
Postgraduate program in Endodontics - Forside · Case 8 Endodontic treatment of mandibular left...
148
1 UNIVERSITY OF OSLO DENTAL FACULTY Department of Endodontics Postgraduate program in Endodontics CASE BOOK by Nabeel Mekhlif Case book in partial fulfillment of the requirements for diploma of specialist training in endodontics Supervisor: Dag Ørstavik Spring Semester 2007
-
Upload
phungthuan -
Category
Documents
-
view
215 -
download
1
Transcript of Postgraduate program in Endodontics - Forside · Case 8 Endodontic treatment of mandibular left...

1
UNIVERSITY OF OSLO DENTAL FACULTY Department of Endodontics Postgraduate program in Endodontics CASE BOOK by Nabeel Mekhlif Case book in partial fulfillment of the requirements for diploma of specialist training in endodontics Supervisor: Dag Ørstavik Spring Semester 2007

2
Contents Surgical Cases Case 1 Apicoectomy of maxillary right central incisor 3- 10 Case 2 Endodontic treatment of mandibular left first premolar
in conjunction with apical surgery 11- 18 Case 3 Endodontic re-treatment of mandibular left first molar
in conjunction with apical surgery 19- 28 Case 4 Apicoectomi of maxillary left first premolar 29- 36 Case 5 Surgical extraction of root canal treated tooth with
vertical root fracture 37- 42 Non-surgical cases Vital cases Case 6 Endodontic treatment of mandibular left first molar with
external root resorption 43- 51 Case 7 Endodontic treatment of maxillary central incisors
with obliteration and in cooperation with prosthodontist 52- 58 Case 8 Endodontic treatment of mandibular left canine
in a medically compromised patient 59- 65 Case 9 Endodontic treatment of dens invaginatus maxillary
right lateral incisor with vital tooth 66- 74

3
Non-vital cases Case 10 Treatment of maxillary right first molar with obliteration 75- 81
Case 11 Endodontic treatment of mandibular right second molar 82- 88 Case 12 Treatment of mandibular left canine with lateral
periapical lesion and suspicious about root resorpsion 89- 94 Case13 Endodontic treatment of maxillary right second molar with two canals 95- 100 Case 14 Endodontic treatment of mandibular left second molar with one visit 101- 106
Case 15 Endodontic treatment of dens invaginatus in maxillary
left later incisor with chronic apical periodontitis 107- 112
Re-treatment cases Case 16 Endodontic re-treatment of mandibular left
second molar in severely distructed tooth 113- 118 Case 17 Endodontic re-treatment of mandibular right
first molar with separated instrument 119- 125 Case 18 Endodontic re-treatment of endodontically treated
mandibular left second molar with perforation 126- 133 Case 19 Endodontic re-treatment of maxillary left central incisor
with sinus tract and use of a novel root filling material 134- 140 Case 20 Endodontic re-treatment of endodontically treated
maxillary left second molar with symptoms 141- 147

4
Case 1 Apicoectomy of maxillary right central incisor Patient
80 years Old Norwegian male (Fig.1) was referred to the Department of Endodontics, University of Oslo, by his dental undergraduate student for treatment of maxillary right central incisor.
Fig.1 frontal view Medical history
The patient uses Albyl- E as a prophylaxis against heart infarction. Dental history and chief complain
The patient had slight intermediate pain. The pain becomes more spontaneous on the last 3 weeks. He had pain with percussion and with palpation of the buccal area adjacent to the apex of the tooth. He feels that the area is slightly swollen. He is very satisfied with the bridge that he got about 20 years ago. Clinical examination
Preoperative photos show the region of the anterior segment (Fig.2) and the palatal surfaces of the anterior teeth. (Fig.3)
Fig.2 Buccal view Fig.3 Palatinal/ incisal view

5
A normal oral mucosa was observed. No extra oral pathosis was found.
Maxillary right first premolar: A metal ceramic restoration. Maxillary right canine : A metal ceramic restoration Maxillary right lateral incisor: A metal ceramic restoration (pontic) Maxillary right central incisor: A metal ceramic restoration. The tooth was tender to
percussion and palpation, and responded negative to electrical sensibility test. Maxillary left central incisor: A metal ceramic restoration (pontic) Maxillary left lateral incisor: A metal ceramic restoration Maxillary left canine : Amalgam filling on the distal surface Maxillary left first premolar: A metal crown with full ceramic restoration
The other teeth in the upper and lower quadrants showed no signs relevant to the chief
complaint. The gingival margin was healthy, and the probing depths were within normal limits. For tooth 11, the gingival margin was slightly inflamed. Radiographic examination
The preoperative radiograph shows area from the extracted maxillary right lateral incisor to the mesial side of the maxillary left lateral incisor. (Fig.4)
Fig.4 Radiographic photo Maxillary right central incisor: the tooth is an abutment for the bridge. Under the margins of the crown, there is a large radio-opaque filling material on both sides of the root. A radio-opaque post can be seen in the canal. No radiographic sign for a root filling material inside the canal could be detected. Lamina dura can be followed around the entire root where it widend to a radiolucent area of approximately 4-5 mm.

6
Diagnosis Acute apical periodontitis of the maxillary right central incisor (K04.50).
Treatment plan
The clinical examination showed no dental pocket. The patient was satisfied with the bridge. He refused to do any treatment that can damage the bridge. The treatment decision was Apicoectomy with retrograde filling. The patient’s doctor have been consulted for the Albyl-E, the patient cut the medicin 3 days before surgery day. Treatment 26.04.2005 The day of surgery Three carpules with Xylocain with Adrenalin (20 mg/ml + 12.5 μg/ml) were used to establish anaesthesia. An incision was made with a scalpel blade nr 15C starting with a vertical releasing incision, starting from the mesiobuccal gingival line angle of the maxillary right central incisor approximately 1 cm in a superior aspect of the oral buccal mucosa. An intrasulcular incision extending from the releasing incision to the distal aspect of maxillary right canine.
Elevation of the full mucoperiostal flap was initiated with an nr 149 periostal elevator.
The flap was carefully elevated at the junction between the vertical releasing incision and horizontal incision extending apical and lateral. A retractor was used facilitating the reflection of the flap. Bone fenestration was detected outside the root (Fig.5). The lesion was removed with periodontal curettes. 2 mm of the root apex was resected with a long fissure bur.
Fig.5 fenestration to the bone
A retrograde preparation was carried out with the piezoelectric Satelec ultrasound device using a pre-bended K- file 30 under constant cooling with rinsing sterile saline (Fig.6).
The cavity was extended up to 5 mm in the root canal and followed the canal wall all the time. A microscope was being used most of the time in order to achieve maximal visibility. Stryphnon gauze was placed in the bone cavity in order to achieve haemostasis.

7
The cavity was then irrigated with sterile saline and dried with sterile paper points. A retrograde MTA filling was placed into the cavity using plastic instrument as a carrier, and condensed with micro condensing pluggers. A burnisher was used at the end. The retro-filling was examined under high magnification with an explorer to check marginal adaptation and integrity.
Fig.6 cleaning the canal retrogrades
The Stryphnon gauze was removed. The surgical field was irrigated with sterile saline. The flap was repositioned and was hold tight in place with finger pressure for five minutes in order to reduce the post operative haematoma and pain. The vertical realising flap was sutured in place with two 4-0 silk suture. The three other interrupted sutures were placed inter-approximaly in the papilla (Fig.7). A final radiograph was taken (Fig.8) and the patient received an ice pack to reduce post operative haematoma and pain. The pain killer Ibuprofen; Ibux 600 mg, was prescribed and the antiseptic mouthwash Corsodyl. Post operative instructions were given.

8
Fig.7 Sutures in place Fig.8 Final radiograph
One week after surgery 03.05.2005
The patient returned back for removal of the sutures. He had severe pain for about 3 days after operation. He was disappointed about the results. The clinical photo showed a slight inflammation in the gingival margin of the area (Fig.9). He got a new appointment for control.
Fig.9 After one week
Five weeks after surgery 29.05.2006
The patient returned for a second control after surgery. Clinical examination showed a good healing of the gingiva, and the symptoms diminished almost completely. A slight gingival retraction could be noticed on the buccal side of the teeth.

9
Fig. 10 Five weeks after surgery
Evaluation The retrograde filling is dens and seems to follow the original canal.
Prognosis
The prognosis is considered to be favourable. 10 months follow up
The patient returned after ten months for control. He had no symptoms. The clinical examination showed a normal gingival margin. The radiograph showed a favourable healing also (Fig.11, and 12).
Fig.11 frontal view Fig.12 follow up radiograph

10
Discussion It was important for the patient to keep the bridge safe and without damage. The
choice to do apical surgery was done because of the post size and the negative results on removing tooth substances while removing the post.
The presence of a post in a root was also a common reason to recommend periapical surgery to treat failed cases rather than attempting to remove the post and complete root canal re-treatment, even though the success rate of retreatment is considered to be higher than for surgery (1, 6).
Apical surgery offers immediate access to the root apex. The periapical pathological tissues are removed by apical curettage and the apical portion of the root, which frequently contains infected canal ramifications (5, 6). Importantly, at surgery the prepared apical canals and exposed isthmuses and accessory canals (9,10) should be carefully located and prepared with the aid of a surgical operation microscope and micro mirror (8), and then irrigated ultrasonically to remove bacteria, debris and smear layer prior to their filling (5). Ninety-seven per cent of the lesions including those >10 mm in diameter completely healed within 1 year after effective apical surgery (8). Ideally, apical surgery and orthograde retreatment should be performed simultaneously (4) because endodontic surgery is not a long-term solution for inadequate orthograde root canal treatment (8).
The use of the prebended K- file may be reducing the damage to the root end structure. This instrument is more flexible and no extra pressure can apply because of fracture risk. This technique allowing the preparation to follow the direction of the original root canal as the same as the usual retrotips (3). A study shows that following the use of ultrasonic vibration to loosen posts, there were more cracks in dentine (2).
References 1. Allen RK, Newton CW, Brown CE (1989) A statistical analysis of surgical and non-surgical endodontic retreatment cases. Journal of Endodontics 15, 261–6. 2. Altshul JH, Marshall G, Morgan LA, Baumgartner JC (1997) Comparison of dentinal crack incidence and of post removal time resulting from post removal by ultrasonic or mechanical force. Journal of Endodontics 23, 683–6. 3. Gilheany P. Figdor D. Tyas MJ (1994) Apical dentin permeability and microleacage associated with root-end resection and retrograde filling. Journal of Endodontics 20. 22-5 4. Hepworth MJ, Friedman S (1997) Treatment outcome of surgical and non-surgical management of endodontic failures. Journal of Canadian Dental Association 63, 364–71. 5. Lee S-J, Wu M-K, Wesselink PR (2004) the ability of syringe irrigation and ultrasound irrigation to remove dentin debris from uninstrumented extensions and irregularities in root canals. International Endodontic Journal 37, 672–8. 6. Molven O, Halse H, Grung B (1991) Surgical management of endodontic failures: indications and treatment results. International Dental Journal 41, 33–42.

11
7. Nair PNR, Henry S, Cano V, Vera J (2005) Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after ‘‘one-visit’’ endodontic treatment. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 99, 231–52. 8. Rubinstein RA, Kim S (1999) Short-term observation of the results of endodontic surgery with the use of a surgical operation microscope and Super-EBA as root-end filling material. Journal of Endodontics 25, 43–8. 9. Von Arx T (2005) Frequency and type of canal isthmuses in first molars detected by endoscopic inspection during periradicular surgery. International Endodontic Journal 38, 160–8. 10. Weller RN, Niemczyk SP, Kim S (1995) Incidence and position of the canal isthmus. Part 1. Mesiobuccal root of the maxillary first molar. Journal of Endodontics 21, 380–3.

12
Case 2 Endodontic treatment of mandibular left first premolar in conjunction with apical surgery Patient
A 59 year-old white Norwegian male (Fig.1) was on 08.12.04 referred from the Department of Periodontics to the Department of Endodontics, University of Oslo for treatment of mandibular left first premolar.
Fig.1 Frontal view Medical history
Non-contributory. Dental History & Chief complaint
The patient had appointment for routine X-ray check. The radiologist fined a lesion in the mandibular left first premolar. The patient had neither pain nor tenderness to percussion. Clinical Examination
Preoperative photos showed region from mandibular left first premolar to mandibular lateral incisors (Fig.2, 3).
Extra-oral no pathosis was found. A slight inflamed oral and retracted mucosa was observed.

13
Fig.2 Buccal View Fig.3 Occlusal view (Mirror image)
Mandibular left first premolar: Tooth-colour restoration on MOD surfaces. The tooth responded negative to sensibility test with Endo Ice, and not tender to percussion.
Mandibular left Canine: Tooth colour restoration on the M surface. The tooth responded positive to sensibility test with Endo-Ice.
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint. The gingival margin was slightly inflamed with a high degree of retraction, but the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed region from mandibualr left first premolar to mandibular canine (Fig. 4).
Mandibular left first premolar: An MOD radio-opaque restoration. Lamina dura can be followed around the root where it widens to a large radiolucent area of approximately 10mm.
Mandibular left Canine: A part of Canine is shown on the radiograph. The lamina dura can be followed around the entire root.
A large radio-opaque area can be seen in the radiograph which is the mandibular tourus.
Fig.4 Radiographic photo

14
The height of the marginal bone was not within normal limits. The patient has a
generalized marginal periodontitis. Diagnosis
Chronic apical periodontitis mandibular left first premolar with cyst (K04.8). Treatment Plan
Treatment of mandibular left premolar. Root canal disinfection, filling and Apicoectomy Treatment 08.12.2004
Access cavity was done. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. One canal was found. No bleeding from the canal. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr.15 K-Flex was taken to working length. Control of working length with apex locator (Root ZX), and verified with a working length radiograph (Fig.5). Working length was 16,5mm with the buccal cusp as a reference point. The last instrument was NiTi nr.60. The root canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM. 12.01.2005
Patient returned to the clinic four weeks later with no symptoms from the tooth. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi nr.60.
Irrigation was done with 1% sodium hypochlorite, 17% EDTA. Master gutta-percha cone #60 was tried in, and a master cone radiograph was taken (Fig.6). The root canal was dried with sterile paper points. The tooth was root-filled with AH Plus and gutta-percha with cold lateral condenser. The gutta-percha was removed approximately 2 mm down in the canal and sealed with an IRM plug. Access cavity was filled with IRM (Fig.7).
Fig.6 Masterpoint Radiograph Fig.7 Final Radiograph

15
Problem list • The root is short and cutting 2-3mm from it will reduce the retention
dramatically. • The location of the mental foramen was taken in consideration, a Panoramic
radiograph is taken to define the relation between them.
Treatment 31.05.2005
The patient met for surgery, 3 carpules with Xylocain-adrenaline were injected to establish anaesthesia. The patient rinsed for 1 minute with Chlorhexidine mouthwash. Intrasulcular buccal incision from the distal surface of tooth 34 to the mesial surface of tooth 33, with vertical releasing incision from tooth 33 towards the inferior aspect of the buccal mucosa (Fig.8).
Surgical blade number 15 was used. The flap was elevated. The apical lesion
perforates the cortical bone (Fig.9). Granulation tissue was removed by curettage and placed in formalin
transmission medium for histological and pathological examination. No retrograde filling has been placed. The flap was repositioned and sutured with 3, 5-0 silk sutures (Fig.10). Radiograph was taken for control (Fig11). Postoperative information was given. Ice bag was kept at the patients’ right cheek, over the surgical site for 10 minutes. Medications were prescribed: Ibuprofen and Paracetamol. Chlorhexidine mouthwash was recommended.
Fig.8 Surgical incision Fig.9 Location of the lesion

16
Fig.10 Sutures in place Fig.11 Immediately after surgery
Prognosis The prognosis is considered to be favourable.
One week later The patient returned for control after surgery and to remove the sutures. He had a
slight pain on the day of operation but not otherwise. The healing was satisfactory despite the bad oral hygiene (Fig11).
Fig.11 One week later 12 moths follow up
The patient return one year after for control. A slight gingival retraction could be noticed (Fig.12). Radiograph photo shows a favourable healing (Fig13).

17
Fig.12 Clinical photo Fig.13 Radiographic photo Discussion
Periapical lesions are usually composed of solid soft tissue (granulomas) or they have a semisolid, liquefied cystic area (bay cyst or true cyst). Therefore, to diagnose these lesions the least dense area of the radiographic lesion should be measured. The gray value measurements allow differentiation of soft tissue and fluid or empty areas.
Radicular cysts have been a source of debate for many years. A general agreement exists on the assumption that periapical cysts evolve from chronic apical periodontitis. The reported incidence of cysts among lesions of apical periodontitis varies from 6% to 55% (4). Some radicular cysts contain cavities completely enclosed by epithelial lining, while others contain epithelium- lined cavities that are open to the root canals (7). There have been reports in the literature over the years of attempts to make a differential diagnosis between cyst and granuloma based on their radiological features; a cystic image would exhibit defined margins with a hyperostotic border, whereas the granuloma would show indistinct margins (9), Also, cysts have been stated to have a clearly defined periapical radiolucency that was approximately circular, a loss of the lamina dura at the apex, and most importantly, a thin radio-opaque lamina to the lesion (1). Earlier reports were even more definite: cysts were considered to be larger than granulomas (3) and if the lesion were more than 1.5 cm in diameter it would certainly be a cyst (5).

18
Attempts to diagnose, the lesion before surgery with periapical radiographs, contrast media. Papanicolou smears, and albumin tests have proven to be inaccurate. Recently with the advent of other imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI), and cone-beam CT, differences in density may permit more accurate preoperative diagnosis.
Trope et al. (8) stated that a cyst could be differentiated from a granuloma by a CT
scan. Using cadavers an oral radiologist selected four granulomas and four cysts, and CT was performed on the root tips and lesions. In the CT, seven lesions had a cloudy appearance with a density similar to surrounding tissue. The eighth lesion had a different density and histologically was a cyst. Shrout et al. (6) digitized radiographic images using a 256 greyscale and computed a cumulative percent histogram. Granulomas had a narrower range and lower greyscale value than did cysts. Camps et al. (2) also used a grey level correction method to assess treatment results.
In my case there was a suspicious about that presence of cyst when there was no healing after 5 months. Histological results show the presence of epithelium which indicates the opportunity of cyst (Fig.14).
Fig.14 Histological results

19
References 1. Browne RM, Edmondson HD, Rout PG. A radiological atlas of diseases of the teeth and jaws. Chichester: John Wiley; 1983. p. 91,146. 2. Camps J, Pommel L, Bukiet F. Evaluation of periapical lesion healing by correction of gray values. J Endod 2004;30:762– 6. 3. Mortensen H, Winther JE, Birn H. Periapical granulomas and cysts. An investigation of 1600 cases. Scand J Dent Res 1970;78:241-50. 4. Nair PNR. New perspectives on radicular cysts: do they heal? Int Endod J 1998;31:155-60. 5. Shear M. Cysts of the oral regions. Bristol: John Wright; 1976. 6. Shrout MK, Hall JM, Hildebolt CE. Differentiation of periapical granulomas and radicular cysts by digital radiometric analysis. Oral Surg Oral Med Oral Pathol 1993;76:356–61. 7. Simon JHS. Incidence of periapical cysts in relation to the root canal. J Endod 1980;6:845-8. 8. Trope M, Pettigrew J, Petras J, Barnett F, Tronstad L. Differentiation of radicular cyst and granulomas using computerized tomography. Endod Dent Traumatol 1989;5:69 –72. 9. Wood NK. Periapical lesions. Dent Clin N Amer 1984;28: 725-66.
20
Case 3 Endodontic retreatment of mandibular left first molar in conjunction with apical surgery Patient
A 52 year-old white Norwegian female (Fig.1) was on 06.01.06 referred to the author for re-treatment of mandibular left first molar.
Fig.1 Frontal view
Medical history
Non-contributory. Dental History & Chief complaint
Endodontic treatment of the mandibular left first molar was done for more than 20 years ago. The patient consults her GP in December 2005 when she get a sinus tract buccally to the tooth. She had never felt pain only a bad taste because of puss from the sinus tract. Clinical Examination
Intra-oral photos showed region from mandibular left second molar to mandibular first premolar (Fig.2, 3, and 4).No extra-oral pathosis was found, and a normal oral mucosa was observed.

21
Fig.2 Occlusal Fig.3 Gutta- Percha in sinus tract Fig.4 Buccal view
Mandibular left second molar: Amalgam restoration on MOD surfaces, and the tooth responded positively to sensibility test with Endo Ice.
Mandibular left first molar: Amalgam restoration on MOL surfaces. The tooth was slightly tender to percussion. A sinus tract buccally, 3-4 mm below the gingival margin.
Mandibular right first premolar: Sound tooth structure and the tooth responded positively to sensibility test with Endo Ice.
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint.
The gingival margin of the other teeth was healthy, and the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed region from mandibular left second molar to second premolar (Fig. 5).
Mandibular left second molar: An MOD radio-opaque restoration. Lamina dura can be followed around the entire root.
Mandibular left first molar: An MOD radio-opaque restoration, the root canal is filled with a high radio-opacity material which is seems like Silver points. Lamina dura can be followed around the entire distal root, while the Lamina Dura can be followed in the mesial surface of the mesial root and widened apically to a large diffuse radiolucency up to the bifurcation area.
Mandibular left second premolar: Sound tooth structure with no restoration. Lamina dura can be followed around the entire root.

22
Fig. 5 Radiographic examination Diagnosis
Chronic apical periodontitis of mandibular left first molar with sinus tract (K04.62) Treatment Plan
Re-treatment of necrotic mandibular left first molar. Root canal disinfection and filling. Treatment 16.01.2006
Access cavity was prepared, and four canals were found filled with silver cones. The cones were removed carefully with ultra- sound and silver points forceps (Fig.6). Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr.15 K-Flex was taken to working length and verified with a working length radiograph (Fig.7).
Working length was:
MB: NiTi 45/20,5mm mb.cusp ML: NiTi 45/17,0mm ml.cusp DB: NiTi 55/20,5mm db.cusp DL: NiTi 55/20,5mm db.cusp The canal was dressed for 5 minutes with 2% chlorhexidine digluconate. The root
canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.

23
Fig.5 control radiograph Fig.6 working length 03.02.06
Patient returned to the clinic three weeks later with no symptoms from the tooth and the sinus tract is gone. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi nr.60. Irrigation was done with 1% sodium hypochlorite, 17% EDTA, and dressed for 5 minutes with 2% chlorhexidine digluconate. Master gutta-percha cones were tried in, and a master cone radiograph was taken (Fig.7). The root canal was dried with sterile paper points. The tooth was root-filled with AH Plus and gutta-percha with cold lateral condenser. The gutta-percha was removed approximately 2 mm down in the canal and sealed with an IRM plug. Access cavity was filled with IRM (Fig.8). The patient was referred to her GP with recommendation of a crown treatment due to a big amalgam filling.
Fig.7 Master Point radiograph Fig.8 final radiograph

24
6 months later The patient returned to her GP with a sinus tract at the same area. She had a slightly
pain and a bad taste in her mouth because of exudates.
Fig. 9 Six month after New treatment plan
Apicoectomy of the mandibular left first molar. Treatment 15.11.2006
The patient returned to the clinic 11 months after the endodontic treatment is finished for performing apicoectomy on mandibular left first molar. Four carpules with Xylocain with Adrenalin (20 mg/ml + 12.5 μg/ml) were used to establish anesthesia. An incision was made with a scalpel blade nr 15C starting with a vertical releasing incision starting from the mesiobuccal gingival line angle of the mandibular second premolar. An intrasulcular incision extending from the releasing incision to the distal aspect of the mandibular left second molar. Elevation of the full mucoperiostal flap was initiated with a periostal elevator. The flap was carefully elevated at the junction between the vertical releasing incision and horizontal incision extending apical and lateral. A retractor was used facilitating the reflection of the flap.
A pathological bone fenestration was detected outside the coronal margin of the bone
between the mesial and distal root near the bifurcation area (Fig.10).

25
Fig.10 Bone fenestration near bifurcation
The lesion was released from the flap by the scalpel. Osteotomy of the outer cortical plate was accomplished with an nr 6 round bur on a 45° angled high speed hand piece under irrigation with sterile saline to adequately expose the root. The lesion was a tunnel shape expanded from the apical region of the mesial root and up to the bifurcation area where the sinus tract was clinically located. Two-three mm of the mesial root apex was resected with a long fissure bur.
A retrograde preparation was carried out with the piezoelectric Satelec ultrasound
device using ultrasonic tip CT under constant cooling with rinsing sterile saline. The cavity was extended up to 3 mm in the root canal and followed gutta-percha at all times. The ultra sound tip was also used over the isthmus area between the tow canals. A microscope was being used most of the time in order to achieve maximal visibility. Stryphnon gauze was placed in the bone cavity in order to achieve haemostasis. The cavity was irrigated with sterile saline and dried with sterile paper points.
A retrograde white MTA filling was placed into the cavity using plastic instrument as
a carrier, and condensed with micro condensing pluggers. A burnisher was used at the end.
The Stryphnon gauze was removed. The surgical field was irrigated with sterile saline. The flap was repositioned and was hold tight in place with finger pressure for five minutes in order to reduce the post operative haematoma and pain. The vertical releasing flap was sutured in place with two 4-0 silk suture. The five other interrupted sutures were placed inter-proximally in the papilla. A final radiograph was taken (Fig.11) and the patient received an ice pack to reduce post operative haematoma and pain. The pain killer Ibuprofen; Ibux 400 mg, combined with Paracetamol; Paracet 500mg, was prescribed. The antiseptic mouthwash Corsodyl. Post operative instructions were given.

26
22.11.06 The patient returned to the clinic one week later. The tooth was asymptomatic and the
sutures were removed (Fig.12).
Fig.11 Final radiograph Fig.12 One week after operation Evaluation
The retrograde filling was difficult to apply, the isthmus was cleaned and a tried to filled with MTA. Prognosis
The prognosis is considered to be uncertain. 4 months follow up
The patient returns back after 4 months. The tooth is with out any symptoms. Radiographic photo shows a favourable healing (Fig.13). A new control will be taken in September then we can decide the best prosthetic treatment for this tooth.

27
Fig.12 Follow up radiograph Discussion
When root canal treatment fails, the cause is generally believed to be intracanal infection resisting treatment, or micro-organisms invading the canal via coronal leakage of the root-filling ( 11, 12). Non- surgical re-treatment of such cases has a modest prognosis (9, 13), which may indicate difficulties in the elimination of the microflora. Therefore a reconsideration of intra-canal antibacterial treatment procedures seems to be required.
Two earlier investigations on the intra-canal bacterial status in root canal treated teeth with apical radiolucencies have reported bacterial growth in 38% (2) and 57% (10) of cultured samples, respectively. In these studies the microbiota was dominated by facultative anaerobic species rather than anaerobes.
Facultative anaerobic bacteria are less susceptible to antimicrobial activities than are anaerobes, and therefore can be expected to persist more frequently in the root canal following inadequate treatment procedures. When facultative anaerobes have been in a quiescent phase with low metabolic activity for a period, changes in the nutritional conditions (e.g. via coronal leakage) may trigger their growth. The most frequently isolated bacteria were enterococci. They are often reported to be low in numbers in untreated infected root canals with necrotic pulps (14). However, when the ecological prerequisites are altered, enterococci may thrive and multiply. Molander et al. (8) found that the use of an intracanal dressing directed specifically towards the anaerobic segment of the microflora brought about a suitable environment for enterococcal growth. Gomes et al. (5) reported multiplication of E. faecalis in some canals following standard biomechanical treatment procedures. The treatment resistance of enterococci in the root canal has been recognized by several authors (2, 5, 10). Importantly, a routinely used interappointment dressing such as calcium hydroxide has shown to be ineffective in killing E. faecalis present in root canals (1, 7).

28
Enterococci have also been shown to have an ability to survive in root canals as single organisms without the support of other bacteria (4). E. faecalis was isolated in 38% of teeth that had recoverable microorganisms, which suggests that it is an important agent in endodontic failure (15).
The importance of conservative re-treatment of canals before surgery showed a re-treatment success rate 24% higher in cases of failed endodontic treatment in which antibacterial measures and refilling of the canal preceded apical surgery than in cases in which apical surgery was the only procedure performed (6).
The presence of Enterococcus faecalis in cases of persistent apical periodontitis is of particular interest because it is rarely found in infected but untreated root canals (15). The organism is resistant to most of the intracanal medicaments, and can tolerate a pH up to 11.5 which may be one reason why this organism survives antimicrobial treatment with calcium hydroxide dressings (1). This resistance occurs probably by virtue of its ability to regulate internal pH with an efficient proton pump (3). Enterococcus faecalis can survive prolonged starvation, and can grow as monoinfection in treated canals in the absence of synergistic support from other bacteria (4). Therefore, E. faecalis is regarded as being a very recalcitrant microbe among the potential aetiological agents of persistent apical periodontitis. However, the presence of E. faecalis in cases of persistent apical periodontitis is not a universal observation.
References 1. Byström A, Claesson R, Sundqvist G (1985) The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endodontics and Dental Traumatology 1, 170–75. 2. Engström B (1964) The significance of enterococci in root canal treatment. Odontologisk Revy 15, 87–106. 3. Evans M, Davies JK, Sundqvist G, Figdor D (2002) Mechanisms involved in the resistance of Enterococcus faecalis to calcium hydroxide. International Endodontic Journal 35, 221–8. 4. Fabricius L, Dahltn G, Holm SE, Mtller JR ( 1982) Influence of combinations of oral bacteria on periapical tissues of monkeys. Scand J Dent Res 90:200-6. 5. Gomes BPFA, Lilley JD, Drucker DB (1996) Variations in the susceptibilities of components of the endodontic microflora to biomechanical procedures. International Endodontic Journal 29, 235–41. 6. Grung B, Molven O, Halse A. (1990) Periapical surgery in a Norwegian county hospital: follow-up findings of 477 teeth. J Endod 16:411-7. 7. Haapasalo M, Ørstavik D (1987) In vitro infection and disinfection of dentinal tubules. Journal of Dental Research 66, 1375–9.

29
8. Molander A, Reit C, Dahlén G (1990) Microbiological evaluation of clindamycin as a root canal dressing in teeth with apical periodontitis. International Endodontic Journal 23, 113–18. 9. Molven O (1974) The frequency, technical standard and results of endodontic therapy. Bergen, Norway: University of Bergen (PhD Thesis.) 10. Möller ÅJR. (1966) Microbial examination of root canals and periapical tissues of human teeth. Odontologisk Tidskrift, 74 (special issue), 1–380. 11. Nair PNR, Sjögren U, Krey G, Kahenberg K-E, Sundqvist G (1990) Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant periapical lesions: a long-term light and electron microscopic follow-up study. Journal of Endodontics 16, 580–8. 12. Ray Ha, Trpoe M (1995) Periapical status of endodontically treated teeth in relation to the technical quality of the root-filling and the coronal restoration. International Endodontic Journal 28, 12–18. 13. Sjögren U, Hågglund B, Sundqvist G, Wing K (1990) Factors affecting the long-term results of endodontic treatment. Journal of Endodontics 16, 498–505. 14. Sundqvist G (1992) Associations between microbial species in dental root canal infections. Oral Microbiology and Immunology 7, 257–62. 15. Sundqvist G, Figdor D, Persson S, Sjögren U (1998) Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surgery, Oral Medicine and Oral Pathology 85, 86–93.

30
Case 4 Apicoectomi of maxillary left first premolar Patient
A 60 years old white Norwegian female (Fig.1) was referred to the Department of Endodontics, University of Oslo, by her postgraduate student for treatment of maxillary left first premolar.
Fig.1 Frontal view Medical History
Prednisolon : Corticosteroid anti-inflammatory and immunosuppressive. Dalacin : Against Acne Vulgaris. Fosamax : Bone resorption inhibitor. Clarityn : Anti histamine for treatment of Rhinitis. Noblegan : Analgesic, mild pain. Paralgin Forte: Analgesic, severe pain.
Dental History & Chief Complaint
The maxillary left first premolar was endodontically treated one year ago in the student clinic. Complications as over instrumentation and over filling were happened. The patient was referred to the postgraduate clinic, Department of Endodontics due to mild symptoms from the tooth. Clinical Examination
The clinical photos (Fig.2, and 3) shows region from maxillary left lateral incisor to maxillary first premolar.
No pathosis was found extra-orally. Inra-oraly a normal oral mucosa was observed.
31
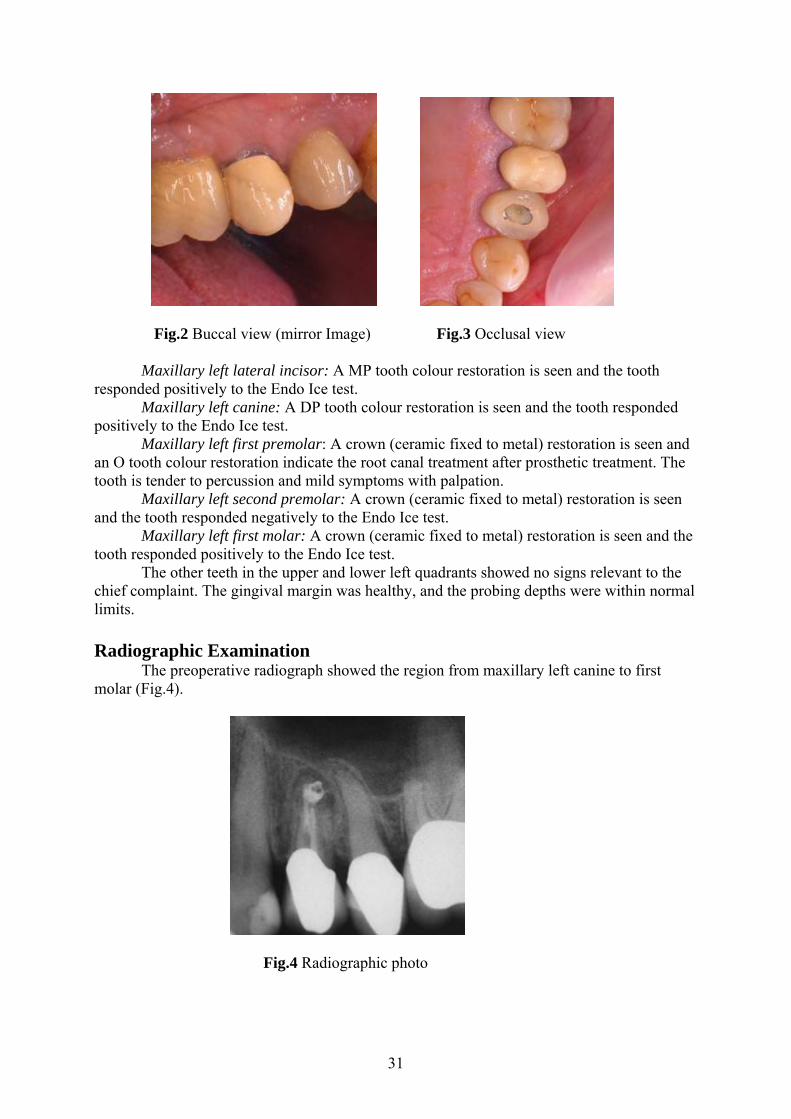
Fig.2 Buccal view (mirror Image) Fig.3 Occlusal view
Maxillary left lateral incisor: A MP tooth colour restoration is seen and the tooth responded positively to the Endo Ice test.
Maxillary left canine: A DP tooth colour restoration is seen and the tooth responded positively to the Endo Ice test.
Maxillary left first premolar: A crown (ceramic fixed to metal) restoration is seen and an O tooth colour restoration indicate the root canal treatment after prosthetic treatment. The tooth is tender to percussion and mild symptoms with palpation.
Maxillary left second premolar: A crown (ceramic fixed to metal) restoration is seen and the tooth responded negatively to the Endo Ice test.
Maxillary left first molar: A crown (ceramic fixed to metal) restoration is seen and the tooth responded positively to the Endo Ice test.
The other teeth in the upper and lower left quadrants showed no signs relevant to the chief complaint. The gingival margin was healthy, and the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed the region from maxillary left canine to first molar (Fig.4).
Fig.4 Radiographic photo

32
Maxillary left canine: A PD radio-opaque restoration was seen and lamina dura could be followed around the entire roots.
Maxillary left first premolar: A radio-opaque restoration in the crown and in the root canal was seen. Lamina dura could be followed around the root were its widened apically to form a circumscribed round radio lucent lesion, and a large amount of radio-opaque root filling material beyond the apex.
Maxillary left second premolar: A radio-opaque material in the root canal was seen and lamina dura could be followed around the entire root.
Maxillary left first molar: A radio-opaque restoration was seen and lamina dura could be followed around the mesial root. Diagnosis
Chronic apical periodontitis of maxillary left first premolar (K04.50). Treatment plan
Re-treatment of endodontically treated maxillary left first premolar. Apicoectomy of maxillary left first premolar.
Treatment 27.04.2005
Access cavity was prepared, and two canals were found filled with gutta-percha. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. Gutta-percha was removed with the help of ProTaper F3 confirmed with a control radiograph (Fig.5). Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr 30 K-Flex and 30 Hedstrøm file was taken to working length. The working length was controlled with an apex locator (ProPex), and verified by a working length radiograph (Fig.6). Working length was: B canal 18 mm, instrument size NiTi nr 60. RP. Buccal cusp P canal 16 mm, instrument size NiTi nr 60. RP. Palatinal cusp
The root canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a Lentulo spiral and sterile paper points. The access cavity was sealed with IRM.
Fig.5 Control radiograph Fig.6 Working length radiograph

33
31.08.2005 The patient returned to the clinic four months later (because of sickness and summer
vacation). Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution.
The calcium hydroxide was removed with NiTi hand instrument. Irrigation was done
with 1% sodium hypochlorite, 17% EDTA, canals were dried with sterile paper points. The tooth was root filled with MTA and condensed with hand instrument. Wet cotton pellet was inserted over the MTA in both canals and the access cavity was filled with IRM (Fig.7).
Fig.7 MTA in the canals 04.10.2005
The patient returned to the clinic six weeks later for performing apicoectomi. Three carpules with Xylocaine with Adrenalin (20 mg/ml + 12.5 μg/ml) were used to establish anaesthesia. An incision was made with a scalpel blade nr 15C starting with a vertical releasing incision, starting from the mesiobuccal gingival line angle of the maxillary left canine approximately 1 cm in a superior aspect of the oral buccal mucosa. An intrasulcular incision extending from the releasing incision to the distal aspect of maxillary left first molar (Fig.8).
Elevation of the full mucoperiostal flap was initiated with an nr 149 periostal elevator.
The flap was carefully elevated at the junction between the vertical releasing incision and horizontal incision extending apical and lateral. A retractor was used facilitating the reflection of the flap. Bone fenestration was detected outside the root (Fig.9). The lesion was removed with periodontal curettes.
Osteotomy of the outer cortical plate was accomplished with an nr 6 round bur on a
45° angled high speed hand piece under irrigation with sterile saline to adequately expose the roots end (fig.10). Three mm of the root apex was resected with a long fissure bur. A retrograde preparation was carried out with the piezoelectric Satelec ultrasound device using ultrasonic tip CT under constant cooling with rinsing sterile saline.

34
The cavity was extended up to 3 mm in the root canal and followed gutta-percha at all times. A microscope was being used most of the time in order to achieve maximal visibility.
Fig.8 The incision line Fig.9 Bone fenestration
Stryphnon gauze was placed in the bone cavity in order to achieve haemostasis. The cavity was then irrigated with sterile saline and dried with sterile paper points. A retrograde MTA filling was placed into the cavity using plastic instrument as a carrier, and condensed with micro condensing pluggers. A burnisher was used at the end.
The retro-filling was examined under high magnification with an explorer to check
marginal adaptation and integrity. The Stryphnon gauze was removed. The surgical field was irrigated with sterile saline. The flap was repositioned and was hold tight in place with finger pressure for five minutes in order to reduce the post operative haematoma and pain.
The vertical realising flap was sutured in place with three 4-0 silk suture. The three
other interrupted sutures were placed inter-approximaly in the papilla (Fig.11). A final radiograph was taken (Fig.12) and the patient received an ice pack to reduce post operative haematoma and pain. The pain killer Ibuprofen; Ibux 600 mg, was prescribed and the antiseptic mouthwash Corsodyl. Post operative instructions were given.

35
Fig.10 The lesion is removed Fig.11 Suture photo ‘
Fig.12 Final radiograph One week later
The patient returned to clinic. The sutures were removed. A good healing result was seen in the incision area. Evaluation
The Apicoectomy was done easy because no retrograde filling was needed. Prognosis
The prognosis is considered to be favourable. 12 month follow up
One year after operation the patient has no symptoms. The radiographic photo shows a favourable healing (Fig.13).

36
Fig.13 One year follow up radiograph Discussion
The purpose of root canal treatment is to eliminate infection in the root canal and to fill the root canal space.Various commercial sealers have been developed and used for this purpose. One of them, AH26 sealer (Dentsply, DeTrey, Konstanz, Germany), is frequently used because of its excellent sealing ability (8).
It has been demonstrated, however, that the sealer was cytotoxic during setting which
can be, to some extent, explained by the release of formaldehyde (2, 4). A modified version of the material AH Plus (Dentsply) was subsequently developed. According to the manufacturer, AH Plus has better physical and clinical properties than AH26 and the formulation no longer releases formaldehyde. Root filling materials are usually inclose contact with living tissues. Thus, the biological properties of these materials are important as cytotoxic materials can damage periapical tissues, and material with mutagenic potential can induce DNA mutations, possibly causing malignant transformation of the cells (1).
Because tissue injury induced by intracanal procedures may result in unfavourable responses to treatment, the practitioner’s choice on procedures to be used during root canal treatment should rely on those that are known to cause as little damage as possible. It has been demonstrated that foreign materials, such as root canal sealers, trapped into periradicular tissues after endodontic treatment can perpetuate apical periodontitis (7). Severe reactions have been reported after extrusion of some commonly used substances into the periradicular tissues (5). Overextended root canal sealers also represent chemical irritation, as virtually all endodontic sealers are highly toxic when freshly prepared (9). Furthermore, their irritating effect conceivably increases as the material/ tissue contact surface area increases. Thus, the larger the volume of over-extended material, the larger the contact surface between sealer
The epoxy resin- based root canal sealer AH plus, according to the manufacturer,
described that AH plus is the new product that has the advantageous properities of AH26, but preserves the chemical property of the epoxy amine better so that material no longer releases formaldehyde. Due to AH plus complex chemical composition, numerous substances may be

37
released from AH plus into the adjacent tissues and might thus induced local and/or systemic adverse effect. Including cytotoxicity and genotoxicity (3).
A study shows that the cytotoxicity was dependent on concentration, setting time and the sealer used. Both materials exhibited reduced cytotoxicity when set for longer and did not have increased toxicity when eluted for a longer period. AH Plus showed significantly stronger cytotoxicity than AH26, both initially and after longer setting intervals (6).
References 1. Bertram JS (2001) The molecular biology of cancer (review). MolecularAspects of Medicine 21,167-223. 2. Gerosa R, Menegazzi G, Borin M, Cavalleri G(1995) Cytotoxicity evaluation of six root canal sealers. Journal of Endodontics 21, 446-8. 3. Geurtsen W, Leyhausen G. (1997) Clin. Oral Inves;1: 5 4. Koch MJ (1999) Formaldehyde release from root-canal sealers: influence of method. International Endodontic Journal 32, 10-6. 5. Lindgren P, Eriksson K-F, Ringberg A. (2002) Severe facial ischemia after endodontic treatment. J Oral Maxillofac Surg 60, 576 –9. 6. Miletic I, Jukic S, Anic I, Zeljezic D, Garaj-Vrhovac V, Osmak M. (2003) Examination of cytotoxicity and mutagenicity of AH26 and AH Plus sealers. International Endodontic Journal 36, 330-35. 7. Nair PNR. (2004) Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med 15, 348–81. 8. Wu M-K, Wesselink PR, Boersma J (1995) A 1-year followup study on leakage of four root canal sealers at different thickness. International Endodontic Journal 28, 185-9. 9. 13. Spångberg L, Pascon EA (1998) The importance of material preparation for the expression of cytotoxicity during in vitro evaluation of biomaterials. J Endod 14, 247–50.

38
Case 5 Surgical extraction of vertical root fractured mandibular right first premolar Patient
A 42 year-old white Caucasian female (Fig.1) was referred to the Department of Endodontics, University of Oslo by her dental undergraduate student for re-treatment of mandibular right first premolar.
Fig.1 Frontal view Medical history
Non-contributory. Dental History & Chief complaint
Endodontic treatment of the mandibular right first premolar was done Feb. 2004 in student clinic followed by a prosthetic treatment (crown restoration). The patient felt a mild pain one and a half year after. Clinical Examination
Preoperative photos showed region from mandibular right first premolar to right lateral incisors (Fig.2).
No extra-oral pathosis was found, and normal oral mucosa was observed.

39
Fig. 2 Buccal view
Mandibular right second premolar: Tooth-coloured restoration on the buccal surface and a ceramic on lay on the MO.
Mandibular right first premolar: A ceramic firmed to metal crown. Mandibular right Canine: A ceramic firmed to metal restoration. The tooth was tender
to palpation. Mandibular right lateral incisors: Sound tooth
The probing depths were within normal limits. Except for the first premolar which has
a periodontal pocket of about 10mm. the mobility of the tooth was with in normal limits. The other teeth in the upper and lower right quadrants showed no signs relevant to the
chief complaint. Radiographic Examination
The preoperative radiograph showed region from mandibualr right second premolar to canine (Fig. 3, 4).
Mandibular right second premolar: ODB radio-opaque restoration. Lamina durra can be followed around the entire roots.
Mandibular right first premolar: A radio-opaque restoration shows a crown restoration. Radio opaque root filling material is in the canal. Lamina durra can be followed around the root were it’s widen in the middle of the root.
Mandibular right canine: B radio-opaque restoration is seen. Lamina durra can be followed around the entire roots.

40
Fig.3 Radiographic photo Fig.4 Gutta-percha in the palatinal pocket (One year follow up)
Diagnosis
Tentative diagnosis was vertical root fracture. Treatment Plan
The diagnosis and treatment was discussed with the patient. She couldn’t accept to extract the tooth only from out clinical diagnosis. The explorative flap elevation was the alternative to confirm the diagnosis.
Explorative flap elevation to see if there is a vertical root fracture or an apical
periodontitis from a wide lateral canal. Treatment 11.10.06
The patient met for surgery, 3 carpules with Xylocain-adrenaline were injected to establish anaesthesia. The patient rinsed for 1 minute with Chlorhexidine mouthwash. Intrasulcular buccal incision from the mesial surface of tooth 43 to the distal area of tooth 45, with vertical releasing incision from tooth 43 towards the inferior aspect of the buccal mucosa.
Surgical blade number 15 was used. The flap was elevated. No lesion was found in the
buccal surfaces, the flap elevation continued from the lingual surface. The area ere released and a fracture line could be seen easely with microscope. The treatment decision at that time was extraction.
The tooth was extracted and the flap was repositioned and sutured with 4, 5-0 silk
sutures Postoperative information was given. Ice bag was kept at the patients’ right cheek, over the surgical site for 10 minutes. Medications were prescribed: Ibuprofen and Paracetamol. Chlorhexidine mouthwash was recommended.

41
No picture have been taken under operation but clinical photos for the extracted tooth which shows the vertical root fracture is shows in fig.5, 6, 7, and 8.
Fig.5 Disto-Buccal view
Fig.6 Mesial and Lingual surface
Fig.6 Lingual root surface
Fig.7 Lingual view

42
Discussion
Vertical root fracture (VRF) occasionally occurs in endodontically treated teeth. It is the second most frequent identifiable reason for loss of endodontically treated teeth (2).
Once VRF occurs little can be done to rectify the situation, yet factors that predispose
to fracture remain largely unknown. A better understanding of factors related to VRF might open the possibility of better prevention and/or management of this catastrophic entity. Dentin thickness, radius of canal curvature and external root morphology have been proposed as factors potentially influencing fracture susceptibility (6). The thinner the dentin, the more likely the tooth is to fracture, and a low radius of canal curvature can act as a stress raiser area (1), which makes the root more susceptible to fracture. External root morphology has also been shown with finite element analysis (FEA) to be a strong determinant of fracture direction (6).
Endodontically treated teeth are widely considered to be more susceptible to fracture than are vital teeth. The reasons most often reported have been the dehydration of dentin after endodontic therapy, excessive pressure during obturation and the removal of tooth structure during endodontic treatment (3, 4, and 10). The strength of an endodontically treated tooth is related directly to the method of canal preparation and to the amount of remaining sound tooth structure. It commonly is believed that the loss of dentin creates an increased susceptibility to fracture (10). Some studies have reported strong evidence that endodontically treated teeth, with or without posts, are susceptible to root fracture (9).
Most fracture lines were found to be incomplete fractures in a buccolingual direction, and the second most common direction was proximal fracture. This is in agreement with that reported in other studies (5, 8). The prevalence of VRF is not equally distributed over the different tooth types. Maxillary and mandibular premolars have both recorded a high prevalence (11). It is important to establish which procedures in the endodontic therapy may increase the risk of VRF. It is generally accepted that the removal of excessive amounts of radicular dentin compromises the root, and that the amount of dentin remaining is directly related to the strength of the root. Clinical and experimental studies have shown that root fractures occur predominantly in a bucco-lingual direction (7, 5) References 1. Callister WD. Failure. In: WD Callister, editor Materials science and engineering: an introduction, 6th edn. New York; [Chichester]: Wiley, 2003:192–245. 2. Caplan DJ, Weintraub JA. Factors related to loss of root canal filled teeth. J Public Health Dent 1997;57:31–9. 3. Helfer AR, Melnick S, Schilder H. Determination of moisture content of vital and pulpless teeth. Oral Surg Oral Med Oral Pathol 1972;34:661-70. 4. Holcomb JQ, Pitts D, Nicholls JI. Further investigation of spreader loads required to cause vertical root fracture during lateral condensation. J Endod 1987;13:277-84.

43
5. Lertchirakarn V, Palamara J, Messer H. Load and strain during lateral condensationand vertical root fracture. J Endod 1999;25:99 –104. 6. Lertchirakarn V, Palamara JE, Messer HH. Patterns of vertical root fracture: factors affecting stress distribution in the root canal. J Endod 2003;29:523– 8. 7. Pitts DL, Natkin E. Diagnosis and treatment of vertical root fractures. J Endod 1983; 9:338–46. 8. Saw L, Messer H. Root strains associated with different obturation techniques. J Endod 1995;21:314 –20. 9. Sorensen JA, Martinoff JT. Intracoronal reinforcement and coronal coverage: a study of endodontically treated teeth. J Prosthet Dent 1984;51:780-4. 10. Sornkul E, Stannard JG. Strength of roots before and after endodontic treatment and restoration. J Endod 1992;18:440-3. 11. Tamse A, Lustig J, Kaplavi J. An evaluation of endodontically treated vertically fractured teeth. Journal of Endodontics 1999;25:506—8.

44
Case 6 Endodontic treatment of mandibular left first molar with external root resorption.
Patient A 23 year-old white Norwegian female (Fig.1) was referred by the authors to the
Department of Endodontics, University of Oslo for treatment of mandibular right second molar.
Fig.1 Frontal view
Medical history Non- contributory.
Dental history & chief complaint The patient felt some sensitivity in her tooth the last days. The tooth was sensitive to
cold and in some degree to hot. She avoids chewing any thing hard on it. But there was no history of acute pulpitis.
She is related to public health system and she was on a routine control almost one time
every 14 to 18 moths. Follow up radiographs since 1999 shows exactly what happened (Fig 2, 3, 4, 5, 6, and 7)

45
Fig.2 Mai 1995 Fig.3 April 1997 Fig.4 July 1999
Fig.5 November 2000 Fig.6 February 2002 Fig.7 August 2004 Clinical Examination
Preoperative photos showed region from mandibular left second molar to mandibular first premolar (Fig.8, 9).
Fig.8 Lingual view Fig.9 Occlusal view
Mandibular left second molar: A tooth-colour restoration on O surfaces, and the tooth
responded negatively to sensibility test with Endo Ice. Mandibular left first molar: A temporary restoration on O surface, after the acute
treatment. The tooth responded positively to sensibility test with Endo Ice, and was tender to percussion.

46
Mandibular left first premolar: Sound tooth, and responded positively to sensibility test with Endo Ice.
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint. The gingival margin was healthy, and the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed region from mandibualr left second molar to first premolar (Fig.10).
Mandibular left second molar: Have an O radio-opaque restoration. Lamina dura can be followed around the entire root.
Mandibular left first molar: Sound tooth Lamina dura can be followed around the entire roots. A large rdiolucency can bee seen in the middle of the crown. The pulp lines can still be follows behind the lucency.
Mandibular left first premolar: Sound tooth. The second premolar was extracted surgically when the patient was 13 years old
because of orthodontics treatment. The height of the marginal bone was within normal limits.
Fig. 10 Radiographic photo ( taken before acute treatment) Diagnosis
External inflammatory root resorption. Third degree (K03.38). Treatment Plan
Treatment of a vital pulp with treatment of resorption. Root canal disinfection and filling

47
Treatment 10.05.2005
Access cavity was done Four canals were found. The granulation tissue, which bleed extensively, was removed and the tooth margins was cleaned and excavated with XL Rosen bur size 10and 12 until a clean dentine was observed . The perforation area was sealed with temporary filling to prevent bleeding inside the cavity form surrounding periodontal tissue. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. Irrigation was done with 1% sodium hypochlorite and 17% EDTA.Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.11).
Preparation was done with ProTaper rotary instruments and manually with NiTi files, to dimension: Mesio-Buccal canal: 45, 20mm, ref point: MB cusp. Mesio- lingual canal: 45, 19,5mm, ref point: MB cusp Disto-buccal canal : 50, 20,5mm. Ref point: DB cusp Disto- palatinal canal: 50, 20,5mm. Ref point: DB cusp.
The root canal was dried with sterile paper points. Calcium hydroxide intra-canal dressing was packed into the canal with the help of a lentulo spiral and sterile paper points. Access cavity was sealed IRM.
Fig.11 Working length radiograph 01.06.2005
Patient returned to the clinic one week later with no symptoms from the tooth. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi hand instrument. Irrigation was done with 1% sodium hypochlorite, 15% EDTA. Master gutta-percha cones were tried in, and a master cone radiograph was taken (Fig.12). The root canal was dried with sterile paper points. The tooth was root-filled with AH Plus and gutta-percha. The gutta-percha was removed approximately 2 mm down in the canal and sealed with an IRM plug (Fig.13).

48
Fig 12. Masterpoint radiograph Fig.13 Final Radiograph
Rubber dam was removed and the perforations area to the surrounding periodontal
ligaments cleaned and a shell was applied mesially to seal the area (Fig.14, 15, 16, and 17). The cavity was cleaned, used of acid etching, bonding (3M), and sealed with composite tooth colour filling material.
Fig.14 Perforation area Fig.15 shell sealed the area Fig.16 dry cavity
Fig.17 Final radiograph

49
Evaluation
Radiographically the root-filling appeared dense and good, with a 1mm from apex
Prognosis The prognosis in this case is considered to be uncertain because of the degree of
resorption. Follow up examination 01.11.2006
The patient returned for control after 17 months. No subjective symptoms from the tooth. The clinical findings show a good oral hygiene (Fig.18 and 19) and a periodontal pocket mesially. The radiographic examination (Fig.20 and 21) demonstrated favourable results. There was no further progression of root resorption process.
Fig.18 Buccal view (mirror Image) Fig.19 Occlusal
Fig.20 Follow up radiograph Fig.21 Gutta- percha point in the pocket

50
Discussion Root resorption is a dental complication that can lead to tooth extraction. There are
many classification and terms for different type of root resorption. For example apical replacement resorption has been used for apical root resorption following orthodontic treatment (2). The same pathological process has been included under the category of inflammatory root resorption (8). In the classical classification of root resorption following traumatic injuries (1), replacement and inflammatory resorption are related to completely different etiologies and treatment protocols.
The etiology of root resorption requires two phases: injury and stimulation (8, 9). Injury is related to non-mineralized tissues covering the external surface of the root, the precementum or internal surface of the rootcanal, the predentin. The injury may be mechanical following dental trauma, surgical procedures, and excessive pressure of an impacted tooth or tumour. It may also occur following chemical irritation during bleaching procedures using 30% hydrogen peroxide or other irritating agents (5).
Heithersay (7) investigate the predisposing factor in a group of 222 patients with a total of 257 teeth that displayed varying degrees of invasive cervical resorptions and found that orthodontics was the most common sole factor identified in 47 patients (21,2%) with 62 affected teeth.
Trauma was the second most frequent sole factor with 31 patients (14%) with 39 affected teeth (15, 1%). Thirty-three (14,9%) of the patients who had a history of intra-coronal bleaching, 10 (4,5%) had bleaching as a sole factor, 17 (7,7%) a history of bleaching and trauma, 2 (0,9%) bleaching and orthodontics and 4 (1,8%) a combination of bleaching, trauma and orthodontics. Surgery, particularly involving the cemento-enamel junction area was identified in 13 patients (5,9%) as a sole factor. The presence of an intracoronal restoration was the only identifiable factor in 15,3% of the patients and 14,4% of the teeth, while 15% of the patients and 16,4% of teeth showed no identifiable predisposing factors.
Denuded mineralized tissue is colonized by multinucleated cells, which initiate the resorption process. However with out further stimulation of the resorption cells, the process will continued spontaneously. Repair with cementum-like tissue will occur with in 2-3 weeks if the damaged surface does not cover a large surface area. If the damaged root surface is large, bone cells will be able to attach the root before the cementum-producing cells.
External root resorption is one type of root resorption that may occur after injury of
the precementum, apical to the epithelial attachment, followed by bacterial stimulation originating from periodontal sulcus. Injury may be caused by dental trauma, chemical irritation, orthodontic treatment or periodontal procedure. Bacteria from the periodontal sulcus may penetrate patent dentinal tubules, coronal to the epithelial attachment and exist apical to the epithelial attachment without penetrating the pulpal space (8). The damage area of the root surface is colonized by hard tissue resorbing cells which penetrate into dentin through a small denuded area, causing the resorption inside the root to spread. At the first stage the resorptive process does not penetrate the pulp space because of the protective layer of predentin (10), but rather spreads around the root in an irregular fashion. With time, the process may penetrate into the root canal. Periodontal infection resorption will include the alveolar bone adjacent to the resorption lacuna in the tooth.

51
If the resorptive process reaches a supragingival area of the crown, the vascularized granulation tissue of the resorption lacuna may be visible through the enamel showing a pink discoloration at the crown.
Radiographically the invasive root resorption can be seen as a single resorption lacuna
in the dentin, usually at the crestal bone level, expanding to the coronal and apical direction with progression of the process. Radiolucency may be observed at the bone adjacent to the resorption lacuna of the dentin.
A clinical classification has been developed by Heithesary for research purposes and also to provide a clinical guide in the assessment of cases of invasive cervical resorption:
Class 1: Denotes a small invasive resorptive lesion near the cervical area with a
shallow penetration into dentine Class 2: Denotes a well-defined resorptive lesion that has penetrated close to the
coronal pulp chamber but shows little or no extensions into the radicular dentine Class 3: Denotes a deeper invasion of dentine by resorbing tissue, not only involving
the coronal dentine but also extending into the coronal third of the root Class 4: Denotes a large invasive resorptive process that has extended beyond the
coronal third of the root
The treatment regimen for patients with an early stage of invasive cervical resorption included careful case selection, the topical application of trichloracetic acid, thorough curettage, nonsurgical root canal treatment if necessary, restoration of the resorptive defect with glass-ionomer cement, and follow-up examinations (3)
The rationale for the topical application of trichloracetic acid in the treatment of these
resorptive lesions was to utilize the proven action of this chemical agent in inducing coagulation necrosis while adjacent tissues remain free of inflammation (6). It was anticipated that this chemical agent would affect not only the resorptive tissue in the body of the lesion, but also the tissue contained in the deeper and often interconnecting channels (4). Guided tissue regenerative techniques are attractive treatment alternatives, but further clinical research is desirable to assess the overall success of these other regenerative methods. The topical application of bisphosphonates, anticlastic agents used in the treatment of osteoporosis, may offer another possible therapy.

52
References 1. Andereasen JO, Hjørting- Hansen E. Replantation of teeth. Part I. Radiographic and clinical study of 110 human teeth replanted after accidental loss. Acta Odontol Scand 1966;24:263-86. 2. Bender IB, Byers MR, Mori K. Periapical replacement resorption of permanent, vital, endodontically treated incisors after orthodontic movement: report of two cases. J Endod 1997: 23: 768–776. 3. Davidovich E, Heling I, Fuks AB. The fate of a mid-root fracture: a case report. Dent Traumatol 2005;21:170-3. 4. Heithersay GS. Treatment of invasive cervical resorption: an analysis of results using topical application of trichloracetic acid, curettage, and restoration. Quintessence Int 1999;30: 96-110. 5. Friedman S, Rotstein ILibfeld H, Stabbola A, Healing I. Incidence of external root resorption and esthetic results in 58 bleached pulpless teeth. Endod Dent Traumatol 1988;4:23-6 6. Heithersay GS, Wilson DF. Tissue responses in the rat to trichloracetic acid–an agent used in the treatment of invasive cervical resorption. Aust Dent J 1988;33:451-61. 7. Heithesary GS. Invasive cervical resorption. An analysis of potential predisposing factors. Quintessence Int 1999; 30: 83-95 8. Tronstad L. Root resorptions- etiology, terminology and clinical manifestations. Dent Traumatol 1988; 4: 241-252 9. Trope M. Root resorption of dental and traumatic origin: Classification based on. etiology. J Pract Periodont Aesthet Dent, 1998: 10: 515–524. 10. Wedenberg C. Evidence for a dentin-derived inhibitor of macrophage spreading. Scand J Dent Res 1987; 95: 381-388

53
Case 7 Endodontic treatment of maxillary central incisors with obliteration and in cooperation with prosthodontist Patient
A 77 years old white Norwegian woman (Fig.1) was on 18.01.2006 referred to the Department of Endodontics, University of Oslo by her dental undergraduate student for treatment of tooth 11 and 21.
Fig.1 Frontal view
Medical history
Parlodel Prolaktin (Anti Parkinsonism drug). Detrusitol (kidneys & urinary tract Infection).
Dental History & Chief complaint
The patient’s chief complaint is colour change of the teeth. She is discomfort with her outlook. She wants to have a crown restoration in her front teeth to change the colour and to close the median diastema in between the central incisors. Clinical Examination
Intra-oral photos showed region from maxillary right canine to maxillary left canine (Fig.2). No extra-oral pathosis was found. A normal oral mucosa was observed.

54
Fig.2 Incisal/ Palatinal view
Maxillary right canine: Amalgam restoration on D surface and the tooth responded positive to sensibility test with Endo Ice.
Maxillary right lateral incisor: A tooth-colour restoration on MIP surfaces and the tooth responded negative to sensibility test with Endo Ice.
Maxillary right central incisors: A tooth-colour restoration on IDP surfaces and the tooth responds negative to sensibility test with Endo Ice, and not tender to percussion.
Maxillary left central incisor: A small tooth-colour restoration on DP surfaces and the tooth responds negative to sensibility test with Endo Ice, and not tender to percussion.
Maxillary left lateral incisor: Sound tooth. Responded negative to sensibility test with Endo-Ice, and not tender to percussion.
Maxillary left canine: A small amalgam restoration on the P surface.
An abrasion line on the palatinal surfaces of the anterior teeth can bee seen. The other teeth in the upper and lower right quadrants showed no signs
relevant to the chief complaint. Radiographic Examination
The preoperative radiograph showed region from maxillary right canine to left lateral incisors (Fig.3).
Maxillary right lateral incisor: A radio-opaque restoration on mesial and distal surfaces. Lamina dura can be followed around the entire root.
Maxillary right central incisors: A radio-lucent restoration on the MIBP surfaces. Lamina dura can be followed around the entire root.
Maxillary left central incisor: A radiolucent-restoration on the DP surfaces. Lamina dura can be followed around the entire root.
Maxillary left lateral incisor: Sound tooth. Lamina dura can be followed around the entire root.

55
Fig. 3 Radiographic photo
Diagnosis
Vital pulp. Pre-prosthetic endodontic treatment of maxillay right and left central incisors. Treatment Plan
Treatment of vital pulp in both maxillary right and left central incisors. Root canal shaping and filling. Treatment 18.01.2006
Access cavity was done on the palatinal surface. In the first step after cavity preparation searching was done with an extra long Rosen bur size 10. The canal was obliterated. Negotiation continued with the help of microscope, 15% EDTA, and ultra-sound with K-file 15. The speed of ultra- sonic was placed on 4 with scale of 14. A control radiograph has been taken with a K- file in the canal under the searching process to control the direction and to avoid perforation to periodontal ligaments (Fig.4). The canal was found and at this time the patient felt a slight pain with treatment. Anaesthesia type (Septopcine Adrenalin) was applied.
Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol
solution. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr.15 K-Flex was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.5). Working length was 21mm with the incisal margin as reference point. The last instrument was NiTi nr.55. The root canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.

56
Fig.4 Control radiograph Fig.5 Working length radiograph 21.01.2006
The patient returned one week later. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution.
The calcium hydroxide was removed with NiTi instruments, and irrigation with 1%
sodium hypochlorite, 17% EDTA. Master gutta-percha cone was tried in, and a master cone radiograph was taken (Fig.6).
The root canal was dried with sterile paper points. The tooth was root-filled with AH
Plus and gutta-percha with a cold lateral condensation technique. The gutta-percha was removed 2mm down in the canal and sealed with IRM plugs. The access cavity was filled with IRM (Fig.7).
Fig.6 Masterpoint radiograph Fig.7 Final radiograph

57
22.01.2006 Anaesthesia type ( Septocaine Adrenalin) was applied. Access cavity was done from
the palatinal surfaces. The canal was obliterated. Searching was done with out extra long Rosen bur but with help of microscope, 15% EDTA as a lubricant and ultra-sound with K-file 15. The speed of ultra- sound was placed on 4 with scale of 14. The canal was found easy and with out the use of rosen bur.
Rubber dam was applied, and the area was disinfected with chlorhexidine- ethanol solution. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr.15 K-Flex was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.8). Working length was 21mm with the incisal margin as reference point. The last instrument was NiTi nr.55. The root canal was dried with sterile paper points. . Master gutta-percha cone was tried in, and a master cone radiograph was taken (Fig.9). The tooth was root-filled with AH Plus and gutta-percha with a cold lateral condensation technique. The gutta-percha was removed 2mm down in the canal and sealed with IRM plugs. The access cavity was filled with IRM (Fig.10).
Fig.8 Working length Fig.9 Masterpoint Fig.10 Final radiograph
Evaluation The root canal filling is dense.
Prognosis
The prognosis is considered to be good. 13 months follow up.
The patient returned to clinic one year after. She gets a crown restoration on her front teeth. She was very satisfied with the results aesthetically.

58
Fig.11 Follow up radiograph Fig.12 Frontal view with crown restoration
Discussion Full coverage crowns have long been used to restore heavily damaged teeth and/or, in
the case of metal ceramic crowns, to satisfy the patient’s aesthetic demand. Any history of dental disease and restorations could have an impact on the health of the dental pulp and further treatment might precipitate pulpal problems in the future (8).
Many authors consider frictional heat as major factor in pulpal injury, but they agree that several other essential procedures may contribute to pulpal necrosis. The procedures studied include frictional heat, desiccation, pressure applied during tooth reduction, chemical injury, ill-fitting provisional restorations, bacterial infection, cementation, and occlusion (1, 2, 4, 7, 9, 10).
Histological studies of 42 teeth prepared with diamond instruments and then extracted
48 hours later showed that coolants, although adequate to prevent burn lesions, did not minimize inflammatory responses when an applied force above 8 oz was used (10).
Jackson et al (3) reported that 5.7% of teeth had received root canal treatment some 1–6 years after cementation of a single crown or fixed bridge; unfortunately, the response rate of their study was just over 10%. Saunders & Saunders (6) conducted a crosssectional, radiographic survey of patients for whom a set of full-mouth periapical radiographs was available and reported that 19% of initially vital teeth developed periradicular radiolucency after crown placement.
The pulp could have lost its vitality due to a multitude of reasons. Mechanical and chemical insults due to tooth preparation and other clinical procedures, such as the use of pins and impression taking, and the temporary or permanent luting cements used during the construction of the restoration can lead to pulpal inflammation. But that usually resolves in time if there is no bacterial contamination (5). The presence of a pre-existing filling may suggest a compromised pulp as a result of previous carious attack and restorative procedures. The period of temporization and the type of cement would have a bearing on the pulp vitality, if marginal leakage of the temporary or permanent restoration was not excluded.

59
In my case the bacterial leakage and the chance to get necrotic pulp was the major reason for prosthodotic postgraduate student to refer the patient for endoodntic treatment. The late endodontic treatment in obliterated teeth after cementation of the crown and the damage of tooth structure was considered before prosthetic treatment. References 1. Anderson DJ, Van Praah G. Preliminary investigation of temperatures produced in burring. Br Dent J 1942;73:62-4. 2. Brannstrom M. Reducing the risk of sensitivity and pulpal complications after the placement of crowns and fixed partial dentures. Quintessence Int 1996;27:673-8. 3. Jackson CR, Skidmore AE, Rice RT (1992) Pulpal evaluation of teeth restored with fixed prostheses. Journal of Prosthetic Dentistry 67, 323–5. 4. Langeland K, Langeland LK. Pulp reactions to crown preparation, impression, temporary crown fixation, and permanent cementation. J Prosthet Dent 1965;15:129-43. 5. Olgart L, Bergenholtz G (2003) The dentine-pulp complex: responses to adverse influences. In: Bergenholtz G, Hørsted- Binslev P, Reit C, eds. Textbook of Endodontology. Oxford: Blackwell Munksgaard, pp. 21–42. 6. Saunders WP, Saunders EM (1998) Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. British Dental Journal 185, 137–40 7. Seltzer S, Bender IB. Early human pulp reactions to full crown preparations. J Am Dent Assoc 1959;59:915-30. 8. Seltzer S, Bender IB (1984) The Dental Pulp – Biologic Considerations in Dental Procedures, 3rd edn. Philadelphia: Lippincott. 9. Siegel SC, von Fraunhofer JA. Dental cutting with diamond burs: heavyhanded or light touch? J Prosthodont 1999;8:3-9. 10. Stanley HR Jr, Swerdlow H. Biological effects of various cutting methods in cavity preparation: the part pressure plays in pulpal response. J Am Dent Assoc 1960;61:450-6.

60
Case 8 Endodontic treatment of mandibular left canine in a medically compromised patient. Patient
A 54 year-Old Norwegian female (Fig.1) was referred to the Department of Endodontics, University of Oslo by his general practitioner in TAKO centre (Tannhelse- kompitansesenter for sjeldene medisinske tilstander) for treatment of mandibular left canine.
Fig.1 Frontal view Medical history
The patient has late stage of systemic lupus erythematosus which is the cause of several endogenous organs fail.
• Have a mitral insufficient and heart failure due to endocarditis. • Angina pectoris • Mild asthma • Stenosis in the internal carotids artery. • Stenosis in the internal carotid artery • epileptic convulsions • pleuritis • SLE affected intracerebral blood vessels. • Muscle weakness and coordination problem.
Her daily problem is severe headache that need the administration of opoied either orally or intra muscular injection.

61
Medicaments
• Morphine injection: For pain relief • Mevacor: Reduction of serum- cholesterol • Marevan: Coagulation inhibitor • Medrol: Cortico- steroid against acute infections when immunity system is affected • Selosok: Beta inhibitors, against hypertention • Monoket: Against angina pectoris • Premperan: Anti- emetic • Vival: Anti- epilepticum • paracet
Dental History & Chief complaint
The patient has a severe dental damage in her lower denture, and extensive caries on the rest of anterior teeth. Clinical Examination
The preoperative photo shows region from the mandibular left canine to the right lateral incisor (Fig. 2).
The examination was restricted on the reffered tooth. The patient had a problem with capacity of her mouth opening. Her skin was very sensitive to touch.
Mandibular left canine: the crown is damaged due to caries. A part of the lingual
surface is appearing above the gingival margin. The tooth responded positively to the sensibility test with Endo Ice.
Mandibular left lateral incisor: The tooth responded positively to the sensibility test with Endo Ice.
Mandibular left central incisor: The tooth responded negatively to the sensibility test with Endo Ice.
Mandibular right central incisor: Caries lesion can be seen in the distal side of the tooth, and responded negatively to the sensibility test with Endo Ice.
Fig.2 intra oral photo

62
Radiographic Examination The preoperative radiograph showed region from the mandibular left first incisor to
the canine (Fig. 3). Mandibular left first premolar: A root rest. Mandibular left canine: An O radio-opaque restoration is seen and the lamina dura can
followed around the entire root. Mandibular left lateral incisor: A D radio-opaque restoration. Lamina dura can be
followed around the entire root. Mandibular left central incisor: radio-opaque restoration in the middle of the tooth.
Lamina dura can be followed along the distal root where it widened at the apex. It seems there is no bone attachment in the mesial side of the tooth.
Mandibular right central incisor: Lamina dura can be followed along the distal root and widened apically, no bone attachment in the mesial surface.
Fig.3 Radiographic photo Diagnosis
Chronic pulpitis of the mandibular left canine. Treatment Plan
Vital pulp treatment. Treatment 24.10.06
Anesthesia type Citanest Octapressin was injected buccaly and lingually to the tooth. The caries were excavated. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. Irrigation was done with 1% sodium hypochlorite and 17% EDTA.
No.20 K-Flex was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.4).

63
Working length was 17, 0 mm with the lingual cusp as reference point. The last instrument was NiTi nr.60. The root canal was dried with sterile paper points. Master gutta-percha cone 60 was tried in, and a master cone radiograph was taken (Fig.5). The tooth was root-filled with AH Plus and gutta-percha with cold lateral condenser. The gutta-percha was removed approximately 2 mm down in the canal and sealed with an IRM plug. Access cavity was filled with IRM (Fig.6).
Fig.4 Working length Fig.5 Master cone Fig.6 Final radiograph Evaluation
The root is dens and a drop of surplus can be seen out of the apex.
Prognosis The prognosis is considered to be favourable.
Discussion
Systemic lupus erythematosus is a multisystem, autoimmune, connective-tissue disorder with a broad range of clinical presentations. There is a peak age of onset in young women between their late teens and early 40s and women to men ratio of 9:1. Ethnic groups, such as those with African or Asian ancestry, are at greatest risk of developing the disorder, which can be more severe than in white patients. This disorder is a chronic illness that can be life threatening when major organs are affected, but more commonly results in chronic debilitating ill health. Factors such as sunlight and drugs could trigger the disorder, but no one causes has been identified and systemic lupus erythematosus has a complex genetic basis.
The most striking studies of the epidemiology of lupus examined the development of
autoantibodies years before the onset of clinical features of lupus and antiphospholipid syndrome (1, 4). The investigators used the US Department of Defense serum repository, which contains about 30 million samples from service personnel taken at baseline and on average alternate years.

64
They identified 130 individuals with systemic lupus erythematosus and reported that 72 developed autoantibodies to DNA on average 2-7 years and up to 9-3 years before diagnosis.
The researchers also described the frequency of other autoantibodies, such as
antinuclear, antiRo, antiLa, antiSm, antiRNP (1), and antiphospholipid antibodies (4), before the development of clinical disease. AntiSm and antiRNP antibodies appeared shortly before diagnosis, suggesting a peak of autoimmunity, resulting in clinical illness. The data also suggest that autoantibodies alone do not necessarily result in clinical disease and that other factors, possibly genetic and environmental, could be important.The frequency of lupus could be increasing because milder forms of the disease are being recognised. For example, Uramoto and co-workers (8) examined the incidence of the disorder in Rochester, MN, USA, and noted that it had more than tripled from 1-51 per 100 000 in the 1950–79 cohort to 5·56 per 100 000 between 1980 and 1992. Trager and colleagues (7) suggested that patients with lupus nowadays could have a milder form of the disease and a better chance of survival than patients described several decades ago, probably because of an earlier diagnosis of milder disease. However, despite these improvements in survival, fatigue and other quality of life measures might not have improved. A review of 32 studies has summarised the incidence and prevalence of systemic lupus erythematosus in several countries and documented the increased disease burden, especially in non-white populations ( Fig. 7). Although there was wide variation in the prevalence of lupus worldwide, the highest prevalences were reported in Italy, Spain, Martinique, and the UK Afro-Caribbean population.
This disease is more common in women with African ancestry but is thought to be rare in West Africa, suggesting that environmental factors can contribute to the development of lupus in women whose ancestors migrated from that region. However, when women who had recently migrated from west Africa were examined, the prevalence of lupus was similar to that seen in Afro-Caribbean women but was much lower in European women (5). These data suggest that systemic lupus erythematosus is fairly common in west Africa and that there is a genetic basis for the higher risk of lupus in these
The pathogenesis of lupus remains unclear. Autoantigens are released by both necrotic
and apoptotic cells. Defects in the clearance of apoptotic cells have been described in this disorder and these defects could lead to aberrant uptake by macrophages, which then present the previously intra cellular antigens to T and B cells, thus driving the auto immune process (6). Further studies have expanded these ideas and examined possible defects in the clearance of apoptotic bodies, including complement deficiencies, defects in macrophage handling, and presentation of these antigens to the immune system (6). Cytokine patterns might also be important in the pathogenesis of lupus. Investigations (3) have drawn attention to the overexpression of the type I interferon pathway in patients—the so-called interferon signature. Abnormal signal transduction could be important in the pathogenesis of systemic lupus erythematosus.
Since 2001, there have been major advances in the treatment of this disorder. Newer, low dose cyclophosphamide regimens have already been described and biological agents are now having an effect.
Rituximab is a chimeric human-murine monoclonal antibody directed against CD20
on B cells and their precursors but not against plasma cells, which do not have this antigen. Rituximab has been widely used in the management of lymphoma and is fairly safe and well

65
tolerated. There is increasing evidence showing substantial and longlasting remissions in patients with lupus, who were previously unresponsive to conventional and novel immunosuppressive agents, such as mycophenolate mofetil.
Dorner and colleagues (2) findings suggest that epratuzumab, a fully human antiCD22
monoclonal antibody, is safe in patients with lupus and is able to reduce disease activity effectively in the short term. Intravenous immunoglobulins are increasingly being used in the treatment of resistant lupus. These drugs have a role in patients who have concomitant infection and active lupus in whom immunosuppression is risky, and they have also been used in the treatment of a wide range of clinical manifestations in systemic lupus erythematosus patients (9).
Fig.7 Table shows the incidence of SLE

66
References 1. Arbuckle MR, McClain MT, Rubertone MV, et al. Development of autoantibodies before the clinical onset of systemic lupus erythematosus. N Engl J Med 2003; 349: 1526–33. 2. Dorner T, Kaufmann J, Wegener WA, Teoh N, Goldenberg DM, Burmester GR. Initial clinical trial of epratuzumab (humanized anti-CD22 antibody) for immunotherapy of systemic lupus erythematosus. Arthritis Res Ther 2006; 8: R74. 3. Hau J, Kirou K, Lee C, Crow MK. Functional assay of type I interferon in systemic lupus erythematosus plasma and association with anti-RNA binding protein autoantibodies. Arthritis Rheum 2006; 54: 1906–16. 4. McClain MT, Arbuckle MR, Heinlen LD, et al. The prevalence, onset, and clinical signifi cance of antiphospholipid antibodies prior to diagnosis of systemic lupus erythematosus. Arthritis Rheum 2004; 50: 1226–32. 5. Molokhia M, Hoggart C, Patrick AL, et al. Relation of risk of systemic lupus erythematosus to west African admixture in a Caribbean population. Hum Genet 2003; 112: 310–18. 6. Munoz LE, Gaipl US, Franz S, et al. SLE-a disease of clearance defi ciency? Rheumatology (Oxford) 2005; 44: 1101–07. 7. Trager J, Ward MM. Mortality and causes of death in systemic lupus erythematosus. Curr Opin Rheumatol 2001; 13: 345–51. 8. Uramoto KM, Michet CJ, Thumboo J, Sunku J, O’Fallon WM, Gabriel SE. Trends in the incidence and mortality of systemic lupus erythematosus, 1950–1992. Arthritis Rheum 1999; 42: 46–50. 9. Zandman-Goddard G, Levy Y, Shoenfeld Y. Intravenous immunoglobulin therapy and systemic lupus erythematosus. Clin Rev Allergy Immunol 2005; 29: 219–28.

67
Case 9 Endodontic treatment of dens invaginatus of maxillary right lateral incisor with vital tooth. Patient
A 19 year-old Lebanese female (Fig.1) was on 01.03.07 referred to the Department of Endodontics, University of Oslo by her general practitioner from public dental health for consultation and treatment of maxillary right lateral incisor.
Fig.1 Frontal view Medical history
Non-contributory. Dental History & Chief complaint
The tooth was treated in her home country since she was eight year. The dentist did a palatinal composite filling on this tooth. The patient had no symptoms but a sinus tract buccaly that she consults her dentist. Clinical Examination
Preoperative photos showed region from maxillary right canine to maxillary left central incisor (Fig.2).
No extra-oral pathosis was found. A normal oral mucosa was observed. A sinus tract buccal to the lateral incisors.
Maxillary right canine: A sound tooth structure. The tooth responded positive to
sensibility test with Endo Ice. Maxillary right lateral incisor: A tooth-colour restoration on the palatinal surface. The
tooth responded positive to sensibility test with Endo-Ice, and tender to percussion. Maxillary right central incisor: A sound tooth structure. The tooth responded positive
to sensibility test with Endo Ice. A Gutta-percha cone was inserted din the sinus tract (Fig.3).

68
The other teeth in the upper and lower right quadrants showed no signs relevant to the
chief complaint. The gingival margin was healthy, and the probing depths were within normal limits.
Fig.2 Palatinal view Fig.3 Gutta-percha point in the sinus tract Radiographic Examination
The preoperative radiograph showed region maxillary right Canine to right central incisor (Fig.4, 5). A radiograph was taken with Gutta-percha point inserted in the sinus tract (Fig.6)
Fig.4 Pre-operative radiograph Fig.5 Mesio-eccentric Fig.6 GP in sinus tract

69
Maxillary right canine: Sound tooth. Lamina dura can be followed around the entire root.
Maxillary right lateral incisor: Had a radio lucent and a radio-opaque restoration. Lamina dura can be followed around the entire distal surface of the root where it widened to a big radiolucency of 12 mm in diameter extended to the mesial side.
Maxillary right central incisor: Sound tooth. Lamina dura can be followed around the entire root.
The height of the marginal bone was within normal limits. Diagnosis
Dens invaginatus of maxillary right lateral incisor. Treatment Plan
Instrumentation, disinfection and filling of dens invaginatus. Treatment 15.03.07
The composite filling material was removed carefully. Searching for the pathway of invaginatus done with the help of microscope (Fig.7, 8). The path way of invagination located mesially and was found with the use of an extra long Rosen bur size 08.
K-file 08 fastened to dental floss was inserted in the orifice of invagination and a
radiograph has been taken (Fig.9, 10, 11, 12).
Fig.7 After removing of filling Fig.8 Invaginatus in the mesial side

70
Fig.9 Pathway of invaginatus Fig.10 K-file 08
Fig.11 K- file 08 in dens invaginatus Fig.12 K-file 08 radiograph
Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. Nr 10 K-File was taken to working length. Control of working length with an apex locator (ProPex), and verified by a working length radiograph (Fig.13).
Working length was 10, 5 mm with the incisal edge as a reference point. The last
instrument was K-Flex nr 50. Irrigation was done with 1% sodium hypochlorite, 17% EDTA and dressed for 5 minutes with 2% chlorhexidine digluconate. The root canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canals with the help of a Lentulo spiral and sterile paper points. The access cavity was sealed with IRM.

71
Fig.13 Working length radiograph 17.04.2007
The patient returned to the clinic 4 weeks later. The sinus tract was diminishe din size and only a red area can be seen (Fig.14). Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. IRM was removed, and calcium hydroxide was removed with irrigation with 1% sodium hypochlorite and 17% EDTA. The root canals were dried with sterile paper points. Masterpoint radiograph was taken with Gutta-percha size 60 (Fig.15). White MTA was filled in canal with the help of an LM endo-plugger and sterile paper points. A wet cotton pellet was palced over inside the canal and 2mm of the canal and the cavity was sealed with IRM. A control radiograph was taken (Fig.16).
Fig.14 Area shows where the sinus tract was

72
Fig.15 Masterpoint radiograph Fig.16 MTA filled in the canal 24.04.2007
The patient returned to the clinic one week later. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. IRM was removed, and the cotton pellet was removed. The cavity was washed with 70% alcohol for removing the effect of euginol. The cavity was filled with Tetic Ceram tooth-coloured composite after the normal filling procedure. A final radiograph was taken (Fig.17).
Fig.17 Final radiograph

73
Evaluation
The filling is dens and fill the whole canal. Prognosis
The prognosis is considered to be favourable. Discussion
Dens invaginatus or “dens in dente” is a rare malformation of teeth resulting from the invagination of the tooth crown before biological mineralization occurs. The anomaly is thought to be caused by infolding of the dental papilla during development, which allows the invagination of the inner dental epithelium (9). Several factors are associated with dens invaginatus, including increased localized external pressure, focal growth retardation, and focal growth stimulation in certain areas of the tooth bud (17). A tooth with dens invaginatus is recognized by the radiopaque invagination of a small tooth-like structure of enamel and dentin tissues, extending from anywhere on the palatal surface to deep in the root. Oehlers (15). classified dens invaginatus into 3 categories according to the depth of penetration and communication with the periodontal ligament or periapical tissue (Fig. 13).
Fig. 13 Oehlers classification
Type I cases are those in which the invagination is lined by enamel and ends as a blind sac within the confines of the crown.

74
In type II, the enamel-lined invagination extends apically beyond the external cementoenamel junction, ending as a blind sac and never reaching the periapical tissues. It may or may not communicate with pulp tissue.
In type III, the invagination forms a second foramen in the apical area or ends somewhere in the periodontal ligament. It does not communicate with the pulp. Enamel can be found throughout the invagination, and sometimes cementum may be observed in the invagination.
The maxillary arch seems to be involved more frequently than the mandibular arch. Maxillary lateral incisor teeth are most commonly affected with this anomaly, and the prevalence of invaginatus is reported to be approximately 9% in maxillary lateral incisors (6, 8). Unilateral expression is common, but bilateral cases are also seen (8). Multiple instances of invagination in different teeth in the same patient and the double existence of the anomaly in the same tooth have also been reported (10, 14).Teeth with dens invaginatus may present with typical or unusual crown forms, such as peg, conic, or barrel shaped teeth, and a greater crown size (2, 5, 11). Gonçalves et al (5) and De Souza et al (1) reported an association between the invagination and talon cusps in the central incisors in both the mandibular and maxillary arches. Eden et al (3) presented a case of dens invaginatus in a mandibular second primary molar. In most cases, the thin or incomplete enamel lining of the invagination cannot prevent the entry of bacteria into the pulp, which leads to pulp necrosis with an eventual periapical inflammatory response.
The complex anatomy of a dens invaginatus may compromise instrumentation,
disinfection, and obturation of the root canals. The diagnosis of pulp vitality can be clinically important in type III cases associated with periapical inflammation when no communication exists with the vital pulp. Moreover, the infected invaginations may also lead to the early necrosis of pulp tissue before the completion of root development, leaving the tooth with an open apical foramen. The treatment options for invaginated teeth include preventive sealing or filling of the invagination, root canal treatment, endodontic apical surgery, intentional replantation, and extraction.
Treatment of invaginated teeth can be combined with periapical surgery following
insufficient root canal treatment or intentional replantation following failed periapical surgery (12, 16) In certain cases, endodontic treatment techniques may involve removal of the dens invaginatus from the root canal, apexification, obturation of the invagination alone while maintaining pulp vitality, and surgical treatment of the invagination alone (4, 7, 13). References 1. De Souza SMG, Tavano SMR, Bramante CM. Unusual case of bilateral talon cusp associated with dens invaginatus. Int Endod J 1999;32:494-8. 2. Duckmanton PM. Maxillary permanent central incisor with abnormal crown size and dens invaginatus: case report. Endod Dent Traumatol 1995;11:150-2. 3. Eden EK, Koca H, Sen BH. Dens invaginatus in a primary molar: report of case. J Dent Child 2002;69:49-53.

75
4. Girsch WJ, McClammy TV. Microscopic removal of dens invaginatus. J Endod 2002;28:336-8. 5. Gonçalves A, Gonçalves M, Oliveira DP, Gonçalves N. Dens invaginatus type III: report of a case and 10-year radiographic follow up. Int Endod J 2002;35:873-9. 6. Gotoh T, Kawahara K, Imai K, Kishi K, Fujuki Y. Clinical and radiographic study of dens invaginatus. Oral Surg Oral Med Oral Pathol 1979;48:88-91. 7. Gound TG, Maixner D. Nonsurgical management of a dilacerated maxillary lateral incisor with type III dens invaginatus: a case report. J Endod 2004;30:448-51. 8. Hamasha AA, Alomari QD. Prevalance of dens invaginatus in Jordanian adults. Int Endod J 2004;37:307-10. 9. Hulsmann M. Dens invaginatus: aetiolgy, classification, prevalence, diagnosis, and treatment considerations. Int Endod J 1997:30:79-90. 10. Jimenez-Rubio A, Segura JJ, Jimenz-Planas A, Llamas R. Multiple dens invaginatus affecting maxillary lateral incisors and a supernumerary tooth. Endod Dent Traumatol 1997;13:196-8. 11. Jung M. Endodontic treatment of dens invaginatus type III with three root canals and open apical foramen. Int Endod J 2004;37:205-13. 12. Lindner C, Messer HH, Tyas MJ. A complex treatment of dens invaginatus. Endod Dent Traumatol 1995;11:153-5. 13. Nallapati S. Clinical management of a maxillary incisor with vital pulp and type III invaginatus: a case report. J Endod 2004;30:726-30 14. Noikura T, Ooya K, Kikuchi M. Double dens in dente with a central cusp and multituberculism in bilateral maxillary supernumerary central incisor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:466-9. 15. Oehlers FAC. Dens invaginatus: variation of the invagination process and associated anterior crown form. Oral Surg Oral Med Oral Pathol 1957;10:1204-18. 16. Ortiz P, Weisleder R, de Justus YV. Combined therapy in the treatment of dens invaginatus: case report. J Endodon 2004;30:672-4. 17. Schafer WG, Hine MK, Levy BM, editors. A textbook of oral pathology. 4th ed. Philadelphia: Saunders; 1983. p. 2-58. .

76
Case 10 Treatment of maxillary right first molar with obliteration Patient
A 70 years old white Norwegian female (fig. 1) was referred to The Department of Endodontics, university of Oslo by her dental undergraduate student for treatment of maxillary right first molar.
Fig.1 Frontal view Medical history
Non- contributory Dental history and chief complain
Endodontic treatment of the maxillary right first molar had been started in the student clinic. The treatment was discontinued because of obliteration and the student found only the palatinal canal and not the others. Clinical examination
Intra- oral photo showed region from the maxillary right first molar to the distal margin of the maxillary right first canine. (Fig. 2). Normal intra- oral mucosa and no extra- oral pathosis.

77
Fig.2 Intra- oral (mirror image)
Maxillary right first molar: A temporary filling on the occlusal surface, amalgam restoration on the mesial and occlusal surface. The tooth responded negative to sensibility test with Endo Ice. The tooth was slightly tender to percussion.
Maxillary right second premolar: Amalgam restoration on MOD surfaces, the tooth responded weakly to sensibility test with Endo Ice.
Maxillary right first premolar: Amalgam restoration on DO surfaces and composite restoration on MO surfaces. The tooth responded weakly to sensibility test with Endo Ice.
The gingival margin was healthy with a slight retraction buccally of the first molar. The probing depths were within normal limits. Radiographic examination
The preoperative radiograph showed the region from the maxillary right molar to the first premolar (fig.3).
Maxillary first molar: An MOD and B radio-opaque restoration separated by tooth substance, which indicated one of the buccal cusps. The lamina dura could not be followed easy, but a radiolucent area in the apical area of all the three roots can be seen easy.
Maxillary right second premolar: a large radio-opaque restoration which cover almost the whole of the crown. The lamina dura can be followed around the entire root.
Maxillary right first premolar: An OD amalgam-like radio-opaque restoration and an MO tooth-coloured restoration. Lamina dura caould be followed and a marginal periodontitis around this tooth can be clearly.

78
Fig.3 Radiographic picture Diagnosis:
Chronic apical periodontitis, with obliteration. (K04.50) Treatment plan:
Treatment of necrotic maxillary first right molar, root canal disinfections and filling. Treatment: 15.11.2005
Removal of the temporary filling which student did. Excavate and remove the calcified tooth substances in the pulp chamber. With the help of microscope and an L and XL round bur, four canal orifices were found. Ca (OH)2 was placed in the pulp chamber and the cavity was sealed with IRM as a temporary filling. 30.11.2005
Removal of the IRM. Rubber dam was applied; the area was disinfected with chlorhexidine- ethanol solution for about one minute. The access cavity was irrigated with 1% sodium hypochlorite.
The obliterated canals were negotiated with K-Flex files 08 and 10 using EDTA as
irrigant. The working lengths were recorded with an electronic apex locator (Ray Pex) and verified radiographically (Fig. 4).

79
Fig.4 Working length The working lengths were: MB cabal 20,5 mm instrument size NiTi no. 45 MB2 canal 20,0 mm instrument size NiTi no. 45 DB canal 20,5 mm instrument size NiTi no. 45 P canal 21,5 mm instrument size NiTi no. 60
Instrumentation was done with 1% sodium hypochlorite and 17% EDTA. The canal was dried and a Ca (OH)2 is applied as an inter appointment dressing. The cavity was sealed with IRM. 11.01.2006
The patient returned one week later. The tooth was asymptomatic. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi instruments, and irrigation with 1% sodium hypochlorite, 17% EDTA. Master gutta-percha cones were tried in, and a master cone radiograph was taken (Fig. 5).
Fig.5 Master Point radiograph

80
The root canals were dried with sterile paper points. The tooth was root-filled with AH Plus and gutta-percha with a cold lateral condensation technique. The gutta-percha was removed 2mm down in the canals and sealed with IRM plugs. The access cavity was filled with IRM. (Fig. 6).
Fig.6 Final radiograph Evaluation The root canal filling in the DB root pointed away from the direction of the root apex. The instrument used in this case was NiTi flex instrument with the balanced force technique. Instrumentation was performed carefully, and the deviation may reflect a true discrepancy between the pulpal exit and the root apex. if this is not the true direction of the canal, the deviation may have happened because of obliteration. Prognosis
The endododntic prognosis was considered favourable. 12 months follow up 23.01.2007
The patient returned to the clinic 12 months later for control. The tooth was asymptomatic. A large part of the amalgam restoration had been removed and a tooth-coloured restoration applied. Clinical examination showed a pocket to the root apeces from the distal surface.

81
Fig.7 Radiographic photo Fig.8 Gutta-percha point in the pocket
Fig.9 Clinical photo New treatment plan
After the clinical examination a new treatment was suggested. An explorative flap elevation was suggested to see weather this is a periodontal pocket or a sinus tract from an apical periodontitis lesion. The patient was informed about the pocket and the new treatment plan, but declined further treatment. Discussion The goal of the treatment was to find the obliterated canals with the help of a microscope and with least possible removal of tooth substance and to disinfect the root canal system. In such cases equipment like the microscope is necessary. Otherwise complications, like perforation to the supporting tissues and bone, may easily occur.
Bacteria and bacterial products play a crucial role for the initiation of apical periodontitis (2, 3). The most common pathways of bacteria to infect the pulp are thorough caries lesion or following cavity preparation when extensive dentinal tubules are opened. Exposure of accessory canals and apical foramen in periodontal disease, erosion or cracking of the enamel, restorative procedures and direct exposure of the pulp are also pathways were bacteria can enter the pulp and cause infection (1).

82
The endodontic flora of the primary apical periodontitis consist of a mixture of both gram-positive and gram-negative bacteria and a mixture of cocci, rods, filamentous forms and spirochetes (1, 7). These micro-organisms obtain their nutritional supply through the mouth, serum proteins from periradicular tissue and metabolites from other bacteria (5). They may be present in all parts of the root canal system. The canal represents a special environment were bacterial interrelations and presence of nutritional supply may be a major factor causing infection (4). The relation between the sizes of the apical lesion is related to the number of bacterial species in the canal. Teeth with large apical lesions shows more bacterial species and large number than those with small lesions (8).
The success rate of endodotic treatment of teeth with primary apical periodontitis is ranged from 46% to 93% most likely dependent on the presence of bacteria at the time of obturation (6). In treatment resistance and failing cases, a high incidence of enteroccoci has been found (1). References 1. Gomes BPFA, Pinheiro ET, Gade-Neto CR, Sousa ELR, Ferraz CCR, Zaia AA, Teixera FB, Souza-Filho FJ. Microbiological examination of infected dental root canals. J Oral Microbial Immunol 2004; 19: 71- 76 2. Kakehasi S, Stanley H, Fitzegerald R. The effect of surgical exposures of dental pulps in germ- free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol 1965; 20: 340 3. Sundqvist G. Bacteriological studies of necrotic dental pulps. Umea University Odontological Dissertations No. 7. Umea, Sweden: University of Umea, 1976 4. Sundqvist G. Ecology of the Root Canal Flora. J Endod 1992; 9: 427-30 5. Sjögren U, Figdor D, Spängberg L, Sundqvist G. The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int Endod J 1991; 24: 119-25 6. Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of the root-filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997; 30: 297-306 7. P. N. Ramachandran Nair, BVSc, DVM. Light and electron Microscop Studies of Root Canal Flora and Periapical Lesions. J Endod 1987; 13; 29-39. 8. Weiger R, Rosendahl R, Löst C. Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesions. Int Endod J 2000; 33: 219-26

83
Case 11
Endodontic treatment of mandibular right second molar Patient
A 58 year-old white Norwegian female (Fig.1) was on 01.06.05 referred to the Department of Endodontics, University of Oslo by her general practitioners for treatment of mandibular right second molar.
Fig.1 Frontal view Medical history
Non-contributory. Dental History & Chief complaint
The patient had had pain in this region of mouth. The tooth was tender to percussion and she avoids eating on this side because of pain. The tooth had a ceramic fixed to metal crown which has been cemented for about 3 years ago. Clinical Examination
Preoperative photos showed region from mandibular right second molar to mandibular first molar (Fig.2, 3). No extra-oral pathosis was found. A normal oral mucosa was observed.

84
Fig.2 Buccal view Fig.3 Occlusal view
Mandibular right second molar: A ceramic fixed to metal crow restoration. The tooth was tender to percussion and responded negative to sensibility test with Endo Ice.
Mandibular right first molar: A ceramic fixed to metal crow restoration, and the tooth responded positive to sensibility test with Endo Ice.
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint. The gingival margin was slightly inflamed. The probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed the region from mandibular right second molar to second premolar (Fig. 4).
Fig.4 Radiographic photo
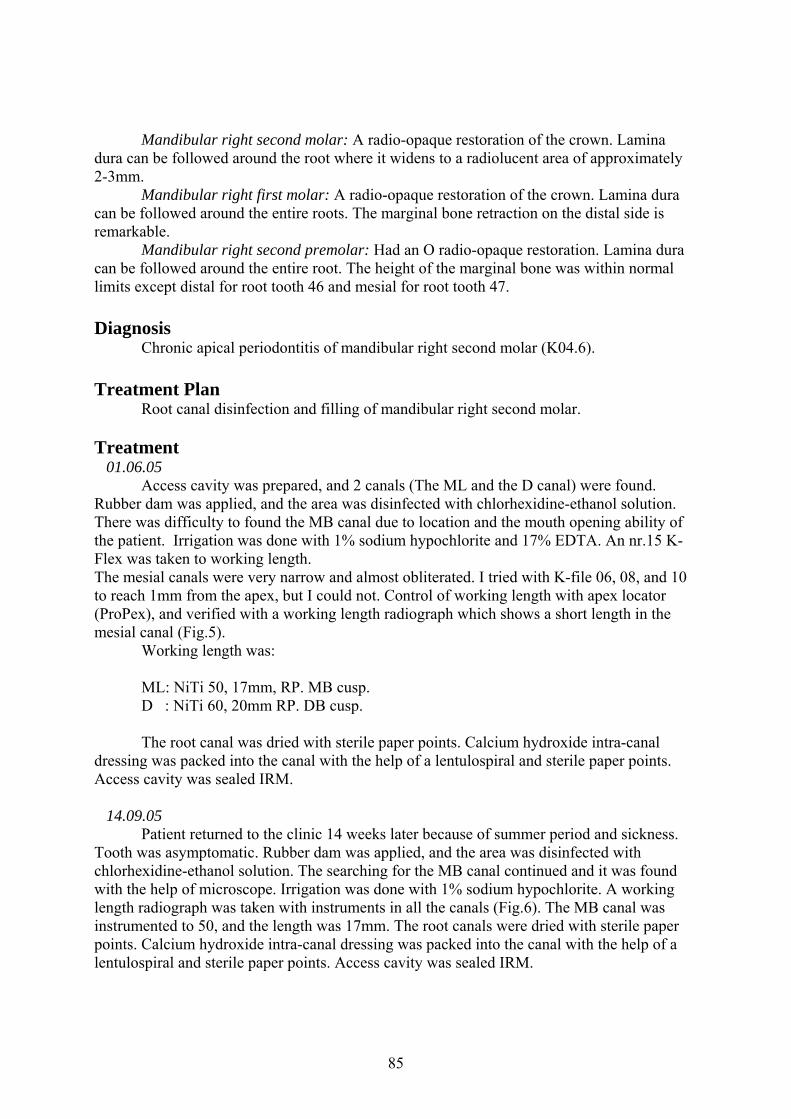
85
Mandibular right second molar: A radio-opaque restoration of the crown. Lamina dura can be followed around the root where it widens to a radiolucent area of approximately 2-3mm.
Mandibular right first molar: A radio-opaque restoration of the crown. Lamina dura can be followed around the entire roots. The marginal bone retraction on the distal side is remarkable.
Mandibular right second premolar: Had an O radio-opaque restoration. Lamina dura can be followed around the entire root. The height of the marginal bone was within normal limits except distal for root tooth 46 and mesial for root tooth 47. Diagnosis
Chronic apical periodontitis of mandibular right second molar (K04.6). Treatment Plan
Root canal disinfection and filling of mandibular right second molar. Treatment 01.06.05
Access cavity was prepared, and 2 canals (The ML and the D canal) were found. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. There was difficulty to found the MB canal due to location and the mouth opening ability of the patient. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr.15 K-Flex was taken to working length. The mesial canals were very narrow and almost obliterated. I tried with K-file 06, 08, and 10 to reach 1mm from the apex, but I could not. Control of working length with apex locator (ProPex), and verified with a working length radiograph which shows a short length in the mesial canal (Fig.5).
Working length was: ML: NiTi 50, 17mm, RP. MB cusp. D : NiTi 60, 20mm RP. DB cusp. The root canal was dried with sterile paper points. Calcium hydroxide intra-canal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed IRM. 14.09.05
Patient returned to the clinic 14 weeks later because of summer period and sickness. Tooth was asymptomatic. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The searching for the MB canal continued and it was found with the help of microscope. Irrigation was done with 1% sodium hypochlorite. A working length radiograph was taken with instruments in all the canals (Fig.6). The MB canal was instrumented to 50, and the length was 17mm. The root canals were dried with sterile paper points. Calcium hydroxide intra-canal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed IRM.

86
Fig.5 First working length Fig.6 Second working length
27.09.05 Patient returned to the clinic 2 weeks later with no symptoms from the tooth. Rubber
dam was applied, and the area was disinfected with chlorhexidine ethanol solution. The calcium hydroxide was removed with NiTi hand instruments. Irrigation was done with 1% sodium hypochlorite, 17% EDTA. Master gutta-percha cones were tried in, and a master cone radiograph was taken (Fig.7). The tooth was root-filled with AH Plus and Gutta-percha. The gutta-percha was removed approximately 2 mm down in the canal and sealed with an IRM plug. Access cavity was filled with IRM (Fig.8). The patient was referred to her dentist to complete the permanent filling.
Fig.7 Master cone radiograph Fig.8 Final radiograph

87
Evaluation The root canal filling is dens. The mesial canals are about 4 mm short.
Prognosis The prognosis is considered to be uncertain because of the short filling mesial, despite
the symptom less tooth after treatment.
16 months follow up The patient returned to clinic for control. The tooth was asymptomatic. She doesn’t
have any pain. The radiographic photo shows a favourable healing. The marginal bone of the first molar is retracted on the mesial side with the involvement of bifurcation.
Fig. 9 follows up radiograph Discussion
An infected root canal system is a reservoir for bacteria that cause apical periodontitis and it will continue until appropriate treatment is provided. This apical inflammatory reaction serves two purposes – one is to try to remove the bacteria while the other is to prevent microbial invasion into the periapical tissues (9). The former purpose is unattainable because of the lack of blood supply in the canal whereas the latter is generally successful but only until local or systemic changes occur to alter the ‘balance’ situation described above. This is when a chronic situation is likely to become acute and the patient may seek treatment because of the presence of symptoms.
There are more than 500 bacterial taxa recognized today as normal inhibitants of the oral cavity. Only a small group of microorganisms have been isolated and cultured from the root canals (about 150 reported microbial species). Individual root canals yield an average of 5-7 different species per canal (2, 4, and 10).

88
The most frequently bacterial bacterial genera isolated from the necrotic pulp are Peptostreptococcus, Prevotella, Prophyromonas, Fusobacterium, Eubacterium, Actinomyces and facultative Stereptococcus (2, 3, 4, 8, 10, and 15). The selective pressures operating in the root canal environment suggest that certain bacteria are more capable of surviving and multiply in the root canal than others, favouring the growth of obligate anaerobes in primary infected root canals (10). It has been reported that the canal microbiota recovered from asymptomatic teeth is different from that isolated from clinically symptomatic teeth (15).
Root canals of symptomatic teeth with necrotic pulps and periapical bone destruction tend to harbour a larger number of bacteria and a more complex anaerobic bacteria flora than the asymptomatic teeth with apical periodontitis. Positive correlation has been found between the number of bacteria and clinical symptoms (1, 12). Several species of bacteria of bacteria have been found in symptomatic infected root canal, with a predominance of obligate anaerobs, especially Fusobacterium, Peptostreptococcus and black pigmented bacteria (3, 15). However endodontic symptomatology itself is not an indication for systemic antimicrobial treatment except in the presence of classic signs of infection, such as swelling, surface erythema, trismus, fever or lymphadenopathy (14).
Black-pigmented bacteria were always associated with other bacteria, confirming the synergetic relationship between the bacteria found in polymicrobial infections, especially the gram-positive microorganisms. Black-pigmented bacteria need very specific nutritional requirements that are made available by some specific bacteria such as P. micros, Eubacterium spp. and Campylobacter rectus (3, 11).
The apical limit of root canal instrumentation and obturation is one of the major controversial issues in root canal therapy. Weine (13) stated that, in general, appoint located 1mm coronal to the apex ( shorter of the radiographic apex) is closed to the area of the cemento-dentine junction is the exact point where the canal preparation should end.
Kuttler (6) identified a smaller diameter or ‘apical constriction’ as the point where the canal preparation should end and where the deposition of calcified tissue is most desirable. Langeland (7) stated that the most frustrating clinical aspect is that no exact distance from the radiographic apex could be given, because it can varies widely from root to root. He demonstrated histologically that the CDJ being highly irregular and up to 3mm higher on one wall than on the opposite.
Gutierrez & Aguayo (5) examined 140 extracted permanent teeth with scanning electron microscope and found that all the canals deviate from the long axis of their roots. The number of foramina ranged from 1 to 6. The openings always ended shorter of the apices by 0.20- 3.80 mm.

89
References 1. Baumgartner JC, Watkins BJ, Bae K, Xia T. Association of black-pigmenetd bacteria with endodontic infection. J Endod 1999: 25: 413–415. 2. Gomes BPFA. An investigation into the root canal microflora [PhD thesis] Manchester (England): University dental hospital of Manchester; 1995. 3. Gomes BPFA, Drucker DB, Lilley JD. Association of endodontic signs and symptoms with particular combinations of specific bacteria. Int Endod J 1996: 29: 69-75. 4. Gomes BPFA, Drucker DB, Lilley JD. Endodotic microflora of different teeth in the same mouth. Anaerobe 1999: 5: 241-245. 5. Gutierrez JH, Aguayo P. Apical foramen openings in human teeth- number and location. Oral surg Oral Med Oral Pathol Oral Radiol Endod 1995, 79: 769-77. 6. Kuttler Y. Microscopic investigation of root apexes. J of American dental Association 1955; 50: 544-52 7. Langeland K. the histological basis in endodontic treatment. Dental Clinics of North America. Pheladelphia and London: WB Saunders Co., 1967: 491-520. 8. Möller AJR. Microbilogical examination of root canals and periapical tissues of human teeth: Methodological studies. Odontol Tidskt 1996; 74(Spec Iss): 1-280 9. Nair PNR. Apical periodontitis: a dynamic encounter between root canal infection and host response. Periodontology 2000 1997: 13: 121–148. 10. Sundqvist G. Ecology of the root canal microflora. J Endod 1992: 18: 427-430. 11. Sundqvist G. Taxanomy, ecology and pathogenicity of the root canal flora. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1994: 78: 522-530. 12. Sundqvist G, Johansson E, Sjögren U. Prevalence of black- pigmented Bacteroids species in root canal infection. J Endod 1989: 15: 13-19 13. Weine FS. Terapi Endodontica, Milano, Italy: Scienza e tecnica dentistica, Edizioni Internazionali 1982. 183-96 14. Wynn RL, Bergman AS. Antibiotic and their use in the treatment of orofacial infections, part 1. Gen Dent 1994: 42: 398-402. 15. Yoshida M, Fukushima H, Yamamoto K, Ogawa K, Toda T, Sagawa H. Correlation between clinical symptoms and microorganisms isolated from root canal with periapical pathosis. J Endod 1987: 13: 24-28.

90
Case 12
Treatment of mandibular left canine with lateral periapical lesion and suspicious about root resorpsion.
Fig.1 Frontal view
A 68 years old white Norwegian male (Fig.1) was on 06.12.2006 referred to the department of endodontics, University of Oslo by his general practitioner for treatment of root- resorption in tooth 33.
Medical history Non-contributory.
Dental history and chief complain The patient consulted his general practitioner for routine control for his teeth. The
dentist noticed that there is a sinus tract on the buccal side between the left lower lateral incisors and the canine. The patient had no pain, but he felt some times a bad odour from this area. The general practitioner takes an X-ray and he thought that it’s a root resorption. The patient has been contacted by telephone and referred to Caprio x-ray clinic to take a CT of this region. This has been done depending on the x-rays we get, to determine the location of the resorption and to win time.
Clinical examination The patient met at the given appointment with a CD of his CT from Caprio clinic.
There was very difficult to se due to scratching from the crown and post of the mandibular first premolar.

91
Fig.2 Buccal view Fig.3 Occlusal view
No extra- oral pathosis was found, and a normal oral mucosa was observed.
Mandibular right first premolar: A metal ceramic crown restoration. The tooth responded negative to sensibility test.
Mandibular right canine: Disto- lingual surfaces is built with tooth colour filling material. The tooth responded negative to sensibility test with Endo- Ice and not tender to percussion.
Mandibular right lateral incisors to mandibualr left lateral incisors are sound teeth and responded positive (with different value) to sensibility test with Endo-Ice.
Mandibualr left Canine: Disto- Lingual surfaces built with amalgam filling. Mandibular left first premolar: A DOL built with amalgam filling.
The gingival margin was healthy, and the probing depths were within normal limits.
Radiographic examination The preoperative radiograph showed region from mandibualr right second premolar to
left lateral incisor (Fig.4). Another radiograph was taken with Gutta- percha in the sinus tract (Fig.5)
Mandibular right second premolar: Had a MOD and B radio-opaque restoration. Lamina dura can be followed around the entire root.
Mandibular left second premolar: A light radio-opaque restoration is seen in the crown. Lamina dura can be followed around the entire roots.
Mandibular left first premolar: A radio-opaque restoration is seen in the crown area with a cone inserted half way in the canal. Lamina dura can be followed around the entire root.
Mandibular left canine: A radio-lucent material is seen in the distal side of the tooth. Lamina dura can be followed around the root and widened in the middle of the root and at the apex.

92
Fig.4 Preoprative radiograph Fig.5 Gutta-percha point in sinus tract
The height of the marginal bone was within normal limits.
The CT pictures were difficult to diagnose, because of metal reflection from the post in the canal of the mandibular left first premolar. After diagnosis, there was very difficult to see root resorption. The periodontal ligament widened in the level of the post in neighbour tooth. Diagnosis
Necrotic mandibular left canine (K04.62). Treatment Plan
Treatment of necrotic mandibular canine with sinus tract. Root canal disinfection and filling. K04.62
Treatment 06.12.2006
Access cavity was done from the lingual surface. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. One wide canal was located. The working length was found with K-file nr.15, and with the help of apex locator, and verified with a working length radiograph (Fig.6). Irrigation was done with 1% sodium hypochlorite, 17% EDTA, and dressed for 5 min. The root canal was dried with sterile paper points. Calcium hydroxide intra canal dressing was packed into the canals with the help of a Lentulo spiral and sterile paper points. The access cavity was sealed with IRM.

93
Fig.6 Working length radiograph 13.12.2006
The patient returned one week later. The tooth was asymptomatic and the sinus tract is diminished in size. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi instruments, and irrigation with 1% sodium hypochlorite, and 17% EDTA.
Master gutta-percha cones were tried in, and a master cone radiograph was taken (Fig.7). The root canals were dried with sterile paper points. The tooth was root-filled with AH Plus and gutta-percha with a cold lateral condensation technique. The gutta-percha was removed 2mm down in the canals and sealed with IRM plugs. The access cavity was filled with IRM (Fig.8).
Fig.7 Masterpoint radiograph Fig.8 Final radiograph

94
Evaluation The root filling looks dens and a sealer surplus was pressed out from the lateral canal.
4 months follow up The patient returns four months after for control. The radiograph (fig.9) shows favourable healing. The AH + surplus is no longer visible in the radiograph.
Fig.9 Follow up radiograph Discussion
It has been recommended that root filling should provide a complete, three-dimensional filling of the main root canal and of all accessory canals, in order to prevent the leakage of fluids and micro organisms (7). Many studies have demonstrated endodontic failure due to patent accessory canals (6, 8).Warm vertical condensation of gutta-percha has been considered to be elective at filling the ramifications of the root canal system (3, 7, and 9).
It has been established that the flow of a root canal sealer is important as it reflects its capacity to penetrate into small irregularities and also into lateral canals (4). If the material flows well, it will not completely obliterate all extensions of the root canal system (2). It has been reported that AH-26 appeared to have many advantages over other sealers as it mixed easily and flowed well. AH-26 has been subsequently replaced by AH-Plus that, according to the manufacturer, has the same physical properties ofAH-26 but no longer releases formaldehyde (5).

95
Accessory and lateral canals extend from the pulp to the periodontium. An accessory canal is any branch of the main pulp canal or chamber that communicates with the external surface of the root. A lateral canal is an accessory canal located in the coronal or middle third of the root, usually extending horizontally from the main root canal (1). They occur 73.5% of the time in the apical third, 11.4% of the time in the middle third and 6.3% of the time in the cervical third of the root. Accessory canals may also occur in the bifurcation or trifurcation of multi rooted teeth. These were called furcation canals (10). References 1. American Association of Endodontists. Glossary of Endodontic Terms, 7th edn. American Association of Endodontists, Chicago, IL, 2003: 9. 2. BenattiO, StolfWL, Ruhnke LA(1978) Verification of the consistency, setting time and dimensional changes of root canal filling materials. Oral Surgery, Oral Medicine and Oral Pathology 46,107^13. 3. Dulac KA, Nielsen CJ, Tomazic TJ, Ferrillo PJ, Hatton JF (1999) Comparison of the obturation of lateral canals by six techniques.Journal of Endodontics 25,376-80. 4. Grossman LI (1976) Physical properties of root canal cements. Journal of Endodontics 2,166-75. 5. Limkangwalmongkol S, Burtscher P, Abbott PV, Sandler AB, Bishop BM (1991) A comparative study of the apical leakage of four root canal sealers and laterally condensed guttapercha. Journal of Endodontics 17, 495-9. 6. Nichols E (1963) Lateral radicular disease due to lateral branching of the root canal. Oral Surgery, Oral Medicine and Oral Pathology16,839-45. 7. Schilder H (1967) Filling the root canal in three dimensions. Dental Clinics of North America 11,723-44. 8. Seltzer S, Bender IB, Smith J, Freedman I, Nazimov H (1967) Endodontic failures: an analysis based on clinical, radiographic and histological findings. Part I. Oral Surgery, Oral Medicine and Oral Pathology 23,500-16. 9. Silver GK, Love RM, Purton DG (1999) Comparison of two vertical condensation obturation techniques:Touch’n Heat modified and System B. International EndodonticJournal 28,35-40. 10. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1984: 58: 589–599.

96
Case13 Endodontic treatment of maxillary right second molar
Patient A 53 year old white Norwegian female (Fig.1) was on 01.12.2004 referred to the
Department of Endodontics, University of Oslo by her dental undergraduate student for treatment of maxillary right second molar.
Fig.1 Frontal view Medical history
Non-contributory. Dental History & Chief Complaint
The patient had severe pain in November 2004. She consults her Dental student where she gets acute treatment. The tooth was with out symptom since that time. Clinical Examination
Preoperative photos showed the region from maxillary right second molar to maxillary right first premolar (Fig.2). No pathosis was found extra-orally and normal oral mucosa was observed.

97
Fig.2 Occlusal view
Maxillary right third molar: Part of the tooth is shown. MO tooth-colour restoration is seen. The tooth responded positively to sensibility test with Endo- Ice.
Maxillary right second molar: MOD amalgam restoration is seen and the tooth. In the O surface there is an IRM restoration after acute treatment. The tooth is slightly tender to percussion, and responded negatively to sensibility test with Endo-Ice
Maxillary right first molar: The tooth was extracted for many years ago. Maxillary right second premolar: MOD tooth-colour restoration is seen. The margin
of restoration is discoloured. The tooth responded positively to the sensibility test with Endo Ice. The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint. The gingival margin was healthy, and the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed the region from maxillary right second molar to second premolar (Fig. 3).
Fig.3 Radiographic photo

98
Maxillary right third molar: An MO radio-opaque restoration was seen and lamina
dura could be followed around the entire roots. Maxillary right second molar: An MOD radio-opaque restoration was seen and lamina
dura could be followed around the roots was its widened 3-4mm apically. Maxillary right second premolar: An MOD radio-lucent restoration was seen and
lamina dura could be followed around the entire root. Maxillary right first premolar: An MOD radio-opaque restoration was seen.
The height of the marginal bone was within normal limits. Diagnosis
Chronic apical periodontitis of maxillary right second molar Treatment Plan
Treatment of maxillary right second molar. Root canal disinfection and filling Treatment 01.12.2004
Access cavity was prepared, and two canals were found. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr 15 K-Flex and Hedstrøm file 20 were taken to working length. The working length was controlled with an apex locator (ProPex), and verified by a working length radiograph (Fig.4). Working length was 21.5 mm with the buccal cusp as reference point for both canals.
The last instrument was NiTi nr 55. The searching for the third canal was done with
the help of microscope and different angle radiograph. Both canals located centrally (Fig.5, and 6). The root canals were dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a Lentulo spiral and sterile paper points. The access cavity was sealed with IRM.
Fig.4 Working length radiograph Fig.5 Disto- eccentric angle

99
Fig.5 Clinical photo for the Canals 14.06.2005
The patient cancelled three appointments because of different reasons. She met on the last appointment on this day. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution.
The calcium hydroxide was removed with NiTi nr 50. Irrigation was done with 1% sodium hypochlorite, 17% EDTA Master Gutta-percha cone nr 55 was tried in, and a master cone radiograph was taken (Fig.6). The root canal was dried with sterile paper points. The tooth was root-filled with AH Plus and gutta-percha with using a cold lateral condenser. The root-filling was removed 2 mm apical to the orifice and sealed with an IRM plug. The access cavity was filled with IRM (Fig.7).
Fig.6 Master Cone radiograph Fig.7 Final radiograph
Evaluation The root canal filling is tight.
B canal
P canal

100
Prognosis The endodontic prognosis is considered to be favourable.
Follow up
The patient didn’t meet for the appointment after one year. She has been called again and she refuses to have control because she lives far away after she removed away last year. She has been asked if her private dentist can take an X-ray and send it to the Endodontic department for control, she didn’t cooperate. Discussion
The evaluation of the root canal system is most accurate when the dentist uses the information from multiple radiographic views together with a thorough clinical exploration of the interior and exterior of the tooth. Diagnostic measures such as multiple pre-operative radiographs, examination of the pulp chamber floor with a sharp explorer, troughing of grooves with ultrasonic tips, staining the chamber floor with 1% methylene blue dye, performing the sodium hypochlorite ‘champagne bubble’ test and visualizing canal bleeding points are important aids in locating root canal orifices. recommends the use of 17% aqueous EDTA, 95% ethanol and the Stropko irrigator, fitted with a 27G notched endodontic irrigating needle to clean and dry the pulp chamber floor prior to visually inspecting the canal system(5).
An important aid for locating root canals is the dental-operating microscope (DOM) which was introduced into endodontics to provide enhanced lighting and visibility. The pulp cavity is divided into two portions: the pulp chamber which is located in the anatomic crown of the tooth and the pulp or root canal(s) which are found in the anatomic root. Other features include pulp horns, lateral, accessory and furcation canals, canal orifices, intercanal connections, apical deltas and apical foramina. A root canal begins as funnel-shaped canal orifices generally present at or slightly apical to the cervical line and ends at the apical foremen which opens onto the root surface between 0 and 3mm from the centre of the root apex ( 2, 3, 6).
Nearly all root canals are curved particularly in a facial-lingual direction (1). These
curvatures may pose problems during shaping and cleaning procedures because they are not evident on a standard facial radiograph. Angled views are necessary to determine their presence, direction and severity. A curvature may be a gradual curve of the entire canal or a sharp curvature near the apex. Double‘s-shaped’ canal curvatures can also occur. In most cases, the number of root canals corresponds with the number of roots but an oval-shaped root may have more than one canal. From the early work to the most recent studies demonstrating anatomic complexities of the root canal system, it has long been established that a root with a tapering canal and a single foremen is the exception rather than the rule (4).
Investigators have shown multiple foramina, additional canals, fins, deltas, intercanal
connections, loops, ‘C- shaped’ canals and accessory canals. Consequently the practitioner must treat each tooth assuming that complex anatomy occurs often enough to be considered normal. A root always contains a root canal even though one is not visible on a radiograph and is difficult to locate and negotiate.

101
The closer they are to each other the greater the chance that the two canals join at some point within the body of the root. The straight facial radiograph provides information about the mesial-distal penetration while an angled radiograph provides information about the facial-lingual penetration. These radiographs help determine the correctness of the penetration angle and its proximity to the elusive canal. When beginning an access preparation on a tooth with a calcified pulp cavity, it is helpful to do so before placing the dental dam. The LN bur (Caulk/ Dentsply, Tulsa, OK, USA), the Mueller bur (Brasseler, Savannah, GA, USA) and thin ultrasonic tips are especially useful for locating calcified root canals.
In this case the rubber dam was applied immediately after accessing the pulp chamber. When only two canals were found, searching was done with LN bur and with the help of microscope. Rubber dam was removed after that to see the canal location and its relation to the tooth counter. The tooth had only two large central canals. References 1. Cunningham CJ, Senia ES. A three-dimensional study of canal curvature in the mesial roots of mandibular molars. J Endod 1992: 18: 294–300. 2. Green D. Double canals in single roots. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1973: 35: 689– 696 3. Gutierrez JH, Aguayo P. Apical foraminal openings in human teeth – number and location. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995: 79: 769–777. 4. Hess W, Zürcher E. The Anatomy of Root Canals of the Teeth of the Permanent and Deciduous Dentitions. New York: William Wood & Co, 1925. 5. Stropko JJ. Canal morphology of maxillary molars, clinical observations of canal configurations. J Endod 1990: 25: 446–450. 6. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1984: 58: 589–599.

102
Case 14 Endodontic treatment of mandibular left second molar with one visit. Patient
A 32 year old white Norwegian female (Fig.1) sought our private dental clinic on Feb. 2006 because of acute pain in the lower right side of the mouth.
Fig.1 Frontal view (after treatment is finished) Medical history
Non-contributory. Dental History & Chief Complaint
The patient ordered appointment by her self because of acute paint in the mandibular right first premolar. She had no private dentist. Her last dental treatment was for three years ago for extraction of mandibular left second premolar as an acute treatment. She didn’t sleep well the last two nights despite the use of pain killer.
Clinical examination There was a big caries lesion in tooth nr. 45 and tooth nr. 37. No clinical photos are
available, but from her frontal view the hygiene was good, gingival margin was healthy and the probing depth was within normal limits.
Tooth 45 was tender to percussion, and responded severely positive to sensibility test with Endo-Ice.
Tooth 37 was slightly tender to percussion and responded negative to sensibility test with Endo-Ice. Radiographic examination
The preoperative radiographs showed the region from mandibular right second molar to first premolar (Fig. 2), and from mandibular left second molar to first molar (Fig.3).

103
Fig.2 Big caries lesion in tooth 45 Fig.3 Apical radiolucency in tooth 37
Mandibular right second molar: An O radio-opaque restoration. The tooth responded positive to sensibility test with Endo- Ice.
Mandibular right first molar: An O radio-opaque restoration was seen and lamina dura could be followed around the entire roots, but it’s slightly missed around the apical part of the mesial root. The tooth responded positive to sensibility test with Endo- Ice.
Mandibular right second premolar: An O radio-opaque restoration was seen and lamina dura could be followed around the entire root where it’s widened to 1-2mm around the apex. The tooth responded to sensibility test with Endo- Ice.
Mandibular right first premolar: An O radio-opaque restoration was seen and lamina dura could be followed around the entire root. The tooth responded positive to sensibility test with Endo- Ice
The height of the marginal bone was within normal limits.
Mandibular left second molar: A big radio-lucent in the crown area shows the damage in the crown part. A small radio-opaque restoration located against the distal part. The lamina dura can followed around the roots where it widened apically to 4-5 mm in diameter lesions on both roots. The tooth responded negative to sensibility test with Endo- Ice.
Mandibular right first molar: An OB radio-opaque restoration was seen and lamina dura could be followed around the entire roots. The tooth responded positive to sensibility test with Endo- Ice
The height of the marginal bone was within normal limits. Diagnosis
Acute pulpitis of mandibular right second premolar (K04.01). Chronic apical periodontitis of mandibular left second molar (K04.50).

104
Treatment The treatment of tooth 45 was done in one visit with use of rubber dam despite the
anxious for dental treatment. The patient was advised to treat the mandibular left second molar. She left the clinic with a decision to treat it. A new appointment was given. 06.02.06
The caries lesion was excavate, a clean margin and clean tooth substance was established. Rubber dam was applied and the area disinfected with chlorhexidine-ethanol solution. The access cavity was irrigated with 1% sodium hypochlorite. Working length was established by the use of K-Flex nr 15 with the aid of an apex locator (ProPex), and verified by a working length radiograph (Fig.4).
The working length was: MB canal 22 mm Last instrument size NiTi nr 45 ML canal 22 mm Last instrument size NiTi nr 45 D canal 23.5 mm Last instrument size NiTi nr 55 The DB cusp was the reference point for all the canals
Fig.4 Working length radiograph
Irrigation was performed with 1% sodium hypochlorite, 17% EDTA and dressed for 5 minutes with 2% chlorhexidine digluconate. The root canals were dried with sterile paper points.
Master Gutta-Percha points were tried in, and a master points radiograph was taken (Fig.5). The tooth was root-filled with AH Plus and gutta-percha with a cold lateral condensation technique. The root-fillings were removed 2 mm apical to the orifices and sealed with IRM plugs. The access cavity was filled with IRM.
After the removal of rubber dam a final radiograph was taken (Fig.6). The patient
referred to prosthodontics for crown treatment.

105
Fig.5 Masterpoint radiograph Fig.6 final radiograph Evaluation
The root filling is seems dens and tight. Prognosis
The prognosis is considered to be favourable. 10 months follow up
The patient is returned after ten month for control. She gets the crown restoration immediately after the root canal treatment is finished (Fig.7). The radiograph shows favourable healing (Fig.8).
Fig.7 Crown restoration Fig.8 Ten months follows up

106
Discussion It has been established beyond doubt that apical periodontitis is caused by bacteria
within root canals (4, 6). Root canal infection (Primary infection) is caused by micro organisms colonizing the necrotic pulp tissue. Micro organisms require a several factor to establish itself in the root canal system and to further participate in the pathogenesis of a periradicular disease (8). These factors like: present in sufficient number, posses a virulence factor, located in the root canal system in was that they or their virulence factors can gain access to the periapical tissues, and environment in the canal must permit the factors to survive and growth. This will cause tissue damage due to host defence mechanism in the periapical tissue.
In general, primary infections are mixed and predominated by anaerobic bacteria. Predominant species usually belong to genera Bacteroides, Porphyromonas, Prevotella, Fusobacterium, Treponema, Peptostreptococcus, Eubacterium and Campylobacter. Facultative or microaerophilic streptococci are also commonly found in primary infections (8).
The treatment of apical periodontitis should be removal of the cause, i.e. bacterial eradication. Mechanical debridement combined with antibacterial irrigation (0.5% sodium hypochlorite) can render 40–60% of the treated teeth bacteria-negative (2, 10). In addition to mechanical debridement and antibacterial irrigation, dressing the canal for 1 week with calcium hydroxide has been shown to increase the percentage of bacteria-negative teeth to around 70% (5). The regimen including calcium hydroxide dressing between appointments should provide a higher healing rate, because bacteria are further reduced. Thus, the healing rate of multiple-visit treatment should be higher than single-visit treatment (without calcium hydroxide dressing).
Single-visit root canal treatment has become common practice and offers several advantages such as a reduced flare-up rate (1, 3).
The argument for single-visit treatment relies heavily on convenience, patient acceptance and reduced postoperative pain. On the other hand, bacterial eradication cannot be predictably maximized without calcium hydroxide dressing between appointments; thus, the potential for healing may be compromised (11). The issue is very controversial, and opinions vary greatly as to the relative risks and benefits of single- versus multiple-visit root canal treatment. The direct evidence comparing healing rates following single- and multiple-visit root canal treatment should provide insight as to which regimen is more effective.
The biological benefit of multiple-visit treatment is that bacterial load can be further reduced by an antibacterial dressing between appointments, but the presence of a pathogen alone is not sufficient for persistence of disease There must be other factors that occur in combination to result in persistence of endodontic disease (9), and calcium hydroxide dressing might not be able to affect these factors. Based on clinical outcomes in Sathorns meta-analysis (7), comparing effectiveness of single- versus multiple- visit endodontic treatment, no additional benefits is provided by the use of an inter-appointment antibacterial dressing such as calcium hydroxide ( 3,12). Probably, elimination of bacteria is not strictly necessary and maximum reduction of bacteria and effective canal filling may be sufficient in terms of healing, rather than complete eradication.

107
In this case the treatment should be done with calcium hydroxide dressing between appointments, but this treatment was decided because:
• Depending on these articles with these results of single visit treatment. • The risk of leakage which may worse the prognosis if the patient didn’t appear again.
References 1. Albashaireh ZS, Alnegrish AS (1998) Postobturation pain after single- and multiple-visit endodontic therapy. A prospective study. Journal of Dentistry 26, 227–32. 2.Byström A, Sundqvist G. Bacteriologic evaluation of the effect of 0,5 percent sodium hypochlorite in endodontic therapy. Oral Surg, Oral Med Oral Pathol 1983; 55: 307-12 3. Imura N, Zuolo ML (1995) Factors associated with endodontic flare-ups: a prospective study. International Endodontic Journal 28, 261–5. 4. Kakehashi S, Stanley H, Fitzgerald R (1965). The effect of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontics 20, 340–9. 5. Law A, Messer HH (2004). An evidenced-based analysis of the antibacterial effectiveness of intracanal medicaments. Journal of Endodontics 30, 689–94. 6. Möller AJ, Fabricius L, Dahle´n G, Ohman AE, Heyden G (1981) Influence on periapical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys. Scandinavian Journal of Dental Research 89, 475–84. 7. Sathorn C, Parashos P, Messer HH. Effectiveness of single- versus multiple- visit endodontic treatment of teeth with apical periodontitis: a systematic review and meta- analysis. Int Endod J 2005; 38: 347- 55 8. Siqueira JF. Endodontic infections: concepts, paradigms, and perspectives. Oral Surg Oral Med Oral Pathol 2002; 3: 281- 293 9. Sundqvist G, Figdor D, Persson S. Life as an endodontic pathogen. Ecological differences between the untreated and root-filled root canals. Endod Topics 2003; 6: 3- 28 10. Sjögren U, Figdor D, Persson S, Sundqvist G (1997) Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. International Endodontic Journal 30, 297–306. 11. Spångberg LS (2001) Evidence-based endodontics: the one visit treatment idea [Comment]. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 91, 617–8. 12. Weiger R, Rosendahl R, Löst C. Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesions. Int Endod J 2000; 33: 219-26

108
Case 15
Endodontic treatment of dens invaginatus in maxillary left later incisor with chronic apical periodontitis Patient
A 15 year-old white Norwegian male (Fig.1) was referred to the Department of Endodontics, University of Oslo by his general practitioner for treatment of maxillary left lateral incisor.
Fig.1 Frontal view Medical history
Non-contributory. Dental History & Chief complaint
Endodontic treatment of the maxillary left lateral incisor was begun in the clinic 04.06. The dentist noticed in radiograph at the canal was very wide and there was a step coronally. She decides to refer the patient because of uncertain results. The patient had no pain and the tooth is not tender to percussion. Clinical Examination
Preoperative photos showed the region from maxillary right canine to maxillary second premolar (Fig.2)
Extra-oral no pathology was found.
From the maxillary right canine to the maxillary left first premolar are sound teeth with no filling. Accept the lateral incisor is with a palatinal white temporary filling IRM.

109
Fig.2 Palatinal view
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint. The gingival margin was slightly inflamed, and the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed region maxillary left central incisor to first premolar (Fig.3).
Maxillary left lateral incisor: Had an O radio opaque restoration. Lamina durra can be followed around the root where it widens to a radiolucent area of approximately 2mm. A radio opaque material was seen in the canal with an area in the apical part with incomplete obturation.
Maxillary left Canine: Sound tooth structure with no filling. Lamina durra can be followed around the entire root
Maxillary left first premolar: Sound tooth structure with no filling.
Fig.3 Radiographic photo

110
Diagnosis Chronic apical periodontitis of maxillary left lateral incisors. Dens invaginatus
Treatment Plan
Root canal disinfection and filling of maxillary left lateral incisors. Treatment 29.05.06
Access cavity was prepared, and one canal was found filled with calcium hydroxide. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr.50 K-Flex was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.4). Working length was 21,0mm with the buccal cusp as reference point. The last instrument was NiTi nr.60. Gates- Glidden bur was used to clean in the irregular shaped canal. The canal was dressed for 5 minutes with 2% chlorhexidine digluconate. The root canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.
Fig.4 Working length Fig.5 Master Point 10.06.06
Patient returned to the clinic three weeks later with no symptoms from the tooth. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi nr.60. Irrigation was done with 1% sodium hypochlorite, and 17% EDTA. Master gutta-percha cone #60 was tried in, and a master cone radiograph was taken (Fig.5). The root canal was dried with sterile paper points. The tooth was root-filled with AH Plus and gutta-percha with a warm Gutta- Prcha technique using the Obtura system. A control radiograph (Fig.6, and 7) to control the apical part and middle part. The gutta-percha was removed approximately 4 mm down in the canal and sealed with IRM plug. Access cavity was filled with IRM. A final radiograph has been taken (Fig.8).

111
Fig.6 Control radiograph Fig.7 Control radiograph Fig.8 Final Radiograph
Evaluation The root filling is condensate well and fill the whole canal.
Prognosis
The prognosis is considered to be good 10 months follow up April.2007
The patient returns ten months later for control. The radiographic photo shows a favourable healing (Fig.9).
Fig.9 Follow up radiograph

112
Discussion Various materials and numerous techniques have been proposed to address the
challenge of reliably filling the prepared root canal space. Currently, gutta-percha and root canal sealer are the materials of choice, but they can be used in a variety of ways to obturate root canals.
Cold lateral compaction of gutta-percha in combination with an insoluble endodontic sealer remains the most widely accepted and used obturation technique. One of the main disadvantages of this technique is its inability to replicate the inner surface of the prepared root canal. Consequently, there will be spaces between the gutta-percha and root canal wall as well as the gutta-percha cones, which are probably filled with sealer (5). Cold gutta-percha techniques rely heavily on root canal sealer to address the problem of the accessory anatomy, since the core filling material will not move out of the main canal. There are a number of warm gutta-percha methods available for filling root canals where movement of filling material from the main canal into the accessory anatomy is possible; these include warm lateral condensation, warm vertical condensation, coated carrier systems, injected thermoplasticized techniques, thermomechanical compaction and multiphase obturation. However, despite the potential flow of thermoplasticized gutta-percha into accessory anatomy, studies have shown that root canal sealer is still required to achieve the optimal seal (6, 12).
The final filling in cold gutta- percha technique is composed of a large number of GP cones tightly pressed together and joined by frictional grip and cementing substance, rather than a homogeneous mass of GP (8). Voids because of spaces between individual GP cones and the root canal walls can be seen with poor root canal preparation, curved canals, inadequate lateral pressure during condensation, or mismatches between GP cones and the prepared root canal. The resulting fill in such cases would lack homogeneity and have to rely on sealer to fill the voids. Compared with warm vertical condensation of GP can provide a high-density filling and better sealing at all portals of entry between the root canal and the periodontium (7). This technique allows the placement of a homogeneous mass of GP into the canal system with the carrier as a means of compaction (3). This technique can be more effective in filling lateral canals than cold technique. In clinical practice, the disadvantage of this technique is that the filling length is hard to control. Rapid insertion is related to overextension, whereas slow insertion tends to result in underfilling (9).
A number of studies in vitro investigated the use of warm GP obturation leading to
increased apical extrusion. Some studies verified a lower rate of overextension seen in the cases of applying cold lateral condensation (2, and 11) whereas Abarca (1) reported that there was no significant difference between the two treatments in the incidence of apical extrusion. Results using simulated models and extracted teeth were totally different from those in vivo. Without any doubt, the results of clinical trials and meta-analyses are more pertinent to clinical practice. Many clinical studies were identified in this systematic review. The results showed overextension was more likely to occur in the warm GP obturation group in comparison with the cold lateral condensation group. It was suggested that accurately defining the working length, avoiding destruction of the narrow part of the apical foramen during preparation, and using an appropriate insertion rate of warm GP can decrease the rate of overextension with warm GP (4, 5, and 10)

113
In this case the first choice for root canal obturation was warm technique due to canal internal structure and to get a full adaptation of root filling material to the walls.
References 1. Abarca AM, Bustos A, Navia M. A comparison of apical sealing and extrusion between Thermafil and lateral condensation techniques. J Endod 2001;27:670 –2. 2. Barkins W, Montgomeny S. Evaluation of Thermafil obturation of curved canals prepared by the Canal Master-U System. J Endod 1992;18:285–9. 3. Becker TA, Donnelly JC. Thermafil obturation: a literature review. General Dentistry 1997;45:46 –55, quiz 59–60. 4. Bing G, Wei R, Li-chao W. Clinical evaluation of root canal obturation with Thermafil technique. J SUN YAT-SEN University (Medical Sciences) 2005;26:470 –2. 5. Chu CH, Lo EC, Cheung GS. Outcome of root canal treatment using Thermafil and cold lateral condensation filling techniques. Int Endod J 2005;38:179–85. 6. Evans JT, Simon JHS. Evaluation of the apical seal produced by injected thermoplasticized gutta-percha in the absence of smear layer and root canal sealer. J Endod 1986;12 , 101–7. 7. Gilbert SD, Witherspoon DE, Berry CW. Coronal leakage following three obturation techniques. Int Endod J 2001;34:293–9. 8. Leduc J, Fishelberg G. Endodontic obturation: a review. General Dentistry 2003;51:232–3. 9. Levitan ME, Himel VT, Luckey JB. The effect of insertion rates on fill length and adaptation of a thermoplasticized gutta-percha technique. J Endod 2003;29:505– 8. 10. Lipski M. Comparative study on the efficacy of root canal filling with gutta-percha by lateral condensation and Thermafil obturators. Ann Acad Med Stetin 2000;46:317–30. 11. Schafer E, Olthoff G. Effect of three different sealers on the sealing ability of both thermafil obturators and cold laterally compacted gutta-percha. J Endod 2002;28:638 – 42. 12. Tagger MA, Katz A, Tamse A. Apical seal using the GPII method in straight canals compared with lateral condensation, with or without sealer. OOO 1994;78 , 225–31.

114
Case 16
Endodontic retreatment of mandibular left second molar Patient
A 65 years old white Norwegian male (Fig.1) was referred by his undergraduate student to the postgraduate student, department of endodontics, University of Oslo for re-treatment of mandibular left lower first molar.
Fig.1 Frontal view
Medical history Non-contributory
Dental history & chief complain The dental student’s plan was a crown restoration on this tooth. The tooth has been
root canal treated for many years ago with a post on the distal root. The patient had no symptoms related to this tooth.
Clinical examination The preoperative photos shows region from the mandibular left first molar to
mandiular left canine.

115
Fig.2 Buccal view Fig.3 Occlusal view
Mandibular left first molar: only 2mm of the crown part is over the gingival margin, 3-4 mm from the lingual surface is still again. An IRM filling in the occlusal surface only.
Mandibular left second premolar: The tooth covered with a crown as a restoration. Mandibular left first premolar: a small OD tooth colour filling. The erosion and
abrasion is seen clearly on the occlusal surface which affects the cusps. Mandibualr left canine: A part of this tooth can be seen with erosion and abrasion on
the occlusal surface. The gingival margin was healthy, and the probing depths were within normal limits.
Radiographic examination The pre-operative radiograph showed region from maxillary right second molar to
second premolar (Fig.4). Mandibualr left first molar: A radio-opaque root canal material which is the root canal
filling, short in the mesial root and it is unsatisfactory quality in both roots. A radio-opaque screw which is the prefabricated post. A radio-opaque filling is on the occlusal surface. Lamina dura can be followed around the root accept the apex, where it’s thickened apicaly to a condensing apical periodontitis.
Mandibular left second premolar: A radio-opaque restoration with post inside half of the canal. The apical half is root canal treated with a radio opaque material. The lamina dura can be followed around the entire root.
Mandibualr left first premolar: a small OD radio-opaque restoration. A caries lesion is seen under the filling. Lamina dura can be followed around the entire root.

116
Fig.4 Radiograph Diagnosis
Unsatisfactory root filled tooth (K04.19). Treatment Plan
Re-treatment of an endodontically treated mandibular left first molar. Root canal disinfection and filling.
Treatment 06.12.2005
The temporary filling was removed. The post was removed with ultra- sound. Excavation and removal of necrotic dentin, 4 canals were localised. Three of these canals were filled with Gutta- perch.
Rubber dam have been applied. The area was disinfected with chlorhexidine-ethanol solution. The Gutta- percha was removed with chloroform and hand instrument. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.5).
The canals were instrumented with ProTaper and after that with hand instrument. Irrigation was done with 1% sodium hypochlorite and 15% EDTA. The root canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.

117
Fig.5 Working length radiograph 11.01.2006
Patient returned to the clinic four weeks later with no symptoms from the tooth. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi hand instrument. Irrigation was done with 1% sodium hypochlorite, and 17% EDTA. Master gutta-percha cone was tried in all canals, and a master cone radiograph was taken (Fig.6).
The tooth was root-filled with AH Plus and gutta-percha using a lateral condensation
technique. The root-filling was removed 2 mm apical to the orifice and sealed with an IRM plug. The access cavity was filled with IRM (Fig.7). The patient was referred back to his undergraduate student to continue a crown treatment.
Fig. 6 Masterpoint Radiograph Fig.7 Final radiograph Evaluation
Radiographically the root-filling appeared dense and good.

118
Prognosis The prognosis is considered to be favourable.
Follow up examination 16.01.2007
The patient was asymptomatic. The clinical examination revealed normal findings, but the tooth had a good and tight a PFM (porcelain fused to metal) crown restoration. The radiographic examination demonstrated favourable healing (Fig.8, and 9).
Fig.8 Favourable healing Fig.9 Crown restoration Discussion Gutta-Percha removal
Conventional endodontic re-treatment has largely replaced endodontic surgery for the management of failed root canal treatment. This has been informed by better understanding of the factors involved in post treatment disease and the development of new instruments and techniques. However, the removal of gutta-percha filling material, particularly from apparently well-condensed root canals may be time-consuming (3). Mechanical systems have been proposed as an alternative to hand instrumentation for removing gutta-percha. A study (5) evaluate the effectiveness of various techniques for removing filling material from root canals in vitro and found that in the apical third, the K3 rotary instruments were more efficient in removing gutta-percha filling material than hand instrumentation with K-type files (SybronEndo, Orange, CA, USA); M4 system (SybronEndo) with K-type files (SybronEndo); and Endo-gripper system (Moyco Union Broach, York, PA, USA) with K-type files (SybronEndo). Coronal restoration
Several studies have shown the importance of coronal protection for the long-term survival of endodontically treated teeth. A study found that 59% of extractions of endodontically treated teeth occurred because of restorative or prosthetic failure and crown fractures (8).

119
It was suggested that endodontically treated teeth were more susceptible to unfavourable subgingival fracture and recommended cuspal coverage in all cases (1). Another study found that 83% of fractured endodontically treated teeth had three or more restored surfaces (4). The majority of factures (84%) occurred below or at the crestal bone level contributing to the poor prognosis of the tooth.
A 20 year retrospective study, found that amalgam without cuspal coverage was not adequate for coronal restoration of endodontically treated teeth and concluded that cuspal coverage was critical for their long-term prognosis (2). Reeh (6) showed that the endodontic access cavity caused only 5% decrease in tooth stiffness while MOD preparation decreased stiffness by more than 60%. Therefore, it is the cumulative loss of tooth structure from caries, restorative as well as endodontic procedures that might increase the possibility of fracture of teeth without full coronal coverage.
A study attempted to analyze the outcomes of initial endodontic treatment from an
epidemiological perspective considering tooth retention in the oral cavity as evidence of treatment success and the occurrence of untoward events as treatment failure. Observation of a large patient population over an 8-yr period revealed a high retention rate of teeth after initial endodontic treatment regardless of the etiology, specific treatment technique, tooth group, or special patient characteristics. Overall, about 97% of teeth were retained in the oral cavity for 8 yr after completion of the initial non-surgical endodontic treatment. The analysis of the teeth extracted during the follow-up period revealed that more than 83% had no full coronal coverage. This group included teeth without any coronal restoration or teeth with large, multiple-surface amalgam or composite restorations. The number of extracted teeth without full coronal coverage was five to six times higher than fully covered teeth (7).
References 1. Fennis WM, Kuijs RH, Kreulen CM, Roeters FJ, Creugers NH, Burgersdijk RC. A survey of cusp fractures in a population of general dental practices. Int J Prosth 2002;15:559–63. 2. HansenEK, AsmussenE, ChristiansenNC. Invivo fractures of endodontically treated posterior teeth restored with amalgam. Endod Dent Traumatol 1990;6:49–55. 3. Ladley R, Campbell AD, Hicks ML, Li SH. Effectiveness of halothane used with ultrasonic or hand instrumentation to remove gutta percha from the root canal. J Endod 1991;17, 221–2. 4. Lagouvardos P, Sourai P, Douvitsas G. Coronal fractures in posterior teeth. Oper Dent 1989;14:28–32. 5. Masiero AV, Barletta FB. Effectiveness of different techniques for removing gutta-percha during retreatment. Int Endod J 2005; 38, 2–7. 6. Reeh ES, Messer HH, Douglas WH. Reductionintooth stiffness as a result of endodontic and restorative procedures. J Endod 1989;15:512–6. 7. Salehrabi R, Rotstein I. Endodontic treatment outcomesin a large patient population in the USA: An epidemiological study. J Endod 2004; 30:846-50 8. Vire DE. Failure of endodontically treated teeth: classification and evaluation. J Endod 1991;17:338–42.

120
Case 17 Endodontic re-treatment of mandibular right first molar with separated instrument. Patient
A 29 year-old white Norwegian male (Fig.1) was on 26.10.04 referred to the Department of Endodontics, University of Oslo by his dental undergraduate student for re-treatment of mandibular right second molar.
Fig.1 Frontal view
Medical history Non-contributory.
Dental History & Chief complaint
Endodontic treatment of the mandibular right first molar was done for 4 years ago. The dental student treatment plan was to do a crown (ceramic fixed to metal) restoration on this tooth. A periapical radiograph had been taken to control the quality of root canal treatment. The patient had no pain in this tooth. Clinical Examination
Preoperative photos showed region from mandibular right third molar to mandibular first premolar (Fig.2). No extra-oral pathosis was found. A normal oral mucosa was observed.

121
Fig.2 Occlusal view
Mandibular right second molar: Amalgam restoration on O surface and the tooth responded positively to sensibility test with Endo Ice.
Mandibular right first molar: Temporary restoration on MO surfaces, and the tooth responded negatively to sensibility test with Endo Ice.
Mandibular right second premolar: Sound tooth and responded positively to sensibility test with Endo Ice.
Mandibular right first premolar: Sound tooth and responded positively to sensibility test with Endo Ice.
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint. The gingival margin was healthy, and the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed region from mandibular right second molar to first premolar (Fig.3).
Mandibular right second molar: O radio-opaque restoration. Lamina dura can be followed around the root.
Mandibular right first molar: MOD radio-opaque restoration. Radio-opaque root filling material is also seen in the canal. A high radio opaque line in the M canal is seen which the separated instrument is. Lamina dura can be followed around the entire roots where it widens to 3-4mm in the apical part of the mesial root.
Mandibular right second premolar: No restoration can be detected. Lamina dura can be followed around the entire root.
Mandibular right first premolar: No restoration can be detected. Lamina dura can be followed around the entire root.
The height of the marginal bone was within normal limits.

122
Fig.3 Radiographic Photo
Diagnosis
Chronic apical periodontitis mandibular right first molar with separated instrument (K04.5) / (K04.19). Treatment Plan
Removal and re-treatment of an endodontically treated mandibular right second molar with separated instrument. Treatment 02.05.06
Access cavity was prepared, and 3 canals were found filled with gutta-percha. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution Gutta-percha was removed with the help of ProTaper F3. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. The instrument could not been seen with microscope but only feel with instrument.
The instrument was bypassed with K-file 08, and 10. The separated instrument type
Lentulospiral was removed (Fig.4) with the help of EDTA as irrigate in the canal and Ultra-sound apparatus (Fig.5) with a low speed just to help the EDTA flow around the separated instrument and with Hedstrøm file.

123
Fig. 4 The separated instrument An nr.15 K-Flex was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.6).
Working length was MB canal: 19,5mm, instrument 45. RP. MB casp. ML cabal : 19,5mm, instrument 45. RP. MB cusp D canal: 19mm, instrument 60. RP. DB cusp The canal was dressed for 5 minutes with 2% chlorhexidine digluconate. The root
canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.
Fig.6 Working lenght radiograph

124
05.09.06 Patient returned to the clinic four months later (because of summer vacation) with no
symptoms from the tooth. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi hand instrument. Irrigation was done with 1% sodium hypochlorite, 17% EDTA, and dressed for 5 minutes with 2% chlorhexidine digluconate. Master gutta-percha cones were tried in, and a master cone radiograph was taken (Fig.7).
The root canals were dried with sterile paper points. The tooth was root-filled with AH
Plus and gutta-percha using cold lateral condenser. The gutta-percha was removed approximately 2 mm down in the canal and sealed with an IRM plug. Access cavity was filled with IRM (Fig.8).
Fig.7 Master Cone radiograph Fig.8 Final radiograph
Evaluation The root filling is dens and tight. A sealer surplus can be seen in the mesial root.
Prognosis The prognosis is considered to be good.
Seven moths follow up The patient returns for control. The tooth has a temporary crown (Fig.9). The
undergraduate dental student had begun with crow preparation of this tooth. The radiographic photo shows a favourable healing (Fig.10).
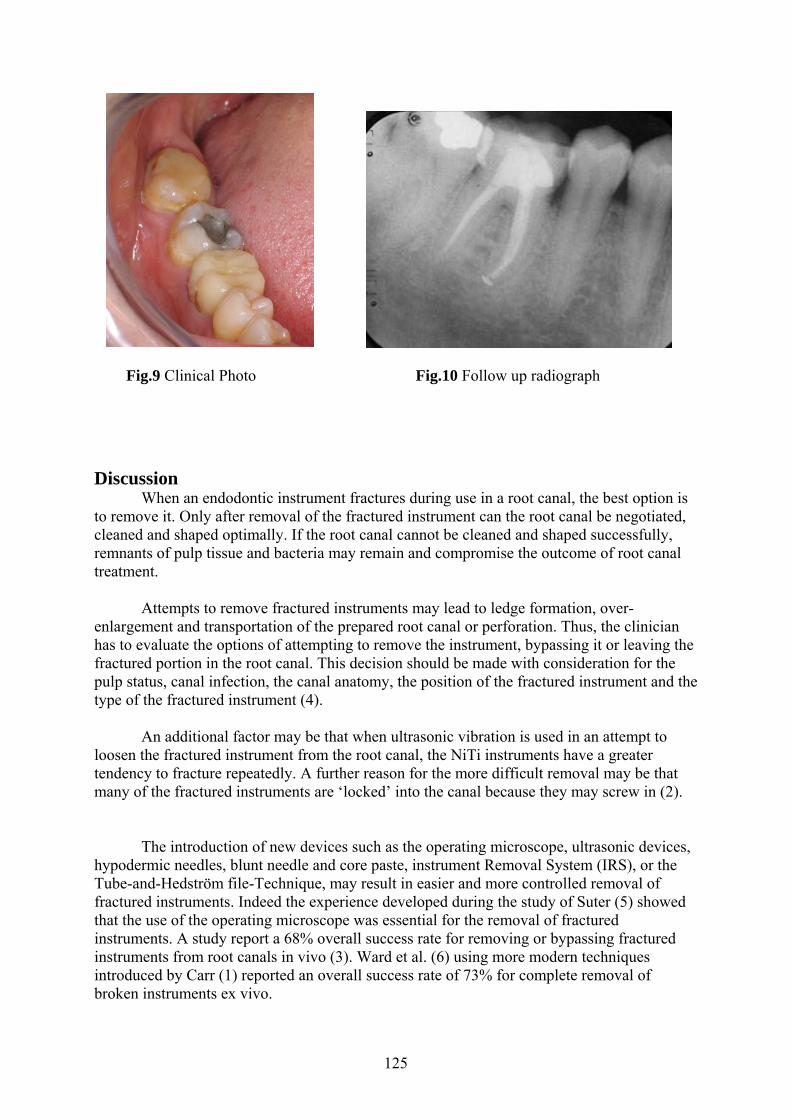
125
Fig.9 Clinical Photo Fig.10 Follow up radiograph Discussion
When an endodontic instrument fractures during use in a root canal, the best option is to remove it. Only after removal of the fractured instrument can the root canal be negotiated, cleaned and shaped optimally. If the root canal cannot be cleaned and shaped successfully, remnants of pulp tissue and bacteria may remain and compromise the outcome of root canal treatment.
Attempts to remove fractured instruments may lead to ledge formation, over-
enlargement and transportation of the prepared root canal or perforation. Thus, the clinician has to evaluate the options of attempting to remove the instrument, bypassing it or leaving the fractured portion in the root canal. This decision should be made with consideration for the pulp status, canal infection, the canal anatomy, the position of the fractured instrument and the type of the fractured instrument (4).
An additional factor may be that when ultrasonic vibration is used in an attempt to loosen the fractured instrument from the root canal, the NiTi instruments have a greater tendency to fracture repeatedly. A further reason for the more difficult removal may be that many of the fractured instruments are ‘locked’ into the canal because they may screw in (2).
The introduction of new devices such as the operating microscope, ultrasonic devices, hypodermic needles, blunt needle and core paste, instrument Removal System (IRS), or the Tube-and-Hedström file-Technique, may result in easier and more controlled removal of fractured instruments. Indeed the experience developed during the study of Suter (5) showed that the use of the operating microscope was essential for the removal of fractured instruments. A study report a 68% overall success rate for removing or bypassing fractured instruments from root canals in vivo (3). Ward et al. (6) using more modern techniques introduced by Carr (1) reported an overall success rate of 73% for complete removal of broken instruments ex vivo.

126
In certain clinical situations it may also be better to leave a fractured instrument in the root canal. For example, when the instrument fractures in a canal with a vital pulp towards the end of the cleaning and shaping phase, or if it fractures when removing a calcium hydroxide dressing in an uncomplicated case (4).
Van Beek (7) described in detail the anatomy of permanent teeth. It was noted that in maxillary first permanent molars, the buccal root canals had a marked distal curvature with respect to the wide palatal canal. In mandibular first permanent molars the distal root canal was less curved than the two mesial root canals. For practical reasons in this in vivo study buccal root canals of maxillary molars and mesial root canals of mandibular molars were defined as curved and all other root canals as straight.
The type of tooth also affects the removal of the fragment from the canal. The length of fragment tended to affect the success rate. Fragments shorter than 5 mm presented the lowest success rate (3). References 1. Carr GB (1992) Microscopes in endodontics. Journal of the Californian Dental Association 20, 55–61. 2. Crump MC, Natkin E. Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation. J Am Dent Assoc 1970;80:1341–7. 3. Hülsmann M, Schinkel I. Influence of several factors on the success or failure of removal of fractured instruments from the root canal. Endod Dent Traumatol 1999;15:252-8. 4. Rocke H, Guldener PHA (1993) Obstruktion des Wurzelkanals. In: Guldener PHA, Langeland K, eds. Endodontologie, 3rd edn. Stuttgart: Thieme, pp. 293–312. 5. Suter B (1998) A new method for retrieving silver points and separated instruments from root canals. Journal of Endodontics 24, 446–8. 6. Ward JR, Parashos P, Messer HH (2003) Evaluation of an ultrasonic technique to remove fractured rotary nickeltitanium endodontic instruments from root canals: an experimental study. Journal of Endodontics 29, 756–63. 7. Van Beek GC (1983) Endodontic anatomy of the permanent teeth. In: Van Beek GC, ed. Dental Morphology. 2nd edn. Bristol: Wright, pp. 109–22.

127
Case 18 Endodontic re-treatment of endodontically treated mandibular left second molar Patient
A 37 year-old white finish female (Fig.1) was referred to the Department of Endodontics, University of Oslo by her dental undergraduate student for re-treatment of mandibular left second molar.
Fig.1 Frontal view Medical history
Non-contributory. Dental History & Chief complaint
Endodontic treatment of the mandibular left second molar was done in her home country for about 4 years ago. The postgraduate student had a plan to do a crown restoration on this tooth. The patient complaints some times of slight pain and tenderness in the buccal area. Clinical Examination
Preoperative photos showed region from mandibular left second molar to the distal part of mandibular canine (Fig.2, and 3). Extra-oral no pathosis was found. A normal oral mucosa was observed.

128
Fig.2 Buccal view Fig.3 Occlusal view
Mandibular left second molar: Amalgam restoration on MODL surfaces, and the tooth was slightly tender to percussion.
Mandibular left first molar: Amalgam restoration on MODBL surfaces, and the tooth responded posetive to sensibility test with Endo Ice.
Mandibular left first premolar: Amalgam restoration on MOD surfaces, and the tooth responded positive to sensibility test with Endo Ice.
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint. The gingival margin was healthy, and the probing depths were within normal limits. Radiographic Examination
The preoperative radiograph showed region mandibular left second molar to first premolar (Fig. 4).
Mandibular left second molar: MOD radio-opaque restoration on the coronal part. The canals are filled with radio-opaque root fillings material. A big radio-opaque post is placed in both the mesial and distal root. Lamina dura can be followed around the root where it widens to a radiolucent area of approximately 3mm.
Mandibular left first molar: MOD radio-opaque restoration. Lamina dura can be followed around the entire roots. In the cervical area of the distal root a radiolucent area was seen.
Mandibular left second premolar: MOD radio-opaque restoration. Lamina dura can be followed around the entire root.
The height of the marginal bone was within normal limits except for the mesial side of the tooth 37.

129
Fig. 4 Radiographic Photo Diagnosis
Chronic apical periodontitis of mandibular right second molar with perforation. Treatment Plan
Retreatment of an endodontically treated mandibular left second molar. Sealed the perforation area. Treatment 28.03.2006.
Access cavity was prepared, and 3 canals were found, one was filled with gutta-percha and the other tow with the post. The posts were removed carefully with the help of microscope and the Ultra- sound (Fig.5, and 6). Gutta-percha was removed with the help of ProTaper F3. The last 4 mm in the D canal was removed with Hedstrøm file to prevent pushing it in the apical area. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. The perforation area in the ML canal and the D canal bleeds a lot. Hedstøm file size 40 was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.7 and 8)
Working length was 18,5mm with the buccal cusp as reference point. The last instrument was Reamer 70.The canals were dressed for 5 minutes with 2% chlorhexidine digluconate. The root canals were dried with sterile paper points. Calcium hydroxide intra-canal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.

130
Fig.5 Post from the D canal Fig.6 Post from the ML canal
Fig.7 Working length Fig.8 Working length 09.05.06
Patient returned to the clinic eight weeks later with no symptoms from the tooth. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed, and the ML and D canals were filled and sealed in the perforation area with grey MTA. Radiograph was taken to control the density of the MTA (Fig.9). Wet cotton pellet was placed over the MTA. The MB canal was dressed with calcium hydroxide intra-canal dressing. The cavity was sealed with IRM.
Fig.9 MTA in the distal canal

131
13.06.06
Patient returned to the clinic five weeks later. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed from the MB canal with NiTi hand instrument. The cotton pellets were also removed from the ML and D canal. Irrigation was done with 1% sodium hypochlorite, and 15% EDTA. Master gutta-percha cone 50 was tried in, and a master cone radiograph was taken (Fig.10). The root canal was dried with sterile paper points. The canal filled with AH Plus and gutta-percha using a cold lateral condenser. The gutta-percha was removed approximately 2 mm down in the canal and all the canals sealed with an IRM plug. Access cavity was filled with IRM (Fig.10).
Fig 10 Final radiograph Evaluation
The root filling material MTA in the distal root is condensed with ultrasonic indirectly and carefully, but a good amount is located out side of the canal. Prognosis
The prognosis is considered to be uncertain. 10 months follow up April. 2007
The patient returns ten months later for control. She hadn’t had any kind of symptoms from this tooth after treatment. The radiographic photo shows a favourable healing especially the distal root (Fig.11).

132
Fig.11 Follow up radiograph Discussion
Mineral trioxide aggregate (MTA) was developed as a root-end filling material for periapical surgery and for the sealing of communications between the root canal system and the surrounding tissues . MTA was shown to be superior to other commonly used root-end filling materials such as amalgam, IRM, and Super-EBA in studies of marginal adaptation and leakage (9, 14).
MTA was reported to be biocompatible in many studies in vitro and in vivo. Koh et al
(4) studied the cytomorphology of osteoblasts and cytokine production in the presence of MTA. They reported that MTA offers a biologically active substrate for bone cells and stimulates interleukin production. Zhu et al (16) reported that osteoblasts have a favourable response to MTA as compared with IRM and amalgam.
At present, MTA is widely used in endodontic therapy. It has shown good results
when used in the treatment of immature apices, for repairs of perforations, and for direct pulp capping as in root-end filling. Recently, studies have compared MTA with Portland cement (PC) and the findings suggest that PC has major ingredients in common with MTA. Some of these ingredients are calcium phosphate, calcium oxide, and silica. MTA also contains bismuth oxide, which increases its radio opacity; this is absent in PC (11). MTA and PC have almost identical properties macroscopically, microscopically, and by x-ray diffraction analysis. It was also shown that PC and MTA have a similar effect on pulpal cells when used as a direct pulp-capping material in rats. Furthermore, osteoblast-like cells had similar growth and matrix formation when grown on either set MTA or PC (15).
The biocompatibility of MTA has been investigated in a number of ways, using cell expression and growth, subcutaneous and intra-osseous implantation and direct contact with dental tissues in vivo. When MTA (Loma Linda University) has been used for root-end filling in vivo, less periradicular inflammation was reported compared with amalgam (10). In addition, the presence of cementum on the surface of MTA (Loma Linda University) was a frequent finding (13). MTA (ProRoot) supported almost complete regeneration of the periradicular periodontium when used as a rootend filling material on noninfected teeth (6).

133
The most characteristic tissue reaction to MTA was the presence of organizing connective tissue with occasional signs of inflammation after the first postoperative week (3). Early tissue healing events after MTA root-end filling were characterized by hard tissue formation, activated progressively from the peripheral root walls along the MTA–soft tissue interface (3). Both fresh and set MTA (ProRoot) caused cementum deposition when used after apical surgery (1). In addition, MTA (ProRoot) showed the most favourable periapical tissue response of three materials tested, with formation of cemental coverage over MTA (2).
MTA (ProRoot) implantation in the mandible of guinea pigs resulted in bone healing
and minimal inflammatory reactions (7). The tissue reaction to MTA (Loma Linda University) implantation was the most favourable reaction observed in both tibia and mandible of test animals, as in every specimen, it was free of inflammation. In the tibia, MTA (Loma Linda University) was the material most often observed with direct bone apposition (8, 12). In another study MTA (ProRoot,) was shown to be biocompatible and did not produce any adverse effect on microcirculation of the connective tissue (5).
References 1. Apaydin ES, Shabahang S, Torabinejad M. Hard-tissue healing after application of fresh or set MTA as root-endfilling material. J Endo 2004;30:21–4. 2. Baek SH, Plenk H, Kim S. Periapical tissue responses and cementum regeneration with amalgam, Super EBA, andMTA as root-end filling materials. J Endo 2005;31:444–9. 3. Economides N, Pantelidou O, Kokkas A, Tziafas D. Short-term periradicular tissue response to mineral trioxide aggregate (MTA) as root-end filling material. Inter Endo 2003;36:44–8. 4. Koh ET, McDonald F, Pitt Ford TR, Torabinejad M. Cellular response to mineral trioxide aggregate. J Endod 1998;24:543-7. 5. Masuda YM, Wang X, Hossain M et al. Evaluation of biocompatibility of mineral trioxide aggregate with an improved rabbit ear chamber. J Oral Rehab 2005;32:145–50. 6. Regan JD, Gutmann JL, Witherspoon DE. Comparison of Diaket and MTA when used as root-end filling materials to support regeneration of the periradicular tissues. IEJ 2002;35:840–7. 7. Saidon J, He J, Zhu Q, Safavi K, Spangberg LS. Cell and tissue reactions to mineral trioxide aggregate and Portland cement. OOOOE 2003;95:483–9. 8. Torabinejad M, Ford TR, Abedi HR, Kariyawasam SP, Tang HM. Tissue reaction to implanted root-end filling materials in the tibia and mandible of guinea pigs. J Endo;24: 468–71. 9. Torabinejad M, Higa RK, McKendry DJ, Pitt Ford TR. Dye leakage of four root-end filling materials: effects of blood contamination. J Endod 1994;20:159-63.

134
10. Torabinejad M, Hong CU, Lee SJ, Monsef M, Pitt Ford TR. Investigation of mineral trioxide aggregate for rootend filling in dogs. J Endo 1995;21:603–8. 11. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR. Physical and chemical properties of a new root-end filling material. J Endod 1995;21:349-53. 12. Torabinejad M, Hong CU, Pitt Ford TR, Kariyawasam SP. Tissue reaction to implanted Super EBA and Mineral Trioxide Aggregate in the mandible of guinea pigs: a preliminary report. J Endo 1995;21:569–71. 13. Torabinejad M, Pitt Ford TR, McKendry DJ, Abedi HR, Miller DA, Kariyawasam SP. Histologic assessment of Mineral Trioxide Aggregate as root end filling material in monkeys. J Endo 1997;23, 225–8. 14. Torabinejad M, Smith PW, Kettering JD, Pitt Ford TR. Comparative investigation of marginal adaptation of mineral trioxide aggregate and other commonly used root-end filling materials. J Endod 1995;21:295-9. 15. Wucherpfennig AL, Green D. Mineral trioxide vs. Portland cement: two biocompatible filling materials [abstract]. J Endod 1999;25:308. 16. Zhu Q, Haglund R, Safavi KE, Spångberg LSW. Adhesion of human osteoblasts on root-end filling materials. J Endod 2000; 26:404-406.

135
Case 19 Endodontic re-treatment of maxillary left central incisor with sinus tract and use of a novel root filling material Patient
A 51 year-old white Russian female (Fig.1) was 10.05.2006 referred to the Department of Endodontics, University of Oslo by her general practitioner for re-treatment of maxillary left central incisor.
Fig. 1 Frontal view Medical history
Non-contributory. Dental History & Chief complaint
Endodontic treatment of the maxillary left central incisor was done in the Russia for about seven years ago. The patient gets pain and slight swellings in the buccal side of the tooth. She went to her private dentist for treatment. He referred her to the department for treatment. Clinical Examination
Inta-oral photos showed region from maxillary right Canine to maxillary left first premolar (Fig.2). No extra oral pathosis was found. A normal oral mucosa was observed.

136
Fig.2 Occlusal/ palatinal view (mirror image)
A sound tooth structures can be seen from the maxillary right Canine to the maxillary left first premolar. Except for maxillary left central incisor which is with a colour tooth restoration in all surfaces. Radiographic Examination
The pre-operative radiograph showed region from maxillary right lateral incisors to maxillary left canine (Fig. 3).
Maxillary left central incisors: A radio-opaque restoration covered all the crown part. A wide radio-opaque post is filling the whole canal, except the last 2 to 3 mm. Lamina dura can be followed around the root except on the apical half part of the root and in the mesial side. A radio lucent area of 4-5 mm can bee seen.
All the adjacent teeth are sound and with no restoration.
Fig.3 Radiographic photo

137
Diagnosis Chronic apical periodontitis of maxillary left central incisors with a sinus tract
(K04.62). Treatment Plan
Re-treatment of endodontically treated maxillary left central incisor. Root canal disinfection and filling.
Treatment 10.05.2006
Access cavity was prepared, and the tip of the post was found. Rubber dam was applied, and the area was disinfected with chlorhexidin- ethanol solution. The composite around the post loosened carefully with the help ultra- sonic machine and a K- file 20 on the cement material. The post was removed with needle forceps and ultra- sound indirectly on the forceps. The post was about 13-14 mm long. Erosion was noticed in almost all the surface of it (Fig.4).
There was a lot of bleeding from the canal. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. Nr. 60 Hedstøm file was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.5).
Working length was 18, 5 mm with the incisal cusp as reference point. The last
instrument was Reamer size 80. There was a perforation, 2-3mm from apex, to the adjacent periodontal ligaments buccaly.
The root canal was dried with sterile paper points. Calcium hydroxide intracanal dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.
Fig.4 After removal of the post Fig.5 Working length radiograph

138
14.06.06
Patient returned to the clinic three weeks later with no symptoms from the tooth. The sinus tract was diminished in size and almost closed. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi nr.80. Irrigation was done with 1% sodium hypochlorite, 17% EDTA, and dressed for 5 minutes with 2% chlorhexidine digluconate.
The canal dried with sterile paper points and was filled with a 5mm MTA. A wet
cotton pellet with sterile water applied over the MTA and the access cavity was sealed with IRM.
Fig.6 final radiograph
Evaluation The root filling material MTA is dens and about 4-5 mm length.
Nine moths follow up The patient returns nine moths later for control. She guts the crown restoration three
weeks after the endodontic treatment was finished. The clinical photos (Fig. 7, and 8) show a good marginal adaptation of the crown. The radiographic photo (Fig.9) shows a favourable healing.

139
Fig.7 Palatinal view Fig.8 Frontal view
Fig.9 Radiographic photo Fig.10 Mesio-eccentric angle Discussion
Endodontic retreatment often involves the removal of intraradicular posts. Abbott (1) studied 2000 patients treated in an endoddontic practice and found that 36.7% of these cases received endodontic re-treatment and 25.7% of these initially required post removal. This represented 9.4% of all cases treated and demonstrates the need to be proficient at removing posts a traumatically to prevent cracks or vertical fractures developing in the roots.
Many techniques have been devised to aid the removal of posts. These include the use
of burs or trephines, devices that grasp the posts so that they can be pulled out of the root with the use of ultrasonic. Many factors that affect the retention of posts like post type, post design ( taper, parallel, smooth, serrated, or threaded), the cementing medium, the cementing depth, and post adaptation to the root canal ( 2, 10). Variation of any of these factors may affect retention.

140
Intraradicular post are usually used in weakened teeth with a little remaining coronal
structure. Therefore, post removal requires special care and techniques to prevent root fracture or perforation. Ultrasonic has provided clinicians with a useful adjunct to facilitate post removal with minimal loss of tooth structure and root damage (2, 6). Many studies have focused on the removal of metallic posts; however, re-treatment of fiber-reinforced composite posts cemented with adhesive systems presents a new challenge in cases in which endodontic treatment has failed (7).
Using ultrasonic involves the initial removal of restorative materials and luting cement around the post, followed by application of the tip of an ultrasonic instrument to the post. Ultrasonic energy is transferred through the post and breaks down the cement until the post loosens (4). This method of post removal minimizes loss of tooth structure and decreases the risk of tooth damage (3, 6). The relative ease of removing prefabricated parallel posts with the use of ultrasonic is probably related to their design, as they do not adapt well to the coronal third of most root canals. This allows for easy breakdown of the cement in the coronal third and subsequent shifting of the fulcrum point toward the apical end of the post. As the fulcrum point shifts apically, the ultrasonic vibrations start to move the post about this point and within the space created in the coronal third. This movement helps to break down the cement/post interface toward the apical end of the post in conjunction with breakdown within the cement itself.
In cases in which the post has a tight fit with adequate length and diameter, and with limited access to the coronal portion, the effect of ultrasonic alone may be limited or even ineffective. In these situations the clinician has to consider other treatment options (8).
Satterthwaite et al. (9) investigated temperature rise of the root surface during ultrasonic instrumentation of ceramic and stainless steel posts and found an inverse relationship between temperature rise and remaining dentine thickness.
Because this generates heat, especially over longer periods of application, cooling with a water spray is of the essence. When heat is transferred to a metal post, it can be transferred to the periodontal ligament, causing damage (5).

141
References 1. Abbott PV (1994). Analysis of a referral based endodontic practice. Part 2. treatment provided. Journal of endodontics 20.253-7. 2. Chan FW, Harcourt JK, Brockhurst PJ (1993) The effect of post adaptation in the root canal on retention of posts cemented with various cements. Austuralian dental Journal 38, 39-45. 3. Chenail BL, Teplitsky PE. Orthograde ultrasonic retrivial of root canal obstructions. J Endod 1987;13:186 –90. 4. Garrido AD, Fonseca TS, Alfredo E, Silva-Sousa YT, Sousa-Neto MD. Influence of ultrasound, with and without water spray cooling, on removal of posts cemented with resin or zinc phosphate cements. J Endod 2004;30:173– 6. 5. Gluskin AH, Ruddle CJ, Zinman EJ. Thermal injury through intraradicular heat transfer using ultrasonic devices: precautions and practical preventive strategies. J Am Dent Assoc 2005;136:1286 –93. 6. Hauman CHJ, Chandler NP, Purton DG. Factors influencing the removal of posts. Int Endod J 2003;36:687–90. 7. Ruddle CJ. Nonsurgical retreatment. J Endod 2004;30:827– 45. . 8. Ruddle CJ. Nonsurgical endodontic retreatment. J Calif Dent Assoc 1997;25: 769–86. 9. Satterthwaite JD, Stokes AN, Frankel NT. Potential for temperature change during application of ultrasonic vibration to intra radicular posts. Eur J Prosthodont Restor Dent 2003;11:51– 6. 10. Siver JE, Johnson WT (1992) Restoration of the Endodontically treated tooth. Dental Clinics of North America 36, 631-50.

142
Case 20 Endodontic re-treatment of endodontically treated maxillary left second molar with symptoms Patient
A 55 year-old white Norwegian male (Fig.1) was referred to the Department of Endodontics, University of Oslo by his dental undergraduate student for re-treatment of maxillary left second molar
Fig.1 Frontal view
. Medical history
Non-contributory. Dental History & Chief complaint
Endodontic treatment of the mandibular right second molar was done in the student clinic 23.02.01. Follow-up radiographs of the tooth revealed an increased radiolucent area at the apex. The patient complains of pain and he used analgesic 3-4 times a day Clinical Examination
Preoperative photos showed region from maxillary left second molar to maxillary second premolar (Fig.5)

143
Fig.5 Occlusal view
Maxillary left second molar: A crown type (metal, ceramic) restoration can be seen. The tooth was tender to percussion, and responded negative to sensibility test.
Maxillary left first molar: A crown restoration on it. The tooth responded positive to sensibility test with Endo Ice.
Maxillary left first second premolar: A pontic.
The other teeth in the upper and lower right quadrants showed no signs relevant to the chief complaint.
The gingival margin was healthy; except for buccal surface which was inflamed. The probing depths were within normal limits except the distal side there was a periodontal pocket of 9mm depth. Radiographic Examination
The preoperative radiograph showed region maxillary left second molar to first molar (Fig. 6).
Maxillary second molar: Had a metal ceramic radio-opaque restoration. Lamina dura can be followed around the root where it widens to a radiolucent area of approximately 5mm in the distal surfaces. A radio-opaque material was seen in the canal with an area in the apical part with incomplete obturation.
Maxillary first molar: Had a metal ceramic radio-opaque restoration. Lamina dura can be followed around the entire root.

144
Fig. 6 Apical radio-lucency of tooth 27
Diagnosis
Acute apical periodontitis of maxillary left second molar (K04.4). Treatment Plan
Re-treatment of an endodontically treated mandibular right second molar. Root canal disinfection and filling. Treatment 25.05.2005
Access cavity was prepared, two canals found filled with gutta-percha. Gutta-percha was removed with the help of ProTaper F3. Two extra canals were found with the help of microscope. Irrigation was done with 1% sodium hypochlorite and 17% EDTA. An nr.15 K-Flex was taken to working length. Control of working length with apex locator (ProPex), and verified with a working length radiograph (Fig.7, and 8).
Working length for each canal was:
MB 45/18 mm mbk MP 45/ 18mm mp.k DB 50/ 18mm mb.k P 60/ 17mm dp.k
The root canal was dried with sterile paper points. Calcium hydroxide intracanal
dressing was packed into the canal with the help of a lentulospiral and sterile paper points. Access cavity was sealed with IRM.

145
Fig.7 Working length Fig.8 Working length Treatment 14.06.2005
Patient returned to the clinic three weeks later with no symptoms from the tooth. The swallowing buccaly was diminished in size. No periodontal pocket could be examined. Rubber dam was applied, and the area was disinfected with chlorhexidine-ethanol solution. The calcium hydroxide was removed with NiTi hand instruments. Irrigation was done with 1% sodium hypochlorite, 15% EDTA. The root canal was dried with sterile paper points.
Master gutta-percha cones were tried in, and a master cones radiograph was taken
(Fig.9). The tooth was root-filled with AH Plus and gutta-percha with cold lateral condenser. The gutta-percha was removed approximately 2 mm down in the canal and sealed with an IRM plug. Access cavity was filled with IRM (Fig.10).
Fig.9 Masterpoint radiograph Fig.10 Final radiograph

146
Evaluation Four canals were found and cleaned. After treatment with calcium hydroxide for six
weeks, healing was already in progress.
22 months follow up The patient has bee contacted by phone for follow up examination, he had travelled to
Stockholm were he live there permanently. He contacted his private dentist where he gets 2 periapical radiographs and sends them to the Depatment of Endodontics. The patient had no symptoms and the radiographic photos showed no change in the apical part (Fig. 11, 12). There are many bone structure and overlapping in this area and that it could be difficult to decide the follow up diagnosis with out clinical examination.
Fig.11 Follow up radiograph Fig.12 Mesio-eccenric radiograph
Discussion A lesion involving both periodontal and pulpal tissues can be of primary endodontic,
primary periodontal or stem from separate origins (meaning that both the endodontic lesion and the marginal periodontal lesion have developed independently). The clinical considerations for each type of lesion was classified by Simon et al. (8), separating lesions involving both periodontal and pulpal tissues into the following groups:
I. Primary endodontic lesions with secondary periodontal involvement. II. Primary periodontal lesions with secondary endodontic involvement. III. True combined lesions.
As in any opportunistic infection, in both pulpal and periodontal disease it is quite
difficult to evaluate which microbiota actually cause the problem and which bacteria are found simply because the environment favours their selection. Exacerbations of periapical lesions appear to be linked to the presence of black-pigmented, Gram-negative anaerobic rods in the root canal system (4, 10, and 12).

147
The similarities between the endodontic and periodontal microflora suggest that cross-infection between the root canal and the periodontal pocket can occur. This idea is supported by the presence of anatomical pathways between the pulp and the periodontal ligament (5).
The major connections between periodontal and pulpal tissues are the apical foramina. In addition to these main avenues of communication, there are a multitude of branches connecting the main root canal system with the periodontal ligament. These root canal ramifications were first described some 100years ago (2,7), and have since been subdivided into furcated, collateral, lateral, secondary, accessory, intercanal and reticular canals (1), as well as furcation canals (11).
In addition to the apical foramina and accessory canals, there is a third possible route
for bacteria and their products, the dentinal tubules. Dentinal tubules are formed or, better, left out during tooth development by odontoblasts, which trail their processes as they grow centripetally while secreting the dentin matrix. The extent of these processes in the dentinal tubules of fully formed dentin is a matter of dispute; however, it is most likely that the odontoblastic process does not reach further than 0.5mm into the dentin (3).
If a tooth with an unusual periodontal breakdown does not have a root filling, the first
step for proper perio-endo diagnosis will be a vitality test. It is well-known that pulp tests cannot provide an accurate assessment of the histological status of the pulp. However, it has been shown that the probability of a nonsensitive reaction representing a necrotic pulp is 89% with the cold test and 88% with the electric pulp test (6).
It has been demonstrated that, after proper root canal treatment, fistulas originating from an endodontic lesion heal even if they have been present for a long time (9).
References 1. DeDeus, Q. D. (1975) Frequency, location, and direction of the lateral, secondary, and accessory canals. Journal of Endodontics 1, 361–366. 2. Fischer, G. (1907) Über die feinere Anatomie der Wurzelkanäle menschlicher Zähne. Vorläufige Mitteilung. Deutsche Monatsschrift für Zahnheilkunde 25, 544–552. 3. Garberoglio, R. & Brännström, M. (1976) Scanning electron microscopic investigation of human dentinal tubules. Archives of Oral Biology 21, 355–362. 4. Gomes, B. P. F. A., Drucker, D. B. & Lilley, J. D. (1994) Association of specific bacteria with some endodontic signs and symptoms. International Endodontic Journal 27, 291–298. 5. Kerekes, K. & Olsen, I. (1990) Similarities in the microfloras of root canals and deep periodontal pockets. Endodontics and Dental Traumatology 6, 1–5. 6. Petersson, K., Söderström, C., Kiani-Anaraki, M. & Le´vy, G. (1999) Evaluation of the ability of thermal and electrical tests to register pulp vitality. Endodontics and Dental Traumatology 15, 127–131.

148
7. Preiswerk, G. (1901). Die Pulpaamputation, eine klinische, pathohistologische und bakteriologische Studie. Österreichisch- Ungarische Vierteljahresschrift für Zahnheilkunde 17, 145–220. 8. Simon, J. H. S., Glick, D. H. & Frank, A. L. (1972). The relationship of endodonticperiodontic lesions. Journal of Periodontology 43, 202–208. 9. Strömberg, R., Hasselgren, G. & Bergstedt, H. (1972a) Endodontic treatment of traumatic root perforations in man. A clinical and roentgenological follow-up study. Swedish Dental Journal 65, 457–465. 10. Sundqvist, G., Johansson, E. & Sjögren, U. (1989) Prevalence of black-pigmented bacteroides species in root canal infections. Journal of Endodontics 15, 13–19. 11. Vertucci, F. J. & Williams, R. G. (1974) Furcation canals in the human mandibular first molar. Oral Surgery, Oral Medicine and Oral Pathology 38, 308–314. 12. Yoshida, M., Fukushima, H., Yamamoto, K., Ogawa, K., Toda, T. & Sagawa, H. (1987) Correlation between clinical symptoms and microorganisms isolated from root canals of teeth with periapical pathosis. Journal of Endodontics 13, 24–28.


















