
Polypharmacy in the Elderly - tnpatientsafety.com · •Beers Criteria • List of potentially...
28
Polypharmacy in the Elderly Matthew Bledsoe, Pharm.D., BCPS Franklin Woods Community Hospital Tennessee Center for Patient Safety May 14, 2019
Transcript of Polypharmacy in the Elderly - tnpatientsafety.com · •Beers Criteria • List of potentially...

Polypharmacy in the Elderly
Matthew Bledsoe, Pharm.D., BCPS
Franklin Woods Community Hospital
Tennessee Center
for Patient Safety
May 14, 2019

Disclosure Statement
• The speaker of this presentation has nothing to disclose

Objectives
• Define polypharmacy
• Describe the pharmacokinetic differences in the elderly
• List the consequences of polypharmacy
• Review risk factors of adverse drug events in the elderly
• Describe how polypharmacy increases patient fall risk and evaluate strategies to improve
• Describe the method for reviewing and reducing polypharmacy
• Identify patient and prescriber barriers with polypharmacy reduction
Polypharmacy
• Wide range of definitions with no consensus
• Simple definition: the use of multiple medications
• Comprehensive definition: the use of medications with duplicative indications, drug-drug interactions, drug-disease interactions, inadequate attention to pharmacokinetics and pharmacodynamics, and the use of medications without a compelling indication
• > 5 medications/day
• > 12 doses/day
• > 2 Fall Risk Inducing Drugs
BMC geriatrics vol. 17,1 230. 10 Oct. 2017

Pharmacokinetic Changes in the Elderly
Absorption Metabolism
• Increased gastric pH
• Delayed gastric emptying
• Decreased absorptive surface
• Decreased splanchnic blood flow
• Decreased intestinal motility
• Decreased hepatic mass
• Decreased hepatic blood flow
• Decreased phase I (oxidative)
metabolism
• Unaltered phase II (conjugative and
acetylation) metabolism
Distribution Excretion
• Altered protein binding
• Decreased serum albumin
• Increased α-acid glycoprotein
• Decreased lean body mass
• Decreased total body weight
• Increased body fat
• Decreased creatinine clearance
• Decreased GFR
• Decreased tubular filtration
British journal of clinical pharmacology vol. 57,1 (2004): 6-14.


Medication Use in the Elderly
• Approximately 30% of adults age 65 and older take 5 or more medications
• Older adults make up approximately 14.5% of the US population, the proportion is expected to increase to 50% by the year 2040.
• JAMA Intern Med 2015;175(5):827–34.
• Administration on Aging. A profile of older Americans: 2015.
• American Geriatrics Society; 2014. p. 81–9.

Relationship Between Age and the Number of Prescribed Medications
Mangin, Dee & Parascandalo, Jenna & Khudoyarova, Olga & Agarwal, Gina &
Bismah, Verdah & Orr, Sherrie. (2019). Multimorbidity, eHealth and
implications for equity: a cross- sectional survey of patient perspectives on
eHealth. BMJ Open.

Why Does Polypharmacy Occur?
Reasons for Polypharmacy
Demographics
Health Factors
Healthcare Access
Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. JAMA 2002;287(3):337–44.

Over The Counter Medications

Prescribing Cascade
• Side effect or adverse drug reaction is misinterpreted as a new health condition
• New medication added
• May lead to further side effects and subsequent medications

Common Prescribing Cascades
Initial Medication Side Effect Secondary Medication
Prescribed for Side Effect
Antipsychotic Extrapyramidal adverse
effects
levodopa,
anticholinergics
Antiepileptics Nausea metoclopramide,
promethazine
Antihypertensives Dizziness prochlorperazine
Cholinesterase inhibitor Incontinence anticholinergics
(oxybutynin)
NSAID Hypertension antihypertensive
Thiazide diuretic Hyperuricemia, gout allopurinol, colchicine
Nurs Clin N AM 52 (2017) 457-468

Polypharmacy
Consequences
Adverse Drug Events/Reactions
Drug-Drug Interactions
Falls
Increased Hospitalization
Risk
Increased Medication Error
Risk
Non-adherence
Increased Costs
Decreased Quality of Life
Rollason V et al. Drugs Aging 2003; 20(11):817-32
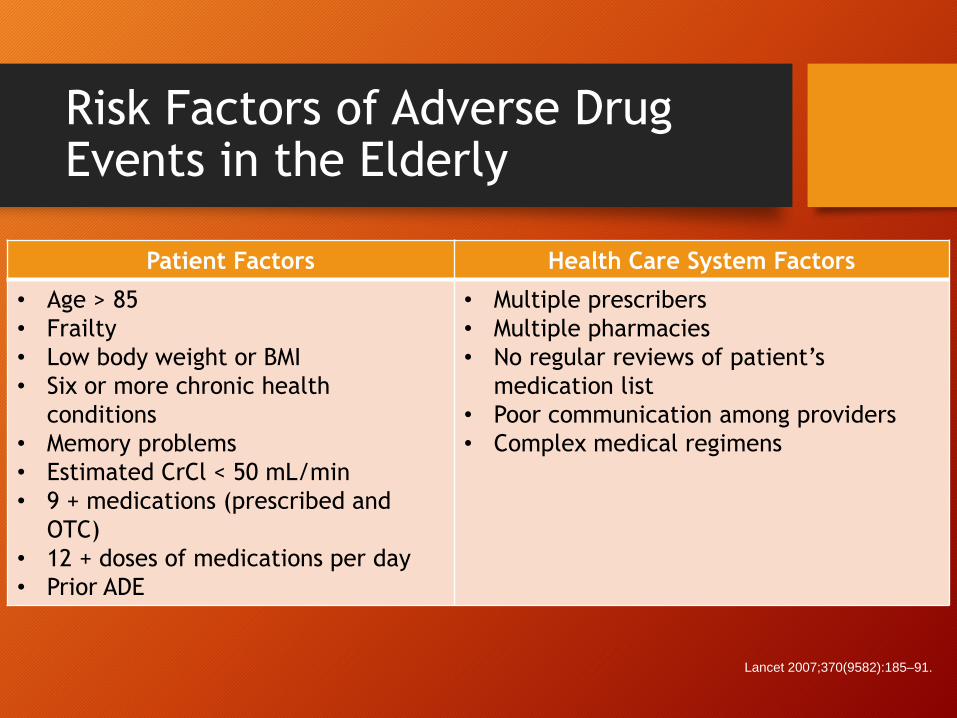
Risk Factors of Adverse Drug Events in the Elderly
Patient Factors Health Care System Factors
• Age > 85
• Frailty
• Low body weight or BMI
• Six or more chronic health
conditions
• Memory problems
• Estimated CrCl < 50 mL/min
• 9 + medications (prescribed and
OTC)
• 12 + doses of medications per day
• Prior ADE
• Multiple prescribers
• Multiple pharmacies
• No regular reviews of patient’s
medication list
• Poor communication among providers
• Complex medical regimens
Lancet 2007;370(9582):185–91.

Common Drug Classes Associated with Adverse Drug Events
Drug Class Common ADEs
• Anticoagulants • Bleeding/ulcerations
• Antipsychotics • Falls, Parkinsonism, Sedation
• NSAIDS • Bleeding/ulceration, Kidney Impairment
• Cardiovascular
Medications
• Falls, Decreased Heart Rate, Hypotension,
Depression, Hyperkalemia
• Diuretics • Falls, Hypotension, Hypo/Hyperkalemia,
SIADH/Hyponatremia
• Anticonvulsants • Sedation, Falls, SIADH/Hyponatremia
• Benzodiazepines • Falls, Delirium, Depression, Sedation
• Hypoglycemic
Medications
• Falls, Extreme Hypoglycemia
Nurs Clin N AM 52 (2017) 457-468

Falls
https://www.cdc.gov/steadi/

https://www.cdc.gov/steadi/

• CDC’s Injury Center created this
initiative, expressly for you—healthcare
providers who treat older adults who
are at risk of falling, or who may have
fallen in the past.
• The STEADI Initiative offers a
coordinated approach to implementing
the American and British Geriatrics
Societies’ Clinical Practice Guideline
for fall prevention.
• STEADI consists of three core elements
• Screen
• Assess
• Intervene (formulate and educate)
https://www.cdc.gov/steadi/

Reduce Medication Burden
Medication Burden Adherence

Identification of Potentially Inappropriate Medications
• Beers Criteria• List of potentially inappropriate medications for use in older adults (> 65 years)• Potentially inappropriate medications- treatments with risks that outweigh the
benefits• Updated in 2019
• STOPP Criteria • Risk > benefit• Overprescribing
• Excessive doses/duration
• Polypharmacy
• Incorrect prescribing- unfavorable choice of medication, dose, or duration• Under prescribing
• These tools are NOT an alternative to professional clinical judgment
J Am Geriatr Soc 00:1–21, 2019.Age and ageing vol. 44,2 (2014): 213-8

What to Do???
EVALUATE STOP REDUCE CONTINUE

Patient Barriers
• Psychologically attached
• Physical dependence
• Abandonment
• Thinks death is imminent
• Think the treatment is not longer useful

Healthcare Provider Barriers
• Concerned with patients’ resistance to change
• Concerned about other clinicians’ resistance to change
• Fear adverse drug reactions and withdrawal events
• Reluctant to stop medications that have been started by a colleague
• Unsure if the drug can be stopped abruptly or tapered

Whose Role?

Conclusion
• The elderly population is increasing at a drastic rate
• Polypharmacy represents a significant cause of morbidity in the elderly population
• Polypharmacy can have many different consequences
• There are several risk factors and polypharmacy concerns that lead to adverse drug events
• STOPP and Beers Criteria help with screening
• Patient barriers and provider barriers exist

References
• Administration on Aging. A profile of older Americans: 2015. 2015. Available at: https://aoa.acl.gov/Aging_Statistics/Profile/2015/docs/2015-Profile.pdf.
• American Geriatrics Society 2019 Updated AGS Beers Criteria. J Am Geriatr Soc 00:1–21, 2019.
• for Potentially Inappropriate Medication Use in Older Adults
• Kaufman, D. W., Kelly, J. P., Rosenberg, L., Anderson, T. E., and Mitchell, A. A. (2002). Recent patterns of medication use in the ambulatory adult population of the United States: the slone survey. JAMA 287, 337–344. doi: 10.1001/jama.287.3.337
• Kim, J., Parish, A. Polypharmacy and Medication Management in Older Adults. Nursing.theclinics.com Nurs Clin N AM 52 (2017) 457-468.
• Mallet L, Spinewine A, Huang A. The challenge of managing drug interactions in elderly people. Lancet 2007;370(9582):185–91.
• Mangin, Dee & Parascandalo, Jenna & Khudoyarova, Olga & Agarwal, Gina & Bismah, Verdah & Orr, Sherrie. (2019). Multimorbidity, eHealth and implications for equity: a cross-sectional survey of patient perspectives on eHealth. BMJ Open.
• Mangoni, A A, and S H D Jackson. “Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications.” British journal of clinical pharmacology vol. 57,1 (2004): 6-14. doi:10.1046/j.1365-2125.2003.02007.
• Masnoon, Nashwa et al. “What is polypharmacy? A systematic review of definitions.” BMC geriatrics vol. 17,1 230. 10 Oct. 2017, doi:10.1186/s12877-017-0621-2
• O'Mahony, Denis et al. “STOPP/START criteria for potentially inappropriate prescribing in older people: version 2.” Age and ageing vol. 44,2 (2014): 213-8. doi:10.1093/ageing/afu145
• Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Intern Med 2015;175(5):827–34.
• Semla TP. Pharmacotherapy. In: Flaherty E, Resnick B, editors. Geriatric nursing review syllabus: a core curriculum in advanced practice geriatric nursing. 4th edition. New York: American Geriatrics Society; 2014. p. 81–9.

Polypharmacy in the Elderly
Matthew Bledsoe, PharmD, BCPS
Franklin Woods Community Hospital
423-302-1088
Tennessee Center
for Patient Safety
May 14, 2019














![Medication review in the elderly: how competent are ...€¦ · Campanelli[4] CM .American Geriatrics Society (2012 )Updated Beers Criteria for Potentially Inappropriate Medication](https://static.fdocuments.net/doc/165x107/6012b764fd28c43c247919e2/medication-review-in-the-elderly-how-competent-are-campanelli4-cm-american.jpg)



