Polycystic ovarian syndrome - Semmelweis
54
Polycystic ovarian syndrome Zoltán Garamvölgyi M.D.
Transcript of Polycystic ovarian syndrome - Semmelweis

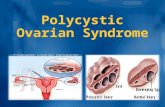
Polycystic ovarian syndrome
Zoltán Garamvölgyi M.D.

Polycystic ovarian syndrome (PCOS)
Most common female endocrin disorder, eg. in German 1 million females
1921. C. Achard and J. Thiers: 7 obese women with hirsutism
Hyperandrogenism associated with carbohydret disorder
„Diabetic women with moustaches“
1935. Stein and Leventhal „polycystic ovaries, hirsutism, amenorrhea, obesity”(may occur in women without ovarian cysts)Menstrual cycle disorders and infertility due to hyperandrogenism andchronic anovulation

Stein IF, Leventhal ML. Amenorrhea associated with bilateral polycystic ovaries. Am J Obstet Gynecol 1935; 29: 181-910

PCOS: from “the diabetes of
bearded women” to Rotterdam
2003 and beyond
1921 1947 1968 1976 1980 1990 2003
Archad and
Thiers, the
diabetes of
bearded women
Kierland et al,
Acanthosis nigricans
is frequent in women
with
hyperandrogenism and
diabetes
Bron and Winkelmann
suggested a genetic
base for Insulin
resistance diabetes
mellitus
Khan et al.
Focus on the
association between
insulin resistance,
acanthosis
nigricans, and
hyperandrogenism
Burghen et al.
PCOS with
hyperandrogenism
had insulin
resistance
NIH expert conference
1) Hyperandrogenism
2) Oligo-ovulation
3) Exclusion of other
disorders
Rotterdam criteria1) Oligo/anovulation
2) Clinical or biochemical
hyperandrogenism
3) Polycystic ovariesStein and
Leventhal
Amenorrhea with
Polycystic ovaries
1935 2011

NIH (United States National Institutes of Health) 1990.
oligo-ovulation or anovulation (oligomenorrhea, amenorrhea)
hyperandrogenism (clinical or/and biochemical evidence of androgen excess)
exclusion of other disorders (menstrual irreg., hyperandrogenism)
Diagnostic criteria
The Androgen Excess and PCOS Society (AE-PCOS) 2006.
Oligo-ovulation and/or polycystic ovaries
Clinical/biochemical evidence of hyperandrogenism
Exclusion of related disorders PCOS, Rotterdam-criterions 2003 (ESHRE/ASRM)Diagnosed when 2 of the 3 criterions fulfilled:
1. chronic anovulation (oligo- or amenorrhea)2. Clinical and/or biochemical
hyperandrogenism3. polycystic ovaries

United States: 4-12%, European countries: 6,5-8%
Ethnic variability in hirsutismAsian: less hirsutism than white women given the same serum androgen values.
In hirsute women: sign. increase in the incidence of acne/menstrualirregul./polycystic ovaries/acanthosis nigricans
PCOS affects premenopausal women
The age of onset is perimenarchal.
(fast mature of reproductive axis/weight gain, less exercise unmaskes PCOS, early manifestation)
Epidemiology

Hispanian women: insulin resistance worse than in caucasian women
Lean women:unmasked when gain weight
Serena Williams

High serum cc. of androgenic hormones (testosterone, androstendione, DHEAS)Individual variation (might have normal androgen levels)
Peripheral insulin resistance and hyperinsulinemia
Obesity
Etiology

Etiology
direct effect on muscle/fatty tissue/liver/ovaries (theca and granulosacells)
Insulin resistance:Secondary to a postbinding defect in insulin rec. signaling pathways
Supression of hepatic generation of SHBG
Supr. of adiponectin (regulates of lipid metab. and glucose levels)
Increased production of IGF-1
Dyslipidemia
PAI-1 increasing (plasminogen activator inhibitor) (risk for thrombosis)
Insulin

Etiology
Hyperinsulinemia not equal with PCOS.
Not every PCOS women have IR.
(genetic background, gene polymorphism: cysteinprotease Calpain 10, proinsulin, insulinrec. (IRS-1, IRS-2)

PCOS: not a consequence of IR!Theca + granulosacells have inzulinreceptors:
Insulin is in synergism with LH.Rec.: insulin + IGF-1.
The androgen production increases. Effect on the ACTH- cortisol axis,
facilitats the androgen production of the adrenalgls.
Insulin enhances the sensitivity of the gran.cells to the FSH: the number of the follicles increase
Enhanced IR: anovulatorical cycles + hyperandrogenism
Damage of the postreceptor pathway of the insulin!

Normal: IRS1 activates the PI3: the intracellular glucose transport increases.
PCOS:the autophosphorisation of the tyrosin decreases, the serin phosphorilisation increasesActivation of the cytochrom P450c17α (adr.glands + ovaries) – level of the androgens increases.
Insulin blocks the production of the IGFBP-1 of the liver: IGF-1 cc. increasesEffect on the granulosacells + thecacells (LH and androgens cc. increase).
Obesity and PCOS:normal LH cc. can also enhancesthe receptors of the LH and the sensitivity of the ovaries to the LH
25 % of the hyperandrogenism of the PCOS is due to the adr.glands!
Peripherial androstendion transforms to testosteron and DHT (5α-reductase)

Ovarial effect of the insulin
Acts on atypical IGF receptors
Upregulation of the IGF-I receptor
Decreases of the IGF-bp cc.
Synergism with the IGF-I and LH
in the androgen production
Hypophyseal effect of the insulin
Anovulation
Endometrial effect of the insulin
Blocks the implantation

Granulosa cell

Etiology Hypothalamic intrinsic disorder + low progesteron cc.Decreased progesteron-sensitivity? (Flutamid- androgen rec. antagonist-increases prog.sensitivity)
GnRH-puls frequence increasing
Pituitary: LH increasing (LH>FSH)
Ovaries: theca-cells: cytochrom P450 c17 (17α-hydroxylase + 17,20 lyase activity)
Androstendion production
17β-hydroxysteroid-dehydrogenase
Testosteron
Eostrogen cc. increases
Gran.cells: FSH decreases

„Two cells- two gonadotropins „ hypothesis
LH
LH-receptor
FSH
FSH-receptor
ATP cAMP
cholesterin
androstendion
Blood vessels
androstendion estrogen
aromatase enzyme
ATP cAMP
Fluid of the follicles
LH-receptor
thecacells
granulosacells

Genetically heterogeneous syndromeDifficult condition to study genetically, candidategene?Fathers of PCOS women: can be abnormal hairyMothers: oligomenorrhea
Family history of type2 diabetes in a first-degreefamily member
Dutch twin-family study: PCOS heritability of 0,71 in monozygotic twin sisters
Link between PCOS and obesity, associated genes:FTO-geneCYP17 promoter activity 4x in cells of PCOS womenHomozygous for an allele of interest in IGF2 (stimulates androgen secretion in the ovaries and adrenal glands)
Genome-wide association:Chinese population: 2p16 locus: near genes formate testis/encode LH-rec and hCG.Near FSHR gene (encodes FSH-receptor)
Family history:
•Menstrual disorders•Adrenal enzyme deficiences•Hirsutism•Infertility•Obesity and metabolic sy. •Diabetes

Intrauterin environment
Maternal: Diabetes
GDM
PCOS
Obesity
Hypothyreoidism

GnRH/LH ↑
PCO PCOS
Chronical anovulation
Insulinresistance Hyperandrogenism
Serotonin↓GABA↑
Pathomechanism of the PCOS
Dopamin ↓ Opioids ↓
Burghen et al: JCEM 1980, 50, 113
Depressive disorders: 35 % (3X)


Phenotypes of the PCOS
Hyperandrogenism + not obes + non IR Extrem obesity + IR + hyperandrogenism
PCOS Severe(complet)
Fourthphenotype
Ovulation Mild(non hyperandrogenic)
Bleeding irregular irregular reggular irregular
UH PCO normal PCO PCO
Androgen cc. high high high Minimal increased
Insulin cc. low high high Normal
Frequency 61% 7% 16% 16%

Metabolic disorder > Metabolic disorderHyperandr./hirsut. Hyperandr./hirsut.Oligoanovulátion Ovulatory ciclus
PCO-form
Hyperinsulinaemia > HyperinsulinaemiaMetabolic sy.: 42,3 %2TDM : 3-6 %
signs A B C D E F G H I
Hyperandr + + + + - - + - +
Hirsutismus + + - - + + + + -
Oligoanov + + + + + + - - -
PCO. + - + - + - + + +
AES, 2006.

0
10
20
30
40
50
60
70
80
90
100
Norm Non
PCOS
obes
PCOS
thin
PCOS
obes
Insulin sensitivity

Signs Frequency
sterility 74%
hirsutism 68%
Irregular bleeding 52%
obesity 44%

Bilaterally or unilaterally enlarged, polycystic ovariesHyperplasia of the theca stromal cells surrounding arrested follicles
80-100 % of all PCOS women. Enlarged ovaries not always be present. >= 12 follicles (2-8 mm in size)
23 % of women with normal menstrual cycle have polycystic ovaries.
Enlarged, polycystic ovaries
Anovulation, monophasic cycle, disorder of the selection of thefollicules because of the prolonged follicular menstrual phase
Overstimulation, twin pregnancies
75 %

Chronic anovulation (menstrual disturbance in premenarche)
Oligomenorrhea (menstr. bleeding occurs at intervals of 35 daysto 6 months, < 9 menstrual periods per year)
Secondary amenorrhea (an absence of menstruation for 6 months)
Ovulatory and menstrual dysfunction 75%

75 % of PCOS women: primaer or secondary sterilitydue to anovulation
Rate of miscarrieges is high: 25-44%
Infertility

ABORTUS SPONTANEUS Maternal Chr. Subclinicalinflammation
Embryo/fetus?Habitualis ab.: 40-80 % of PCOS!
LH: effect on to the implantation (non PCOS vs PCOS= 12-15% vs 30-50%)
Uterinal factor: perifollicular bloodcirculation worse
Folliculus gene expression (androgén hatás)
IGF-1: Y IGF-1 rec. downregulation
(morula’s gl.uptake decreases before the implantation)
GLUT-4 (cc. decr.)
IGFBP-1(cc.decr.) implantation/adhesion romlik

Diabetes Prevention Program (DPP)Troglitazine in prevention of Diabetes (TRIPOD)
Metformin and PCOS
CC CC + metformin
Ovulation 42 % 76 %
More effective:>28 age + visceral.fatty tissue
(p<0,001) CC CC + metformin metformin
Pregnancy 22,5 % 26,8 % 7,2 %

Metformin és PCOS
Diabetes Prevention Program (DPP)Troglitazine in prevention of Diabetes (TRIPOD)
Ab.spontaneus Metformin vs. placebo Odds r. 0,36, 95% CI, 0,09-1,47
CC vs. CC + metformin Odds r. 1,61, 95% CI, 1,00-2,60
No advantage
Metformin placebo
PE 7,4 % 3,7 % P=0,18
GDM 17,6 % 16,9 % P=0,87
Premature
labour
3,7 % 8,2 % P=0,12
Σ 25 % 24,4 % P=0,78Previous GDM: metformin mitigates 2TDM risk 50 % vs 14 %

excess terminal body hair in a male distribution pattern(upper lip, chin, nipples, linea alba, lower abdomen)
acneandrogenic alopecia
other signs: clitoromegaly+ increased mucle mass + voicedeepening
(extreme forms of PCOS, hyperthecosis or androgen-producingtumors, virilizing congenital adrenal hyperplasia)
Hyperandrogenism 60-80%

Female type of metabolic sy.?Manifestation: later than acne or hirsutism.
50% of PCOS women are obese.28 % of all obese women suffered from PCOS.
American PCOS women have a higher BMI than italian PCOS women.
PCOS: obesity and metabolic syndrome
43% prevalence of metabolic syndrome, characterized by:
→abdominal obesity (waist circumference: >88 cm.)→dyslipidemia (TG level > 150 mg/dL)→ High-density lipoprotein cholesterol (HDL-C) level <50 mg/dL→ elevated blood pressure (> 130/85 mmHg)→ IFG or IGT
(>=3: metabolic sy. )
+: elevated C-reactive protein level, elevated plasminogen
activator inhibitor-1 (PAI-1), fibrinogen levels.

1/3 of PCOS women had IFG or IGT within 13-19 years old
40% of patients with PCOS have insulin resistance that is independent of body weight.(increased risk for type 2 diabetes and cardiovascular complications)
American Association of Clinical Endocrinologists:
screening for diabetes by age 30 years in all patients with PCOS! Should be periodically reassessed throughout their lifetime.
Every 3-5 years screening for diabetes!
PCOS: obesity and metabolic syndrome

PCOS: obesity and metabolic syndrome
Diabetes mellitus:
Insulin resistance compensated long in most PCOS women. (problem in women with positive familiy history.)
2 type diabetes risk: 7x
10% of women with PCOS have type 2 diabetes mellitus
30-40 % of women with PCOS have impaired glucose tolernace (IGT) by 40 yeares of age
Screening with OGTT. Early diagnosis. Latens state of insulin resistance willchanged to manifested IR in GDM/th. with glucocorticoids
HOMA-index:
normal ≤ 1suspicious of IR: > 2 possibility of IR: > 2,5 diabetes mellitus: > 5

Elevated serum lipoprotein levelsLean PCOS women: also endothelian dysfunction (thickened intima media)
CRP and endothelin-1 increase
Coronarian diseases and macroangiopathy: TG/LDL increase, HDL level decreasescoronary artery calcification
Risk for AMI:7X in women at age of 40-60 years
Sleep apnea: obstructive sleep apnea syndrome (OSAS)An independent risk factor for cardiovascular disease. (excessive daytime somnolence)
HypoD-vitamism (73%)Vit.D-gene regulates 3% of the human genom (glucose/lipid/ metabolism/blood pressure)
Decreased D-vit. level associated with•Dylipidemia•Insulin resistance•Obesity
Risk for cardiovascular and cerebrovascular disease

Increased risk for endometrial hyperplasia and carcinoma. (constant endometrial stimulation with estrogen without progesterone).
Recommended induction of withdrawal bleeding with progesterons a minimum of every 3-4 months.
No known association with breast or ovarian cancer has been found.
Carcinoma

common symptom of PCOS.Rare in japanese women with PCOS. (In caucasian PCOS women: 9% hirsutism)
In the skin-cells:
testosteron ---- 5α-reductase ---- dihydrotestosteron (DHT)the enzyme is activated by insulin/IGF-1/androgens
Physical examinationHirsutism and virilizing signs
Hirsutism: 60 %

1961: Ferriman-Gallwey score (9 body areas. 0 (no hair) to 4 (frankly virile))
upper lip, chin, chest, upper and lower abdomenthighs, upper and lower back, arm, forearm, buttocks. >=8: hirsutism
A total score of 8 or more: abnormal for an adult white womenScore of 44: most severe
The modified Ferriman-Gallwey score grades 11 body areas.

Acne:12 % of all adult women23-35 % of all PCOS women.
Androgen alopecia: 5 %not common, responsible is the DHT (+ ovarian and adrenalandrogenes)
Physical examination
Hirsutism and virilizing signs

Diffuse, velvety thickening and hyperpigmentation of the skin
Present at the nape of the neck/axillae/beneath the breasts/intertriginousareas/exposed areas (elbows, knuckles)
Result of insulin resistance.
Can also be a cutaneous marker of malignancy!
Physical examination Acanthosis nigricans
Scoring system: Absent (0)Present (1): on close visual inspection, extent not measurableMild (2): limited to the base of the skull (does not extend tot the lateral margins of the neck)Moderate (3): extends tot he lateral margins of the neckSevere (4): visible anteriorlySevere (5): circumferential

PCOS appearance
forms
Hyperandrogenism, acne, hirsutism
,acanthosis nigricansalopecia
Menstruation disorder,oligo/anovulation and
Sterility
Psychologicalproblems,
Depression
dermatologistendocrinologist
DiabetologistEndocrinologist
Gynecologist
Psychologist
Insulin resistanceHyperinsulinism
2TDM
Worsening folliclesquality
Unsuccessful ART
IVFspecialist

PCOS: else metab./endocrin. disorders
CRH-ACTH-kortizol axis activated
Hyperreninaemia/hyperaldosteronismus
PRL 2-3X
PAI-1/fibrinogen incr.
Hyperuricaemia/homociszteinaemia
Ferritin cc. Incr. (storage of iron incr.)
NAD(P)H-oxidase aktiv.Szuperoxid freeradical incr.
obesity
Musculature: gl.uptake decr.
Liver: inz.metab.decr.IR
GI tr.:Iron uptake incr.

Diagnosis of the PCOS
testosterone (total or free) and SHBG
Free Androgen Index (FAI).
FAI = total testosterone [nmol/l] x 100 / SHBG [nmol/l]
LH, FSH, estradiol, progesteron, prolaktin, TSH
17-OH progesteron, androstendion, DHEAS, basal cortisol
LH>FSH (2x-3x): seeing in follicule phase of the menstrual cycle
OGTT
Liver enzymes, kidney function, serum ions

LHRH-test: 25 ug Buserelin iv. 0-30-60 min. (GnRH-analog: the constans stimulation of the pituitarydecreases LH and FSH secretion)
LH level increasing > FSH level increasing (not diagnostic)
Diagnosis of PCOS

DD.:
Ovarian hyperthecosis (luteinized cells throughout the stroma)
Congenital adrenal hyperplasia (late-onset)
Drugs (Danazol, androgenic progestins)
Hypothyroidism
Idiopathic/familial hirsutism
Masculinizing tumors of the adrenal gland or ovary (rapid onset of signs of
virilisation)
Cushing –sy. (low K+, striae, central obesity, high cortisol, high androgens)
Hyperprolactinemia
Exogenous anabolic steroid use
Stromal hyperthecosis (valproic acid)
Diagnostic considerations

Therapy of the PCOS
Variability of the clinical symptomps!
Fit the therapy to the
• Actuel symptomps (hirsutism, acne etc.)
• Wishes (contraception, pregnancy)
• Different life periods (adolescence, praemenopausa, postmenopausa)

Oral contraceptive pill
estragens: LH level decreases/SHBG level increasesbut: insulin resistance and cardiovascular risk enhanced(recommended progestin only pill)
progestins: II.generations of the progestins- levonogestrel- have androgen effect!cyproteron acetat Le Figaro: „Sept décès en France liés à la pilule Diane 35”
dienogestspironolacton
flutamid (non steroid antiandrogen drug: very effective, but hepatotoxic effect)
Glucocorticoids (Lowers only adrenal glands –DHEA,DHEAS, androstendion-androgens level)
Finasterid (non steroid antiandrogen drug: benign hyperplasia of prostata, against adrogen alopecia)
Therapy of the PCOS

Induce the sensitivity of insulinby more exercise/life style modifications/insulin sensitisers
Insulin sensitisers:
Metformin(contraindicated the use of it in pregnancy in Hungary/German)
Thiazolidtroglitazon: effective, but hepatotoxic (1997.: prohibited in the U.K.)rosiglitazon: not hepatotoxic, but increase the liver enzymes reversible.
Enzyme inhibitors:
Acarbose /Glucobay/Lowers the enteral uptake/absorption of glucose, lowers the postprandialhyperinsulinemiaReversible blocks (competetive antagonism) the α-glucosidase-hydroxylaseenzyme of the bowel-musosa. Flatulation, tenesmus, diarrhea!
Therapy of the PCOS


Inositol:
6-C-atoms, cyclic polyalcohol.
9 stereo-isomer knownmyo-inositol:The most frequent natural form

• Intracellular Ca2++ cc. control– Maintenance of the cellular membranpotential
• Metabolic effects– Insulin signal transduction– Lipolysis , serum cholesterin cc. decreasing
• Other– Serotonin activity modulation– Nervous system regulation
• Gen expression
Function of the inositolSignal transmission and sec. messenger

Inositol-foszfolipid-Ca++ as sec. messenger
OOCYTA evolutionOOCYTAMaturity
FERTILISATION(early stadium)

METFORMIN (biguanid)PRO: Insulinsensitiser
KONTRA: GI side effects
CLOMIPHENE CITRATE
PRO: Anti-oestrogen, stimulation of the FSH, LH secretion
KONTRA endometrium atrophied
EXOGEN GONADOTROPIN
PRO: direct effect on the ovaries, subcutan injection,
monitorisation of its effect by ultrasound
KONTRA Ovarium hyperstimulation syndrome
Combined therapy:Metformin + clomiphen citrate:>28 years, waist-hip ratio is high
(metformin therapy decreases the development of the hyperstimulation)
Ovulation: 60-85 %
Pregnancy: 30-50 %
After 6 ovulatory cycles

Therapy of the PCOS
Clomiphen-resistance: laparoscopic ovarian drilling
ovulation increasing (30% to 90%)
possibility of gravidity increasing (13,5 to 88 %)