Polycystic Ovary Syndrome PCOS Talia Eldar-Geva, MD, PhD Director Reproductive Endocrinology and...
41
Polycystic Ovary Polycystic Ovary Syndrome Syndrome PCOS PCOS Talia Eldar-Geva, MD, PhD Director Reproductive Endocrinology and Genetics Unit, IVF Unit Shaare-Zedek Medical Center 5 th year Medical Students, 2014
-
Upload
joanna-lambert -
Category
Documents
-
view
218 -
download
1
Transcript of Polycystic Ovary Syndrome PCOS Talia Eldar-Geva, MD, PhD Director Reproductive Endocrinology and...

Polycystic Ovary SyndromePolycystic Ovary SyndromePCOSPCOS
Talia Eldar-Geva, MD, PhD
Director Reproductive Endocrinology and Genetics Unit, IVF Unit
Shaare-Zedek Medical Center
5th year Medical Students, 2014

אז מה זה??

“Stein-Leventhal Syndrome”
Stein, Leventhal. Am J Obstet Gynecol 1935:
Amenorrhea associated with bilateral polycystic ovaries.
Seven women with amenorrhea, hirsutism, obesity, and a characteristic polycystic appearance of their ovaries.

Ovarian Morphology
Vaginal US 12 follicles of 2-9 mm in diameter in one ovary and/or
ovarian volume > 10cm3
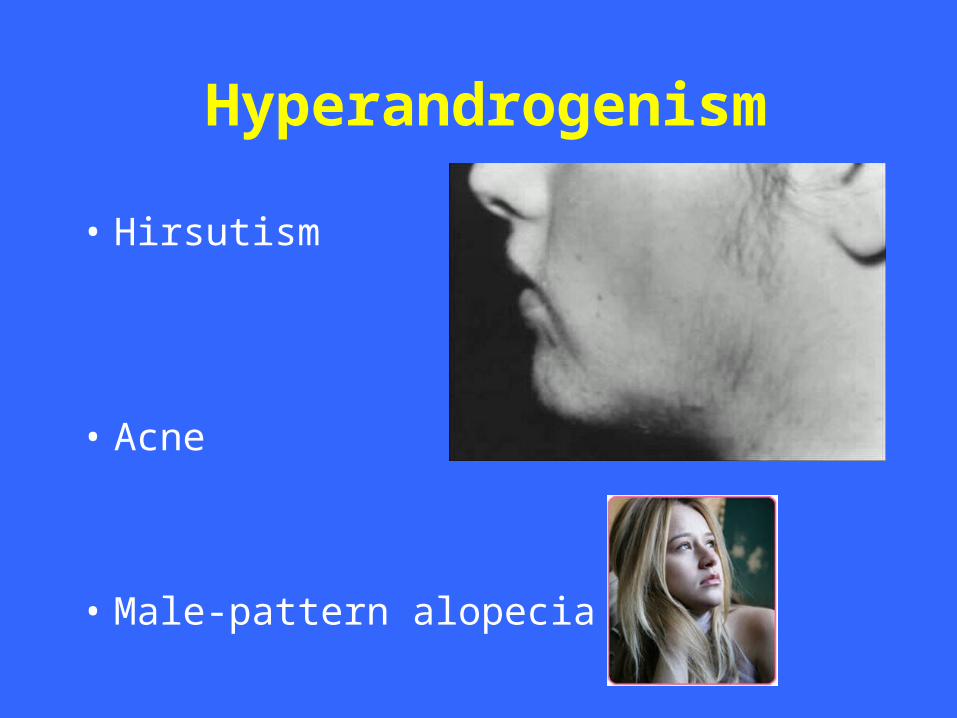
Hyperandrogenism
• Hirsutism
• Acne
• Male-pattern alopecia

HirsutismFerriman-Gallwey scoring system
0-36mild
Moderate
severe

Diagnostic criteria ESHRE/ASRM PCOS Consensus
(Rotterdam, July 2003)
• Two out of three:Two out of three:–Ovarian morphology
–Hyperandrogenism (biochemical or clinical)
–Chronic Oligo/anovulation

Range of clinical manifestations of PCOS
Mensrual disturbence two thirds Oligomenorrhoea 50% Amenorrhoea 20% Regular cycles 30% Infertility (~75% of anovulatory
infertility)
Hyperandrogenism 50%
Obesity 30-75%Insulin resistance >50%
Asymptomatic (20% of those with PCO)

Pathogenesis
• No single etiologic factor fully accounts for the spectrum of abnormalities in PCOS
• GnRH pulse frequencyGnRH pulse frequency• Pituitary responsePituitary response
– LH LH/FSHLH LH/FSH – stimulate androgens secretion by theca cells
• Cytochrome P-450c17Cytochrome P-450c17– ovarian theca cells of PCOS women are more efficient at
converting androgenic precursors to testosterone than are normal theca cells.
• InsulinInsulin
• ??

Weight increase
Genetic defects ininsulin action
Insulin receptor disorders
INSULINincreases
IGFBP-1decreases
SHBP decreases
LH THECA
Androstenedioneincreases
Testosteroneincreases
+
Free Testosteroneincreases
Free E2increases
Free IGF-Iincreases

Acanthosis Nigricans

INSULIN RESISTANCE: DIAGNOSIS & SCREENING
•OGTT (75 gr)– Glucose response, Insulin response – area under curves– Glucose Insulin (G:I) ratio
Fasting G:I ratio < 4.5 is the single best screening measure for detecting Insulin Resistance in PCOS

Differential Diagnosis
• Hyperprolactinemia• Nonclassic congenital adrenal hyperplasia• Cushing’s syndrome• Androgen-secreting neoplasm• Acromegaly• Hypothyroidism• Drugs-related (androgens, valproic acid,
cyclosporine, or other drugs).


Hormones profile
• Testosterone– SHBG– Free Androgen Index
• Androstenedione
• DHEA-S• 17-OH-Progesterone
• LH• LH/FSH
• Lipids profile• Glucose• Insulin

Dermatologist
Disorder of hair growth, Acne
Fertility problem Menstrual dysfunctionGynecologyst
Obesity problem pseudo Cushing’s diseaseInternist General
practitioner
?
Frequency: 5-10% of females
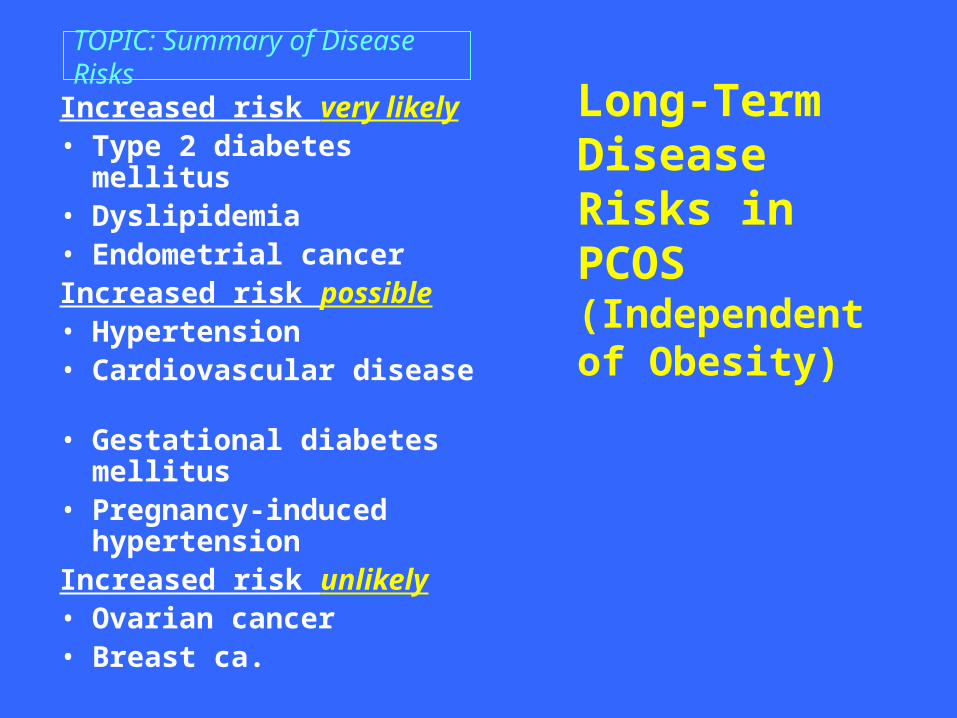
Long-Term Disease Risks in PCOS (Independent of Obesity)
Increased risk very likely• Type 2 diabetes mellitus• Dyslipidemia• Endometrial cancerIncreased risk possible• Hypertension• Cardiovascular disease• Gestational diabetes
mellitus• Pregnancy-induced
hypertensionIncreased risk unlikely • Ovarian cancer• Breast ca.
TOPIC: Summary of Disease Risks

לו הייתם שטיין ולוונטלאיך הייתם מטפלים?
WEDGE RESECTION

Laparoscopic Ovarian “Drilling”/CauterizationLaparoscopic Ovarian “Drilling”/Cauterization))Stein-Leventhal - wedge resectionStein-Leventhal - wedge resection

הצגת מקרה
45 ימים, וסת אחרון לפני 45-60, וסת אחת ל 32בת •ימים.
ק"ג למ"ר(, BMI 31 ס"מ )165 ק"ג, גובה 82משקל •עודף שיער בפנים.
• LH=IU/L16.טסטוסטרון תקין ,
– SHBGאבל •
נמוך, ולכן...•
האם חסר משהו לאבחנה?•
INDUCTION OF OVULATIONINDUCTION OF OVULATION WHO Group IIWHO Group II
PRINCIPLE - need stimulation with FSHPRINCIPLE - need stimulation with FSH
Clomiphene CitrateClomiphene Citrate
HMGHMG
FSHFSH - -urinaryurinary - -recombinantrecombinant
Pulsatile GnRHPulsatile GnRH
))Ovarian cauterizationOvarian cauterization((

Clomiphene citrate (CC) )Ikaclomin, Clomid(
Synthesized 1956
Clinical use 1960
Approved )US( 1967
Orally active
Non-steroidal
Similar to estrogen
Estrogen agonist / antagonist
1-3 months in serum

CC: Mechanism of ActionPRINCIPLE: Weak ESRM (estrogen receptor modulator)
Binding to Hypothalamic Estrogen receptors
Occupying Estrogen-receptors for long time
Inhibition of receptor replenishment
“mimicking” hypoestrogenism
Increase in GnRH pulse frequency (& amplitude)
FSH & LH levels rise

Treatment cycle with CC
First step –Progesterone
treatment – induce bleeding–decreases LH levels –opposes estrogen-
induced endometrial hyperplasia
Cycle days5 9
CC50-200mg/day
5 days
LH
FSH
Progesterone

CC: Minor EffectsCC: Minor Effects
Directly stimulates FSH secretion from hypophysis
Direct ovarian effect
BUTBUTAnti-estrogenic effect in the
Cervix
Endometrium
Can induce/aggravate luteal-phase defect

Response to clomipheneResponse to clomiphene
No responseNo response20%20%
OvulationOvulation & & pregnancypregnancy
OvulationOvulation - -no pregnancyno pregnancy
45%45%
35%35%
Cumulative 6 cycles pregnancy (75%) rate approaches the normal rate (if no other cause of infertility)
CC: Side Effects
•Vasomotor flushes10-20%
•Abdominal bloating, pain 5.5%
•Breast discomfort 2%
•Nausea, vomiting 3%
•Visual symptoms 1.5%
•Headache 1.3%
•Dryness, loss of hair 0.3%

CC: Complications
• Multiple pregnancy 8-10%
• high-order <1%
• OHSS 5-10%
• mostly mild - moderate• No or slightly increased ectopic pregnancy rate )1%(
• No change in miscarriage rate )15%(
• No change in congenital malformations rate
• Inconclusive data regarding increased cancer rate

What to do with CC failures?• Extended protocols • Add dexamethasone• Add pretreatment suppression )pill, GnRH-a(• Treat obesity• Treat hyperinsulinemia• Add intra-uterine insemination• Ovarian cauterization• Estrogen to improve endometrial factor is ineffective
• Do not treat for more that 6 cycles
GONADOTROPINS TREATMENT
• Human menopausal Gonadotropins )hMG(– FSH 75IU + LH 75IU
• Urinary FSH - FSH 75IU, <1% LH
• Highly purified urinary FSH - < 0.1% LH
• Recombinant FSH
• hCG
• Recombinant LH
• Could be replaced by GnRH / GnRH agonist

Treatment Cycle with Menotropins
++5-75-7 ++55 ++55
Cycle DaysCycle Days55
7575
150150
225225
US & E2 measurement
every 2 -5 days
US for follicular number and size
hCGhCG, 5000-10000IUFSH dailyFSH daily
When follicle 17-20mmand E2 600-1500pmol/L

Complications of Complications of Gonadotropins Gonadotropins StimulationStimulation
• MULTIPLE FOLLICULOGENESISMULTIPLE FOLLICULOGENESIS– MULTIPLE PREGNANCIES – 20%!MULTIPLE PREGNANCIES – 20%!– OHSS – (severe 1-3%)OHSS – (severe 1-3%)
• HIGH MISCARRIAGE RATEHIGH MISCARRIAGE RATE (25%)(25%)
Low dose protocolsLow dose protocols
•Step-down
•Step up
•Sequential
step-up/step-down

LOW DOSE FSHLOW DOSE FSHThe FSH threshold theoryThe FSH threshold theory
1414 77 77
DAYSDAYS
37.537.5
37.537.5

Low dose FSHLow dose FSH
•Monovulation 70%Monovulation 70%
•Fecundity/cycle 20%Fecundity/cycle 20%
• OHSS <0.1%OHSS <0.1%
•Multiple pregnancies 6%Multiple pregnancies 6%

FSH or HMG in PCOS?FSH or HMG in PCOS?Recombinant or urinary FSH?Recombinant or urinary FSH?
• Same pregnancy rates
• Same OHSS rates
• Same multiple pregnancy rate
OBESE PCOS - LOSS OF WEIGHTOBESE PCOS - LOSS OF WEIGHT
Improves signs of hyperandrogenismImproves signs of hyperandrogenismInduces/facilitates ovulationInduces/facilitates ovulation
Loss of >5% of body weight -Loss of >5% of body weight - Reduces - insulin levelsReduces - insulin levels - ovarian androgen production- ovarian androgen production - circulating free testosterone- circulating free testosterone Increases - SHBG, IGFBP-1 Increases - SHBG, IGFBP-1 75% conceived75% conceived
Insulin sensitizing agentsInsulin sensitizing agents Metformin (Glucophage) Metformin (Glucophage)
• Inhibits hepatic glucose production.Inhibits hepatic glucose production.
• Reduces insulin resistance and secretion.Reduces insulin resistance and secretion.
• Causes weigh loss.Causes weigh loss.
• Directly inhibits ovarian steroidogenesis.Directly inhibits ovarian steroidogenesis.
• Reduces T, free T, A4, DHEAS, LH,Reduces T, free T, A4, DHEAS, LH,
Waist to hip ratio, BMI, BP.Waist to hip ratio, BMI, BP.
• Increases FSH, SHBGIncreases FSH, SHBG
• Side effects - gastrointestinal (30%).Side effects - gastrointestinal (30%).
• 1500mg-2500mg/day, at least 3 months.1500mg-2500mg/day, at least 3 months.

Metformin as adjuvant therapy for Metformin as adjuvant therapy for induction of ovulationinduction of ovulation
• Restored menstruation and ovulation Restored menstruation and ovulation
• Improves ovulation rate with CCImproves ovulation rate with CC
• Metformin + FSH = fewer follicles, less Metformin + FSH = fewer follicles, less OHSSOHSS
• Improved quality of mature oocytes, Improved quality of mature oocytes, fertilization & pregnancy ratesfertilization & pregnancy rates

Laparoscopic Ovarian “Drilling”/CauterizationLaparoscopic Ovarian “Drilling”/Cauterization))Stein-Leventhal - wedge resectionStein-Leventhal - wedge resection

Treatment sequence in PCOSTreatment sequence in PCOSWeight loss / change life stileWeight loss / change life stile
ClomipheneClomiphene
Low dose FSHLow dose FSH
Metformin (only if insulin Metformin (only if insulin resistant/obese?)resistant/obese?)
GnRH-agonist (if LH very high)GnRH-agonist (if LH very high)
Laparoscopic ovarian drillingLaparoscopic ovarian drilling
IVFIVF
?