
Postmortem use of advanced imaging techniques: Is autopsy
10
OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et al Submitted 7/2008 – Accepted 10/2008 – Published 12/2008 Copyright 2007-2008 OPUS 12 Foundation, Inc. 17 Sharing Quality Science Worldwide… Postmortem use of advanced imaging techniques: Is autopsy going digital? S. Peter Stawicki, MD 1,6 , Anil Aggrawal, MD 2,6 , Anthony J. Dean, MD 3,6 , David A. Bahner, MD 4,6 , Steven M. Steinberg, MD 1,6 , Christy D. Stehly, BS 5 , Brian A. Hoey, MD 5,6 1 Department of Surgery, Division of Critical Care, Trauma, and Burn, The Ohio State University Medical Center, Columbus, OH, USA 2 Professor of Forensic Medicine, Maulana Azad Medical College, New Delhi, India 3 Department of Emergency Medicine, University of Pennsylvania School of Medicine, Philadelphia, PA, USA 4 Department of Emergency Medicine, The Ohio State University Medical Center, Columbus, OH, USA 5 St Luke’s Regional Level I Resource Trauma Center, Bethlehem, PA, USA 6 OPUS 12 Foundation, Columbus, OH, USA ABSTRACT The use of modern high-resolution imaging has been well described in the setting of post-mortem investigations. Used for some time in forensics, computed tomography (CT) and magnetic resonance imaging (MRI) are now being evaluated as complementary or, at times, alternative means of performing cause-of-death determination. The authors briefly review the history of autopsy and the reasons for the gradual decrease in autopsy rates over the last two decades. An overview of advantages and limitations of modern imaging autopsy techniques is then presented, including a discussion of the potential roles of imaging autopsy in clinical performance improvement process as well as in medical education. Controversies surrounding this relatively new method of acquiring postmortem information are briefly reviewed. Potential future applications of modern imaging techniques in postmortem analysis, including the incorporation of modern ultrasound technology, are then discussed. Cite as: Stawicki SP, Aggrawal A, Dean AJ, Bahner DA, Steinberg SM, Hoey BA. Postmortem use of advanced imaging techniques: Is autopsy going digital? OPUS 12 Scientist 2008;2(4):17-26. Correspondence to: S. P. Stawicki, MD, Department of Surgery, Division of Critical Care, Trauma, and Burn, The Ohio State University Medical Center, Suite 634, 395 West 12 th Avenue, Columbus, OH 43210 USA. Keywords: Autopsy, Imaging autopsy, Postmortem examination, Computed tomography, Magnetic resonance imaging, Ultrasound, Controversies. INTRODUCTION AND DEFINITIONS High-resolution imaging methods are slowly making inroads into the setting of postmortem investigation. 1 Used for some time in forensics, computed tomography (CT) and magnetic resonance imaging (MRI) are now being evaluated as complementary or even as alternative means of cause-of-death determination. 1-4 It has been proposed that modern multi-detector CT technology constitutes a viable complementary method or an alternative to traditional autopsy, especially when considering the decline of the latter as a diagnostic tool since the late 20 th century [Figure 1]. 5-6 Autopsy can be defined as the examination of a cadaver to determine or confirm the cause of death. It is derived from the Greek words for “self” (autos) and “I will see” (opsomei) – “To see with one's own eyes”. 7 Imaging autopsy can be defined as the use of high-definition CT and/or MRI scans of the decedent in addition to, or in lieu of, traditional autopsy. HISTORICAL PERSPECTIVE In ancient Egypt and Mesopotamia postmortem dissections were frequently performed during the process of embalming. 1 In India, autopsy and dissection were practiced by Sushruta, an early pioneer of ayurveda (the Indian art of medicine) in the sixth century B.C. 8 In the third century B.C., Greek scholars used autopsy for the purpose of enhancing their understanding of anatomy and disease. 9 Similar approaches re-emerged in Europe during the Middle Ages and the Renaissance with the work of Vesalius and others. The first organized treatise on pathological findings at autopsy was The seats and causes of diseases investigated by anatomy, published in 1761 by Giovanni Batista Morgagni when he was 79 years old. This book, describing nearly 700 autopsies performed by the author, is the foundation of modern post-mortem science. 9-11 At the end of the nineteenth century, Osler established the autopsy as one of the cornerstones of his approach to both medical training and the clinical method. 12-13 Students were not only expected to attend the autopsies – they were trained to perform them. 14 During the same period, Cabot reported on the autopsies of thousands of patients. 15 In the first half of the twentieth century autopsy rates steadily increased. In the 1960’s and 1970’s, many of the advances in cardiovascular surgery developed by DeBakey and his team were pioneered using cadaveric testing. 1 The second half of the 20 th century and the beginning of 21 st century saw continued decline in autopsy rates. This was largely a global phenomenon, with only a few countries where autopsy rates remained relatively constant or decreased less dramatically, including Sweden and Finland. 16-17 TRADITIONAL AUTOPSY: WHY THE DECLINE? Despite the previously mentioned medical advances and educational benefits attributed to the postmortem investigations, autopsy rates have been significantly declining. 1,18 Over the past three decades, there has been a 40-50% drop in autopsy rates across the world. 18 In the United States, autopsy rates fell from the reported high of 41% in the 1960’s to between 5% and 23% at present. 19-20 The most commonly cited factors accounting for this phenomenon include physician discomfort in requesting permission from the family, cost containment measures, risk of blood borne pathogen transmission, as well as the perceived absence of the curricular/educational value of autopsies. 1,18-23 Fear of medical malpractice suits and pathologist apathy have also
Transcript of Postmortem use of advanced imaging techniques: Is autopsy

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 17
Sharing Quality Science Worldwide…
Postmortem use of advanced imaging techniques: Is autopsy going digital?
S. Peter Stawicki, MD 1,6, Anil Aggrawal, MD 2,6, Anthony J. Dean, MD 3,6, David A. Bahner, MD 4,6,
Steven M. Steinberg, MD 1,6, Christy D. Stehly, BS 5, Brian A. Hoey, MD 5,6
1 Department of Surgery, Division of Critical Care, Trauma, and Burn, The Ohio State University Medical Center, Columbus, OH, USA2 Professor of Forensic Medicine, Maulana Azad Medical College, New Delhi, India3 Department of Emergency Medicine, University of Pennsylvania School of Medicine, Philadelphia, PA, USA4 Department of Emergency Medicine, The Ohio State University Medical Center, Columbus, OH, USA5 St Luke’s Regional Level I Resource Trauma Center, Bethlehem, PA, USA6 OPUS 12 Foundation, Columbus, OH, USA
ABSTRACTThe use of modern high-resolution imaging has been well described in the setting of post-mortem investigations. Used for some time in forensics, computed tomography (CT) and magnetic resonance imaging (MRI) are now being evaluated as complementary or, at times, alternative means of performing cause-of-death determination. The authors briefly review the history of autopsy and the reasons for the gradual decrease in autopsy rates over the last two decades. An overview of advantages and limitations of modern imaging autopsy techniques is then presented, including a discussion of the potential roles of imaging autopsy in clinical performance improvement process as well as in medical education. Controversies surrounding this relatively new method of acquiring postmortem information are briefly reviewed. Potential future applications of modern imaging techniques in postmortem analysis, including the incorporation of modern ultrasound technology, are then discussed.
Cite as: Stawicki SP, Aggrawal A, Dean AJ, Bahner DA, Steinberg SM, Hoey BA. Postmortem use of advanced imaging techniques: Is autopsy going digital? OPUS 12 Scientist 2008;2(4):17-26.
Correspondence to: S. P. Stawicki, MD, Department of Surgery, Division of Critical Care, Trauma, and Burn, The Ohio State University Medical Center, Suite 634, 395 West 12th Avenue, Columbus, OH 43210 USA.
Keywords: Autopsy, Imaging autopsy, Postmortem examination, Computed tomography, Magnetic resonance imaging, Ultrasound, Controversies.
INTRODUCTION AND DEFINITIONSHigh-resolution imaging methods are slowly making inroads into the setting of postmortem investigation.1 Used for some time in forensics, computed tomography (CT) and magnetic resonance imaging (MRI) are now being evaluated as complementary or even as alternative means of cause-of-death determination.1-4 It has been proposed that modern multi-detector CT technology constitutes a viable complementary method or an alternative to traditional autopsy, especially when considering the decline of thelatter as a diagnostic tool since the late 20th century [Figure 1].5-6
Autopsy can be defined as the examination of a cadaver to determine or confirm the cause of death. It is derived from the Greek words for “self” (autos) and “I will see” (opsomei) – “To see with one's own eyes”.7 Imaging autopsy can be defined as the use of high-definition CT and/or MRI scans of the decedent in addition to, or in lieu of, traditional autopsy.
HISTORICAL PERSPECTIVEIn ancient Egypt and Mesopotamia postmortem dissections were frequently performed during the process of embalming.1 In India, autopsy and dissection were practiced by Sushruta, an early pioneer of ayurveda (the Indian art of medicine) in the sixth century B.C.8 In the third century B.C., Greek scholars used autopsy for the purpose of enhancing their understanding of anatomy and disease.9 Similar approaches re-emerged in Europe during the Middle Ages and the Renaissance with the work of Vesalius and others. The first organized treatise on pathological findings at autopsy was The seats and causes of diseases investigated by anatomy, published in 1761 by Giovanni Batista Morgagni when he was 79 years old. This book, describing nearly 700 autopsies performed by the author, is the foundation of modern post-mortem science.9-11
At the end of the nineteenth century, Osler established the autopsy as one of the cornerstones of his approach to both medical training and the clinical method.12-13 Students were not only expected to attend the autopsies – they were trained to perform them.14 During the same period, Cabot reported on the autopsies of thousands of patients.15 In the first half of the twentieth century autopsy rates steadily increased. In the 1960’s and 1970’s, many of the advances in cardiovascular surgery developed by DeBakey and his team were pioneered using cadaveric testing.1
The second half of the 20th century and the beginning of 21st
century saw continued decline in autopsy rates. This was largely a global phenomenon, with only a few countries where autopsyrates remained relatively constant or decreased less dramatically, including Sweden and Finland.16-17
TRADITIONAL AUTOPSY: WHY THE DECLINE?Despite the previously mentioned medical advances and educational benefits attributed to the postmortem investigations, autopsy rates have been significantly declining.1,18 Over the past three decades, there has been a 40-50% drop in autopsy rates across the world.18 In the United States, autopsy rates fell from the reported high of 41% in the 1960’s to between 5% and 23% at present.19-20 The most commonly cited factors accounting for this phenomenon include physician discomfort in requesting permission from the family, cost containment measures, risk of blood borne pathogen transmission, as well as the perceived absence of the curricular/educational value of autopsies.1,18-23 Fear of medical malpractice suits and pathologist apathy have also

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 18
Sharing Quality Science Worldwide…
been mentioned.22,24 One report from Australia demonstrated a sharp drop in autopsies from nearly 40% in the year 2000 to just over 10% in 2001 that was attributed to a significant increase in autopsy refusals.25
This decline in autopsy rates does not seem to correlate with any evidence that there is a proportional decrease in need for the performance of this procedure. This is exemplified by findings of one large meta-analysis, which demonstrated that approximately one-third of death certificates executed without autopsy do not correctly identify the cause of death.26 Conversely, about 25% of autopsies reveal the presence of a previously unidentified but clinically significant pre-mortem finding 27 and over 30% of autopsies on intensive care unit patients reveal evidence of major diagnostic “misses”, including strokes, myocardial infarctions, and pulmonary emboli. 28 These findings support the notion that the gradual decline of the autopsy is likely to result in lost opportunities for both quality improvement in patient care and constructive learning among practicing clinicians.
Figure 1. A graph demonstrating the dramatic decline in the number of traditional autopsies in various geographic areas and individual medical institutions. Regardless of the reporting region or institution, note that autopsy rates have decreased similarly in terms of percentages.
HISTORY OF IMAGING AUTOPSYAdvanced imaging techniques have been used for some time during forensic investigations. In 1977, Wullenweber et alreported one of the earliest forensic applications of computed tomography to describe radiographic patterns of gunshot injuries to the head.29 In 1980, Flodmark et al performed a comparison study of premortem computed tomographic findings and subsequent autopsy results in neonates who suffered perinatal asphyxia.30 Kalender et al followed in 1990 by developing acquisition and processing of three-dimensional digital radiographic imaging data.31
The 1990's saw the inception of large-scale research programs dedicated to imaging autopsy. The most prominent of those programs is the Virtopsy Project at the University of Bern,
Switzerland.6-7 Other programs include those headed by Donchin et al 32, military-sponsored programs in the USA 33, and the CATopsy program at St Luke's Hospital in Bethlehem, Pennsylvania, USA.4 Computed tomography and magnetic resonance imaging are now being evaluated as complementary or even as alternative means of postmortem examination.1,4,6-7,32-33
Figure 2. Examples of critical findings on imaging autopsies (IA). (Top image) This trauma victim was found to have traumatic aortic injury. (Bottom image) After analyzing IA of another trauma victim it was found that the endotracheal tube was placed into the esophagus during the prehospital setting. Both of these IA studies were reviewed during the clinical performance improvement process at the performing institution.
BASIC PRINCIPLES OF IMAGING AUTOPSYImaging autopsy (IA) is based on the use of high-definition CT and/or MRI imaging of the decedent prior to, or in lieu of, traditional autopsy. At times, imaging autopsy can be performed after traditional autopsy in order to obtain additional information regarding skeletal, muscular, and other anatomic structures not fully examined during the traditional autopsy.
The logistics of imaging autopsy can be difficult. The decedent is transported on a gurney, covered in a body bag, to the CT and/or MRI scanner. This intra-hospital transport can be quite challenging and has to be carefully planned and executed so that the process of obtaining the imaging autopsy does not interfere with the care of other patients and does not cause potentially

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 19
Sharing Quality Science Worldwide…
significant emotional distress among the patients/personnel who may be simultaneously present in the patient holding area and/or the scanner room.1 Eventually, dedicated CT and/or MRI scanners may become available for the purpose of exclusively performing imaging autopsies. There is also a significant amount of controversy surrounding how and by whom imaging autopsies should be interpreted.1 This topic area is continuing to evolve and will most likely result in a multi-disciplinary approach to these complex and often difficult-to-interpret radiographic studies.1 It is likely that imaging autopsies in the future will involve cooperation between pathologists, radiologists, as well as the patient's primary physician. Such cooperation will enable the expertise of the radiologist and the pathologist to be used in conjunction with pertinent clinical information about the decedent provided by the primary physician.
WHY USE ADVANCED POSTMORTEM IMAGING?There are many reasons to perform imaging autopsy, including: (a) cause of death determination; (b) decedent gender identification in difficult forensic cases; (c) body length and individual decedent feature identification; (d) identifying distinct foreign bodies – retained bullets, blades, etc.; (e) identification of injuries and forensic reconstructions – three dimensional reconstructions, bullet tract identification; (f) education and clinical performance improvement process; and (g) research –from medical to historical (i.e., mummies, etc).1,6
Figure 3. Imaging autopsy of a patient who sustained lethal trans-cranial gunshot wound. Trajectory determination and detection of retained bullet fragments can be easily performed using CT-based IA techniques.
The concept of using CT and MRI technology to obtain autopsy information is slowly gaining popularity. The relatively slow acceptance of IA is likely related to certain medico-legal aspects, uncertainty over who should be responsible for interpreting such
studies, as well as the cost and reimbursement associated with these studies. In addition, the precise relationship between IA and traditional autopsy in terms of overall accuracy, overlap of findings, and missed findings remains to be fully described.1,30 Correlations between CT/MRI and traditional autopsy findings are certainly not perfect.1,30 While imaging autopsies are unlikely to ever match some of the histological and metabolic information available from traditional autopsies, it may be that for certain diseases radiographic postmortem examination may actually be superior. For example, in one study, CT identified the cause of death in 5 out of 20 decedents in which comparable information was still uncertain after traditional autopsy.34 Thus, postmortem imaging seems to be useful as an adjunct to the traditional postmortem examination.
As early as 1980, a comparison study was published of pre-mortem computed tomography of the brain and subsequent autopsy findings in premature and full-term neonates who suffered perinatal asphyxia.30 Since this sentinel work, significant amount of progress on imaging autopsies was made by research teams around the globe.4,35-36 While numerous studies support the notion that CT/MRI constitutes a useful method of obtaining autopsy information, the overall experience is still limited.2,37
When using CT/MRI in the setting of postmortem examination, cause-of-death determination rates vary between 49% and 91%, depending on the ability of these imaging modalities to “capture” relevant radiographic findings.2,30,38 For example, in a comparison study of pre-mortem CT and subsequent autopsy in neonates who suffered perinatal asphyxia, CT was able to detect subependymal hemorrhage and intraventricular hemorrhage in 91% of cases, with only a few small hemorrhages found on autopsy that weremissed on CT studies.30 However, the same study found that the accuracy of CT for intracerebral hemorrhage, subarachnoid hemorrhage, and ischemic brain injury was substantially lower (71%, 61%, and 49%, respectively).30
Postmortem imaging can demonstrate findings that are not readily recognized during the traditional autopsy. In one study, over 40% of postmortem CT exams were noted to have clinically significant findings that were not identified on traditional autopsy.4 In addition, CT and MRI autopsy techniques have revealed unexpected presence of air in various areas of the body and in the circulatory system [Figure 5].4,28 The significance of this gas remains to be determined although it has been postulated that it could represent air embolism and/or postmortem decay depending on its location and timing.4 In addition, modern CT/MRI technology is also capable of highly accurate estimation of individual solid organ weights, as verified by traditional postmortem examination findings.40
In the setting of forensic evaluation, three-dimensional surface scanning using multi-slice CT technology provides excellent visualization of injury patterns and allows re-examination of digital images of the decedent long after the actual time of death.5
Thali et al demonstrated how three-dimensional reconstructions based on radiographic autopsy allowed forensic data to be used in connecting decedent injury patterns to vehicle deformities.35 Two-and three-dimensional CT and MRI image reformatting is also very useful in determining bullet paths [Figures 3 and 9] and air emboli in the heart and blood vessels, as well as in demonstrating patterns of pulmonary blood aspiration in trauma victims.41
Finally, IA of severely deformed or charred bodies can provide

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 20
Sharing Quality Science Worldwide…
important clues with regards to the mechanism of injury and the cause of death.42
ADDITIONAL ADVANTAGES OF IMAGING AUTOPSYThere are numerous potential advantages to performing imaging autopsy. The most appealing aspects of IA include its noninvasive nature and the fact that radiation dosing is of no consideration when performing postmortem imaging studies. Imaging autopsies take only a few minutes on modern CT scanners and are reasonably brief when performed on modern MRI scanners.1
Imaging autopsies may be viewed remotely without loss of imaging detail, enabling sharing of imaging data among experts at different physical locations. Moreover, the ability to conduct repeated examinations of the acquired images make IA especially appealing as the examining physician is able to return, re-examine, and reconstruct (including three-dimensional reconstructions) the same information without losing any of the relevant pathologic information forever.1 Of importance, imaging autopsies do not require specialized facilities (i.e., autopsy rooms) other than one-time use of the imaging suite.
Additional advantages of IA utilizing modern visualization techniques include the ability to detect small fractures that may not be apparent on traditional autopsies, the ability to identify radiodense foreign bodies (i.e., bullets or blades) embedded deep within the soft tissues, and to clearly determine trajectories of penetrating injuries (i.e., bullets, knives, etc).1,6 The most advanced application of modern imaging is the ability to recreate realistic, three-dimensional anatomic reconstructions of injuries, a feature that is especially useful when relating the patterns of injury to various environmental factors at the time of death.1,41-42
Figure 4. Computed tomographic imaging autopsy showing a large subdural hematoma that was the direct cause of death in a pediatric patient.
LIMITATIONS OF IMAGING AUTOPSYThere are several limitations to modern imaging autopsies. First, radiographic autopsy techniques do not detect all causes of death.2,4,30,38 Second, certain relatively minor but critical findings can be “missed” on imaging autopsy studies – a problem that is less likely to occur as modern radiologic techniques continue to evolve and their accuracy improves.30 Included in this area is the fact that imaging autopsy lacks the ability to demonstrate active contrast extravasation or any other process that require metabolic and/or circulatory activity to be visualized.1 Thirdly, the great majority of IA experience reported to date comes from trauma andforensic medicine and it is unclear how CT and MRI techniques will be helpful in postmortem evaluations in the general medical/surgical population – a vast area open to further research. After all, while devastating traumatic injuries may be obvious on a “virtual” autopsy [Figures 2-4], causes of death due to certain medical conditions (i.e., metabolic disorders) may elude even the most specialized and sensitive imaging techniques.1 Lastly, certain imaging artifacts (i.e., intravascular or intrahepatic air) on postmortem CT/MRI studies are still being investigated and their meaning remains to be fully elucidated [Figure 5].40
Figure 5. Examples of abnormally located air found on postmortem computed tomographic examinations. The first image (top) shows intrahepatic venous gas. The second image (bottom) demonstrates intracardiac air. The precise meaning of such findings on imaging autopsies remains to be fully determined.

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 21
Sharing Quality Science Worldwide…
IMAGING AUTOPSY: COMPLEMENTARY TO TRADITIONAL AUTOPSYCurrently, imaging autopsies do not replace traditional autopsy, but they do offer complementary information and certain additional advantages. First, in one study over 40% of postmortem CT studies revealed clinically significant findings that were not identified on traditional autopsy.4 Second, IA offers excellent accuracy, including very close estimation of solid organ weights40, excellent visualization of penetrating projectile tract 41, and the ability to match decedent-environment relationships in fatal traumatic injuries.35 Third, imaging autopsies provide visualization of soft tissue patterns in cases of severe putrefaction. This is especially important when structural patterns are not otherwise distinguishable on traditional autopsy.6
SUMMARY OF IMPORTANT IMAGING AUTOPSY STUDIESIn 1994, Donchin et al performed CT imaging of 25 trauma victims within six hours of the time of death.32 The study blinded radiologists and pathologists to each others' examination findings and interpretations. Out of the total 127 pathologic findings, 45% were seen on both traditional and imaging autopsy, 30% were missed on CT scanning, and 25% were missed on traditional autopsy.32 Overall, IA demonstrated approximately 71% of findings and traditional autopsy demonstrated nearly 75% of findings. In terms of specific types of findings, computed tomography appeared to be superior for skeletal injuries. Although not more effective than traditional autopsy, IA increased the overall yield of significant pathologic findings when combined with the traditional autopsy.32
Figure 6. Postmortem CT imaging of a blunt trauma patient who was involved in high-speed automobile collision. This case was characterized by prolonged extrication from the vehicle and loss of vital signs in the field. Imaging autopsy demonstrated right-sided tension pneumothorax.
Using both multi-slice computed tomography (MSCT) and MRI, Thali et al found in a 2003 study that 55% of causes of death were found independently using only radiographic data.41 The authors reported that IA may be superior to traditional autopsy in revealing certain types of cranial, skeletal, and soft tissue trauma.41 Further research from the same group demonstrated that imaging autopsy using both MSCT and MRI may be superior to traditional autopsy in demonstrating the extent and distribution of gas in intraparenchymal blood vessels, internal organs, and in various body regions that are poorly accessible to standard autopsy.39
Aghayev et al described the use of both MSCT and MRI to document herniation of cerebellar tonsils prior to traditional autopsy in patients with blunt head injuries.43 The same group also advocated postmortem imaging as a good forensic visualization tool for documentation and examination of traumatic injuries and other pathologic findings in a broad range of scenarios.43-45 Recent reports also describe the use of CT image-guided techniques for postmortem tissue sampling.46 Jackowski et al point to the fact that the ability to use more radiation leads to better image quality in postmortem radiographic examinations, without concern for biologic effects of ionizing radiation.47
Using mobile CT imaging units to determine the accuracy of superficial autopsies, Hayakawa et al found that the cause of death as demonstrated by IA was different from that determined by superficial postmortem examination in 25% of cases.48 The authors describe a case of a traumatic subdural hematoma found on CT images in the setting of superficial examination suggesting no traumatic injury.48
Oyake et al conducted an IA study to help determine the etiology of sudden death due to non-traumatic causes in infants and children. Imaging autopsies in that study were able to point to the cause of death in 14 of 15 decedents when radiographic information was combined with premortem clinical and laboratory data.49
In 2007, Levy et al published a series of postmortem CT examinations of military air mishap victims.50 In that study, pockets of ectopic air in various anatomic areas were found in 24% of victims.50 The authors point out that significance of such ectopic air is still unclear. Of note, they also noted that detection of solid organ injury and superficial trauma were significantly worse on CT than on a traditional autopsy, corroborating the complementary character of IA studies.50
Also in 2007, Hoey et al published a series of postmortem CT examinations of trauma victims.4 When comparing imaging autopsies to traditional postmortem examinations, the study showed that imaging correctly identified the cause of death in 83% of decedents and revealed as many as 40% of clinically significant findings that were not recognized on traditional autopsies.4 The authors strongly advocate for the use of IA as a clinical performance improvement tool in the setting of trauma.
THE ROLE OF IMAGING AUTOPSY IN MEDICAL EDUCATIONSadly, fewer than half of American medical schools require autopsy attendance, and most medical students complete their medical education without attending a single session.51 The gradual abandonment of the use of autopsy as an educational tool

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 22
Sharing Quality Science Worldwide…
was paralleled by significantly fewer postmortem examinations being performed around the globe.22 Some postulate that part of the reason why autopsy rates are decreasing is the widespread use of advanced imaging techniques in modern clinical practice (i.e., clinicians often know the most likely cause of death from pre-mortem high-definition imaging studies).1
At the same time, contemporary imaging techniques present a unique opportunity to “resuscitate” the concept of autopsy in medical and surgical education – this time in the form of imaging autopsy.1,18 This makes even more sense when one considers that while most medical students regard autopsies as educationally useful, nearly 20% of students find traditional autopsies to be “distasteful”.52 Image-based autopsy makes the cause-of-death determination process much less invasive and certainly much more “acceptable” to both the decedent’s family and the participating physician or medical trainee. In addition, the routine performance of IA could also help build an atmosphere of interdisciplinary cooperation between radiologists, pathologists, and primary physicians involved in clinical care of the decedent prior to his or her death [Figure 7].
Medical and surgical education stands to benefit greatly from the use of non-invasive imaging techniques in cause-of-death determination. All too often, the reason for the patient’s demise can only be an “educated guess”. As discussed previously, such “guesstimates” are frequently inaccurate.26-28 Information obtained from imaging autopsies offers the potential to do away with such guesswork. As already being done at several medical centers, imaging autopsies are proving to be very valuable during the process of performance improvement and confidential peer-review.4
Figure 7. Interdisciplinary character of imaging autopsy. Skills of the radiologist and the pathologist are augmented by the clinical knowledge provided by the primary physician. After the imaging autopsy is completed, direct feedback facilitates continued clinical education.
RECOMMENDATIONS AND POTENTIAL FUTURE DIRECTIONSAt present, the evidence is insufficient to abandon the tradition autopsy and rely exclusively on imaging autopsy. Published studies looking at the use of modern imaging technologies for cause-of-death determination are few in number and the experience with the technology and what it offers in the context of postmortem analysis is still limited. As our understanding of IA grows, we will learn where it fits best into the currently established paradigm.4 Moreover, one has to consider who will be interpreting these studies and how exactly will this process occur, both in relation to the traditional autopsy and within the framework of the inter-disciplinary nature of such an endeavor. Ultimately, the IA may supplement or even replace its more invasive counterpart in various subsets of patients, contingent upon continued technological advances and improvements in our ability to reveal the cause of death using radiographic means. Most likely, imaging autopsy will evolve to become an important adjunct and a quality improvement tool in cases where a traditional autopsy is performed, but it may also assume more primary role in cases where traditional autopsy was declined or otherwise not feasible.
Figure 8. Proposed algorithm for the use of imaging autopsy in medical and surgical education. *Note that the role of imaging autopsy in the setting of failure of traditional autopsy to determine the cause of death is limited largely to the examination of skeletal, muscular, and other anatomic areas not fully examined during the traditional autopsy.
Imaging autopsy may be offered as an alternative to traditional autopsy in the pediatric population, especially when there is parental reluctance to give permission to perform an autopsy.53
This is especially important when considering that additional diagnostic information can be obtained in as many as one third of pediatric deaths upon the performance of an autopsy.53 In other situations, traditional autopsy may be refused because of religious,
OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 23
Sharing Quality Science Worldwide…
social, cultural and/or personal beliefs.54-55 Here, imaging autopsy may offer a non-invasive alternative of discovering the cause of death and perhaps providing answers where none would have been known otherwise.55 In such cases, IA may also have potentially important implications with regards to confidential peer-review and clinical performance improvement.4
Finally, medical and surgical education programs stand to benefit greatly from more widespread use of imaging autopsy. Knowing why the patient died is instrumental to our medical education paradigm. A proposed algorithm for the utilization of CT/MRI autopsy in medical/surgical education has been previously published by our group [Figure 8].1
CONTROVERSIESWhile promising, IA studies involve a number of controversial issues. First, who should be responsible for obtaining and interpreting these studies? Should pathologists be trained to read radiographic studies or should radiologists have the domain over the CT and MRI autopsy studies? All these questions remain to be answered, and the most likely solution will be some form of inter-disciplinary cooperation.1,14
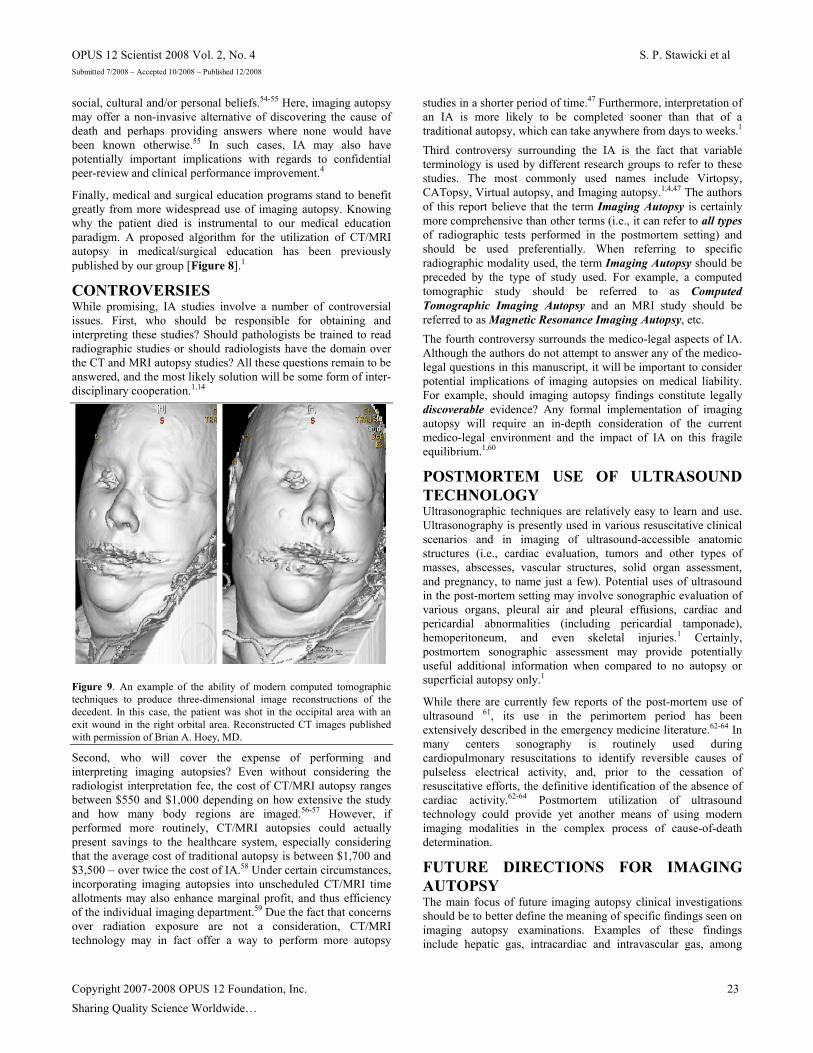
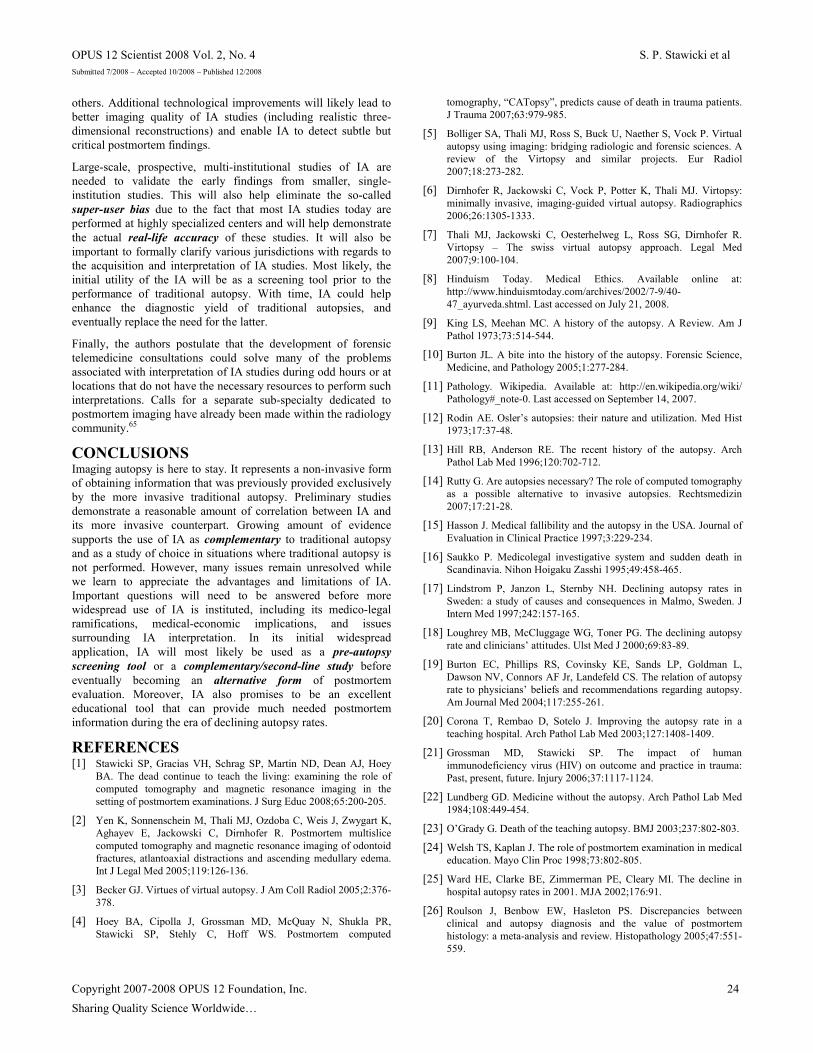
Figure 9. An example of the ability of modern computed tomographic techniques to produce three-dimensional image reconstructions of the decedent. In this case, the patient was shot in the occipital area with an exit wound in the right orbital area. Reconstructed CT images published with permission of Brian A. Hoey, MD.
Second, who will cover the expense of performing and interpreting imaging autopsies? Even without considering the radiologist interpretation fee, the cost of CT/MRI autopsy ranges between $550 and $1,000 depending on how extensive the study and how many body regions are imaged.56-57 However, if performed more routinely, CT/MRI autopsies could actually present savings to the healthcare system, especially considering that the average cost of traditional autopsy is between $1,700 and $3,500 – over twice the cost of IA.58 Under certain circumstances, incorporating imaging autopsies into unscheduled CT/MRI time allotments may also enhance marginal profit, and thus efficiency of the individual imaging department.59 Due the fact that concerns over radiation exposure are not a consideration, CT/MRI technology may in fact offer a way to perform more autopsy
studies in a shorter period of time.47 Furthermore, interpretation of an IA is more likely to be completed sooner than that of a traditional autopsy, which can take anywhere from days to weeks.1
Third controversy surrounding the IA is the fact that variable terminology is used by different research groups to refer to these studies. The most commonly used names include Virtopsy, CATopsy, Virtual autopsy, and Imaging autopsy.1,4,47 The authors of this report believe that the term Imaging Autopsy is certainly more comprehensive than other terms (i.e., it can refer to all typesof radiographic tests performed in the postmortem setting) and should be used preferentially. When referring to specific radiographic modality used, the term Imaging Autopsy should be preceded by the type of study used. For example, a computed tomographic study should be referred to as Computed Tomographic Imaging Autopsy and an MRI study should be referred to as Magnetic Resonance Imaging Autopsy, etc.
The fourth controversy surrounds the medico-legal aspects of IA. Although the authors do not attempt to answer any of the medico-legal questions in this manuscript, it will be important to consider potential implications of imaging autopsies on medical liability. For example, should imaging autopsy findings constitute legally discoverable evidence? Any formal implementation of imaging autopsy will require an in-depth consideration of the current medico-legal environment and the impact of IA on this fragile equilibrium.1,60
POSTMORTEM USE OF ULTRASOUND TECHNOLOGYUltrasonographic techniques are relatively easy to learn and use. Ultrasonography is presently used in various resuscitative clinical scenarios and in imaging of ultrasound-accessible anatomic structures (i.e., cardiac evaluation, tumors and other types of masses, abscesses, vascular structures, solid organ assessment, and pregnancy, to name just a few). Potential uses of ultrasound in the post-mortem setting may involve sonographic evaluation of various organs, pleural air and pleural effusions, cardiac and pericardial abnormalities (including pericardial tamponade), hemoperitoneum, and even skeletal injuries.1 Certainly, postmortem sonographic assessment may provide potentially useful additional information when compared to no autopsy or superficial autopsy only.1
While there are currently few reports of the post-mortem use of ultrasound 61, its use in the perimortem period has been extensively described in the emergency medicine literature.62-64 In many centers sonography is routinely used during cardiopulmonary resuscitations to identify reversible causes of pulseless electrical activity, and, prior to the cessation of resuscitative efforts, the definitive identification of the absence of cardiac activity.62-64 Postmortem utilization of ultrasound technology could provide yet another means of using modern imaging modalities in the complex process of cause-of-death determination.
FUTURE DIRECTIONS FOR IMAGING AUTOPSYThe main focus of future imaging autopsy clinical investigations should be to better define the meaning of specific findings seen on imaging autopsy examinations. Examples of these findings include hepatic gas, intracardiac and intravascular gas, among
OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 24
Sharing Quality Science Worldwide…
others. Additional technological improvements will likely lead to better imaging quality of IA studies (including realistic three-dimensional reconstructions) and enable IA to detect subtle but critical postmortem findings.
Large-scale, prospective, multi-institutional studies of IA are needed to validate the early findings from smaller, single-institution studies. This will also help eliminate the so-called super-user bias due to the fact that most IA studies today are performed at highly specialized centers and will help demonstrate the actual real-life accuracy of these studies. It will also be important to formally clarify various jurisdictions with regards to the acquisition and interpretation of IA studies. Most likely, the initial utility of the IA will be as a screening tool prior to the performance of traditional autopsy. With time, IA could help enhance the diagnostic yield of traditional autopsies, and eventually replace the need for the latter.
Finally, the authors postulate that the development of forensic telemedicine consultations could solve many of the problems associated with interpretation of IA studies during odd hours or at locations that do not have the necessary resources to perform such interpretations. Calls for a separate sub-specialty dedicated to postmortem imaging have already been made within the radiology community.65
CONCLUSIONSImaging autopsy is here to stay. It represents a non-invasive form of obtaining information that was previously provided exclusively by the more invasive traditional autopsy. Preliminary studies demonstrate a reasonable amount of correlation between IA and its more invasive counterpart. Growing amount of evidence supports the use of IA as complementary to traditional autopsy and as a study of choice in situations where traditional autopsy is not performed. However, many issues remain unresolved while we learn to appreciate the advantages and limitations of IA. Important questions will need to be answered before more widespread use of IA is instituted, including its medico-legal ramifications, medical-economic implications, and issues surrounding IA interpretation. In its initial widespread application, IA will most likely be used as a pre-autopsy screening tool or a complementary/second-line study before eventually becoming an alternative form of postmortem evaluation. Moreover, IA also promises to be an excellent educational tool that can provide much needed postmortem information during the era of declining autopsy rates.
REFERENCES[1] Stawicki SP, Gracias VH, Schrag SP, Martin ND, Dean AJ, Hoey
BA. The dead continue to teach the living: examining the role of computed tomography and magnetic resonance imaging in the setting of postmortem examinations. J Surg Educ 2008;65:200-205.
[2] Yen K, Sonnenschein M, Thali MJ, Ozdoba C, Weis J, Zwygart K, Aghayev E, Jackowski C, Dirnhofer R. Postmortem multislice computed tomography and magnetic resonance imaging of odontoid fractures, atlantoaxial distractions and ascending medullary edema. Int J Legal Med 2005;119:126-136.
[3] Becker GJ. Virtues of virtual autopsy. J Am Coll Radiol 2005;2:376-378.
[4] Hoey BA, Cipolla J, Grossman MD, McQuay N, Shukla PR, Stawicki SP, Stehly C, Hoff WS. Postmortem computed
tomography, “CATopsy”, predicts cause of death in trauma patients. J Trauma 2007;63:979-985.
[5] Bolliger SA, Thali MJ, Ross S, Buck U, Naether S, Vock P. Virtual autopsy using imaging: bridging radiologic and forensic sciences. A review of the Virtopsy and similar projects. Eur Radiol 2007;18:273-282.
[6] Dirnhofer R, Jackowski C, Vock P, Potter K, Thali MJ. Virtopsy: minimally invasive, imaging-guided virtual autopsy. Radiographics 2006;26:1305-1333.
[7] Thali MJ, Jackowski C, Oesterhelweg L, Ross SG, Dirnhofer R. Virtopsy – The swiss virtual autopsy approach. Legal Med 2007;9:100-104.
[8] Hinduism Today. Medical Ethics. Available online at: http://www.hinduismtoday.com/archives/2002/7-9/40-47_ayurveda.shtml. Last accessed on July 21, 2008.
[9] King LS, Meehan MC. A history of the autopsy. A Review. Am J Pathol 1973;73:514-544.
[10] Burton JL. A bite into the history of the autopsy. Forensic Science, Medicine, and Pathology 2005;1:277-284.
[11] Pathology. Wikipedia. Available at: http://en.wikipedia.org/wiki/Pathology#_note-0. Last accessed on September 14, 2007.
[12] Rodin AE. Osler’s autopsies: their nature and utilization. Med Hist 1973;17:37-48.
[13] Hill RB, Anderson RE. The recent history of the autopsy. Arch Pathol Lab Med 1996;120:702-712.
[14] Rutty G. Are autopsies necessary? The role of computed tomography as a possible alternative to invasive autopsies. Rechtsmedizin 2007;17:21-28.
[15] Hasson J. Medical fallibility and the autopsy in the USA. Journal of Evaluation in Clinical Practice 1997;3:229-234.
[16] Saukko P. Medicolegal investigative system and sudden death in Scandinavia. Nihon Hoigaku Zasshi 1995;49:458-465.
[17] Lindstrom P, Janzon L, Sternby NH. Declining autopsy rates in Sweden: a study of causes and consequences in Malmo, Sweden. J Intern Med 1997;242:157-165.
[18] Loughrey MB, McCluggage WG, Toner PG. The declining autopsy rate and clinicians’ attitudes. Ulst Med J 2000;69:83-89.
[19] Burton EC, Phillips RS, Covinsky KE, Sands LP, Goldman L, Dawson NV, Connors AF Jr, Landefeld CS. The relation of autopsy rate to physicians’ beliefs and recommendations regarding autopsy. Am Journal Med 2004;117:255-261.
[20] Corona T, Rembao D, Sotelo J. Improving the autopsy rate in a teaching hospital. Arch Pathol Lab Med 2003;127:1408-1409.
[21] Grossman MD, Stawicki SP. The impact of human immunodeficiency virus (HIV) on outcome and practice in trauma: Past, present, future. Injury 2006;37:1117-1124.
[22] Lundberg GD. Medicine without the autopsy. Arch Pathol Lab Med 1984;108:449-454.
[23] O’Grady G. Death of the teaching autopsy. BMJ 2003;237:802-803.
[24] Welsh TS, Kaplan J. The role of postmortem examination in medical education. Mayo Clin Proc 1998;73:802-805.
[25] Ward HE, Clarke BE, Zimmerman PE, Cleary MI. The decline in hospital autopsy rates in 2001. MJA 2002;176:91.
[26] Roulson J, Benbow EW, Hasleton PS. Discrepancies between clinical and autopsy diagnosis and the value of postmortem histology: a meta-analysis and review. Histopathology 2005;47:551-559.

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 25
Sharing Quality Science Worldwide…
[27] Shojania KG, Burton EC, McDonald KM, Goldman L. Changes in rates of autopsy-detected diagnostic errors over time: a systematic review. JAMA 2003;289:2849-2856.
[28] Combes A, Mokhtari M, Couvelard A, Trouillet JL, Baudot J, Henin D, Gilbert C, Chastre J. Clinical and autopsy diagnoses in the intensive care unit: a prospective study. Arch Intern Med 2004;164:389-392.
[29] Wullenweber R, Schenider V, Grumme T. A computer-tomographical examination of cranial bullet wounds. Z Rechtsmed 1977;80:227-246.
[30] Flodmark O, Becker LE, Harwood-Nash DC, Fitzhardinge PM, Fitz CR, Chuang SH. Correlation between computed tomography and autopsy in premature and full-term neonates that have suffered perinatal asphyxia. Radiology. 1980;137:93-103.
[31] Kalender WA, Seissler W, Klotz E, Vock P. Spiral volumetric CT with single-breath-hold technique, continuous transport, and continuous scanner rotation. Radiology 1990;176:181-183.
[32] Donchin Y, Rivkind AI, Bar-Ziv J, Hiss J, Almog J, Drescher M. Utility of postmortem computed tomography in trauma victims. J Trauma 1994;37:552–555.
[33] Levy AD, Abbott RM, Mallak CT, Getz JM, Harcke HT, Champion HR, Pearse LA. Virtual autopsy: preliminary experience in high-velocity gunshot wound victims. Radiology 2006;240:522.
[34] Hayakawa M, Yamamoto S, Motani H, Yajima D, Sato Y, Iwase H. Does imaging technology overcome problems of conventional postmortem examination? A trial of computed tomography imaging for postmortem examination. Int J Legal Med 2006;120:24-26.
[35] Thali MJ, Braun M, Buck U, Aghayev E, Jackowski C, Vock P, Sonnenschein M, Dirnhofer R. Virtopsy - scientific documentation, reconstruction and animation in forensic: individual and real 3D data based geo-metric approach including optical body/object surface and radiological CT/MRI scanning. J Forensic Sci 2005;50:428-442.
[36] Levy AD, Harcke HT, Getz JM, Mallak CT, Caruso JL, Pearse L, Frazier AA, Galvin JR. Virtual autopsy: Two- and three-dimensional multidetector CT findings in drowning with autopsy comparison. Radiology 2007;243:862-868.
[37] Paperno S, Riepert T, Grug B, Rotschild MA, Schultes A, Staak M, Lackner L. Value of postmortem computed tomography in comparison to autopsy. Rofo 2005;177:130-136.
[38] Thali MJ, Yen K, Schweitzer W, Vock P, Boesch C, Ozdoba C, Schroth G, Ith M, Sonnenschein M, Doernhoefer T, Scheurer E, Plattner T, Dirnhofer R. Virtopsy, a new imaging horizon in forensic pathology: virtual autopsy by postmortem multislice computed tomography (MSCT) and magnetic resonance imaging (MRI) – a feasibility study. J Forensic Sci 2003;48:386-403.
[39] Plattner T, Thali MJ, Yen K, Sonnenschein M, Stoupis C, Vock P, Zwygart-Brugger K, Kilchor T, Dirnhofer R. Virtopsy-postmortem multislice computed tomography (MSCT) and magnetic resonance imaging (MRI) in a fatal scuba diving incident. J Forensic Sci 2003;48:1347-1355.
[40] Jackowski C, Thali MJ, Buck U, Aghayev E, Sonnenschein M, Yen K, Dirnhofer R, Vock P. Noninvasive estimation of organ weights by postmortem magnetic resonance imaging and multislice computed tomography. Invest Radiol 2006;41:572-578.
[41] Thali MJ, Yen K, Vock P, Ozdoba C, Kneubuehl BP, Sonnenchein M, Dirnhofer R. Image-guided autopsy findings of gunshot victims performed with multi-slice computed tomography and magnetic resonance imaging and subsequent correlation between radiology and autopsy findings. Forensic Sci Int 2003;138:8-16.
[42] Thali MJ, Yen K, Plattner T, Schweitzer W, Vock P, Ozdoba C, Dirnhofer R. Charred body: virtual autopsy with multi-slice computed tomography and magnetic resonance imaging. J Forensic Sci 2002;47:1326-1331.
[43] Aghayev E, Yen K, Sonnenschein M, Ozdoba C, Thali M, Jackowski C, Dirnhofer R. Virtopsy post-mortem multi-slice computed tomography (MSCT) and magnetic resonance imaging (MRI) demonstrating descending tonsillar herniation: comparison to clinical studies. Neuroradiology 2004;46:559–564.
[44] Aghayev E, Christe A, Sonnenschein M, Yen K, Jackowski C, Thali MJ, Dirnhofer R, Vock P. Postmortem imaging of blunt chest trauma using CT and MRI: comparison with autopsy. J Thorac Imaging 2008;23:20-27.
[45] Aghayev E, Thali MJ, Jackowski C, Sonnenschein M, Dirnhofer R, Yen K. MRI detects hemorrhages in the muscles of the back in hypothermia. Forensic Sci Int 2008;176:183-186.
[46] Aghayev E, Thali MJ, Sonnenschein M, Jackowski C, Dirnhofer R, Vock P. Post-mortem tissue sampling using computed tomography guidance. Forensic Sci Int 2007;166:199-203.
[47] Jackowski C, Schweitzer W, Thali M, Yen K, Aghayev E, Sonnenschein M, Vock P, Dirnhofer R. Virtopsy: postmortem imaging of the human heart in situ using MSCT and MRI. Forensic Sci Int 2005;149:11-23.
[48] Hayakawa M, Yamamoto S, Motani H, Yajima D, Sato Y, Iwase H. Does imaging technology overcome problems of conventional postmortem examination? A trial of computed tomography imaging for postmortem examination. Int J Legal Med 2006;120:24-26.
[49] Oyake Y, Aoki T, Shiotani S, Kohno M, Ohashi N, Akutsu H, Yamazaki K. Postmortem computed tomography for detectingcauses of sudden death in infants and children: retrospective review of cases. Radiat Med 2006;24:493-502.
[50] Levy G, Goldstein L, Blachar A, Apter S, Barenboim E, Bar-Dayan Y, Shamis A, Atar E. Postmortem computed tomography in victims of military air mishaps: radiological-pathological correlation of CT findings. Isr Med Assoc J 2007;9:699-702.
[51] Anderson RE, Hill RB. The current status of the autopsy in academic medical centers in the United States. Am J Clin Pathol 1989;92:S31-37.
[52] Benbow EW. Medical students’ views on necropsies. J Clin Pathol 1990;43:969-976.
[53] Kumar P, Taxy J, Angst DB, Mangurten HH. Autopsies in children: Are they still useful? Arch Pediatr Adolesc Med 1998;152:558-563.
[54] Lishimpi K, Chintu C, Lucas S, Mudenda V, Kaluwaji J, Story A, Maswahu D, Bhat G, Nunn AJ, Zumla A. Necropsies in African children: consent dilemmas for parents and guardians. Arch Dis Child 2001;84:463-467.
[55] Versweyveld L. Forensic radiology makes minimally invasive virtual autopsy a reality. Available at: http://www.hoise.com/vmw/04/articles/vmw/LV-VM-01-04-4.html. Last accessed on September 14, 2007.
[56] Bone, Joints, and Muscles Center: Imaging Studies. Available at: http://health.usnews.com/usnews/health/bones/back-pain/back.test.imaging.htm. Last accessed on September 14, 2007.
[57] Your health. Your answers. Your scan. Available at: http://www.yourscan.com/faq.html. Last accessed on September 14, 2007.
[58] Northwest autopsy services. Why an autopsy? Available at: http://www.emphasis-technography.com/nas/page3.htm. Last accessed on September 14, 2007.

OPUS 12 Scientist 2008 Vol. 2, No. 4 S. P. Stawicki et alSubmitted 7/2008 – Accepted 10/2008 – Published 12/2008
Copyright 2007-2008 OPUS 12 Foundation, Inc. 26
Sharing Quality Science Worldwide…
[59] Forman HP, Yin D. Cost analysis and the practicing radiologist/manager: an introduction to managerial accounting. AJR Am J Roentgenol 1996;166:1249-1253.
[60] Dippolito A, Braslow BM, Lombardo G, Hoddinott KM, Nace G, Stawicki SP. How david beat goliath: history of physicians fighting frivolous lawsuits. OPUS 12 Scientist 2008;2(1):1-8.
[61] Uchigasaki S. Postmortem ultrasound imaging in forensic pathology. Forensic Pathology Reviews 2006;4:405-412.
[62] Hendrickson RG, Dean AJ, Costantino TG. A novel use of ultrasound in pulseless electrical activity: the diagnosis of an acute abdominal aortic aneurysm rupture. J Emerg Med 2001;21:141-144.
[63] Salen P, O’Connor R, Sierzenski P, Passarello B, Pancu D, Melanson S, Arcona S, Reed J, Heller M. Can cardiac sonography and capnography be used independently and in combination to predict resuscitation outcomes? Acad Emerg Med 2001;8:610-615.
[64] Blavais M, Fox JC. Outcome in cardiac arrest patients found to have cardiac standstill on the bedside emergency department echocardiogram. Acad Emerg Med 2001;8:616-621.
[65] O’Donnell C, Woodford N. Post-mortem radiology – a new sub-specialty? Clin Radiol 2008;63:1189-1194.
Permission to make digital or hard copies of all or part of this work for personal or classroom use is granted without fee provided that copies are not made or distributed for profit and that copies bear this notice and the full citation on the first page. To copy otherwise, or republish, to post on servers or to redistribute to lists, requires prior permission and/or a $5.00 fee.
OPUS 12 Scientist – A Quarterly Publication of OPUS 12 Foundation.© 2007-2008 OPUS 12 Foundation, Inc., Columbus, OH 43235 USA.


















