Polio eradication program
46
Dr. Anita Lamichhane
Transcript of Polio eradication program

Dr. Anita Lamichhane

Acute Flaccid Paralysis
Rapid onset of weakness, including weakness of
the muscles of respiration and swallowing,
progressing to maximum severity within several
days to weeks

Acute Flaccid Paralysis
WHO:
Poliomyelitis
Gullain Barrie syndrome
Transverse myelitis
Traumatic Neuritis

Components of AFP Surveillance
The AFP surveillance network and case
notification
Case & laboratory investigation
Outbreak response & active case search in the
community
60 day follow up, cross notification & tracking of
cases

Data management & case classification
Virologic classification scheme
Surveillance performance indications

Case and laboratory investigation
Immediate investigation into the case within 48 hrs
of notification
Stool specimen collection & transportation
2 stool specimen collected as soon as possible
after the onset of paralysis (ideally within 14 days
of onset of paralysis & at least 24 hrs apart)
Each specimen should be 8 gms- each about the
size of the adult thumb

Stool container

Collected in a clean, dry, screwed capped container
No preservative or transport media should be used
The specimens collected, labeled ,transported in the
cold chain-on frozen ice packs/ ice, in a stool
specimen carrier or a vaccine carrier
In Pakistan, the specimen is sent to NIHL( National
Institute 0f Health Laboratories ) at Islamabad

Poliomyelitis
Two Greek words: polios (gray) & myelios (spinal
cord..anterior horn cells )
In 1908, the polio virus was discovered by Karl
Landsteiner

An enterovirus
3 serotypes-P1,P2,P3
P1 - causes outbreaks—is the most likely virus to
cause paralysis.
P2 - the easiest to eradicate followed by P3
Human are the only hosts without which the virus
cannot survive

The Virus is excreted in the stools for three to six
weeks.
It is more stable than most viruses ,can stay alive
for several weeks in contaminated food or water.
It is one of the most contagious viruses.
If one family member is infected, nearly all the rest
of the family becomes infected.

multiplies in the cells of the mucous membranes in the pharynx and intestines
Invades local lymphoid tissue
Hematological spread
• virus becomes neurotropic • produces destruction of the motor neurons in the anterior horn and brainstem
Portal of entry is the mouth


Cold chain- Maintenance of temperature from
vaccines synthesis to delivery to child.
Reverse cold chain- Maintenance of cold chain
from stool collection to delivery to the laboratories

Yearly report
Total casesYear-to-date
2010Year-to-date
2009 Total in 2009
Globally 39 110 1606
in endemic countries 32 80 1256
in non-endemic countries: 7 30 350

Yearly report …of Pakistan
In Pakistan, one new WPV3 case was reported on
the 17th February 2010, from Quetta, Baluchistan.
Bivalent OPV was used for the first time in
Pakistan in NIDs held from 15-17 Feb 2010
The next round will be held from 15-17 March
2010 in targeted high and medium risk districts,
using bOPV

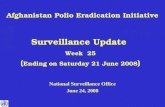
Number of confirmed cases of poliomyelitis in Pakistan, 1997–2008

Number of districts with confirmed poliomyelitis cases in Pakistan, 1997–2008

Pakistan has recorded 76 cases in 2009 to date:
52 type 1
23 type 3
one type 1/3 mixture.

SNIDs in Afghanistan
the Provincial Government of Nangarhar, UN
agencies jointly launched sub-national
immunization days (SNID) in Jalalabad on
Sunday, 14 February 2010.

Disease Surveillance
The ongoing systematic collection & analysis of
data & the provision of information which leads to
action being taken to prevent & control a disease,
usually one of an infectious nature

Herd immunity
Immunity of a sufficient number of individuals in a
population such that infection of one individual will
not result in an epidemic.

Wild polioviruses
Isolates known or believed to have circulated
persistently in the community & reference strains
derived from these isolates.
May be present in a variety of clinical materials
faeces & throat specimens
less commonly in blood
rarely in CSF in non-paralytic & paralytic infections.
.

In fatal infections, wild poliovirus may be present in
faeces
intestinal contents
lymph nodes
brain tissue
spinal cord tissue

Vaccination
1955 - Mr. Salk discovered IPV
1957 - Mr. Sabin discovered OPV
EPI- globally launched in 1974
In Pakistan in 1978 training was started and
became apparent in 1979

Polio Eradication
In 1988 , World Health Assembly, in its resolution
41.28 – set goals of A global polio eradication
program
OPV was recommended.
In Pakistan started in 1993-94
Led by the World Health Organization, UNICEF,
and The Rotary Foundation

Global Eradication of polio program was established in
1989.
Today only 4 countries are endemic to polio
Pakistan,
Nigeria,
India,
Afghanistan

What is Eradication ???
The World Health Organization (WHO) defines
polio eradication essentially as ‘zero incidence of
wild poliovirus transmission anywhere in the
world’.

Polio eradication requires
Finding and controlling wild
poliovirus in human populations
+
Finding and controlling wild
poliovirus in laboratories

Why was it launched ???
Humans are thought to be poliovirus's only host
Virus survival in the environment is limited.
Immunization with vaccines interrupts virus
transmission

Objectives of the Global polio Eradication initiative
To interrupt transmission of the wild poliovirus as
soon as possible
To achieve certification of global polio eradication
To contribute to health system ,development &
strengthening routine immunization & surveillance
for communicable disease in a synergistic way

Strategies of achieving the goal
High routine infant immunization
Supplementary doses of OPV to all children under 5 yrs of
age during SIAS( Supplementary immunization activities)
Active AFP Surveillance for wild poliovirus through
reporting & lab testing of all AFP cases among children
under 15 yrs of age
Targeted “Mop-up" campaigns once wild poliovirus
transmission is limited to a specific focal area.

High routine infant immunization
All countries aim to immunize at least 90% of
infants with four OPV doses
These doses are part of the basic (EPI)
High routine immunization coverage decreases the
incidence of polio & sets the stage for eradication

National Immunization Days (NIDs)
It is the 2nd part of the four-pronged strategy and is also
known as mass immunization campaign.
Important activity for interrupting wild poliovirus
circulation in endemic countries
A supplementary immunization
Intended to complement - not replace - routine
immunization.

The aim of mass campaigns is to interrupt
circulation of poliovirus by immunizing every child
under 5 years of age with two doses of OPV,
regardless of previous immunization status.
Three to five years of NIDs are usually required to
eradicate polio
NIDs are needed for at least 3 consecutive years
to interrupt transmission

NIDs are normally conducted during the cool, dry
season
( immunological response to OPV is improved and
the potential damage to heat-sensitive OPV is
reduced.)
SNIDs) target children for polio vaccination in
specific high-risk regions of countries rather than
the entire country.

Surveillance of new cases of polio
Countries to ensure that all cases of poliomyelitis
are detected
The goal of AFP surveillance is to report and
investigate “any case of acute flaccid (floppy)
paralysis

surveillance systems should be capable of
detecting at least one case of AFP per 100 000
population < 15 years;
collecting adequate stool specimens from at least
80% of AFP cases
testing all specimens at a WHO-accredited
laboratory.

Mop-up Activities
AFP surveillance data are used to identify the final
chains of wild poliovirus transmission in each
geographical area
In these areas, two doses of OPV are
administered to all children < 5 years, regardless
of their prior immunization status, by immunization
teams that go house-to-house.

Improve coverage & ensure that the most difficult-to-
reach children are immunized, thereby interrupting the
last chains of wild poliovirus transmission
In addition to delivering supplemental OPV doses,
mop-up activities often include an active search for AFP
cases

Summary of Proposed Milestones
Milestones for future Target year
1. Establish comprehensive policy for future management.
2003
2. Eliminate wild poliovirus transmission. 2003
3. Certification of ‘eradication’ of wild viruses. 2006
4. Introduction of IPV in routine immunization. 2006
5. Complete withdrawal of OPV. 2009
6. Certification of ‘true eradication’ of polioviruses.
2012
7. Discontinue polio immunization. 2015

Polio Eradication in Pakistan
In Jan 2010, meeting covered the tribal leaders
and religious scholars
In South Waziristan, Mufti Maulana Abdul
Qayuum issued a fatwa supporting polio efforts, 15
mosques were made after the ceremony
Women also played an important role in increasing
the coverage

Special teams of women were mobilized & trained
to go house-to-house and address the recent rise
in refusal rates
The delivery teams equipped with appropriate
messages, were able to cover 61% of all the
refusal families in Larana.

Recent advances of polio virus
Researches use crippled Polio Virus to attack
Brain Cancer
Polio virus has a natural affinity to invade the
brain, by binding to the CD155 receptor on the
surface of the motor neurons
Brain tumors overproduce the CD155 receptors
which makes the cell in the tumors more
susceptible to poliovirus infection

The genetically engineered altered poliovirus
when introduced in the body
Enters the normal motor neurons (it shares the
same CD155 receptors as brain tumour cells )but
cannot grow in normal neurons
Kills the brain tumor cells

no cure for polio
it can be prevented