the sample had the 1,4 cis stereochemicalstructure.
Gutta-percha exists in two distinct crystalline forms,alpha and beta.22 Raw gutta-percha, as it comesdirectly from the tree, is in the alpha form. Oncepurified, gutta-percha, as it appears commercially inmanufactured gutta-percha products, is in the betacrystalline form. There are few differences in physicalproperties between the two forms, merely a differencein the crystalline lattice depending on the annealingand/or drawing process used when manufacturing thefinal product.25 Although there is apparently no differ-ence in the mechanical properties of the two crystallineforms, there are thermal and volumetric differences.11
Unlike many materials, there are volumetric changesassociated with temperature changes in gutta-percha,which has clinical implications.
If the natural alpha form which comes from the treeis heated above 65�C, it will melt and become amor-phous. If it is very slowly cooled at a rate of 0.5� perhour, the original alpha form will recrystallize. How-ever, if the heated amorphous form cools normally,the beta form will crystallize.11 Schilder et al.26 inves-tigated the temperatures at which the crystalline phasetransitions occurred. They found that, when dentalgutta-percha in the beta crystalline form was heated,a crystalline phase transition to the alpha form tookplace between 42� and 49�C, depending on the spe-cific compound being tested. The alpha-to-amorphousphase transition occurred at a higher temperature ofbetween 53� and 59�C, again depending on the makeup of the specific compound being tested. This infor-mation is useful clinically, when the clinician needs theamorphous form of gutta-percha in order to flowgutta-percha into all parts of the canal and to utilizethermoplastic techniques.
In a study on the thermomechanical properties ofgutta-percha, Schilder et al.27 found that compaction, asopposed to compression, is what occurs in clinicalsituations with gutta-percha. Additionally, the reduc-tion in volume that takes place with mechanical manip-ulation of gutta-percha is due to the consolidation andcollapse of internal voids in gutta-percha, and thisoccurs within compaction forces. Finally, there is nomolecular spring back after compaction of gutta-perchathat would aid in the seal of gutta-percha within theroot canal system. To overcome the shrinkage of gutta-percha as it cools, it is necessary to put pressure on thegutta-percha with a plugger.
Traditionally, the beta form of gutta-percha wasused to manufacture endodontic gutta-percha pointsto achieve an improved stability and hardness and toreduce stickiness. However, through special proces-sing and/or modifications to the formulation of thegutta-percha compound, more alpha-like forms ofgutta-percha have been introduced, resulting inchanges in the melting point, viscosity, and tackinessof the gutta-percha. Gutta-percha with low viscositywill flow with less pressure or stress,25 whereas anincrease in tackiness will help create a more homo-geneous filling. Various manufacturers have intro-duced products to take advantage of these properties(e.g., Themafil, Densfil, MicroSeal).16
Gutta-percha points come in the standardized ISO(International Standards Organization) sizes to cor-respond to endodontic instruments. Initially, theISO-sized gutta-percha points came in the standard0.02 taper to match the instruments available in thatera. Now gutta-percha points are available in theincreased taper sizes of 0.04, 0.06, etc to match theendodontic instruments that have these greatertapers. Color coding to match the ISO size is avail-able on most gutta-percha points marketed today(Figure 2).
The traditional configuration of gutta-percha pointsis manufactured in a form that does not correspond to
Figure 2 Assorted gutta-percha points and absorbent paper points with0.06 taper are shown here, with color coded ends for easy identificationof the size of the point. Reproduced with permission of Brasseler USA.
1022 / Endodontics

ISO sizes but has tapers that closely match the finalinstrumented size of canals. These traditional sizes(extra-fine, fine-fine, medium-fine, fine, fine-medium,medium, medium-large, large, and extra-large) havelong been used in warm vertical obturation techniquesand also match spreader sizes used in lateral compac-tion techniques.
With the thermoplasticized injectable techniques ofgutta-percha placement and obturation of canals, thegutta-percha is produced in pellet form that may beloaded into the heating devise (Obtura III) or asprepackaged cannulas or cartridges (UltraFil, Cala-mus, Elements). Carrier-based gutta-percha productshave gutta-percha surrounding a carrier made ofmetal or plastic.
Gutta-percha that has been stored for extendedperiods of time can become brittle with aging. Sorinet al.28 presented a method to rejuvenate aged andbrittle gutta-percha by immersing it in hot tap water(above 55�C) until the grasping forceps indents thenow softened gutta-percha. The gutta-percha is thenremoved from the hot water and immediatelyquenched in cold tap water (less than 20�C) for severalseconds. The gutta-percha point can now be sterilizedand used to obturate the canal.
Gutta-percha should be stored in a cool locationwith low humidity. Kolokruis et al.29 investigated theeffects of moisture and aging on gutta-percha. Theyfound that high humidity causes the absorption ofwater by the gutta-percha points, which lowers thevalues for tensile strength and torsional strain resis-tance, increases the value for elongation, and has aplasticizing effect on the gutta-percha cones. The plas-ticizing effect is due to the insertion of water mole-cules in the polymer chains.
Senia et al.30 suggested sterilizing gutta-percha priorto insertion into the canal by immersion into 5.25%sodium hypochlorite for at least 1 minute to kill bac-teria and spores on gutta-percha. Examination with adissecting microscope showed no adverse effects on thegutta-percha points that were immersed for 5 minutesin 5.25% sodium hypochlorite.
In a scanning electron microscope (SEM) study,Short et al.31 examined the affect of the sodium hypo-chlorite on gutta-percha points and determined thatgutta-percha fresh from the box had no crystals on itssurface. All the gutta-percha points placed in sodiumhypochlorite had sodium chloride crystals present afterthe rapid-sterilization technique using 5.25 and 2.5%sodium hypochlorite. However, the sodium chloridecrystals could be removed from the gutta-percha surface
by 96% ethyl alcohol, 70% isopropyl alcohol, or dis-tilled water.
The structural effects of sodium hypochlorite solu-tions on gutta-percha points were examined in anatomic force microscopy study by Valois et al.32 Theyfound aggressive deteriorating effects on the gutta-percha points that had been placed in 5.25% sodiumhypochlorite for 1 minute. After 5 minutes in either2.5% or 5.25% sodium hypochlorite, there were topo-graphic changes. However, a 0.5% solution of sodiumhypochlorite did not cause any alteration in the topo-graphy or elasticity of gutta-percha points. They con-cluded that a 0.5% solution of sodium hypochloritewould be a safe alternative for rapid decontaminationof gutta-percha points.
As another alternative for the disinfection of gutta-percha points, Gomes et al.33 looked at the effectivenessof chlorhexidine and sodium hypochlorite as solutionsfor the disinfection of gutta-percha points. In theirboxes, gutta-percha points had a contamination rate of5.5%. Microbes found most frequently, after intentionalcontamination with gloves, were Staphylococcus organ-isms. Chlorhexidine was not effective in eliminatingBacillus subtilis spores on gutta-percha, whereas 5.25%sodium hypochlorite eliminated spores on gutta-perchaafter 1 minute of disinfection.
THERMOPLASTICIZED GUTTA-PERCHAYee et al.34 introduced the concept of obturating rootcanals using injection-molded thermoplasticized dentalgutta-percha. They developed a prototype devise (PAC-160) where gutta-percha points were loaded into a pres-sure syringe and heated to 160�C. They injected theheated and softened gutta-percha into prepared canals,with and without sealer. They found injected thermo-plasticized gutta-percha could produce an effective apicalseal, especially when used with sealer. They introducedwhat would become the Obtura unit.
Injectable thermoplasticized gutta-percha may beused as a primary obturation technique, or, as it is usedmost often today, as a back-filling technique to fill thecoronal aspects of the canal after the initial placementand compaction of gutta-percha by other techniques inthe apical portion of the canal. The thermoplasticizedgutta-percha injection techniques are classified ashigh-temperature and low-temperature thermoplasti-cized gutta-percha injection systems. These systemshave made obturation quicker with the back-fillingtechnique.
The first commercially available thermoplasticizedgutta-percha system was the Obtura system. The Obtura
Chapter 29 / Root Canal Filling Materials / 1023

III Unit (Obtura/Spartan Corp., Fenton, MO) (Figure 3)is a high-temperature thermoplasticized gutta-percha sys-tem that requires gutta-percha pellets to be inserted into adelivery system gun, and then the gutta-percha pellet isheated to 150� to 200�C prior to delivery into the canalsystem. The warmed and softened gutta-percha is thendelivered through 20-, 23-, or 25-gauge needles. Obturagutta-percha also comes in the Flow-150 pellets, which islower temperature thermoplasticized gutta-percha, andrequires heating only to 150�C. The Obtura III also canbe used with Resilon pellets, and lower temperatures arerequired to thermally soften the Resilon.
In a clinical study using the Obtura II system, Tani-Ishii and Teranaka35 reported an overall success rateof 96% with a 1-year follow-up with cases obturatedonly with the Obtura II thermoplasticized injectiontechnique.
Several studies have evaluated the safety of thetemperatures used with injectable thermoplasticizedsystems and, for the most part, found them to be wellbelow the critical 10�C rise in temperature that willcause damage to the periodontal ligament andbone.36–39 According to a study by Lipski,40 high-temperature thermoplasticized injectable gutta-perchain mandibular incisors may show an increase in tem-perature above the 10�C rise that is crucial if damageto the attachment apparatus is to be prevented. Max-illary incisors, however, did not show an externaltemperature rise above 10�C.
The Elements system (Sybron Endo, Orange, CA) is ahigh-temperature thermoplasticized gutta-percha systemthat uses preloaded gutta-percha cartridges that areheated prior to delivery through the unit by an activa-tion button. The gutta-percha is heated to 200�C. Thegutta-percha is delivered through a 45� pre-bent needlethat comes in sizes 20, 23, or 25 gauges (Figure 4).
The Calamus system is manufactured by (TulsaDental Products, Tulsa, OK). The high-temperaturesystem heats the gutta-percha cannulas from 60� to200�C. The delivery system may be activated byfinger pressure on a blue ring with multiple posi-tions. Besides the temperature control, the flow ratemay be controlled by the operator as well. The flowrate of the softened and heated gutta-percha may be
Figure 3 Obtura III Thermoplasticized gutta-percha delivery system byObtura Spartan. Reproduced with permission from Obtura Spartan.
Figure 4 Elements thermoplasticized gutta-percha delivery system withSystem B heat source by Sybron Endo. Reproduced with permission fromSybron Endo.
1024 / Endodontics

regulated from 20, 40, 60, 80, and 100%. The Cala-mus unit only comes with needle sizes of 20 and 23gauges (Figure 5).
UltraFil (Hygienic Corp., Akron, OH) is a low-temperature thermoplasticized gutta-percha deliverysystem that has prepackaged cannulas with attached22-gauge needles. The gutta-percha is prepared in thealpha phase form so that it softens at a temperature of70� to 90�C in the heating unit. Once heated, thecannulas are then placed in the injection syringe andthe softened thermoplasticized gutta-percha is readyfor injection into canal.
Michanowicz and Czonstkowsky41 in a dye studyusing a low-temperature injection system (70 �C)found that when sealer was used, there was verylittle leakage. They used no compaction withthis technique. Lipski42 found temperatures trans-mitted to the periodontal ligament with the Ultra-Fil system were below levels causing damage orinjury.
Thermomechanical Compaction
of Gutta-Percha
Several thermomechanical compaction methods andproducts have been marketed. McSpadden first intro-duced the McSpadden Compactor, which resembled areverse Hedstrom file, which was rotated at up to20,000 rpm. Heat generated by friction softened
gutta-percha, and the blade design pushed materialapically.
The MicroSeal System (Sybron Endo) was also devel-oped by John McSpadden. He redesigned the Compac-tor into the NT Condenser that is used with the Micro-seal System. The NT Condenser rotates at slower speeds(1,000 to 4,000 rpm) than the original McSpaddenCompactor and utilizes nickel–titanium instruments.
The system uses MicroSeal gutta-percha mastercones, and specially formulated gutta-percha, termedlow-fusing or ultra-low-fusing gutta-percha, in a car-tridge that is heated in the MicroSeal heater. Thisspecially formulated low-fusing gutta-percha is adver-tised to be alpha phase gutta-percha, as are the points.A rotating mechanical condenser in a handpiece iscoated with the heated gutta-percha and inserted intothe canal. This rotating condenser creates heat fromfriction that thermally softens the single gutta-perchamaster point previously seated in the canal. It alsoflows laterally, by centrifugal force, the low-fusing orultra-low-fusing gutta-percha coated on the condenserinto all aspects of the canal.43
Cathro and Love44 compared MicroSeal with a tech-nique using the System B with Obtura II backfillobturation. The MicroSeal technique produced a densehomogenous gutta-percha fill at the apical 1 and 2 mmsimilar to the System B/Obtura II technique. Furthercoronally, the sealer became mixed into the MicroFlowgutta-percha, producing a heterogeneous mass with lesssolid gutta-percha compared with the System B/ObturaII technique.
Carrier-Based Gutta-Percha
The concept of a carrier-based thermoplasticizedgutta-percha obturation method was introduced byJohnson in 1978.45 These products are marketed todayas ThermaFil Plus Obturators (Tulsa Dental Products)(Figure 6), GT Obturators (Tulsa Dental Products),ProTaper Obturators (Tulsa Dental Products), Densfil
Figure 5 Calamus thermoplasticized gutta-percha delivery system byTulsa Dentsply. Reproduced with permission of Tulsa Dentsply.
Figure 6 ThermaFil Plus Obturator by Tulsa Dentsply. Reproduced withpermission of Tulsa Dentsply.
Chapter 29 / Root Canal Filling Materials / 1025

(Dentsply Tulsa, Tulsa, OK), and Soft-Core (Soft-CoreSystem, Inc., CMS Dental, Copenhagen, Denmark).
The original ThermaFil obturators had a metalcarrier, now replaced with a grooved plastic carrier.Gutta-percha, which coats the carrier, is said to bealpha phase gutta-percha, and certainly after heatingin the ThermaFil oven, the gutta-percha is in thealpha or amorphous phase.
Gutmann et al.46 compared lateral compaction withThermaFil obturation and found that curved canals,treated with ThermaFil, resulted in a denser, better-adapted obturation on radiographic examination thanthose obturated with lateral compaction. However,both showed acceptable root canal fills in the apicalone third, and ThermaFil extruded more materialbeyond the apex. In the second part of the study, nosignificant difference was seen in dye leakage afterobturation with lateral compaction or ThermaFil.Both demonstrated dye leakage over a 5-month per-iod.47
Becker and Donnelly48 in a literature review of Ther-maFil obturation made these observations. ThermaFilappears to seal the apical foramen as well as other ther-moplasticized techniques, lateral compaction techniques,or vertical compaction techniques.47,49–60 ThermaFilappears to adapt well to canal walls, but the long-termseal may be affected by exposed (bare) carrier.61 Corro-sion of metal carriers should not cause concern. There issignificantly more extrusion of gutta-percha comparedwith lateral compaction.46,56,60 Coronal leakage varies bystudy, but ThermaFil appears to allow significantly moreleakage.62–64 The effect of post-space preparation on theapical leakage of ThermaFil obturators varied dependingon the particular study.65–72 Re-treatment may be moredifficult, especially with metal carriers and if the canal hasbeen prepared for a post.72–76 Metal carriers may limit theability to perform root-end resection.77,78
Felstead et al.52 examined apical leakage and foundno statistically significant difference among teethobturated with ThermaFil when heated to 100�,120�, or 144�C, but there was a trend toward lessleakage with lower temperatures. There was no sig-nificant leakage difference between teeth obturatedwith ThermaFil or lateral condensation.
Clark and El Deeb56 investigated the sealing abilityof plastic versus metal carriers in ThermaFil obtura-tors. Both carrier types were rarely completelyentombed by gutta-percha in the apical third; how-
ever, no leakage was detected in any of the obturatedcanals. Both ThermaFil groups yielded significantlymore cases of apically extruded gutta-percha com-pared with the lateral condensation group. Extrusionswere found to occur significantly more in straightthan curved canals.
Weller et al.79 compared three types of ThermaFilobturators, the Obtura II technique, and lateral com-paction for the ability of the gutta-percha to adapt tothe canal walls. The Obtura II injectable techniquedemonstrated the best adaptation of gutta-percha tothe prepared root canal followed by the plastic andtitanium ThermaFil obturators that were similar, fol-lowed by the stainless steel ThermaFil obturators, andfinally by the lateral compaction technique, whichshowed the poorest adaptation of gutta-percha to thecanal walls.
GT Obturators are designed to be used after pre-paration with GT files (Tulsa Dental Products), andProTaper obturators after preparing a canal with Pro-Taper files (Tulsa Dental Products).
Robinson et al.80 compared extrusion of gutta-percha in teeth instrumented with ProFile 0.06 orProFile GT and obturated with ThermaFil Plusobturators or ThermaFil GT obturators, respectively,or with warm vertical condensation. Extrusion ofgutta-percha was seen more often in the teeth obtu-rated with ThermaFil GT obturators, followed by teethobturated with ThermaFil Plus obturators, with theleast amount of extrusion occurring with the warmvertical condensation technique with either instru-mentation method.
In one study, the percentage of gutta-percha-filledarea in the apical third of root canals obturated witheither lateral condensation technique, System B tech-nique, or ThermaFil technique was examined. Therewas no significant difference between the percentagesof gutta-percha-filled area for lateral condensation orSystem B technique, but the coated carrier gutta-percha system (ThermaFil) produced a significantlyhigher percentage of gutta-percha-filled area than theother two techniques.81
Temperatures produced by heated carrier-basedgutta-percha have been found to be at levels safe forbone and periodontal ligament.40,82
Densfil (Maillefer/Dentsply International, York,PA) is a carrier-based gutta-percha system with bothplastic and titanium carriers, a spin-off of ThermaFil.
1026 / Endodontics

SimpliFil (LightSpeedUSA, San Antonio, TX) (Figure 7)is a 5 mm apical plug of gutta-percha or Resilon on the endof a file and is used similar to a carrier-based system. It hasthe advantage of not leaving the carrier in the canal, as it istwisted off of the apical plug.
Jarrett et al.83 compared the apical density ofgutta-percha in palatal roots of maxillary molarswhen filled with SimpliFil, as recommended by themanufacturer; ThermaFil; warm vertical condensa-tion Schilder technique; warm vertical continuouswave technique; mechanical lateral technique; coldlateral condensation technique; and a modifiedSimpliFil technique. SimpliFil, as recommended,and ThermaFil had the greatest mean obturatedarea, but neither was statistically better thanmechanical lateral or warm vertical condensation(Schilder) technique. SimpliFil, as recommended,and ThermaFil were statistically better than coldlateral condensation technique, warm vertical con-densation (continuous wave) technique, and themodified SimpliFil group. Mechanical lateral andwarm vertical condensation (Schilder) techniqueshad statistically more obturated area than warm ver-tical condensation (continuous wave) and modifiedSimpliFil techniques. Cold lateral and warm verticalcondensation (continuous wave) had significantlymore obturated area than modified SimpliFil.
Shipper and Trope84 compared microbial leakagein canals obturated with one of the following techni-ques: lateral compaction, vertical compaction, ObturaII thermoplasticized injection technique, SimpliFilwith Obtura II, FibreFil (Pentron Clinical Technolo-gies, Wallingford, CT), or a combination of FibreFiland SimpliFil. Microbial leakage occurred morequickly in the lateral and vertical compaction techni-ques compared with SimpliFil and FibreFil techni-ques. A combination of an apical plug of gutta-perchawith SimpliFil and a FibreFil coronal seal provided thebest obturation.
SuccessFil is a carrier-based gutta-percha systemcombined with the UltraFil thermoplasticizied injec-tion system to create what is marketed as the TrifectaSystem (Hygenic/Coltene/Whaledent). Goldberget al.85 compared the sealing ability of Trifecta, lateralcondensation and SuccessFil with lateral condensa-tion. No statistically significant differences in leakagewere seen between the groups.
JS Quick-Fill (JS Dental Manufacturing, Inc., Ridge-field, CT) is an alpha phase gutta-percha-coated tita-nium core in ISO sizes 15 to 60. The carrier-basedmaterial is spun into the canal at low speed, and thecore may be left in the canal or slowly removed.
Properties of Gutta-Percha
Gutta-percha is generally regarded as a very acceptablematerial with good biocompatibility with the periapicaltissues. This has, for the most part, been verified inseveral studies, with the exception that some formula-tions of gutta-percha have produced localized severeinflammatory reactions in animals.86 Wolfson and Selt-zer,87 in a 1975 study, found severe tissue reaction toeight brands of gutta-percha they injected into the skinof rats.
Tavares et al.88 looked at the reaction of rat subcu-taneous tissue to implants of different commerciallyavailable gutta-percha compared with Teflon controlcylinders. Studies were conducted on Kerr andHygenic brands of gutta-percha, and cylinders usedwith the UltraFil thermoplastic injectable gutta-perchafrom Hygenic Corp. The Kerr points gave mild reac-tions throughout all experimental periods, and theUltraFil cylinders initially produced a foreign bodyreaction caused by the dispersion of filling materialparticles mediated by macrophages and giant cells,but this response decreased with time and thus wasconsidered biologically acceptable. The Hygenic gutta-percha points caused a severe initial inflammatorytissue reaction suggestive of bioincompatibility.
Figure 7 SimpliFil has a metal carrier that comes in ISO sizes 35 to 130with a 5 mm plug of gutta-percha or Resilon on the end. Reproducedwith permission of LightSpeed.
Chapter 29 / Root Canal Filling Materials / 1027

The ingredients of gutta-percha, such as zinc oxide,may contribute to the cytotoxic effects of some com-mercial gutta-percha.89 However, other studies havesuggested that the zinc oxide component may reducethe toxicity of other ingredients, especially rosin andresin acids.90
The tissue toxicity exerted by gutta-percha is moreevident in the advent of an overfill or overextension ofgutta-percha into the periapical area. Sjogren et al.91
demonstrated that the size of gutta-percha particlemay make a difference in the intensity of the inflam-matory response. Large gutta-percha particles hadvery little inflammation around them, and appearedto be well encapsulated, whereas the smaller particlesof gutta-percha caused a more intense localizedresponse. Additionally, they found that gutta-perchawith a rosin and chloroform component invoked aresponse considered severe.
In a study by Holland et al.,92 one brand or formula-tion of gutta-percha caused a severe inflammatoryresponse in rat connective tissue with a fibrous capsuleformation, whereas another brand was well tolerated.
Serene et al.93 looked at the activation of comple-ment to examine the inflammatory response of fourdifferent commercially available brands of gutta-percha, and the ingredients in one of the brands. Thisin vitro study showed that each of the four brands ofcommercially available gutta-percha and each of theingredients could cause activation of the complementsystem.
Although some gutta-percha has been shown tobe cytotoxic, invoking inflammatory reactions inconnective tissue, the most toxic portion of thesealer–gutta-percha obturation is the sealer.86
Because gutta-percha and gutta-balata are derivedfrom the Paliquium gutta and M. globsa trees, whichare of the same botanical family of trees as the naturalrubber latex tree, H. brasiliensis, there was concernabout the possible cross-reactivity between gutta-percha and natural rubber latex in individuals whomay have immediate-type hypersensitivity to naturalrubber latex. There have been case reports suggestingthat gutta-percha may release proteins that inducereactions in latex-allergic individuals.94,95 In thesecases, the symptoms were uncharacteristic of thoseroutinely experienced by patients with latex allergies.Other causes, more directly related to the quality ofthe endodontic treatment itself, may have been thereason for the patients’ symptoms. These case reportsdid not prove the cross-reactivity between Hevea latexand gutta-percha. On the other hand, Knowles et al.96
and Kleier and Shibilski97 presented case reportswhere gutta-percha was successfully used to obturate
canals in patients with documented IgE antibody-mediated allergy to natural rubber latex.12 Studiesby Costa et al.12 and Hamann et al.98 usingthe radioallergosorbent test (RAST) inhibition andenzyme-linked immunosorbent assay (ELISA)98
showed that commercially available gutta-perchaalone is not likely to induce symptoms in the patientwith type I natural rubber latex allergy and thatcommercially available gutta-percha can safely beused in these patients. The refining process forgutta-percha is so severe that most proteins wouldbe denatured by the process. Raw gutta-balata was theonly substance that showed cross-reactivity with nat-ural rubber latex.12 None of the processed gutta-percha products, or natural raw gutta-percha, showedany cross-reactivity with natural rubber latex.12
Nevertheless, it is always prudent to investigate nat-ural rubber latex allergies in patients because it is verycommon, particularly among health care workers(17%) and spina bifida patients (67%).99–101
Newer Solid-Core Filling Materials
Resilon (Pentron Clinical Technologies), and RealSeal(Sybron Endo), is a polycaprolactone core materialwith difunctional methacrylate resin, bioactive glass,bismuth and barium salts as fillers, and pigments,which is used with a resin sealer (Epiphany or Real-Seal) that is packaged with the core filling material(Figures 8). The rational behind the product is tocreate a ‘‘monoblock’’ consisting of a resin sealer with
Figure 8 Epiphany sealer is a resin type of sealer used with polyca-prolactone core materials such as Resilon core material. Courtesy,James David Johnson.
1028 / Endodontics

resin tags that enter into and bond to dentinaltubules, and to the dentin on the canal wall, as wellas adhesively bonding to the core material, and whichcan also be light cured and sealed coronally as well.The Resilon system consists of a primer, a sealer, andsynthetic polymer points or pellets.
Whereas the sealer used with Resilon is discussedunder the discussion on sealers later in this chapter,the Resilon system, core material and sealer, has to beused together, as it is one system, and each part relieson the other parts to be successful.
The polyester core material is marketed in ISO-sized points with accessory points for lateral compac-tion and warm vertical techniques, or pellets for use inthermoplasticized techniques.101 The temperaturesused in the thermoplasticized techniques for thepolyester resin core materials are lower than thoseused for gutta-percha techniques (150�C, comparedto 200�C), but otherwise has handling characteristicsthat are similar to gutta-percha and allows for lateralcompaction or warm vertical obturation techniques.In the case of using Resilon with the System B unit,the temperature is set at 150�C and the power is set at10. If Resilon is used with the Obtura III thermoplas-ticizing unit with 25-gauge needles, the temperature isset at 160�C; with 23-gauge needles, the temperatureis set at 140�C; and for use with 20-gauge needles, thetemperature is set at 120� to 130�C.
One study compared Resilon with gutta-percha interms of the melting point, specific heat capacity,enthalpy change with melting, and heat transfer. Itwas found that there was no difference in the meltingpoint temperatures for the two materials, but Resilonhad a significantly greater specific heat capacity andendothermic enthalpy change. There was a significantdifference in the heat transfer test in the temperatureincrease between gutta-percha and Resilon within 3mm of the heat source, with gutta-percha having agreater temperature change. They concluded thatResilon may not be thermoplasticized the same asgutta-percha because there is a higher specific heat,higher enthalpy change with melting, and less heattransfer.102
Nielsen and Baumgartner103 examined the depth ofnickel–titanium spreader penetration in root canalshaving a 0.04 preparation size taper using 0.02 and0.04 tapered master gutta-percha or Resilon points. Asignificant difference in penetration depth was foundfor both taper of the point and the material used. Thedepth of spreader penetration was greatest for 0.02tapered Resilon, followed by 0.02 gutta-percha, fol-lowed by 0.04 tapered Resilon, and the least spreaderpenetration occurred with the 0.04 gutta-percha.
Shipper et al.104 investigated the resistance to bac-terial penetration of gutta-percha with AH 26 sealer,gutta-percha with Epiphany sealer, and Resilon withEpiphany sealer. Each combination of core materialand sealer was obturated with both lateral and verticalcondensation techniques. The Resilon groups werefound to have less leakage than the gutta-perchagroups with respect to the number and rate of thespecimens in each group that leaked. All Resilon andEpiphany sealer groups leaked significantly less thanall groups in which AH 26 was used as a sealer.
By contrast, other investigators105 performed anultrastructural evaluation of the apical seal in rootsfilled with a polycaprolactone-based root canal fillingmaterial. This study compared the ultrastructuralquality of the apical seal achieved with Resilon andEpiphany sealer with that produced by gutta-perchaand AH Plus sealer. The SEM revealed both gap-freeregions and gap-containing regions in canals filledwith both materials. The transmission electron micro-scope revealed the presence of silver deposits along thesealer-hybrid layer interface in the Resilon/Epiphanysamples and between the sealer and gutta-percha sam-ples. They concluded that a complete apical seal can-not be achieved with either combination of root canalfilling material and sealer.
The susceptibility of a polycaprolactone-based rootcanal filling material (Resilon) to degradation hasbeen investigated. Tay et al.106 examined what effectalkaline hydrolysis would have on disks of Resilon orgutta-percha using scanning electron microscopy andenergy dispersive X-ray analysis. They found thatfor Resilon, the surface resinous component washydrolyzed after 20 minutes of immersion in sodiumethoxide, which exposed the spherulitic polymerstructure and subsurface glass and bismuth oxychlor-ide fillers. Gutta-percha did not undergo alkalinehydrolysis when immersed in sodium ethoxide.
Tay et al.107 evaluated the susceptibility of Resilon,gutta-percha, and polycaprolactone disks to hydrolyticenzymes present in saliva or secreted by endodontically-relevant bacteria. All three materials had slight weightgains when incubated in phosphate-buffered saline.Gutta-percha showed similar weight gains with theenzymes, lipase polysaccharide, and cholesterol esterase,but Resilon and polycaprolactone exhibited extensivesurface thinning and weight loss after incubation inlipase polysaccharide and cholesterol esterase. Glass fil-ler particles in Resilon were exposed following surfacedissolution of the polymer matrix, which created arough surface topography. They concluded that biode-gradation of Resilon by bacterial and salivary enzymeswarrants further investigation.
Chapter 29 / Root Canal Filling Materials / 1029

The interfacial strengths of Resilon with Epiphanysealer have been compared with those of gutta-perchawith AH Plus sealer by Gesi et al.108 The gutta-percha/AH Plus testing group exhibited significantly higherinterfacial strength than did the Resilon/Epiphanygroup, when premature failures that occurred in Resi-lon root slices were included. The gutta-percha rootslices failed exclusively along the gutta-percha/sealerinterface. The Resilon root slices failed predominantlyalong the sealer/dentin interface with recognizable,fractured resin tags. Detachment of Resilon from theEpiphany sealer was also observed in some specimens.The relatively low interfacial strengths of materials,gutta-percha/AH Plus, and Resilon/Epiphany seemedto challenge the concept that root strengthening isaccomplished with either material.
Stratton et al.109 looked at the sealing ability ofResilon and Epiphany sealer versus that of gutta-percha and AH Plus sealer, by means of fluid filtrationtesting. They found significantly less leakage usingResilon and Epiphany as compared with the gutta-percha and AH Plus sealer.
Another study found Resilon with Epiphany sealerhad less leakage after 30 days than gutta-percha andsealer. All canals obturated with gutta-percha and sea-ler, and those obturated with Resilon or gutta-perchawithout sealer leaked within 30 days.110
Wang et al.111 investigated the effects of calciumhydroxide medication on the sealing ability of Resilonand found that calcium hydroxide did not adverselyaffect the seal of the root canal system that was sub-sequently filled with Resilon.
In an investigation comparing the completeness ofroot canal obturation with gutta-percha techniquesversus Resilon with Epiphany sealer, using lateralcompaction and continuous wave obturation, resultsshowed that lateral compaction of gutta-percha wasthe only group with significantly more voids thangutta-percha with the continuous wave obturation,or Resilon with Epiphany sealer using either obtura-tion technique.112
Resilon has been reported to reinforce the rootcanal system because of its adhesion to the canal walland integration of the core material.113 On the otherhand, another study compared cohesive strength andthe stiffness of Resilon and gutta-percha under dryconditions and after 1 month of water storage, todetermine whether they are stiff enough to reinforceroots. They found that both Resilon and gutta-perchahad relatively low cohesive strength and modulus ofelasticity, and did not have enough stiffness to rein-force roots after endodontic therapy.114
Long-term results and clinical trials will be useful inthe evaluation of Resilon as compared with gutta-percha, and the evolution of newer generations ofResilon may further improve the material.
Paste Filling Materials
Zinc oxide is a major component of many paste mate-rials used in endodontics. It is the other ingredients inmany zinc oxide paste materials that are responsiblefor other properties and potential toxicity. These pasteswill be discussed under the pastes containing otheringredients. Because of the solubility of zinc oxide, theydo not make effective core filling materials.
A paste filling material that has been widely usedin Eastern European countries and some Asian andPacific Rim nations is a resin type of material knownas ‘‘Russian Red.’’115 This is resorcin–formaldehydepaste, a type of phenol–formaldehyde or Bakeliteresin.101 Ørstavik101 reported it is strongly antimicro-bial, but with the disadvantage of shrinkage in thecanal once placed, and that it often stains tooth struc-ture a dark red. Sometimes re-treatments can bedifficult, if the resin sets completely and there issufficient bulk to the material.115
Trailement SPAD is another resin-based type ofpaste material that has been used in Europe.
Mineral Trioxide Aggregate
Mineral trioxide aggregate (MTA) has many uses inendodontics (Figure 9). MTA is used as a pulp-capping material,116–118 as a perforation repairagent,119–122 as a root-end filling material,123–125 as anapical barrier,126–128 and as an intraorifice barrier,129 and
Figure 9 White and gray ProRoot mineral trioxide aggregate (MTA) byTulsa Dentsply. Reproduced with permission of Tulsa Dentsply.
1030 / Endodontics

may be considered as a paste filling material for theobturation of root canals. Because of its sealing ability,biocompatibility, and other desirable properties, it wouldseem to be a paste filling material that is indicated whenmore conventional core filling materials cannot be used.The major drawbacks of MTA are its somewhat difficulthandling characteristics, which may be overcome withexperience, and its extended setting time of at least 3hours or more. Its many favorable properties and char-acteristics make it a valuable material in many aspects ofendodontics.
ProRoot MTA (Tulsa Dental Products, Tulsa, OK)was introduced by Torabinejad et al.123 in 1993 as aroot-end filling material and as a root perforationrepair material.119 They reported the ingredients astricalcium silicate, tricalcium aluminate, tricalciumoxide, and silicate oxide, with some other mineraloxides that were responsible for the chemical andphysical properties of the aggregate. The powder con-sists of fine hydrophilic particles that set in the pre-sence of moisture. The hydration of the powderresults in a colloidal gel with a pH of 12.5 that willset in approximately 4 hours.130
Several studies have stated that MTA is very similarin nature to commercial Portland cement.131–135
Wucherpfenning and Green132 analyzed MTA andPortland cement by X-ray diffraction and reportedthat they were similar macroscopically and microsco-pically. Estrela et al.133 showed that Portland cementcontains the same chemical elements as MTA, withthe exception of bismuth oxide, which is added toMTA to increase its radiopacity. Duarte et al.136
reported that MTA Angelus is 80% Portland cementand 20% bismuth oxide. Sarkar et al.137 stated thatMTA is a mechanical mixture of three powder ingre-dients, which are Portland cement (75%), bismuthoxide (20%), and gypsum (5%), with trace amountsof SiO2, CaO, MgO, K2SO4, and Na2SO4. They alsolisted the ingredients of the major component, Port-land cement, as dicalcium silicate, tricalcium silicate,tricalcium aluminate, and tetracalcium aluminofer-rite.
One of the very favorable properties of MTA is itsoutstanding sealing ability. This has been verified inmany studies using MTA as a root-end filling materialand for sealing perforations in both dye leakage andbacterial leakage models. Torabinejad et al.123 usingan aqueous solution of rhodamine B fluorescent dyefound MTA leaked significantly less than amalgam orethoxybenzoic acid (Super EBA) as a root-end fillingmaterial. In another dye study, Torabinejad et al.138
found MTA sealed better as a root-end filling material
than amalgam, Intermediate Restorative Material(IRM), or Super EBA, even in the presence of bloodcontamination. Gondim et al.139 demonstrated, with adye study, that MTA leaked significantly less thanSuper EBA or IRM, regardless of the finishing techni-que employed. In a bacterial leakage investigation ofroot-end filling materials, Torabinejad et al.140
showed that MTA leaked significantly less than theother root-end filling materials tested. MTA was alsofound to allow less leakage of endotoxin in a study byTang et al.141 Tselnik et al.129 examined bacterialleakage with MTA or a resin-modified glass ionomeras a coronal barrier. They found both gray and whiteMTA, when used as a coronal barrier, preventedmicrobial leakage for over 90 days. Nakata and cow-orkers121 found that MTA provided a better seal thanamalgam to prevent the leakage of F. nucleatum intofurcation perforations.
In a SEM study, Torabinejad et al.142 showed thatMTA had better marginal adaptation than amalgam,Super EBA or IRM. Other studies using the SEM haveagreed with these findings with regard to MTA adap-tation.143,144 Xavier et al.145 examined both dye leak-age and marginal adaptation as viewed under the SEMand found that MTA Angelus leaked significantly lessthan a glass ionomer, but statistically more than SuperEBA. They found that MTA Angelus had much bettermarginal adaptation than EBA, or the glass ionomerwhen viewed under the SEM. Mangin et al.146 foundno difference in leakage of radioactive labeled bacteriabetween hydroxyapatite cement, MTA, and SuperEBA when used as root-end filling materials.
In a fluid filtration model, Bates et al.147 found MTAwas comparable with Super EBA in the prevention ofleakage, but Wu et al.148 reported MTA leaked signifi-cantly less than Super EBA. DeBruyne et al.149 using afluid transport and capillary flow porometry techniquefound that after 1 day, and after 1 month there was nostatistical significant difference in leakage between areinforced glass ionomer cement and white MTA inroot-end fillings. At 6 months, however, the glass iono-mer leaked significantly less than MTA. There were nosignificant differences observed with flow porometrybetween pore diameters of the materials tested.
The effects of the thickness and of resection of MTAhave been investigated. Andelin et al.150 examined leak-age after the resection of MTA placed in canals beforethe root end was resected and found that the resectionof set MTA did not affect its sealing ability. Lambet al.151 had similar findings, as long as at least 3 mmof MTA remained. Valois et al.152 examined the influ-ence of thickness of MTA on the sealing ability of the
Chapter 29 / Root Canal Filling Materials / 1031

material and showed that a 4 mm thickness of MTA wassignificantly more effective in preventing protein leak-age than lesser thicknesses of MTA. Matt et al.153 foundthat for an apical barrier, 5 mm of MTA was signifi-cantly harder than a 2 mm barrier, and allowed signifi-cantly less leakage. These dimensions may be important,not only in the depth of root-end fillings with MTA butwhen it is used as an apical barrier, or as a perforationrepair material, or for other purposes.
MTA has been studied extensively for its biocom-patibility with its application as a root-end fillingmaterial in root-end endodontic surgery. Cell culturestudies have demonstrated that the cytotoxicity ofMTA was significantly less than that of IRM or SuperEBA.154 Implantation of MTA into tibias and mand-ibles of guinea pigs resulted in a tissue reaction con-sidered favorable and slightly milder than that ofSuper EBA.155 Koh et al.156 found favorable biologicresponses to MTA from human osteoblasts, andfavorable cellular response to MTA.157
Haglund et al.158 compared MTA, amalgam, IRM,and a composite resin for their effects on mouse fibro-blasts and macrophages. They found all four materialsinhibited cell growth. There were significantly fewercells cultured with the fresh IRM and compositegroups compared with the MTA and amalgam groups,and there was no difference between a fresh mix ofMTA and a fresh mix of amalgam. For set materials,there was no significant differences in the fibroblastcell growth between MTA, amalgam, and the compo-site resin. In the fibroblast cell line, set IRM hadsignificalntly fewer surviving cells than the other setmaterials. There was a significant difference in thesurvival of cells in the macrophage cell line in thepresence of the set materials between the compositeresin group and MTA, and between the compositeresin group and amalgam, with fewer macrophagessurviving in the presence of the composite resin setmaterial. Set IRM had significantly fewer cells survivethan the other set material in the macrophage cell linealso. DeDeus et al.159 compared the cytotoxicity ofProRoot MTA, MTA Angelus, and Portland cementand found no significant difference between the threematerials in terms of cytotoxicity and that all threeinitially showed similar elevated cytotoxic effects thatdecreased gradually with time, allowing the cell cultureto become reestablished.
Hernandez et al.160 studied the effect of mixingchlorhexidine with MTA versus MTA mixed withwater on the apoptosis and cell cycle of fibroblastsand microphages. They found that mixing MTA withchlorhexidine induced apoptosis of fibroblasts andmacrophages and decreased the percentage of both cell
types in the S phase (DNA synthesis) of cell cycles.Thus, mixing sterile water with MTA was determinedto be less cytotoxic than mixing MTA with chlorhex-idine. Melegari et al.161 studied the production ofprostaglandin E2 (PGE2) and the viability of cells cul-tured in contact with freshly mixed Roth’s 801 sealer,Sealapex sealer, and MTA. It was found that none ofthe materials stimulated the release of PGE2.
MTA is also reported to have qualities that mayprovide an environment for repair and regenerationof periapical tissues. MTA has shown an inductiveeffect on cementoblasts in dogs and monkeys.124,125
Zhu et al.162 showed osteoblasts attaching and spread-ing on MTA. Regan et al.163 demonstrated that bothMTA and Diaket can support almost complete regen-eration of the periradicular periodontium when usedas a root-end filling material on teeth that are notinfected. Baek et al.164 found that MTA showed themost favorable periapical tissue response and thatthere was neoformation of cemental coverage overMTA.
There is conflicting information as to whether grayand white MTA have the same physical propertiesand biocompatibility. Holland et al.135,165,166 haveshown that both white and gray formulations arebiocompatible when implanted into rat connectivetissue. Perez et al.167 demonstrated that white MTAwas less biocompatible than gray MTA. Camilleriet al.168 showed no difference between the gray andwhite formulations of MTA. Ribeiro et al.169 showedno difference in cytotoxic effects for gray MTA,white MTA, or Portland cement. The same groupfound no difference in genotoxicity or cytotoxicitybetween gray or white MTA.170 Asgary et al.171 byelectron probe microanalysis observed that the con-centrations of Al2O3, MgO, and particularly FeO inwhite MTA are considerably lower than those foundin gray MTA. The FeO is thought to be the primaryingredient responsible for the color differencesbetween white and gray MTA. Oviir et al.172 investi-gated the proliferation of oral keratinocytes andcementoblasts on gray and white MTA. They foundboth cell types grew significantly better on the sur-face of white MTA compared with gray MTA. Inaddition, both cell types showed significantly higherproliferation when grown on 12-day-cured grayMTA compared with 24-hour-cured gray MTA. Mattet al.153 found that white MTA leaked significantlymore than did gray MTA and that a two-step tech-nique, where a moist cotton pellet is placed over theMTA for 24 hours to allow it to set, showed lessleakage than a one-step technique for placing anapical barrier.
1032 / Endodontics

There is some conflicting opinion as to whether amoist cotton pellet is needed to allow the MTA to setproperly when used within the root canal system, otherthan as a root-end filling material where it is in contactwith moisture. This step adds another appointment tothe treatment when MTA is used as a perforation repairmaterial, as an apical barrier, or as an intraorifice bar-rier. There have been case reports where a moist cottonpellet is used between appointments to allow for theMTA to set.126–128 On the other hand, Sluyk et al.173
showed that the retention characteristics of MTA usedas a perforation repair material was not altered by theplacement of either a dry or a moist cotton pellet overthe MTA, and the moisture from the periradiculartissues may provide adequate moisture to allow theMTA to set properly. Matt et al.153 did show, however,that the application of a moist cotton pellet significantlyreduced leakage of MTA used as an apical barrier.
The long-term solubility of MTA was investigatedby Fridland et al.174 Their results showed that MTAis capable of partially releasing its soluble fractioninto an aqueous environment over a long period oftime and it still maintains its high pH level of 11 to12 over at least 78 days, while also maintaining itsinsoluble matrix of silica which produces MTA’sstructural integrity even while in contact with water.This soluble fraction is mainly composed of calciumhydroxide, which may provide the alkalinity favor-able for cell division and matrix formation forhealing of periradicular tissues and for anti-microbial activity. Sarkar et al.137 speculated thatafter placement of MTA in root canals and its gra-dual dissolution, hydroxyapatite crystals nucleateand grow, filling the microscopic space betweenMTA and the dentinal wall. This seal is first mechan-ical, but then they envision a reaction between theapatite layer and the dentin in the form of a chemicalbond, and a seal between MTA and dentin.
Some investigators are looking into modificationsof Portland type cements to alter the setting proper-ties and handling characteristics. One of the maindisadvantages of using MTA is its extended settingtime. In industrial uses of Portland cement, the set-ting time may be increased by adding gypsum orreduced to a flash set by removing gypsum. Camilleriet al.175 investigated a new accelerated Portlandcement. The setting time of the Portland cementwas reduced by excluding gypsum in the last stageof the manufacturing process. The biocompatibilitytesting of this accelerated Portland cement was notaltered by adding bismuth oxide for radiopacity andhad similar biocompatibility as gray MTA, whiteMTA, and white Portland cement. Future research
will have to determine whether altering the undesir-able aspects of MTA can be accomplished withoutaffecting its very desirable properties of sealing, bio-compatibility, and favorable conditions for repairand regeneration of periradicular tissues.
Paraformaldehyde Pastes
Paraformaldehyde pastes may also be considered assealers, and are used as sealers by some. The additionof paraformaldehyde is for its antimicrobial andmummifying effects, but unfortunately its severetoxicity to host tissues outweighs any antimicrobialeffects it may possess as an ingredient in endodonticmaterials.
N2 paste (Indrag-Agsa, Losone, Switzerland) and itsUS counterpart, RC2B, is a liquid and powder paste.The liquid contains zinc oxide, bismuth nitrate, bis-muth carbonate, paraformaldehyde, and titaniumoxide. The liquid consists of eugenol, peanut oil, androse oil.176 The contents of N2 have changed over theyears in response to studies identifying toxic substances,such as lead oxide and organic mercury.177 It still con-tains large amounts of paraformaldehyde (4–8%).86 N2has been found to be extremely toxic.178,179 Further-more, because it is used as a paste, the extrusion of thistoxic material is easier and has caused severe neurolo-gical damage in reported cases.180–183 The Food andDrug Administration (FDA) lists N2 or RC2B as anunapproved new drug not legally imported or shippedacross interstate lines.184 The American Dental Associa-tion (ADA) Council of Dental Therapeutics does notapprove the use of paraformaldehyde pastes or sealers.A case report of a dentist who was found liable for apatient’s permanent disability as a result of root canaltherapy with N2 (Sargenti’s) paste was presented in thestatus report. The canal was obturated with N2, whichreportedly extruded into the mandibular canal causingnerve damage, facial dysesthesia, and pain. The patientwas awarded $250,000 (US) for injury.185
The American Association of Endodontists has issueda position paper on the use of paraformaldehyde-containing endodontic materials, recommendingagainst their use.186 Some states, including Florida, havebanned the use of paraformaldehyde pastes.187 Becauseof the toxicity, legal issues, risks to patients, and the factthere are numerous other obturating materials availablethat provide a better outcome, without risk to thepatient, the use of these materials in modern-day endo-dontics cannot be supported.
Endomethasone (Septodont, Paris, France) is aliquid-powder sealer used in Europe. The powder
Chapter 29 / Root Canal Filling Materials / 1033

contains dexamethasone, hydrocortisone acetate,thymol iodide, paraformaldehyde, and a radiopaqueexcipient, whereas the liquid contains eugenol, pep-permint oil, and Anise oil.176 The difference betweenEndomethasone and other paraformaldehyde-containingsealers is the addition of the hydrocortisone. Thetoxicity of the paraformaldehyde still remains.
Riebler’s paste (Amubarut; Wera Karl, Biesingen,Germany) is another paraformaldehyde-containingpaste as is Trailement SPAD, another resin-based typeof paste material that has been used in Europe.
Sealers
REQUIREMENTS FOR AN IDEAL ROOTCANAL SEALING MATERIALIn addition to the basic requirements for core fillingmaterials, Grossman also listed the following 11requirements for a root canal sealer:188,189
1. It should be tacky when mixed to provide goodadhesion between it and the canal wall when set.
2. It should make a hermetic seal.3. It should be radiopaque so it can be visualized in
the radiograph.4. The particles of powder should be very fine so
they can mix easily with the liquid.5. It should not shrink upon setting.6. It should not stain tooth structure.7. It should be bacteriostatic or at least not encou-
rage bacterial growth.8. It should set slowly.9. It should be insoluble in tissue fluids.
10. It should be tissue tolerant, that is, nonirritatingto periradicular tissues.
11. It should be soluble in a common solvent, if it isnecessary to remove the root canal filling.
One might add the following to Grossman’s originalbasic requirements:
12. It should not provoke an immune response inperiradicular tissues.190–193
13. It should be neither mutagenic nor carcino-genic.194,195
Zinc Oxide-Containing Sealers
For many years, zinc oxide-containing sealers havebeen the most popular and widely used sealers. Thereare many formulations and brands of sealers that have
zinc oxide as the primary ingredient, differing only byother components added to the sealers.
Zinc oxide sealers allow for addition of otherchemicals, such as paraformaldehyde, rosin, Canadabalsam, and others, all of which may increase theirtoxicity.86 Zinc oxide-containing sealers that haveother ingredients will be discussed under thosesections.
Grossman’s original formula contained zinc oxide,staybelite resin, bismuth subcarbonate, barium sul-fate, and sodium borate (anhydrous) with eugenol asthe liquid component.188 It has been marketed asProcosol sealer, as well as other product names.
Roth’s 801 sealer (Roth’s Pharmacy, Chicago, IL) isessentially the same as Grossman’s original formula-tion, with the substitution of bismuth subnitrate forbismuth subcarbonate. Eugenol is used as the liquidof the sealer (Figure 10).
Rickert’s formula was an early zinc oxide-containingsealer. It has long been an acceptable standard, meetingmost of Grossman’s requirements for an ideal sealer.Its major drawback was the staining of tooth struc-ture from the silver that was used for radiopacity.16
Rickert’s formula was marketed as Kerr’s Pulp CanalSealer (Sybron Endo/Kerr, Orange, CA). Pulp CanalSealer has been popularized by clinicians using thewarm vertical obturation techniques. A major disad-vantage of Pulp Canal Sealer was its rapid settingtime, especially with heat and in regions with hightemperatures and high humidity.16 To overcomethis disadvantage, researchers formulated Pulp CanalSealer EWT (Extended Working Time) (Sybron
Figure 10 Roth Root Canal Cement is an example of a zinc oxide andeugenol sealer. Courtesy, James David Johnson.
1034 / Endodontics

Endo/Kerr) which reportedly has a working time of6 hours.16
Tubli-Seal (Sybron Endo/Kerr) is a two-paste sys-tem contained in two separate tubes. Developed as anonstaining alternative to the silver-containing PulpCanal Sealer, Tubli-Seal is a zinc oxide-base paste withbarium sulfate for radiopacity, and mineral oil, corn-starch, and lecithin. The catalyst tube has polypaleresin, eugenol, and thymol iodide. Tubli-Seal is easyto mix but has the disadvantage of rapid setting time.16
Tubli-Seal EWT has the same properties as the regularsetting Tubli-Seal but has an extended working time.
Wach’s cement (Roth International Inc., Chicago,IL) consists of a powder of zinc oxide, bismuth sub-nitrate, bismuth subiodide, magnesium oxide, andcalcium phosphate. The liquid contains oil of cloves,eucalyptol, Canada balsam, and beechwood creosote.The liquid gives Wach’s cement a rather distinctiveodor of an old-time dental office.16 It has the advan-tage of having a smooth consistency, and the Canadabalsam makes the sealer tacky.
Nogenol (GC America, Inc., Alsip, IL) was devel-oped to overcome the irritating effects of eugenol.196
This product is an extension of the noneugenol per-iodontal dressings. It is a two-tube, base and catalystsystem with a base of zinc oxide, barium sulfate,bismuth oxychloride, and vegetable oil. Hydrogenatedrosin, methyl abietate, lauric acid, chlorothymol, andsalicylic acid in the catalyst accelerate the settingtime.16
Medicated Canal Sealer (Medidenta International,Inc.) was developed by Martin.15 This sealer containsiodoform for antibacterial purposes and is to be usedwith MGP gutta-percha, which also contains 10%iodoform.16
Calcium Hydroxide-Containing Sealers
Sealapex (Sybron Endo/Kerr) is a calcium hydroxide-containing noneugenol polymeric sealer that is pack-aged as two tubes. Sealapex has zinc oxide in the basealong with calcium hydroxide and also containsbutyl benzene, sulfonamide, and zinc stearate. Thecatalyst tube has barium sulfate and titanium dioxidefor radiopacity, and a proprietary resin, isobutylsalicylate, and aerocil R792.16 Sealapex had nogreater dissolution than Tubli-Seal at both 2 and 32weeks. It appears that Sealapex had a sealing abilitycomparable with Tubli-Seal and could withstandlong-term leakage.197
Holland and De Souza198 studied Sealapex sealer tosee if it could induce hard tissue formation. Sealapex
with calcium hydroxide did encourage apical closureby cementum deposition. Closure was also observedin the control groups (5%) and in Kerr Pulp CanalSealer groups (10%), but was associated with dentinchips that also stimulate cementum formation. BothSealapex and Kerr Pulp Canal Sealer, when overex-tended, provoke a chronic inflammatory reaction inthe periodontal ligament (PDL).
Apexit (Ivoclar Vivadent, Schaan, Liechtenstein) isa calcium hydroxide sealer with salicylates also incor-porated into the formula.
CRCS (Calciobiotic Root Canal Sealer; Coltene/Whaledent/Hygenic, Mahwah, NJ) is a calcium hydroxide-containing sealer with a zinc oxide–eugenol–eucalyptolbase. CRCS is a rather slow setting sealer, especially indry or in humid climates. It may require up to 3 days tofully set.16 The set sealer is quite stable, which improvesits sealing qualities, but may mean that calcium hydro-xide is not as readily released, and the stimulation ofcementum and bone formation may be severely limited.
Beltes et al.199 did an in vitro evaluation of cyto-toxicity of calcium hydroxide-based root canal sealers.Sealapex was the most cytotoxic, followed by CRCS,with Apexit being the least cytotoxic with the leastdecrease in cell density.
Siqueira et al.200 investigated the sealing ability, pH,and flow rate of three calcium hydroxide-based sealers(Sealapex, Sealer 26, and Apexit). There was no sig-nificant difference found between apical sealing abilityand dye penetration. All calcium hydroxide sealersalkalinized adjacent tissues. Sealer 26 had significantlysuperior flow characteristics. They concluded calciumhydroxide sealers compare favorably with zinc oxideand eugenol (ZOE) cements for use in obturation.
Vitapex (NEO Dental International, Inc, FederalWay, WA) is a sealer, which was developed in Japan,and contains, not only calcium hydroxide, but also 40%iodoform and silicone oil among other ingredients.
Resin Sealers
Epoxy resin sealers have an established record inendodontics, especially in the form of AH 26 and itssuccessor AH Plus (Dentsply International, York, PA).
AH 26 (Dentsply International/Maillefer) is a bis-phenol epoxy resin sealer that uses hexamethylenete-tramine (methenamine) for polymerization and hasbeen used for many years as a sealer.101,201 The methe-namine will give off some formaldehyde as it sets, andthis has been one of its major drawbacks. The highestamount of formaldehyde release is in the freshlymixed sealer, and the amount of formaldehyde
Chapter 29 / Root Canal Filling Materials / 1035

released goes down after 48 hours, and after 2 weeksthe amount released is insignificant.202 The amount offormaldehyde produced during the setting process hasbeen reported to be several thousand times lower thanthe long-term release from formaldehyde-containingsealers such as N2.86,201 Other disadvantages are stain-ing and an extended working time. On the otherhand, AH 26 does not seem to be affected by moist-ure, and will even set under water.16
AH Plus and ThermaSeal Plus (Dentsply Interna-tional) (Figure 11) were formulated with a mixture ofamines that would allow for polymerization without theunwanted formation of formaldehyde,201,203 but with allthe advantages of AH 26, such as increased radiopacity,low solubility, slight shrinkage, and tissue compatibility.AH Plus is an epoxy–bis-phenol resin that also containsadamantine.101 AH Plus comes as a two-paste system,unlike the liquid-powder system of AH 26. AH Plus hasa working time of 4 hours and a setting time of 8 hours.Other improvements over the older AH 26 formulationare the thinner film thickness and the decreased solubi-lity of AH Plus, both about half that of AH 26. AHPlus has been shown to be less cytotoxic than AH 26,but both caused a dose-dependent increase ingenotoxicity.176
Epiphany (Pentron Clinical Technologies) or Real-Seal (Sybron Endo) is a sealer that contains urethanedimethacrylate (UDMA), Poly(ethylene glycol)dimethacrylates (PEGDMA), ethoxylated bisphenolA-dimethacrylate (EBPADMA), Bisphenol-A-glycidyl-dimethacrylate (BisGMA) resins designed for use withthe polycaprolactone core materials. Additionally,these sealers contain silane-treated barium borosi-licate glass, barium sulfate, silica, calcium hydroxide,bismuth oxychloride with amines, peroxide, a photoinhibitor, and pigments. Epiphany sealer is a dual-curedental resin composite sealer that self-cures in about25 minutes. It comes with a self-etch primer with
sulfonic acid-terminated functional monomer, Hydro-xyethylmethacrylate (HEMA), water, and polymeriza-tion initiator. Sodium hypochlorite may negativelyaffect bond strength of the primer, so after usingsodium hypochlorite for irrigation, one should irrigatewith ethylenediaminetetraacetic acid (EDTA) and ster-ile water. Peroxide-containing lubricants might alsohave a retarding effect on the resins, so a final rinsewith EDTA and sterile water is recommended afterusing these lubricants. Chlorhexidine does not affectthe bond strength. When obturation is completed, thecoronal surface may be light-cured for 40 seconds tocreate a coronal seal.
In a study comparing Epiphany sealer with AH Plusand EndoREZ sealers for intraosseous biocompatibilityfor 4 and 12 weeks, as recommended by the TechnicalReport 9 of the Federation Dentaire Internationale(FDI), Sousa et al.204 found the inflammatory tissuereaction to EndoREZ was severe and the AH Plusinflammatory reaction went from severe to moderatewith time, whereas Epiphany showed biological com-pataibility in regard to bone formation, and it alsoproduced either no, or very slight inflammation.
In a direct comparison of physical and chemicalproperties of AH Plus and Epiphany sealers, Versianiet al.205 found there was no significant difference inflow or film thickness between AH Plus and Epiphanysealers. There was a statistical difference between thetwo with the solubility of Epiphany being 3.41% ver-sus 0.21% for AH Plus, and for dimensional stability,there was also a statistical difference with AH Plusexpanding 1.3% on setting and Epiphany expanding8.1% following setting. The setting time, flow, andfilm thickness tests for both cements conformed toAmerican National Standards Institute (ANSI)/ADAstandards. Dimensional alteration tests for both sea-lers were greater than values considered acceptable byANSI/ADA standards, and the values for Epiphanysealer with regard to solubility were also greater thanvalues considered acceptable by ANSI/ADA.
Ungor et al.206 evaluated the push-out bond strength ofthe Epiphany–Resilon root canal filling system with thebond strengths of different pairings of AH Plus, gutta-percha, Epiphany, and Resilon. Their results showed thatEpiphany with gutta-percha had significantly greaterbond strength than all the other groups. There was nosignificant difference between the Epiphany with Resiloncombination and the AH Plus with gutta-percha. Inspec-tion of the surfaces revealed the bond failure to be mainlyadhesive to dentin for all groups.
Diaket (3M/ESPE, Minneapolis, MN) has been apopular sealer in Europe for many years and is a
Figure 11 AH Plus Root Canal Sealer by Tulsa Dentsply is a resin typesealer shown here in a mixing syringe. Reproduced with permission of TulsaDentsply.
1036 / Endodontics

polyketone compound containing vinyl polymersmixed with zinc oxide and bismuth phosphate.86
Diaket is a sealer that sets by chelation, but it containspolyvinyl chloride in polymer form as a main ingre-dient.101 It has a liquid component of B-diketone. It isa tacky material that contracts upon setting, but this isoffset by its absorption of water.16 It has done well inin-vitro tests, including biocompatibility studies.101
Studies have shown that after initial mild tissue reac-tions, and after longer times of 2 weeks or more, thereseems to be a decrease in tissue irritation.207–209
Ørstavik and Mjor210 reported that Diaket demon-strated good biocompatibility compared with othersealers.
Eldeniz et al.211 evaluated the shear bond strength ofthree resin-based sealers (Diaket, AH Plus, andEndoREZ) to dentin with and without the smear layer.Bond strength of root canal sealers to dentin is animportant property for the integrity of the sealing ofroot canals. A significant difference was found amongthe bond strength of the sealers, smear layer, and con-trol groups. AH Plus sealer showed the highest bondstrength in smear layer-free surfaces, and had thestrongest bond to dentin with the smear layer intact.
Glass Ionomer-Based Sealers
There are currently no glass ionomer sealers beingmarketed. Ketac-Endo (3M, Minneapolis, MN) ismentioned here because it appears in many studiesas a comparative sealer.
Silicone-Based Sealers
Silicone-based sealers utilize the same qualities ascaulking compounds used in household constructionaround kitchen and bathroom structures providingadhesion, a moisture-resistant seal, and stability.101
Lee Endo-Fill (Lee Pharmaceuticals, El Monte, CA)is an example of a silicone-based root canal sealer.
RoekoSeal (Roeko/Coltene/Whaledent, Langenau,Germany) is a polyvinylsiloxane that is a white paste-like sealer.212 RoekoSeal is reported to polymerizewithout shrinkage and utilizes platinum as a catalyzingagent.101
Wu et al.213 reported a 1-year follow-up study onleakage, using a fluid transport model, of single-conefillings with RoekoRSA sealer. The apical filling in allroots did not show leakage either at 1 week or at1 year.
GuttaFlow (Roeko/Coltene/Whaledent) is a polyvi-nylsiloxane with finely milled gutta-percha particlesadded to the RoekoSeal sealer. GuttaFlow also con-tains silicone oil, paraffin oil, platin catalyst, zirco-nium dioxide, nano-silver as a preservative, and acoloring agent. It is eugenol free. It is a cold flowablegutta-percha filling system for the obturation of rootcanals. GuttaFlow is triturated in its cannula andpassively injected into the canal and then used withsingle or multiple gutta-percha points.
Solvent-Based Sealers
The use of chloroform or solvent-based sealers waspopularized by Johnston and Callahan.214 The tech-nique is still practiced today with various types ofchloroform sealers, including chloropercha andKloropercha N-Ø. Gutta-percha particles are addedto the chloroform to produce a sealer, which has thesame color as gutta-percha. The mixture can then beused as a sealer with gutta-percha points for obtura-tion of the canal. There is more shrinkage with thechloroform solvent techniques, and this often trans-lates into leakage, with the material pulling awayfrom the canal walls as it shrinks creating voidsthrough which leakage may occur.215
Chlororosin lateral condensation uses 5% to 8% rosinin chloroform, which leaves a very adhesive residue.
Chloropercha is white gutta-percha with chloroformand has no adhesive properties.
Kloropercha N-Ø contains additional resin, plusCanada balsam, that adds adhesive property to thematerial.
Urethane Methacrylate Sealers
EndoRez (Ultradent, South Jordon, UT) is a hydro-philic UDMA resin sealer that reportedly has goodcanal wetting and flow into dentinal tubules.212 Thehydrophilic property improves its sealing abilities, ifsome moisture is still in the canal at obturation.101
EndoRez is introduced into the canal with a narrow30-gauge Navitip needle (Ultradent). A single gutta-percha point technique or the lateral compactionobturation technique may be used.
EndoRez resin-coated gutta-percha is also mar-keted, which reportedly chemically bonds to theEndoRez sealer and works with all resin-based sealers.EndoRez points come in ISO standard sizes.
Chapter 29 / Root Canal Filling Materials / 1037

Tay et al.216 investigated the effectiveness ofobturating root canals with the polybutadiene–diisocyanate–methacrylate resin-coated gutta-percha(EndoREZ). This enables the polyisoprene in thegutta-percha to chemically couple with the metha-crylate-based resin sealer (EndoREZ). This studyexamined the effectiveness of using passively fittingresin-coated gutta-percha points with the dual-curedversion of EndoREZ sealer. It was found thatthe hydrophilic nature of the sealer enabled the crea-tion of an extensive network of 800 to 1200 mmlong sealer resin tags after removal of the endo-dontic smear layer. Still there were interfacialgaps and silver leakage could be observed along thesealer–dentin interfaces. This was primarily attribu-ted to polymerization shrinkage of the sealer. Gapsand silver leakage was also seen between the resin-coated gutta-percha and the sealer.
The shear strength of EndoREZ to resin-coatedgutta-percha was examined, and it was also exam-ined whether shear strength is improved by creatingan oxygen inhibition resin layer via the applicationof a dual-cured dentin adhesive to resin-coatedgutta-percha.217 The authors concluded that in-situdentin adhesive application may be valuable inenhancing the coupling of resin-coated gutta-perchato methacrylate sealers.
A study of bone response to the methacrylate-basedsealer, EndoREZ, revealed, that at 10 days after place-ment, the amount of reactionary bone formation indirect contact with EndoREZ was significantly less thanthat observed with the controls, and the number ofinflammatory cells next to the EndoREZ sealer was sig-nificantly higher than the controls. However, after60 days, no differences were noted between the experi-mental and control groups. This indicated that the sealerproduces a response similar to that of many sealers.218
Zmener et al.219 looked at the apical seal produced withthe methacrylate-based sealer (EndoREZ) and Gross-man’s sealer. Three groups were evaluated. The firstcombination of materials and techniques was a singlegutta-percha point with the methacrylate sealer, the sec-ond was lateral compaction with the methacrylate sealer,and the third technique was gutta-percha with Gross-man’s sealer. The results demonstrated that the dye pene-tration in the two methacrylate sealer groups occurred atthe sealer–dentin or sealer–gutta-percha interface. In theGrossman’s sealer group, the dye leakage occurred atboth interfaces, and throughout the mass.
EZ Fill (Essential Dental Systems, South Hacken-sack, NJ) is a noneugenol epoxy resin sealer that isplaced with a bidirectional spiral, rotating in a hand-piece, and used with a single gutta-percha point tech-
nique. The spiral is designed to spread the sealerlaterally in the apical region of the canal. It is report-edly nonshrinking on setting and is hydrophobic innature, making it resistant to fluid degradation. Onestudy has shown EZ fill to seal as well as other tech-niques.220 Favorable clinical outcomes have also beenreported.212,222
MetaSEAL (Parkell, Inc., Edgewood, NY) marketedin the United States and Canada is a thinner versionof 4-Meta, used for years as a restorative sealer. Belliet al.223 compared MetaSEAL for leakage against Epi-phany/Real Seal and AH Plus and found it to showsignificantly lower leakage after the first week. After 4and 12 weeks, there was no significant differenceamong the groups. MetaSEAL’s self-etching formulahybridizes the canal wall preventing leakage andbonds to gutta-percha (Figure 12) and Resilon.
Paraformaldehyde-Containing Sealers
(Riebler’s)
Reibler’s paste is a paraformaldehyde-containing sea-ler and was discussed earlier under paraformaldehyde-containing paste materials.
Evaluation and Comparison of Sealers
Ørstavik101,224 has listed the various evaluation para-meters for testing endodontic sealers. They includetechnologic tests standardized by the ADA/ANSI inthe United States, and the ISO internationally. Thesetechnologic tests include flow, working time, setting
Figure 12 Micrograph showing hybrid bond between MetaSEAL andgutta-percha by penetration of the gutta-percha. Courtesy, Parkell.
1038 / Endodontics

time, radiopacity, solubility and disintegration, anddimensional change following setting. Additionally,biologic tests, usage testing, and antibacterial testingare useful. Clinical testing should be included toestablish outcomes of treatment.
LEAKAGEThe influence of root canal shape (curved or straight)on the sealing ability of sealers has been studied in afluid transport model.225 Canals were laterally com-pacted with gutta-percha with either Pulp Canal Sea-ler or Sealapex sealer. It was found that Sealapexallowed more leakage than Pulp Canal Sealer at 1 year.The authors concluded that canal form affects sealingability at 1 month, but the sealer affects the quality ofseal at 1 year.
The sealing ability of four sealers was evaluatedquantitatively by Cobankara et al.226 The sealers testedwere Rocanal, a zinc oxide–eugenol powder-liquidsystem; AH Plus, an epoxy resin-based sealer; Seala-pex, a calcium hydroxide-based sealer; and RC Sealer,an adhesive resin sealer. Apical leakage decreased gra-dually for all sealers from 7 to 21 days. Sealapexdemonstrated better apical sealing than the other sea-lers, and AH Plus, RC Sealer, and Rocanal all showedsimilar apical leakage at every time period.
Another in vitro study evaluated the apical leak-age, by a fluid filtration meter, of three root canalsealers, AH Plus, Diaket, and EndoREZ.227 Statisticalanalysis indicated that root canal fillings with Diaketin combination with the cold lateral compactiontechnique showed less apical leakage than the othertwo sealers.
Saleh et al.228 used the SEM and energy dispersivespectroscopy to evaluate the adhesion of sealers. Themicroscopic details of the debonded interfacesbetween endodontic sealers and dentin or gutta-percha were assessed in this study. Grossman’s sealer,Apexit, Ketac-Endo, AH Plus, RoekoSeal Automix,and RoekoSeal Automix with an experimental primerwere examined. After tensile bond strength testing,the morphologic aspects of the fractured surfaces wereassessed. The energy-dispersive spectroscopy success-fully traced sealer components to the debonded sur-faces. Some of the sealers penetrated into the dentinaltubules when the dentin surface had been pretreatedwith acids. However, these sealer tags remained,occluding the tubules after bond failure in someinstances only (Grossman’s sealer, RoekoSeal Auto-mix with an experimental primer, AH Plus/EDTA).Penetration of the endodontic sealers into the dent-inal tubules, when the smear layer was removed, wasnot associated with higher bond strength.
Pommel et al.229 examined the efficacy of four typesof sealers in obtaining an impervious apical seal, andto correlate those seals with their adhesive properties.Pulp Canal Sealer, Sealapex, AH 26, and Ketac-Endowere the sealers evaluated. The results showed thatteeth filled with Sealapex displayed higher apical leak-age than the other sealers. No statistically significantdifference was found between AH 26, Pulp CanalSealer, and Ketac-Endo. No correlation was foundbetween the sealing efficiency of the four sealers andtheir adhesive properties.
Lee et al.230 investigated the adhesion of endodonticsealers to dentin and gutta-percha. The bond strengthto the dentin of the four sealers gave the followingorder from lowest to highest: Kerr Sealer < Sealapex< Ketac-Endo < AH 26. The bond strengths to gutta-percha gave the following order from lowest to high-est: Ketac-Endo < Sealapex < Kerr < AH 26. The bondbetween the Kerr Sealer and dentin all failed adhe-sively, whereas the Sealapex bonds failed cohesively(80%). AH 26 demonstrated no adhesive failures. TheAH 26 gave the highest bond strength values to bothdentin and gutta-percha. These finding suggest thatthe resin may not only react with the collagen to formbonds but react with gutta-percha as well.
In another study, Tagger et al.231 showed AH 26had a significantly stronger bond to gutta-percha thanthe remaining five sealers, including Roth’s 801 andSealapex.
TISSUE TOLERANCEThe cytotoxicity of RoekoSeal Automix and AH Pluswas evaluated using human cervical carcinoma cells andmouse skin fibroblasts.232 AH Plus was significantlymore cytotoxic for both cell lines after 1 hour, 24 hours,and 48 hours, compared with the 7-day and 1-monthsetting periods. RoekoSeal had no cytotoxic effects oneither cell line at any setting time.
Spangberg and Pascon233 examined the cytotoxicityof seven endodontic sealers (Wach’s, Grossman’s,Tubli-Seal, AH 26, Nogenol, Diaket, and Endo-Fill).Evaluated as solid materials, Wach’s Sealer, Grossman’sSealer, Tubli-Seal, and Diaket were the most toxic.Nogenol was less toxic and the least toxic materialswere AH 26 and Lee Endo-Fill. When solubilized, how-ever, Grossman’s sealer, Tubli-Seal, and Endo-Fill hadvery low toxicity, Nogenol had low to medium toxicity,and AH 26, Diaket, and Wach’s sealers were very toxicas liquids.
Economides et al.234 investigated the biocompat-ibility of four root canal sealers (AH 26, Roth’s 811,CRCS, and Sealapex). Sealapex and Roth’s 811 sealers
Chapter 29 / Root Canal Filling Materials / 1039

caused moderate to severe inflammation reactions,whereas CRCS caused a mild to moderate reaction.AH 26 caused the greatest irritation initially, but thisinflammatory reaction decreased with time.
Bernath and Szabo235 examined tissue reactioninitiated by different sealers. The aim of this study wasto analyze the tissue reactions of the calcium hydroxidesealer, Apexit, and to compare it with the reactions ofsealers with different chemical compositions (Endo-methasone, AH 26, and Grossman’s sealer). When filledwithin the root, AH 26 and Endomethasone initiated amild lymphocytic/plasmocytic reaction in some cases.In the group of overfilled canals, all four sealers initiatedan inflammatory response: Endomethasone initiated aforeign body-type granulamatous reaction; AH 26 par-ticles were engulfed by macrophages; Apexit and Gross-man’s sealers initiated only a lymphocytic/plasmocyticreaction.
Huumonen and coworkers236 evaluated the healingof patients with apical periodontitis after endodontictreatment by comparing a silicone-based sealer(RoekoSeal Automix) and a zinc oxide-based sealer.After a 1-year follow-up, 199 teeth were assessed toevaluate their periapical status. The results of thestudy showed that there was no statistical differencebetween the success rates of the two study groups. Theoverall success rate at 12 months was 76%.
FLOWØrstavik224 rated the flow for Tubli-Seal to be greaterthan that of Kerr’s PCS, which was better than Diaketand Kloroperka NØ. He also stated that flow proper-ties may be affected by changes in the powder-to-liquid ratio.
The rheologic properties of Apexit, Tubli-SealEWT, Grossman’s sealer, and Ketac-Endo were testedin a capillary system by Lacey and coworkers.237
Tubli-Seal EWT had a thinner film thickness thanthe other sealers. Tubli-Seal EWT had lower viscosityand better flow than the other sealers. Increased strainrate gave a significant increase in the flow rate of allsealers. The reduction in powder-to-liquid ratio forGrossman’s sealer significantly increased flow in nar-row tubes, and at a higher strain rate. Increasing therate of insertion gave increased volumetric flow andtherefore a reduced viscosity for all sealers. As theinternal width of the canals was reduced, there was areduction in volumetric flow and therefore anincreased viscosity.
McMichen et al.238 did a comparative study ofselected physical properties of five root canal sealers.This study sought to investigate the physical proper-
ties of five sealers: Roth’s 801, Tubi-Seal EWT, AHPlus, Apexit, and Endion. Solubility in water, filmthickness, flow, working time, and setting time weretested. AH Plus had the greatest stability in solution.But AH Plus also had the greatest film thickness. Flowrates were similar, and the working times for all weregreater than 50 minutes. Setting time for Roth’s 801was 8 days.
Tagger et al.239 studied the interaction betweensealers and gutta-percha cones. AH 26 silver-free hada notable softening effect on most gutta-perchabrands, resulting in increased flow. Liquid (bisphenolepoxy resin) and chemical-bond formation could actas partial solvent effect of the resin. Eugenol has asolvent effect on gutta-percha. The combination ofApexit and UDM gutta-percha cones (United DentalManufacturers, Zipperer, VDW, Munich, Germany)gave the greatest penetration in lateral canals. Under-standing the interaction between gutta-percha andsealers may serve as a guide for using the most sui-table combination for specific clinical cases. A toothwith a wide apical foramen should be filled with acombination that provides little flow; conversely,canals with very fine apical foramina and internalirregularities should be filled with a more fluid com-bination.
SETTING TIMEThe setting time for 11 sealers was determined in bothaerobic and anaerobic environments by Nielsenet al.240 Kerr Tubli-Seal and Ketac-Endo were thefastest sealers to set under aerobic environments, andKetac-Endo and Resilon sealer (Epiphany) were thefastest sealers to set under anaerobic environments.Roth’s 801 and Roth’s 811 sealers were the slowestsealers to set under both aerobic and anaerobic envir-onments, taking over 3 weeks to set. Resilon sealer(Epiphany) set in 30 minutes under anaerobic condi-tions, but in the presence of air, Resilon sealer (Epi-phany) took a week to set, and an uncured layerremained on its surface.
WORKING TIMEØrstavik224 stated that the assessment of working timeis preferably done with measurements of flow as afunction of time. It is the time from the start ofmixing to the point at which the flow has beenreduced to 90% of the initial flow measurement. Theworking time for zinc oxide–eugenol sealers demon-strated an initial increase in flow, followed by a laterreduction in flow.
1040 / Endodontics

SOLUBILITYThe zinc oxide sealers and the calcium hydroxidesealers appear to have greater solubility than othersealers.197,241–243
Schafer and Zandbiglari244 studied the solubility ofroot canal sealers in water and artificial saliva. Thesealers examined were (epoxy resin [AH 26, AH Plus],silicone [RSA RoekoSeal], calcium hydroxide [Apexit,Sealapex], zinc oxide–eugenol [Aptal-Harz], glassionomer [Ketac-Endo], and a polyketone-based sealer[Diaket]). Most sealers were of low solubility, althoughSealapex, Aptal-Harz, and Ketac-Endo showed amarked weight loss in all liquids. Even after 28 daysof storage in water, AH 26, AH Plus, RSA RoekoSeal,and Diaket showed less than 3% weight loss. AH Plusshowed the least weight loss of all sealers tested, inde-pendent of the solubility medium used. Sealapex,Aptal-Harz, and Ketac-Endo had a marked weight lossin all liquids.
DIMENSIONAL CHANGE FOLLOWINGSETTINGKazemi et al.245 examined the long-term comparisonof the dimensional changes of four sealers, ZnOE, AH26, Endo-Fill, and Endomethasone. The two zincoxide and eugenol sealers started to shrink withinhours after mixing. The first volumetric loss for AH26 and Endo-Fill was recorded after 30 days. The leastdimensional change at any time period was observedfor Endo-Fill. Significant dimensional change andcontinued volume loss can occur in some endodonticsealers. The setting times for Endo-Fill, ZnOE, Endo-methasone, and AH 26 were 2.5, 4, 9, and 12 hours,respectively. Endo-Fill and AH 26 had lower rates ofsolubility, water sorption, and dimensional changethan ZnOE and Endomethasone over 180 days.
ANTIBACTERIAL ACTIVITYThe in vitro antibacterial activity of Fill Canal (zincoxide based sealer), Sealapex, Sealer 26, Apexit, andcalcium hydroxide against various species of micro-organisms was studied.246 Fill Canal demonstratedlarge zones of inhibition against all bacteria tested.Sealer 26 was not effective against Porphyromonasendodontalis or Porhyromonas gingivalis. Sealapexand calcium hydroxide showed similar effects againstthe various bacteria, being effective against Actino-myces israelii, and Actinomyces naeslundii. Sealapexwas not effective against Staphylococcus aureus, butcalcium hydroxide was effective against Staphylococcusaureus. Apexit was not effective against any of themicroorganisms tested.
An in vitro antibacterial activity study of four rootcanal sealers tested AH Plus, Endomethasone, PulpCanal Sealer, and Vcanalare, a zinc oxide and ortho-phenylphenol containing sealer.247 All of the freshlymixed sealers showed complete inhibition of bacterialgrowth. Similar results were obtained after 24 hours,with the exception of AH Plus. Vcanalare was the onlysealer still inhibiting bacterial growth 7 days aftermixing.
The amount of bacterial endotoxin penetrationthrough root canals obturated either with cold lateralcompaction or with a continuous wave techniquewith backfill of thermoplasticized gutta-percha, witheither Roth’s 801 sealer or AH 26 sealer, was evaluatedby Williamson et al.248 The groups differed signifi-cantly. Thermoplasticized gutta-percha with Roth’s801 sealer permitted the least amount of endotoxinpenetration, suggesting that the Roth’s 801 sealer mayhave a role in inhibiting endotoxin penetration intoobturated root canals.
Siqueira and Goncalves249 found that zincoxide–eugenol sealers inhibited all the bacteria testedin their study. Sealer 26, the epoxy resin containingcalcium hydroxide, was inhibitory on most strains ofbacteria tested, but not against Porphyromonas endo-dontalis and Porphyromonas gingivalis. Sealapex hadlow antibacterial activity.
Leonardo et al.250 examined the antimicrobialactivity of four root canal sealers (AH plus, Sealapex,Ketac-Endo, and Fill Canal), two calcium hydroxidepastes (Calen and Calasept), and a zinc oxide pasteagainst seven bacterial strains. All sealers and pastespresented in vitro antimicrobial activity for all bacter-ial strains after a 24-hour incubation period at 37�C.
Kayaoglu et al.251 tested short-term antibacterialactivity of root canal sealers toward E. faecalis.E. faecalis suspensions were exposed to freshly mixedsealers (MCS [Medidenta International, Inc.], AH Plus,Grossman’s, Sealapex, Apexit). MCS contains iodo-form. MCS, AH Plus, and Grossman’s sealer signifi-cantly reduced the number of viable bacteria in bothtests. Sealapex and Apexit were not statistically differentfrom the controls. MCS, AH Plus, and Grossman’ssealer were effective in reducing the number of cultiva-ble cells of E. faecalis. Calcium hydroxide-based sealers,Sealapex and Apexit, were ineffective in this short-termexperiment.
Intraorifice Barriers
The prevention of coronal bacterial leakage back intothe root canal system is crucial for the ultimate
Chapter 29 / Root Canal Filling Materials / 1041

success of endodontic therapy. Several studies haveshown that leakage can occur through the obturatedroot canal system in a relatively short time per-iod.252–255 The issue of coronal leakage and its effecton endodontic outcomes has been investigated.Whereas some authors feel that the quality of theendodontic obturation is a more important factorthan the quality of the coronal restoration,256–258
others feel that preventing coronal microleakage canplay a significant role in the success of endodontictherapy.259 In any event, the placement of anotherbarrier to the penetration of microorganisms intothe obturated root canal system would seem to pre-vent leakage due to delay in placement of a permanentrestoration or leakage from failed or inadequate cor-onal restorations. Several studies have looked at mate-rials that may be used as intraorifice barriers placed1 to 2 mm into the orifice of canals, or on thepulpal floor, to add another layer to prevent micro-leakage.129,260–268
COMPOSITE RESINSYamauchi et al.,269 in a dog study, examined the effectof an orifice plug of 2 mm of IRM or a dentin bond-ing/composite resin on coronal leakage of teeth thathad canals obturated with gutta-percha and the accesscavities left open for 8 months. Periapical inflamma-tion was observed in 89% of the group without plugs,but in those with composite plugs only 39% hadperiapical inflammation and only 38% in the IRM-plugged group.
An investigation, comparing Cavit, against a flow-able light-cured composite resin (Tetric), and MTA(ProRoot) as intraorifice barriers at 1, 2, 3, or 4 mmin canals obturated with gutta-percha, demonstrated abetter seal with the flowable composite than witheither MTA or Cavit.270
GLASS IONOMERSChailertvanitkul et al.261 investigated coronal bacterialleakage, through coronal access using Vitrebond(3M), a resin-modified glass ionomer liner, as a bar-rier on the pulpal floor. The teeth with the Vitrebondliner that had been placed on the pulpal floor showedno leakage of bacteria, whereas 60% of the specimenswithout a Vitrebond liner showed leakage after 60days.
Wolcott et al.260 found that there was no significantdifference between Vitrebond, a colored trial GCAmerica glass ionomer, and Ketac-Bond. There wassignificantly less coronal leakage when the glass iono-mers were used than when no barrier was placed.
Maloney et al.267 found that thermocycling Triage(GC America, Inc.), a colored resin-modified glassionomer, had no effect on the seal produced by Triage,when it was used as an intraorifice barrier at depths of1 or 2 mm. The 1 and 2 mm intracoronal barriersignificantly reduced coronal microleakage comparedwith no barrier placement.
Mavec et al.271 investigated the use of a glass iono-mer barrier against bacterial leakage a when post spaceis required. They found that a 1 mm barrier of glassionomer over as little as 2 or 3 mm of gutta-perchacould reduce the risk of recontamination of the apicalgutta-percha. This could be beneficial in cases wherethere is a minimum amount of root length for a post.
OTHER MATERIALSPisano et al.262 compared Cavit, IRM, and Super EBAas intraorifice barriers to prevent coronal microleak-age and found that all three groups leaked less thanthose obturated canals that did not receive a barrier.
Wolanek et al.265 tested the effectiveness of a den-tin-bonding agent used as an intraorifice barrier andfound that it reduced coronal bacterial leakage.
Galvan et al.264 evaluated Amalgbond Plus, C&BMetabond, One-Step Adhesive with Eliteflo composite,One-Step Dentin Adhesive with Palfique composite,and IRM as intracoronal barriers. At 7 days, theIRM, AEliteflo, and Palfique composite leaked signifi-cantly more than Amalgabond or C&B Metabond.Amalgabond consistently produced the best sealthrough all time periods.
Temporary Filling Materials
The problem of coronal leakage is also important inthe choice of an interim restoration material to sealoff the access preparation, either between appoint-ments or before the endodontically treated toothreceives a permanent restoration.
Cavit (ESPE, Seefeld, Germany), in a number ofstudies, has been found to prevent leakage, when usedas a temporary filling material to close access prepara-tions, either as an interim filling material or afterfinal obturation before a permanent restoration isplaced.272–280 Cavit is premixed and is easily intro-duced into the access cavity, as well as being easy toremove from the access cavity at the subsequentappointment. The ingredients in Cavit are zinc oxide,calcium sulfate, zinc sulfate, glycoacetate, polyvinyl-acetate resin, polyvinylchloride-acetate, triethanol-amine, and red pigment.272 The calcium sulfate ishydrophilic and causes hydroscopic expansion of
1042 / Endodontics

Cavit. This absorption of moisture and subsequentexpansion cause Cavit to seal very well as it sets in amoist environment.
In a survey of Diplomates of the American Board ofEndodontics, Vail and Steffel281 found that Cavit wasthe temporary restoration of choice for both anteriorand posterior teeth.
Webber et al.282 found that to seal adequately, Cavitmust have a depth of at least 3.5 mm.
The ability of Cavit to prevent bacterial penetrationinto root canals containing four medicaments wasevaluated.283 The medicaments were calcium hydro-xide, chlorhexidine, an antibiotic-corticoid compound(Ledermix), and chloromono-campherphenolic com-pound (ChKM). The authors found that Cavit pro-longed the protection of all the medicaments from13 to 18 days but that an adequate seal could not beprovided for more than 1 month.
Balto274 assessed microbial leakage of three tempor-ary filling materials (Cavit, IRM, and Dyract). IRMbegan to leak after 10 days, whereas Cavit and Dyractdid not leak until after 2 weeks.
After 3 weeks, Beach et al.273 found that 4 of 14TERM samples and 1 of 18 IRM samples leaked andshowed positive bacterial growth. None of the Cavitsamples in the study leaked. It was shown that Cavitprovided a significantly better seal than the othertemporary filling materials.
Kazemi and coworkers277 found that Tempit (Cen-trix, Milford, CT) and IRM (Dentsply International/L.D. Caulk Division, Milford, DE) seemed less appro-priate as an interim endodontic restoration than Cavitbased on an assessment of marginal stability andpermeability to dye penetration.
IRM is a temporary filling material that comesin a liquid-powder form that requires mixing. It is apolymer-resin-reinforced zinc oxide–eugenol mate-rial. Although many studies show it has inferiorsealing abilities compared with Cavit, in clinical situa-tions, however, which require greater bulk andresistance to occlusal forces, IRM may be used as atemporary restorative material. Zinc oxide and euge-nol materials, such as IRM, possess about double thecompressive strength value of Cavit.284 Glass ionomercements or composite resins may also be used in thesesituations and may have better sealing ability andgreater compressive strength.
The antibacterial properties of several temporaryfilling materials were examined. Revoltek LC (GC Cor-poration, Tokyo, Japan), Tempit (Centrix), Systempinlay (Vivadent, Schaan, Liechtenstein), and IRM weretested against Streptococcus mutans and E. faecalis. Sys-temp inlay exhibited antibacterial properties when in
contact with S. mutans for at least 7 days, whereasTempit and IRM sustained this ability for at least 14days. When in contact with E. faecalis, Tempit andIRM were antibacterial immediately after setting, andIRM sustained this activity for at least 1 day.285
Zmener et al.286 found no statistically significantdifference in the marginal leakage between Cavit,IRM, and Ultratemp Firm after thermocycling. All ofthe materials leaked at the interface of the materialwith the dentin, and some of the IRM specimensabsorbed the dye into the bulk of the material.
Orahood et al.287 found there was no difference inmarginal leakage between Cavit and ZOE when usedto seal access preparations through either alloy orcomposite restorations. One study found IRM morewatertight than Fermit-N or Cavit G intermediaterestorative materials.288
TERM (Dentsply International/L.D. Caulk Divi-sion) is a composite resin interim restorative materialfor endodontics. It is a visible-light-cured resin con-taining UDMA polymers, inorganic radiopaque filler,pigments, and initiators.272
Seiler289 studied bacterial leakage of three glassionomers, IRM, and Cavit as used as a temporaryendodontic restorative material. Cavit provided aslightly better seal than IRM; however, the glass iono-mer and resin-modified glass ionomer materials pro-vided better seals against bacteria than either IRM orCavit. If 3.5 mm of space does not exist for a tem-porary filling material, Hansen and Montgomery290
found that TERM may provide a superior temporaryrestoration. They found that TERM provides an ade-quate seal at 1, 2, 3, and 4 mm.
Summary
As new materials are introduced to fill the root canalsystem, it is important to remember Grossman’stenets and to remember the proven success of manyof the materials currently in use. However, there stillis a need to constantly improve what we can offer ourpatients, and to improve the outcome of endodontictreatment, in order to preserve the natural dentition.Long-term randomized clinical trials are needed on allthe materials, new and time tested, which are used inmodern-day endodontics.
With advances in materials and other aspects ofendodontics, one cannot imagine materials that willbe available to use in root canal systems in the future.They, no doubt, will be much more biocompatibleand, one might hope, may promote regeneration oftissues within the tooth and bone.
Chapter 29 / Root Canal Filling Materials / 1043

References
1. Grossman LI. Endodontics 1776–1976: a bicentennial his-tory against the background of general dentistry. J Am DentAssoc 1976;93:78–87.
2. Milas VB. History. In: Cohen S, Burns RC, editors. Pathwaysof the pulp. 2nd ed. St. Louis: C V Mosby Company; 1980,pp. 687–701.
3. Keane HC. A century of service to dentistry. Philadelphia:S.S. White Dental Manufacturing Co.; 1944.
4. Grossman LI. Root canal therapy. Philadelphia: Lea &Febiger; 1940.
5. Brownlee WA. Filling of root canals in recently devitalizedteeth. Dominion Dent J 1900;12(8):254.
6. Seltzer S, Green DB, Weiner N, DeRensis F. A scanning EMexamination of silver cones removed from endodonticallytreated teeth. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1972;33:589–605.
7. Brady JM, Del Rio CE. Corrosion of endodontic silver conesin humans: a scanning electron microscope and x-raymicroprobe study. J Endod 1975;1:205–10.
8. Goldberg F. Relationship between corroded silver points andendodontic failure. J Endod 1981;7:224–7.
9. Gutierrez JH, Villena F, Gigoux C, Mujica F. Microscopeand scanning electron microscope examination of silverpoints corrosion caused by endodontic materials. J Endod1982;8:301–11.
10. Kehoe JC. Intracanal corrosion of a silver cone producinglocalized argyria. J Endod 1984;10:199–201.
11. Goodman A, Schilder H, Aldrich W. The thermomechanicalproperties of gutta-percha. II. The history and molecularchemistry of gutta-percha. Oral Surg Oral Med Oral PatholOral Radiol Endod 1974;37(6):954–61.
12. Costa GE, Johnson JD, Hamilton RG. Cross-reactivity stu-dies of gutta-percha, gutta-balata, and natural rubber latex(Hevea brasiliensis). J Endod 2001;27(9):584–7.
13. Friedman CM, Sandrik JL, Heuer MA, Rapp GW. Composi-tion and mechanical properties of gutta-percha endodonticpoints. J Dent Res 1975;54(5):921–5.
14. Moorer WR, Genet JM. Evidence for antibacterial activity ofendodontic gutta-percha cones. Oral Surg Oral Med OralPathol Oral Radiol Endod 1982;53:503–7.
15. Martin H, Martin TR. Iodoform gutta-percha: MGP a newendodontic paradigm. Dent Today 1999;18:76.
16. Ingle JI, Newton CW, West JD, et al, editors. Obturation ofthe radicular space. In: Ingle JI, Bakland LK, editors. Endo-dontics. 5th ed. Hamilton, London: BC Decker, Inc.; 2002,pp. 571–668.
17. Chogle S, Mickel AK, Huffaker SK, Neibaur B. An invitro assessment of iodoform gutta-percha. J Endod2005;31:814–16.
18. Holland R, Murata SS, Dezan E, Garlipp O. Apical leakageafter root canal filling with an experimental calcium hydro-xide gutta-percha point. J Endod 1996;22:71–3.
19. Lin S, Levin L, Weiss EI, et al. In vitro antibacterial efficacyof a new chlorhexidine slow-release device. Quintessence Int2006;37(5):391–4.
20. Podbielski A, Boeckh C, Haller B. Growth inhibitory activityof gutta-percha points containing root canal medications oncommon endodontic bacterial pathogens as determined byan optimized in vitro assay. J Endod 2000;26:398–403.
21. Melker KB, Vertucci FJ, Rojas MF, et al. Antimicrobialefficacy of medicated root canal filling materials. J Endod2006;32(2):148–51.
22. Bunn CW. Molecular structure of rubber-like elasticity. PartI: The crystal structure of gutta-percha, rubber and poly-chloroprene. Proc R Soc Lond B Biol Sci 1942;80:40.
23. Baterman L. The chemistry and physics of rubber-like sub-stances. London: McLaren & Sons, Ltd; 1963.
24. Marciano J, Michailesco P, Abadie MJ. Stereochemical struc-ture characterization of dental gutta-percha. J Endod1993;19(1):31–4.
25. Arvanitoyannis I, Kokokuris I, Blanshard JMV, Robinson C.Study of the effect of annealing, draw ratio, and moistureupon the crystallinity of native and commercial gutta-percha(transpolyisoprene) with DSC, DMTA, and x-rays: determi-nation of the activation energies of T. Appl Polymer Sci1993;48:987.
26. Schilder H, Goodman A, Aldrich W. The thermomechanicalproperties of gutta-percha. 3. Determination of phase transi-tion temperatures for gutta-percha. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1974;38(1):109–14.
27. Schilder H, Goodman A, Aldrich W. The thermomechanicalproperties of gutta-percha. I. The compressibility of gutta-percha. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1974;37(6):946–53.
28. Sorin SM, Oliet S, Pearlstein F. Rejuvenation of aged (brittle)endodontic gutta-percha cones. J Endod 1979;5(8):233–8.
29. Kolokruis I, Arvanitoyannis I, Robinson C, Blanchard JM.Effects of moisture and aging on gutta-percha. J Endod1992;18:583–8.
30. Senia ES, Marraro RV, Mitchell JL, et al. Rapid sterilizationof gutta-percha cones with 5.25% sodium hypochlorite.J Endod 1975;1(4):136–40.
31. Short RD, Dorn SO, Kuttler S. The crystallization of sodiumhypochlorite on gutta-percha cones after the rapid-steriliza-tion technique: an SEM study. J Endod 2003;29(10):670–3.
32. Valois CR, Silva LP, Azevedo RB. Structural effects ofsodium hypochlorite solutions on gutta-percha cones:atomic force microscopy. J Endod 2005;31:749–51.
33. Gomes BP, Vianna ME, Matsumoto CU, et al. Disinfectionof gutta-percha cones with chlorhexidine and sodium
1044 / Endodontics

hypochlorite. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2005;100:512–17.
34. Yee FS, Marlin J, Krakow AA, Gron P. Three dimensionalobturation of the root canal using injection-molded thermo-plasticized dental gutta-percha. J Endod 1977;3:168–74.
35. Tani-Ishii N, Teranaka T. Clinical and radiographic evalua-tion of root-canal obturation with Obtura II. J Endod2003;29:739–42.
36. Eriksson AR, Albrektsson T. Temperature threshold levelsfor heat-induced bone tissue injury: A vital-microscopicstudy in the rabbit. J Prosthet 1983;50:101–7.
37. Weller RN, Koch KA. In vitro radicular temperature pro-duced by injectable-thermoplasticized gutta-percha. IntEndod J 1995;28:86–90.
38. Gutmann JL, Rakusin H, Powe R, Bowles WH. Evaluation ofheat transfer during root canal obturation with thermoplas-ticized gutta-percha. Part II: In vivo response to heat levelsgenerated. J Endod 1987;13:441–8.
39. Sweatman TL, Baumgartner JC, Sakaguchi RL. Radiculartemperature associated with thermoplasticized gutta-percha.J Endod 2001;27:512–15.
40. Lipski M. In vitro infrared thermographic assessment of rootsurface temperatures generated by high-temperature ther-moplasticized injectable gutta-percha obturation technique.J Endod 2006;32:438–41.
41. Michanowicz A, Czonstkowsky M. Sealing properties ofan injection-thermoplasticized low-temperature (70�C)gutta-percha: a preliminary study. J Endod 1984;10:563–6.
42. Lipski M. Root surface temperature rises in vitro during rootcanal obturation using hybrid and Microseal techniques.J Endod 2005;31:297–300.
43. Maggiore F. MicroSeal systems and modified technique.Dent Clin North Am 2004;48:217–64.
44. Cathro PR, Love RM. Comparison of MicroSeal and System B/Obtura II obturation techniques. Int Endod J 2003;36:876–82.
45. Johnson WB. A new gutta-percha filling technique. J Endod1978;4:184.
46. Gutmann JL, Saunders WP, Saunders EM, Nguyen L. Anassessment of the plastic thermafil obturation technique.Part 1: Radiographic evaluation of adaptation and place-ment. Int Endod J 1993;26:173–8.
47. Gutmann JL, Saunders WP, Saunders EM, Nguyen L. Anassessment of the plastic thermafil obturation technique.Part 2: Material adaptation and sealability. Int Endod J1993;26:179–83.
48. Becker TA, Donnelly JC. Thermafil obturation: a literaturereview. Gen Dent 1997;45:46–54.
49. Bhambhani SM, Sprechman K. Microleakage comparison ofThermafil vs vertical condensation using two different sea-lers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1994;78:105–8.
50. Dalat DM, Spangberg LSW. Comparison of apical leakagein root canals obturated with various gutta-percha techni-ques using a dye vacuum tracing method. J Endod 1994;20:315–19.
51. Dummer PMH, Lyle L, Rawle J, Kennedy JK. A laboratorystudy of root fillings in teeth obturated by lateral condensa-tion of gutta-percha or Thermafil obturators. Int Endod J1994;27:32–8.
52. Felstead AM, Lumley PJ, Harrington E. An in vitro investi-gation of Thermafil obturation at different temperatures.Endod Dent Traumatol 1994;10:141–3.
53. Hata G, Kawazoe S, Toda T. Sealing ability of various ther-moplastic techniques. J Endod 1993;19:207–10.
54. Hata G, Kawazoe S, Toda T, Weine FW. Sealing ability ofThermafil with and without sealer. J Endod 1992;18:322–6.
55. Lares C, ElDeeb ME. The sealing ability of the Thermafilobturation technique. J Endod 1990;16:474–9.
56. Clark DS, ElDeeb ME. Apical sealing ability of metal versusplastic carrier Thermafil obturators. J Endod 1993;19:4–9.
57. Fabra-Campos H. Experimental apical sealing with a newcanal obturation system. J Endod 1993;19:71–5.
58. McMurtrey LG, Krell KV, Wilcox LR. A comparisonbetween Thermafil and lateral condensation in highly curvedcanals. J Endod 1992;18:68–71.
59. Dummer PMH, Kelly T, Meghji A, et al. An in vitro study ofthe quality of root fillings in teeth obturated by lateralcondensation of gutta-percha or Thermafil obturators. IntEndod J 1993;29:99–105.
60. Scott AC, Vire DE, Swanson R. An evaluation of the Ther-mafil endodontic obturation technique. J Endod 1992;18:340–3.
61. Juhlin JJ, Walton RE, Dovgan JS. Adaptation of Thermafilcomponents to canal walls. J Endod 1993;19:130–5.
62. Taylor JK, Baumgardner KR, Walton RE. Comparison of thecoronal leakage in lateral condensation and Thermafilobturations [abstract]. J Endod 1991;17:195.
63. Baumgardner KR, Taylor J, Walton RE. Canal adaptationand coronal leakage: lateral condensation compared to Ther-mafil. J Am Dent Assoc 1995;126(3):351–6.
64. Saunders WP, Saunders EM. Influence of smear layer on thecoronal leakage of Thermafil and laterally condensed rootfillings with a glass ionomer sealer. J Endod 1994;20:155–8.
65. Dalat DM, Spangberg LS. Effect of post preparation on theapical seal of teeth obturated with plastic Thermafil obtura-tors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1993;76:760–5.
66. Ravanshad S, Torabinejad M. Coronal dye penetration of theapical filling materials after post preparation. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1992;74:644–7.
67. Mattison GD, Hwang CL, Cunningham C, Pink FE. The effectof the post preparation on the apical seal in teeth filled withThermafil [abstract]. J Dent Res 1992;72:600.
Chapter 29 / Root Canal Filling Materials / 1045

68. McGinnity TL, Mueninghoff LA, Brandt RE. Obturationefficiency after post-space preparation: effect of obturationdiameter. J Dent Res 1990;69(176): Abstract 542.
69. Ricci ER, Kessler JR. Apical seal of teeth obturated by thelateral condensed gutta-percha, the Thermafil plastic, andThermafil metal obturator techniques after post-space pre-paration. J Endod 1994;20:123–6.
70. Rybicki R, Zillich R. Apical sealing ability of Thermafilfollowing immediate and delayed post-space preparations.J Endod 1994;20:64–6.
71. Saunders WP, Saunders EM, Gutmann JL, Gutmann ML. Anassessment of the plastic Thermafil obturation technique.Part 3: The effect of post-space preparation on the apicalseal. Int Endod J 1993;26:184–9.
72. Zuolo ML, Imura N, Fernandes Ferreira MO. Endodonticretreatment of Thermafil or lateral condensation obturationsin post-space prepared teeth. J Endod 1994;20:9–12.
73. Imura N, Zuolo ML, Kherlakian D. Comparison of endodon-tic retreatment of laterally condensed gutta-percha and Ther-mafil with plastic carriers. J Endod 1993;19:609–12.
74. Ibarrola JL, Knowles KI, Ludlow MO. Retrievability of Therma-fil plastic cores using organic solvents. J Endod 1993;19:417–18.
75. Wilcox LR. Thermafil retreatment with and without chloro-form solvent. J Endod 1993;19:563–6.
76. Wilcox LR, Juhlin JJ. Endodontic retreatment of Thermafil vs.lateral condensation gutta-percha. J Endod 1994;20:115–17.
77. Baker PS, Oguntebi BR. Effect of apical resection and reversefillings on Thermafil root canal obturations. J Endod1990;16:227–9.
78. Mock ES, Olson AK, DeWald EJ, Radke PK. Apicoectomyand retrofilling preparation of Thermafil obturators. GenDent 1993;41:471–3.
79. Weller RN, Kimbrough WF, Anderson RW. A comparisonof thermoplastic obturation techniques: adaptation to thecanal walls. J Endod 1997;23:703–6.
80. Robinson MJ, McDonald NJ, Mullally PJ. Apical extrusion ofthermoplasticized obturating material in canals instrumentedwith Profile 0.06 or Profile GT. J Endod 2004;30:418–21.
81. De-Deus G, Gurgel-Filho ED, Magalhaes KM, Coutinho-Filho T. A laboratory analysis of gutta-percha-filled areaobtained using Thermafil, System B and lateral condensa-tion. Int Endod J 2006;39:378–83.
82. Lipski M. Root surface temperature rises in vitro during rootcanal obturation with thermoplasticized gutta-percha on acarrier or by injection. J Endod 2004;30:441–3.
83. Jarrett IS, Marx D, Covey D, et al. Percentage of canals filledin apical cross sections—an in vitro study of seven obtura-tion techniques. Int Endod J 2004;37:392–8.
84. Shipper G, Trope M. An vitro microbial leakage of endo-dontically treated teeth using new and standard obturationtechniques. J Endod 2004;30:154–8.
85. Goldberg F, Massone EJ, Artaza LP. Comparison of thesealing capacity of three endodontic filling techniques.J Endod 1995;21:1–3.
86. Hauman CH, Love RM. Biocompatability of dental materialsused in contemporary endodontic therapy: a review. Part 2:Root canal filling materials. Int Endod J 2003;36(3):147–60.
87. Wolfson EM, Seltzer S. Reaction of rat connective tissue tosome gutta-percha formulations. J Endod 1975;1:395–402.
88. Tavares T, Soares IJ, Silveira NL. Reaction of rat subcuta-neous tissue to implants of gutta-percha for endodontic use.Endod Dent Traumatol 1994;10(4):174–8.
89. Pascon EA, Spangberg LS. In vitro cytotoxicity of root-canal-filling materials. Part 1: Gutta-percha. J Endod 1990;16:429–33.
90. Munaco FS, Miller WA, Everett MM. A study of long-termtoxicity of endodontic materials with use of an in vitromodel. J Endod 1978;4:151–7.
91. Sjogren U, Sundquist G, Nair PNR. Tissue reaction to gutta-percha particles of various sizes when implanted subcuta-neously in guinea pigs. Eur J Oral Sci 1995;103:313–21.
92. Holland R, DeSouza V, Nery MJ, et al. Reaction of ratconnective tissue to gutta-percha and silver points. A long-term histological study. Aust Dent J 1982;27:224–6.
93. Serene TP, Vesely J, Boackle R. Complement activation as apossible in vitro indication of the inflammatory potential ofendodontic materials. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1988;65:354–7.
94. Gazelius B, Olgart L, Wrangsjo K. Unexpected symptoms toroot filling with gutta-percha. A case report. Int Endod J1986;19:202–4.
95. Boxer MB, Grammer LC, Orfan N. Gutta-percha allergy in ahealthcare worker with latex allergy. J Allergy Clin Immunol1994;93:943–4.
96. Knowles II, Ibarrola JL, Ludlow MO, et al. Rubber latex allergyand the endodontic patient. J Endod 1994;24:760–2.
97. Kleier D, Shibilski K. Management of the latex hypersensitivepatient in the endodontic office. J Endod 1999;25:825–8.
98. Hamann C, Rodgers PA, Alenius H, et al. Cross-reactivitybetween gutta-percha and natural latex: assumption vs. rea-lity. J Am Dent Assoc 2002;133:1357–67.
99. Charous BL, Hamilton RG, Yunginger JW. Occupationallatex exposure: characteristics of contact and systemic reac-tions in 47 workers. J Allergy Clin Immunol 1994;94:12–18.
100. Yunginger JW. Natural rubber latex allergy. In: MiddletonEM, Jr., Ellis EF, Yunginger JW, et al, editors. Allergy:principles and practice. 5th ed. St Louis: Mosby Year Book;1998, pp. 1073–18.
101. Ørstavik D. Materials used for root canal obturation: technical,biological and clinical testing. Endod Topics 2005; 12:25–38.
102. Miner MR, Berzins DW, Bahcall JK. A comparison of ther-mal properties between gutta-percha and a synthetic
1046 / Endodontics

polymer based root canal filling material (Resilon). J Endod2006;32:683–6.
103. Nielsen BA, Baumgartner JC. Spreader penetration duringlateral compaction of Resilon and gutta-percha. J Endod2006;32:52–4.
104. Shipper G, Ørstavik D, Teixeira FB, Trope M. An evaluationof microbial leakage in roots filled with a thermoplasticsynthetic polymer-based root canal filling material (Resilon).J Endod 2004;30:342–7.
105. Tay FR, Loushine RJ, Weller RN, et al. Ultrastructural evalua-tion of the apical seal in roots filled with a polycaprolactone-based root canal filling material. J Endod 2005;31:514–19.
106. Tay FR, Pashley DH, Williams MC, et al. Susceptibility of apolycaprolactone-based root canal filling material to degrada-tion. I. Alkaline hydrolysis. J Endod 2005;31(8):593–8.
107. Tay FR, Pashley DH, Yiu CK, et al. Susceptibility of a poly-caprolactone-based root canal filling material to degrada-tion. II. Gravimetric evaluation of enzymatic hydrolysis.J Endod 2005;31:737–41.
108. Gesi A, Raffaelli O, Goracci C, et al. Interfacial strength ofresilon and gutta-percha to intraradicular dentin. J Endod2005;31:809–13.
109. Stratton RK, Apicella MJ, Mines P. A fluid filtration compar-ison of gutta-percha versus Resilon, a new soft resin endo-dontic obturation system. J Endod 2006;32:642–5.
110. Von Fraunhofer JA, Kurtzman GM, Norby CE. Resin-basedsealing of root canals in endodontic therapy. Gen Dent2006;54:243–6.
111. Wang CS, Debelian GJ, Teixeira FB. Effect of intracanalmedicament on the sealing ability of root canals filled withResilon. J Endod 2006;32:532–6.
112. Epley SR, Fleischman J, Hartwell G, Cicalese C. Complete-ness of root canal obturations: Epiphany techniques versusgutta-percha techniques. J Endod 2006;32:541–4.
113. Teixeira FB, Teixeira EC, Thompson JY, Trope M. Fractureresistance of roots endodontically treated with a new resinfilling material. J Am Dent Assoc 2004;135:646–52.
114. Williams C, Loushine RJ, Weller RN, et al. A comparison ofcohesive strength and stiffness of Resilon and gutta-percha.J Endod 2006;32(6):553–5.
115. Schwandt NW, Gound TG. Resourcinol-formaldehyderesin ‘‘Russian Red’’ endodontic therapy. J Endod2003;29:435–7.
116. Pitt Ford TR, Torabinejad M, Abedi HR, et al. Mineraltrioxide aggregate as a pulp capping material. J Am DentAssoc 1996;127:1491–4.
117. Andelin WE, Shabahang S, Wright K, Torabinejad M. Iden-tification of hard tissue using dentin sialoprotein (DSP) as amarker. J Endod 2003;29:646–50.
118. Bakland LK. Management of traumatically injuried pulps inimmature teeth using MTA. Calif Dent Assoc J 2000:855–8.
119. Lee SJ, Monsef M, Torabinejad M. Sealing ability of amineral trioxide aggregate for repair of lateral root perfora-tions. J Endod 1993;19:541–4.
120. Pitt Ford TR, Torabinejad M, Hong CU, Kariyawasam SP.Use of mineral trioxide aggregate for repair of furcal per-forations. Oral Surg Oral Med Oral Pathol Endod1995;79:756–63.
121. Nakata TT, Bae KS, Baumgartner JC. Perforation repaircomparing mineral trioxide aggregate and amalgam usingan anaerobic bacterial leakage model. J Endod 1998;24:184–6.
122. Main C, Mirzayan N, Shabahang S, Torabinejad M. Repairof root perforations using mineral trioxide aggregate: a long-term study. J Endod 2004;30:80–3.
123. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of amineral trioxide aggregate when used as a root-end fillingmaterial. J Endod 1993;19:591–5.
124. Torabinejad M, Hong CU, Lee SJ, et al. Investigation ofmineral trioxide aggregate for root end fillings in dogs.J Endod 1995;21:603–8.
125. Torabinejad M, Pitt Ford TR, McKendry DJ, et al. Histologicassessment of MTA as a root end filling in monkeys. J Endod1997;23:225–8.
126. Torabinejad M, Chivian N. Clinical applications of mineraltrioxide aggregate. J Endod 1999;25:197–205.
127. Shabahang S, Torabinejad M. Treatment of teeth with openapices using mineral trioxide aggregate. Pract PeriodonticsAesthet Dent 2000;12:315–20.
128. Hayashi M, Shimizu A, Ebisu S. MTA for obturation ofmandibular central incisors with open apices: case report. JEndod 2004;30:120–2.
129. Tselnik M, Baumgartner JC, Marshall JG. Bacterial leakage withmineral trioxide aggregate or a resin-modified glass ionomerused as a coronal barrier. J Endod 2004;30(11):782–4.
130. Torabinejad M, Hong CU, Pitt Ford TR. Physical propertiesof a new root end filling material. J Endod 1995;21:349–53.
131. Holland R, de Souza V, Nery MJ, et al. Reaction of dog’s teethto root canal filling with mineral trioxide aggregate or a glassionomer sealer. J Endod 1999;25:728–30.
132. Wucherpfenning AL, Green DB. Mineral trioxide vs. Portlandcement: two biocompatible materials. J Endod 1999;25:308.
133. Estrela C, Bammann LL, Estrela CRA, et al. Antimicrobialand chemical study of MTA, Portland cement, calciumhydroxide paste, Sealapex, and Dycal. Braz DentJ 2000;11:3–9.
134. Holland R, Souza V, Nery MJ, et al. Reaction of rat con-nective tissue to implanted dentin tube filled with mineraltrioxide aggregate, Portland cement or calcium hydroxide.Braz Dent J 2001;12:3–8.
135. Holland R, de Souza V, Murata SS, et al. Healing process ofdog dental pulp after pulpotomy and pulp covering with
Chapter 29 / Root Canal Filling Materials / 1047

mineral trioxide aggregate or Portland cement. Braz Dent J2001;12:109–13.
136. Duarte MAH, Demarchi ACCO, Yamashita JC, et al. pH andcalcium ion release of 2 root-filling materials. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2003;95:245–7.
137. Sarkar NK, Caicedo R, Ritwik P, et al. Physicochemical basisof the biologic properties of mineral trioxide aggregate.J Endod 2005;31(2):97–100.
138. Torabinejad M, Higa RK, McKendry DJ, Pitt Ford TR. Dyeleakage of four root end filling materials: effects of bloodcontamination. J Endod 1994;20(4):159–63.
139. Gondim EJ, Kim S, Souza Filho FJ. An investigation ofmicroleakage from root-end fillings in ultrasonic retrogradecavities with or without finishing: a quantitative analysis.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2005;99(6):755–9.
140. Torabinejad M, Rastegar AF, Kettering JD, Pitt Ford TR.Bacterial leakage of mineral trioxide aggregate as a root-end filling material. J Endod 1995;21(3):109–12.
141. Tang HM, Torabinejad M, Kettering JD. Leakage evaluationof root end filling materials using endotoxin. J Endod2002;28(1):5–7.
142. Torabinejad M, Smith PW, Kettering JD, Pitt Ford TR.Comparative investigation of marginal adaptation of mineraltrioxide aggregate and other commonly used root-end fillingmaterials. J Endod 1995;21(6):295–9.
143. Peters CI, Peters OA. Occlusal loading of EBA and MTA root-end fillings in a computer-controlled masticator: a scanningelectron microscope study. Int Endod J 2002;35:22–9.
144. Gondim EJ, Zaia AA, Gomes BA, et al. Investigation of themarginal adaptation of root-end filling materials in root-endcavities prepared with ultrasonic tips. Int Endod J 2003;36:491–9.
145. Xavier CB, Weismann R, de Oliveira MG, et al. Root-endfilling materials: apical microleakage and marginal adapta-tion. J Endod 2005;31(7):539–42.
146. Mangin C, Yesilsoy C, Nissan R, Stevens R. The comparativesealing ability of hydroxyapatite cement, mineral trioxideaggregate, and super ethoxybenzoic acid as root-end fillingmaterials. J Endod 2003;29(4):261–4.
147. Bates CF, Carnes DL, Del Rio CE. Longitudinal sealingability of mineral trioxide aggregate as a root-end fillingmaterial. J Endod 1996;22:575–8.
148. Wu MK, Kontakiotis EG, Wesselink PR. Long-term sealprovided by some root-end filling materials. J Endod1998;24:557–60.
149. DeBruyne MAA, DeBruyne RJE, Rosiers L, DeMoor RJG.Longitudinal study on microleakage of three root-end fillingmaterials by the fluid transport method and by capillary flowporometry. Int Endod J 2005;38:129–36.
150. Andelin WE, Browning DF, Hsu G-HR, et al. Microleakageof resected MTA. J Endod 2002;28(8):573–4.
151. Lamb EL, Loushine RJ, Weller RN, et al. Effect of rootresection on the apical sealing ability of mineral trioxideaggregate. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;95(6):732–5.
152. Valois CRA, Costa EDJ. Influence of the thickness of mineraltrioxide aggregate on sealing ability of root-end fillings invitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2004;97(1):108–11.
153. Matt GD, Thorpe JR, Strother JM, McClanahan SB. Com-parative study of white and gray mineral trioxide aggregate(MTA) simulating a one- or two-step apical barrier techni-que. J Endod 2004;30(12):876–9.
154. Torabinejad M, Hong CU, Pitt Ford TR, Kettering JD. Cyto-toxicity of four root end filling materials. J Endod1995;21:489–92.
155. Torabinejad M, Pitt Ford TR, Abedi HR, et al. Tissuereaction to implanted potential root-end filling materialsin the tibia and mandible of guinea pigs. J Endod1998;24:568–71.
156. Koh ET, Torabinejad M, Pitt Ford TR, et al. Mineral trioxideaggregate stimulates a biological response in human osteo-blasts. J Biomed Mater Res 1997;37:432–9.
157. Koh ET, McDonald F, Pitt Ford TR, Torabinejad M. Cellularresponse to mineral trioxide aggregate. J Endod 1998;24:543–7.
158. Haglund R, He J, Jarvis J, et al. Effects of root-end fillingmaterials on fibroblasts and macrophages in vitro. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2003;95:739–45.
159. DeDeus G, Ximenes R, Gurgel-Filho ED, et al. Cytotoxicityof MTA and Portland cement on human ECV 304 endothe-lial cells. Int Endod J 2005;38:604–9.
160. Hernandez EP, Botero TM, Mantellini MG, et al. Effect ofProRoot MTA mixed with chlorhexidine on apoptosis andcell cycle of fibroblasts and macrophages in vitro. Int Endod J2005;38:137–43.
161. Melegari KK, Botero TM, Holland GR. Prostaglandin Eproduction and viability of cells cultured in contactwith freshly mixed endodontic materials. Int EndodJ 2006;39:357–62.
162. Zhu Q, Haglund R, Safavi KE, Spangberg LSW. Adhesion ofhuman osteoblasts on root-end filling materials. J Endod2000;26(7):404–6.
163. Regan JD, Gutmann JL, Witherspoon DE. Comparison ofDiaket and MTA when used as root-end filling materials tosupport regeneration of the periradicular tissues. Int Endod J2002;35:840–7.
164. Baek S-H, Plenk HJ, Kim S. Periapical tissue responses andcementum regeneration with amalgam, Super EBA, and MTAas root-end filling materials. J Endod 2005;31(6):444–9.
165. Holland R, deSouza V, Nery MJ, et al. Reaction of ratconnective tissue to implanted dentin tubes filled withmineral trioxide aggregate or calcium hydroxide. J Endod1999;25:161–6.
1048 / Endodontics

166. Holland R, deSouza V, Nery MJ, et al. Reaction of rat con-nective tissue to implanted dentin tubes filled with a whitemineral trioxide aggregate. Braz Dent J 2002;13:23–6.
167. Perez AL, Spears R, Gutmann JL, Opperman LA. Osteoblastsand MG63 osteosarcoma cells behave differently when incontact with ProRoot MTA and white MTA. Int Endod J2003;36:564–70.
168. Camilleri J, Montesin FE, Papaioannou S, et al. Biocompat-ibility of two commercial forms of mineral trioxided aggre-gate. Int Endod J 2004;37:699–704.
169. Ribeiro DA, Duarte MAH, Matsumoto MA, et al. Biocompat-ibility in vitro tests of mineral trioxide aggregate and regularand white portland cements. J Endod 2005;31(8):605–7.
170. Ribeiro DA, Matsumoto MA, Duarte MA, et al. Exvivo biocompatibility tests of regular and white forms of mineraltrioxide aggregate. Int Endod J 2006;39:26–30.
171. Asgary S, Parirokh M, Eghbal MJ, Brink F. Chemical differ-ences between white and gray mineral trioxide aggregate.J Endod 2005;31(2):101–3.
172. Oviir T, Pagoria D, Ibarra G, Geurtsen W. Effects of gray andwhite mineral trioxide aggregate on the proliferation of oralkeratinocytes and cementoblasts. J Endod 2006;32(3):210–13.
173. Sluyk SR, Moon PC, Hartwell GR. Evaluation of settingproperties and retention characteristics of mineral trioxideaggregate when used as a furcation perforation repair mate-rial. J Endod 1998;24:768–71.
174. Fridland M, Rosado R, Eng C. MTA solubility: a long termstudy. J Endod 2005;31(5):376–9.
175. Camilleri J, Montesin FE, DiSilvio L, Pitt Ford TR.The chemical constitution and biocompatibility of acceler-ated Portland cement for endodontic use. Int Endod J2005;38:834–42.
176. Huang FM, Tai K-W, Chou M-Y, Chang Y-C. Cytotoxicityof resin-, zinc oxide-eugenol, and calcium hydroxide-basedroot canal sealers on human periodontal ligament cells andpermanent V79 cells. Int Endod J 2002;35:153–8.
177. England MC, West NM, Safavi K, Green DB. Tissue leadlevels in dogs with RC-2B root canal fillings. J Endod1980;6:728–30.
178. Spangberg LS. Biologic effects of root-canal-filling materials.The effect on bone tissue of two formaldehyde-containingroot canal pastes: N2 and Riebler’s paste. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1974;38:934–44.
179. Spangberg LS, Langeland K. Biologic effects of dental mate-rials. I. Toxicity of root-canal-filling materials on HeLa cellsin vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1973;35:402–14.
180. Orlay H. Overfilling in root canal treatment. Two accidentswith N2. Br Dent J 1964;120:376.
181. Grossman LI. Paresthesia from N2 or N2 substitute. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1978;45:114–15.
182. Grossman LI, Tatoian G. Paresthesia from N2. Report of acase. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1978;46:700–1.
183. Montgomery S. Paresthesia following endodontic treatment.J Endod 1976;2:345–7.
184. FDA explains status of N2 material. J Am Dent Assoc1992;123(7):236–7.
185. Council on Dental Therapeutics ADA. The use of root canalfilling materials containing paraformaldehyde: a statusreport. J Am Dent Assoc 1987;114:95.
186. American Association of Endodontists. Position Statement:Paraformaldehyde-containing endodontic filling materialsand sealers. American Association of Endodontics, Chicago,IL, April, 1991.
187. Notice: Board bans cement in Florida. ADA News 1992;23:15.
188. Grossman LI. Endodontic practice. 10th ed. Philadelphia:Lea & Febiger; 1982. p. 297.
189. Grossman LI. Physical properties of root canal cements.J Endod 1976;2(6):166–75.
190. Block RM, Lewis RD, Sheats JB, Burke SH. Antibody forma-tion to dog pulp tissue altered by N2-type paste within theroot canal. J Endod 1977;8:309–15.
191. Block RM, Sheats JB, Lewis RD, Fawley J. Cell-mediatedresponse to dog pulp tissue altered by N2 paste within theroot canal. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1978;45:131–42.
192. Block RM, Lewis RB, Sheats JB, Fawley J. Cell-mediatedimmune response to dog pulp tissue altered by Kerr (Rick-ert’s) sealer via the root canal. J Endod 1978;4:110–16.
193. Torabinejad M, Kettering JD, Bakland LK. Evaluation ofsystemic immunological reactions to AH-26 root canal sea-ler. J Endod 1979;5:196–200.
194. Harnden DG. Tests for carcinogenicity and mutagenicity. IntEndod J 1981;14:35–40.
195. Lewis BB, Chestner SB. Formaldehyde in dentistry: a reviewof the mutagenic and carcinogenic potential. J Am DentAssoc 1981;103:429–34.
196. Grossman LI. An improved root canal cement. J Am DentAssoc 1958;56:381–5.
197. Sleder FS, Lumley PJ, Bohacek JR. Long-term sealing abilityof a calcium hydroxide sealer. J Endod 1991;17:541–3.
198. Holland R, de Souza V. Ability of a new calcium hydroxideroot canal filling material to induce hard tissue formation.J Endod 1985;11(12):535–43.
199. Beltes P, Koulaouzidou E, Kotoula V, Kortsaris AH. Invitro evaluation of the cytotoxicity of calcium hydroxide-based root canal sealers. Endod Dent Traumatol1995;11(5):245–9.
200. Siqueira FJ, Jr., Fraga RC, Garcia PF. Evaluation of sealingability, pH and flow rate of three calcium hydroxide-basedsealers. Endod Dent Traumatol 1995;11(5):225–8.
Chapter 29 / Root Canal Filling Materials / 1049

201. Spangberg LS, Barbosa SV, Lavigne GD. AH 26 releasesformaldehyde. J Endod 1993;19:596–8.
202. Koch MJ. Formaldehyde release from root-canal sealers:influence of method. Int Endod J 1999;32:10–16.
203. Leonardo MR, da Silva LAB, Filho MT, da Silva RS. Releaseof formaldehyde by 4 endodontic sealers. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1999;88:221–5.
204. Sousa CJ, Montes CR, Pascon EA, et al. Comparison of theintraosseous biocompatibility of AH Plus, EndoREZ, andEpiphany root canal sealers. J Endod 2006;32:656–62.
205. Versiani MA, Carvalho JRJ, Padiha MI, et al. A comparativestudy of physiochemical properties of AH Plus and Epi-phany root canal sealants. Int Endod J 2006;39:464–71.
206. Ungor M, Onay EO, Orucoglu H. Push-out bond strengths:the Epiphany-Resilon endodontic obturation system com-pared with different pairings of Epiphany, Resilon, AH Plusand gutta-percha. Int Endod J 2006;39:643–7.
207. Olsson B, Siwkowski A, Langeland K. Intraosseous implan-tation for biological evaluation of endodontic materials.J Endod 1981;7:253–65.
208. Olsson B, Siwkowski A, Langeland K. Subcutaneous implan-tation in the biological evaluation of endodontic materials.J Endod 1981;7:355–65.
209. Olsson B, Wennberg A. Early tissue reaction to endodonticfilling materials. Endod Dent Traumatol 1985;1:138–41.
210. Ørstavik D, Mjor IA. Histopathology and X-ray microana-lysis of the subcutaneous tissue response to endodonticsealers. J Endod 1988;14:13–23.
211. Eldeniz AU, Erdemir A, Belli S. Shear bond strength of threeresin based sealers to dentin with and without the smearlayer. J Endod 2005;31(4):293–6.
212. Whitworth J. Methods of filling root canals: principles andpractices. Endod Topics 2005;12:2–24.
213. Wu MK, van der Sluis LW, Wesselink PR. A 1-year follow-up study on leakage of single-cone fillings with RoekoRSAsealer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2006;101:662–7.
214. Johnston HB. The principle of diffusion applied to the Call-ahan method of pulp canal filling. Dental Summ1927;43:743.
215. Beyer-Olsen EM, Ørstavik D, Eriksen HM. Radiographicvoids and leakage along root fillings in vitro. Int Endod J1983;16:51–8.
216. Tay FR, Loushine RJ, Monticelli F, et al. Effectiveness ofresin-coated gutta-percha cones and a dual-cured, hydro-philic methacrylate resin-based sealer in obturating rootcanals. J Endod 2005;31:659–64.
217. Hiraishi N, Loushine RJ, Vano M, et al. Is an oxygen inhib-ited layer required for bonding of resin-coated gutta-perchato a methacrylate-based root canal sealer? J Endod2006;32:429–33.
218. Zmener O, Banegas G, Pameijer CH. Bone tissue response toa methacrylate-based endodontic sealer: a histological andhistometric study. J Endod 2005;31(6):457–9.
219. Zmener O, Pameijer CH, Macri E. Evaluation of the apicalseal in root canals prepared with a new rotary system andobturated with a methacrylate based endodontic sealer: anin vitro study. J Endod 2005;31:392–5.
220. Cohen BI, Pagnillo MK, Musikant BL, Deutsch AS. Theevaluation of apical leakage for three endodontic fill systems.Gen Dent 1998;46:618–23.
221. Musikant BL, Cohen BI, Deutsch AS. A two-and-a-half yearperspective on simplified endodontic techniques. CompendContin Educ Dent 2003;24:46–52.
222. Deutsch AS, Musikant BL, Cohen BI, Kase D. A study of onevisit treatment using EZ-fill root canal sealer. Endod Pract2001;4:29–36.
223. Belli S, Ozcan E, Derinbay O. Comparative evaluation ofapical leakage of a new-root canal sealer. J Dent Res 2007;86 (Spec Issue A):#0369.
224. Ørstavik D. Physical properties of root canal sealers: mea-surement of flow, working time, and compressive strength.Int Endod J 1983;16(3):99–107.
225. Juhasz A, Verdes E, Tokes L, et al. The influence of rootcanal shape on the sealing ability of two root canal sealers.Int Endod J 2006;39:282–6.
226. Cobankara FK, Orucoglu H, Sengun A, Belli S. The quanti-tative evaluation of apical sealing of four endodontic sealers.J Endod 2006;32(1):66–8.
227. Orucoglu H, Sengun A, Yilmaz N. Apical leakage of resinbased root canal sealers with a new computerized fluidfiltration meter. J Endod 2005;31:886–90.
228. Saleh IM, Ruyter IE, Haapasalo MP, et al. Adhesionof endodontic sealers: scanning electron micros-copy and energy dispersive spectroscopy. J Endod2003;29(9):595–601.
229. Pommel L, About I, Pashley D, Camps J. Apical leakage offour endodontic sealers. J Endod 2003;29(3):208–10.
230. Lee KW, Williams MC, Camps JJ, Pashley DH. Adhesion ofendodontic sealers to dentin and gutta-percha. J Endod2002;28:684–8.
231. Tagger M, Tagger E, Tjan AH, Bakland LK. Shearing bondstrength of endodontic sealers to gutta-percha. J Endod2003;29:191–3.
232. Miletic I, Devcic N, Anic I, et al. The cytotoxicity of Roeko-Seal and AH plus compared during different setting periods.J Endod 2005;31(4):307–9.
233. Spangberg L, Pascon EA. The importance of material prepara-tion for the expression of cytotoxicity during in vitro evalua-tion of biomaterials. J Endod 1988;14(5):247–50.
234. Economides N, Kotsaki-Kovatsi VP, Poulopoulos A, et al.Experimental study of the biocompatibility of four root
1050 / Endodontics

canal sealers and their influence on the zinc and calciumcontent of several tissues. J Endod 1995;21(3):122–7.
235. Bernath M, Szabo J. Tissue reaction initiated by differentsealers. Int Endod J 2003;36:256–61.
236. Huumonen S, Lenander-Lumikari M, Sigurdsson A, Ørsta-vik D. Healing of apical periodontitis after endodontic treat-ment: a comparison between a silicone-based and a zincoxide based sealer. Int Endod J 2003;36:295–301.
237. Lacey S, Pitt Ford TR, Watson TF, Sherriff M. A study of therheological properties of endodontic sealers. Int Endod J2005;38(8):499–504.
238. McMichen FR, Pearson G, Rahbaran S, et al. A comparativestudy of selected physical properties of five root-canal sea-lers. Int Endod J 2003;36(9):629–35.
239. Tagger M, Greenberg B, Sela G. Interaction between sealersand gutta-percha cones. J Endod 2003;29(12):835–7.
240. Nielsen BA, Beeler WJ, Vy C, Baumgartner JC. Setting timesof Resilon and other sealers in aerobic and anaerobic envir-onments. J Endod 2006;32(2):130–2.
241. Peters DP. Two year in vitro solubility evaluation of four gutta-percha sealer obturation techniques. J Endod 1986;12:139–45.
242. Crane DL, Heuer MA, Kaminski EJ, Moser JB. Biologicaland physical properties of an experimental root canal sealerwithout eugenol. J Endod 1980;6:438–45.
243. Caicedo R, von Fraunhofer JA. The properties of endodonticsealers. J Endod 1988;14:527–34.
244. Schafer E, Zandbiglari T. Solubility of root-canal sealers in waterand artificial saliva. Int Endod J 2003;36(10):660–9.
245. Kazemi RB, Safavi KE, Spangberg LS. Dimensional changesof endodontic sealers. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1993;76(6):766–71.
246. Sipert CR, Hussne RP, Nishiyama CK, Torres SA. In vitroantimicrobial activity of Fill Canal, Sealapex, Mineral Tri-oxide Aggregate, Portland cement and EndoRez. Int Endod J2005;38(8):539–43.
247. Pizzo G, Giammanco GM, Cumbo E, et al. In vitro antibac-terial activity of endodontic sealers. J Dent 2006;34(1):35–40.
248. Williamson AE, Dawson DV, Drake DR, et al. Effect ofroot canal filling/sealer systems on apical endotoxinpenetration: a coronal leakage evaluation. J Endod2005;31(8):599–604.
249. Siqueira FJ, Jr., Goncalves RB. Antibacterial activities of rootcanal sealers against selected anaerobic bacteria. J Endod1996;22(2):79–80.
250. Leonardo MR, da Silva LAB, Filho MT, et al. In vitroevaluation of antimicrobial activity of sealers and pastes usedin endodontics. J Endod 2000;26:391–4.
251. Kayaoglu G, Erten H, Alacam T, Ørstavik D. Short-termantibacterial activity of root canal sealers towards Entero-coccus faecalis. Int Endod J 2005;38(7):483–8.
252. Swanson K, Madison S. An evaluation of coronal microleak-age in endodontically treated teeth. Part I: Time periods.J Endod 1987;13:56–9.
253. Torabinejad M, Ung B, Kettering JD. In vitro bacterialpenetration of coronally unsealed endodontically treatedteeth. J Endod 1990;16:556–9.
254. Magura ME, Kafrawy AH, Brown CE, Newton CW. Humansaliva coronal microleakage in obturated root canals: an invitro study. J Endod 1991;17:324–31.
255. Khayat A, Lee SJ, Torabinejad M. Human saliva penetrationof coronally unsealed obturated root canals. J Endod1993;19:458–61.
256. Tronstad L, Asbjornsen K, Doving L, et al. Influence of coronalrestorations on the periapical health of endodontically treatedteeth. Endod Dent Traumatol 2000;16:218–21.
257. Ricucci D, Grondahl K, Bergenholtz G. Periapical status ofroot-filled exposed to the oral environment by loss ofrestoration or caries. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2000;90:254–9.
258. Ricucci D, Bergenholtz G. Bacterial status in root-filled teethexposed to the oral environment by loss of restoration andfracture or caries—a histobacteriological study of treatedcases. Int Endod J 2003;36:787–802.
259. Saunders WP, Saunders EM. Coronal leakage as a cause offailure in root-canal therapy: a review. Endod Dent Trau-matol 1994;10:105–8.
260. Wolcott JF, Hicks ML, Himel VT. Evaluation of pigmentedintraorifice barriers in endodontically treated teeth. J Endod1999;25:589–92.
261. Chailertvanitkul P, Saunders WP, Saunders EM, MacKenzieD. An evaluation of microbial coronal leakage in the restoredpulp chamber of root-canal treated multirooted teeth. IntEndod J 1997;30:18–22.
262. Pisano DM, DiFiore PM, McClanahan SB, et al. Intraorificesealing of gutta-percha obturated root canals to preventcoronal microleakage. J Endod 1998;24:659–62.
263. Beckham BM, Anderson RW, Morris CF. An evaluation ofthree materials as barriers to coronal microleakage in endo-dontically treated teeth. J Endod 1993;19:388–91.
264. Galvan RR, West LA, Liewehr FR, Pashley DH. Coronalmicroleakage of five materials used to create an intraoral sealin endodontically treated teeth. J Endod 2002;28:59–61.
265. Wolanek GA, Loushine RJ, Weller RN, et al. In vitro bacter-ial penetration of endodontically treated teeth coronallysealed with a dentin bonding agent. J Endod 2001;27:354–7.
266. Schwartz RS, Fransman R. Adhesive dentistry and endodon-tics: materials, clinical strategies and procedures for restorationof access cavities: a review. J Endod 2005;31(5):151–65.
267. Maloney SM, McClanahan SB, Goodell GG. The effect ofthermocycling on a colored glass ionomer intracoronal bar-rier. J Endod 2005;31(7):526–8.
Chapter 29 / Root Canal Filling Materials / 1051

268. Hommez GMG, Coppens CRM, DeMoor RJG. Periapicalhealth related to the quality of coronal restorations and rootfillings. Int Endod J 2002;35:680–9.
269. Yamauchi S, Shipper G, Buttke T, et al. Effect of orifice plugs onperiapical inflammation in dogs. J Endod 2006;32(6):524–6.
270. Jenkins S, Kulild J, Williams K, et al. Sealing ability of threematerials in the orifice of root canal systems obturated withgutta-percha. J Endod 2006;32(3):225–7.
271. Mavec JC, McClanahan SB, Minah GE, et al. Effects of anintracanal glass ionomer barrier on coronal microleakage inteeth with post space. J Endod 2006;32(2):120–22.
272. Barkhordar RA, Stark MM. Sealing ability of intermediaterestorations and cavity design used in endodontics. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1990;69(1):99–101.
273. Beach CW, Calhoun JC, Bramwell JD, et al. Clinical evalua-tion of bacterial leakage of endodontic temporary fillingmaterials. J Endod 1996;22(9):459–62.
274. Balto H. An assessment of microbial coronal leakge of tem-porary filling materials in endodontically treated teeth.J Endod 2002;28:762–4.
275. Lee YC, Yang SF, Hwang YF, et al. Microleakage of endodontictemporary restorative materials. J Endod 1993;19(10):516–20.
276. Noguera AP, McDonald NJ. A comparative in vitro coronalmicroleakage study of new endodontic restorative materials.J Endod 1990;16:523–7.
277. Kazemi RB, Safavi KE, Spangberg LS. Assessment of mar-ginal stability and permeability of an interim restorativeendodontic material. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1994;78(6):788–96.
278. Mayer T, Eickholz P. Microleakage of temporary restora-tions after thermocycling and mechanical loading. J Endod1997;23(5):320–2.
279. Teplitsky PE, Meimaris IT. Sealing ability of Cavit and TERMas intermediate restorative materials. J Endod 1988;14:278–82.
280. Paris L, Kapsimalis P. The effect of temperature change onthe sealing properties of temporary filling materials: Part 1.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1960;13:982–9.
281. Vail MM, Steffel CL. Preference of temporary restorationsand spacers: a survey of Diplomates of the American Boardof Endodontics. J Endod 2006;32:513–15.
282. Webber RT, del Rio CE, Brady JM, Segall RO. Sealing qualityof a temporary filling material. Oral Surg Oral Med OralPathol Oral Radiol Endod 1978;46(1):123–30.
283. Barthel CR, Zaritzki FF, Raab WH, Zimmer S. Bacterialleakage in roots filled with different medicaments and sealedwith Cavit. J Endod 2006;32(2):127–9.
284. Wilderman FH, Eames WB, Serene TP. The physical and bio-logic properties of Cavit. J Am Dent Assoc 1971;82(2):378–82.
285. Slutzky H, Slutzky-Goldberg I, Weiss EI, Matalon S. Anti-bacterial properties of temporary filling materials. J Endod2006;32(3):214–17.
286. Zmener O, Banegas G, Pameijer CH. Coronal microleakageof three temporary restorative materials: an in vitro study.J Endod 2004;30(8):582–4.
287. Orahood JP, Cochran MA, Swartz M, Newton CW. Invitro study of marginal leakage between temporary sealingmaterials and recently placed restorative materials. J Endod1986;12(11):523–7.
288. Jacquot BM, Panighi MM, Steinmetz P, G’Sell C. Evaluationof temporary restorations’ microleakage by means ofelectrochemical impedance measurements. J Endod1996;22(11):586–9.
289. Seiler KB. An evaluation of glass ionomer–based restorativematerials as temporary restorations in endodontics. GenDent 2006;54(1):33–6.
290. Hansen SR, Montgomery S. Effect of restoration thickness onthe sealing ability of TERM. J Endod 1993;19(9):448–52.
1052 / Endodontics

CHAPTER 30
OBTURATION OF THE RADICULAR SPACE
FRED W. BENENATI
It has been four decades since the late Dr. HerbertSchilder published his classic article on filling the rootcanal space in three dimensions.1 Ironically, it came 7years before his treatise on cleaning and shaping the rootcanal system.2 One might extrapolate from this fact thatclosing off or obturating a cleaned and shaped radicularspace has considerable importance.
Rationale of Obturation
HISTORICAL PERSPECTIVEObturation of the radicular space has been describedin various ways for well over 100 years, includingEdward Hudson’s 1825 report of filling with goldfoil.3 Controlled length obturation of the root canalsystem was not verified until Edmund Kells producedthe first endodontic radiograph in 1899.
Root canal therapy, including obturation, exper-ienced a setback in 1910 when William Hunter deliveredhis address entitled ‘‘the role of sepsis and asepsis.’’Chivian3 stated that Hunter’s thesis regarding focalinfection was ‘‘misinterpreted to include periapicallesions and root canal therapy in general.’’ This likelyled to, as the modern-day challenge against amalgamhas, more careful practice and a rebirth of research anddevelopment in the specialty of endodontics. Perhapsone could view this as a deja vu impetus for the modern-day call for evidence-based endodontics!
In 1967 Grossman4 described the reasons for thegrowth and acceptance of endodontics in spite of thefocal infection theory. These included better researchmethods, minimal health risks, and the demand forrestorative dentistry. His principles may be consideredclassic, including his ‘‘Principle 9,’’ having to do withobturation, or as he termed it ‘‘hermetic seal of thecanal’’ terminating at the dentinocemental junction.Principle 10 dealt with the acceptability of the fillingmaterial. The term ‘‘hermetic seal’’ is now considered
inaccurate. ‘‘Hermetic’’ is defined as ‘‘airtight byfusion or sealing.’’ The concern in closing or obturat-ing the canal space is not related to air; it is aboutfluid leakage at the apex or the coronal level. An‘‘impermeable seal’’ is a more accurate term.5
OBJECTIVE OF OBTURATIONSchilder1 describes the final objective of endodonticprocedures as being ‘‘the total obturation of the rootcanal space.’’ He also stated ‘‘in the final analysis, it isthe sealing of the complex root canal system from theperiodontal bone that ensures the health of the attach-ment apparatus against breakdown of endodonticorigin.’’ Nearly a decade later, Dubrow6 questionedthe validity of a ‘‘hermetic seal’’ produced by silverpoints or gutta-percha and sealer. He described casesthat healed after instrumentation, medication, and acoronal seal, but no obturation. The question has notbeen answered, however: will this last, and for howlong, without full canal length obturation?
In the previous edition of this text, the authors of thechapter on obturation of the root canal space describedbacteria and bacterial toxin ingress as the major causeof tissue irritation. Even in bacterial absence, degradedserum may serve as a periapical tissue irritant. Theypointed out that ‘‘bacteria are the primary source ofpersistent periradicular inflammation and endodonticfailure.’’7 Thus, it may be deduced that following totaldebridement of the radicular space, ‘‘the developmentof a fluid-tight seal of the apical foramen and the totalobliteration of the root canal’’ must follow to ensurethe best chance of long-term success (Figure 1). Thepresent-day knowledge of the importance of a coronalseal cannot be overlooked as well.
WHEN IS THE CANAL READYTO OBTURATE?Radicular space obturation is ideally accomplished aftercleaning and shaping has been completed to an optimum
1053

size.7 Although there is no universal agreement on whatconstitutes an optimal size, it seems that the canal(s)should be dry, with no ‘‘weeping’’ of fluids into theradicular space.7
The tooth should ideally be asymptomatic, al-though those completely instrumented, yet with mildsymptoms or even significant symptoms, have beenshown to become asymptomatic upon obturation.7,8
There are also reports showing the importance ofobturating canals following negative bacterial cul-tures.9,10 Sjogren et al.10 found that upon a 5-yearrecall, 94% of cases exhibiting negative cultures werefound to be successful, whereas only 68% of thosefilled with positive cultures were successful.
APICAL EXTENT OF OBTURATION:WHERE AND WHY?As early as 1930 and again in 1967, Grossman4 remarkedthat there was no general agreement on where a canalfilling should end. However, the consensus was that itshould be the dentinocemental junction. The trend at thetime was to obturate a canal ‘‘even with the root apex orjust short of it, rather than to overfill the canal.’’ Today, werecognize a difference in semantics between overfilling andoverextension. Overfilling actually denotes ‘‘total obtura-tion of the root canal space with excess material extrudingbeyond the apical foramen.’’11 Overextension also denotesfilling material beyond the apex, but the canal may nothave been filled adequately within its confines.
The dentinocemental junction has been described byKuttler12 as an average of approximately 0.5 to 0.7 mmfrom the external surface of the apical foramen (Figure 2).Thus, it could be construed that filling to the radiographic
Figure 1 A, Failure of reactive iodine (131 I) to penetrate into wellobturated root canal. Only periapical cementum that was not coatedwith sticky wax has absorbed isotope. B, Massive reaction to penetra-tion of radioactive iodine (131 I) into poorly filled canal. Violent responseat periapex is comparable to in vivo response to toxic and/or infectivecanal products. Reproduced with permission from Dow PR. Ingle JI.22
Figure 2 Ideal termination of canal preparation and obturation. A, Apical constriction at cementodentinal junction marks end of root canal. From this point toanatomic apex (0.5 to 0.7mm), tissue is periodontal. B, Photomicrograph of periapex. Small arrows at cementodentinal junction. Large arrow (bottom) at denticleinclusion. A, Reproduced with permission from Goerig AC in Besner E, Practical Endodontics CV Mosby; 1993. B, Permission from Brynolf I in Odontol Revy; 1967.
1054 / Endodontics



![Making TDD [Somewhat] Bearable on OpenStack](https://static.fdocuments.net/doc/165x107/554bcda7b4c905706a8b4933/making-tdd-somewhat-bearable-on-openstack.jpg)














