Polygon -...
103
ANCD research paper 18 Polygon the many sides to the Australian opioid pharmacotherapy maintenance system
Transcript of Polygon -...
AN
CD r
esea
rch
pape
r
18
Polygon
the many sides to the Australian opioid
pharmacotherapy maintenance system
Alison Ritter and Jenny Chalmers
Drug Policy Modelling Program, University of New South Wales
A report prepared for the Australian National Council on Drugs, 2009
AN
CD r
esea
rch
pape
r
18
Polygonthe many sides to the Australian opioid pharmacotherapy maintenance system
© Australian National Council on Drugs 2009
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without the written permission of the publisher.
Published by the Australian National Council on Drugs PO Box 205, Civic Square ACT 2608 Telephone: 02 6166 9600 Fax: 02 6162 2611 Email: [email protected] Website: www.ancd.org.au
National Library of Australia Cataloguing-in-Publication entry
Ritter, Alison.
Polygon: the many sides to the Australian opioid pharmacotherapy maintenance system / Alison Ritter, Jenny Chalmers.
ISBN: 9781877018213 (pbk)
ANCD Research Paper; 18.
Bibliography.
Drug addicts — Medical care — Australia. Chemotherapy — Australia. Opioid abuse — Treatment — Australia. Opioid abuse — Government policy — Australia. Drug abuse and crime — Australia.
Chalmers, Jenny. Australian National Council on Drugs.
615.580994
Editor: Julie Stokes Design: Starkis Design Printer: New Millennium Print
Acknowledgement:
This work has been supported by funding from the Australian Government Department of Health and Ageing.
The opinions expressed in this publication are those of the authors and are not necessarily those of the Australian National Council on Drugs or of the Australian Government.

Foreword
iii
ForewordThe evidence base to support the effectiveness of pharmacotherapy maintenance treatment for opioid dependence worldwide is compel-ling and substantial.1 Currently, 62 countries provide methadone while 35 countries provide buprenorphine as a medication treatment for opioid dependence.
In Australia, pharmacotherapy maintenance treatment is the most commonly provided treatment for heroin dependence with all juris-dictions, including to a much lesser extent pris-ons, now providing this form of treatment. As at June 2008 there were 41 347 people in treatment.
Since pharmacotherapy maintenance treatment for opioid dependence was introduced in 1969, Australia has continued to receive international recognition for its research and innovation. The early introduction of the pharmacotherapy maintenance program in Australia is credited, along with needle and syringe programs, with helping to avert and prevent an HIV epidemic.
Despite this good news, it is important to re-mind ourselves that no treatment system is per-fect. Unlike the period leading up to the early 2000s where Australia saw over 15 per cent growth each year in the number of people in treatment, it is now evident that there is in-creasing difficulty in gaining access to phar-macotherapy maintenance treatment. This situation is concerning, particularly with the identification by the United Nations Office of Drugs and Crime of an increase in heroin pro-duction from both Afghanistan and Myanmar as well as a growing increase in prescription opioid dependence in Australia.
To gain a clearer understanding of the issues facing pharmacotherapy maintenance treat-ment in Australia, the Australian National Council on Drugs (ANCD) commissioned Associate Professor Alison Ritter and Dr Jenny Chalmers from the Drug Policy Modelling Pro-gram at the University of New South Wales to undertake a project that assessed unmet demand, current capacity and the issues asso-ciated with supply and demand for pharmaco-therapy programs in the treatment of opioid dependence in Australia.
The project, which was conducted in two parts, produced two separate but comple-mentary reports. This report, hence known as the Polygon report, reviews the issues asso-ciated with the Australian pharmacotherapy program while the second report, Modelling Pharmacotherapy Maintenance in Australia: exploring affordability, availability, accessi-bility and quality using system dynamics assesses the extent to which such a model can inform relevant policy questions.
The Polygon report acknowledges that al-though pharmacotherapy services in Australia are better than in many other countries, there are aspects that warrant improvement. The authors raise a number of points which generally relate to the three key issues of ac-cessibility (access); affordability (cost); and availability (number of treatment places). In relation to these key issues it is important to note that the vast majority of pharmaco-therapy maintenance prescribing is provided
1 Mattick, R.P., Breen, C., Kimber, J., Davoli, M. & Breen, R. (2003). Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database of Systematic Reviews [online], 2003, Issue 2. Art. No.: CD002209. DOI: 10.1002/14651858.CD002209. Mattick, R.P., Kimber, J., Breen, C. & Davoli, M. (2008). Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database of Systematic Reviews [online] 2008, Issue 2. Art. No.: CD002207. DOI: 10.1002/14651858.CD002207.pub3.

Poly
gon
iv
within the private sector through general practice, and through specialist clinic serv-ices. Medication is mostly provided through community pharmacies.
The estimated $11.73 million per month in total program costs for the provision of meth-adone maintenance comes predominantly from State and Territory governments (43%) and, to a lesser extent, from the Australian Government. Consumers contribute 33 per cent of the amount; that is, approximately $3.8 million per month overall and an aver-age of $142 per month per client. While the total cost is substantially lower than the cost of managing a chronic disease, and substantially lower than the costs associated with not being in treatment, the consumer contribution is a significant barrier to access.
The Australian Government’s commitment to this program, which includes payment for the medication, private sector medical consultations and pathology costs as part of Medicare, has been an important contribu-tion to making treatment more accessible and affordable. Inclusion of these medicines into the Pharmaceutical Benefits Scheme (PBS) could however substantially reduce consumer costs and improve access to treat-ment. This point is discussed in Modelling Pharmacotherapy Maintenance in Australia in which the authors of the report examine the implications of reduced consumer costs in terms of longer treatment duration and better treatment access.
The Polygon report also highlights various other options that warrant further considera-tion. These include the introduction of other/alternate models of dispensing which do not involve daily attendance at a pharmacy for those who have been in long-term treat-ment and have maintained good treatment compliance. The importance of meaningful consumer involvement is also noted.
The ANCD is pleased to make this Polygon report available. It is a valuable report that confirms the effectiveness of pharmacother-apy maintenance treatment and its role in reducing the burden of harm to the individ-ual and the broader community. The ANCD thanks those who have participated in pro-viding information and the research team who have completed it. This report together with its companion report, Modelling Phar-macotherapy Maintenance in Australia, form two important pieces of research providing a solid foundation for the sector to work with government in developing the best mix of services to provide adequate availability, accessibility and affordability of the mainte-nance treatment program in Australia. Par-ticular thanks must also be paid to members of the ANCD who have worked to develop, support and oversee this report.
Dr John Herron, Chairman, Australian National Council on Drugs
July 2009
v
ContentsForeword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iii
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Notes on perspective and terminology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Executive summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ix
1 Background and context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Pharmacotherapy maintenance in Australia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.1 Australian pharmacotherapy program funding systems . . . . . . . . . . . . . . . . . . . . . . 7
2.2 Demand and unmet need for pharmacotherapy treatment . . . . . . . . . . . . . . . . . . 11
3 The issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1 What does the program aim to achieve? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.2 Service delivery models . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.3 Affordability for the client . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3.4 Accessibility of the program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
3.5 Efficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
3.6 Managing medication non-adherence and diversion . . . . . . . . . . . . . . . . . . . . . . 31
3.7 The role of unsupervised treatment and take-away dosing . . . . . . . . . . . . . . . . . 34
3.8 Counselling and psychosocial interventions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
3.9 Pharmaceutical opioid use and misuse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
3.10 Coordinating care in the Australian service system . . . . . . . . . . . . . . . . . . . . . . . . 43
3.11 Meaningful consumer involvement in the program . . . . . . . . . . . . . . . . . . . . . . . . 45
3.12 Keeping people in treatment (retention) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
3.13 Child protection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
3.14 Stigma in the Australian pharmacotherapy system . . . . . . . . . . . . . . . . . . . . . . . . 54
3.15 Creating and sustaining the workforce . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
3.16 Prisoners and pharmacotherapy maintenance . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3.17 Rural and remote issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
3.18 Clinical issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
3.19 Other issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
3.20 Future research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
4 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
5 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
vi
6 Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
6.1 Appendix A: Stakeholders consulted as part of the project . . . . . . . . . . . . . . . . . 86
6.2 Appendix B: Take-away policies for buprenorphine . . . . . . . . . . . . . . . . . . . . . . . 89
Tables and figuresTable 1: Estimated number of pharmacotherapy clients by prescriber type and
jurisdiction (on a specified/snapshot day) 2007 (%) . . . . . . . . . . . . . . . . . . . . . 7
Table 2: Proportion of pharmacotherapy clients and contributions to funding by prescriber and dispenser type in 2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Table 3: Complaints mechanisms for pharmacotherapy clients . . . . . . . . . . . . . . . . . . . 46
Figure 1: Pharmacotherapy treatment clients from 1985 to 2007 . . . . . . . . . . . . . . . . . . 5
vii
Expert Advisory GroupAn Expert Advisory Group provided important input into this report. The group comprised: Associate Professor Nick Lintzeris, Tamara Speed, Dr Bob Batey, Dr Alex Wodak and Professor Richard Mattick.
AcknowledgementsA large number of people contributed vital information for this report. Health depart-ments around Australia, especially in Victoria and New South Wales, were extremely helpful. Researchers provided access to documenta-tion. Consumers around Australia engaged with us on the consultation paper and pro-vided significant feedback. All the people who provided input are listed at Appendix A. Over and above this, we would like to particularly thank the Expert Advisory Group, the ANCD project reference group, Colleen Faes who provided invaluable assistance with referenc-ing, and David Bright for his editorial advice.
Notes on perspective and terminologyPolygon: We chose to call this work ‘Polygon’. A polygon is a many-sided figure. Our choice of this title is designed to help the reader appreciate that:
• pharmacotherapy maintenance in Australia is multi-faceted
• depending on your point of view, some of the sides will be more important or have more value than others
• each of the sides, including those that are not apparent to the viewer, is essential to making the figure whole.
This project takes a systems perspective, view-ing pharmacotherapy maintenance in Australia as one system, with a range of interwoven components, including the types of treatment available and the range of treatment provid-ers (both prescribers and dispensers). Varying perspectives on the components and on the system as a whole are held by the clients in the program: medical practitioners, pharma-cists, allied health and support services, policy makers, researchers and active drug users.

Poly
gon
viii
In writing this research paper, we have en-deavoured to cover all the perspectives. In doing so, it has been quite challenging to accurately represent the issues from the variety of conflicting and contrasting per-spectives. Reconciling those perspectives is an even more demanding task and some-times not achievable. The medical profes-sion talks of patients and recovery; while the drug-using community talks of users, con-sumers, reduction of drug-related harm, and rights to use drugs. An example of different perspectives is in relation to the goals of the program: for medical practitioners, the focus is on cessation of drug use and improved health status; for drug users, the goals may be temporary relief from injecting drug use. The objective of the report is to represent all the issues from all the perspectives.
In endeavouring to fairly and accurately rep-resent the issues, we have also had to make some pragmatic decisions about terminol-ogy. So rather than change the terminology depending on whose perspective we are de-scribing, we have elected to use a standard set of terms in the report.
Patient, client, consumer?
People who receive pharmacotherapy main-tenance treatment are variously referred to as patients, clients or consumers, sometimes even customers. We have chosen to use the term ‘client’ throughout this report.
Pharmacotherapy maintenance program
There are a number of terms used to denote the pharmacotherapy maintenance program: opiate substitution treatment (OST), opioid agonist medication, methadone maintenance program (MMP), buprenorphine maintenance program (BMP), opioid maintenance program. Some of these terms have potential unwanted connotations. For example, ‘maintenance’ can imply a life-long program; ‘substitu-tion’ can mean to some that the program merely replaces illegal drugs (rather than ‘cures’ people). The ‘opioid agonist’ term is highly technical. We have chosen the term ‘pharmacotherapy maintenance program’ as the most acceptable of the available options.
Executive summ
ary
ix
Executive summaryIntroductionThe Australian National Council on Drugs (ANCD) commissioned the Drug Policy Modelling Program to undertake a project to investigate and review the availability, accessibility and affordability of pharmaco-therapy maintenance treatment. The project was conducted in two parts: a qualitative review of the issues associated with the Australian pharmacotherapy program (this research report); and a system dynamics model of the pharmacotherapy treatment system (a separate companion report: see ANCD Research Paper 19).
No treatment service system is perfect. While pharmacotherapy services in Australia are better than in many other countries, there are aspects of the program that could be improved. There are also aspects that some people find concerning.
We acknowledge the multiple and divergent perspectives of the many stakeholders to the Australian pharmacotherapy system: govern-ment officials; current clients; prospective clients (active drug users); and practitioners (doctors, pharmacists, nurses, case workers and counsellors). Our goal was not neces-sarily to resolve the issues we present, but in representing the various perspectives and communicating a critical appraisal of rele-vant research findings, we intend to provide a basis for informed discussion and debate.
MethodsMultiple sources of data were used to derive the final list of issues. First, a preliminary list of all potential issues was generated by the research team in consultation with the Advisory Group. This list was then circu-lated widely for stakeholders to add to it. A literature search followed. Both academic and grey literatures were consulted. A con-sultation document was then prepared and circulated widely for feedback from all stake-holders. A range of stakeholders provided feedback, amendment and new information.
Results — the issuesThe top seven key issues for the Australian pharmacotherapy maintenance program are: the overall goals of the program; service delivery models; affordability of the pro-gram to clients; accessibility of the program; medication non-adherence and diversion; unsupervised dosing; and the role of coun-selling. There are also a number of other issues which are addressed in the report.
Poly
gon
x
1. What does the program aim to achieve?
The goals of the Australian pharmacotherapy maintenance treatment system are:
• to reduce or cease harmful heroin use
• to improve physical health
• to reduce risk for infectious diseases
• to improve psychological, social and occu-pational functioning, including a reduc-tion in crime.
There is no consensus across all stakehold-ers that abstinence as well as reduction in drug use are both acceptable program goals. There is also debate about whether absti-nence means abstinence from illicit drugs, or from all drugs, including prescribed drugs. This partly stems from a tension between community expectations and the reality of heroin dependence as a chronic relapsing condition. Given the heterogeneity of cli-ents in the program, with their own goals and expectations, and practitioner expertise in tailoring the program to best meet each client’s needs, we believe that focusing on an individual client’s treatment goals will produce the most effective outcomes at the individual level and hence for the Australian program as a whole.
2. Service delivery models
There are two predominant models of phar-macotherapy service provision in Australia: public clinics and primary health care/ general practitioner (GP) services. A key issue is the extent to which there are differences in out-come according to service model. Existing international research suggests that there are no systematic outcome differences between the different models of care. The thera-peutic milieu, relationships between clients and the practitioners, staff attitudes and
organisational climate all have a significant impact on treatment outcomes, regardless of the service delivery model. In this context then, it is useful to explore the implications of the relative mix between the service models of public clinics and primary health care/GP services; the risks and vulnerabilities with each model; the resource implications for government; and from a client perspective, the coordination between these systems of care.
3. Affordability for the client
Currently State, Territory and federal gov-ernments, as well as clients, all contribute to the funding of opioid pharmacotherapy treatment services. A central issue for the Australian program is the affordability of the program for clients. Clients incur costs associ-ated with: dispensing fees; other fees (such as the gap between the fee charged by a medical practitioner and the Medicare benefit); and other costs (such as travel costs). The most significant cost tends to be dispensing fees, and we estimate that close to 80 per cent of Australian pharmacotherapy clients pay fees. Many clients struggle to afford these fees, and this can impact on future access (debts, black lists) and on local welfare services (which pay either directly, or indirectly by covering food/ accommodation). There is no means testing or State/national agreement on appropriate fee levels per dosing frequency. There are two major concerns with dispensing fees: the potential negative impact that they have on treatment entry and on retention in treatment; and secondly, the fact that they are inequita-ble. The inequities associated with dispensing fees would be significantly ameliorated with the introduction of a system consistent with current Australian Government funding of Pharmaceutical Benefits Scheme (PBS) medi-cations. Alternatively, efforts could be directed towards ensuring that clients in financial need are given access to free dispensing.
Executive summ
ary
xi
4. Accessibility of the program
Accessibility problems exist in relation to both access to prescribers and access to dispensing services. New entrants to treatment often have to wait, but the numbers of people waiting and the length of waiting time are difficult to determine and vary considerably geographically. There were not only concerns about the access problems associated with rural and remote areas, but also concerns about areas of limited access in cities and regional areas. To what extent are programs operating at full capacity? Can efficiency be improved? Or will efficiencies result only in a lower standard of care? There is a trade-off between making programs highly accessible, for example through low- threshold programs, and ensuring high- quality interventions for individual clients.
5. Managing medication non-adherence and diversion
We distinguish between medication non- compliance and diversion. Non- compliance means the client is not taking the medica-tion as prescribed. Diversion involves selling/exchanging the medication on the black mar-ket. Non- compliance, in the form of injecting one’s own medication, can be associated with significant harms. At the same time, non- compliance is common in most client groups and arguably enables a more individually tai-lored regime. Diversion can also be associated with significant harm and criminal activity. The program has been threatened by the behav-iour of people who fail to comply or who divert drugs. Measures to minimise the harms caused by diversion and non-compliance are important.
6. The role of unsupervised treatment and take-away dosing
Take-away doses, in which clients are given future supplies to consume without su-pervision, have always formed part of the Australian pharmacotherapy maintenance program. Unsupervised treatment (or unob-served treatment) is a relatively new con-cept associated with the introduction of buprenorphine-naloxone. In general, unsu-pervised treatment refers to a program where clients are provided with a ‘script’ to collect one supply of medication at a time (being scripted for a week, a month, or as prescribed by the doctor). At present, the term ‘take- away’ and the term ‘unsupervised treatment’ are being used interchangeably in Australia, despite the difference in connotation and the different aetiology of the terms. It is sug-gested that the terms be used more specifi-cally as defined above.
Take-away doses provide opportunities for autonomy and independence for clients. Preferably, take-away policies would be built around an evidence base that balances risks and benefits, and provides for individ-ual tailoring. There is substantial variation in take-away policies between jurisdictions. Nation ally consistent policies and clini-cal guidelines for take-away doses may be warranted. There is limited evidence to in-dicate that unsupervised treatment is effec-tive in enhancing treatment retention early in the treatment episode (within the first six months). However, unsupervised treatment for long- term stable clients is linked to bet-ter treatment retention and should be further explored as a treatment model.
Poly
gon
xii
7. The role of counselling and psychosocial interventions
There is evidence that both counselling and support services improve client outcomes in pharmacotherapy maintenance, if they are sought by the client rather than man-dated. Ensuring effective referral pathways and access to counselling and mental health services is important. Both counselling and psychosocial support should be available but neither should be a mandatory component of pharmacotherapy maintenance.
Other issues identified in the report include the importance of collaborative care planning; growth in the prescribing of pharmaceutical opioids, which may have implications for the pharmacotherapy maintenance treatment sys-tem; the importance of meaningful consumer involvement in the Australian pharmaco-therapy maintenance program; the negative impacts of stigma and discrimination against pharmacotherapy maintenance programs; the challenging issues associated with the interface between the program and child protection services; creating and sustaining the workforce; meeting the needs of prison-ers; and issues for service provision in rural and remote areas of Australia.
Future researchThe report identifies a number of impor-tant areas for future research. These include research questions such as:
• What are the implications for the clients and the system of the current inequitable dispensing fee system?
• What is more important: cumulative reten-tion or overall time in treatment?
• What is the appropriate balance between low-threshold public health service deliv-ery models and individually tailored treat-ment models?
• Could Australian programs be made more efficient?
• What is the unmet demand for pharma-cotherapy treatment?
• What are the benefits for mothers (or primary carers of children) of being in pharmaco-therapy maintenance?
• What role does a model of unsupervised treatment have in Australia?
ConclusionThe aim of this project was to examine the issues associated with pharmacotherapy main-tenance treatment in Australia. The key issues surround accessibility (access); affordability (cost); and availability (number of treatment places). Effective planning for a sustainable future for pharmacotherapy programs in Aus-tralia requires consideration and debate of the issues identified in this project.

Background and context
1
1. Background and contextThe Australian National Council on Drugs (ANCD) commissioned the Drug Policy Mod-elling Program to undertake a project to investigate the availability, accessibility and affordability of pharmacotherapy maintenance treatment. The project was conducted in two parts: a qualitative review of the issues asso-ciated with the Australian pharmacotherapy program (this report); and a system dynam-ics model of the pharmacotherapy treatment system (a separate companion report : see ANCD Research Paper 19).
No treatment service system is perfect. While pharmacotherapy services in Australia are bet-ter than in many other countries, there are aspects of the program that could be improved. There are perceived problems and issues with the program’s current structure, risks for future service provision and concerns with ongoing quality improvements to the programs, such as meaningful consumer involvement. We have used the term ‘issues’ to denote these various problems, perceived problems, potential future problems and concerns.
The treatment focus of this report is on opi-oid agonist maintenance (in this case, meth-adone and buprenorphine). It does not cover withdrawal, naltrexone or other forms of medication treatment for opioid dependency.
We acknowledge the multiple and divergent perspectives of the many stakeholders to the Australian pharmacotherapy system: govern-ment officials; current clients; prospective clients (active drug users); and practitioners (doctors, pharmacists, nurses, case workers and counsellors). Our goal is not necessarily to resolve the issues presented, but in rep-resenting the various perspectives and com-municating a critical appraisal of relevant research findings, our intention is to provide a basis for informed discussion and debate.
Multiple sources of data were used to derive the final list of issues. First, a preliminary list of potential issues was generated by the research team in consultation with the Advi-sory Group. This list was circulated widely for stakeholders to add to it. A literature search followed — of both academic and grey litera-tures with the focus on Australian literature. A consultation document (referred to herein as the ‘issues paper’) was then prepared and circulated widely for feedback from all stake-holders. A range of stakeholders provided feedback, amendment and new information. The stakeholders are listed at Appendix A. This report presents a consolidation of in-formation from the literature, stakeholders and the Advisory Group.
Finally, by way of preamble, despite our iden-tification of a significant number of issues, it is not the authors’ belief that the program is highly problematic. Nor that all these issues could or should be immediately attended to and rectified. Like all clinical services, the pharmacotherapy program should be subject to ongoing improvement over time. Many of the issues are long- running and have already been identified. Some have received atten-tion resulting in some incremental improve-ments. Our goal is to identify and document the issues, so that the relevant authorities can continue to refine and improve upon a vital treatment type.
Poly
gon
2
2. Pharmacotherapy maintenance in AustraliaThis section describes Australian pharmaco-therapy maintenance from a systems per-spective. We view it as a range of overlapping and interlinked systems of care, each with its own stakeholders, viewpoints and issues. For example, States and Territories represent one level of the overall system, and are respon-sible for the development of the treatment system within their own State or Territory. Medical practitioners are another system of care, prescribing pharmacotherapies in vari-ous ways. A significant amount of dispens-ing is undertaken in community pharmacies, and the system of community pharmacies can be differentiated from other forms, or systems, of dispensing. Even a public clinic (undertaking both prescribing and dispens-ing) and a GP practice can be seen as unique systems of care.
We contend that there is much to be gained from viewing Australian pharmacotherapy maintenance from a systems perspective, especially in light of the many interlinked and overlapping components. From such a perspective, an overall view of the current program is impeded by the separate models of care in different jurisdictions, separate funding arrangements (State/federal/client), and lack of national consistency in policy and practice (for example, take- away dos-ing; dispensing fees). For these reasons we have endeavoured to view the topography of pharmacotherapy maintenance in Australia from above rather than from within.
Methadone has proven to be a highly effec-tive treatment for heroin dependence. Over 20 years of research have demonstrated that methadone reduces heroin use, reduces crimi-nal behaviour, improves health and improves psychosocial functioning. Both methadone and buprenorphine have been demonstrated
to be highly cost- effective relative to other treatments such as detoxification alone or residential rehabilitation (Moore, Ritter & Caulkins, 2007). Of the pharmacological treat-ments available, methadone maintenance is the most cost-effective (Amato, Davoli, Perucci et al., 2005; Doran, Shanahan, Digiusto et al., 2006; Doran, Shanahan, Mattick et al., 2003; Harris, Gospodarevskaya & Ritter, 2005).
The benefits of methadone maintenance ex-tend beyond the client to society at large. Cost–benefit research has demonstrated that the costs associated with providing metha-done maintenance are significantly lower than the accrued societal economic bene-fits. Estimated across more than 20 studies, the ratio of economic benefits to costs of the program range from 2:1 to 38:12 (see Belenko, Patapis & French, 2005; Cartwright, 2000; Connock, Juarez-Garcia, Jowett et al., 2007; Simeons, Matheson, Inkster et al., 2002; Zarkin, Dunlap, Hicks & Mamo, 2005).
With a study of the benefits of pharmaco-therapy maintenance from this summary perspective, it can be easy to overlook the complexity of the client group and de-mands on service providers. Clients are a heterogeneous group. Some clients are high-functioning members of society. Other phar-macotherapy clients are polydrug users, not only on entry to treatment, but also dur-ing treatment (Ross, Teesson, Darke et al., 2005). Co- occurring mental and/or physical health problems are common amongst phar-macotherapy clients (Darke & Ross, 1997). Many clients have significant psychosocial problems (such as housing, family and em-ployment). Over the span of treatment these problems and issues represent continued and changing needs.
2 One study, the Harwood study on the TOPS participants, had a cost–benefit ratio of 1:0.92, as cited in Cartwright (2000).

Pharmacotherapy m
aintenance in Australia
3
Despite the strength of the evidence base, there are some who believe that the pro-vision of a legal opioid to heroin users is problematic for moral reasons. Unfortunately pharmacotherapy maintenance treatment has been misappropriated into debates about harm minimisation and zero tolerance ap-proaches to drug policy (see, for example, the Australian Parliamentary Library research paper by Thomas and Buckmaster (2007)).
Methadone was introduced into Australia in 1970 but did not have a major role within heroin treatment until the mid-1980s, with the injection of new funds to support methadone maintenance programs as part of the National Campaign Against Drug Abuse (NCADA) and in the context of the then new HIV (human immunodeficiency virus) concerns. Numbers in methadone maintenance treatment have increased progressively since then.
The original methadone maintenance pro-grams were provided by State and Territory government services (public clinics) and cov-erage across jurisdictions was uneven (with some jurisdictions lacking any programs). As the demand for methadone grew, there was pressure to develop alternate systems of service delivery. Overseas, public clinics were associated with problems of client congre-gation (antisocial behaviour, drug dealing), limited geographic accessibility, and mar-ginalisation of clients and staff. In parallel, some State governments in Australia were also reconfiguring the role of government in direct service provision and moving towards a ‘purchaser–provider split’ in service provision. In these cases, notably Victoria, the public clinics were replaced with a small number of specialist services and a new system of
service delivery established: prescribing by general medical practitioners with dispens-ing in community pharmacies. Arguably the relative advantage of this model of service delivery was greater integration of methadone maintenance into primary health care settings and improved accessibility for clients. The funding implications were also significant: medical and investigation (urinalysis) costs shifted from the State to the federal govern-ment, and dispensing fees shifted from the State government to the client.
Until 2000, methadone was the only main-tenance medication available to treat heroin dependence. Buprenorphine (in the mono product form, Subutex) was registered in November 2000 and PBS approval gained in August 2001. The service system established for buprenorphine treatment in Australia paralleled that for methadone. That is, the same prescribers and dispensers were trained and able to provide buprenorphine treatment. Buprenorphine, a partial opiate agonist, pro-vided the possibility for less than daily dosing, less risk of opioid toxicity (overdose) during both induction and maintenance, and greater utility as a detoxification medication than methadone.
Early trials of the relative efficacy and cost-effectiveness of buprenorphine in Australia illustrated demonstrably equitable efficacy between methadone and buprenorphine (Lintzeris, Ritter, Panjari et al., 2004; Mattick, Kimber, Breen & Davoli, 2007), mirrored in overseas research (Johnson, Chutaupe, Strain et al., 2000). The latest review (Connock

Poly
gon
4
et al., 2007) concludes that methadone is slightly more effective and less costly than buprenorphine (see also Harris et al., 2005; Mattick et al., 2007).
However, with a less demanding withdrawal syndrome than methadone, and less than daily dosing for some clients, buprenorphine represents some advantages for clients and providers. Two maintenance medications pro-vide greater client choice.3
The drug company (Reckitt Benckiser) de-veloped a new medication, buprenorphine-naloxone (Suboxone), to discourage diversion of buprenorphine. This was vital to the suc-cessful introduction of buprenorphine into the American market, as it would be provided in primary health care settings (with associ-ated unsupervised dispensing) rather than the existing methadone clinics (Mintzer, Ei-senberg, Terra et al., 2007). Buprenorphine-naloxone was registered in Australia in July 2005 and listed on the PBS in April 2006.
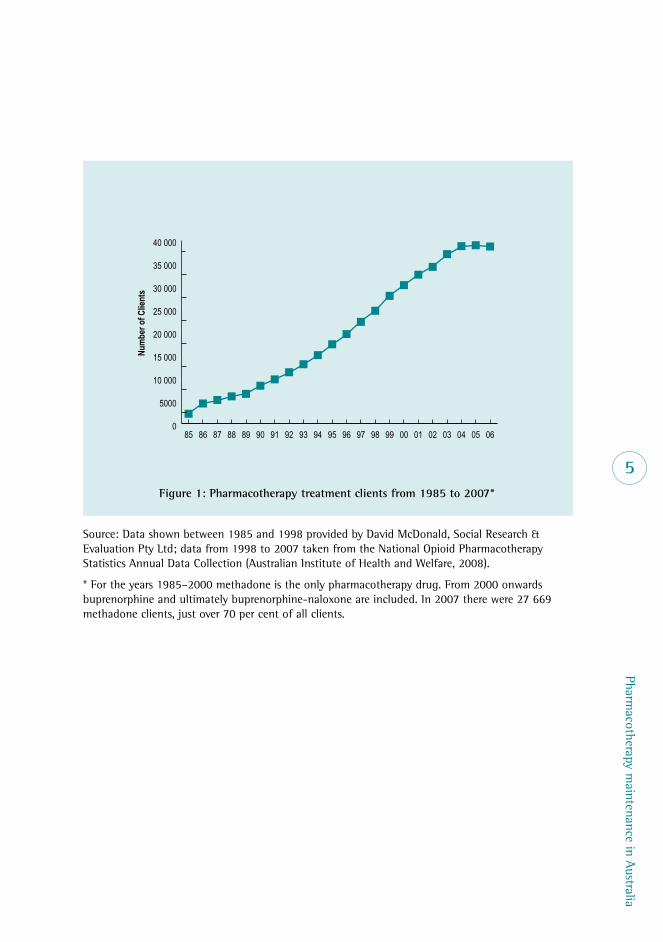
Methadone was still the most widely pre-scribed pharmacotherapy (72%) at June 2007, followed by buprenorphine alone (22.5%), then buprenorphine-naloxone (5.5%).4 Figure 1 shows the numbers of clients reg-istered to be in pharmacotherapy treatment in Australia on a specified day in June of each year from 1985 to 2007. It is a compilation of the State and Territory registration figures.
The building blocks of the systems of care for pharmacotherapy maintenance in Aus-tralia are the prescribing, dispensing and counselling systems. Prescribing of opioid maintenance pharmacotherapies occurs in four settings: specialist pharmacotherapy clinics (usually referred to as ‘public clinics’), staffed by specialist addictions practition-ers; GP settings (sometimes referred to as office-based care, or primary health care); private clinics where the prescriber is a GP; and prisons.5 Clients may be prescribed their maintenance medication from any one of these settings and, within any one continu-ous episode of care, they may be transferred between settings in some jurisdictions; for example, the client may be inducted in a public clinic and, once stabilised, transferred to a GP prescriber.
The system for dispensing the opioid phar-macotherapies is equally layered. Dispensing can occur in a public clinic, in a chemist/pharmacy, at a private clinic, in prison or in hospital. Dispensing sites are associated with different fee arrangements. There is no direct concordance between the prescriber arrange-ments and the dispensing arrangements. For example, some clients are prescribed and dis-pensed within public clinics; some are pre-scribed in public clinics and dispensed in local pharmacies, and so on.
3 However, there are no data to indicate the extent to which the introduction of buprenorphine in Australia encouraged new heroin and pharmaceutical opioid users into treatment.
4 The 2007 data are the most recent that are publically available. These data have distinguished between buprenorphine and buprenorphine–naloxone only from 2006. We are aware that the extent of buprenorphine-naloxone prescribing has substantially increased in some jurisdictions.
5 The datasets used by the Australian Government do not distinguish between private clinics and GP settings — both are classified as ‘private’ because the prescribing is paid for through Medicare.
Pharmacotherapy m
aintenance in Australia
5
0
5000
10 000
15 000
20 000
25 000
30 000
35 000
40 000
06050403020100999897969594939291908988878685
Num
ber o
f Clie
nts
Figure 1: Pharmacotherapy treatment clients from 1985 to 2007*
Source: Data shown between 1985 and 1998 provided by David McDonald, Social Research & Evaluation Pty Ltd; data from 1998 to 2007 taken from the National Opioid Pharmacotherapy Statistics Annual Data Collection (Australian Institute of Health and Welfare, 2008).
* For the years 1985–2000 methadone is the only pharmacotherapy drug. From 2000 onwards buprenorphine and ultimately buprenorphine-naloxone are included. In 2007 there were 27 669 methadone clients, just over 70 per cent of all clients.
Poly
gon
6
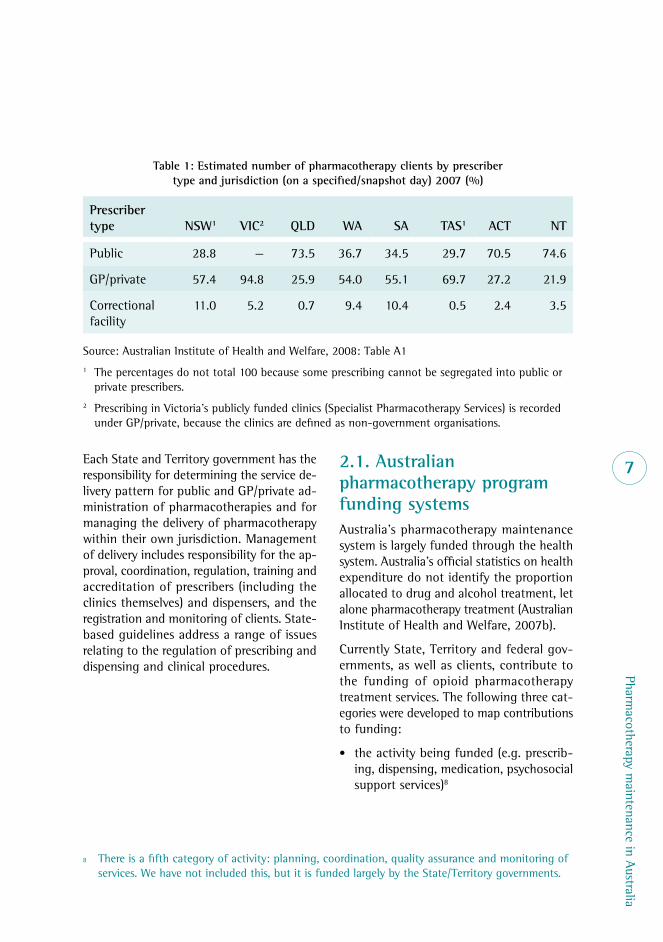
Jurisdictions in Australia differ in the ways in which pharmacotherapy programs are provid-ed.6 All jurisdictions have public clinics while only New South Wales has private clinics. In some jurisdictions the majority of pharma-cotherapy service provision occurs in general practice settings. Table 1 demonstrates the high variability across Australian jurisdictions in the proportions of clients associated with each of the prescriber types.
Jurisdictional differences in service provision are complemented by variations in regulatory arrangements and structures. For example, the regulations around take-away dosing vary between jurisdictions. In addition, the availa-bility of pharmacotherapy maintenance varies between and within jurisdictions. New South Wales and Victoria account for 70.5 per cent of all pharmacotherapy maintenance clients.7 We did not seek to compare, nor describe in detail, the various jurisdictional differences, but it is important to keep these in mind as the issues identified below will not be evenly applicable.
In 1985, the first national policy for metha-done was developed by federal, State and Territory governments and was endorsed by the Ministerial Council on Drug Strategy
(MCDS), the peak body for drug and alcohol policy development. This policy was designed to provide a common set of principles for pharmacotherapy treatment, a framework for State and Territory policies and clinical guidelines for pharmacotherapy treatment. In 2002–2003 there was a separation of the national policy framework (a responsibility of the Intergovernmental Committee on Drugs (IGCD) Methadone and Other Treat-ment Subcommittee) and clinical treatment guidelines (the responsibility of the National Expert Advisory Committee on Illicit Drugs). The current national policy is the National Pharmacotherapy Policy for People Depend-ent on Opioids (Commonwealth of Australia, 2007). National clinical practice guidelines are available for methadone and buprenorphine (Henry-Edwards, Gowing, White et al., 2003; Lintzeris, Clark, Winstock et al., 2006). The Expert Committee was disbanded in 2004 and since then there has been limited oppor-tunity for jurisdictions and experts to come together to discuss and debate policy and clinical guidelines in the pharmacotherapy maintenance area.
6 The funding body for this research requested that comparisons between jurisdictions not be made.
7 These data and other data about numbers of pharmacotherapy clients within this report come from the annual Australian Institute of Health and Welfare publication on alcohol and drug treatment services in Australia (Australian Institute of Health and Welfare, Alcohol and Other Drug Treatment Services in Australia: report on the National Minimum Data Sets 2000–2006. Drug Treatment Series: nos 1–7. Canberra, 2002–2007). The latest published report is for 2007 (Australian Institute of Health and Welfare, 2008). There are some substantial uncertainties with the data: the jurisdictions record and report the data in different ways. Currently all, except Western Australia, are census date data (i.e. they reflect a single day in June). Western Australia reports over the month of June. Sometimes the data are reported as registration (for treatment) data (Figure 1). The registration data overestimate numbers (as registrations can remain active when the client has ceased treatment). Sometimes the data include only clients who were dosed on the census date, which is an under-estimation of numbers (as clients miss doses). Jurisdictions have also changed the method of reporting over time. For this reason, the data need to be treated as indicative only.
Pharmacotherapy m
aintenance in Australia
7Each State and Territory government has the responsibility for determining the service de-livery pattern for public and GP/private ad-ministration of pharmacotherapies and for managing the delivery of pharmacotherapy within their own jurisdiction. Management of delivery includes responsibility for the ap-proval, coordination, regulation, training and accreditation of prescribers (including the clinics themselves) and dispensers, and the registration and monitoring of clients. State-based guidelines address a range of issues relating to the regulation of prescribing and dispensing and clinical procedures.
2.1. Australian pharmacotherapy program funding systemsAustralia’s pharmacotherapy maintenance system is largely funded through the health system. Australia’s official statistics on health expenditure do not identify the proportion allocated to drug and alcohol treatment, let alone pharmacotherapy treatment (Australian Institute of Health and Welfare, 2007b).
Currently State, Territory and federal gov-ernments, as well as clients, contribute to the funding of opioid pharmacotherapy treatment services. The following three cat-egories were developed to map contributions to funding:
• the activity being funded (e.g. prescrib-ing, dispensing, medication, psychosocial support services)8
Table 1: Estimated number of pharmacotherapy clients by prescriber type and jurisdiction (on a specified/snapshot day) 2007 (%)
Prescriber type NSW1 VIC2 QLD WA SA TAS1 ACT NT
Public 28.8 — 73.5 36.7 34.5 29.7 70.5 74.6
GP/private 57.4 94.8 25.9 54.0 55.1 69.7 27.2 21.9
Correctional facility
11.0 5.2 0.7 9.4 10.4 0.5 2.4 3.5
Source: Australian Institute of Health and Welfare, 2008: Table A11 The percentages do not total 100 because some prescribing cannot be segregated into public or
private prescribers.2 Prescribing in Victoria’s publicly funded clinics (Specialist Pharmacotherapy Services) is recorded
under GP/private, because the clinics are defined as non-government organisations.
8 There is a fifth category of activity: planning, coordination, quality assurance and monitoring of services. We have not included this, but it is funded largely by the State/Territory governments.
Poly
gon
8
• the setting or provider of those services (e.g. public clinics, GPs, private clinics, correctional facilities), and
• the funding body (e.g. State, federal, client).
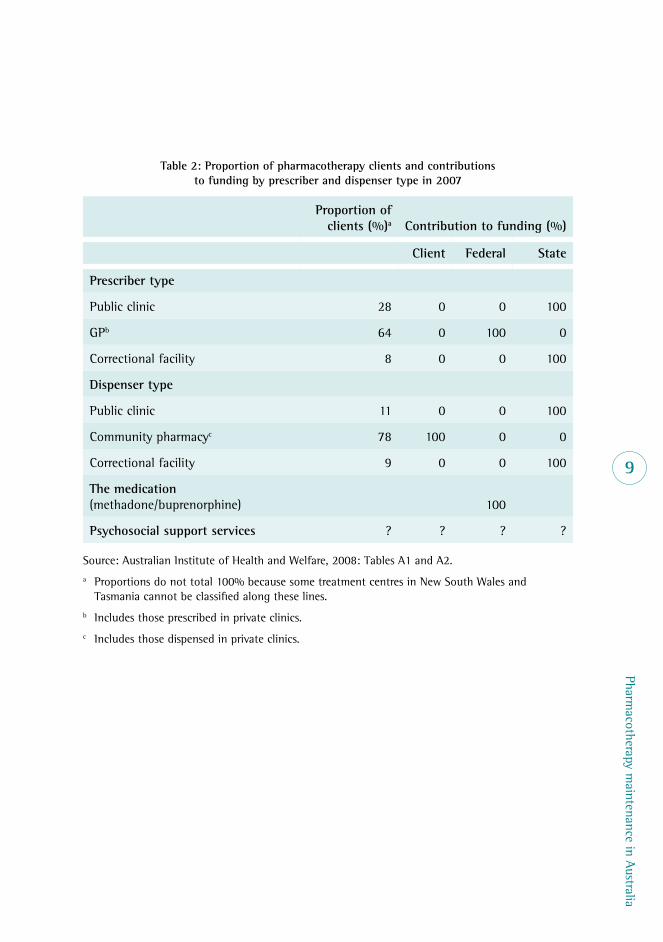
Table 2 shows the proportion of clients within each prescriber and dispenser type, and the contributions to funding by each funding body. The contributions to funding are stylised, in the sense that they do not represent the actual contributions. Rather they represent the ‘spirit’ of the relevant funding model. The table shows that the State/Territory governments fund all costs of prescribing undertaken in public clinics and in prisons, covering 36 per cent of cli-ents. The remaining clients are prescribed in the private sector where, assuming that the medical practitioner bulk-bills, the Australian Government provides the funds. The federal government covers the costs of the pharma-cotherapy medications; the State/ Territory governments pay for dispensing in all prisons and most public clinics. Almost 80 per cent of clients are dispensed in community phar-macies and private clinics and most of them pay for the dispensing themselves.
Table 2 highlights that there is no available information on the number of clients access-ing psychosocial support services, nor who bears the costs of such services.
Prescribing
In public clinics and in prisons the prescrib-ing is funded entirely by the relevant State/Territory government.9
In the GP and private sector the costs of medical consultations and pathology tests for methadone and buprenorphine clients are covered by the federal government under Medicare. It is assumed that no costs are borne by the clients, based on an assump-tion that the doctor charges no more than the Medicare benefit, i.e. the rebate patients receive from the federal government. The GP payment structure is consistent with the funding of other primary health care services to the wider community. As such, it reinforces the concept that pharmaco-therapy maintenance treatment is akin to other forms of care provided by private prac-titioners, and avoids any stigma that might be generated by a payment method which differs from that for other primary care serv-ices. Medicare-funded services associated with pharmacotherapy maintenance are not distinguishable from other visits to medi-cal practitioners in the Medicare Benefits Schedule (MBS) statistics.10 The frequency of service provision is a matter of practitioner judgement, in concert with recommenda-tions in clinical guidelines (Henry-Edwards, Gowing, White et al., 2003; Lintzeris et al., 2006).
9 These funds come out of the pool of State spending on health funded through State general taxation revenue via transfers from the federal government.
10 <http://www.medicareaustralia.gov.au/statistics/dyn_mbs/forms/mbsgtab4.shtml>.
Pharmacotherapy m
aintenance in Australia
9
Table 2: Proportion of pharmacotherapy clients and contributions to funding by prescriber and dispenser type in 2007
Proportion of clients (%)a Contribution to funding (%)
Client Federal State
Prescriber type
Public clinic 28 0 0 100
GPb 64 0 100 0
Correctional facility 8 0 0 100
Dispenser type
Public clinic 11 0 0 100
Community pharmacyc 78 100 0 0
Correctional facility 9 0 0 100
The medication (methadone/buprenorphine) 100
Psychosocial support services ? ? ? ?
Source: Australian Institute of Health and Welfare, 2008: Tables A1 and A2.a Proportions do not total 100% because some treatment centres in New South Wales and
Tasmania cannot be classified along these lines.b Includes those prescribed in private clinics.c Includes those dispensed in private clinics.
Poly
gon
10
Pharmacotherapy drugs
The Australian Government has the financial responsibility for providing pharmaceutical services through the Pharmaceutical Benefits Scheme (PBS). Methadone and buprenor-phine are listed as Schedule 8 (controlled) drugs in Australia, meaning there are strict regulatory controls associated with their use. The Australian Government funds the cost of both drugs for treatment of opioid depend-ence supplied under the PBS. Both drugs are supplied through the PBS under the opiate dependence treatment program, provided for under section 100 of the National Health Act 1953. The federal government thus provides the drugs free of charge to the body respon-sible for dispensing (be it a public clinic, community pharmacy, prison or hospital).
Dispensing
In community pharmacies and private clinics, clients themselves pay the cost of dispensing. This dispensing fee varies across dispensing sites (see 3.3 on affordability for details re-garding dispensing fee variations).
In public clinics in New South Wales, Queens-land, the Northern Territory, South Australia and Western Australia, the State/Territory government covers the dispensing fee. In the other jurisdictions (Tasmania, Victoria and the Australian Capital Territory) the clients pay some proportion of the dispensing fee. Prison dispensing is funded by State/Territory governments.
Case management, counselling and psychosocial support
Case management and counselling provided within public clinics is funded by State/ Territory governments.
Since 2006, GPs can provide case manage-ment using Medicare items and rebates specific to assessment and management of patients with mental disorders. Drug use disorders are considered to be a mental disorder for the purpose of these items. There are two forms of case management in the Medicare system — the GP Mental Health Care Plan (introduced on 1 November 2006); or a referred psychia-trist assessment and management plan. Once a care plan is completed under either a GP Mental Health Care Plan or a referred psychia-trist assessment and management plan, the patient is eligible to be referred by their GP for allied mental health services. Pharmacotherapy clients can attend psychiatrists and be covered by the Medicare system; in 2006 the Australian Government extended the Medicare system to cover psychologists and some other allied health professionals in providing psychological therapy. Allied mental health services under this initiative include psychological assess-ment and therapy provided by eligible clini-cal psychologists, and focused psychological strategies provided by eligible psychologists, social workers and occupational therapists. The service providers must be registered with Medicare Australia. Clients are eligible for up to 12 individual and 12 group sessions per year. Clients in public clinics can receive addi-tional counselling support through these new Medicare arrangements. Clients are required to cover any gap between the Medicare benefit and the fee charged for psychological therapy.

Pharmacotherapy m
aintenance in Australia
11
Other points
State/Territory governments also subsidise service providers in some instances. For exam-ple, the New South Wales Government pays a once-only incentive payment to pharma-cies new to dispensing and pays pharmacies ongoing incentives for continuous clients.11 The Australian Capital Territory Government subsidises community pharmacies to the value of $15 per week per client.12 The Tasmanian Government also provides incentive payments to pharmacists (see 3.15).
2.2 Demand and unmet need for pharmacotherapy treatmentDemand for treatment is usually measured by the numbers of people wishing to be in treat-ment. It is comprised of those in treatment (met demand) plus those desirous of treat-ment, but not currently in treatment (unmet demand). Measurement of unmet demand is problematic. There is no systematic monitoring of waiting times in the pharmacotherapy sys-tem. In addition, people desirous of treatment can be deterred from seeking out treatment, perhaps because they know about the waiting times or because the service provision does not meet their needs. Hence they will not be counted within waiting lists.
The ‘need’ for treatment, on the other hand, is a broader concept than demand for treat-ment. It is possible to estimate the ‘need’ for treatment by examining the numbers of opioid-dependent people relative to the numbers of people in treatment (see, for
example, Cathcart, Patton, Hickman et al., 2007). In this instance the difference between the population prevalence and the numbers in treatment is a measure of ‘unmet need’. Such an analysis was conducted for Vic toria in 2001, with the finding that treatment pen-etration for opioid dependence in Victoria was between 35 per cent and 62 per cent of the population (Ritter, Berends, Clemens et al., 2003).
One problematic assumption underlying such calculations is that all opioid- dependent peo-ple will at some time benefit from, or require, pharmacotherapy maintenance. However, not all opioid- dependent people require phar-macotherapy treatment: some successfully reduce their drug use of their own accord; others obtain other forms of treatment, such as thera peutic communities. Another compli-cating factor is the chronic relapsing nature of drug use, which adds a degree of uncer-tainty to future need for treatment among the population of former opioid- dependent people who are currently abstinent.
Despite these substantial uncertainties and caveats, we can do a rough calcula-tion. Based on estimates of approximately 80 000 opioid- dependent, injecting drug-using Australians in 2005 (Razali, Thein, Bell et al., 2007) and 39 000 Australians in some form of pharmacotherapy maintenance in mid-2005 (Australian Institute of Health and Welfare, 2008), the treatment penetra-tion rate at that time was likely to be about 49 per cent. This means that the potential unmet demand could be as high as 41 000. Given that some members of the group for whom demand is potentially unmet would
11 Source: <http://beta.guild.org.au/nsw/content.asp?id=1081> accessed 12 September 2007.
12 Source: ACT Health, Alcohol and Other Drug Policy Unit (2005). Increasing Community Based Pharmacotherapy Places in the ACT: ACT Pharmacotherapy Program — issues and options (May 2005): <http://www.health.act.gov.au/c/health?a=sendfile&ft=p&fid=1157423833&sid=> accessed 12 September 2007.

Poly
gon
12
never seek treatment, regardless of the way in which the treatment was offered, and that some will prefer other treatments, this figure of 41 000 would be the uppermost limit. More reasonably, there may be between 10 000 and 30 000 individuals with unmet demand if it is assumed that about half of the not-in-treatment group would obtain treatment if available and in a form that they were happy with.
Importantly, any calculation of unmet de-mand at a national level may be meaning-less at a State or local level. Whereas some jurisdictions or locations may have suf-ficient treatment places available to meet demand, other locations — notably in rural and regional areas — experience substantial unmet demand.
This calculation of 10 000–30 000 people is crude and could not sensibly be used for planning purposes. However, the calculation usefully suggests that there is likely to be unmet demand for pharmacotherapy main-tenance treatment. In addition, it should be noted that there has been no real growth in treatment numbers in pharmacotherapy maintenance since 2004 (see Figure 1).
Australia lacks an approach for assessing the demand for pharmacotherapies. Such an approach should have the capacity to answer the following questions: How many treatment places are currently needed? How many will be needed into the future? What is the best mix between low-intervention, primary care treatment places and high-intervention, specialist treatment places? How is treatment-seeking behaviour affected by changes in the availability of opioids? For example, how many new treatment places are required to satisfy the changing profile of opioid use in our community? Is there a relationship between the supply of pharma-cotherapy treatment places and the demand for them? In particular, would an increase in supply and/or changes in the way that treatment is supplied encourage people into treatment and/or encourage people to stay in treatment for longer periods of time?
The questions outlined above are impor-tant because many of the issues identified in this project relate directly to both sup-ply and demand. For example, affordability and accessibility of programs are factors that reduce demand for treatment, while service models and workforce issues have an impact on the supply of treatment.
The issues
13
3. The issues3.1 What does the program aim to achieve?The National Pharmacotherapy Policy for People Dependent on Opioids states:
The broad goal of treatment for opioid dependence is to reduce the health, social and economic harms to individuals and the community arising from illicit opioid use. Pharmacotherapies for opioid dependence should be part of a comprehensive treat-ment program, with access to counselling and other ancillary services available to all individuals. The objectives of pharmaco-therapy treatment are to:
• bring to an end or significantly reduce an individual’s illicit opioid use;
• reduce the risk of overdose;
• reduce the transmission of blood borne diseases; and
• improve general health and social func-tioning, including a reduction in crime.
These objectives are achieved by engag-ing and retaining people dependent on opioids in treatment. (Commonwealth of Australia, 2007, p.7)
At a program level, the positive outcomes that the community may wish to see from the phar-macotherapy maintenance program include: reductions in drug use, including public inject-ing; improved public amenity; reductions in crime; and improvements in health, psychologi-cal wellbeing and social functioning.
The treatment outcome literature provides another perspective on the goals of treat-ment. Treatment outcome research generally focuses on:
• reduction in harmful heroin use
• cessation of heroin use
• reduction or cessation of other drug use
• improvement in psychological wellbeing
• reduction in criminal activity
• reduction in risk of blood-borne virus con-traction
• improvement in physical health
• improvement in social functioning
• employment and productive use of time.
(See, for example, the National Evaluation of Opioid Dependence trials (Mattick, Digiusto, Doran et al., 2001) and the Australian Treat-ment Outcome Study (Teesson, Ross, Darke et al., 2006).)
From the client perspective, the goals of treat-ment are heterogeneous. For some, cessation of drug use may be a primary goal; for others, it may be temporary relief from the drug-using lifestyle. Thus, there is no agreed definition of ‘treatment success’ among clients and across stakeholders. Even the term ‘abstinence’ can be contested. There is no shared understand-ing of the meaning of ‘abstinence’. Does it stand for abstinence from heroin, abstinence from all illicit drugs, abstinence from illicit drugs plus harmful licit drug use, or absti-nence from methadone/ buprenorphine? Most stakeholders to the pharmacotherapy program would agree that abstinence from methadone/buprenorphine is not the primary goal — given addiction is a chronic relapsing condition, it may require long-term maintenance treatment.
Poly
gon
14
Questions about the aims of the overall pro-gram — whether it is long-term maintenance, cessation of illicit drug use temporarily, or cessation of all opioids, whether prescribed or not — remain contentious. Given the hetero-geneity of client presentations, their own goals and expectations, and practitioner expertise in tailoring the program to best meet the client’s needs, focusing on individual client treatment goals will produce the most effective outcomes at the individual level and hence for the Australian program as a whole.
There is some tension between minimising the harms to individuals and minimising the harms to the community. This is usually articulated as a tension between intensive high- quality care for individuals and a low-threshold public health pharmacotherapy program. In the case
of the former, the program places great empha-sis upon individual goal attainment for clients within the program and ensures that each cli-ent is allocated sufficient resources to allow access to a variety of different support services, including counselling, employment retraining, housing support, financial counselling, and so on. In general, individually focused programs are more resource-intensive. At the other end of the spectrum is the low- threshold public health model. This is largely reliant on medication as the primary mechanism of behaviour change, and encourages as many clients as possible to enter the program, irrespective of the level of individual motivation or willingness to engage in the variety of support services. In general, this latter public health model sees many more people in the treatment system, but with less chance of individual goal attainment.
Summary of issue: program goals
• There is tension between community expectations and the reality of heroin depend-ence as a chronic relapsing condition.
• A practitioner’s views about treatment goals may differ from a client’s own views.
• There is broad agreement that the goals of the Australian pharmacotherapy mainte-nance treatment system are:
• to reduce or cease harmful heroin use
• to improve physical health
• to reduce risk for infectious diseases
• to improve psychological, social and occupational functioning, including a reduc-tion in crime.
• Given significant heterogeneity in the treatment population, best outcomes are likely to be achieved by tailoring treatment goals to the individual client, rather than assum-ing abstinence (or reduced use) for everybody.
• A distinction is sometimes drawn between individually enhanced programs and public health low-threshold programs because these reflect different goals for the program.
The issues
15
The individually enhanced and the public health (low-threshold) models of pharmaco-therapy maintenance are not mutually exclu-sive.13 But the two views of pharmacotherapy maintenance can stand in stark contrast to each other, especially when placed against the program goals: abstinence versus reduc-tion of harmful use.
3.2 Service delivery modelsThe Australian pharmacotherapy maintenance service system is built on a premise of two primary models of service provision: public clinics and primary health care service provi-sion (‘office-based’ treatment as it is known in the United States). While every service has unique features and is not easily classified into one of these two categories, the fol-lowing features distinguish the two models of service delivery:
Public clinics
• services usually free or subsidised
• located within a specialist alcohol and drug centre
• a putative role to treat clients with more complex presentations and comorbidities
• provision of psychosocial support is usu-ally enhanced/available
• addictions-based medical care only
Primary health care services
• located in GP practices14
• comprehensive medical care available
• access to psychosocial support services lim-ited to the extent to which the GP is well connected with surrounding services.
Internationally these two models of service provision are acknowledged: specialist clinic-based pharmacotherapy maintenance; and office-based or primary care pharmacother-apy maintenance. There is a growing body of research that examines these two models. Wittchen, Apelt, Soyka et al. (2008) com-pared outcomes (retention and drug use) in primary care settings versus specialist centres and found better outcomes in the primary care settings. A number of other researchers have documented equivalent clinical out-comes between specialist and primary care settings (see, for example, Keen, Rowse, Mathers et al., 2000; Mintzer et al., 2007; Vignau & Brunelle, 1998).
The advantages of the primary health care setting for pharmacotherapy maintenance are the potential to reduce stigma and to provide more holistic medical services. Gunderson and Fiellin (2008) argue that, given the het-erogeneous nature of the opioid- dependent population, there is no one model that will suit all clients, and having different models available is likely to be more effective. Thus it would appear that there is no net advantage to either model based on international re-search. In this context, we turn to examining how the models can be best implemented.
13 In the next section on treatment models, specialist clinics are contrasted with primary health care settings. Sometimes specialist centres are aligned with the individually enhanced model of care, and the primary care settings associated with the low-threshold public health model. In Australia, this is not necessarily the case.
14 Some are located in private clinics, which operate only in New South Wales. The provision of psychosocial services is likely to be variable within the private clinic system.

Poly
gon
16
There are a number of issues associated with two models of care: the relationship between the care models; the relative number of treat-ment places ‘allocated’ to the two service delivery models; coordination between the systems; and issues particular to each model. We deal with relationships between the care systems first.
Relationships between the systems of care
There are three ways in which the two sys-tems of care can be related. They can:
i. exist independently of each other
ii. exist independently but more explicitly treat different groups and/or have explicit ‘streaming’ processes to determine where clients should be best placed
iii. be connected through referral pathways and shared care models.
In relation to the first possibility, there does not seem to be any advantage to two models of care existing completely independently, with the likely result being a fractured serv-ice system.
The second option — treating different pop-ulation groups — has potential merit. Indeed ‘streaming’ was described in early federal and State policy documents, with descrip-tions of high- intervention streams and low- intervention streams, largely corresponding to the specialist clinic and primary health care modalities (see also earlier discussion under treatment goals). However, this lan-guage is no longer used and the current
national pharmacotherapy policy does not refer to streaming (Commonwealth of Aus-tralia, 2007). While the streaming of clients into specialist versus primary health care set-tings makes sense, there is no evidence base to support it. Indeed, the research suggests that it may not be required (Wittchen et al., 2008).
The third possibility — referral systems and shared care models — is implemented in vari-ous ways in Australia. Referring clients from public clinics to GPs/private clinics is analo-gous to the HIV medicine model where initial assessment takes place at a specialist hos-pital, and ongoing management is under-taken by accredited GPs. The advantage of this approach is that it mirrors other areas of medicine. In addition, it may encourage greater GP participation in the program.
Treatment places — relative allocations between service types
It is not possible to determine the optimal allocation of treatment places to the two models within any one area or jurisdiction. Currently there is a unique treatment system in each jurisdiction. In some States there is a strong reliance upon the general practice model (primary health care providers). In oth-ers, the private model plays a significant role. All jurisdictions have public clinics, although concern was expressed by respondents to the issues paper that public clinics appear to have reduced capacity to respond to the more seri-ous and complex presentations.

The issues
17
Other concerns
Respondents to the issues paper expressed concern about the fragility and vulnerability of the system. For example, in some places a small number of GPs carry large caseloads. If these GPs were to retire or discontinue treat-ing opioid pharmacotherapy clients, there could be a potential crisis in the system.
Consideration of the models of care should not be seen in isolation from many of the other issues identified in this paper. For example, there is significant disparity between service models in the fees charged to clients — most simply whether there is a dispensing fee or not. Access to counselling and psychologi-cal therapies is likely to vary between the service models.15
So far, we have discussed the different models of care as a primary distinguish-ing feature of the system. This reflects the prevalent view that the model of care (spe-cialist clinic versus primary health setting) is the critical variable. As we note above, however, the research does not show great differentiation between the models on clini-cal outcomes. In a study of client outcomes in public and private clinics in New South Wales, Bell, Ward, Mattick et al. (1995) found that differences in outcomes (as measured by retention in treatment and heroin use) between clinics within each sector were greater than differences between the sec-tors. Having controlled for dosing level, the authors concluded that: ‘Aspects of staff– client interaction are important determinants of outcome, but the availability of coun-selling, at least as delivered in the public clinics, was not one of those aspects. Rather, organizational and logistic factors within
the clinics appeared to be the major factors which contributed to differential treatment effectiveness’ (Bell et al., 1995, p.2).
Some research has detected systematic differ-ences in client outcomes between individual clinics. The National Treatment Outcome Research Study (NTORS) showed significant inter-agency variation in outcome, as meas-ured by heroin use (Gossop, Marsden & Stew-art, 1998). On the basis of average heroin use among clients, agencies were divided into four groups, with the top quartile achieving heroin use reduction levels that were twice that of programs in the bottom quartile. In a major study of seven public methadone programs in Sydney, Taplin (2000) found that clinical practices affected treatment outcomes, meas-ured by retention in treatment, over and above client characteristics, and dose level. The per-ceived helpfulness of the counselling received had a positive impact on retention while the extent to which the client was disciplined by program staff and the number of urine sam-ples required each week had a negative impact on retention. Taplin’s findings on retention and staff attitudes towards abstinence support those of an earlier Australian study (Caplehorn, Lumley, Irwig & Saunders, 1998).
Another large body of research and practice examining the impact of agency characteris-tics on treatment outcomes comes from the Texas Institute of Behavioral Research at Texas Christian University (http://www.ibr.tcu.edu). Their focus has been on the organisational climate of a treatment service (and the rela-tionship between climate and motivation to change practice models). Organisational climate is a multi-dimensional construct that includes: motivation; resources; staff attributes; and climate. Measures of client
15 We assume significant variations in access to counselling services based on anecdotal feedback, but have no data that can inform our view either way.

Poly
gon
18engagement in treatment (rapport, satisfac-tion and participation) were shown to be higher in programs with more positive staff ratings of organisational climate (Broome, Flynn, Knight & Simpson, 2007; Greener, Joe, Simpson et al., 2007).
In conclusion, there is sufficient evidence that treatment outcomes vary between clinics, but are not systematically related to medi-cation regime or client characteristics. The therapeutic milieu, staff attitudes, underlying beliefs about the goals of pharmacotherapy maintenance treatment, and the organisa-tional climate all appear to have a significant impact on individual client outcomes.
3.3 Affordability for the clientProbably the most talked about issue for Australian pharmacotherapy programs is that of client dosing fees. The issue is consist-ently raised by service providers, consumers and policy makers as a major area of con-cern (Muhleisen, Clark, Teo & Brogan, 2005; ANCD Alcohol and Drug Agency Forum16). In health care generally, user fees are con-sidered to be
the most regressive form of healthcare financing available; they contribute to the unaffordable cost burdens imposed on poor households; and they represent one facet of the social exclusion expe-rienced by these households. (Gilson & McIntyre, 2005)
While the cost of methadone and buprenor-phine medication is funded by the Australian Government, the cost associated with dis-pensing the drug is not. In public-funded
Summary of issue: treatment model types and service differences
• There are two predominant models of pharmacotherapy service provision in Australia: public clinics; and primary health care/GP services.
• In the context of these two models, it is useful to explore the implications of the rela-tive mix between the models; the risks and vulnerabilities with each model; the resource implications for government; and the coordination from a client perspective between these systems of care.
• A key issue is the extent to which there are differences in outcome according to service setting: public clinic / private clinic / GP / pharmacy / clinic dispensing. The existing international research would suggest that there are no systematic outcome differences between the different models of care.
• Over and above any differences in service delivery model, there are more fundamental differences between individual clinics/programs that result in different clinical outcomes.
• The therapeutic milieu, relationships between clients and the practitioners, staff atti-tudes and organisational climate all have a significant impact on treatment outcomes.
16 <http://www.ancd.org.au/publications/forums/forum7.htm> accessed 15 September 2007.

The issues
19
clinics, the cost of dispensing the medica-tion is generally paid for by the jurisdiction government, but sometimes by the client (Tasmania, Victoria and the Australian Cap-ital Territory). All clients who receive their medication at a private clinic or at a com-munity pharmacy pay a dispensing fee. Based on official figures for the numbers of clients dispensed in public clinics, private clinics and pharmacies in 2007 (Australian Institute of Health and Welfare, 2008), we estimate that close to 80 per cent of pharmacotherapy cli-ents pay for dispensing.
There are significant differences in the level of dispensing fees paid by clients both between and within jurisdictions. For example, Muh-leisen et al. (2005) noted weekly fees ranging from $9 to $53 in New South Wales, and from $15 to $30 in Victoria. A number of pharma-cies charge the same weekly fees, regardless of the number of take-away doses. Clients who do not receive take-away doses, regardless of whether they are in receipt of methadone or buprenorphine, could be paying up to $70 per week (Winstock, Lea & Ritter, 2007). There are also a variety of exemptions and special arrangements: for example, free dispensing for juveniles in Victoria; newly released prisoners receive dispensing fee relief in a number of jurisdictions; the Northern Territory Govern-ment pays the dispensing fees for mothers and pregnant women; and South Australia provides the first six weeks of treatment in public clinics free of charge.
A comparison between the fees and the ac-tual costs incurred by pharmacists would be valuable. In a study of a small number of pharmacies, the Pharmacy Guild recently calculated the average cost of dispensing a daily dose as $3.27 ($1.61–$7.37) for metha-done, based on ten pharmacies; and $3.29
($1.03–$8.18) for buprenorphine, based on eight pharmacies (Pharmacy Guild of Aus-tralia, 2007). Eight of the ten pharmacies were making some positive financial return with the average annual return per pharmacy being $15 424 (the median was $16 850).
An obvious concern with dispensing fees is that clients simply cannot afford them and, as such, they present a barrier to treatment. The majority of clients are reliant on income support payments. Lintzeris, Koutroulis, Odg-ers et al. (1996) estimated that in the mid-1990s approximately two-thirds of Victorian methadone clients were unemployed. To ex-emplify the impost of dispensing fees on income support recipients, consider that the current maximum rate of income sup-port for a single person of at least 21 years of age is the Disability Support Pension of $537.70 per fortnight or $268.85 per week.17 A weekly dispensing fee of $70 represents one-third of this income and allows only $199 per week for all other expenses, in-cluding accommodation, food etc.
A recent study of income support recipi-ents in pharmacotherapy treatment in Mel-bourne highlights the difficulties that clients face in meeting their dispensing fees (Rowe, 2008). Clients regard their dispensing fees as a priority. Rather than not pay these fees, they would sooner go without food or go to emergency organisations for food and ac-commodation, commit crimes and/or obtain loans from Centrelink (Rowe, 2008). For cli-ents with families these hardships are often also borne by children. Even so, it is com-mon for this group of clients to acquire debts at pharmacies. The implications of acquir-ing a debt depend on the pharmacist. Rowe (2008) found that some pharmacies refuse to continue dispensing, for a day or so, or
17 <http://www.centrelink.gov.au/internet/internet.nsf/payments/pay_how_dsp.htm> accessed 20 September 2007.
Poly
gon
20
else cease providing medication to that cli-ent altogether. It is difficult to transfer to a new pharmacist because the new pharma-cist requires a reference from the previous pharmacist. Some pharmacists clear the debt on the condition that the client debits his/her dispensing fees directly from a bank ac-count. Others require payment of the debt in instalments, often again as a direct debit.
Another study found that some pharmacies charge penalty fees for prolonged failure to pay (Pharmacy Guild of Australia, 2007). Pharmacists estimated that approximately 45 per cent of all pharmacotherapy treatment terminations were due to financial difficulties (Lintzeris et al., 1996). In New South Wales, at least one of the public clinics (the Lang-ton Centre) has a number of respite places for people on temporary transfer (only one month) from the private system if they have financial problems. According to respondents to the issues paper, the lack of subsidised dispensing in jurisdictions without a public treatment system — most notably Victoria — is problematic.
Pharmacists who responded to the issues paper articulated the need for clear guide-lines, from perhaps the Pharmacy Guild, as to how to manage the dispensing payment process so as to minimise pharmacy debt. There was a suggestion, from both inside and outside the pharmacy sector, that the accumulation of debt is being facilitated, to some extent, by pharmacy practices.
A second concern with dispensing fees arises from equity issues. Two key economic princi-ples regarding the consequences for clients in relation to the costs they face are horizontal equity and vertical equity. Although these terms strictly relate to tax contributions, they also relate to the costs faced by clients.
In this situation, horizontal equity refers to the principle that clients with the comparable ability to pay should face the same costs. The principle of vertical equity, on the other hand, maintains that those who can pay more should pay more. Just as the rate of taxation increases as income increases, the cost of pharmacotherapy should increase with the client’s capacity to pay. Currently the system does not attempt to shield clients on low incomes from the financial impost of dispens-ing fees. Ability to pay seems to be largely ignored as an issue, since there is no means testing. Even if we were to assume that each client had a similar ability to pay, there is no State or national agreement on appropriate fee levels. Similar dispenser types charge dif-ferently across jurisdictions, as they also do within jurisdictions. There is no consistency of pricing within the pharmacy sector, nor between different dispenser types. There is an argument that price-fixing is inappropriate in the private sector, but it is difficult to envisage pharmacotherapy dispensing as a free market service. In a free market clients could supposedly seek out dispensers that charge fees matching their financial situation. In reality, clients have little opportunity and sometimes ability to do this.
The fee structure, rather than fees themselves, can hinder the most appropriate match of client to service. Public clinics tend to pro-vide the more expensive specialist support needed by less stable clients. Once stabilised, the client may not need such intensive sup-port. However, if the choice is between free dispensing in the public clinic and fee-for-service dispensing in community pharmacies, there is a financial incentive for the client to remain with the public clinic. With limited places in public clinics this may restrict new entrants to public clinics.
The issues
21
There are also inherent inequities in the way dispensing fees are structured. For example, in some private clinics in New South Wales the fees for take-away doses of buprenorphine- naloxone are the same as for a dispensed dose (i.e. same fee for daily dosing and weekly dispensing).
Furthermore, there is inequity compared with other drug treatments. The appropriate com-parator is long-term treatments for opioid dependence (such as long-term counselling or rehabilitation). Long-term rehabilitation (such as a therapeutic community) generally does not incur client fees other than some accommodation costs. Long-term counsel-ling is not associated with client fees in the public system.
Other fees
(a) Private clinics in New South Wales charge a $20 administration fee to enter treatment. Some Victorian GPs charge a commencement fee of up to $100, as these GPs consider that Medicare does not adequately reimburse the time involved in inducting a client on methadone. Lintzeris et al. (1996) reported that GPs on average spent approximately one hour assessing and formulating a treatment plan with the client, completing the neces-sary paperwork and organising prescriptions. Of this, approximately half was non- client contact time, which was not reimbursed by Medicare.
(b) There is evidence that some clients pay to see a medical practitioner for services asso-ciated with pharmacotherapy treatment. In March 2005 ACT Health conducted a phone survey of GP practices to ascertain the extent
and nature of bulk billing. The results of that survey are not publicly available but ‘there is thought to be considerable diversity in the amount being paid by [pharmacotherapy] clients for GP consultations’ (ACT Health, Alcohol and Other Drug Policy Unit, 2005: 6). The authors then go on to speculate about the amount that clients pay. In the Aus-tralian Capital Territory a stable methadone client usually consults a GP once every three months for a methadone script. Clients could pay between $7 and $23.50 for a standard consultation.
(c) The costs of ancillary medications, such as antidepressants or other medication for mental health disorders required by this cli-ent group with significant comorbidities, are not necessarily covered and reflect a cost to the client.
(d) Counselling services may incur additional fees to clients. GP-based programs and many public clinic programs have waiting lists for counselling services. The introduction of the GP Mental Health Care Plan in 2006 may go some way towards redressing this.
Other costs to clients
We have focused on dosing fees as the most significant issue, but additional costs should also be considered, such as travel costs. Fried-mann, Lemon & Stein (2001) found some evidence that assistance with transportation improved treatment retention.
Regardless of the financial burden of service costs on low-income clients and the ‘fair-ness’ or otherwise of the current arrange-ments, the fees may have implications for client behaviour and outcomes.

Poly
gon
22
Impact of dispensing fees on access and retention
Despite the above commentary about the impact of fees and reports from clients and pharmacists that fees are associated with treatment drop-out, there is surprisingly little research that quantifies the impact of fees on clients. Research by Bammer, Battisson, Ward and Wilson (2000) is often cited as a piece of Australian research supporting the position that fees reduce treatment retention. However, this does not seem to be the case. The authors followed a major expansion in treatment places in the Australian Capital Territory. Simultaneously, dispensing fees were introduced. In the ensuing two years the authors found no evidence of a fall in the number of new admissions, or a decrease in treatment retention.
The evidence base for the extent of the impact of fees on retention and entry to treatment derives predominantly from the United States although, as outlined below, the evidence is not persuasive. Nor does it necessarily apply to the Australian situation. Our critical appraisal leads us to believe that there is some evidence that fees discourage entry to treatment, but no substantive evidence that fees encourage clients to leave treatment earlier than they otherwise would.
Des Jarlais, Paone, Friedman et al. (1995) reported that during the mid-1970s one-year retention rates in publicly supported metha-done programs (at low or no cost to clients) in New York were almost 60 per cent com-pared with retention rates in fee-for-service treatment of less than 40 per cent. But it is not clear that the analysis controlled for dif-ferences in the types of clients that entered the two programs.
Research cited in Maddux, Prihoda and Des-mond (1994) suggests that treatment fees impair retention in methadone treatment. Maddux et al. (1994) conducted a con trolled clinical trial which randomly assigned sub-jects at the time of admission to metha-done maintenance to a fee ($2.50 per day) or no-fee status. Multiple regression survival analysis of the hazard (or likelihood) of ter-mination of treatment suggested that fee payment increased the likelihood of treat-ment cessation, although the relationship be-tween fee status and treatment cessation was of borderline significance (at 10 per cent).
Another study considered the impact of fees on a group of street-recruited drug injectors who may not have contemplated treatment. All of the participants were told that the cus-tomary $US40 fee to enter treatment was waived and half were randomly selected to receive a coupon for 90 days of free treat-ment. Thirty per cent of the group entered treatment. Members of the group with the coupon were substantially more likely to enter treatment than others, suggesting that treatment uptake is sensitive to costs faced by clients (Booth, Corsi & Mikulich, 2003). The researchers claimed that the free cou-pon encouraged longer retention, although the analysis was cursory, based on the find-ing that, after 90 days, those in treatment were more likely to have a free coupon than those who had left treatment (75 per cent versus 43 per cent) (Booth, Corsi & Mikulich-Gilbertson, 2004).
The issues
23
Colameco, Armando and Trotz (2005) trace the experiences of 35 clients of an American fam-ily practice centre for one year following com-mencement on buprenorphine-naloxone. The basis for their argument that client fees were associated with poorer retention rates was the finding that none of the 22 clients retained in the program had paid for their drug, while ten of the thirteen clients lost to follow-up or therapeutically discharged had paid. The cost for those who paid ranged from $300 to $500 per month, which is substantially higher than Australian fees. Furthermore the clients who did not pay were subsidised by their families or medical insurance. Their heightened ability to pay may have been associated with a higher level of social functioning, which is a strong predictor of treatment outcome.
There are some who argue that there may be possible benefits attached to fees. Fees may enhance treatment compliance by increas-ing the perceived value of the service to the client.18
In summary, there appears to be some interna-tional research evidence supporting the view that fees discourage entry to treatment, but little evidence to support the view that fees have an impact on retention. The absence of Australian research evidence on the impact of fees on entry and retention does not negate the equity and hardship arguments noted earlier. The Australian Government, in concert with the Pharmacy Guild of Australia,
recently funded the National Drug and Alco-hol Research Centre and Price Waterhouse Coopers to explore the repercussions of dis-pensing fees for treatment retention, health outcomes, missed doses and patient satisfac-tion, among other things. From November 2008, approximately 100 community pharma-cies, which dispense pharmacotherapies, will be recruited from all jurisdictions, except the Australian Capital Territory. Each pharmacy will be charged with recruiting pharmaco-therapy clients to participate in a randomised controlled trial lasting six months. Roughly 700 clients will be recruited. Half the clients will continue paying their usual dispensing fee while the remaining clients will pay half their dispensing fee.
For a significant number of clients dis-pensing fees present a substantial financial burden. This situation, when compared to other chronic diseases (such as depression, diabetes and high blood pressure), is ineq-uitable. A commonly discussed solution is that the government should subsidise dis-pensing of pharmacotherapy medications, in the same way that the Australian Gov-ernment subsidises almost all PBS-registered medications. This would make a substantial difference, but does not deal with the other costs to patients that have gradually crept into the system, such as application fees to enter treatment.
18 Respondents to the issues paper made this point.

Poly
gon
24
Potential solution
One solution is for dispensing of pharma-cotherapy drugs to be included in the PBS. Importantly, for this to happen, the medica-tions do not necessarily have to be moved from section 100 to section 85 of the National Health Act 1953. Dispensing of some drugs within section 100 is being subsidised (e.g. highly specialised drugs).19 The PBS system was designed to satisfy both equity principles mentioned earlier. It recognises capacity to pay and acknowledges that the chronically ill should receive greater assistance. Methadone and buprenorphine for opioid substance abuse have been listed as PBS drugs. As such, they are judged to be necessary and cost-effective medicines.
According to the description of the PBS sys-tem in Brown, Abello and Harding (2006), there are two key components to the federal subsidy: the patient co-payment and the safety net. The co-payment is the patient’s contribution toward the cost of the medicine and dispensing of the medicine for each pre-scription, and the contribution depends on ability to pay. At the time of writing, the co-payment was $5 for concessional20 patients and up to $31.30 for non- concessional patients.21 The federal government cov-ers the balance between the co- payment and the listed price. Some income support recipients, roughly corresponding to conces-sional patients, also receive a pharmaceutical
allowance. The pharmaceutical allowance is a non-taxable payment of $5.80 a fortnight for single people and $2.90 a fortnight for each eligible member of a couple ($5.80 combined), and is included in the income support payment.22 The safety net protects individuals and families from having to make large outlays for all PBS medicines over a calendar year. In other words, it protects those whose medical condition warrants regular PBS-approved medicines. Thresholds are set on the annual outlays on PBS medicines. The threshold depends on ability to pay, with a lower threshold set for concessional patients (Brown et al., 2006). Once the threshold is reached, the concessional patients no longer pay for PBS medicines for the rest of the year while non-concessional patients pay the concessional price. The threshold for concessional patients is $290 and for other patients is $1141.80.23
A mechanism already exists for the federal government to determine the financial return to pharmacies for dispensing. Currently the Pharmaceutical Benefits Remunera-tion Tribunal implements agreements on the determination of the federal price of PBS medicines between the Minister of Health and Ageing and the Pharmacy Guild of Australia. The current agreement, the Fourth Community Pharmacy Agreement, allows for the cost of handling and stor-age of medicines by the pharmacy and the
19 <http://www.pbs.gov.au/html/healthpro/browseby/section100?subbook=HS> accessed 1 September 2008.
20 Concessional patients include those on Department of Veterans Affairs pensions, social security pensions and some other low-income groups.
21 <http://www.pbs.gov.au/html/consumer/pbs/about> accessed 26 May 2008.
22 <http://www.centrelink.gov.au/internet/internet.nsf/payments/pay_how_phar.htm> accessed 26 May 2008.
23 <http://www.medicareaustralia.gov.au/public/services/msn/pbs.jsp#what_to_do> accessed 26 May 2008.
The issues
25
pharmacist’s specialist skills in dispensing the medicines, both costs particularly associated with dispensing restricted medicines such as methadone and buprenorphine.24
This is not to recommend that the Aus-tralian Government per se subsidise the cost of dispensing. It is merely to illustrate that an adequate mechanism exists, a mechanism designed to deliver necessary medication on
an equitable basis. The principles of federal pricing of PBS drugs could be applied by the State/Territory governments. For example, medications funded under the PBS Highly Specialised Drugs Program are subsidised by the federal government only for commu-nity patients. The cost of medications for inpatients remains the responsibility of the treating hospital (i.e. State governments).25
Summary of the issue: affordability
• Clients incur costs associated with: dispensing fees; other fees (payment for GP services); and other costs (such as travel costs).
• For the majority of patients the most significant cost tends to be dispensing fees. We esti-mate that close to 80 per cent of Australian pharmacotherapy clients pay dispensing fees.
• Clients can experience payment problems and this can impact on future access (debts, black lists) and on local welfare services (which pay the dispensing fee either directly or indirectly by covering for food/accommodation).
• There is no means testing or State/federal agreement on appropriate fee levels per dos-ing frequency.
• The fee structure can hinder the most appropriate matching of the client to the service (e.g. there are financial incentives for clients to remain in free public clinics even though they do not need the high level of specialist support offered by the public clinic).
• There has been much focus on the negative impact of dispensing fees, including the impact on retention in treatment, and the financial burden to clients.
• The academic literature suggests that fees discourage treatment uptake but does not unambiguously show a strong relationship between fees and retention in treatment.
• Equity arguments must also be taken into consideration: equity vis-à-vis client fees for dispensing of other medications; equity vis-à-vis costs of other treatments (e.g. long-term counselling).
• The inequities associated with dispensing fees would be significantly ameliorated with the introduction of a system consistent with current federal funding of PBS medications.
• Alternatively, if such a system were not introduced, efforts could be directed towards ensuring that clients in financial need are given access to free dispensing.
24 <http://www.health.gov.au/internet/main/publishing.nsf/Content/pharmacy-4cpa2> accessed 26 May 2008.
25 <http://www.health.vic.gov.au/hsdp/app2d.htm> accessed 1 September 2008.
Poly
gon
26
3.4 Accessibility of the programWhereas affordability focuses on ‘ability to pay’ issues, accessibility explores the ability to access treatment, assuming the potential client has the wherewithal to pay for treat-ment. Access to treatment includes consid-eration of:
• availability of treatment places (entry sys-tems, waiting times, caps on client num-bers, numbers of practitioners), and
• location of treatment (prescribing and dispensing).
Access to pharmacotherapy programs for new clients across Australia varies, although the consultation process revealed concerns about delays in accessing treatment in some areas in most jurisdictions.
The process of entering treatment varied across jurisdictions. Some jurisdictions have a relatively open access system, in which new clients may arrange appointments with pre-scribers as required. Other jurisdictions have a centralised intake system, so that new clients have their first consultation within a public clinic. This requirement to commence treat-ment through the public/specialist system can slow down or prevent access. However, the balance between service accessibility and quality assurance is a delicate one. We found no evidence to determine which system of access is the most effective and safest for the client.
Data regarding waiting times are not pub-licly available. We sourced information about waiting times from respondents to the issues paper, both consumers and practitioners. Con-sumers around Australia described long delays
in gaining access to the program. Waiting lists of up to six months were reported by practi-tioners. Apparently, in one jurisdiction entry is allowed only when an existing client leaves the program. We were advised that entry to treatment has been hampered in situations where there are insufficient prescribers and long delays to access treatment. At the same time, we were also informed of delayed ac-cess to a dispensing point.
The extent of waiting times varied both be-tween jurisdictions and within jurisdictions. Indeed there appears to be marked geograph-ical variation within jurisdictions. Clients re-ported travelling substantial distances for dispensing because there were no available dispensing locations nearby. At the same time we were advised that community pharmacies in other locations had excess capacity.
There does seem to be some reluctance to acknowledge the extent of restricted access as measured by waiting times. At least two jurisdictions questioned the evidence for waiting times. We have reported what we have been told in relation to delays, problem-atic access and waiting lists but we cannot independently verify all the information. We believe that the message was fairly consist-ent across Australia — demand for treatment outstrips supply.
There are a range of possible reasons for the inability of programs to meet current demand: insufficient number of treatment places; limits on clients per prescriber and/or dispenser; inefficient service provision; a rela-tive allocation of places in specialist services versus generalist service modalities that does not match demand; and insufficient work-force. These factors are all interconnected.

The issues
27
Insufficient number of treatment places
An insufficient number of treatment places is the most obvious reason for the inability of treatment programs to meet demand. This in turn is linked to the current capacity of pro-grams, as limited by the resources available to the services; and the available workforce. To what extent are programs operating at full capacity? Do we find public programs at capacity while private programs are not? Could programs be run more efficiently? (See 3.5.) Or will improvements in efficiency result only in lower levels of care?
The delicate balance between greater through- put versus quality of care is one that needs careful consideration and recogni-tion that the balance or trade-off will result in different public health and treatment out-comes. A highly accessible, low- intervention treatment model will enable large numbers of clients to receive methadone or buprenor-phine medication, and will probably be asso-ciated with significant public health benefits (e.g. reducing overdoses and rates of blood-borne virus transmission). However, such a model may also be associated with poorer in-dividual client outcomes and with more ad-verse events (e.g. diversion of medication26). A restricted high-intervention system is likely to result in better quality services for the few who can access treatment, but result in larger numbers of under-treated opioid users, and increased frequency of opioid misuse.
This is not a question of which is inherently better — it is more about the desired outcome. The introduction of buprenorphine in France exemplifies the highly accessible model. Access to buprenorphine treatment was putatively associated with reductions in heroin over-doses (Auriacombe, Fatseas, Dubernet et al., 2004). By contrast, in the United States (pre buprenorphine-naloxone), access was limited and hence was highly problematic. There is a trade-off between accessibility (through low-threshold programs with good public health outcomes at a population level) and quality (through high-intervention restricted programs with better individual client outcomes). (This issue was earlier discussed under 3.1, goals of the program.)27 There has been limited research on the trade-offs. There is more to be learned from international comparisons that pay attention to political, cultural and societal differences.
Limits on clients
Jurisdiction-imposed ‘caps’ on the number of clients treated by individual prescribers and pharmacists can limit the availability of treat-ment places if there are insufficient service providers in a particular geographic area. Caps are perhaps a crude way of ensuring quality control. The New South Wales Department of Health recently loosened its 50-client cap on pharmacies so that clients who are dispensed once per week are no longer counted in the 50-client cap. The extent to which a relaxing of the ‘caps’ on client numbers would be sufficient to improve unmet demand is not
26 There is an argument that low-threshold programs may actually reduce diversion because clients can gain access to treatment readily and frequently.
27 It is important to note that the low-threshold versus high-threshold characterisation should not be confused with the primary health care/office-based treatment versus specialist clinic characterisation. There is evidence to support equal if not superior outcomes in the primary care setting model relative to the specialist clinic model (Wittchen et al., 2008).

Poly
gon
28
known. In addition, some practitioners place their own ‘caps’ on client numbers. Hence any change in jurisdictional policy may have limited impact.
Another inherent limitation on supply of treat-ment places is the relative allocation between specialist services (public clinics), GP-based services and, in some instances, private clinics. Clients in jurisdictions with a predominantly generalist-based system (i.e. GP-based) tend to experience shorter waiting times. The special-ist clinics can become ‘silted up’ with clients and there is little incentive for clients to leave because of the dispensing fees charged by community pharmacies and private clinics.
Access to dispensing locations
The accessibility of dispensing locations is also a potential limitation on treatment places. Dispensing locations include public clinics, local pharmacies, hospitals and private clinics. The extent to which dispensing locations are a barrier seems to depend on local conditions, jurisdictional arrangements and whether the client is located in a rural, regional or urban area. Use of public transport to visit a dis-pensing location can take considerable time and money. Another identified issue is the opening hours of the dispensing services. Some of the public specialist services have restricted dosing hours during the day (e.g. 10am to noon). Under some jurisdictional guidelines, it is recommended that all new clients commence treatment in such clinics. Their restricted dispensing hours may impair accessibility for some clients, such as those in employment.
This issue is also confounded by the client dispensing fees — in some locations clients do not have a choice of dispenser, resulting in financial hardship if they are in an area with high dispensing fees.
Number of service providers
Finally, accessibility is fundamentally lim-ited by the numbers of service providers, which in turn relates to the workforce and uptake of pharmacotherapy programs by new practitioners (addressed in 3.15). One way to expand accessibility of the program is to concentrate on building services within the existing primary care setting (i.e. through GPs). The extent to which this strategy has been implemented across Australia is unclear. Certainly Western Australia, Victoria and New South Wales have invested significant effort in growing the primary care practitioner base for the program.28
The traditional view of pharmacotherapy maintenance is that it requires medical doc-tors trained to prescribe opioids. However, other models could be considered. For exam-ple, arguably most of the treatment could be coordinated by trained health professionals (e.g. nurses). The nurse practitioner models are worth exploring in this regard, particu-larly in light of the recent Cochrane Review indicating that appropriately trained nurses can provide a quality of patient care equiv-alent to that provided by doctors (Laurant, Reeves, Hermens et al., 2006).
28 The potential to increase prescriber numbers is also linked to the establishment of the Addiction Speciality, as discussed in 3.15.
The issues
293.5 EfficiencyWhile there is ample evidence that pharma-cotherapy maintenance treatment is a highly cost-effective intervention for opioid depen-dence, two equally potent questions arise in relation to the resources allocated to the pharmacotherapy system: Are the resources sufficient enough; and is the usage of the resources structured in ways that promote the most gains to society? As Cartwright and Solano (2003, p.248) ask, in relation to the entire United States drug treatment system, ‘Are there ways in which the drug treatment programs can be reorganised to achieve better results with the same amount of expenditure?’
Is the overall level of funding sufficient?
Unlike other health conditions, neither the need nor the demand for pharmacotherapy treatment has been estimated with any accu-racy (see earlier discussion on this point). Es-timating the population of dependent heroin and pharmaceutical opioid users is difficult enough, but the demand for treatment is a more unpredictable concept, depending on a range of factors, including the way that treatment is provided.
Uncertainty about unmet demand is also mirrored in uncertainty about the number of available treatment places in Australia. It may be possible to count the treatment places in a clinic. But, enumeration of all prescribing places through private practitioners and all dispensing places through community phar-macies is problematic. During the consulta-tion process we were told that jurisdictional systems had excess capacity and could ab-sorb many more clients, even though we also heard of long delays in accessing treatment
Summary of issue: accessibility
• Accessibility problems exist in relation to both access to prescribers and access to dis-pensing services.
• There are waiting times for new treatment entrants.
• The extent of waiting times is difficult to determine.
• ‘Caps’ on client numbers may be an impediment to accessibility.
• The accessibility of dispensing locations is probably more crucial than accessibility of prescribers (given daily attendance requirements and the fact that people can accu-mulate debts with the local pharmacist).
• The accessibility of dispensing is highly variable, depending upon where the client lives and their personal circumstances (employment and so on).
• There is a trade-off between making programs highly accessible through, for example, low-threshold programs, and ensuring high-quality interventions for individual clients. More research is required in this area.

Poly
gon
30
in the same jurisdictions. These two per-spectives are not irreconcilable. It may be that treatment places are found for exist-ing clients who are already dependent upon pharmacotherapy maintenance, whereas new treatment entrants incur delays.
Theoretically an assessment of funding ef-ficiency should also consider the level of resources allocated to other forms of treat-ment in relation to the benefits of pharma-cotherapy maintenance. Should money be redirected from other treatments? From an even wider perspective we need to compare pharmacotherapy maintenance funding with the funds allocated to other drug control policies, such as prevention and policing.
An assessment of whether the program fund-ing is sufficient requires knowledge about both the unmet demand and the current availability of vacant treatment spaces; the current system’s capacity for expansion; and some agreement about the principles we need to use to assess funding adequacy. These matters have not received attention to date.
Cost-shifting
The current funding arrangements might lead to waste, duplication and cost-shifting between federal and State/Territory govern-ments. It is also possible that cost-shifting could occur between the clients and gov-ernment. These matters have not been the subject of independent objective analysis.
Cost-shifting is a feature of the pharmaco-therapy maintenance system, just as it is of the health system as a whole.29 The potential and incentive for cost-shifting are inevitable consequences of the involvement of the fed-eral government, State/Territory governments and clients in the provision and/or funding of pharmacotherapy services. Victoria’s deci-sion to rely on private health care providers for prescribing can be seen as an example of cost-shifting. The responsibility for funding medical practitioner services is shifted to the federal government through the Medicare system. If prescribing services were provided by public clinics or hospitals, State govern-ments would be financially responsible for the services. Analogously, the Australian Government’s decision not to subsidise the dispensing of pharmacotherapy drugs under the PBS shifts the costs of dispensing from the government to clients. When public clin-ics do not charge fees for dispensing, clients can shift costs onto the government by not moving to private sector dispensing, even when they no longer need the services pro-vided by the public clinic and are financially able to pay the dispensing fee.
Cost-shifting is a problem if it affects the incentives for providers to supply treatment and for patients to access appropriate care options. This can then lead to inefficient al-location of clients and resources to one form of service delivery over another.
29 There is discussion of cost-shifting in the Australian health system as a whole (see Buckmaster and Pratt, 2005). The National Health and Hospitals Reform Commission (the Commission) was recently established by government to develop a long-term health reform plan for Australia. By June 2009 the Commission will report on a plan to improve the performance of the health system by, among other things, reducing inefficiencies generated by cost-shifting (see the terms of reference for the Commission: <http://www.health.gov.au/internet/main/publishing.nsf/Content/nhrc-1> accessed 27 October 2008).
The issues
31
Economic efficiency of different funding mechanisms
Although the comparison of different fund-ing arrangements seems to be a fundamental issue, there are insufficient data to inform the debate. Can this issue be determined only by comparing jurisdictions? Or does it make sense to ask, ‘Are public clinics worth the extra expense?’ What does it mean now that the federal mental health program has the potential to cover some aspects of care that would previously have been provided only through public clinics? Could this make a difference?
Treatment supply, even among public clin-ics, is characterised by heterogeneity in the content of service provision and in the cost of that service provision. As demonstrated in the National Evaluation of Pharmacotherapies for Opioid Dependence (NEPOD) research, the cost of service provision varied substan-tially between individual clinics (Mattick et al., 2001). Is this an example of inefficient service delivery, or was the variation in cost matched by a variation in client presentations and outcomes?
In summary, there are a significant number of issues that require examination in explor-ing whether the Australian pharmacotherapy maintenance treatment system is efficient in its service delivery. These issues are rarely explored, and we have no data to inform the analysis. The key questions include: the extent of inefficiency within the current services (both public and GP); the extent to which cost- shifting is problematic if and when it occurs; the extent to which different types of service delivery are associated with greater or lower efficiencies; and the equity of funding (State, federal and client).
3.6 Managing medication non-adherence and diversionClarifying terminology is the first issue we identified in relation to medication misuse and diversion. The term ‘diversion’ has been used as a ‘catch-all’ that encompasses both non-adherence to medication as well as sell-ing (or swapping) medication on the black market. It is preferable to distinguish these two types of medication misuse. In the first instance, non-adherence (or non- compliance) to a medication regime encompasses not tak-ing the medication as prescribed. In opioid pharmacotherapy maintenance this may in-clude taking only half the dose, taking the dose at intervals over the day rather than at one time, saving doses for another day, in-jecting the dose, or missing the dose. Selling or trading medication on the black market is most accurately described as diversion.
Non-compliance
Non- compliance with general medication has been identified as a major medical prob-lem (Wertheimer & Santella, 2003). In their review of American non-compliance litera-ture, Wertheimer and Santella (2003) found that: 14–21 per cent of clients never fill their original prescriptions; 30–50 per cent of all clients ignore or otherwise compromise in-structions concerning their medication; and 12–20 per cent of clients take other peo-ple’s medicines. And for those with chronic diseases such as diabetes and hypertension, compliance with recommended behavioural changes occurs in less than 30 per cent of cases (O’Brien & McLellan, 1996).
Summary of issue: efficiency
• Is the available funding sufficient?
• Is it used efficiently?
Poly
gon
32
If opioid pharmacotherapy maintenance cli-ents exhibited the same level of medication non-compliance as the general population, we would expect that 20–50 per cent of pharma-cotherapy maintenance clients would be non- compliant with their medication. There are, however, two good reasons to expect higher adherence in pharmacotherapy maintenance programs — clients take their medication under supervision; and, if doses are missed, a with-drawal syndrome will ensue.
Consumers have argued that non- compliance may be beneficial to the extent that it ena-bles a client to tailor his/her own program. In the context of general population non- compliance with medications, we should ex-pect non-compliance and understand that it can enable more client control over treat-ment. However, in the case of pharmaco-therapy maintenance, there is a particular harm associated with one type of non- compliance — that is, injecting the medica-tion. The possible health harms associated with methadone injection include fistulas, venous thrombosis and a heightened risk of overdose (Fiellin & Lintzeris, 2003). Health harms associated with intravenous buprenor-phine use include skin infections and in-fections of the surrounding soft tissue, the ‘spread’ of infections to osteoarticular in-fections (or infections of bones and joints), infectious endocarditis (or infection of the inner lining of the heart muscle), cerebral in-fection, pulmonary infection through septic pulmonary embolism, disseminated candi-diasis, and vein damage (Jenkinson, Clark, Fry & Dobbin, 2005; Reisenger, 2006; Win-stock, Lea & Sheridan, 2008). Overdose is also a risk, especially if the person taking the medication has lowered tolerance to opioids.
Diversion
Diversion is different from non- compliance, and involves a third party taking the medica-tion. The medication is sold or exchanged on the black market. It is hard to prove, but it seems logical that economic factors are important in drug diversion. Where there is unmet demand for pharmacotherapy main-tenance, there is potential for a market to develop. The majority of the population of pharmacotherapy clients are reliant on income support. Clients can supplement income support by selling or exchanging some of their medication. Where pharmacotherapy programs are limited, the existence of these medications on the black market may assist a drug user in withdrawal and may increase access to unmanaged treatment. The harms associated with diversion extend the harms of injecting the diverted medication beyond the client group and increase the risk of overdose.
A number of Australian studies have doc-umented rates of non-adherence and di-version of methadone and buprenorphine, revealing substantial inter-jurisdictional dif-ferences (see Humeniuk, Ali, McGregor and Darke (2003) for a review of the findings on methadone diversion before the introduction of buprenorphine). Since the introduction of buprenorphine there has been interest in the question of whether it might be associ-ated with changes in the diversion and non- adherence rates. The Illicit Drug Reporting System (IDRS) (O’Brien, Black, Degenhardt et al., 2006), an annual surveillance of in-jecting drug users in Australia, reported the emergence of buprenorphine as an injected street drug. Jenkinson et al. (2005) reported that 33 per cent of the Victorian IDRS sam-ple had injected buprenorphine in the last six months. Pharmacists have high levels of suspicion in relation to the extent of bu-prenorphine misuse and diversion (Nielsen,

The issues
33
Dietze, Dunlop et al., 2007). One widespread practice in Australia to avoid diversion is to crush the buprenorphine tablet prior to dis-pensing. There are differences between juris-dictions and individual clinics in the extent to which buprenorphine is crushed (Winstock et al., 2008). There is no research on whether crushing of buprenorphine changes the bio-availability, pharmacodynamics or pharma-cokinetics of the medication.
Differences between jurisdictions
Jurisdictional differences in the extent of bu-prenorphine injection are unsurprising since the uptake rates of buprenorphine have var-ied markedly across Australia. For example, New South Wales has experienced one of the slowest uptake rates. Winstock et al. (2008) found that in New South Wales 23.8 per cent of buprenorphine-maintained clients reported diverting their dose in the preced-ing 12 months. This compared with only 2.2 per cent for methadone clients. In relation to non-adherence, however, 17 per cent of methadone clients had injected their take-away dose in the last 12 months compared with only 9.1 per cent of buprenorphine clients.30 Furthermore, one study hypoth-esised that the relatively high rates of bu-prenorphine diversion in Victoria could be explained by the fact that methadone is di-luted in Victoria, making methadone much less attractive to inject (Fraser, Valentine,
Treloar & Macmillan, 2007). While research would be required to examine this closely, it is highly plausible that there is a dynamic relationship between the clinical practices for buprenorphine and methadone and the rates of diversion of the drugs.
Misuse and diversion of buprenorphine are of course not unique to Australia. In France, in the context of a low-threshold buprenor-phine program, a significant amount of di-version was reported (Vidal-Trecan, Varescon, Nabet & Boissonnas, 2003). Likewise in the United States, buprenorphine misuse and di-version have been reported (Smith, Bailey, Woody & Kleber, 2007; Stimmel, 2007). And as noted earlier, diversion of methadone also occurs, in some cases at higher rates than buprenorphine (Winstock et al., 2008).
Both non- compliance and diversion represent a significant public image problem for opioid pharmacotherapy programs and damage a highly vulnerable but very valuable program.
Lintzeris (2006) notes four points that are likely to drive the extent of both non- adherence and diversion of pharmacotherapy medications:
• the conditions of supervised dosing
• the size of the dose
• availability of other opioids (e.g. heroin)
• local cultural variations in the injecting community.
30 Reckitt Benckiser has funded the National Drug and Alcohol Research Centre through an untied educational grant to conduct post-marketing surveillance studies of the diversion and injection of buprenorphine-naloxone.
Poly
gon
34Service providers and governments want to reduce the extent of medication non- compliance and diversion. Diversion and to a much lesser extent non-compliance under-mine the viability of the entire program. The strategies employed to reduce non- compliance and diversion include: reducing the availability of take-away medications; ensuring super-vised dosing; crushing buprenorphine tablets before dispensing; introducing buprenorphine- naloxone; and diluting methadone take- away doses. Importantly improving access to the program and the overall quality of the treat-ment provided is likely to reduce misuse and diversion.
3.7 The role of unsupervised treatment and take-away dosingAs with diversion, terminology needs to be clarified at the outset for this issue. Take- away doses, in which clients are given future supplies to consume without supervision, have always formed part of the Australian pharmacotherapy maintenance program. Un-supervised treatment (or unobserved treat-ment) is a relatively new concept associated with buprenorphine-naloxone. In general, unsupervised treatment refers to a program in which clients are provided with a prescrip-tion to collect one supply of medication at a time (being prescribed for a week, a month, or as prescribed by the doctor). At present, the term ‘take-away’ and the term ‘unsuper-vised treatment’ are being used interchange-ably in Australia, despite the difference in connotation and the different aetiology of the terms. It is suggested that the terms be used more specifically as defined above.
Summary of issue: medication non-adherence and diversion
• Terminology is important. We distinguish between medication non-compliance and diversion. Non-compliance occurs when the client does not take the medication as prescribed. Diversion involves selling/exchanging the medication on the black market.
• Non-compliance is common in most client groups and arguably enables a more indi-vidually tailored regime. One form of non-compliance, injection of the dose, is asso-ciated with significant harms.
• Diversion can also be associated with significant harm and engagement with the black market for pharmacotherapy drugs.
• The program has been threatened by the behaviour of people who fail to comply or who divert drugs. It is imperative to have measures in place to minimise the harms caused by diversion and non-compliance. It is also important to identify aspects of the pro-gram that encourage diversion or non-compliance, and rectify them where appropriate.
The issues
35
Take-away doses
Take- away doses have traditionally been avail-able in the following circumstances:
• to reward clients who are doing well in treatment
• when daily attendance represents signif-icant hardship for an individual client, and or
• where dispensing cannot occur on certain days of the week (e.g. Sundays).
The National Pharmacotherapy Policy states:
In general, methadone and buprenor-phine should be consumed under direct supervision at a location approved by the responsible jurisdictional authority. While supervised dosing can be an important strategy to manage risks, it can also deter people from engaging with treatment services and can be a serious obstacle to both the ongoing participation in treat-ment and social reintegration. Hence, it is appropriate in certain circumstances, for a prescriber to authorise either regu-lar or one- off takeaway doses for people receiving maintenance treatment. (Com-monwealth of Australia, 2007, p.18)
Take-away dosing allows the client more in-dependence and autonomy. Daily attendance is time-consuming and, combined with the inflexibility of dosing times, inhibits compet-ing aspects of life such as travel, parenthood, paid employment, job seeking and activities that must be undertaken in order to receive income support from the government. Some clients also value the fact that there is less need to socialise with other pharmacotherapy maintenance clients, their privacy is better protected and they feel trusted (Fraser et al., 2007). Take-away doses may also give cli-ents more control over some aspects of their treatment (Robles, Miller, Gilmore-Thomas
& McMillan, 2001). Quality of life may be improved through the reduction in daily at-tendance at a clinic. Although not generally available at entry to treatment, the promise of take-away dosing may also make treat-ment more attractive. Studies have found that take-away dosing improves treatment retention (Pani & Pirastu, 2000; Rhoades, Creson, Elk et al., 1998). Overall, take-away doses imbue clients with an increased sense of lifestyle normality and a better fit with society (Fraser et al., 2007). These are, after all, the overarching gaols of pharmacother-apy treatment.
From a service provider’s point of view, take- away dosing enables greater flexibility in clinic hours and pharmacy pick-up times. Indeed, in some jurisdictions take-away doses are essen-tial because dosing sites are not accessible seven days a week. Take-away dosing can also provide clinicians with the opportunity to implement contingency management strat-egies by rewarding clients for abstinence or compliance with treatment (Chutape, Silver-man & Stitzer, 2001).
On the downside there are risks of harm to the clients themselves, and to society in gen-eral, associated with take-away dosing. There is potential for non-compliance and diver-sion. The potential harms to clients include the ingestion or injection of multiple take- away doses with the possible risk of over-dose. Diversion of take-away doses to other individuals may lead to withdrawal symp-toms and heroin use in clients. The avail-ability of take-away doses has contributed to a ‘black market’ for pharmacotherapy drugs (Lintzeris, Lenne & Ritter, 1999). As noted earlier, there are risks associated with injecting methadone (Lintzeris et al., 1999; Southgate, Kippax, Bammer et al., 2001) and buprenorphine (Jenkinson et al., 2005; Reisenger, 2006; Vidal-Trecan et al., 2003), and there have been overdose deaths from

Poly
gon
36
diverted methadone (Sunjic & Zador, 1999). Take-away dosing has also been linked to in-cidents of accidental oral ingestion of take- away doses by opiate-naive individuals, and in rare cases the death or injury of children.
Consumers, like clinicians and researchers, see a need for supervised dosing for all cli-ents at the commencement of treatment and for clients who are experiencing crises (see Stone and Fletcher (2003) for consumer views). There is no evidence that take- away dosing leads to poorer adherence to treat-ment and hence poorer treatment outcomes. But, clients with take-away doses will have less contact with clinicians and pharmacists, and this could lead to poorer outcomes in some clients. Consumers reported that the current take-away policies are restrictive and appeared to be geared towards the more complex clients, not acknowledging the needs of long-term stable clients who have been in treatment for many years. In this sense, take-away policies cater for the ‘lowest common denominator’.31,32
Finally, while it would appear that greater numbers of unsupervised doses would reduce the costs of the services, this may not neces-sarily be so. Increasing unsupervised dosing may increase the costs of providing services because of the greater need for clinical mon-itoring, assessment of stability, and urine testing. In addition, regardless of the num-bers of clients attending for dispensing on any particular day, staff have to be available for dispensing at all times during dispens-ing hours. Efficiencies would be gained only through reductions in the number of staff required for dispensing each day.
There is substantial variation in take-away policies between jurisdictions. In some juris-dictions take-away doses are given from the first week in treatment, while in others the client must wait for upwards of six months. The form of the medication also varies. In Victoria dilution of methadone take-away doses with cordial is mandatory, whereas in New South Wales this is not the case. There is also jurisdictional variation in the criterion for access to take-away dosing. In some ju-risdictions access is based on an assessment of patient stability and in others the length of time in treatment. In addition, there are policy differences between methadone, bu-prenorphine and buprenorphine- naloxone. Indeed, the introduction of buprenorphine-naloxone has led to the reconsideration of take-away policies in many jurisdictions in recent years (see Appendix B for details).
Many of the respondents to the consultation process for the issues paper suggested that a take-away policy should be standardised nationally. The substantial variations in poli-cies are perceived as problematic, especially in the context of client travel and transfer between jurisdictions. There appears no logi-cal reason for jurisdictions to have different policies on take-away doses.
31 This point was made by the Australian Injecting and Illicit Drug Users League during the consultation process.
32 We were told that the public methadone program in South Australia has been providing unsupervised dosing six days per week for a small number of long-term stable clients and that there may be a similar approach in New South Wales.
The issues
37
Unsupervised treatment
Unsupervised treatment occurs when a client has reached a level of stability such that there is no need for them to attend frequently to receive their medication, and treatment is then conducted in an unobserved fashion.33 The National Pharmacotherapy Policy does not mention unsupervised treatment.
With the introduction of buprenorphine- naloxone, the issue of unsupervised treatment has become prominent — buprenorphine- naloxone provides for the possibility of unsu-pervised treatment in a way that methadone has not. For our purposes, we use the term ‘unsupervised treatment’ to mean greater than one week’s supply of medication (i.e. we do not consider six take-away doses per week as unsupervised treatment — we appreciate this distinction is arbitrary).
Despite the potential window of opportu-nity for ‘unsupervised treatment’ in Aus-tralia, it does appear that the introduction of buprenorphine- naloxone has merely cre-ated a re-examination of take- away policies around the country, rather than an examina-tion of a new treatment model. The focus has turned to ‘assessment of stability’ as the guiding clinical principle in the provision of take-away doses and a simple expansion of the availability of take-away does to clients assessed as stable.34
The Australasian Chapter of Addiction Med-icine has published a document outlining clinical guidelines for the assessment of sta-bility (Winstock & Bell, 2006). They note a number of important overarching principles for unsupervised dosing:
• careful client selection
• ongoing clinical monitoring
• the importance of transparency in treat-ment decisions and the involvement of the client in that process (Winstock & Bell, 2006).
This document indicates that a thorough as-sessment of stability is required. Stability is defined as non-risky drug use; stable social, personal and physical functioning; and psy-chosocial stability. We understand that there are differences of opinion about assessing suitability for unsupervised treatment.
An important Australian randomised controlled trial (Bell, Shanahan, Mutch et al., 2007) com-pared daily supervised buprenorphine- naloxone to weekly unsupervised buprenorphine- naloxone. The study found no significant difference in treatment retention or client outcomes between the two groups three months into the trial. The authors them-selves note that the particularities of this study may have artificially enhanced treat-ment retention among the daily supervised
33 We do not know how many programs of ‘unsupervised treatment’ are being offered around Australia. The Langton Centre conducted trials but it is unclear whether this ‘new’ model of service delivery is being implemented or whether take-away policies are just being expanded.
34 The ‘assessment of stability’ in association with receipt of take-away doses may place some jurisdictions or services that cannot provide seven-day-a-week dosing in a difficult position — in those instances, take-away doses are provided because of service delivery constraints, not because a client is judged suitable for take-away dosing.

Poly
gon
38
group.35 With no difference between re-tention rates, these findings can be used as support for those arguing that unsuper-vised dosing should be discouraged, just as they support the argument that unsupervised dosing is preferable. The ideal proportion of supervised doses to unsupervised doses is undetermined and likely to depend on in-dividual client characteristics. (See also Bell (2007) for further discussion of these issues.)
It seems fair to say that the area is fraught. There is no agreement among specialist practitioners on the issue of unsupervised treatment; little concordance between juris-dictions on their take-away policies; vary-
ing clinical practice; the use of changed take-away policies in lieu of an unsupervised treatment model; and concern from clients that their opinions have been disregarded.
Balancing the degree of regulation by the State with individual medical clinical decision making is complex. Ultimately the balance of benefits and risks needs to be consid-ered in developing take-away policies. While there are both benefits and risks to clients and the wider community, often the broader benefits of the positive impact of take-away doses on client outcomes are ignored and discussion of risk is focused on a worst-case scenario, such as child deaths from metha-done overdose.
35 All participants were aware that at the end of the three-month efficacy study they could gain access to unobserved administration, and the incentive of unobserved doses may have enhanced retention in the observed group. Secondly, only 131 out of 591 heroin users were recruited. One major reason for non-recruitment was homelessness or unstable accommodation, and in that setting safe storage of medication would be difficult to guarantee.
Summary of issue: unsupervised treatment and take-away dosing
• Take-away doses provide opportunities for autonomy and independence for clients.
• There is limited evidence to indicate that unsupervised dosing is effective in enhancing treatment retention early in treatment episode (within the first six months). However, take-away doses for long-term stable clients are linked to better treatment retention.
• Preferably take-away policies should be built around an evidence base that weighs up both risks and benefits, and provides for individual tailoring. This requires the capac-ity for greater monitoring and review of clients by service providers (e.g. urine testing, clinical reviews) to ensure that treatment decisions are based upon client needs and safety aspects.
• There is substantial variation in take-away policies between jurisdictions.
• Nationally consistent policies and clinical guidelines for take-away doses may be warranted.
• The introduction of buprenorphine-naloxone provided the opportunity for consid-eration of a new treatment model — ‘unsupervised treatment’. However, jurisdictions have reconsidered their take-away policies rather than consider the possibility of a new treatment model.
The issues
39
3.8 Counselling and psychosocial interventionsCounselling can cover a range of issues such as relapse prevention, coping skills, man-agement of emotional wellbeing and rela-tionships. Counselling can take the form of cognitive–behavioural therapies, group psy-chotherapy or other forms, such as narrative therapy. Psychosocial support services cover a range of different life domains, such as housing, personal financial management, skills retraining for employment, and so on.36
There is debate about the extent of benefit derived from the provision of counselling. There are those who argue that the coun-selling component is vital to the successful behaviour change necessary for ceasing illicit drug use. Others claim that counselling is useful only for those clients who seek it out and wish to engage with psychological serv-ices. More recently, the acknowledgement of substantial mental health problems within the client group has added fuel to calls for effective psychological services that can also attend to mental health problems.37
A number of studies have examined outcomes of pharmacotherapy treatment with and with-out psychosocial interventions. Research from the 1990s seemed to indicate a preference for psychosocial services. For example, Woody, McLellan, Luborsky and O’Brien (1995) and McLellan, Arndt, Metzger et al. (1993) both concluded that the provision of psychosocial support enhanced treatment outcomes. It is somewhat difficult, however, to interpret these findings within an Australian context. Even the
‘standard care’ provided by the services under scrutiny included more intensive psychoso-cial support than most intensive programs in Australia. A study by Bickel, Amass, Higgins et al. (1997) found that the group receiv-ing behavioural treatment had significantly higher retention rates than those from the standard treatment group. They also found a strong association between completion of behavioural activities and both treatment retention and opioid abstinence. Simpson, Joe, Rowan-Szal and Greener (1997) reported that counselling improved the quality of the therapeutic relationship and was associated with lower drug use during treatment.
More recently, Rowan-Szal, Chatham, Greener et al. (2004) reported that those pharmacother-apy clients who spent a longer time in coun-selling had better therapeutic relationships and that manualised counselling treatment can improve participation. This research group has also shown strong associations between therapeutic relationship, treatment improve-ments and retention (Joe, Flynn, Broome & Simpson, 2007; Joe, Simpson, Dansereau & Rowan-Szal, 2001). In the United Kingdom, pharmacotherapy maintenance clients who received drug-focused counselling were less likely to be using heroin at follow-up. How-ever, the intensity of the counselling (number and duration of sessions) was not predictive of outcome (Gossop, Stewart & Marsden, 2006).
On the other side of the ledger, there are stud-ies that have demonstrated that counselling does not lead to improvements in outcomes over and above standard care. Gruber, Delucchi, Kielstein and Batki (2008) found no differences
36 Case management and the coordination of a range of welfare and social services are covered under collaborative care planning (see 3.10).
37 The high rates of psychiatric comorbidity among heroin users are well documented, most commonly mood disorders, anxiety disorders, and antisocial personality disorder (Darke & Ross, 1997; Krausz, Degkwitz, Kuhne & Vertheim, 1998). Post-traumatic stress disorder is also highly prevalent among this group (Mills, Lynskey, Teesson et al., 2003).
Poly
gon
40
in outcomes at seven months between mini-mal counselling and standard care (monthly counselling plus access to psychosocial services as required). In office-based buprenorphine maintenance, intensive counselling did not produce superior outcomes compared with standard care (Fiellin, Pantalon, Chawarski et al., 2006).
The Cochrane Review found that:
Structured psychosocial treatment gave added benefit on reducing the use of heroin during treatment (relative risk 0.7). There was a trend but no clear benefit to additional psychosocial treatment on peo-ple staying in treatment and heroin use at follow up. Insufficient evidence was avail-able on psychiatric symptoms, distress and quality of life in terms of employment or study and positive lifestyle changes. (from Amato, Minozzi, Davoli et al., 2004)
The efficacy of both counselling and psycho-social support for clients in pharmacotherapy maintenance will depend on a number of factors:
• the client’s level of psychological well-being and need for counselling (recall that clients in the pharmacotherapy program are heterogeneous)
• the willingness of the client to engage in counselling, since motivation to engage in counselling appears to be a determinant of outcome (as cited above)
• the service provider’s provision of coun-selling: whether on-site within a public clinic, or via referral from a GP — self- evidently access to counselling is a pre-requisite of clients obtaining it, and
• the degree of proactive case management, which will encourage and facilitate appro-priate referral to counselling.
‘Most [Canadian] users, in general, underlined the importance of counselling but they just wanted to have choices, options, and input into the decision-making about it’ (Fischer, Chin, Kuo et al., 2002, p.506). We suspect that Australian users feel likewise.
In summary, it appears that the provision of counselling can enhance treatment outcomes but there is no indication that counselling should be a compulsory or essential com-ponent of pharmacotherapy maintenance.
Summary of issue: counselling and support services
• There is evidence that both counselling and support services improve client outcomes in pharmacotherapy maintenance, provided the client participates on a voluntary basis.
• Ensuring good referral pathways and access to counselling and mental health services is important.
• Both counselling and psychosocial support should be available but neither should be a mandatory component of pharmacotherapy maintenance.
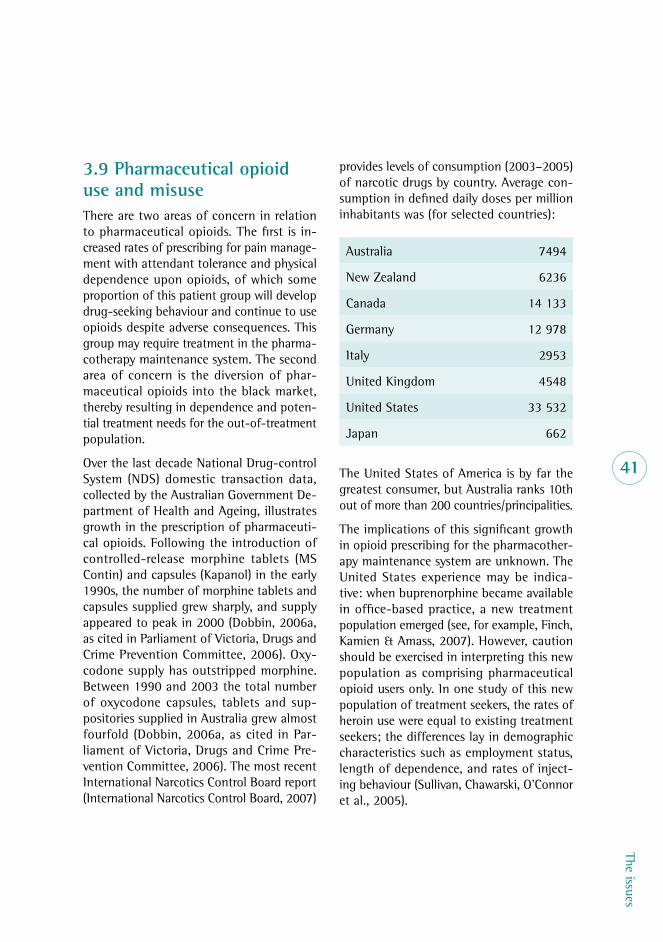
The issues
41
3.9 Pharmaceutical opioid use and misuseThere are two areas of concern in relation to pharmaceutical opioids. The first is in-creased rates of prescribing for pain manage-ment with attendant tolerance and physical dependence upon opioids, of which some proportion of this patient group will develop drug-seeking behaviour and continue to use opioids despite adverse consequences. This group may require treatment in the pharma-cotherapy maintenance system. The second area of concern is the diversion of phar-maceutical opioids into the black market, thereby resulting in dependence and poten-tial treatment needs for the out-of-treatment population.
Over the last decade National Drug-control System (NDS) domestic transaction data, collected by the Australian Government De-partment of Health and Ageing, illustrates growth in the prescription of pharmaceuti-cal opioids. Following the introduction of controlled- release morphine tablets (MS Contin) and capsules (Kapanol) in the early 1990s, the number of morphine tablets and capsules supplied grew sharply, and supply appeared to peak in 2000 (Dobbin, 2006a, as cited in Parliament of Victoria, Drugs and Crime Prevention Committee, 2006). Oxy-codone supply has outstripped morphine. Between 1990 and 2003 the total number of oxycodone capsules, tablets and sup-positories supplied in Australia grew almost fourfold (Dobbin, 2006a, as cited in Par-liament of Victoria, Drugs and Crime Pre-vention Committee, 2006). The most recent International Narcotics Control Board report (International Narcotics Control Board, 2007)
provides levels of consumption (2003–2005) of narcotic drugs by country. Average con-sumption in defined daily doses per million inhabitants was (for selected countries):
Australia 7494
New Zealand 6236
Canada 14 133
Germany 12 978
Italy 2953
United Kingdom 4548
United States 33 532
Japan 662
The United States of America is by far the greatest consumer, but Australia ranks 10th out of more than 200 countries/principalities.
The implications of this significant growth in opioid prescribing for the pharmacother-apy maintenance system are unknown. The United States experience may be indica-tive: when buprenorphine became available in office- based practice, a new treatment population emerged (see, for example, Finch, Kamien & Amass, 2007). However, caution should be exercised in interpreting this new population as comprising pharmaceutical opioid users only. In one study of this new population of treatment seekers, the rates of heroin use were equal to existing treatment seekers; the differences lay in demographic characteristics such as employment status, length of dependence, and rates of inject-ing behaviour (Sullivan, Chawarski, O’Connor et al., 2005).

Poly
gon
42
Recent research from the United States indicates that 69 per cent of methadone maintenance clients reported abusing phar-maceutical opioids (Rosenblum, Parrino, Schnoll et al., 2007). There are no published Australian data on the rates of pharmaceuti-cal misuse of opioids in pharmacotherapy maintenance clients. 38
Research has shown the presence of illicit drug markets for pharmaceutical opioids and benzodiazepines in Australia (Bruno, 2007; Degenhardt, Black, Breen et al., 2006; O’Reilly, Leibrick, Huxtable & Chenhall, 2004; Smith, Miller, O’Keefe & Fry, 2004). Data from the sentinel sample of injecting drug users (IDRS) suggest that, in 2007, 28 per cent of the national convenience sample had used illicit oxycodone (e.g. OxyContin, Endone) in the last six months (Black, Roxburgh, Degenhardt et al., 2008). In 2006, Western Australia and Tasmania reported the highest levels of recent illicit oxycodone use — 42 per cent and 29 per
cent respectively. In 2007, Western Australia’s recent use rate was still the highest (at 44 per cent), Queensland’s (39 per cent) surpassed that of Tasmania (36 per cent). Even though the IDRS data indicate increases in recent use of illicit oxycodone in all jurisdictions over the last two years, only Queensland, Tasmania and, to a less extent, New South Wales have seen substantial increases.39 While the IDRS data provide some indications of trends, the IDRS is not a random survey of drug users. Nonetheless, these trends are consistent with some substitution of illicit oxycodone for heroin consequent on the heroin drought. And, it is unsurprising that the jurisdictions with tenuous pre-drought heroin supply (Western Australia, South Australia and Tas-mania) have experienced the largest increases in illicit oxycodone use. The availability of heroin is likely to be an important driver — when quality heroin is readily available, the rates of pharmaceutical opioid misuse may decrease.
38 There is a project underway across Victoria, Queensland, Western Australia and Tasmania examining the use of pharmaceutical drugs in treatment populations.
39 Oxycodone has been identified in the data only since 2005. Before then it was included with ‘other opioids’.
Summary of issue: pharmaceutical opioid use and misuse
• The growth in prescribing of pharmaceutical opioids has implications for the pharma-cotherapy maintenance treatment system.
• Sentinel data warn that growing numbers of people are becoming dependent on phar-maceutical opioids, necessitating the establishment of suitable treatment options.
• The appropriate regulation of pharmaceutical opioids is a delicate balance.
• Education and training are required for the pharmacotherapy maintenance workforce in order to better manage dependence on pharmaceutical opioids — for GPs involved in prescribing pharmaceutical opioids, and for pain management centres.
The issues
43
Treatment implications
What are the treatment and service system implications? There are no data on the num-bers of pharmacotherapy maintenance clients in Australia whose primary drug of depend-ence is a pharmaceutical opioid. We received informal advice from South Australia that in that State around 7–8 per cent of pharmaco-therapy maintenance clients were morphine- dependent. A poster presented at the 2007 APSAD Conference by Lloyd, Ballantyne and Loveday (2007) indicated increasing proportions of pharmacotherapy mainte-nance presentations with pharmaceutical opioids as the primary drug of concern (in 2006, 12.5% morphine, 2.4% other opioids, 62.1% heroin). Across Australia, in the non- pharmacotherapy maintenance treatment services, 4 per cent of episodes of care are for pharmaceutical opioids (Australian Insti-tute of Health and Welfare, 2007a).
It is likely that the numbers of pharmaceuti-cal opioid-dependent people in pharmaco-therapy maintenance treatment will grow. Does the current treatment service system have the appropriate services for this poten-tial new group of treatment recipients? There is currently no evidence to inform practition-ers about the preferred medication regimes for those misusing pharmaceutical opioids, although both methadone and buprenor-phine are being used without apparent ill- effect. More research in this area is clearly warranted.
3.10 Coordinating care in the Australian service systemCollaborative care planning refers to a com-prehensive clinical management approach where the key issues, concerns and problems regarding drug use, medical, psychological, social and forensic wellbeing are identified. Once these issues are identified, a care plan is negotiated with the client and with the various allied services that may be required.40 This comprehensive approach is especially important for this marginalised client group who have multiple comorbidities and often cannot easily access care in health services.
In the formulation of an effective service system for clients, consideration needs to be given to the linkages and cross- referral systems between prescribers of pharmaco-therapies and those services that can provide welfare and support services. The kinds of services required include financial counsel-ling, employment support, accommodation and welfare services.41 In addition, a good service system will also enable smooth refer-ral between specialist services for those with HIV, hepatitis and other medical needs, pregnancy services, child care services and support for dispensing psychiatric medica-tion. The assignment of a case manager to oversee this coordinated care is the preferred model.
The national clinical guidelines refer to the importance of a collaborative working relationship between the pharmacotherapy client and his/her prescriber and pharmacist (Henry-Edwards et al., 2003; Lintzeris et al., 2006). For example, it is strongly encour-aged that clients receive a copy of their care plan with the negotiated and agreed goals.
40 Of course, not every client requires comprehensive services across a range of areas.
41 The issue of the provision of counselling and other psychological therapies is covered in 3.8. Here comments are limited to coordinated care for social and welfare needs.

Poly
gon
44
Key informants from the pharmacy sector suggested that there be more consultation between pharmacists and prescribers over clinical matters, such as optimal dosing and suitability of patients for take-away dosing. Anecdotal evidence suggests that where a drug and alcohol clinician is involved in the client’s treatment and facilitates communica-tion between the GP, pharmacist and client, there are improved client compliance and improved treatment outcomes. Respondents to the issues paper from within the pharmacy sector indicated that they would welcome research exploring the contribution that their profession could make towards supporting treatment. For example, pharmacists could be trained to assist with counselling.
While collaborative care planning is regarded as essential and is recommended in national guidelines, the actual implementation is more difficult. In the context of service
provision within a general practice setting, the provision of case management leading to collaborative care planning may be limited. However, the federal government now explic-itly funds GPs to prepare care plans and engage in collaborative case management.
Unfortunately there is little research evidence to inform the degree of importance of case management/collaborative care planning. In addition, some pharmacotherapy clients do not want their regular GP to know that they are on methadone /buprenorphine due to the stigma. Fifty-four per cent of clients contin-ued to see another doctor other than their methadone prescriber for their general health needs (Ezard, Lintzeris, Odgers et al., 1999, p.420). Hence, stigma (see 3.14) also deters appropriate collaborative case planning.
Summary of issue: collaborative care plans
• Collaborative care planning is thought to be important, especially in the context of the pharmacotherapy client population.
• Achieving coordinated care across a web of services is complicated and time-consuming.
• Strategies that can improve collaborative care planning are required.
The issues
45
3.11 Meaningful consumer involvement in the programThere are a number of reasons why it is es-sential for meaningful involvement of con-sumers in the Australian pharmacotherapy program:42
• Evidence-based medicine (EBM) now can-not proceed without consumer involvement in a meaningful and collaborative way.
• It is ethical. Consumer involvement is regarded as a basic right.
• Consumers have different forms of knowl-edge, expertise and perspectives from those of practitioners.
• Consumers are one group of many stake-holders, but they lack formal mechanisms for involvement.
There are a number of aspects to meaningful consumer involvement in pharmacotherapy treatment programs in Australia. One involves the ways in which consumers (active drug users, existing clients of the program, and those who have previously received treatment) can provide input into the development of the program over time. Another means of involvement is the role of consumer com-plaints mechanisms. Finally, there is the individual client’s involvement in treatment decisions. There is no discussion on consumer involvement in the National Pharmacotherapy Policy nor in the jurisdictional policies.
The Australian Injecting and Illicit Drug Users League (AIVL) (2008) identifies a hierarchy of consumer involvement, including:
• participation in treatment and care
• employment of consumers by services as consultants and advocates
• participation in service delivery and evalu-ation
• participation in policy and planning
• participation in education and training
• participation in staff recruitment.
Specific pharmacotherapy consumer complaints mechanisms have been established in most jurisdictions. Table 3 describes the complaints mechanisms noted by AIVL, the national organ-isation representing people who use drugs and drug treatment consumers. In all jurisdictions AIVL suggests that clients in clinics first turn to the in-house complaints mechanism.43 If the in-house complaints mechanism proves unsatisfactory, AIVL suggests that the client approach the State/Territory-based drug user organisation. The drug user organisation can represent the client’s case at the various forums. Even without the support of the drug user organisation, the client can access the same forums.
42 Boote, Barber and Cooper (2005) list eight best practice principles for consumer involvement.
43 In response to the issues paper, NSW Users and AIDS Association noted that in-house complaints mechanisms do not exist in many clinics in New South Wales and, even if they do, the fear of losing access to treatment impinges on the client’s capacity to make a complaint.
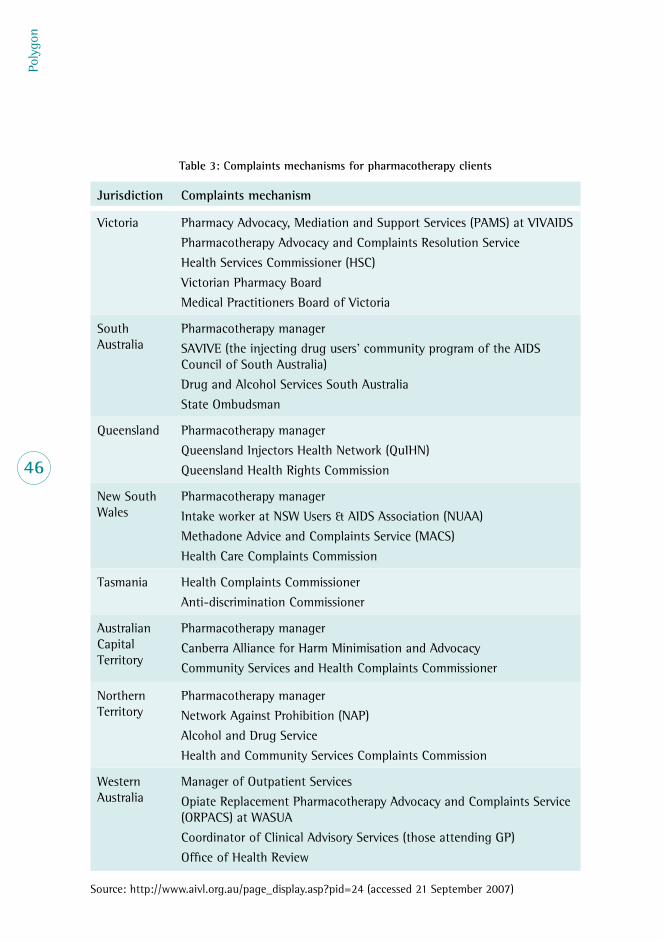
Poly
gon
46
Table 3: Complaints mechanisms for pharmacotherapy clients
Jurisdiction Complaints mechanism
Victoria Pharmacy Advocacy, Mediation and Support Services (PAMS) at VIVAIDS
Pharmacotherapy Advocacy and Complaints Resolution Service
Health Services Commissioner (HSC)
Victorian Pharmacy Board
Medical Practitioners Board of Victoria
South Australia
Pharmacotherapy manager
SAVIVE (the injecting drug users’ community program of the AIDS Council of South Australia)
Drug and Alcohol Services South Australia
State Ombudsman
Queensland Pharmacotherapy manager
Queensland Injectors Health Network (QuIHN)
Queensland Health Rights Commission
New South Wales
Pharmacotherapy manager
Intake worker at NSW Users & AIDS Association (NUAA)
Methadone Advice and Complaints Service (MACS)
Health Care Complaints Commission
Tasmania Health Complaints Commissioner
Anti-discrimination Commissioner
Australian Capital Territory
Pharmacotherapy manager
Canberra Alliance for Harm Minimisation and Advocacy
Community Services and Health Complaints Commissioner
Northern Territory
Pharmacotherapy manager
Network Against Prohibition (NAP)
Alcohol and Drug Service
Health and Community Services Complaints Commission
Western Australia
Manager of Outpatient Services
Opiate Replacement Pharmacotherapy Advocacy and Complaints Service (ORPACS) at WASUA
Coordinator of Clinical Advisory Services (those attending GP)
Office of Health Review
Source: http://www.aivl.org.au/page_display.asp?pid=24 (accessed 21 September 2007)

The issues
47
The complaints mechanisms perform an impor-tant function in enabling/empowering clients to have an independent third- party advocate on their behalf. The pharmacotherapy- specific consumer- led complaints mechanisms, how-ever, do not have investigatory or enforcement powers. Matters are ultimately referred to a more generic health complaints system, such as the relevant practitioner professional body or the Ombudsman, especially where they concern clinical practice issues rather than administrative issues. Jurisdictions may be reluctant to act on complaints as this may mean stopping a prescriber with a large caseload from continuing to work in this area. Given the shortage of prescribers, this would result in a major logistical problem.
During the consultation process a key in-formant suggested that we look to the Men-tal Health Review Tribunals operating in each of the jurisdictions as mechanisms that are more supportive of the client. These tribu-nals have a wide range of powers enabling them to make and review orders (and to hear appeals) about the treatment and care of people with a mental illness.44
Client involvement in treatment decision making is a longstanding issue in pharma-cotherapy maintenance programs. Although fundamental to good clinical practice, some perceive client involvement to be problem-atic in the case of pharmacotherapy main-tenance. We provide below three examples where there is contention about meaningful client input. There is an argument that clini-cians are trying to act in the long-term inter-ests of clients, whereas clients may perceive the inflexibility in terms of the asymmetric power relationship.
The first example is in relation to dose levels. We are aware of circumstances where dosing levels are not always negotiated with the cli-ent — sometimes increased, sometimes de-creased against the client’s wishes. There are also instances of clients being punished for illicit drug use with dose reductions (a para-doxical intervention).
The second example is the choice of medica-tion. Three types of medication are now avail-able in Australia: methadone, buprenorphine and buprenorphine-naloxone.45 In theory both prescribers and clients now have greater choice. The client should be involved in the decision, but in some circumstances the regu-lations may force a medication shift — as in the example of transferring from buprenorphine to buprenorphine-naloxone for unsupervised dosing. Forced transfer to another medication may not represent meaningful client involve-ment in treatment decisions.
The third and final example is the medication formulation decision. Methadone syrup and Biodone are the two formulations of meth-adone that are prescribed in Australia. The Biodone Forte available in Australia is the same strength as methadone syrup (5mg = 1ml) but has fewer additives than metha-done syrup. They are both fully subsidised by the federal government. There is no evi-dence of any difference in pharmacokinetics or pharmacodynamics. Increasingly pharma-cists are using Biodone. However, some cli-ents believe that methadone ‘holds them better’ and there is a preference for metha-done over Biodone. Practical constraints can impede the extent of client choice. In this example, the implications for a pharmacy are both practical and financial (the pharmacy would have to stock two forms of metha-done, maintain two drugs of dependence
44 As an example, see <http://www.mhrt.nsw.gov.au/> accessed 24 May 2008.
45 We understand that not all three medications are available in every Australian jurisdiction.

Poly
gon
48
registers, and spend more time handling two different forms of methadone).46 The pre-scribing doctor has no control over these things.
The three examples above highlight the deli-cate balance between the provision of the best pharmacotherapy treatment as judged by the practitioner and meeting the client’s wishes. In many circumstances, these issues are part of the normal exchange between doctor and client and require good commu-nication skills, trust and compromise. What might appear to be a case of lack of client choice or collaborative clinical decision mak-ing can be the result of a complex array of systems factors, such as regulations, phar-macy business requirements and the like.
3.12 Keeping people in treatment (retention)A substantial body of literature suggests that, to effect a meaningful reduction in drug use, clients need to be retained in treatment for as long as it takes to make often consider-able lifestyle changes (usually many years). Even before those lifestyle changes are made, research shows that the longer a client remains in treatment, the better the treatment outcome (Corsi, Kwiatowski & Booth, 2002; Simpson, Joe, George & Brown, 1997; Simpson, Joe, Rowan-Szal & Greener, 1997).
Summary of issue: meaningful consumer involvement
• Meaningful consumer involvement in the Australian pharmacotherapy maintenance program is essential.
• Consumer-led complaints mechanisms have been an important part of consumers having a voice.
• Consumers should also be engaged in policy development.
• A longstanding issue is the balance between client preference and medical decision making. In most instances these coincide. Effective communication and a good work-ing relationship between client and doctor are important.
46 Notwithstanding that pharmacies do stock multiple brands and generics of other drugs and aside from inconvenience/time, there is no other reason for pharmacies not to stock both methadone and Biodone.

The issues
49
However, the extent to which retention per se should be encouraged as a primary treat-ment outcome is unclear. It is important to appreciate that retention in treatment is not necessarily the client’s goal. Most clients do not want long-term maintenance treatment lasting for many years. The study by Lenne, Lintzeris, Breen et al. (2001) demonstrated that the vast majority of Australian clients (70%) wanted to cease maintenance treat-ment, but very few of them met clinical criteria indicative of successful treatment termination. Likewise, Lintzeris, Pritchard & Sciacchitano (2007) noted client expectations consistent with brief, time-limited mainte-nance treatment.
Therefore concentrating upon improving re-tention needs to be balanced against cli-ent preference for short programs and more attention to approaches that assist clients to successfully end methadone treatment (see 3.18).
The average retention in pharmacotherapy programs in Australia is substantially less than a year, from the perspective of a treat-ment episode. Analysis of Australian Treat-ment Outcome Study (ATOS) data found that between 36 per cent and 44 per cent of methadone/buprenorphine clients remained in continuous treatment for 12 months, de-pending on whether those who were un-available for interview at 12 months were counted as having terminated (Teesson et al., 2006).
The typical pattern of treatment usage in Aus-tralia is one where clients cycle through multi-ple episodes of care: that is, clients commence then cease treatment reasonably rapidly. In New South Wales the average length of the first episode of treatment has been measured as only six months (Bell, Burrell, Indig & Gil-mour, 2006). The same research finds that
half of those who leave treatment will have returned to treatment within 12 months, and this cycle continues. Bammer et al.’s (2000) survival analysis of Australian Capital Terri-tory administrative data suggests that there was no significant difference in the length of the first and second episodes of pharmaco-therapy treatment. Nor was there a relationship between the length of time between episodes of treatment and the ensuing length of time in treatment.
One pressing research question is whether the outcomes associated with receiving treatment in multiple relatively short episodes of care are significantly different to the outcomes from one extended episode of care. To rephrase the question: Is treatment outcome driven only by continuous time in treatment or does the cumulative amount of treatment also improve outcomes? This is an impor-tant question because it speaks to whether policies should focus on retaining clients for longer on a continuous basis, or alternately focusing on cumulative retention and ease of re-entry. These two policy options (retention versus accessibility) have significant implica-tions which can counteract each other. For example, improving continuous retention, without expanding treatment places or leav-ing a proportion of treatment places unfilled to maintain some continuity for those that have slipped out of treatment, will result in less accessibility for those currently outside the program.
The literature is not clear on this point. For example, in contrast to Bammer et al. (2000), a United States study found that repeat epi-sodes of treatment were of shorter dura-tion than the initial episodes (Strike, Gnam, Urbanoski et al., 2004). In this case, efforts to retain clients when they first appear for treatment are very important. Zhang, Fried-mann and Gerstein (2003) found that clients

Poly
gon
50
with more than three prior treatment epi-sodes showed significantly less change in their drug use compared with those with more sustained treatment.
Another way of thinking about the cycle of treatment entry is to place it in the con-text of the drug-using career. An American study of the treatment process concluded that drug treatment often follows a similar pattern to drug use, with cycles of cessation and resumption occurring over extended pe-riods of time. The authors claim that these multiple treatment episodes may be better understood as parts of a cyclic process of re-covery rather than as failed efforts (Hser, An-glin, Grella et al., 1997).47 In further analyses, Hser, Grella, Chou and Anglin (1998) found that cumulative treatment experience was associated with increased length of stay in the current treatment episode and reduced use of heroin. It was suggested that reduc-tion in heroin use may be related to the user acquiring an increasing number of coping
skills throughout his or her treatment ca-reer. This enhanced skill set was thought to assist users in their successful reduction of heroin use.
In summary, one consideration is whether continuous treatment or cycling through multiple episodes is associated with better treatment outcomes. As discussed above, the evidence is equivocal on this point. There are other considerations too. Multiple episodes of treatment are often difficult to coordinate as clients often go to different service providers for each episode. This has implications for continuity of care. The impact on the capacity of the system is also likely to be complex. It is probable that continuous treatment will result in fewer treatment places for new clients. Under a model of continuous treatment, at any point in time there would be more clients in treatment, using more staff and resources. The increase in demands on staff would be tempered by any reduction in the staff time/resources needed by long-term clients.
Summary of the issue: retention
• Retention is viewed as a measure of successful treatment outcome.
• Is there evidence to support a focus on continuous time in treatment, or is cumulative time in treatment equally predictive of good outcome?
• How can we balance the desire for higher retention on behalf of practitioners, because of its association with better treatment outcomes, with client preferences for shorter treatment?
• What do we know about treatment cycling? (e.g. length of each episode, time between episodes, and outcomes for each episode)
• How can decision makers balance good program accessibility for new clients with improv-ing retention for existing clients?
47 Note that these researchers covered all drug treatment, including episodes of detoxification and so on.
The issues
51
3.13 Child protectionAgainst the background of heightened con-cern about child abuse and neglect there has been substantial activity in the child pro-tection arena in the last five years or so. In almost all States and Territories there has been a review or inquiry about child pro-tection services. As a result there have been major organisational changes accompanied by new funding commitments (Ainsworth & Hansen, 2006).
In this context of increased awareness of child abuse and neglect, the association between parental drug use and children’s welfare has also come to the fore. For example, in New South Wales parental substance abuse has been increasingly emphasised as a child protection concern in recent years (National Drug and Alcohol Research Centre, 2008). Particular attention was paid to parental substance misuse in the Report of Reviewable Deaths in 2005 (New South Wales Ombuds-man, 2006).48
While we acknowledge that both mothers and fathers play a crucial role in a child’s upbring-ing, research in the area of parental drug use and children has concentrated on mothers. There is a widespread belief that mothers who inject drugs are by definition poor parents, that drug use is antithetical to good parent-ing. However, there is research evidence to suggest that this belief is largely unjustifiable. In a comparison of four groups of mothers (mothers who inject drugs; mothers on low incomes; mothers who were mobile, socially isolated women whose partners were employed in the Australian Defence Forces and who frequently moved; and women with medium
and high incomes), the difficulties of mother-hood cut across all four groups (Banwell & Bammer, 2006). All the mothers, irrespective of drug use, found it difficult to live on a low income, to endure social isolation or to be at home with young children, at least some of the time. However, drug-using women tend to be blamed for these difficulties in ways that other mothers are not, and they do not receive the social support to alleviate their difficulties (Banwell & Bammer, 2006). Research demon-strates that heroin- using mothers employ a range of strategies to protect their children from their own heroin use (Richter & Bammer, 2000).
Those comments notwithstanding, a body of research has identified that children liv-ing with at least one parent using illicit substances have relatively poor outcomes. They are more likely to be subject to child abuse and neglect and tend to experience early conduct and behavioural problems, school failure and adolescent substance use (see Dawe, Frye, Best et al., 2007; Dawe & Harnett, 2007, for a review of the literature). Families with drug-using parents also tend to be in poverty, experiencing social isola-tion and financial difficulties. The mothers, at least, have high levels of depression and anxiety, lack parenting skills, have been poorly parented themselves, neglect their children and have relationship problems (see Banwell and Bammer, 2006, for a review of the lit-erature). Research has largely been unable to attribute the poor child outcomes, including child maltreatment, to any one factor. They are seen as a result of the ‘complex interplay between drug use, maternal psychopathol-ogy, parenting practices, family environment
48 The definition of reviewable deaths includes children, or siblings of children, who were reported to the New South Wales Department of Community Services in the three years before they died (New South Wales Ombudsman, 2006).
Poly
gon
52
(including spousal relationship and the avail-ability of social support), and socioeconomic factors such as unemployment and poverty’ (Dawe & Harnett, 2007, pp.381–382).
There is no clear evidence that pharmacother-apy maintenance treatment in and of itself leads to improved family dynamics and a re-duction of child behaviour problems for those families where drug use is an issue. The only relevant study — Kolar, Brown, Haertzen & Michaelson (1994) — found equivocal results.49
With that context in mind, tension between the child protection and pharmacotherapy maintenance sectors arises in three main arenas: take-away policy; mandatory report-ing; and parenting interventions.
Take-away policy
Over the life of pharmacotherapy mainte-nance programs there have been reports of child deaths relating to methadone poison-ing.50 This issue has been particularly note-worthy as a topic of concern in New South Wales. The methadone- related deaths that have been reviewed in that State show that in roughly half of the cases the source of the methadone was the take- away doses of the parents and in the other half black- market methadone (New South Wales Child Death Review Team, 2006, 2007; New South Wales Commission for Children and Young People, 2008). In response to these deaths the New South Wales child protection arena has fo-cused its attention on take-away policy with
calls for reform ranging from removal of all take-away dispensing to stricter controls on the access of methadone for those with re-sponsibility for children (New South Wales Ombudsman, 2006, 2007).
There is a risk of consumption of take-away doses of methadone by small children. There-fore the provision of regular take- away doses may require the prescribing doctor to be satis-fied that the patient understands the potential risks to children of accidental ingestion and is able to provide adequate storage arrange-ments for take-away doses (New South Wales Department of Health, 2006b, p.45).
A 2006 survey of 87 public patients receiving take-away doses at community pharmacies in Sydney revealed that all but one were aware of the risks of methadone ingestion by small children. Eighty-seven per cent had discussed safe storage with a health professional and over 80 per cent stored their take-away doses in a cupboard, wardrobe, medicine cabinet or other secure box (Winstock & Lea, 2007).
The New South Wales clinical guidelines (New South Wales Department of Health, 2006a, p.77) advise that:
when assessing eligibility for takeaway doses, it is important to consider the safety and welfare and wellbeing of any children within the patient’s care. This may include a patient’s own children, children living at the same residence, or children to whom the patient has access.
49 There is a growing literature on the addition of parenting programs to existing methadone maintenance treatment which shows improved parental outcomes. For example, see Dawe et al., (2007); Catalano, Gainey, Fleming et al. (1999) discussed below.
50 The total numbers of deaths are unclear.
The issues
53
Mandatory reporting
Mandatory reporting of suspected cases of child abuse and neglect is now in place in all Australian States and Territories, with the exception of Western Australia (Australian Institute of Health and Welfare, 2008b).51 In recent years there have been substan-tial increases in the number of mandatory reports. In New South Wales at least, this is regarded as more indicative of net widening than of increases in the incidence of child maltreatment. Concurrently the number of non-mandatory reports has risen signifi-cantly, as has the number of reports per child (National Drug and Alcohol Research Centre, 2008). ‘One explanation for this may be that increased scrutiny of the child protection system … [has increased] the number of “false positives” in the system: those work-ing within the child protection system may be experiencing increased fear of failing to identify a genuine case of child maltreatment’ (National Drug and Alcohol Research Centre, 2008, p.3).
Women drug users who are also mothers typically experience marginalisation … the main form of assistance they receive is scrutiny of their parenting practices and the subsequent removal of their children — children who often provide a key source of stability and self-worth in their other-wise chaotic lives. (Dawe et al., 2007, p.76)
A potential downside of mandatory reporting is that parents may be discouraged from en-tering treatment for fear of child protection involvement (Richter & Bammer, 2000, for example). The New South Wales Commis-sion for Children and Young People (2008), in its submission to the current New South Wales inquiry into child protection services, stressed the importance of improving the access of parents to treatment without in-volving the Department of Community Serv-ices. The submission includes a proposal for service providers to be able to respond to the needs of vulnerable families without jeop-ardising relationships by making unnecessary mandatory reports.
Opportunities for intervention
Pharmacotherapy maintenance treatment does provide opportunities to support par-ents. A number of studies have found evi-dence for improvement in parenting skills following interventions designed to improve family functioning, whereas the parenting skills of those on pharmacotherapy treat-ment alone remain unchanged (Catalano et al., 1999; Dawe & Harnett, 2007; Luthar & Suchman, 2000).
The ANCD-funded research into drug use in the family (Dawe et al., 2007) makes a series of recommendations for good prac-tice, including principles for organisations, clinicians and treatment content.
51 A major report for the Western Australia Child Protection Council concluded that there was no national or international evidence that mandatory reporting was an effective way to reduce the incidence of child abuse and neglect (Harries & Clare, 2002).
Poly
gon
543.14 Stigma in the Australian pharmacotherapy systemDespite being a treatment program, from the outset the methadone maintenance program was stigmatised by the belief that methadone treatment merely substitutes one drug for another (Joseph, Stancliff & Langrod, 2000). In keeping with the marginalisation of illicit drug users in today’s society, ‘stigma and dis-crimination are routine aspects of the daily lives of many people who use illicit drugs, resulting in poor treatment, no treatment or abusive treatment at the hands of health, legal and social services’ (Madden & Cavaleri, 2007).
Discrimination of clients is largely endemic in the health sector, the workplace and the social welfare system. For example, hepatitis C-related discrimination was found to occur across many areas of public life. It is widespread in health care settings and common in employ-ment. The experience of discrimination acts as a deterrent to people accessing the health system and makes it more difficult to find and keep employment (Anti- Discrimination Board of New South Wales, 2001).
Stigmatisation has been shown to have substantial detrimental impacts on the ef-fectiveness of the pharmacotherapy treat-ment system, discouraging new entrants and tainting clients’ experiences of treatment. The American National Alliance of Metha-done Advocates states that stigma, prejudice and discrimination are the greatest barriers to recovery confronting methadone clients today (Woods, 2001). Potential clients them-selves internalise this stigma and prejudice. As Wodak (2002, p.527) claims: ‘Some of the complaints about methadone by treat-ment consumers also reflect community con-tempt of drug use that has been internalised by heroin injectors.’ Indeed Wodak (2002) argues that many of the deficiencies of methadone treatment are the consequence of community fear and ‘loathing’ for people who choose to use heroin.
Public opinion towards pharmacotherapy is generally negative. Nonetheless the commu-nity prefers that the opioid- dependent per-son be in treatment rather than dependent on heroin. Only a small minority (less than 10 per cent) of the 2007 National Drug Strat-egy Household Survey respondents supported
Summary of issues: child protection
• The prevalent assumption is that injecting drug users are poor parents.
• There is a complex interplay of factors that combine poor parenting with social dep-rivation, injecting drug use, poor coping skills and so on.
• Some parents who inject drugs endeavour to minimise the risks for their children.
• Clinical judgement of potential risk to children from unsupervised doses needs to be made sensitively and carefully.
• Mandatory reporting may be a disincentive to presenting for treatment, yet treatment provides the opportunity for parenting support.
• Some evidence suggests that pharmacotherapy treatment alone has no impact on parent-ing skills, but there have been positive outcomes associated with interventions designed to improve family functioning attached to treatment.

The issues
55
regular illicit drug use while over half of the respondents supported measures designed to reduce the problems associated with her-oin use. The level of support for methadone maintenance programs (68%) falls beneath abstinence-based measures, such as rapid detoxification therapy (79%) and use of nal-trexone (75%), but is somewhat above meas-ures designed to limit harms associated with heroin use, such as needle and syringe pro-grams (67%) and regulated injecting rooms (50%) (Australian Institute of Health and Welfare, 2008a: Table 4.4).
Practitioners’ attitudes towards drug users are of more concern than the general pub-lic’s attitude, inasmuch as they represent direct stigma within the program. Australian studies, for example, have documented the negative stereotypical views held by medi-cal practitioners about patients using illicit drugs (Jacka, Clode, Patterson et al., 1999; Roche, 1997). Gjersing, Butler, Caplehorn et al. (2007) found that the level of disapproval of drug use among correctional health staff was higher than in the community.
A number of examples of discrimination and stigma were raised during the consultation processes resulting from the issues paper. For example, in some pharmacies pharmacother-apy clients are forced to wait and are served last, despite arriving first and paying for the
services. Some clients felt that staff lacked empathy. Clients told of ‘punishments’ in the form of dose refusals. Consumers also felt that police presence around pharmacotherapy clin-ics was problematic, while acknowledging the need for police to have access to offenders. The practical implications of stigma include the fact that clients are reluctant to readily identify themselves as recipients of mainte-nance pharmacotherapy. This can then create problems with dispensing sites, as these clients would prefer not to be dosed at their local pharmacy. This issue is notable in rural areas.
There are no government-enforced guide-lines or codes of conduct for practitioners providing pharmacotherapy treatment. Clients are subject to the individual practi-tioner’s judgements and opinions. Consumers noted inconsistent application of clinic rules, citing ‘different decisions on different days with different staff’. This does not encourage faith on behalf of the client nor represent good care planning. In turn, these factors can lead to premature termination of treat-ment by the client. Research conducted in the United States indicates that the qual-ity of the relationship between client and practitioner, the range of services delivered, and consumer satisfaction ratings directly increased program retention (Simpson et al., 1997).
Summary of issue: stigma
• Stigma and discrimination against pharmacotherapy maintenance programs are common.
• Pharmacotherapy clients also suffer from stigma and discrimination.
• Specific examples of discrimination were reported to this research team.
• Stigma may have an impact on discouraging entry to treatment, poor treatment progress and premature treatment termination.
• There has been no systematic research examining the extent of stigma or its impacts in the Australian pharmacotherapy treatment system.
Poly
gon
56
3.15 Creating and sustaining the workforceThe Australian pharmacotherapy service sys-tem depends crucially on having sufficient practitioners (prescribers and dispensers). There appear to be insufficient numbers to meet demand — as assessed by waiting lists for programs and difficulties with accessibil-ity in particular locations. In addition, there is concern that the workforce is ageing, and that new younger prescribers are required. Just as the clinical population is marginal-ised, the workforce — prescribers, pharmacists and counsellors — may also feel marginal-ised. Pharmacotherapy maintenance could be better integrated into the mainstream of medical service provision by encourag-ing regular medical practice arrangements; building relationships between GPs and spe-cialists; creating dispensing as a normal ac-tivity in pharmacies; and training as part of mainstream medical education.
GPs are already overburdened and take in-creasing responsibility for all manner of public health care, especially screening and assessment. This may discourage them from prescribing pharmacotherapies. Research ex-amining the factors associated with GP re-luctance to treat drug users suggests that to be willing to work with drug users GPs need, at the very least, to be adequately trained and to have quality support from special-ist drug treatment services. Still, a survey of GPs from outer London concluded that, even with training and support, GPs were unwill-ing to work with drug users (Deehan, Taylor & Strang, 1997). Less than 10 per cent felt that primary care was an appropriate setting for working with drug users, and the provi-sion of access to, or more support from, the
community drug team would make less than one-third more willing to work with drug users. In contrast, a survey of GPs from greater Manchester found that more than half, when focused on treating opiate users, felt that the treatment of opiate users was within their competence and nearly 80 per cent felt that access to local community drug teams would encourage treatment (Davies & Huxley, 1997). Even if such access to support were to be pro-vided, over 60 per cent felt that they would need more training, but were confident that this training would further encourage them to treat drug- dependent people.
Most jurisdictions have been actively endeav-ouring to recruit new prescribers (general medical practitioners) into the pharmaco-therapy programs. It is a general require-ment that prescribers be trained. (This issue is discussed below.) In New South Wales a GP can prescribe to up to five patients with-out training, although few exercise this op-tion. There appear to be few concerns about the availability of training programs. Not all those who do attend training become pre-scribers. This is consistent with international experience, where approximately one-third of GPs who complete the Royal College of General Practitioners Diploma in Substance Misuse in the United Kingdom do not pre-scribe substitution treatment, and a similar proportion of United States doctors com-pleting the Food and Drug Administration training program for buprenorphine do not take up buprenorphine prescribing within the next two to three years. But failure to prescribe does not necessarily imply failure of training. Some GPs may choose to complete the training in order to support a colleague (e.g. holiday cover) or for their own profes-sional development.52
52 One of the main reasons GPs get involved is so that they can satisfy their obligations to undertake continual professional development (Robert Ali, personal communication, 5 November 2008).

The issues
57
Jurisdictions have engaged in a number of strategies to encourage practitioner partici-pation. One mechanism is through incentive payments. Incentives have been considered for both pharmacists and prescribers as one way to encourage greater participation in the program. By way of example, in New South Wales new pharmacies dispensing pharmaco-therapies receive a once-only incentive pay-ment of $1100 (including GST). Both new and existing pharmacies are eligible to re-ceive an incentive of $110 per client twice a year for clients dosed continuously for two months prior to 30 April and 31 October each year (for a maximum of 20 clients).53 The Australian Capital Territory Govern-ment subsidises community pharmacies to the value of $15 per week per client.54 Tas-mania also provides incentive payments to pharmacists.
We could not locate details of any incentive payments to prescribers. However, training GPs in ways to maximise income from phar-macotherapy clients via Medicare has been suggested as a strategy in New South Wales.
We explore below in more detail two poten-tial areas for change:
• training requirements
• regulations.
Training requirements
All prescribers in Australia are required to undertake some form of additional train-ing in order to prescribe opioid pharmaco-therapies. One possibility is the adoption of a more flexible system which does not re-quire GPs to receive additional training to prescribe opioids (as in the United Kingdom, for example). There are clearly a significant
number of issues that would require con-sideration under this scenario, not least of which is quality assurance and clinical care standards.
There is no unambiguous answer to the question of whether training results in im-proved practice and better treatment out-comes. Observational studies of training suggest that it has little impact (see Strang, Hunt, Gerada & Marsden, 2007). The pro-duction and dissemination of clinical guide-lines, however, do appear to have produced significant change in United Kingdom pre-scribing over a 10-year period (Strang, Man-ning, Mayet et al., 2007). Is it plausible that dissemination of clinical guidelines in the absence of training programs is a sufficient strategy to improve practice?
A randomised study by Strang, Hunt et al. (2007) found a modest effect for training of general medical practitioners in the manage-ment of drug users. Those randomised to the training demonstrated positive attitudes and were more actively involved in treating drug users. Australian research by Lintzeris, Ritter, Dunlop & Muhleisen (2002) demonstrated improvements in knowledge with training and subsequent uptake of buprenorphine prescribing, but clinical outcomes were not assessed.
It is possible that the requirement for training may impact upon availability of services. The introduction of buprenorphine- naloxone pro-vides a good example of the impact of training requirements: the rates of buprenorphine- naloxone prescribing are higher in those jurisdictions where there were no additional training requirements placed upon prescrib-ers. In Victoria, where no additional train-ing was required, the proportion of clients
53 Source: <http://beta.guild.org.au/nsw/content.asp?id=1081> accessed 12 September 2007.
54 Source: ACT Health, Alcohol and Other Drug Policy Unit (2005).
Poly
gon
58
on buprenorphine- naloxone is significantly higher than in New South Wales, which has a compulsory training program for doctors to prescribe buprenorphine- naloxone.
A more recent development (since 2002) in the organisation of addiction treatment services is the establishment of the Fellow-ship of the Australasian Chapter of Addic-tion Medicine (FAChAM) as part of the Royal Australasian College of Physicians. There are approximately 200 FAChAM specialists, many of whom hold specialty accreditation with other disciplines, including Psychiatry, Inter-nal Medicine or General Practice. While at present there are no Medicare rebate items specifically identified for FAChAM special-ists, an application for these is in process. Should these Medicare items be created, the potential will exist to change the way in which general practitioner- based prescrib-ing is undertaken.
One of the barriers for GPs to become involved in pharmacotherapy maintenance treatment is that they effectively have to practise in isolation. Their capacity to refer complex or ‘difficult’ clients to special-ist public clinics is constrained by various obstacles, including waiting lists and inac-cessibility of consultancy services at public clinics. In effect, this is an area of medicine unlike most others. Many GPs are prepared to take on management of chronic conditions (such as mental health, diabetes etc) in the knowledge that they have access to a large specialist sector (psychiatrists, physicians). The introduction of FAChAM specialists will allow for similar networks of GPs supported by addiction specialists. Under Australia’s public clinic models there has been no engagement between GPs in the community and specialist
practitioners in the public clinics. Such an interaction would also provide the oppor-tunity for alternative shared-care models between specialists and GP prescribers, which could enable GPs (who have not necessarily undergone special training or accreditation, or do not desire to become involved in onerous methadone-related paperwork and regula-tions) to prescribe to stable maintenance clients in a shared-care arrangement under the supervision of a specialist prescriber. A key informant to the issues paper reported that the Royal Australian College of General Practitioners agrees that stepped or shared care is appropriate for general practice: gen-eral practice will provide support and care for uncomplicated cases while complicated cases will be managed by FAChAM doctors.
Regulations
The extent of regulation of the pharmaco-therapy program may also be worth consider-ing. Overall, when compared with other drug treatment programs and pharmacotherapy programs overseas, the Australian program is highly regulated (training requirements, caseload limits, permits for special conditions for treatment, requirements regarding start-ing dose, requirements regarding take-away doses). There are also costs associated with the level of regulation. In the United King-dom there is a significant amount of unsu-pervised methadone, many more deaths from methadone overdose, and lower methadone doses. The United States has even higher regulatory costs and even poorer coverage than Australia. Maybe Australia has the best balance. But we certainly need to make it much more attractive for doctors and phar-macists to work in this area.
The issues
59
Australia may profit from exploring alternate models that rely more on health practitioners other than doctors. As we noted earlier (3.4), nurse practitioner models enable GPs with minimal time to prescribe to a small number of methadone or buprenorphine clients by working with a nurse case manager who coordinates the treatment or with a nurse practitioner.
A final regulatory issue is the absence of national accreditation programs for doctors. Each State has its own system of accredi-tation and training. Mutual recognition of accreditation status and/or national accredi-tation systems could be considered.
3.16 Prisoners and pharmacotherapy maintenancePrisoners are entitled to the same level of medical care as people in the community at large. There are two compelling reasons for ensuring access to pharmacotherapy treat-ment for those in detention. The first is evi-denced by a study of male heroin users in detention in New South Wales. Although the study found that an individual’s drug use de-creased on entry to prison, there were added risks associated with drug use in prison. In-jecting drug use in prison is more likely to involve sharing needles and syringes than it is in the general community (Dolan, Wodak, Hall et al., 1996). The second reason is that shortly after release from prison the majority of heroin-dependent men use heroin (Dolan et al, 1996) and those who have had little exposure to opiates while in detention are vulnerable to overdose consequent on their
Summary of issue: workforce issues
• The overall availability of Australian pharmacotherapy programs is limited by the number of participating practitioners (both prescribers and pharmacists).
• Encouraging greater participation of practitioners is an important issue.
• Training programs for prescribers ensure clinical standards.
• Training requirements may act as a barrier to program participation.
• Incentives schemes have been unevenly deployed for pharmacists across Australia. No incentive schemes for GPs were identified.
• Australia may profit from exploring alternate models that rely more on health practi-tioners other than doctors.
• The overall extent of regulation of the program may discourage participation.
• These considerations need to be balanced against care standards.
• The more recent development of the addiction specialist (FAChAM) should be consid-ered in future service system planning and the opportunities this development repre-sents should be maximised.

Poly
gon
60
lower tolerance (Bird & Hutchinson, 2003; Darke, Ross, Zador & Sunjic, 2000). The provision of pharmacotherapy maintenance treatment to detainees could protect against such an outcome. Continuity of treatment and of dosage is key to the protective ca-pacity of pharmacotherapy treatment, and both these factors can be difficult to achieve upon discharge from prison.
Studies have shown that pharmacotherapy maintenance is an effective intervention within prisons, just as it is in the community (Dolan, Shearer, White et al., 2005; Dolan, Hall & Wodak, 1998; Dolan, Shearer, MacDonald et al., 2003; Haig, 2003; Shearer, Wodak & Dolan, 2004). Economic evaluation has also demonstrated that pharmacotherapy programs in prisons are cost-effective (Warren, Viney, Shearer et al., 2006).
All jurisdictions operate pharmacotherapy programs for inmates, although not in every prison. Some programs are also limited in terms of treatment places and others allow access only to those already enrolled in a community program (Black, Dolan & Wodak, 2004). Aus-tralian Institute of Health and Welfare figures for 2007 suggest that the jurisdictions most supportive of pharmacotherapy for inmates were Western Australia, New South Wales and South Australia. Close to 10 per cent of
pharmacotherapy clients were dispensed in cor-rectional facilities in each of these jurisdictions (Australian Institute of Health and Welfare, 2008). Dolan et al. (2003) also reported that some of those participating in a methadone trial in prison had been discouraged by health staff from remaining in or entering methadone treatment.
The risk of re-incarceration is reduced by 70 per cent if inmates on methadone mainte-nance treatment continue taking methadone for eight months upon their release (Dolan et al., 2005). How do different jurisdictions help people transition into community pro-grams once they leave prison? According to the NSW Health Justice Health Annual Report 2006–07, post-release care is arranged routinely for any inmate on a long-term pharmacotherapy program, such as metha-done or buprenorphine, to ensure continuity of care. In Victoria likewise, there has been attention to continuity of care for prison-ers at the point of release. 2007 saw the commencement of a pilot methadone and buprenorphine dispensing subsidy program for Victorian prisoners on their release from prison. Under the program Corrections Vic-toria pays for dosing fees at pharmacies approved to provide the services for the first four weeks after the prisoner is released, at a cost of $140.
Summary of issue: prisons and pharmacotherapies
• Prisoners are entitled to the same standard of care as community members.
• There are two compelling reasons for ensuring access to pharmacotherapy in prison: high risk of infectious disease transmission in prison; and high risk of post-release over-dose. Prison provides an opportunity to engage this population in treatment.
• Pharmacotherapy programs are available in Australian prisons, although not in every prison, and programs differ in their intake criteria which may prevent some people from gaining access.
• Areas of concern have been point of release and continuity of dosing for ex-prisoners.

The issues
61
3.17 Rural and remote issuesAround 6.5 million people — almost one-third of the population — live in what is referred to as regional and remote Australia (29.2% in regional areas; and 2.3% in remote and very remote areas: Australian Bureau of Statistics, 2008). Whereas Indigenous Australians com-prise 2.5 per cent of the Australian population, they make up 16 per cent of the population in remote areas and nearly half the population in very remote areas (Australian Bureau of Statistics, 2008). Hence, discussions of rural and remote issues go hand in hand with In-digenous issues.
The disparity between health service provision in urban, rural and remote areas of Australia is well recognised. The number of medical practitioners per head of population decreases with increasing geographic remoteness.55 This limits access to medical practitioners for peo-ple in rural and remote areas.
As a higher proportion of Indigenous Aus-tralians live in rural and remote areas, they are more likely to have to move or travel substantial distances in order to access medi-cal care (Australian Bureau of Statistics & Australian Institute of Health and Welfare, 2008). Indigenous access to and use of serv-ices depend not only on availability, but also on language skills, availability of interpreters, gender issues, physical set-up of the services, method of service delivery, sensitivity of staff to Indigenous issues, presence of appropriate Indigenous staff, racism, community owner-ship of services, and confidentiality (Carson & Bailie, 2004).
In 2000 the ANCD ran a number of forums in rural and regional areas. These forums were attended by a range of non- government and government sector representatives. Represent-atives from most areas said that the opiate problem was small but felt that it was increas-ing. Heroin was thought not to be common unless the location was within 2–3 hours of a capital city. There were reports of sporadic shipments of heroin to more rural and remote locations. However, it was thought that there could be greater levels of prescription diver-sion and misuse of methadone and morphine (Australian National Council on Drugs, 2001).
In a comparison of rural and metropolitan injecting drug users in New South Wales, Day, Conroy, Lowe et al. (2006) found no substantial demographic differences between the two groups. However, while almost all the members of both groups had used heroin and over half of both groups had used heroin within six months of the interview, the rural participants were far more likely to have used morphine. Half of them had used it in the previous six months compared with less than one-fifth of the metropolitan groups.
Despite the similarities in profile, the study found that access to services was signifi-cantly more limited in rural areas. Almost all the issues raised in this report are exac-erbated and compounded by being in a rural or remote location, including access to pre-scribers, access to dosing, costs associated with travel for the client, low levels of service providers willing to take up service provision, stigma and discrimination, and poor work-force support.
55 The supply rate of medical practitioners is measured by the full-time equivalent (FTE) rate per 100 000 population. In 2005 there were more than twice as many medical practitioners per person in major cities (335 FTE per 100 000) than in remote/very remote areas (148 FTE per 100 000) (Australian Bureau of Statistics & Australian Institute of Health and Welfare, 2008, Table 10.4).

Poly
gon
62
Day et al. (2006) found that their rural par-ticipants seemed more concerned with lack of knowledge about treatment and treatment options than with accessibility. Treatment was often accessible only by private car. Some participants had to hitchhike into town daily to receive methadone. Privacy was also a concern, especially since the participants felt that drug use is particularly stigmatised in rural areas. In light of this stigmatisation, par-ticipants also complained about attitudes of employees of pharmacies where methadone was dispensed and of drug services including prescribers and general practitioners.
A recent study of pharmacotherapy programs (Fraser et al., 2007) highlighted a number of features of rural service provision: the fra-gility of the services; concerns about staff burn- out; and difficulties accessing qualified professionals. They concluded that rural and
regional services required additional resources and funding in order to provide quality care. These concerns were also brought to light in the ANCD forums (Australian National Council on Drugs, 2001), during which it was also noted that services needed to be more responsive to the needs and issues of Indigenous Australians.
We did not source any creative innovations that would address the particular issues in rural and regional communities — the re-sounding call was for more resources. Other treatment models may be worth exploring, such as a roving dispensing bus that trav-els between regional towns on a daily basis. Other solutions could be generated through a concerted effort to engage rural, remote and Indigenous stakeholders in the pharma-cotherapy program.
Summary of issue: rural and remote issues
• Every point identified in this document needs to be specifically attended to in the context of rural and remote locations:
• affordability
• accessibility
• case management and collaborative care plans
• access to counselling and therapy services
• staff attitudes and stigma
• workforce development
• models of service delivery.
• Even less is known about unmet need in rural and remote locations compared to urban areas. It seems that pharmaceutical opioid use is more prevalent among rural and remote injecting populations.
• Service providers and service provision models need to be mindful of the needs of Indigenous Australians.
The issues
63
3.18 Clinical issuesA number of clinical issues were raised by key informants. We discuss them briefly in this section, but note that the majority of these are not concerned with the system per se but with individual clinical practices.
Polydrug use
Findings from the Australian Treatment Out-come Study (ATOS) underscore that, like their peers in other countries, pharmacotherapy clients are not just heroin/pharmaceutical opioid users, but are polydrug users. On entry to methadone maintenance treatment, clients had, on average, used 4.6 other drug types in the preceding month. The most com-monly used drugs, other than heroin, in the preceding month were tobacco (96%), can-nabis (70%), alcohol (55%), benzodiazepines (52%) and amphetamines (33%) (Ross et al., 2005). At two-year follow-up, the ATOS findings were that there was reduced use of other opioids and alcohol but sustained use of cocaine, amphetamine, cannabis and benzodiazepines (Darke, Williamson, Ross & Teesson, 2006). These data demonstrate that pharmacotherapy maintenance clients tend to be polydrug users, not only on entry to treatment but also while in treatment. Good clinical care will involve attention to their non-opioid drug use.
With an 80 per cent or greater rate of smok-ing among pharmacotherapy clients, smok-ing cessation programs seem an obvious and essential service. Programs that provide free nicotine replacement therapy for clients are likely to save lives given that 50 per cent of smokers die of a tobacco-related disease (Doll, Peto, Boreham & Sutherland, 2004).
Comorbidity
Co-occurring mental and/or physical health problems are almost the norm among pharma-cotherapy clients (Darke & Ross, 1997, Krausz et al., 1998; Mills et al., 2003). This adds complexity as treatment providers must be able to assess and either treat or refer clients to receive treatment for co-existing conditions.
Optimal dose
There has been much discussion about ‘opti-mal dosing’. There is a strong evidence base that higher pharmacotherapy maintenance doses are associated with better treatment outcomes (see Lintzeris et al., 2007, for a re-view). The principles of dose adequacy are to reduce or eliminate cravings, block or elimi-nate withdrawal, and diminish or reduce/eliminate the effects of ‘on top’ heroin use. These principles equate to methadone dose ranges of 60–100mg, as noted in the Aus-tralian clinical guidelines (Henry-Edwards et al., 2003); and buprenorphine dose ranges of 12–16mg (Lintzeris et al., 2006).
Research demonstrates that average doses in Australia are below those recommended. For example, the average dose in Victoria has been reported as 54mg methadone, with buprenorphine at 11.6mg (Lintzeris et al., 2007). A similar tendency towards low doses has been reported in the United Kingdom, the United States and Italy. However, there is jurisdictional variation around Australia. For example, the average New South Wales methadone dose is 80mg (Lintzeris et al., 2007). The main factor in low dose phar-macotherapy is client preference (Lintzeris et al., 2007). Lintzeris et al. (2007) found that most clients were satisfied with their

Poly
gon
64
dose. Another Victorian study (Ezard et al., 1999) reported that the majority of clients (75%) were satisfied with their doses, and levels of satisfaction were higher for those on lower doses. Of course, some clients would prefer higher doses (10% in Lintzeris et al., 2007). The main message from the limited research is that clients are generally satis-fied, but the majority are not being dosed in the medically ‘optimal’ range. Lintzeris et al. (2007) explored some of the reasons for client preferences for lower doses. The main factors appeared to be client concerns about medication side-effects, the desire by clients to reduce off methadone ‘as early as possible’, and the concomitant belief that lower doses were easier to withdraw from.
Transfers and the degree of mobility for clients
Clients (and providers) experience difficulties with temporary transfers as well as long-term or permanent transfers. There is reportedly poor coordination between jurisdictions. In addition to the relatively simple practicali-ties of arranging a temporary or long-term transfer to another jurisdiction, there are also client management issues, such as differ-ences in accessibility of unsupervised doses (a client cannot have take-away doses when on temporary transfer from another State, at least when transferring to New South Wales) and financial complications (it could be more expensive). International travel is even more complicated. It was suggested that tempor-ary transfers could be better facilitated if prescriptions were valid across jurisdictions.
Side-effects
More attention should be paid to the side-effects of methadone and buprenorphine. For many years client concerns about side-effects (e.g. osteoporosis, dental decay, ‘gets in my bones’, sexual functioning, sleep disorder, immune system problems, and cognitive func-tion) have been dismissed or not addressed by the service sector, yet this continues to be a major source of complaint by clients. Increas-ingly there is evidence to show that methadone in particular is associated with a range of side-effects which are not as apparent in other opioids such as morphine or buprenorphine (for example, Bliesener, Albrecht, Schwager et al., 2005; Krantz, Garcia & Mehler, 2005; Rapeli, Fabritius, Alho et al., 2007). While transfer to buprenorphine is an option for many clients experiencing methadone side-effects, it is not suited to all clients, and alternate full ago-nist substitution (e.g. slow-release morphine) could be reconsidered in Australia (Clark, Khoo, Lintzeris et al., 2002). There is little information available on the long-term effects of metha-done or of the effects of methadone on older people. The Australian cohort of people who have been in maintenance treatment for 20 years or more provides an ideal opportunity to conduct systematic research on these issues.
Cessation of treatment
Little attention has been paid to exit strategies for long-term clients who want to reduce their dose and ultimately cease treatment. Consum-ers reported that there was insufficient sup-port for withdrawal. Australian research has reinforced the finding that many pharmaco-therapy maintenance clients want to cease treatment (Lenne et al., 2001).56 Research has
56 In that work, 70 per cent of clients were interested in withdrawal. However, only 17 per cent were judged to have good withdrawal prognosis. Despite this pessimistic outlook, attention to improving client expectations and strategies for effective withdrawal from maintenance treatment is warranted.
The issues
65
shown that buprenorphine is an effective with-drawal medication (Lintzeris, Bell, Bammer et al., 2002) and more effective than clonidine, but may be of equivalent efficacy to metha-done (Gowing, Ali & White, 2006). Slow-release oral morphine is also an option. More atten-tion could be paid to successful reduction and cessation of pharmacotherapy maintenance.
At the same time, we also received disturbing reports of involuntary cessation of treatment. We were informed of ‘doses being withheld’ for three days due to poor behaviour, and of clients ‘stood down’ from methadone for a few days, and subsequently not re-inducted. Cessation or rapid reduction of methadone dose is recommended only in circumstances of
violence or assault, but not for other behav-ioural difficulties (Commonwealth of Australia, 2007; Henry-Edwards et al., 2003). Greater clarity on this issue may be required.57 It would be preferable that consequences for most behavioural difficulties not be directly associ-ated with provision of prescribed medications.
Urine drug screening
Greater unsupervised dosing requires im-proved capacity for monitoring and review of clients by service providers (e.g. urine test-ing, clinical reviews) to ensure that treat-ment decisions are based upon client needs and safety aspects. This in turn has funding implications.
Summary of issue: clinical issues
• Pharmacotherapy clients tend to be polydrug users, on entry to treatment and dur-ing treatment.
• Co-occurring mental and/or physical health problems are the norm, adding complex-ity to assessment and treatment.
• Although there is evidence that better treatment outcomes are associated with higher doses, Australian average doses tend to be below those recommended.
• More Australian research is required on the side-effects of methadone and buprenor-phine. Despite long-held client concerns about side-effects there is a small, but grow-ing body of evidence that methadone, in particular, is associated with side-effects not as apparent in other opioid use.
• Clients are concerned at the lack of support for withdrawal despite research evidence that many clients want to cease treatment.
• Greater clarity is required on the use of involuntary cessation of treatment as a disci-plinary tool. It is preferable that consequences of most behavioural difficulties not be directly associated with being dosed.
57 We understand that New South Wales plans to develop policy on withholding doses/treatment cessation with appropriate consumer input.
Poly
gon
66
3.19 Other issuesIn the course of conducting this research our consultations uncovered a number of issues not discussed above.
The sudden, and sustained, reduction in the availability of heroin in Australia in 2001 is a reminder to be alert to changes in drug use that impact upon the treatment service system and its capacity to be responsive. The subsequent reduction in heroin use and asso-ciated harms should not be interpreted as an opportunity to scale back or reduce opioid pharmacotherapy programs. Indeed there are two compelling reasons warranting further expansion and improvement of the services: the current system is unable to meet demand and, for some, the services are inaccessible; and the growing misuse of pharmaceutical opioids indicates a potential burgeoning in the demand for treatment.
Furthermore, there is no evidence that the heroin shortage resulted in a reduction in the demand for pharmacotherapy treatment. Degenhardt, Conroy, Day et al.’s (2005) analy-sis of New South Wales administrative data suggests that the repercussions of the heroin shortage on pharmacotherapy treatment are complex. The study found that the number of new registrations declined but re- registrations increased, as did retention in treatment. The authors concluded that older, more entrenched users reacted less to the shortage than did younger, less entrenched users, in terms of both their consumption of heroin and their demand for pharmacotherapy treatment.
We note the increase in methamphetamine use, and that many clients in pharmacother-apy maintenance in Australia have been or are using either stimulants or alternate opioids.
Australia does not have the full array of opi-oid pharmacotherapy maintenance options. For example, there is no prescribed heroin program, and morphine is infrequently used as a maintenance medication. There is in-creasing recognition that a minority of cli-ents do not respond to conventional opioid substitution treatment with methadone or buprenorphine. These clients continue to inject heroin and experience considerable drug-related harms, and often utilise con-siderable resources within a clinic. Several countries have developed injectable opioid treatment for this population, such as in-jectable methadone in the United Kingdom and more recently in Denmark, or injectable heroin (in the United Kingdom, Switzerland, Holland, Germany, Spain, Canada and Den-mark). New technologies are available that enable alternate routes of administration which may be feasible and effective in this client group, including intranasal and topical cutaneous patches. A reconsideration of al-ternate opioid pharmacotherapies and routes of administration is warranted for the group of people who do not respond to existing pharmacotherapy treatment.
Accessing treatment through diversion schemes
It is essential that there be fair and equitable access to treatment services through self-referral and through referral by the criminal justice system. There is a perception among practitioners that it is easier to gain access to treatment via referral through the crimi-nal justice system than via self-referral. This perception is supported by recent research (Winstock, 2007). In addition, there is concern that with the increase in court-mandated and police diversion into treatment, the impor-tance of informed consent and voluntary treatment uptake may be compromised.
The issues
67
Permit systems
Prescription and dispensing of drugs of dependence require regulation. The per-mit system, whereby all individuals seeking pharmacotherapy require state approval, is an appropriate regulation. Consumers do, however, express concerns about privacy and confidentiality, although there are no known cases where these have been breached. From the practitioners’ point of view, the regula-tions and associated paperwork can be quite burdensome.
National policy
The group responsible for developing and up-dating the National Pharmacotherapy Policy (the Methadone and Other Treatment Sub-committee of the Intergovernmental Commit-tee) and the group responsible for developing and updating the clinical guidelines (the Na-tional Expert Advisory Committee on Illicit Drugs) have both been disbanded. There is a lack of coordination in responding to issues at a national level. A national pharmacother-apy forum comprising representatives, includ-ing consumers, from each State and Territory would be valuable for policy and procedural development. A number of respondents to the issues paper suggested a national ap-proach to treatment: for example, nationally agreed practices in relation to take-away dos-ing, permits and accreditation of prescribers.
Poly
gon
68
3.20 Future researchIn conducting this research, we have identi-fied a significant number of research ques-tions. Here we have endeavoured to list those
research questions that we see as critically important, rather than simply list all the pos-sible research questions that arose through-out the project. We have provided a rationale for each research question.
Research questions Rationale, importance for policy
What are the implications of the inequitable dispensing fee system for clients and for the overall program?
Dispensing fees are the biggest concern for many stakeholders. We do not have good Australian research that demonstrates the impact of dispensing fees on clients’ lives, nor the impact on treatment outcomes. Such research would enable policy makers to more definitively attend to the inequity in the current system.
What is more important: cumulative retention or overall time in treatment?
This research question is important for policy decision making because it will allow either a concentration on keeping clients in treatment longer, or investment in encouraging people to return to treatment, irrespective of their length of stay.
What should be the balance between low-threshold public health service delivery models and high-threshold treatment models?
The relative balance between these two models will inform policy decision making about the best options for program expansion: in either the low- or high-threshold direction.
What is the relative balance between specialist clinics and primary care settings?
While there is a body of international research indicating that client outcomes do not differ between these two settings, and one study in Australia (the National Evaluation of Pharmacotherapies for Opioid Dependence) which similarly found no advantage to clinical outcomes in specialist settings over GP settings, some question remains in the minds of policy makers about whether they should expand primary care or specialist services. Ideally, there will be a balance between these two settings across all jurisdictions in Australia. Research on the relative balance would be valuable.
The issues
69
Research questions Rationale, importance for policy
To what extent are Australian programs efficient?
It is important for policy makers to know whether the current system is efficient and operating near capacity, or whether there are inefficient service models which can absorb greater numbers. This question is fundamental to the extent to which policy makers need to invest new resources into new services versus improving the efficiency of existing services. The research needs to be conducted objectively and independently from government.
What is the unmet demand for pharmacotherapy treatment?
Australia lacks an approach for assessing the demand for pharmacotherapies. Such an approach should have the capacity to answer the following questions: How many treatment places do we need now? How many will we need in the future? What is the best mix between low-intervention, primary care treatment places and high-intervention, specialist treatment places? With the changing profile of opioid use in our community (the increase in misuse of pharmaceutical opioids), how many new treatment places are required? Is there a relationship between the supply of pharmacotherapy treatment places and the demand for them? In particular, would an increase in supply and/or changes in the way that treatment is supplied encourage people into treatment and/or encourage people to stay in treatment for longer periods of time?
What role does a model of unsupervised treatment have in Australia?
The advent of buprenorphine-naloxone has provided an opportunity to consider a model of unsupervised treatment. To date, limited Australian research has endeavoured to understand the impact of unsupervised treatment on treatment outcomes. The results are equivocal. Further research that either confirms this, or provides more substantive evidence to move forward with new treatment models is required.
Poly
gon
70
4. ConclusionThe aim of this project was to examine the issues associated with pharmacotherapy main-tenance treatment in Australia. The key issues surround accessibility (access); affordability (cost); and availability (number of treatment places). In delineating these issues we found multiple interconnections. The extent to which treatment is readily available for any one indi-vidual is dependent on an available prescriber, the location of dispensing, the fees a person would incur, the reputation of the program and the extent to which the person feels stig-matised through participation in the program. The attractiveness of the program to a client and to practitioners is also dependent upon a shared understanding of treatment goals, the role of unsupervised dosing, and the avail-ability of counselling and case management. From a policy perspective, other considerations include the models of care that are available, diversion and medication misuse, the relative allocations between specialist and primary care settings, the efficiency of the program, fund-ing arrangements, and creating and sustain-ing the workforce. These interconnections are often complicating and some have come to dominate others, adding to the difficulties of identifying and discussing the interconnec-tions and resultant complexities.
The second part of this project, reported in ANCD Research Paper 19, was to explore the implications of affordability, accessibility and availability through the use of a system dynamics model. The model represents the flows into, around and out of treatment. The typical pattern of pharmacotherapy treatment usage in Australia is that of cycling through multiple episodes of care: that is, clients commence then cease treatment reasonably rapidly, but many return to treatment after
a break (Bell & Burrell, 2006). This cycling behaviour formed the basis of the model. In addition to the basic cycling behaviour, the model differentiates between prescrib-ers in public clinics, GPs (primary care) and the prison system; and dispensing in public clinics, community pharmacies and prison. The model was designed to characterise the pharmacotherapy system in the simplest pos-sible way while being recognisable to the stakeholders and able to depict the repercus-sions of the various policy scenarios.
The scenarios explored with the system dy-namics model were taken from this qualita-tive review of the issues. As discussed herein (see 3.3), one of the important current issues facing Australian pharmacotherapy programs is the dispensing fees incurred by clients. This is one of the issues we explore in our system dynamics model, through examin-ing scenarios for the costs to government of changes in the dispensing fee arrange-ments. Availability of treatment places is a critical issue for treatment access (see 3.4). We examine the potential impact of reduced numbers of treatment places on the system. Accessibility of services is also related to the numbers of people seeking treatment. One issue of concern is a potential increase in treatment-seeking from a new population of people dependent on pharmaceutical opi-oids. Finally, an issue identified here (see 3.1 and 3.2) was the potential trade-off between quality of services and availability of services: that is, the balance between more treatment places with lower quality of care versus fewer treatment places but with enhanced care. We explore this issue in the system dynam-ics model.

Conclusion
71
Australia has been regarded as an inter-national leader in the provision of opioid pharmacotherapy maintenance. Within this context, Australia should be proud of its phar-macotherapy maintenance programs. As one respondent to the issues paper commented, ‘Just having a pharmacotherapy program in Darwin is a miracle.’ Some countries do not have any programs; many countries have programs but the accessibility is extremely limited and client numbers are capped at very low limits (Solberg, Burkhart & Nilson, 2002). Some countries have programs that are highly punitive — any illicit drug use and the client is withdrawn from the program. Some countries provide methadone for withdrawal only (i.e. no maintenance).
Although it is hard to know the extent of the opioid-dependent population, Australia appears to have a relatively large share of this population in opioid pharmacotherapy maintenance compared to other countries.
Australia’s treatment approaches are also relatively sophisticated compared to other countries. Having government-funded user organisations (although their remit is focused on HIV prevention as a consequence of the funding apparatus) helps to keep the program accountable to drug users through the provi-sion of advocacy.
Any country that desires an effective and coordinated pharmacotherapy maintenance treatment service system must consider the longer-term perspective, including:
• unknown future demand
• the possibility of new medications and treatment approaches
• potential risks in the service systems.
Effective planning for a sustainable future for pharmacotherapy programs in Australia requires consideration and debate of the issues identified in this project.
Poly
gon
72
5. ReferencesACT Health, Alcohol and Other Drug Policy Unit (2005). Increasing Community Based Pharmacotherapy Places in the ACT: ACT Pharmacotherapy Program — issues and options. <http://www.health.act.gov.au/c/health?a=sendfile&ft=p&fid=1157423833&sid=> accessed 12 September 2007.
Ainsworth, F. & Hansen, P. (2006). Five tumultuous years in Australian child protection: little progress. Child & Family Social Work, 11(1): 33–41.
Amato, L., Davoli, M., Perucci, C., Ferri, M., Faggiano, F. & Mattick, R. (2005). An overview of systematic reviews of the effectiveness of opiate maintenance therapies: available evidence to inform clinical practice and research. Journal of Substance Abuse Treatment, 28: 321–329.
Amato, L., Minozzi, S., Davoli, M., Vecchi, S., Ferri, M. & Mayet, S. (2004). Psychosocial combined with agonist maintenance treatments versus agonist maintenance treatments alone for treatment of opioid dependence. Cochrane Database of Systematic Reviews [Online], Issue 4. Art. no.: CD004147. DOI: 10.1002/14651858.CD004147.pub3.
Anti-Discrimination Board of New South Wales (2001). Report of the Inquiry into Hepatitis C Related Discrimination. <http://www.lawlink.nsw.gov.au/lawlink/adb/ll_adb.nsf/pages/adb_hepatitis_c_enquiry#key>.
Auriacombe, M., Fatseas, M., Dubernet, J., Daulouede, J.P. & Tignol, J. (2004). French field experience with buprenorphine. American Journal of Addictions, 13 (Suppl. 1): S17–S28.
Australian Bureau of Statistics (2008). Australian Social Trends 2008. Cat. no. 4102.0. Canberra: ABS.
Australian Bureau of Statistics & Australian Institute of Health and Welfare (2008). The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples 2008. ABS cat. no. 4704.0; AIHW cat. no. IHW 21. Canberra: ABS and AIHW.
Australian Injecting and Illicit Drug Users League (2008). Treatment Service Users Project: final report. Canberra: AIVL.
Australian Institute of Health and Welfare (2007a). Alcohol and Other Drug Treatment Services in Australia 2005–2006: report on the National Minimum Data Set. Canberra: AIHW. <http://www.aihw.gov.au/publications/hse/aodtsia05-06-ronmds/aodtsia05-06-ronmds.pdf>.
Australian Institute of Health and Welfare (2007b). Health Expenditure Australia 2005–06. Canberra: AIHW.
Australian Institute of Health and Welfare (2008). National Opioid Pharmacotherapy Statistics Annual Data Collection: 2007 report. AIHW Bulletin no. 62. <http://www.aihw.gov.au/publications/index.cfm/title/10586> accessed 22 August 2008.
Australian Institute of Health and Welfare (2008a). 2007 National Drug Strategy Household Survey: first results. Canberra: AIHW.
Australian Institute of Health and Welfare (2008b). Child Protection Australia 2006–07. Canberra: AIHW.
Australian National Council on Drugs (2001). Rural and Regional: Alcohol and Other Drugs Consultation Forums: ANCD National Report. <http://www.ancd.org.au/publications/pdf/rural_regional_aod_report.pdf>.
References
73
Bammer, G., Battisson, L., Ward, J. & Wilson, S. (2000). The impact on retention of expansion of an Australian public methadone program. Drug and Alcohol Dependence, 58(1–2): 173–180.
Banwell, C. & Bammer, G. (2006). Maternal habits: narratives of mothering, social position and drug use. International Journal of Drug Policy, 17(6): 504–513.
Belenko, S., Patapis, N. & French, M.T. (2005). Economic Benefits of Drug Treatment: a critical review of the evidence for policy makers. Pennsylvania: Treatment Research Institute, University of Pennsylvania.
Bell, J. (2007). The role of supervision of dosing in opioid maintenance treatment. Background document prepared for 3rd meeting of Technical Development Group, for the WHO Guidelines for Psychosocially Assisted Pharmacotherapy of Opioid Dependence. Geneva, 17–21 September 2007.
Bell, J., Burrell, T., Indig, D. & Gilmour, S. (2006). Cycling in and out of treatment: participation in methadone treatment in NSW, 1990–2002. Drug and Alcohol Dependence, 81(1): 55–61.
Bell, J., Shanahan, M., Mutch, C., Rea, F., Ryan, A., Batey, R., Dunlop, A. & Winstock, A. (2007). A randomized trial of effectiveness and cost-effectiveness of observed versus unobserved administration of buprenorphine- naloxone for heroin dependence. Addiction, 102:1899–1907.
Bell, J., Ward, J., Mattick, R., Hay, A., Chan, J. & Hall, W. (1995). An Evaluation of Private Methadone Clinics. Research Report Series, no. 4. Canberra: Australian Government Publishing Service. <http://www.sarnia.com/groups/antidrug/wrldnews/methclnc.html>.
Bickel, W.K., Amass, L., Higgins, S.T., Badger, G.J. & Esch, R.A. (1997). Effects of adding behavioral treatment to opioid detoxification with buprenorphine. Journal of Consulting and Clinical Psychology, 65(5): 803–810.
Bird, S. & Hutchinson, S. (2003). Male drugs-related deaths in the fortnight after release from prison: Scotland, 1996–99. Addiction, 98(2): 185–190.
Black, E., Dolan, K. & Wodak, A. (2004). Supply, Demand and Harm Reduction Strategies in Australian Prisons: implementation, cost and evaluation. ANCD Research Paper 9. Canberra: Australian National Council on Drugs.
Black, E., Roxburgh, A., Degenhardt, L., Bruno, R., Campbell, G., De Graaff, B., Fetherston, J., Kinner, S., Moon, C., Quinn, B., Richardson, M., Sindicich, N. & White, N. (2008). Australian Drug Trends 2007: findings from the IDRS. Sydney: National Drug and Alcohol Research Centre.
Bliesener, N., Albrecht, S., Schwager, A., Weckbecker, K., Lichtermann, D. & Klingmüller, D. (2005). Plasma testosterone and sexual function in men receiving buprenorphine maintenance for opioid dependence. Journal of Clinical Endocrinology & Metabolism, 90(1): 203–206.
Boote, J., Barber, R. & Cooper, C. (2005). Principles and indicators of successful consumer involvement in NHS research: results of a Delphi study and subgroup analysis. Health Policy, 75(3): 280–297.
Booth, R.E., Corsi, K.F. & Mikulich, S.K. (2003). Improving entry to methadone maintenance among out-of-treatment injection drug users. Journal of Substance Abuse Treatment, 24(4): 305–311.
Poly
gon
74
Booth, R.E., Corsi, K.F. & Mikulich-Gilbertson, S.K. (2004). Factors associated with methadone maintenance treatment retention among street-recruited injection drug users. Drug and Alcohol Dependence, 74(2): 177–185.
Broome, K.M., Flynn, P.M., Knight, D.K. & Simpson, D.D. (2007). Program structure, staff perceptions, and client engagement in treatment. Journal of Substance Abuse Treatment, 33(2): 149–158.
Brown, L., Abello, A. & Harding, A. (2006). Pharmaceutical benefits scheme: effects of the safety net. Agenda, 13(3): 211–224.
Bruno, R. (2007). Benzodiazepine and Pharmaceutical Opioid Misuse and Their Relationship to Crime: an examination of illicit prescription drug markets in Tasmania. Tasmania: National Drug Law Enforcement Research Fund. <http://www.ndlerf.gov.au/pub/Monograph_22.pdf>.
Buckmaster, L. & Pratt, A. (2005). Not on my account! Cost shifting in the Australian health system. Research Note, no. 6, 2005–06. Canberra: Australian Parliamentary Library.
Caplehorn, J.R., Lumley, T.S., Irwig, L. & Saunders, J.B. (1998). Changing attitudes and beliefs of staff working in methadone maintenance programs. Australian and New Zealand Journal of Public Health, 22(4): 505–508.
Carson, B.E. & Bailie, R.S. (2004). National health workforce in discrete Indigenous communities. Australian and New Zealand Journal of Public Health, 28(3): 235–245.
Cartwright, W.S. (2000). Cost-benefit analysis of drug treatment services: review of the literature. Journal of Mental Health Policy and Economics, 3: 11–26.
Cartwright, W.S. & Solano, P.L. (2003). The economics of public health: financing drug abuse treatment services. Health Policy, 66: 247–260.
Catalano, R.F., Gainey, R.R., Fleming, C.B., Haggerty, K.P. & Johnson, N.O. (1999). An experimental intervention with families of substance abusers: one-year follow-up of the focus on families project. Addiction, 94(2): 241–254.
Cathcart, S., Patton, R., Hickman, M., Chiara, H. & Ashworth, M. (2007). Comparing population estimates for drug users, the prevalence of blood borne viruses and the provision of services in one London borough: evidence of a gap in provision? Drugs: Education, Prevention and Policy, 14(3): 205–215.
Chutape, M.A., Silverman, K. & Stitzer, M.L. (2001). Effects of urine testing frequency on outcome in a methadone take-home contigency program. Drug and Alcohol Dependence, 62: 69–76.
Clark, N., Khoo, K., Lintzeris, N., Ritter, A. & Whelan, G. (2002). A randomized trial of once-daily slow-release oral morphine versus methadone for heroin dependence. Drug and Alcohol Dependence, 66(1): S33.
Colameco, S., Armando, J. & Trotz, C. (2005). Opiate dependence treatment with buprenorphine: one year’s experience in a family practice residency setting. Journal of Addictive Diseases, 24(2): 25–32.
Commonwealth of Australia (2007). National Pharmacotherapy Policy for People Dependent on Opioids. Canberra: Australian Government. <http://www.health.gov.au/internet/drugstrategy/publishing.nsf/Content/A720C27C3AC3C149CA25717D000499A3/$File/pharmacotherapy.pdf>.
References
75
Connock, M., Juarez-Garcia, A., Jowett, S., Frew, E., Liu, Z., Taylor, R., Fry-Smith, A., Day, E., Lintzeris, N., Roberts, T., Burl, S.A. & Taylor, R. (2007). Methadone and burprenorphine for the management of opioid dependence: a systematic review and economic evaluation. Health Technology Assessment, 11(9): 1–190.
Corsi, K., Kwiatowski, C. & Booth, R. (2002). Predictors of positive outcomes for out-of-treatment opiate injectors recruited into methadone maintenance through street outreach. Journal of Drug Issues, 32(3): 999–1016.
Darke, S. & Ross, J. (1997). Polydrug dependence and psychiatric comorbidity among heroin injectors. Drug and Alcohol Dependence, 48: 135–141.
Darke, S., Ross, J., Zador, D. & Sunjic, S. (2000). Heroin-related deaths in New South Wales 1992–96. Drug and Alcohol Dependence, 60: 141–150.
Darke, S., Williamson, A., Ross, J. & Teesson, M. (2006). Residential rehabilitation for the treatment of heroin dependence: sustained heroin abstinence and drug-related problems two years after treatment entrance. Addictive Disorders & Their Treatment, 5: 9-18.
Davies, A. & Huxley, P. (1997). Survey of general practitioners’ opinions on treatment of opiate users. British Medical Journal, 314: 1173–1174.
Dawe, S. & Harnett, P. (2007). Reducing potential for child abuse among methadone-maintained parents: results from a randomized controlled trial. Journal of Substance Abuse Treatment, 32(4): 381–390.
Dawe, S., Frye, S., Best, D., Moss, D., Atkinson, J., Evans, C., Lynch, M. & Harnett, P. (2007). Drug Use in the Family: impacts and implications for children. ANCD Research Paper 13. Canberra: Australian National Council on Drugs.
Day, C., Conroy, E., Lowe, J., Page, J. & Dolan, K. (2006). Patterns of drug use and associated harms among rural injecting drug users: comparisons with metropolitan injecting drug users. Australian Journal of Rural Health, 14(3): 120–125.
Deehan, A., Taylor, C. & Strang, J. (1997). The general practitioner, the drug misuser, and the alcohol misuser: major differences in general practitioner activity, therapeutic commitment, and ‘shared care’ proposals. British Journal of General Practice, 47(424): 705–709.
Degenhardt, L., Black, E., Breen, C., Bruno, R., Kinner, S., Roxburgh, A., Fry, C., Jenkinson, R., Ward, J., Fetherston, J., Weekley, J. & Fischer, J. (2006). Trends in morphine prescriptions, illicit morphine use and associated harms among regular injecting drug users in Australia. Drug and Alcohol Review, 25(5): 403–412.
Degenhardt, L., Conroy, E., Day, C., Gilmour, S. & Hall, W. (2005). The impact of the Australian heroin shortage on demand for and compliance with treatment for drug dependence. Drug and Alcohol Dependence, 79: 129–135.
Des Jarlais, D.C., Paone, D., Friedman, S.R., Peyser, N. & Newman, R.G. (1995). Regulating controversial programs for unpopular people: methadone maintenance and syringe exchange programs. American Journal of Public Health, 85(11): 1577–1584.
Poly
gon
76
Dolan, K., Shearer, J., White, B., Zhou, J., Kaldor, J. & Wodak, A. (2005). Four-year follow-up of imprisoned male heroin users and methadone treatment: mortality, re-incarceration and hepatitis C infection. Addiction, 100: 820–828.
Dolan, K., Wodak, A., Hall, W., Gaughin, M. & Rae, F. (1996). HIV risk behaviour of IDUs before, during and after imprisonment. Addiction Research, 4(2): 151–160.
Dolan, K.A., Hall, W.D. & Wodak, A.D. (1998). Methadone maintenance treatment reduces heroin injection in New South Wales prisons. Drug and Alcohol Review, 17(2): 153–158.
Dolan, K.A., Shearer, J., MacDonald, M., Mattick, R.P., Hall, W. & Wodak, A.D. (2003). A randomised controlled trial of methadone maintenance treatment versus wait list control in an Australian prison system. Drug and Alcohol Dependence, 24: 59–65.
Doll, R., Peto, R., Boreham, J. & Sutherland, I. (2004). Mortality in relation to smoking: 50 years’ observations on male British doctors. British Medical Journal, 328(7455): 1519.
Doran, C.M., Shanahan, M., Digiusto, E., O’Brien, S. & Mattick, R.P. (2006). Cost-effectiveness analysis of maintenance agonist treatments in NEPOD. Expert Review of Pharmacoeconomics & Outcomes Research, 6(4): 437–446.
Doran, C.M., Shanahan, M., Mattick, R.P., Ali, R., White, J. & Bell, J. (2003). Burprenorphine versus methadone maintenance: a cost-effectiveness analysis. Drug and Alcohol Dependence, 71: 295–302.
Ezard, N., Lintzeris, N., Odgers, P., Koutroulis, G., Muhleisen, P. & Lanagan, A. (1999). An evaluation of community methadone services in Victoria, Australia: results of a client survey. Drug and Alcohol Review, 4: 417–423.
Fiellin, D. & Lintzeris, N. (2003). Methadone syrup injection in Australia: a sentinel finding? Addiction, 98(4): 385–386.
Fiellin, D.A., Pantalon, M.V., Chawarski, M.C., Moore, B.A., Sullivan, L.E., O’Connor, P.G. & Schottenfeld, R.S. (2006). Counseling plus buprenorphine-naloxone maintenance therapy for opioid dependence. New England Journal of Medicine, 355(4): 365–374.
Finch, J.W., Kamien, J.B. & Amass, L. (2007). Two-year experience with buprenorphine-naloxone (Suboxone) for maintenance treatment of opioid dependence within a private practice setting. Journal of Addictive Medicine, 1(2): 104–110.
Fischer, B., Chin, A.T., Kuo, I., Kirst, M. & Vlahov, D. (2002). Canadian illicit opiate users’ views on methadone and other opiate prescription treatment: an exploratory qualitative study. Substance Use & Misuse, 37(4): 495–522.
Fraser, S., Valentine, K., Treloar, C. & Macmillan, K. (2007). Methadone Maintenance Treatment in New South Wales and Victoria: takeaways, diversion and other issues. Sydney: National Centre in HIV Social Research, University of New South Wales.
References
77
Friedmann, P., Lemon, S. & Stein, M. (2001). Transportation and retention in outpatient drug abuse treatment programs. Journal of Substance Abuse Treatment, 21(2): 97–103.
Gilson, L. & McIntyre, D. (2005). Removing user fees for primary care in Africa: the need for careful action. British Medical Journal, 331(7519): 762–765.
Gjersing, L., Butler, T., Caplehorn, J., Belcher, J. & Matthews, R. (2007). Attitudes and beliefs towards methadone maintenance treatment among Australian prison health staff. Drug and Alcohol Review, 26(5): 501–508.
Gossop, M., Marsden, J. & Stewart, D. (1998). NTORS at One Year: the National Treatment Outcome Research Study — changes in substance use, health and criminal behaviours one year after intake. London: Great Britain Department of Health.
Gossop, M., Stewart, D. & Marsden, J. (2006). Effectiveness of drug and alcohol counselling during methadone treatment: content, frequency, and duration of counselling and association with substance use outcomes. Addiction, 101: 404–412.
Gowing, L., Ali, R. & White, J.M. (2006). Buprenorphine for the management of opioid withdrawal. Cochrane Database of Systematic Reviews [Online], Issue 2. Art. no. CD002025. DOI: 10.1002/14651858.CD002025.pub3.
Greener, J.M., Joe, G.W., Simpson, D.D., Rowan-Szal, G.A. & Lehman, W.E.K. (2007). Influence of organizational functioning on client engagement in treatment. Journal of Substance Abuse Treatment, 33(2): 139–147.
Gruber, V.A., Delucchi, K.L., Kielstein, A. & Batki, S.L. (2008). A randomized trial of 6-month methadone maintenance with standard or minimal counseling versus 21-day methadone detoxification. Drug and Alcohol Dependence, 94: 199–206.
Gunderson, E.W. & Fiellin, D.A. (2008). Office-based maintenance treatment of opioid dependence. CNS Drugs, 22(2): 99–111.
Haig, T. (2003). Randomized controlled trial proves effectiveness of methadone maintenance treatment in prison. HIV/AIDS Policy & Law Review, 8(3): 48.
Harries, M. & Clare, M. (2002). Mandatory Reporting of Child Abuse: evidence and options. Report for the Western Australian Child Protection Council. Nedlands, WA: University of Western Australia, Discipline of Social Work and Social Policy.
Harris, A., Gospodarevskaya, E. & Ritter, A. (2005). A randomised trail of the cost effectiveness of buprenorphine as an alternative to methadone maintenance treatment in a primary care setting. Pharmacoeconomics, 23(1): 77–91.
Henry-Edwards, S., Gowing, L., White, J., Ali, R., Bell, J., Brough, R., Lintzeris, N., Ritter, A. & Quigley, A. (2003). Clinical Guidelines and Procedures for the Use of Methadone in the Maintenance Treatment of Heroin Dependence. Canberra: Commonwealth of Australia.
Hser, Y., Anglin, M., Grella, C., Longshore, D. & Prendergast, M. (1997). Drug treatment careers: a conceptual framework and existing research findings. Journal of Substance Abuse Treatment, 14(6): 543–558.

Poly
gon
78
Hser, Y., Grella, C., Chou, C. & Anglin, M. (1998). Relationships between drug treatment careers and outcomes: findings from the National Drug Abuse Treatment Outcome Study. Evaluation Review, 22(4): 496–519.
Humeniuk, R., Ali, R., McGregor, C. & Darke, S. (2003). Prevalence and correlates of intravaneous methadone syrup administration in Adelaide, Australia. Addiction, 98(4): 413–418.
International Narcotics Control Board (2007). Estimated World Requirements for 2007: statistics for 2005. Vienna: United Nations. <http://www.incb.org/pdf/e/tr/nar/2006/Narcotics_publication_2006_part4_tables.pdf>.
Jacka, D., Clode, D., Patterson, S. & Wyman, K. (1999). Attitudes and practices of general practitioners training to work with drug using patients. Drug and Alcohol Review, 18: 287–291.
Jenkinson, R., Clark, N., Fry, C. & Dobbin, M. (2005). Buprenorphine diversion and injection in Melbourne, Australia: an emerging issue? Addiction, 100(2): 197–205.
Joe, G.W., Flynn, P.M., Broome, K.M. & Simpson, D.D. (2007). Patterns of drug use and expectations in methadone patients. Addictive Behaviors, 32(8): 1640–1656.
Joe, G.W., Simpson, D.D., Dansereau, D.F. & Rowan-Szal, G.A. (2001). Relationships between counselling rapport and drug abuse treatment outcomes. Psychiatric Services, 52(9): 1223–1229.
Johnson, R.E., Chutaupe, M.A., Strain, E.C., Walsh, S.L., Stitzer, M.L. & Bigelow, G.E. (2000). A comparison of levomethadyl acetate, buprenorphine, and methadone for opioid dependence. New England Journal of Medicine, 283: 1290–1297.
Joseph, H., Stancliff, S. & Langrod, J. (2000). Methadone maintenance treatment (MMT): a review of historical and clinical issues. Mount Sinai Journal of Medicine, 67(5 & 6): 347–364.
Keen, J., Rowse, G., Mathers, N., Campbell, M. & Seivewright, N. (2000). Can methadone maintenance for heroin dependent patients retained in general practice reduce criminal conviction rates and time spent in prison? British Journal of General Practice, 50(450): 48–49.
Kolar, A.F., Brown, B.S., Haertzen, C.A. & Michaelson, B.S. (1994). Children of substance abusers: the life experiences of children of opiate addicts in methadone maintenance. American Journal of Drug and Alcohol Abuse, 20: 159–171.
Krantz, M.J., Garcia, J.A. & Mehler, P.S. (2005). Effects of buprenorphine on cardiac repolarization in a patient with methadone-related torsade de pointes. Pharmacotherapy, 25(4): 611–614.
Krausz, M., Degkwitz, P., Kuhne, A. & Verthein, U. (1998). Comorbidity of opiate dependence and mental disorders. Addictive Behaviors, 23: 767–783.
Lander, J. (1990). Fallacies and phobias about addiction and pain. British Journal of Addiction, 85: 803–809.
References
79
Laurant, M., Reeves, D., Hermens, R., Braspenning, J., Grol, R. & Sibbald, B. (2004). Substitution of doctors by nurses in primary care. Cochrane Database of Systematic Reviews [Online], Issue 4. Art. No.: CD001271. DOI: 10.1002/14651858.CD001271.pub2.
Lenne, M., Lintzeris, N., Breen, C., Harris, S., Hawken, L., Mattick, R. & Ritter, A. (2001). Withdrawal from methadone maintenance treatment: prognosis and participant perspectives. Australian and New Zealand Journal of Public Health, 25: 121–125.
Lintzeris, N. (2006). Harm reduction with buprenorphine. Paper presented at the Hong Kong Dialogue on Opiate Dependence, Hong Kong College of Psychiatry and the International Society of Addiction Medicine.
Lintzeris, N., Bell, J., Bammer, G., Jolley, D. & Rushworth, L. (2002). A randomized controlled trial of buprenorphine in the management of short-term ambulatory heroin withdrawal. Addiction, 97(11): 1395–1404.
Lintzeris, N., Clark, N., Winstock, A., Dunlop, A., Muhleisen, P., Gowing, L., Ali, R., Ritter, A., Bell, J., Quigley, A., Mattick, R.P., Monheit, B. & White, J. (2006). National Clinical Guidelines and Procedures for the use of Buprenorphine in the Treatment of Opioid Dependence. Canberra: Commonwealth of Australia.
Lintzeris, N., Koutroulis, G., Odgers, P., Muhleisen, P. & Ezard, N. (1996). Report on the Evaluation of Community Methadone Services in Victoria. Fitzroy: Turning Point Alcohol and Drug Centre.
Lintzeris, N., Lenne, M. & Ritter, A. (1999). Methadone injecting in Australia: a tale of two cities. Addiction, 94(8): 1175–1178.
Lintzeris, N., Pritchard, E. & Sciacchitano, L. (2007). Investigation of Methadone Dosing in Victoria: factors and influencing dosing levels. Fitzroy: Turning Point Alcohol and Drug Centre.
Lintzeris, N., Ritter, A., Dunlop, A. & Muhleisen, P. (2002). Training primary health care professionals to provide buprenorphine and LAAM treatment. Substance Abuse, 23(4): 245–254.
Lintzeris, N., Ritter, A., Panjari, M., Clark, N., Kutin, J. & Bammer, G. (2004). Implementing buprenorphine treatment in community settings in Australia: experiences from the Buprenorphine Implementation Trial. American Journal of Addicitions, 13 (Suppl. 1): S29–S41.
Lloyd, B., Ballantyne, S. & Loveday, W. (2007). Changes in the culture of drug dependence treatment populations: the rise of pharmaceutical opiates. Paper presented at the APSAD Conference, Auckland, New Zealand.
Luthar, S.S. & Suchman, N.E. (2000). Relational Psychotherapy Mothers’ Group: a developmentally informed intervention for at-risk mothers. Development and Psychopathology, 12: 235–253.
Madden, A. & Cavaleri, W. (2007). Hepatitis C prevention and true harm reduction. International Journal of Drug Policy, 18: 335–337.
Maddux, J., Prihoda, T. & Desmond, D. (1994). Treatment fees and retention on methadone maintenance. The Journal of Drug Issues, 24: 429–443.
Poly
gon
80
Mattick, R., Digiusto, E., Doran, C.M., O’Brien, S., Shanahan, M., Kimber, J., Henderson, N., Breen, C., Shearer, J., Gates, J., Shakeshaft, A. & NEPOD Trial Investigators (2001). National Evaluation of Pharmacotherapies for Opioid Dependence: report of results and recommendations. Sydney: National Drug and Alcohol Research Centre.
Mattick, R.P., Kimber, J., Breen, C. & Davoli, M. (2008). Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database of Systematic Reviews [Online], Issue 2. Art. No.: CD002207. DOI: 10.1002/14651858.CD002207.pub3.
McLellan, A.T., Arndt, I.O., Metzger, D.S., Woody, G.E. & O’Brien, C.P. (1993). The effects of psychosocial services in substance abuse treatment. Journal of the American Medical Association, 269: 1953–1959.
Mills, K., Lynskey, M., Teesson, M., Ross, J. & Darke, S. (2003). Prevalence and Correlates of Post Traumatic Stress Disorder (PTSD) among People with Heroin Dependence: findings from the Australian Treatment Outcome Study (NSW). NDARC Technical Report no. 169. Sydney: National Drug and Alcohol Research Centre.
Mintzer, I.L., Eisenberg, M., Terra, M., MacVane, C., Himmelstein, D.U. & Woolhandler, S. (2007). Treating opioid addiction with buprenorphine-naloxone in community-based primary care settings. Annals of Family Medicine, 5(2): 146–150.
Moore, T., Ritter, A. & Caulkins, J. (2007). A cost effectiveness comparison of three policy options for reducing heroin dependency. Drug and Alcohol Review, 26(4): 269–378.
Muhleisen, P., Clark, N., Teo, A. & Brogan, D. (2005). Opioid substitution therapy: considering the costs to consumers. Of Substance, 3(1): 14–17.
National Drug and Alcohol Research Centre (2008). Submission to the Special Commission of Inquiry into Child Protection Services in New South Wales <http://www.lawlink.nsw.gov.au/lawlink/Special_Projects/ll_splprojects.nsf/vwFiles/NDARC_Submission.pdf/$file/NDARC_Submission.pdf> accessed 5 May 2008.
New South Wales Child Death Review Team (2006). Annual Report 2005. Sydney: NSW Commission for Children and Young People.
New South Wales Child Death Review Team (2007). Annual Report 2006. Sydney: NSW Commission for Children and Young People.
New South Wales Commission for Children and Young People (2008). Think Child, Think Family, Think Community: from a child protection system to a system for protecting children. Joint Submission to the Special Commission of Inquiry into Child Protection Services in New South Wales. <http://www.lawlink.nsw.gov.au/lawlink/Special_Projects/ll_splprojects.nsf/vwFiles/CCYP_submission_Received.pdf/$file/CCYP_submission_Received.pdf> retrieved 5 May 2008.
New South Wales Department of Health (2006a). New South Wales Opioid Treatment Program: clinical guidelines for methadone and buprenorphine treatment of opioid dependence. North Sydney: NSW Health.
References
81
New South Wales Department of Health (2006b). Your Child’s Safety: advice for parents on storing methadone, safe sleeping and settling babies. Sydney: NSW Health.
New South Wales Department of Health (2007). Justice Health Annual Report 2006–07. Sydney: NSW Health <http://www.justicehealth.nsw.gov.au/publications/A_R06_07WEB.pdf>.
New South Wales Ombudsman (2006). Report of Reviewable Deaths in 2005. Volume 2: Child Deaths. Sydney: NSW Ombudsman.
New South Wales Ombudsman (2007). Report of Reviewable Deaths in 2006. Volume 2: Child Deaths. Sydney: NSW Ombudsman.
Nielsen, S., Dietze, P., Dunlop, A., Muhleisen, P., Lee, N. & Taylor, D. (2007). Buprenorphine supply by community pharmacists in Victoria, Australia: perceptions, experiences and key issues identified. Drug and Alcohol Review, 26(2): 143–151.
O’Brien, C.P. & McLellan, A.T. (1996). Myths about the treatment of addiction. The Lancet, 347: 237–240.
O’Brien, S., Black, E., Degenhardt, L., Roxburgh, A., Campbell, G., de Graaff, B., Fetherston, J., Jenkinson, R., Kinner, S., Moon, C. & White, N. (2006). Australian Drug Trends 2006: findings from the Illicit Drug Reporting System (IDRS). Sydney: National Drug and Alcohol Research Centre.
O’Reilly, B., Leibrick, F., Huxtable, D. & Chenhall, R. (2004). Benzodiazepine and Pharmaceutical Opioid Misuse and Their Relationship to Crime: an examination of illicit prescription drug markets in Melbourne, Hobart and Darwin: Northern Territory report. NDLERF Monograph Series no. 23. Hobart: National Drug Law Enforcement Research Fund.
Pani, P. & Pirastu, R. (2000). Take-home and compliance with methadone maintenance treatment. Heroin Addiction and Related Clinical Problems, 2(1): 33–38.
Parliament of Victoria, Drugs and Crime Prevention Committee (VDCPC) (2006). Inquiry into the Misuse/Abuse of Benzodiazepines and Other Forms of Pharmaceutical Drugs in Victoria: interim report. Melbourne: VDCPC. <http://www.parliament.vic.gov.au/dcpc_new/inquiries/pharmaceuticalmisuse/DCPC-Report_Benzo_2006-08-24.pdf>.
Pharmacy Guild of Australia (2007). Funding Model Options for Dispensing of Pharmacotherapies for Opioid Dependence in Community Pharmacy: final report. Melbourne: Healthcare Management Advisors Pty Ltd.
Rapeli, P., Fabritius, C., Alho, H., Salaspuro, M., Wahlbeck, K. & Kalska, H. (2007). Methadone vs buprenorphine/naloxone during early opioid substitution treatment: a naturalistic comparison of cognitive performance relative to healthy controls. BMC Clinical Pharmacology, 12(7): 5.
Poly
gon
82
Razali, K., Thein, H.H., Bell, J., Cooper-Stanbury, M., Dolan, K., Dore, G., George, J., Kaldor, J., Karvelas, M., Li, J., Maher, L., McGregor, S., Hellard, M., Poeder, F., Quaine, J., Stewart, K., Tyrrell, H., Weltman, M., Westcott, O., Wodak, A. & Law, M. (2007). Modelling the hepatitis C virus epidemic in Australia. Drug and Alcohol Dependence, 91: 228–235.
Reisenger, M. (2006). Injecting buprenorphine tablets: a manageable risk. Heroin Addiction and Related Clinical Problems, 8(4): 29–40.
Rhoades, H., Creson, D., Elk, R., Schmitz, J. & Grabowski, J. (1998). Retention, HIV risk, and illicit drug use during treatment: methadone dose and visit frequency. American Journal of Public Health, 88: 4–9.
Richter, K.P. & Bammer, G. (2000). A hierarchy of strategies heroin-using mothers employ to reduce harm to their children. Journal of Substance Abuse Treatment, 19(4): 403–413.
Ritter, A., Berends, L., Clemens, S., Devaney, M., Richards, J., Bowen, K. & Tiffen, R. (2003). Pathways: a review of the Victorian drug treatment service system. Final report. Fitzroy, Victoria: Turning Point Alcohol and Drug Centre.
Robles, E., Miller, F., Gilmore-Thomas, K. & McMillan, D. (2001). Implementation of a clinic policy of client-regulated methadone dosing. Journal of Substance Abuse Treatment, 20(3): 225–230.
Roche, A. (1997). Have efforts to improve medical students’ drug and alcohol knowledge, skills and attitudes worked? Drug and Alcohol Review, 16(2): 157–170.
Rosenblum, A., Parrino, M., Schnoll, S., Fong, C., Maxwell, C., Cleland, C., Magura, S. & Haddox, J. (2007). Prescription opioid abuse among enrollees into methadone maintenance treatment. Drug and Alcohol Dependence, 90(1): 64–71.
Ross, J., Teesson, M., Darke, S., Lynskey, M., Ali, R., Ritter, A. & Cooke, R. (2005). The characteristics of heroin users entering treatment: findings from the Australian Treatment Outcome Study (ATOS). Drug and Alcohol Review, 24: 411–418.
Rowan-Szal, G.A., Chatham, L.R., Greener, J.M., Joe, G.W., Payte, J.T. & Simpson, D.D. (2004). Structure as a determinant of treatment dose. Journal of Maintenance in the Addictions, 2(4): 55–70.
Rowe J. (2008). A Raw Deal? Impact on the health of consumers relative to the cost of pharmacotherapy. Melbourne: Salvation Army & RMIT. <http://www.salvationarmy.org.au/salvwr/_assets/main/documents/crisisservices/pdf/9591%20raw%20deal_book.pdf>.
Shearer, J., Wodak, A. & Dolan, K. (2004). The Prison Opiate Dependence Treatment Trial. Sydney: National Drug and Alcohol Research Centre. <http://ndarc.med.unsw.edu.au/NDARCWeb.nsf/resources/TR_3/$file/TR.199.pdf>.
Simeons, S., Matheson, C., Inkster, K., Ludbrook, A. & Bond, C. (2002). The Effectiveness of Treatment for Opiate Dependent Drug Users. Edinburgh: Scottish Executive, Effective Interventions Unit.
References
83
Simpson, D.D., Joe, G.W., George, W. & Brown, B.S. (1997). Treatment retention and follow-up outcomes in the drug abuse treatment outcome study. Psychology of Addicitive Behaviors, 11(4): 294–307.
Simpson, D.D., Joe, G.W., Rowan-Szal, G.A. & Greener, J.M. (1997). Drug abuse treatment process components that improve retention. Journal of Substance Abuse Treatment, 14(6): 565–572.
Smith, B., Miller, P., O’Keefe, B. & Fry, C. (2004). Benzodiazepine and Pharmaceutical Opioid Misuse and Their Relationship to Crime: an examination of illicit prescription drug markets in Melbourne. Hobart: National Drug Law Enforcement Research Fund.
Smith, M.Y., Bailey, J.E., Woody, G.E. & Kleber, H.D. (2007). Abuse of buprenorphine in the United States: 2003–2005. Journal of Addictive Diseases, 26(3): 107–111.
Solberg, U., Burkhart, G. & Nilson, M. (2002). An overview of opiate substitution treatment in the European Union and Norway. International Journal of Drug Policy, 13: 477–484.
Southgate, E., Kippax, S., Bammer, G., Isaac-Toua, G., MacDonald, M., Hopwood, M. & Aspin, C. (2001). Methadone Injection in New South Wales. Sydney: National Centre in HIV Social Research, University of New South Wales.
Stimmel, B. (2007). Buprenorphine misuse, abuse and diversion: when will we ever learn? Journal of Addictive Diseases, 26(3): 1–3.
Stone, E. & Fletcher, K. (2003). User views on supervised methadone consumption. Addiction Biology, 8(1): 45–48.
Strang, J., Hunt, C., Gerada, C. & Marsden, J. (2007). What difference does training make? A randomized trial with waiting-list control of general practitioners seeking advanced training in drug misuse. Addiction, 102: 1637–1647.
Strang, J., Manning, V., Mayet, S., Ridge, G., Best, D. & Sheridan, J. (2007). Does opiate prescribing for addiction change after national guidelines? Methadone and buprenorphine prescribing to opiate addicts by general practitioners and hospital doctors in England, 1995–2005. Addiction, 102: 761–770.
Strike, C.J., Gnam, W., Urbanoski, K., Fischer, B., Marsh, D.C. & Millson, M. (2004). Factors predicting 2-year retention in methadone maintenance treatment for opioid dependence. Addictive Behaviors, 30(5): 1025–1028.
Sullivan, L.E., Chawarski, M., O’Connor, P.G., Schottenfeld, R.S. & Fiellin, D.A. (2005). The practice of office-based burenorphine treatment of opioid dependence: is it associated with new patients entering into treatment? Drug and Alcohol Dependence, 79(1): 113–116.
Sunjic, S. & Zador, D. (1999). Methadone syrup-related deaths in New South Wales, Australia, 1990–95. Drug and Alcohol Review, 18(4): 409–415.
Taplin, S. (2000). Factors affecting retention on methadone maintenance programs. Unpublished PhD dissertation, University of Sydney, Sydney.
Teesson, M., Ross, J., Darke, S., Lynsky, M., Ali, R., Ritter, A. & Cooke, R. (2006). One year outcomes for heroin dependence: findings from the Australian Treatment Outcome Study (ATOS). Drug and Alcohol Dependence, 83(2): 174–180.
Poly
gon
84
Thomas, M. & Buckmaster, L. (2007). ‘Naltrexone or methadone’? Debates about drug treatments for heroin dependence in the context of drugs policy. Canberra: Australian Parliamentary Library. <http://www.aph.gov.au/library/pubs/RP/2007-08/08RP07.pdf>.
Vidal-Trecan, G., Varescon, I., Nabet, N. & Boissonnas, A. (2003). Intravenous use of prescribed buprenorphine tablets by drug users receiving maintenance therapy in France. Drug and Alcohol Dependence, 69(2): 175–181.
Vignau, J. & Brunelle, E. (1998). Differences between general practioner- and addiction center-prescribed buprenorphine substitution therapy in France. European Addiction Research, 4 (Suppl. 1): 24–28.
Ward, P. & Mattick, R. (2005). Health Care Utilisation and Cost under the Commonwealth Medicare Benefit Scheme by Methadone Maintenance Treatment Patients in NSW. NDARC Technical Report no. 240. Sydney: National Drug and Alcohol Research Centre.
Warren, E., Viney, R., Shearer, J., Shanahan, M., Wodak, A. & Dolan, K. (2006). Value for money in drug treatment: economic evaluation of prison methadone. Drug and Alcohol Dependence, 84(2): 160–166.
Wertheimer, A. & Santella, T. (2003). Medication compliance research: still so far to go. Journal of Applied Research in Clinical and Experimental Therapeutics, 3(3): 254–261.
Winstock, A. (2007). Global SWAT Report. Report prepared for Mental Health and Drug and Alcohol Office, New South Wales Department of Health, and Pharmacy Guild of Australia, NSW Branch.
Winstock, A. & Bell, J. (2006). Clinical Guidelines Assessing Suitability for Unsupervised Medication Doses for Treating Opioid Dependency. Sydney: Royal Australasian College of Physicians, Australasian Chapter of Addiction Medicine.
Winstock, A. & Lea, T. (2007). Safe storage of methadone takeaway doses: a survey of patient practice. Australian and New Zealand Journal of Public Health, 31(6): 526–528.
Winstock, A., Lea, T. & Ritter, A. (2007). The impact of community pharmacy dispensing fees on the introduction of buprenorphine–naloxone in Australia. Drug and Alcohol Review, 26(4): 411–416.
Winstock, A., Lea, T. & Sheridan, J. (2008). Prevalence of diversion and injection of methadone and buprenorphine among clients receiving opioid treatment at community pharmacies in New South Wales, Australia. International Journal of Drug Policy, 19(6): 450–458.
Wittchen, H.-U., Apelt, S.M., Soyka, M., Gastpar, M., Backmund, M., Golz, J., Kraus, M.R., Tretter, F., Schafer, M., Siegert, J., Scherbaum, N., Rehm, J. & Buhringer, G. (2008). Feasibility and outcome of substitution treatment of heroin-dependent patients in specialized substitution centers and primary care facilities in Germany: a naturalistic study in 2694 patients. Drug and Alcohol Dependence, 95(3): 245–257.
References
85
Wodak, A. (2002). Methadone and heroin prescription: babies and bath water. It’s the context, stupid: methadone treatment in an unsympathetic environment. Substance Use & Misuse, 37(4): 523–530.
Woods, M.A. (2001). Methadone advocacy: the voice of the patient. Mount Sinai Journal of Medicine, 68(1): 75–78.
Woody, G.E., McLellan, A.T., Luborsky, L. & O’Brien, C.P. (1995). Psychotherapy in community methadone programs: a validation study. The American Journal of Psychiatry, 152: 1302–1308.
Zarkin, G.A., Dunlap, L.J., Hicks, K.A. & Mamo, D. (2005). Benefits and costs of methadone treatment: results from a lifetime simulation model. Health Economics, 14: 1133–1150.
Zhang, Z., Friedmann, P.D. & Gerstein, D.R. (2003). Does retention matter? Treatment duration and improvement in drug use. Addiction, 98(5): 673–684.
Poly
gon
86
6. Appendices6.1 Appendix A: Stakeholders consulted as part of the project
Robert Ali Director, WHO Collaborating Centre, South Australia
ANCD Project Reference Group member
Mark Anns Mental Health and Drug & Alcohol Office, New South Wales
Fiona B. Network Against Prohibition, Northern Territory
Susan Ballantyne Associate Director, Drugs of Dependence Unit, Queensland
Mark Bartlett Policy Officer, ACT Health
Merri Blair Mobile Drug Safety Worker, Goulburn Valley Community Health Service, Victoria
Warren Blee Maroochydore Pharmacy, Queensland
Chris Boag Drugs Policy and Services Branch, Department of Human Services, Victoria
Laura Bondeson Tasmanian Council on AIDS, Hepatitis and Related Diseases
Melissa Bull Lecturer, School of Criminology & Criminal Justice, Griffith University, Queensland
Jude Byrne Australian Injecting & Illicit Drug Users League (AIVL)
Maureen Chesler Drugs and Poisons Unit, Department of Human Services, Victoria
Fiona Clarke Northern Territory Harm Reduction Peer Education Coordinator
Malcolm Dobbin Drugs and Poisons Unit, Department of Human Services, Victoria
Adrian Dunlop Area Director, Drug & Alcohol Clinical Services, New South Wales
Silvia Engels Tasmania Health
Robin Fisher Drugs Policy and Services Branch, Department of Human Services, Victoria
Appendices
87
Amie Frewen Senior Research Officer, National Cannabis Prevention and Information Centre, National Drug and Alcohol Research Centre
Paul G. NSW Users & AIDS Association Inc.
Paul Haber Area Medical Director, Drug Health Services, Royal Prince Alfred Hospital, New South Wales
Margaret Hamilton Chairperson, Multiple and Complex Needs Panel, Victoria
ANCD Project Reference Group member
Jeremy Hayllar Clinical Director, Brisbane Northside, Queensland
Trish Heath Manager, Community Clinical Programs, Next Step Drug & Alcohol Services, Western Australia
Jennifer Holmes CNC Health Informatics, Drug & Alcohol Services, New South Wales
Chris Ireland Pharmacist, Sharpe’s Pharmacy, Darlinghurst, New South Wales
Joy Knight Coordinator, Community Program for Opioid Pharmacotherapy, Professional Standards Board, Department of Health, Western Australia
Phuong–Phi Le Coordinator, Community Pharmacy Program, Drug and Alcohol Services SA
Sam Liebelt Needle & Syringe Program Community Development Coordinator, Western Australian Substance Users Association
Sarah Lord VIV AIDS (Victorian Drug User Group)
Annie Madden Executive Officer, Australian Injecting & Illicit Drug Users League (AIVL)
Eugene McGarrell Manager, Opioid Treatment & Clinical Policy, New South Wales
David McGrath Director, Mental Health and Drug & Alcohol Office, New South Wales
Benny Monheit Drug and Alcohol Physician, Alfred Hospital Medical Director, Victoria
Poly
gon
88
Keith Moyle Drugs and Poisons Unit, Department of Human Services, Victoria
NSW Users & AIDS Association Inc. (NUAA)
Adrian Reynolds Clinical Director, Department of Health & Human Services, Tasmania
Chris Shipway Mental Health and Drug & Alcohol Office, New South Wales
Laurie Snow Nurse Unit Manager, and Cecily Collison RN, Bungara Opioid Treatment Unit, Wollongong, New South Wales
Kay Sorimachi Director, Policy and Regulatory Affairs, Pharmaceutical Society of Australia
Tamara Speed Treatments and Policy Manager, Australian Injecting & Illicit Drug Users League (AIVL)
Dayle Stubbs Finance Manager, Australian Injecting & Illicit Drug Users League (AIVL)
Amber Summerhill Senior Project Officer, Australian Institute of Health and Welfare
Stephanie Taplin Senior Research Officer, National Drug and Alcohol Research Centre
Nicole Wiggins Canberra Alliance for Harm Minimisation and Advocacy, Australian Capital Territory
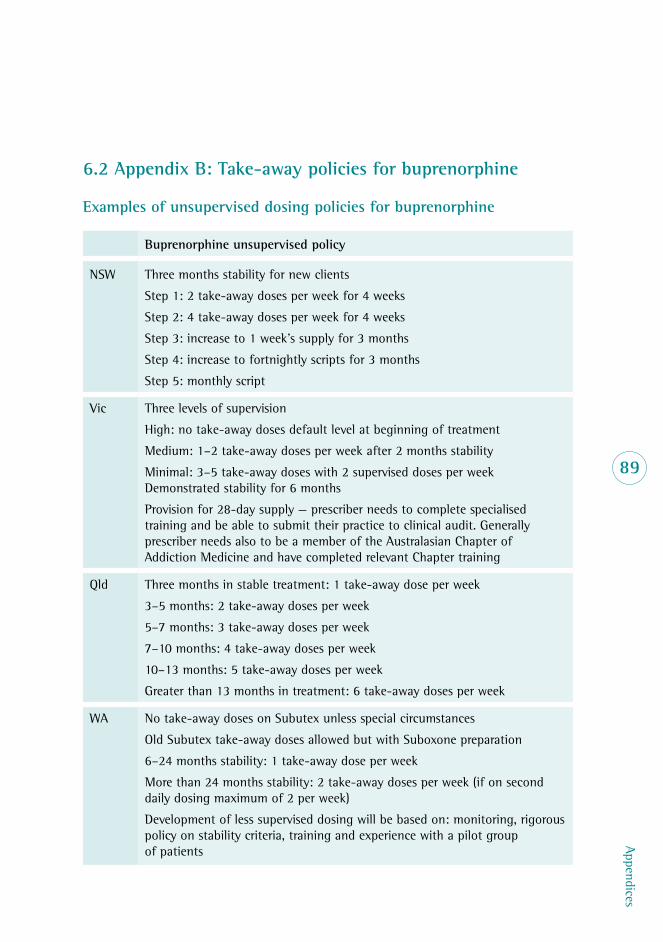
Appendices
89
6.2 Appendix B: Take-away policies for buprenorphine
Examples of unsupervised dosing policies for buprenorphine
Buprenorphine unsupervised policy
NSW Three months stability for new clients
Step 1: 2 take-away doses per week for 4 weeks
Step 2: 4 take-away doses per week for 4 weeks
Step 3: increase to 1 week’s supply for 3 months
Step 4: increase to fortnightly scripts for 3 months
Step 5: monthly script
Vic Three levels of supervision
High: no take-away doses default level at beginning of treatment
Medium: 1–2 take-away doses per week after 2 months stability
Minimal: 3–5 take-away doses with 2 supervised doses per week Demonstrated stability for 6 months
Provision for 28-day supply — prescriber needs to complete specialised training and be able to submit their practice to clinical audit. Generally prescriber needs also to be a member of the Australasian Chapter of Addiction Medicine and have completed relevant Chapter training
Qld Three months in stable treatment: 1 take-away dose per week
3–5 months: 2 take-away doses per week
5–7 months: 3 take-away doses per week
7–10 months: 4 take-away doses per week
10–13 months: 5 take-away doses per week
Greater than 13 months in treatment: 6 take-away doses per week
WA No take-away doses on Subutex unless special circumstances
Old Subutex take-away doses allowed but with Suboxone preparation
6–24 months stability: 1 take-away dose per week
More than 24 months stability: 2 take-away doses per week (if on second daily dosing maximum of 2 per week)
Development of less supervised dosing will be based on: monitoring, rigorous policy on stability criteria, training and experience with a pilot group of patients
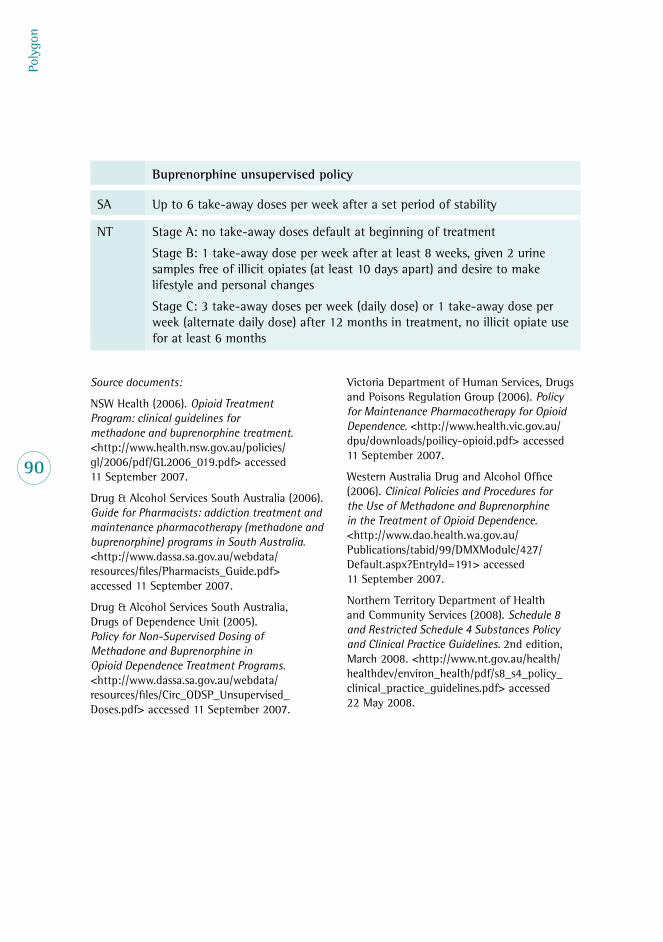
Poly
gon
90
Source documents:
NSW Health (2006). Opioid Treatment Program: clinical guidelines for methadone and buprenorphine treatment. <http://www.health.nsw.gov.au/policies/gl/2006/pdf/GL2006_019.pdf> accessed 11 September 2007.
Drug & Alcohol Services South Australia (2006). Guide for Pharmacists: addiction treatment and maintenance pharmacotherapy (methadone and buprenorphine) programs in South Australia. <http://www.dassa.sa.gov.au/webdata/resources/files/Pharmacists_Guide.pdf> accessed 11 September 2007.
Drug & Alcohol Services South Australia, Drugs of Dependence Unit (2005). Policy for Non-Supervised Dosing of Methadone and Buprenorphine in Opioid Dependence Treatment Programs. <http://www.dassa.sa.gov.au/webdata/resources/files/Circ_ODSP_Unsupervised_Doses.pdf> accessed 11 September 2007.
Victoria Department of Human Services, Drugs and Poisons Regulation Group (2006). Policy for Maintenance Pharmacotherapy for Opioid Dependence. <http://www.health.vic.gov.au/dpu/downloads/poilicy-opioid.pdf> accessed 11 September 2007.
Western Australia Drug and Alcohol Office (2006). Clinical Policies and Procedures for the Use of Methadone and Buprenorphine in the Treatment of Opioid Dependence. <http://www.dao.health.wa.gov.au/Publications/tabid/99/DMXModule/427/Default.aspx?EntryId=191> accessed 11 September 2007.
Northern Territory Department of Health and Community Services (2008). Schedule 8 and Restricted Schedule 4 Substances Policy and Clinical Practice Guidelines. 2nd edition, March 2008. <http://www.nt.gov.au/health/healthdev/environ_health/pdf/s8_s4_policy_clinical_practice_guidelines.pdf> accessed 22 May 2008.
Buprenorphine unsupervised policy
SA Up to 6 take-away doses per week after a set period of stability
NT Stage A: no take-away doses default at beginning of treatment
Stage B: 1 take-away dose per week after at least 8 weeks, given 2 urine samples free of illicit opiates (at least 10 days apart) and desire to make lifestyle and personal changes
Stage C: 3 take-away doses per week (daily dose) or 1 take-away dose per week (alternate daily dose) after 12 months in treatment, no illicit opiate use for at least 6 months