Post Cs Na Revised Na Toh

of 31
-
Upload
minerva-cortal -
Category
Documents
-
view
226 -
download
0
Transcript of Post Cs Na Revised Na Toh
-
8/6/2019 Post Cs Na Revised Na Toh
1/30
1 | P a g e
Arellano University
College Of Nursing
Legarda, Manila
CASE STUDY
POST CESAREAN SECTION
SUBMITTED BY:
BSN III-12
GROUP 48
LIMUCO, JANNA ZENNA
MANTALA, MICHELLE
MARTINEZ, MARK KEVIN
MARZO, AYESHA CLAIRE
MURILLO, ROSE ANN
NAPULE, CHARLOTTE
NUGUID, GLACIE LYNNE
REAGO, JESTORI
REMOLLO, KEVIN
VILLARANTE, JHUNNAR
-
8/6/2019 Post Cs Na Revised Na Toh
2/30
2 | P a g e
I. INTRODUCTIONCesarean birth, birth accomplished through an abdominal incision into the uterus, is one
of the oldest typed of surgical procedure known. Unfortunately, it is a procedure always more
hazardous than vaginal birth. Fortunately, when compared with other surgical procedures, it
is one of the safest types of surgeries and one with few complications.
The word cesarean is derived from the Latin caedore which means to cut. At one
time, there was a popular belief that Julius Caesar was delivered by a cesarean birth and that
procedure was named for him. However, because Caesar was born before antibiotics and
sterile surgical techniques, it seems likely that his mother would have survived the said
procedure. Currently, cesarean birth is used most often prophylactic measures, to alleviate
problems of birth for conditions such as cephalopelvic disproportion, cervical cerclage,
placenta previa, umbilical cord prolapsed, fetal distress, transverse fetal lie, etc. It is
generally contraindicated when there is a documented dead fetus.
You might need to have a planned cesarean delivery if a patient condition is in
Cephalopelvic disproportion (CPD), Previous cesarean birth, Multiple pregnancy, Placenta
previa, Transverse lie, or Breech presentation. In a Cephalopelvic disproportion (CPD), thebabys head or body is too large to pass safely through the mothers pelvis, or the mothers
pelvis is too small to deliver a normal-sized baby. In Previous cesarean birth,although it is
possible to have a vaginal birth after a previous cesarean, it is not an option for all women.
Factors that can affect whether a cesarean is needed include the type of uterine incision used
in the previous cesarean and the risk of rupturing the uterus with a vaginal birth. In Multiple
pregnancy, although twins can often be delivered vaginally, two or more babies might
require a cesarean delivery. In Placenta previa, a cesarean delivery is done if the placenta is
attached too low in the uterine wall and blocks the babys exit through the cervix. A mother
also underwent a cesarean delivery if the baby is in a Transverse Lie presentation because
the baby is in a horizontal or sideways position in the uterus. In this condition, a cesarean
delivery is always used. And for Breech presentation or Breech birth, the baby is
-
8/6/2019 Post Cs Na Revised Na Toh
3/30
3 | P a g e
positioned to deliver feet or bottom first. If your doctor determines that the baby cant be
turned through abdominal manipulation, you will need to have a cesarean delivery.
The term cesarean birth rather than cesarean delivery is generally used to accentuate that
this is a birth more than surgical procedure. A major concern in maternal and child health
nursing is the increasing number of cesarean births being performed annually.
In South East Asian countries, Overall 27% of women had a caesarean section, with rates
varying from 19% to 35% between countries and 12% to 39% between hospitals within
countries. The most common indications for caesarean were previous caesarean (7.0%),
cephalopelvic disproportion (6.3%), malpresentation (4.7%) and fetal distress (3.3%).
Neonatal resuscitation rates ranged from 7% to 60% between countries. Prophylactic
antibiotics were almost universally given but variations in timing occurred between countries
and between hospitals within countries.
There are two types of Cesarean Birth: scheduled and emergency. In the first instance,
there is time for thorough preparation, some women may have even taken a child preparation
class specifically for cesarean birth. Scheduling cesarean birth this freely also resulted in
preterm births. A physical indication for cesarean birth such as transverse presentation,
genital herpes, cephalopelvic disproportion, or avoidance of post-procedure stress
incontinence, must be documented before a cesarean procedure can be performed. Cesarean
birth reduces the transfer of HIV from mother to newborn (Read et al. 2001). With new
surgical techniques, particularly a low cervical incision, once a cesarean, always a cesarean
no longer applies. Most of women who have had cesarean birth, after 10 years are eligible to
give birth vaginally in subsequent pregnancies if the circumstances are otherwise are
appropriate for vaginal birth. About 60% of woman todat have vaginal birth after a cesarean
birth (VBAC). VBACs are the most successful if there is an interval greater than 19 months
between the cesarean and the VBAC (Huonget Al., 2002). Emergency cesarean births are
done for reasons such as placenta previa, abruption placentae, fetal distress or failure to
progress in labor. An emergency cesarean birth carries with it the risk of all emergency
surgery: a woman may not be a prime candidate for anesthesia and who is psychologically
-
8/6/2019 Post Cs Na Revised Na Toh
4/30
4 | P a g e
unprepared for the experience. In addition, the woman may have a fluid electrolyte
imbalance and be both physically and emotionally exhausted form a long labor.
II. OBJECTIVES
General objective:
We, BSN 3 Group 48 of Arellano University College of Nursing aims to develop our
skills in performing assessment procedures and the necessary intervention for quality client care
of patient with post cesarean client, to enhance our knowledge in understanding the procedure
and identify specific treatment and last and foremost is for us to be able to give knowledge about
cesarean.
Specific objectives:
At the end of the presentation our group will be able:
y To describe indications of cesarean birth.y Formulate diagnosis related to Cesarean birth.y Establish outcomes that meet the needs of woman requiring cesarean birth.y Plan appropriate nursing care to ensure family centered care.y Evaluate outcomes for achievement and effectiveness of nursing care.
III.THEORETICAL FOUNDATION
D o r o t h e a O r e m ' s S e l f - C a r e T h e o r y
This theory composed of three related theories including self care, self care agency, and
therapeutic self care demand. In Self care theory, an individualinitiate and perform his/her own
activities to maintain life, health and well being. In Self care agency, a multidimensional
concept in nursing theory includes motivation, decision-making, energy, and knowledge
necessary to perform self-care actions. In Therapeutic self care demand, "totality of self care
-
8/6/2019 Post Cs Na Revised Na Toh
5/30
5 | P a g e
actions to be performed for some duration in order to meet self care requisites by using valid
methods and related sets of operations and actions".
A Self care requisite is anaction directed towards provision of self care. There are 3 categories
of self care requisites are: 1) The Universal, which includes developmental and health deviation;
2) the Universal self-care requisites associates with life processes and the maintenance of the
integrity of human structure and functioning and activity of daily living (ADL). These requisites
identify maintenance of sufficient intake of air, water, and food. Also provision of care
associated with elimination process, balances between activity and rest between solitude and
social interaction, prevention of hazards to human life well-being and promotion of human
functioning and lastly; 3) the Developmental self care requisites associates with developmental
processes/derives from a condition or associates with an event and this also includes healthdeviation self-care that requires condition of illness, or disease. It also seeks and secures
appropriate medical assistance, being aware of and attending to the effects and results of
pathologic conditions, effectively carrying out medically prescribed measures, modifies self
concept in accepting oneself as being in a particular state of health and in specific forms of
health care and learning to live with effects of pathologic conditions.
Dorothea Orems theory encompasses that patient is requiring nursing care. It is needed if there
is a problem that prevents a person from reaching their optimal health. Restoring, promoting and
maintaining health are the goals of Dorothea Orems Self-care Model, these include the interventions
and teachings design to return a person to or sustain a level of optimal health and well being, It is when
an adult is incapable or limited in the provision of continuous effective self-care. In this case, the
patient has ineffective health continuance because of the procedure she had undergone and due to
the incision she had have the nurses role in helping the client to achieve or maintain a level of
optimal health and wellness to act as an advocate, redirector, support person and teach and to
provide an environment conducive to therapeutic ddevelpoment.
-
8/6/2019 Post Cs Na Revised Na Toh
6/30
6 | P a g e
IV. NURSING HISTORY
A. Biographical Data
Patient Name: A. M.
Address: Delpan ST., Barangay Kasilawan, Makati City
Date of Birth: April 13, 1981
Place of Birth: Pangasinan City
Age: 25 years old
Nationality: Filipino
Educational Attainment: BS Electrical and Communications Engineering
Religion: Roman Catholic
Data of Admission: August 24, 2006
Mode of arrival: Ambulatory
B. Chief Complaint
Noong pag-ihi ko may sumabay na dugo as verbalized by the patient.
C. History of present Illness
Two days prior to admission, patient experienced bloody vaginal discharge upon
urinating. The bloody vaginal discharge she noted prompted her to go to the hospital and
subsequently admitted. (delte breast changes. Eklabu)
-
8/6/2019 Post Cs Na Revised Na Toh
7/30
7 | P a g e
Pain experienced:
Location is in right and lower left quadrant of abdomen specifically on the incision site.
Radiation localized pain. Quality is recurrent and throbbing pain. Aggravating Factor is during
activity. Alleviating factor was medications. Time usually lasts for 1-2 hours
D. History of Past Illness
On the 1st
trimester of her pregnancy, she experienced discomforts like breast changes,
urinary frequency, fatigue, nausea and vomiting. Urinary frequency accompanied by leg cramps
was also experienced in the 2nd
and 3rd
trimester. The patient had her Urinary tract Infection
when she was in her 7th
month of pregnancy and her Physician prescribed her a Cefalexin as
treatment for the said illness. And She have had undergone a procedure of dilatation and
curettage due to her miscarriage. And had no allergies to any food and medications.
E. Family Health History
Patients father was noted to be hypertensive.
F. Social History
Work Environment: She works at MDS, a web design company located at The Fort Strip.
Home Environment: Resides in 2 bedrooms, 1 bathroom concrete house.
Education: A degree holder of Bachelor of Science in Electrical and Communications
Engineering.
Role Relationship: Wife and daughter.
Childhood Immunization: Patient had completed childhood immunization.
G. Obstetrical History
Menarche: 14 years old.
Monthly cycle duration: 3-5 days, 2-3 pads moderately soaked.
-
8/6/2019 Post Cs Na Revised Na Toh
8/30
8 | P a g e
Last Menstrual Period: November 19, 2005
Age of Gestation: 40 weeks and 2 days (via LMP)
: 38 weeks and 4 days (via pelvic ultrasound)
Expected Date of Confinement: September 2, 2006
OB Score: G2 P1 (T1 P0 A1 L1 M0)
-
8/6/2019 Post Cs Na Revised Na Toh
9/30
9 | P a g e
V. ANATOMY AND PHYSIOLOGY
-
8/6/2019 Post Cs Na Revised Na Toh
10/30
10 | P a g e
ANATOMY
The pelvic girdle is the place where the lower limbs attach to the body. The right and left
coxae, or hip bones, join each other anteriorly and the sacrum posteriorly, to form a ring of bone
called the pelvic girdle and the coccyx. The sacrum and the coccyx form part of the pelvis but
are also part of the axial skeleton. Each coxa formed by the three bones fused to one another to
form a single bone. The ilium is the most superior, the ischium is the inferior and the pubis is the
anterior and inferior. An iliac crest can be seen alongthe superior margin of each ilium and an
anterior iliac spine, an important hip landmark, is located at the anterior end of the iliac crest.
The coxae join each other anteriorly at the pubic symphysis and join the sacrum posteriorly at the
sacro ilac joints. The acetabulum is the socket of the hip joint. The obturator foramen is the large
hole in each coxa that is closed off by muscles and other structures.
-
8/6/2019 Post Cs Na Revised Na Toh
11/30
11 | P a g e
PHYSIOLOGY
The organs of the reproductive systems are concerned with the general process of
reproduction, and each is adapted for specialized tasks. These organs are unique in that their
functions are not necessary for the survival of each individual. Instead, their functions are vital to
the continuation of the human species. In providing maternity gynecologic health care to women,
you will find that it is vital to your career as a practical nurse and to the patient that you will
require a greater depth and breadth of knowledge of the female anatomy and physiology than
usual. The female reproductive system consists of internal organs and external organs. The
internal organs are located in the pelvic cavity and are supported by the pelvic floor. The external
organs are located from the lower margin of the pubis to the perineum. The appearance of the
external genitals varies greatly from woman to woman, since age, heredity, race, and the number
of children a woman has borne determines the size, shape, and color.
-
8/6/2019 Post Cs Na Revised Na Toh
12/30
12 | P a g e
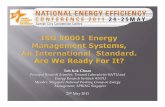
VI. PATHOPHYSIOLOGY
Launch Internet Explorer Browser.lnk
Predisposing Factors:
y Occupationy History of Abortiony UTI during her 7th month of pregnancy
Physiologic Factors:
y Presumptive signs: breasts changes,urinary frequency, fatigue, nausea and
vomiting on the 1st
trimester and leg
cramps on her 2nd
and 3rd
trimester.
y LMP: November 19 , 2005 and her EDC:September 2, 2006
y Pelvic Ultrasound
TRUE LABOR
During Transition Phase the
presenting part was at
station -1
(+) bloody vaginal discharge
Arrest in Cervical
Dilatation
The Presenting part was still
above the ischial spine and
has not crowned yet
Immediate Low Transverse
Cesarean Section
Low Segment Incision on
the Abdomen
Expulsion of Fetus
Expulsion of Placenta accompanied
by blood loss of800 cc
Acute Pain r/t surgical incision
(PS: 5/10)
Activity Intolerance as
manifested by Weakness and
discomfort
Swelling or discharges on the
surgical incision site
-
8/6/2019 Post Cs Na Revised Na Toh
13/30
13 | P a g e
VII. GORDONS FUNCTIONAL PATTERN
BEFOREHOSPITALIZATION
DURINGHOSPITALIZATION
ANALYSIS
HEALTHPERCEPTION/HE
ALTHMANAGEMENT
PATTERN
-The patient had completeimmunizations and had
undergone laboratory anddiagnostic procedures of
ultrasound and urinalysis. Sheregularly intakes
multivitamins and Iron (caltrate and honorate). And
throughout the preganancy,she had completed the pre-
natal check up.
-parang hindi ko kaya nahindi ako kakain ng ganon
katagal, paano akolalakas? As verbalized by
the patient..
Konek?
-The patient was anxious
about her condition and howwill she able to recover easily
if shes under NPO.
- Early and consistentprenatal care is essential to
the health and health of herbaby.
(maternal &child healthnursing vol.1,p595)
NUTRITIONAL-METABOLIC
PATTERN
-The patient eats usual foodssuch as sinigang and adobo
and she has ability inswallowing and chewing
foods and feeds herself. Shestaking regular meals.
-The patient was underNPO and being given by
an IVF of D5LR 1L to runfor 8 hours at 32 gtts/ min
as ordered. And she lossblood about 800 cc on the
operation.
-There is a change in the dietmodification of the patient
because the patient is a postCS she must be in NPO since
her peristalsis movement isnot yet returning to normal.
Theres a risk in deficientfluid volume.
-a pregnant woman shouldeat a sufficient diet to allow
for the growth of fetus andalso provide for the need of
her on growing baby.(maternal and child nursing
vol.1,p657)-most women have a IVF line
before the surgery with afluid .it helps to ensure that a
woman is fully hydrated.(maternal &child health
nursing vol.1,p657)
-The patient had a regular
bowel movement. Her lastmenstrual period was last
-The patient was
catheterized her urine isbloody in color and has an
-There is a change in the
urine pattern because thepatient had been catheterized
-
8/6/2019 Post Cs Na Revised Na Toh
14/30
14 | P a g e
ELIMINATIONPATTERN
November 19, 2005. Duration
of her menstrual period was3- 5 days, 2-3 pads,
moderately soaked.Transfer the mens eke k sa
sexual ekek.
-Nung pag-ihi ko maysumabay na dugo as
verbalized by the patient.
output of 400cc per/hr.
The patient undergonewater glycerine enema
prior to the procedure.
-di ko naman masyadong
nararamdaman nalumalabas yoong ihi ko
pero nakikita ko maylaman naman yoong bag
as verbalized by thepatient.
and the patients elimination
was also changed becausewater glycerine enema was
administered to the client dueto her condition.
-before the hospitalization
patient had a normalelimination pattern, can void
freely but when she gothospitalized her sensation of
voiding become altered.
Not approrioate. Sensation
eklabu.
ACTIVITY-EXERCISE
PATTERN
-The patient is able to feed,bathe and groom herself. She
has sufficient energy fordesired and/or required
activity. She is in full range ofmotion. And practices active
exercises.
Delete feeding churva.
-The patient was not ableto do things independently
and became dependent.She had a difficult time
moving around the bed tochange position due to the
pain
- the patient uses her fullrange of motion and have
active exercise before shehospitalized and become
altered when she got into thehospital because of pain and
weakness due to theprocedure.
-People often define theirhealth and physical fitness by
their activity because mentalwell-being and the
effectiveness of bodyfunction depend largely on
their mobility status.(fundamentals of nursing
vol.2, p1106)
SLEEP AND
REST PATTERN
-She had a normal sleep and
rest pattern.
Not applicable yung normal
-She experienced
difficulty in sleeping asshe experienced pain.
-Due to the procedure that
the client had undergone, shewas having difficulty, since
she cannot move freely andthe presence of incision in
her abdomen and the pain init, made her difficult to sleep.
-
8/6/2019 Post Cs Na Revised Na Toh
15/30
15 | P a g e
COGNITIVEPERCEPTUAL
PATTERN
-Before the hospitalization,the patient experienced
discomforts like breastchanges, urinary frequency
nausea and vomiting. Andurinary frequency
accompanied by leg crampson the 2nd and 3rd trimester of
pregnancy.
Not applicable.what was the
perceptiot the s/sn abou
- Patient was then askedhow she felt after the
operation and sheverbalized
nararamdaman ko yoongsakit ng tahi and kung i-
rarate ko yoong sakit mga5/10. She also added
medyo nauuhaw ako naparang natutuyo
lalamunan ko siguro dahilsa pagod tsaka sa tagal ng
operasyon and paranghindi ko kaya na hindi ako
kakain ng ganoon katagal,
paano ako lalakas?
-The patients cognitiveperceptual pattern changed
due to the patients conditionand maybe due to knowledge
deficit.
-According to Piaget stage ofCognitive development-
formal operational- theperson can solve hypothetical
problems with scientificreasoning understand s
causality and can deal withthe past present and future.
(maternal &child health
nursing vol.2,p801)
SELF
PERCEPTIONPATTERN-SELF
CONCEPTPATTERN
-The patient believes that herneeds for intimacy and
affection are being met. Shefeels good most of the time.
-The patient is concernwith her current health
condition and how shewill be getting well and
her present health goal isto eat to be able to get
well.
-
-Herself perception is mainlyfocused on her health
condition.
ROLE
RELATIONSHIP
-She is living with herhusband and a family oriented
person. She isnt a member ofany organization.
-Patient AM had moderate
self esteem with closerelationship with the member
of her family.
-She was a mom now, andtrying to adjust on things
like taking care of hernewborn, etc.
--throughout life peopleunder go numerous role
changes.(fundamentals of nursing
vol.2,p1006)
SEXUALITY-REPRODUCTIVE
-Her first menstrual periodwas when she was 14 yearsold and her Last Menstrual
Period was last November 19,2005. And have had
undergone D&C due tomiscarriage on her first
pregnancy.
-She had delivered a livefull term baby girl. - according to Freud stages ofpsychosexual a persondevelops sexual maturity and
learns to establishsatisfactory relationship with
the opposite sex.(maternal &child health
nursing vol.2,p803)
-
8/6/2019 Post Cs Na Revised Na Toh
16/30
16 | P a g e
- She was married to hishusband on March 2005.
-She got pregnant to her first
baby but unluckilyexperienced miscarriage due
to week fetal heart tone.
-Later on she had an OBhistory of gravida 2, parity 1,
and abortion 1.
-And lastly became pregnantto a 40 weeks and 2/7 days
baby girl.
STRESS
TOLERANCEPATTERN
-She is coping well in every
problems encountered withthe help of her husband and
faith to God.
-She is stressed and has
worries and fears.
-She became stressful
because of her condition.
VALUE BELIEF
PATTERN
-She is a Roman Catholic and
goes to church regularly, it iswhere she gets her courage in
every circumstances thatcomes along her way.
??????? - religion may be considered
a system of belief, practicesand ethical values about
divine or superhuman poweror power of worshipped as
the creators and rulers of theuniverse.
(fundamentals of nursingvol.1,p315)
Relate before and during.
-
8/6/2019 Post Cs Na Revised Na Toh
17/30
17 | P a g e
VIII. PHYSICAL ASSESSMENT
General Survey: The patient is conscious and coherent upon examination, weighs for 64kg and
stands 53. The client dont have body odor nor breath odor. The client is relaxed every time we
speak to her.
Vital Signs:
BP: 130/80 mmHg
PR: 92 bpm
RR: 20 cpm
TEMP: 37.6
y P (Precipitating Factor) Aggravated by activityy Q(Quality) Localized, recurrent and throbbing qualityy R(Radiating) Right and Lower left quadrant of the abdomen specifically
on the site of incision
y S (Severity) 5/10y T (Time or Onset) Onset of pain is gradual, usually lasts for 1-2 hours
BODY
PART
FINDINGS ANALYSIS NURSING ALERT
Head Normocephalic withsmooth, black and
evenly distributed hairand small traces of
dandruff on the scalp
Normal no signs ofasymmetry and deformities.
????
Face Symmetrical eyebrows,eyelids, eyelashes,pupils and eyeballs are
normally aligned
No deviations likeincreased facial hair, moonface.
Eyes Smooth clear cornea
and lens, (+) reflexes,whitish sclera, pinkish
conjunctivae, intact and
No signs of trauma or
abration that results toopaque appearance of the
eye. Positive reflexes
-
8/6/2019 Post Cs Na Revised Na Toh
18/30
18 | P a g e
normal lacrimal
apparatus.
means no neurological
impairment of the cranialnerves.
Ears Symmetrical,(-)
discharges and waxytexture and normal
hearing acuity
Normal, no signs of
congenital abnormality likelow set ears (Trisomy 21)
Nose Normally deviated with
patent nostril, nontender sinuses, pinkish
turbinates, moist andpinkish nasal mucosa
with (-) discharge
Pt. is not experiencing
DOB, nasal flaring and noabnormal discharge.
(-) lesions like polypsNasal septum intact at the
middle.
Mouth Lips were slightly dry
and pink in color,
symmetrical and withno lesions.Slightly yellowish
complete set of teethpinkish gums and
buccal mucosa, tonsilswith midline tongue
and uvula
No signs of cyanosis, no
mucosal cysts or tumor.
Slightly yellowish teethindicates the pt. have notperforming good oral
hygiene the past days afterthe surgery
Lung Symmetrical lung
expansion and resonantrespiratory sounds
Indicates healthy lung and
normal lung sounds
Heart Apical Heart soundheard at the 5th
intercostals space, leftmid clavicular line with
(-) murmur
Apical sound is normallyheard on that part because
the apex of the heart isnormally located there nad
absence of murmursindicates the pt. has no
heart problem
Abdomen Presence of linea nigra
and striae gravidarum.Low segment Incision
due to CS delivery with
extreme swelling and ordischarge.
Umbilicus is stretched
during pregnancy to suchextent that by the 28
thweek.
Extrapigmentation
generally appears on theabdominal wall. A narrowbrown like linea nigra may
form running from theumbilicus to the symphisis
pubis.Reference: Maternal and
Childs Health 6th edition
-
8/6/2019 Post Cs Na Revised Na Toh
19/30
19 | P a g e
vol. 1 Adele Pilliteri page
234Lower segment incision is
one made horizontallyacross the abdomen just
over the symphysis pubisand also horizontally across
the uterus just over thecervix
Reference: Maternal andChilds Health 6
thedition
vol. 1 Adele Pilliteri page661
Skin Smooth, warm and withgood turgor
No signs of pallor,cyanosis, jaundice and
erythema. Warm skin may
indicate risk for infectiondue to surgical incision.
Nails Nail beds pink, intact
with soft texture 1-2sec. of capillary refill.
No signs of infection or
injuries on the nailsandpoor circulating problem.
-
8/6/2019 Post Cs Na Revised Na Toh
20/30
20 | P a g e
IX. Laboratory Examination
Examination Results
Pelvic Examination
Impression: Single live intrauterine pregnancy
in cephalic presentation of about 38 weeks and4/7 days age of gestation based on biparietaldiameter, fetal lie and abdominal
circumference with normal placentallocalization and amniotic fluid volume.
Sonographic fetal weight is appropriate forgestational age.
X. Medical/Surgical Management
I. Management:
A. Transfer to postpartum ward when stableB. Vital Signs q15 minutes for 1 hour, then q4 hoursC. Monitor intakes and outputs every 4 hours for 24 hoursD. Activity:
1. Bed rest2. Supine for 8 hours after spinal anesthetic3. Incentive Spirometry every 1 hour while awake
E. Standard Diet1.
Nothing by mouth for 8 hours after cesarean section
2. Sips of water after 8 hour window3. Advance to clear liquids as tolerated4. Advance to Regular diet when flatus or Bowel Movement
-
8/6/2019 Post Cs Na Revised Na Toh
21/30
21 | P a g e
F. Early Solid Diet Protocol1. Solid food within 8 hours of C-Section2. Well tolerated3. Resulted in faster bowel function return4. Shortened hospital stay by 24 hours5. Patolia (2001) Obstet Gynecol 98:113-6
G. Intravenous fluids1. D5LR OR D51/2NS at 125 cc/hour2.
Foley to gravity
3. Urine outputa. Foley Catheter in place:
-
8/6/2019 Post Cs Na Revised Na Toh
22/30
Name of Drug Mechanism of
Action
Indication Contraindicatio
n
Adverse Reactio
Generic Name:
CefuroximeSodium
Brand Name:Zegen
Drug
Classification:Anti- Effectives
Second
generationcephalosporins
that inhibits cellwall synthesis,
promotingosmotic
instability,usually
bacteracidal
Skin structuringinfections cause by
streptococcuspneumonia and
S.pyogenes,haemophilus
influenzastaphylococcus
aureus, E.coli.
Use cautiously inpatients
hypersensitive topenicillin
because ofpossibility of
cross sensitivitywith other beta
lactamantibiotics.
CV:phlebitis,
thrombophlebitis
GI: pseudo membranoscolitis, nausea, anorexi
vomiting, diarrhea
HEMA: Transient neuteosinophilia, hemolitic
anemia andthrombocytopenia
SKIN: Maculopapular erythematous rashes,
urticaria, pain,in duratisterile abcesses, temp.
elevation, sloughing IMinjection site
OTHER:
Hypersensitivity reactioserum sickness, anaphy
-
8/6/2019 Post Cs Na Revised Na Toh
23/30
Name of
Drug
Dosage Indication Contraindication Adverse React
Demerol Injection-10mg/ml,
12mg/ml,
100mg/ml
Syrup-
50mg/ml
Tablets-
500mg, 100mg
moderate tosevere pain
preoperativeanalgesia
adjunct toanesthesia
obstetricanalgesia
contraindicated topatients
hypersensitive to
the drug and in
those who have
received MAO
inhibitors within
the past 14 days.
Avoid use inpatients with end
stage renal
disease.
CNS: physicaldependence, se
CV: hypotensio
bradycardia
GI: constipatio
mouth, nausea
GU: urine reten
-
8/6/2019 Post Cs Na Revised Na Toh
24/30
ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE
Subjective:
Nararamdaman
ko yoong sakit ng tahi
ko as verbalized by
the patient.
Objective:
y Pain scale of5/10
y Difficulty inmovingwithout
assistance
y Surgicalincision
y FacialGrimace
Acute pain related
to surgical incision
secondary to
cesarean section as
manifested by pain
scale of5/10 and
difficulty moving
without assistance
Inference: Since the
patient had
undergone delivery
via low transverse
caesarean section,she has incision on
the lower quadrant
of her abdomen
which causes pain.
Short Term:
-After 30 minutes to
1 hour ofnursing
intervention the
patients pain scale
of5/10 will decrease
to 2/10.
Long Term:
-After 2 days of
nursing intervention,
the patient will be
able to move freely
with less discomfortand without
assistance.
INDEPENDENT:
y Providecomfort
measures such
as
repositioning
to supine
position, use of
heat packs,
quiet
environment,
and calm
activities.
y Instruct orencourage use
of relaxation
techniques
such as focused
breathing,
listening to
music and
socialization.
yIn
struct theclient on how
to do deep
breathing
exercise
y Teach the
y To avdirect
press
the in
site a
prom
pharm
c pain
mana
y To disatten
reduc
tensio
y It willthe pa
-
8/6/2019 Post Cs Na Revised Na Toh
25/30
patient on how
to do coughing
exercise and
instruct the
client not to lift
heavy objects
or do straneous
activities. n/a
y Encouragedadequate rest
periods.
y Check for foulsmelling
discharge and
swelling on the
site
y Evaluates clientresponse to
analgesics and
assists altering
drug regimen
based on
patients
needs.
DEPENDENT:
y Administeranalgesics
(Mefenamic
y To avaccide
remo
the su
and b
on
th
y To prefatigu
y To heearly
detec
infect
other
comp
y To maaccep
level
y Increaand
decredosag
in self
mana
of pai
-
8/6/2019 Post Cs Na Revised Na Toh
26/30
References sa ifernce at rationale.
acid), as
needed.
Collaborative:
y Providephysicaltherapy/
exercise
program based
on clients
ability.
N/A
-use of abdominal
binder
y Promactiveand e
sense
contr
-
8/6/2019 Post Cs Na Revised Na Toh
27/30
-
8/6/2019 Post Cs Na Revised Na Toh
28/30
28 | P a g e
DISCHARGE PLAN
MEDICATION:
Take home medication as prescribed by the physicians.E- Exercise
Encouraged early ambulation (walking )T Treatment
Explain to the patient how she will take care of her situation toward the treatmentshe had undergone.
H- Health Teaching
Informed patient to avoid lifting heavy objects for one to two weeks. Stressed the importance of perineal cleanliness. Instructed patient to increase intake of protein-rich foods to promote faster wound
healing.
Instructed to promote adequate fluid intake. Discouraged patient to participate in strenuous activities that might precipitate
stress and trauma to the wound.
Instructed patient to promote wound healing/ breast feeding Contact physician for
Temperature > 100.4 Systolic Blood Pressure 140 mmHg Diastolic Blood Pressure >90 mmHg or 130 or 32 or
-
8/6/2019 Post Cs Na Revised Na Toh
29/30
29 | P a g e
O- OPD follow-up
Informed patient to have a follow-up check up. Instructed the patient to report to physician any signs of infection.
D- Diet
Encouraged client to increase intake of fiber to avoid constipation. Instructed to increase fluid intake. Instructed to increase intake of nutritious food such as fruits and vegetables.
S- Sex
3-4 weeks or if the client dont feel pain nor discomforts.
BUBBLES
B- Breast Encourage the client to breastfeed 15 mins. Each breast. Instruct the client to check her nipples or signs of sores or cracks which may lead to
discomfort.
U- Uterus Instructed the patient that distended uterus is normal. B- Bladder Encouraged patient to increased fluid intake. Instruct the client that day by day her uterus will go back into its normal position.B- Bowel
-
8/6/2019 Post Cs Na Revised Na Toh
30/30
Encouraged patient to increased fiber intake to avoid constipation.L- Lochia
Check for cervical secretions characteristics, amount, color, and odor.S- Sex
3-4 weeks or if the client dont feel pain nor discomforts.H- Hygiene
Regularly wound cleaning/ dressing.E- Exercise
Encouraged early ambulation (walking )