Polycystic Ovarian Syndrome (PCOS) Pathophysiology
48
1 Polycystic Ovarian Polycystic Ovarian Syndrome (PCOS) Syndrome (PCOS) Pathophysiology & Wider Pathophysiology & Wider Health Issues Health Issues Dr. Mariam Al-Saqqa Dr. Mariam Al-Saqqa Consultant Obstetrics & Consultant Obstetrics & Gynecology Gynecology
Transcript of Polycystic Ovarian Syndrome (PCOS) Pathophysiology

11
Polycystic Ovarian Syndrome Polycystic Ovarian Syndrome (PCOS) Pathophysiology & (PCOS) Pathophysiology &
Wider Health IssuesWider Health Issues
Dr. Mariam Al-SaqqaDr. Mariam Al-Saqqa
Consultant Obstetrics & Consultant Obstetrics & Gynecology Gynecology

22
IntroductionIntroduction::
• In 1935 Stein & Leventhal described In 1935 Stein & Leventhal described seven women presenting with seven women presenting with oligomenorrhea combined with the oligomenorrhea combined with the presence of bilateral polycystic ovaries presence of bilateral polycystic ovaries (PCO) established during surgery.(PCO) established during surgery.
• Three of these seven women also Three of these seven women also presented with obesity, while five presented with obesity, while five showed signs of hirsutism.showed signs of hirsutism.

33
Introduction (cont)Introduction (cont)::
• Only one woman has both obesity & Only one woman has both obesity & showed hirsutism.showed hirsutism.
• The polycystic ovarian syndrome, The polycystic ovarian syndrome, one of the most common causes of one of the most common causes of infertility due to anovulation infertility due to anovulation affecting 4-10% of women affecting 4-10% of women

44
Introduction (cont)Introduction (cont)::
• The presentations of PCOS are heterogeneous The presentations of PCOS are heterogeneous & may change through out the lifespan, & may change through out the lifespan, starting from adolescence to post-menopausal starting from adolescence to post-menopausal age, & may have health impaction later in life.age, & may have health impaction later in life.
• Rotterdam consensus 2003, PCOS is defined as Rotterdam consensus 2003, PCOS is defined as a syndrome of ovulation dysfunction along with a syndrome of ovulation dysfunction along with the cardinal features of hyperandrogenism & the cardinal features of hyperandrogenism & polycystic ovaries morphology.polycystic ovaries morphology.

55
Pathophysiology of PCOSPathophysiology of PCOS::
• PCOS is a condition that originates possibly PCOS is a condition that originates possibly at the time of puberty due to interplay of:at the time of puberty due to interplay of:
(1) obesity & excess of ovarian androgen (1) obesity & excess of ovarian androgen production, due to hyperinsulinemiaproduction, due to hyperinsulinemia
(2)(2) intrauterine environment.intrauterine environment. (3) genetic factors both X-linked, autosomal (3) genetic factors both X-linked, autosomal
dominant modes dominant modes of inheritance.of inheritance.
(4) disturbance to hypothalamic-pituitary-(4) disturbance to hypothalamic-pituitary-ovarian axis.ovarian axis.

66
(1) Impact of obesity in PCOS (1) Impact of obesity in PCOS pathophysiology:pathophysiology:
• Obesity is strongly associated with PCOS, Obesity is strongly associated with PCOS, it ranges from 30%-75% of cases.it ranges from 30%-75% of cases.
• Increased body weight in PCOS is often Increased body weight in PCOS is often due to increased visceral fat, central due to increased visceral fat, central obesity which is particularly associated obesity which is particularly associated with increased risk of cardiovascular with increased risk of cardiovascular diseases & type 2 diabetes & diseases & type 2 diabetes & hypertention.hypertention.

77
Impact of obesity in PCOS Impact of obesity in PCOS pathophysiology (cont)pathophysiology (cont): :
• Obesity induces, through the path of insulin Obesity induces, through the path of insulin resistance, high levels of insulin-related resistance, high levels of insulin-related growth factors, these will stimulate theca cells growth factors, these will stimulate theca cells to produce supranormal amounts of to produce supranormal amounts of androgens & reduce (SHBG) syntheses by liver androgens & reduce (SHBG) syntheses by liver cells, thereby raising the proportion of free cells, thereby raising the proportion of free circulating testosterone. circulating testosterone.
• The resulting androgen excess is considered The resulting androgen excess is considered to contribute to the presence of increased to contribute to the presence of increased number of follicles in all stages, as well as number of follicles in all stages, as well as arrested maturation of (FSH) sensitive follicles.arrested maturation of (FSH) sensitive follicles.

88
Obesity & sex hormone binding Obesity & sex hormone binding protein (SHBG)protein (SHBG)::
• Obesity is considered a condition of Obesity is considered a condition of SHBG imbalance.SHBG imbalance.
• Levels of SHBG tend to decrease with Levels of SHBG tend to decrease with increasing body fat, this lead to an increasing body fat, this lead to an increased fraction of free androgens increased fraction of free androgens delivered to target sensitive tissues.delivered to target sensitive tissues.

99
Obesity & sex hormone binding Obesity & sex hormone binding protein (SHBG)protein (SHBG)::
• SHBG levels are regulated by a complex of SHBG levels are regulated by a complex of factors including estrogens, iodothyronines factors including estrogens, iodothyronines & GH as stimulating agents and androgens & GH as stimulating agents and androgens & insulin as inhibitory factors.& insulin as inhibitory factors.
• The net balance , with the dominant role of The net balance , with the dominant role of insulin which inhibits SHBG synthesis in the insulin which inhibits SHBG synthesis in the liver, may be responsible for the decrease of liver, may be responsible for the decrease of SHBG concentrations observed in obesity.SHBG concentrations observed in obesity.

1010
Role of leptin in the Role of leptin in the pathophysiology of PCOS:pathophysiology of PCOS:
• Leptin is considered as one of the Leptin is considered as one of the major peripheral signals that affects major peripheral signals that affects food intake & energy balance.food intake & energy balance.
• Obesity is a classic condition of Obesity is a classic condition of circulating leptin excess.circulating leptin excess.

1111
Role of leptin in the Role of leptin in the pathophysiology of PCOSpathophysiology of PCOS::
• The discrepancy between increased The discrepancy between increased leptin blood levels & its central effects leptin blood levels & its central effects represents a leptin resistance as represents a leptin resistance as shown by study of Moschos et al 2002 shown by study of Moschos et al 2002 in Fertility Sterility Journal.in Fertility Sterility Journal.
• Mitchell m in 2005, there is evidence Mitchell m in 2005, there is evidence that leptin acts directly on the ovaries that leptin acts directly on the ovaries through functional receptors defect.through functional receptors defect.

1212
Potential role of the Potential role of the endocannabinoid systemendocannabinoid system::
• Endocannabinoids are derivatives of arachidonic Endocannabinoids are derivatives of arachidonic acid & they belong to a family composed of an acid & they belong to a family composed of an increasing numbers of compounds , the most increasing numbers of compounds , the most studied so far being arachidonoyl ethanolamide studied so far being arachidonoyl ethanolamide (AEA) named anandamide.(AEA) named anandamide.
• Pagotto U in Endocrine review 2006, he focused Pagotto U in Endocrine review 2006, he focused on the emerging role of the endocannabinoid on the emerging role of the endocannabinoid system in endocrine regulation & energy system in endocrine regulation & energy balance, through specific cannabiniod receptors balance, through specific cannabiniod receptors type 1 (CB1) & type 2 (CB2).type 1 (CB1) & type 2 (CB2).

1313
Potential role of the Potential role of the endocannabinoid system endocannabinoid system
(cont)(cont)::• An interesting aspect of the endocannabinoid An interesting aspect of the endocannabinoid
system is its activity “on demand”, meaning system is its activity “on demand”, meaning that the system can b activated with a closely that the system can b activated with a closely regulated selectivity: only “when” & “where” it regulated selectivity: only “when” & “where” it is needed.is needed.
• Astonishing amount of data accumulated Astonishing amount of data accumulated providing deeper insights regarding the providing deeper insights regarding the biological notes of the endocannabinoid biological notes of the endocannabinoid system, it can be summarizes that it is system, it can be summarizes that it is involved in different physiological functions involved in different physiological functions many of which are related to the stress many of which are related to the stress recovery systems & to the maintenance of recovery systems & to the maintenance of homeostatic balance.homeostatic balance.

1414
Potential role of the Potential role of the endocannabinoid system endocannabinoid system
(cont):(cont):• Endocannabinoids are deeply involved in the Endocannabinoids are deeply involved in the
dynamic & homeostatic regulation of feeding dynamic & homeostatic regulation of feeding & energy metabolism.& energy metabolism.
• Di Marzo et al 2004 showed that antagonists Di Marzo et al 2004 showed that antagonists of CB1 receptors may reduce food intake.of CB1 receptors may reduce food intake.
• The regulation of metabolic process includes The regulation of metabolic process includes both central at the hypothalamic level & both central at the hypothalamic level & peripheral actions in the adipose tissue & peripheral actions in the adipose tissue & liver.liver.

1515
Potential role of the Potential role of the endocannabinoid system endocannabinoid system
(cont)(cont)::• The peripheral action of the The peripheral action of the
endocannabinoids has been documented in endocannabinoids has been documented in animal models treated with a selective CB1 animal models treated with a selective CB1 antagonist “rimonabant” by Jbiloo et al 2005.antagonist “rimonabant” by Jbiloo et al 2005.
• Despite JP et al 2005 used rimonabant in Despite JP et al 2005 used rimonabant in patients as a new pharmacological treatment patients as a new pharmacological treatment for tackling obesity. for tackling obesity.
• The endocannabinoid system has been found The endocannabinoid system has been found to regulate multiple endocrine functions to regulate multiple endocrine functions including H-P-O axis.including H-P-O axis.

1616
Potential role of the Potential role of the endocannabinoid system endocannabinoid system
(cont)(cont)::• Van et al in Lancet 2005, showed that CB1 Van et al in Lancet 2005, showed that CB1
antagonist have been found to increase antagonist have been found to increase energy expenditure through activation of energy expenditure through activation of futile cycles, enhance lipolysis & stimulate futile cycles, enhance lipolysis & stimulate glucose metabolism increasing glucose glucose metabolism increasing glucose transport for recruitment & activation.transport for recruitment & activation.
• It has been demonstrated that AEA It has been demonstrated that AEA fluctuates during ovarian cycle in both the fluctuates during ovarian cycle in both the hypothalamus & pituitary, thus influencing hypothalamus & pituitary, thus influencing hormonal secretion & sexual behavior hormonal secretion & sexual behavior through CB1 receptor activation. through CB1 receptor activation.

1717
Insulin resistance, Insulin resistance, hyperinsulinemia & hyperinsulinemia & hyperandrogenism:hyperandrogenism:
• The association between increased insulin The association between increased insulin resistance & PCO is well recognized.resistance & PCO is well recognized.
• Acanthosis nigricans in hyperandrogenic Acanthosis nigricans in hyperandrogenic women is dependent upon the presence & women is dependent upon the presence & severity of hyperinsulinemia.severity of hyperinsulinemia.
• There are several mechanisms for the state There are several mechanisms for the state of insulin resistance: peripheral target tissue of insulin resistance: peripheral target tissue resistance, decrease hepatic clearance or resistance, decrease hepatic clearance or increased pancreatic sensitivity.increased pancreatic sensitivity.

1818

1919
Insulin resistance, Insulin resistance, hyperinsulinemia & hyperinsulinemia &
hyperandrogenism (cont)hyperandrogenism (cont)::• Insulin resistance leads to compensatory Insulin resistance leads to compensatory
hyperinsulinemia to the target tissues of hyperinsulinemia to the target tissues of insulin action, that become resistant to insulin action, that become resistant to insulin, the ovaries remain responsive to insulin, the ovaries remain responsive to insulin throughout the interaction with its insulin throughout the interaction with its own receptors, (fasting glucose/insulin ratio own receptors, (fasting glucose/insulin ratio < 0.25 mmol/ mU)< 0.25 mmol/ mU)
• Excess insulin participate in increased Excess insulin participate in increased ovarian androgen syntheses ovarian androgen syntheses (androsteindione & testosterone)(androsteindione & testosterone)

2020
How does hyperinsulinemia How does hyperinsulinemia produse hyperandrogenismproduse hyperandrogenism??
• Android obesity is the result of fat Android obesity is the result of fat deposition in the abdominal wall & deposition in the abdominal wall & visceral mesenteric locations.visceral mesenteric locations.
• This fat is more active metabolically, This fat is more active metabolically, resulting in higher free fatty acid resulting in higher free fatty acid concentrations leading to hyperglycemia.concentrations leading to hyperglycemia.
• At higher concentrations, insulin binds to At higher concentrations, insulin binds to the IGF-1 receptors & augmenting the the IGF-1 receptors & augmenting the thecal androgen production. thecal androgen production.

2121
How does hyperinsulinemia How does hyperinsulinemia produse hyperandrogenismproduse hyperandrogenism??
• Hyperinsulinemia leads to inhibition of Hyperinsulinemia leads to inhibition of hepatic syntheses of SHBG & inhibition of hepatic syntheses of SHBG & inhibition of hepatic production of IGF-1 binding protein.hepatic production of IGF-1 binding protein.
• In vitro studies indicate that both insulin & In vitro studies indicate that both insulin & IGF-1 directly inhibit SHBG secretion by IGF-1 directly inhibit SHBG secretion by human hepatoma cells.human hepatoma cells.
• Hyperandrogenism, considered Hyperandrogenism, considered biochemically, free androgen index > 4.5 biochemically, free androgen index > 4.5 (FAI= total testosterone x 100 /SHBG). (FAI= total testosterone x 100 /SHBG).

2222
Metabolic abnormalities in Metabolic abnormalities in PCOSPCOS::
• Several metabolic abnormalities that are Several metabolic abnormalities that are strongly influenced by the presence of obesity.strongly influenced by the presence of obesity.
• Obese women affected by PCOS who present Obese women affected by PCOS who present with glucose intolerance ranging from 20- 49%.with glucose intolerance ranging from 20- 49%.
• Alterations of both lipid & lipoprotein Alterations of both lipid & lipoprotein metabolism, the coexistence of obesity leads metabolism, the coexistence of obesity leads to more atherogenic lipoprotein pattern.to more atherogenic lipoprotein pattern.

2323
Metabolic abnormalities in Metabolic abnormalities in PCOSPCOS::
• A great reduction of (HDL) with higher A great reduction of (HDL) with higher increase of both triglycerides & total increase of both triglycerides & total cholesterol, may make them prone to cholesterol, may make them prone to hypertension as well.hypertension as well.
• Risk of atherosclerosis & premature Risk of atherosclerosis & premature cardiovascular events increases cardiovascular events increases whether or not the woman is diabetic. whether or not the woman is diabetic.

2424
((22 ) )Intrauterine environment & Intrauterine environment & PCOSPCOS::
• Hague et al 1988 postulated that the intrauterine Hague et al 1988 postulated that the intrauterine environment has a role in the pathogenesis of environment has a role in the pathogenesis of PCOS, & suggested that hyperandrogenism PCOS, & suggested that hyperandrogenism during fetal life may be the determining factor.during fetal life may be the determining factor.
• The apparent influence of intrauterine milieu in The apparent influence of intrauterine milieu in poorly controlled diabetics who end with stillborn poorly controlled diabetics who end with stillborn fetuses, showed ovarian changes similar to those fetuses, showed ovarian changes similar to those seen in PCOS.seen in PCOS.
• Aerts et al have shown that maternal diabetes Aerts et al have shown that maternal diabetes induces insulin resistance in her offspring, this induces insulin resistance in her offspring, this defect is acquired & not hereditary.defect is acquired & not hereditary.

2525
(3) Familial studies of PCOS:(3) Familial studies of PCOS:
• Goind et al 1999 studied 1Goind et al 1999 studied 1stst degree degree relatives of 29 women affected by PCOS relatives of 29 women affected by PCOS & 10 asymptomatic control volunteers of & 10 asymptomatic control volunteers of reproductive age; sibling of the PCOS reproductive age; sibling of the PCOS probands were affected for a probands were affected for a segregation ratio of 55% which is segregation ratio of 55% which is considered with autosomal dominant considered with autosomal dominant inheritance with nearly complete inheritance with nearly complete penetrance in comparison to the control penetrance in comparison to the control families with segregation ratio of 25% families with segregation ratio of 25%

2626
Familial studies of PCOS Familial studies of PCOS (cont)(cont)::
• Urbbanek et al 1999, carried out a Urbbanek et al 1999, carried out a multicenter study using the same multicenter study using the same diagnostic criteria for PCOS, tested 37 diagnostic criteria for PCOS, tested 37 candidate genes for PCOS from 150 candidate genes for PCOS from 150 families with at least one affected families with at least one affected member, they found follistatin gene with member, they found follistatin gene with the strongest evidence & remained the strongest evidence & remained significant even after correction for significant even after correction for multiple testing.multiple testing.

2727
Familial studies of PCOS Familial studies of PCOS (cont)(cont)::
• Follistatin is a glycosylated Follistatin is a glycosylated polypeptide homologous to polypeptide homologous to epidermal growth factor, it binds to epidermal growth factor, it binds to activin thereby reducing serum activin thereby reducing serum follicle stimulating hormone levels & follicle stimulating hormone levels & increasing ovarian androgen increasing ovarian androgen production.production.

2828
((44 ) )The disturbance of the The disturbance of the hypothalamic-pituitary-ovarian hypothalamic-pituitary-ovarian
axis H-P-Oaxis H-P-O::• Evidence of dysfunction at the level of both Evidence of dysfunction at the level of both
the pituitary & the ovary in women with PCOS the pituitary & the ovary in women with PCOS gave rise to the hypothesis of self-perpetual gave rise to the hypothesis of self-perpetual vicious cycles.vicious cycles.
• Abnormal gonadotrophin secretion Abnormal gonadotrophin secretion characterized by overproduction of LH characterized by overproduction of LH relative to FSH induces hyperactivity of relative to FSH induces hyperactivity of ovarian stromal tissue, atresia of antral ovarian stromal tissue, atresia of antral follicles & disordered ovarian steroidogenesis.follicles & disordered ovarian steroidogenesis.
• The resulting imbalance of estrogenic & The resulting imbalance of estrogenic & androgenic steroids in turn accentuates the androgenic steroids in turn accentuates the hypersecretion of LH by anterior pituitary.hypersecretion of LH by anterior pituitary.

2929
Abnormal folliculogenesisAbnormal folliculogenesis::
• Estradiol levels may not fall low enough to allow Estradiol levels may not fall low enough to allow sufficient FSH response for initial growth sufficient FSH response for initial growth stimulus & levels of estradiol may be inadequate stimulus & levels of estradiol may be inadequate to produce the positive stimulatory effects to produce the positive stimulatory effects necessary to induce the ovulatory surge of LH. necessary to induce the ovulatory surge of LH.
• The mechanism of the disturbed folliculogenesis The mechanism of the disturbed folliculogenesis includes relative FSH deficiency & loss of LH includes relative FSH deficiency & loss of LH stimulation, deficiency of certain local growth stimulation, deficiency of certain local growth factors & abnormal ovarian steroidogenesis.factors & abnormal ovarian steroidogenesis.

3030
Abnormal steroidogenesisAbnormal steroidogenesis::
• The LH stimulates the theca cells to The LH stimulates the theca cells to produce androgens witch are the produce androgens witch are the precursor for estrogen synthesis.precursor for estrogen synthesis.
• The raising intraovarian estrogen & inhibin The raising intraovarian estrogen & inhibin B concentration result in a negative B concentration result in a negative feedback on FSH secretion & a positive feedback on FSH secretion & a positive feedback on LH secretion.feedback on LH secretion.
• The resulting increase in LH, together with The resulting increase in LH, together with the rising inhibin B level, leads to further the rising inhibin B level, leads to further increase of androgen.increase of androgen.

3131
Abnormal LH stimulusAbnormal LH stimulus
• Granulosa cells of small antral follicles in Granulosa cells of small antral follicles in anovulatory women with PCOS acquire LH anovulatory women with PCOS acquire LH receptors prematurely at follicular diameter receptors prematurely at follicular diameter of 4mm.of 4mm.
• LH receptors acquisition of the granulosa LH receptors acquisition of the granulosa cells seem to switch the follicle from cells seem to switch the follicle from proliferative to differentiation, resulting in a proliferative to differentiation, resulting in a suppression of granulosa cell growth & suppression of granulosa cell growth & ultimately inducing an arrest of follicular ultimately inducing an arrest of follicular development & a failure of dominance. development & a failure of dominance.

3232
Clinical features of PCOSClinical features of PCOS::
oMenstrual abnormalities 80%Menstrual abnormalities 80%o Infertility “anovulation”Infertility “anovulation”oHirsutism 60%, acne 70%, alopleciaHirsutism 60%, acne 70%, alopleciao Increased risk of atherosclerosis & Increased risk of atherosclerosis &
cardiovascular events.cardiovascular events.o Increased risk of diabetes mellitus in Increased risk of diabetes mellitus in
patients with hyperinsulinemia.patients with hyperinsulinemia.

3333
Clinical features of PCOSClinical features of PCOS::
o Increased risk of endomentreal cancer & ? Increased risk of endomentreal cancer & ? Breast cancerBreast cancer
o Hyperlipidemia with its impact on Hyperlipidemia with its impact on atherosclerotic changes.atherosclerotic changes.
o Hypertension observed later in lifeHypertension observed later in lifeo Obesity 40% with health risks including Obesity 40% with health risks including
saphenous varicosities, hemorrhoids, saphenous varicosities, hemorrhoids, hernias & osteoarthritis.hernias & osteoarthritis.
o Several mental health problems, Several mental health problems, depression, anxiety..etcdepression, anxiety..etc

3434
Criteria for classification of Criteria for classification of PCOSPCOS::
Major criteriaMajor criteria
• AnovulationAnovulation
• OligominorrheaOligominorrhea
• HyperandrogenemiHyperandrogenemiaa
• Severe hirsutismSevere hirsutism
• Insulin resistanceInsulin resistance
Minor criteriaMinor criteria
• Polycystic ovaries Polycystic ovaries on ultrasoundon ultrasound
• Elevated LH:FSHElevated LH:FSH
• AcneAcne
• Mild hirsutismMild hirsutism
• ObesityObesity

3535
Diagnosis of PCOSDiagnosis of PCOS::
TendencyTendency of PCOS; presence of one minor of PCOS; presence of one minor criteriacriteria
Mild formMild form of PCOS; presence of two minor of PCOS; presence of two minor criteriacriteria
Moderate formModerate form of PCOS; presence of one of PCOS; presence of one major & one minor criteriamajor & one minor criteria
Severe formSevere form of PCOS; presence of one or of PCOS; presence of one or more major & two or more minor criteria.more major & two or more minor criteria.

3636

3737

3838
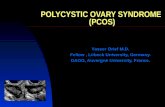
Differential diagnosis of Differential diagnosis of PCOSPCOS::
The differential diagnosis of The differential diagnosis of hirsutism & oligomenorrha includes:hirsutism & oligomenorrha includes:
- congenital adrenal hyperplasia- congenital adrenal hyperplasia
- cushing syndrome- cushing syndrome
- hyperthecosis ovarii- hyperthecosis ovarii
- benign & malignant androgen- benign & malignant androgen
secreting tumors or ovaries.secreting tumors or ovaries.

3939
InvestigationsInvestigations::
o History & physical examinationHistory & physical examination
o CD3: LH:FSH, E2, testosterone, CD3: LH:FSH, E2, testosterone, androstendione, SHBG, 17-OHp, DHEAS, androstendione, SHBG, 17-OHp, DHEAS, prolactin, TSH, T3, T4 & fasting insulin level.prolactin, TSH, T3, T4 & fasting insulin level.
o FBS, total cholesterol, LDL & HDL.FBS, total cholesterol, LDL & HDL.
o Pelvic ultrasound scan for the ovarian Pelvic ultrasound scan for the ovarian features of PCOfeatures of PCO
o Specific imaging procedures to exclude Specific imaging procedures to exclude adrenal tumors if presentation is rapid.adrenal tumors if presentation is rapid.

4040
TreatmentTreatment::
The first step is to help the patient The first step is to help the patient understand that this chronic disease understand that this chronic disease process can be controlled by changes process can be controlled by changes in lifestyle.in lifestyle.
Lifestyle modification must be Lifestyle modification must be emphasized to include appropriate emphasized to include appropriate diets & exercise program is essential.diets & exercise program is essential.

4141
Treatment (cont)Treatment (cont)::
Metformin may complement the effects of Metformin may complement the effects of lifestyle modification, it causes marked lifestyle modification, it causes marked improvement in menstrual pattern & may improvement in menstrual pattern & may improve the response to ovulatory agents. improve the response to ovulatory agents.
Clomifene-citrate is the standard Clomifene-citrate is the standard first linefirst line method of medical ovulation induction in method of medical ovulation induction in anovulatory women.anovulatory women.
The The second linesecond line treatment, laparoscopic treatment, laparoscopic ovarian diathermy, gonadotrophin therapy.ovarian diathermy, gonadotrophin therapy.

4242

4343
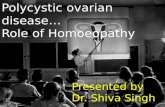
Treatment (cont)Treatment (cont)::
Adrenal suppression by dexamethasone Adrenal suppression by dexamethasone 0.5mg at night facilitate ovulation.0.5mg at night facilitate ovulation.
Anti-androgens: cyproterone acetate & EE Anti-androgens: cyproterone acetate & EE in combination (dianatte)in combination (dianatte)
Spironolactone: alternative anti-Spironolactone: alternative anti-androgen.androgen.
Low dose of oral contraceptives are Low dose of oral contraceptives are effective in treating acne & hirsutism, effective in treating acne & hirsutism, minimum of 2 years & cosmetic measures minimum of 2 years & cosmetic measures are needed to achieve good results. are needed to achieve good results.

4444
Case presentation of PCOSCase presentation of PCOS::
Mrs.: S.J.Mrs.: S.J. Age: 35 yearsAge: 35 years Nationality: IndianNationality: Indian Status: married for 8 yearsStatus: married for 8 years Obstetrical Hx: Nulliparous + ? Complete Obstetrical Hx: Nulliparous + ? Complete
abortion 6 years ago.abortion 6 years ago. Presented: irregular period & failure to Presented: irregular period & failure to
conceive.conceive. Weight: 50kg, height: 150cm → Weight: 50kg, height: 150cm →
BMI:22.2kg/mBMI:22.2kg/m Hirsute lady.Hirsute lady.

4545
Investigation:Investigation:• LH:17 IU/LLH:17 IU/L• FSH:5 IU/LFSH:5 IU/L• Testosterone: ↑3.05 (0.2-2.9) nmol/LTestosterone: ↑3.05 (0.2-2.9) nmol/L• Free testosterone: ↑0.04 (0.02-0.3) nmol/LFree testosterone: ↑0.04 (0.02-0.3) nmol/L• Bioavailable testosterone: ↑1.3 (0.1-1.0) nmol/LBioavailable testosterone: ↑1.3 (0.1-1.0) nmol/L• SHBG:40.2 (20-100) nmol/LSHBG:40.2 (20-100) nmol/L• Free androgen index = total testosterone x 100 / SHBGFree androgen index = total testosterone x 100 / SHBG = 3.05 x 100 /40.2= 3.05 x 100 /40.2 = ↑7.5 (>4.5)= ↑7.5 (>4.5)• Pelvic scan showed cystic ovaries.Pelvic scan showed cystic ovaries.
ManagementManagement::

4646
Management (cont)Management (cont)::
Treatment:Treatment:
• Ovulation was induced by clomiphine-Ovulation was induced by clomiphine-citrate 100mg daily.citrate 100mg daily.
• She was put on 0.5mg She was put on 0.5mg dexamethasone daily at night for 2 dexamethasone daily at night for 2 monthsmonths
• Pregnyl 10000 IU to target ovulation Pregnyl 10000 IU to target ovulation when mature follicle ≈ 18mm.when mature follicle ≈ 18mm.

4747
Management (cont)Management (cont)::
• Pregnancy achieved after 3 cycles of Pregnancy achieved after 3 cycles of Rx & it was twin pregnancy.Rx & it was twin pregnancy.
• Gestational diabetes diagnosed at 5Gestational diabetes diagnosed at 5thth month of pregnancy & she was month of pregnancy & she was managed by diet control.managed by diet control.
• Delivered by LSCS at 35 weeks Delivered by LSCS at 35 weeks gestation & delivered 2 baby girls gestation & delivered 2 baby girls 2.2kg & 2.3kg in good condition.2.2kg & 2.3kg in good condition.

4848
Thank YouThank You