Post-paroxysmal Tachycardia SyndromePost-paroxysmal Tachycardia Syndrome ROBERTJ. KERNOHAN From...
4
Brit. Heart J., 1969, 31, 803. Post-paroxysmal Tachycardia Syndrome ROBERT J. KERNOHAN From Waveney Hospital, Ballymena, Co. Antrim, N. Ireland Inversion of the T wave of the electrocardiogram may persist for a long time after an episode of paroxysmal tachycardia in the absence of detectable heart disease. Mattingly (1959) has stressed the existence of "spurious heart disease" as a result of erroneous diagnosis. This may lead to unnecessary restriction of physical activity and diet, expensive diagnostic procedures and therapy, and loss of time from work. The false diagnosis may result from misinterpretation of ST segment and T wave chan- ges in the electrocardiogram. ST segment and T wave changes may be caused by digitalis, quinidine, hyperventilation, drinking ice-water, electrolyte im- balance, and exercise. Likoff, Segal, and Dreifus (1962) reported 6 asymptomatic men, aged 16 to 24 years, with low intensity systolic murmurs but pro- nounced multiple T wave inversion suggestive of myocardial ischaemia in the presence of normal coronary arteriograms. Levine and White (1962) described prolonged QT interval and multiple T wave inversion in a patient with subarachnoid haemorrhage and without abnormal cardiac findings at necropsy. In the case reported here several episodes of supraventricular paroxysmal tachycardia were fol- lowed by prolonged T wave inversion without clinical or laboratory evidence of cardiac disease. Case Report A 21-year-old man was admitted on December 16, 1967, with an attack of rapid heart action. He had a history of four similar episodes during the previous four years. His most recent attack had started suddenly, with a tight sensation across the upper abdomen. He was not conscious of his heart's action and did not com- plain of dyspnoea. On admission he had a regular tachycardia of 170 a minute. The blood pressure was 120/70 mm. Hg and no cardiac murmurs were audible. The jugular venous pressure was not raised. The electrocardiogram (Fig. la) showed a regular ventricular rate of 170 a minute and P waves with a PR interval of 0-16 sec. The ven- tricular complexes had the configuration of complete right bundle-branch block. The findings were indica- tive of paroxysmal atrial tachycardia with aberration of ventricular conduction. The arrhythmia failed to revert with direct current countershock. He was treated with lanatoside C 0-25 mg. 6-hourly for 24 hours. The tachycardia persisted for 24 hours and then reverted to regular sinus rhythm at a rate of 54 a minute. After reversion to sinus rhythm the electrocardiogram (Fig. lb) showed con- spicuous T wave inversion in leads II, III, aVF, V3 to V6, and associated ST segment depression of 3 mm. The T wave inversion was maximal in lead V3 with an amplitude of 13 mm. There were no abnormal Q waves. The serum enzymes (serum aspartate aminotransferase and lactic acid dehydrogenase) were normal. Chest x-ray showed a normal cardiac silhouette. The serum cholesterol was 152 mg./100 ml. Gradual regression of the T wave abnormality occurred. Ten days later T wave inversion had diminished to 2 mm. in lead V4 and the ST segment was isoelectric (Fig. 2A). The electro- cardiogram was normal 19 days after admission (Fig. 2B). Episodes of paroxysmal tachycardia had been previ- ously recorded in May 1964, August 1966, January 1967, and May 1967. On each of these occasions the electro- cardiogram during the episode showed supraventricular tachycardia and ventricular complexes of right bundle- branch block configuration. Each attack of tachycardia was followed by T-wave inversion and ST segment depression in the same leads as in the episode of December 1967. The patient was investigated in the cardiovascular unit of the Belfast City Hospital 4 days after the episode in August 1966, when conspicuous T wave abnormality was present. Right heart catheterization and pulmonary angiography were performed. Pulmonary artery, right ventricular, and right atrial pressures were normal. The angiogram revealed no evidence of any anomalous coronary artery. There was no evidence of cardiomyo- pathy, coronary artery disease, or other cardiac abnor- mality. There has been no recurrence since his last episode in December, 1967, and he leads a normal active life. 03 on June 14, 2021 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.31.6.803 on 1 November 1969. Downloaded from
Transcript of Post-paroxysmal Tachycardia SyndromePost-paroxysmal Tachycardia Syndrome ROBERTJ. KERNOHAN From...
-
Brit. Heart J., 1969, 31, 803.
Post-paroxysmal Tachycardia SyndromeROBERT J. KERNOHAN
From Waveney Hospital, Ballymena, Co. Antrim, N. Ireland
Inversion of the T wave of the electrocardiogrammay persist for a long time after an episode ofparoxysmal tachycardia in the absence of detectableheart disease. Mattingly (1959) has stressed theexistence of "spurious heart disease" as a result oferroneous diagnosis. This may lead to unnecessaryrestriction of physical activity and diet, expensivediagnostic procedures and therapy, and loss of timefrom work. The false diagnosis may result frommisinterpretation of ST segment and T wave chan-ges in the electrocardiogram. ST segment and Twave changes may be caused by digitalis, quinidine,hyperventilation, drinking ice-water, electrolyte im-balance, and exercise. Likoff, Segal, and Dreifus(1962) reported 6 asymptomatic men, aged 16 to 24years, with low intensity systolic murmurs but pro-nounced multiple T wave inversion suggestive ofmyocardial ischaemia in the presence of normalcoronary arteriograms. Levine and White (1962)described prolonged QT interval and multiple Twave inversion in a patient with subarachnoidhaemorrhage and without abnormal cardiac findingsat necropsy.
In the case reported here several episodes ofsupraventricular paroxysmal tachycardia were fol-lowed by prolonged T wave inversion withoutclinical or laboratory evidence of cardiac disease.
Case ReportA 21-year-old man was admitted on December 16,
1967, with an attack of rapid heart action. He had ahistory of four similar episodes during the previous fouryears. His most recent attack had started suddenly,with a tight sensation across the upper abdomen. Hewas not conscious of his heart's action and did not com-plain of dyspnoea.On admission he had a regular tachycardia of 170 a
minute. The blood pressure was 120/70 mm. Hg andno cardiac murmurs were audible. The jugular venouspressure was not raised. The electrocardiogram (Fig.
la) showed a regular ventricular rate of 170 a minuteand P waves with a PR interval of 0-16 sec. The ven-tricular complexes had the configuration of completeright bundle-branch block. The findings were indica-tive of paroxysmal atrial tachycardia with aberration ofventricular conduction.The arrhythmia failed to revert with direct current
countershock. He was treated with lanatoside C 0-25mg. 6-hourly for 24 hours. The tachycardia persistedfor 24 hours and then reverted to regular sinus rhythmat a rate of 54 a minute. After reversion to sinusrhythm the electrocardiogram (Fig. lb) showed con-spicuous T wave inversion in leads II, III, aVF, V3 toV6, and associated ST segment depression of 3 mm.The T wave inversion was maximal in lead V3 with anamplitude of 13 mm. There were no abnormal Q waves.The serum enzymes (serum aspartate aminotransferaseand lactic acid dehydrogenase) were normal. Chestx-ray showed a normal cardiac silhouette. The serumcholesterol was 152 mg./100 ml. Gradual regression ofthe T wave abnormality occurred. Ten days later Twave inversion had diminished to 2 mm. in lead V4 andthe ST segment was isoelectric (Fig. 2A). The electro-cardiogram was normal 19 days after admission (Fig. 2B).
Episodes of paroxysmal tachycardia had been previ-ously recorded in May 1964, August 1966, January 1967,and May 1967. On each of these occasions the electro-cardiogram during the episode showed supraventriculartachycardia and ventricular complexes of right bundle-branch block configuration. Each attack of tachycardiawas followed by T-wave inversion and ST segmentdepression in the same leads as in the episode ofDecember 1967.The patient was investigated in the cardiovascular
unit of the Belfast City Hospital 4 days after the episodein August 1966, when conspicuous T wave abnormalitywas present. Right heart catheterization and pulmonaryangiography were performed. Pulmonary artery, rightventricular, and right atrial pressures were normal.The angiogram revealed no evidence of any anomalouscoronary artery. There was no evidence of cardiomyo-pathy, coronary artery disease, or other cardiac abnor-mality.There has been no recurrence since his last episode in
December, 1967, and he leads a normal active life.03
on June 14, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.31.6.803 on 1 N
ovember 1969. D
ownloaded from
http://heart.bmj.com/
-
Robert J. Kernohan
...A
VI
III
HIII
aVR t
aVL
GVF
I _
B
v1I
IIr V2
V3 X _4 h \'V-
I/~~~ UI
V4
V5
Vb
v
V4,oVR r '
AIf aVL - *\
V t aVF 4 _ VS i
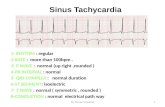
FIG. 1.-The electrocardiogram, (A) during the paroxysm of tachycardia, and (B) immediately afterreversion to sinus rhythm two days later.
CommentPersistence ofT wave inversion for days or weeks
after paroxysmal tachycardia may lead to an errone-ous diagnosis of myocardial infarction. The truediagnosis of post-tachycardia syndrome may beestablished by the absence of symptoms during theperiod of electrocardiographic abnormality, normalblood enzyme levels, absence of pathological Qwaves, multiple T wave inversions without circum-scribed anatomical localization, and recurrence ofthe T wave inversion in identical character and formeach time the patient has a paroxysm of tachycardia.
Graybiel and White (1935) stressed the need forcaution in the diagnosis of serious heart diseasewhen T wave inversion is the only abnormal find-ing. They also emphasized the importance of cor-
relation of electrocardiographic findings with thepatient's history and physical examination. In thisconnexion they cited two cases of paroxysmal ven-tricular tachycardia in young robust adults fol-lowed by T wave inversion in leads I, II, and IIIand with gradual return to a normal cardiogram;there was no sign of organic disease. Geiger (1943)later reported electrocardiograms simulating thoseof coronary thrombosis after cessation of paroxys-mal supraventricular tachycardia of 48 hours' dura-tion; electrocardiographic pattern was character-ized by prominent T wave inversion in leads I, II,and III which persisted for 35 days, depression ofST segments in the leads with inverted T waves,and absence of abnormal Q waves. Smith (1946)reported a further example of the cardiographic
804
I I
xi r,
on June 14, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.31.6.803 on 1 N
ovember 1969. D
ownloaded from
http://heart.bmj.com/
-
Post-paroxysmal Tachycardia Syndrome
A
II
iIIIJ-
aVR
IL
V4 J
V5
oVF
V6
I1I
III
II!~~V
__j>\_ v2
c'VR 0.V4 :
V51
oVF 4 L.i
v....-..
FIG. 2.-The electrocardiogram, (A) 10 days after, and (B) 17 days after tachycardia had ceased.
syndrome occurring after ventricular tachycardia,characterized by broad-base T wave inversion inone or more leads, with depression of ST segmentin the leads with the most prominent T wave inver-sion. He believed this to be the nineteenth casereported and noted that only two cases of electro-cardiographic abnormality occurring after supra-ventricular tachycardia had been described. Fur-ther cases of prolonged benign T wave inversionafter paroxysmal ventricular tachycardia weredescribed by Rakov in 1964, and after supraventricu-lar tachycardia by Sargin and Demirkol in 1965.The mechanism of production of the post-tachy-
cardia syndrome is obscure. It is important, how-ever, in order to avoid an erroneous diagnosis ofcoronary thrombosis, to recognize that the electro-cardiographic changes which may follow an episode
of paroxysmal tachycardia may be benign. It isnot known how frequently this syndrome followsparoxysmal atrial tachycardia. Though paroxys-mal atrial tachycardia is much more common thanparoxysmal ventricular tachycardia, most reportedcases of post-tachycardia syndrome have occurredafter paroxysmal ventricular tachycardia.
SummaryA case of recurrent supraventricular paroxysmal
tachycardia in a 21-year-old man is described.Prolonged, deeply inverted T waves occurred aftereach paroxysm, with spontaneous reversion to anormal electrocardiogram. There was no evidenceof organic heart disease.
Misinterpretation of the electrocardiogram after
805
vi
on June 14, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.31.6.803 on 1 N
ovember 1969. D
ownloaded from
http://heart.bmj.com/
-
Robert J. Kernohan
paroxysmal tachycardia may lead to spurious heartdisease and unnecessary invalidism.
I am grateful to Dr. Evan Fletcher in whose Unit inthe Belfast City Hospital the haemodynamic studieswere performed.
ReferencesGeiger, A. J. (1943). Electrocardiograms simulating those of
coronary thrombosis after cessation ofparoxysmal tachy-cardia. Amer. HeartJ., 26, 555.
Graybiel, A., and White, P. D. (1935). Inversion of the T-wave in Lead I or II of the electrocardiogram in youngindividuals with neurocirculatory asthenia, with thyro-toxicosis, in relation to certain infections, and followingparoxysmal ventricular tachycardia. Amer. Heart J.,10, 345.
Levine, H. J., and White, N. W. (1962). Unusual ECGpatterns in rupture of vertebral artery aneurysm. Arch.intern. Med., 110, 523.
Likoff, W., Segal, B., and Dreifus, L. (1962). Myocardialinfarction patterns in young subjects with normal coron-ary arteriograms. Circulation, 26, 373.
Mattingly, T. W. (1959). Spurious heart disease. A prob-lem in the management of coronary disease. Arch.intern. Med., 104, 914.
Rakov, H. L. (1964). Prolonged benign T-wave inversionfollowing paroxysmal ventricular tachycardia. N. Y.St. J. Med., 64, 2100.
Sargin, O., and Demirkol, C. (1965). Deeply inverted T-waves after supraventricular paroxysmal tachycardia.Dis. Chest, 48, 321.
Smith, L. B. (1946). Paroxysmal ventricular tachycardiafollowed by electrocardiographic syndrome, with areport of a case. Amer. Heart J., 32, 257.
806
on June 14, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.31.6.803 on 1 N
ovember 1969. D
ownloaded from
http://heart.bmj.com/