Policy Evaluation of Healthy Hunger Free Kids Act of 2010_Brittney Gajewski_March 2015
23
Running Head: Health Care Policy Evaluation 1 Health Care Policy Evaluation Brittney Gajewski Collie Richard Monica Sosa Parthenia Williams Robbin Winters Capella University MHA-5030 Instructor: Dr. Neil Mathur
-
Upload
brittney-gajewski -
Category
Documents
-
view
215 -
download
0
Transcript of Policy Evaluation of Healthy Hunger Free Kids Act of 2010_Brittney Gajewski_March 2015

Running Head: Health Care Policy Evaluation 1
Health Care Policy Evaluation
Brittney Gajewski
Collie Richard
Monica Sosa
Parthenia Williams
Robbin Winters
Capella University
MHA-5030
Instructor: Dr. Neil Mathur

Health Care Policy Evaluation 2
Health Care Policy Evaluation
Childhood Obesity has been a growing global trend. Initiatives such as The Healthy,
Hunger Free Kids Act of 2010 has been included to address this issue. As with many health care
policies, strategic planning and evaluation has demonstrated a need for possible policy
improvements. This paper will evaluate the driving forces behind the policy, evaluate the policy
from abroad, propose improvements, and synthesize financial components of the policy. The
analysis will also include the short-term and long-term effects of the policy and then analyze
operational recommendations.
Driving Forces behind a Domestic Health Care Policy in Need of Improvement and Provide
Insightful Analysis. (Brittney)
The driving forces behind this domestic health care policy analysis involve the concern of
children’s physical and nutritional health. With over 12.5 million youths already affected by
childhood obesity, concerns about the chronic condition continue to rise (Foltz et al., 2012). To
address obesity with children on an interpersonal level, Foltz et al., (2012) explained that school-
based interventions would allow focus to change the environment and reacted behaviors using a
socioecological approach. With greater means of physical activity and recovered nutrition,
intervention strategies for obesity can be promoted through health behaviors within the child’s
environment (Foltz et al., 2012). To effectively analyze the domains of a health policy one needs
to understand the likelihood an enhanced approach will be adopted through a policy (Brownson,
Chriqui, & Stamatakis, 2009).
The Healthy, Hunger Free Kids Act ( HHFKA) of 2010 has provided the opportunity to
address childhood obesity and was the first time that the national school lunch program received

Health Care Policy Evaluation 3
increased funding in over thirty years (Mortazavi, 2011). This increase in funding may be an
incentive for schools to adopt the necessary standards appointed by the Secretary of Agriculture,
however they lack the necessary funding that would be allow for healthier fruits and vegetables
to be available in schools (Mortazavi, 2011). With funding increased by only six cents, schools
are still unable to budget for the dietary guidelines within the HHFKA. Even if funding
increased further, many schools would not be able to receive increased funding because schools
would still be unable to meet the necessary dietary guidelines within their budgets because of the
current market price for healthier fruits and vegetables (Mortazavi, 2011).
Finally, the increase made in federal funds, already surpasses proposed regulations of the
national school lunch program (Mortazavi, 2011). Fiscal challenges continue to combat a
significant change in addressing childhood obesity. The USDA estimates production costs to
meet the regulations within the HHFKA to be set at seven cents per meal (Mortazavi, 2011).
These estimates provide impractical budget options for schools to meet HHFKA nutritional
regulations (Mortazavi, 2011).
The current HHFKA aimed to limit junk food and eliminate foods with added sugars on
school campuses, the discretional guidelines are exerted to their own interpretation by the USDA
(Mortazavi, 2011). With guidelines left to be interpreted, competitive foods have created loop
holes that allow for high sugar based junk food to be sold during ‘school sponsored fundraisers’
(Mortazavi, 2011). These loopholes allow for a large amount of foods with little to no nutritional
value to remain unfettered and unsupervised (Mortazavi, 2011). The USDA’s discretional
guidelines innate vagueness and litigates loopholes within the competitive food market and
inherently neglects to define ‘frequency’ (Mortazavi, 2011).
Health Care Policy Evaluation 4
In 2011, Motazavi explained that only 7%-15% of schools currently comply with the
national school lunch program nutritional requirements. Perhaps the most complex challenge
that faces the HHFKA is its enforcement and compliance. The USDA does not have a current
infrastructure available to cite school district nutritional programs that lacked responsibility
ensuring children’s nutritional needs (Motazavi, 2011). This challenge remains, as the USDA is
unable to inherently neglect the basic needs of children (Motazavi, 2011).
Evaluate a Health Care Policy from Abroad for Criteria to Integrate into Domestic Health
Care Reform (Collie)
Health care policy abroad that effect young children as in the United States is obesity.
Obesity has become a major problem in Pakistan and policies are being implemented to control
this problem. Warraich et al. stated “Obesity is becoming an increasingly prevalent problem in
Pakistan, as it has in other developing countries, with under nutrition remaining a problem
simultaneously” (Warraich et al., 2009). More and more countries are facing the rise in youth
becoming obesity. Pakistan compared to the Unites States has tried to implemented exercise into
the daily active of their youth. On behalf of the United States a policy was put in action to assist
and implement youth obesity to regain youth health. As stated by Garcia & Fenwick “The major
goals are, first, to help students learn the skills and knowledge to move more, eat well, stay
healthy, and do their best in school and in life; second, to alleviate unfair disparities based on
race, ethnicity, and income; and third, to engage, educate, and empower people to improve
public education and health” (Garcia & Fenwick et al, 2009). Once these goals are met students
should be able to incorporate these lifestyle changes into their daily routine. Pakistan also came
up with a policy to incorporate exercise and education to the students and community. Warraich
Health Care Policy Evaluation 5
stated “Integrated approaches that promote intake of a balanced diet and increased physical
activity to both underweight and overweight children would be more cost-effective than separate
strategies for underweight and overweight children” (Warraich et al., 2009). Underweight youth
also need to apart of this plan, so that in the future they won’t face the challenge of being
obesity.
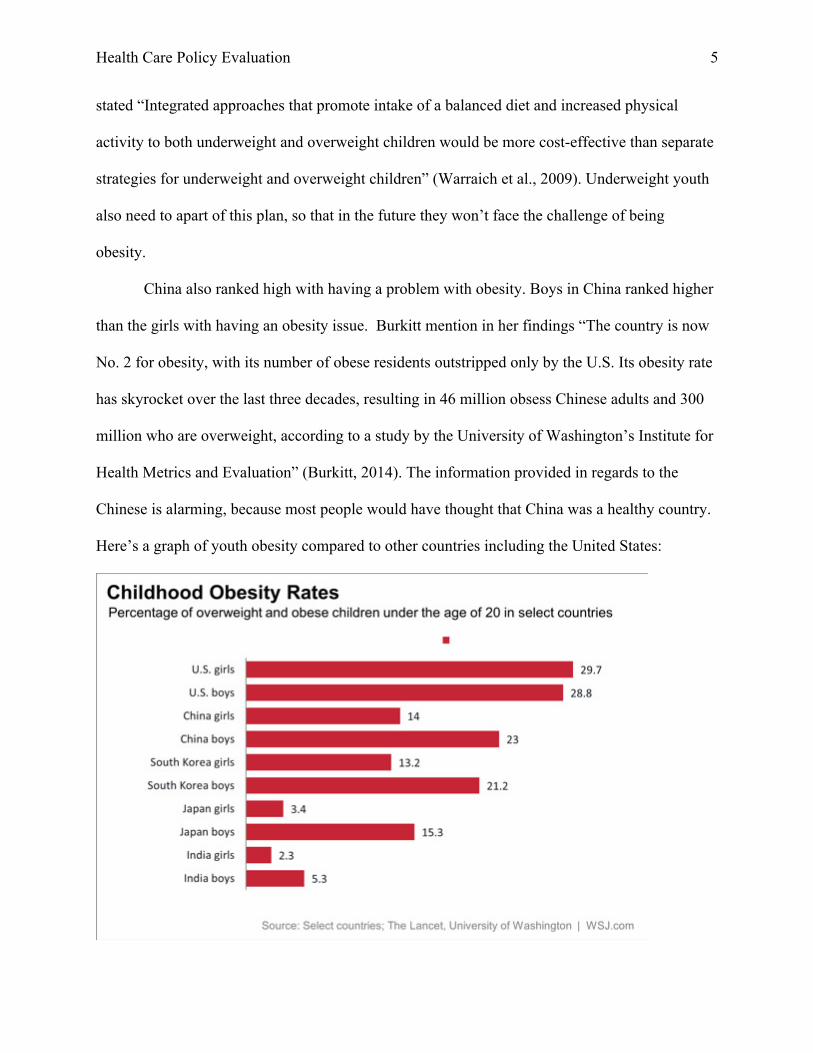
China also ranked high with having a problem with obesity. Boys in China ranked higher
than the girls with having an obesity issue. Burkitt mention in her findings “The country is now
No. 2 for obesity, with its number of obese residents outstripped only by the U.S. Its obesity rate
has skyrocket over the last three decades, resulting in 46 million obsess Chinese adults and 300
million who are overweight, according to a study by the University of Washington’s Institute for
Health Metrics and Evaluation” (Burkitt, 2014). The information provided in regards to the
Chinese is alarming, because most people would have thought that China was a healthy country.
Here’s a graph of youth obesity compared to other countries including the United States:

Health Care Policy Evaluation 6
A stand has to be taken to get obesity under control in the United States and other countries. Our
youth is the future and we as lawmakers and citizens has to make an impact to education and
provide the necessary policies. Feeg stated “To implement this recommendation, the committee
believes the federal government should strengthen and support a variety of surveillance
activities, health education programs, and research activities, including an independent
assessment of federal nutrition assistance programs and agricultural policies (Feeg, 2004).
Proposes and Applies Strategic and Plausible Improvements to the Community Health and
National Health Care Policy (Brittney)
Due to insufficient funding schools are unable to meet the nutritional standards appointed
by the Secretary of Agriculture and are therefore unable to budget greater healthier fruits and
vegetables. Improvements can be made through the reallocation of subsidies through congress to
redistribute the production of nutritional and fresh foods. Shift in subsidies would lower the cost
production of nutritional foods. A change to the Farm Bill would need to involve congress to
allot subsidies that could be used to restore the national food stamp program, who’s funding was
recently cut for the HHFKA (Mortazavi, 2011).
These congressional changes would create an overarching obstacle for all school districts
to systematically receive fresh foods for children (Motazavi, 2011). To overcome this challenge
schools will need to work on a community level to implement programs and create partnerships
will local farmers to further educate children on the agricultural aspects supplementing
nutritional foods. Further, budget bound schools could create their own vegetable gardens to be
used as educational and nutritional resources. This would successfully employ modified food
practices, classroom-based nutrition education, and additional integrational opportunities for

Health Care Policy Evaluation 7
physical education, and activities involving parents becoming engaged through school
newsletters (Patel, & Hampton, 2011).
The complete elimination of competitive foods within schools is not an attainable
solution. Because of this, there is a need for the Secretary of Agriculture to specifically define
the rules of ‘infrequent exceptions’ for high sugar based junk foods that are sold on school
campuses. With a strongly defined statute, Congress can better address the current competitive
food limitations within schools and on school campuses (Motazavi, 2011). Another intervention
that could effectively address the amount of competitive foods in schools includes increasing
access to drinking water. Coupled with educational promotions for drinking water, this can
effectively alter drinking preferences among students (Patel, & Hampton, 2011).
To address the lack of nutritional infrastructure being practiced by the USDA, congress
would need to provide a ‘floor’ rather than a ‘ceiling’ based regulation to term nutritional
regulations. A plausible solution involves nutritional standard liaisons on the state, county and
school district level. This multisectoral relationship would allow for local monetization of
school lunch programs and provide further options for compliance and enforcement of the
HHFKA dietary regulations.
To allow for a more efficient flow of federal budgeting sectoral changes need to be made
to determine the federal nutritional and dietary guidelines. Currently the department of
agriculture has an ‘inherent loyalty’ to its own agriculture sector and should not be making
determinations pertaining to federal dietary and nutritional guidelines (Motazavi, 2011). Rather,
the department for human services, science, and the coalition of health should be the principle
voices influencing health nutrition dietary guidelines.
Health Care Policy Evaluation 8
Without stringent action to reallocate, redistribute, and better define the federal
regulations seen within the HHFKA, schools are left with impractical options to address
childhood obesity. Modifying the preparation structure of food ought to be viewed as a program
that can create jobs within the food service industry through the improvement of knowledge and
level of skilled labor (Motazavi, 2011). The current fiscal infrastructure for HHFKA
supplements’ training for food programs, but it is training is aimed on management instead of
training for food preparation. This change of focus to food preparation could benefit further
from schools that have their own gardens to grow fresh foods. These programs could be
combined to involve the education of proper food preparation. When food preparation is
involved within schools, children adopt better nutritional habits that are carried with them and
practiced within their homes (Motazavi, 2011).
Operational and Financial Components to the Policy (Monica)
The Healthy, Hunger-Free Kids Act of 2010 gave guidelines regulating “competitive”
foods with low nutritional value in schools (Turner & Chaloupka, 2012). One of the first things
to go was vending machines in schools that offered sugary drinks and candy. Although, the
availability of “competitive” food in schools through vending machines has decreased most
schools still face a major challenge in funding healthier food in the lunch line.
Recommendations in re-allocating subsidies into training and managing new food
requirements can benefit the nation in the long run. The following is a cost-benefit analysis of
implementing the new policies:

Health Care Policy Evaluation 9
Studies have shown that an increase in the consumption of fruits and vegetables can
contribute to a reduction in major chronic diseases associated with obesity (Terry-McElrath,
O’Malley, & Johnston, 2014). Obesity has been linked to diseases such as diabetes and heart
disease. These diseases cost an estimated $150 billion to $200 billion annually in health care
expenditures (Kass et al, 2014). As demonstrated on the Cost-Analysis table, the net benefit of
implementing changes will outweigh the costs associated with managing chronic health
conditions. Having healthy food available can have a direct influence on behaviors associated
with the types of foods chosen by individuals, consequently decreasing the costs associated in
treating obesity ailments.

Health Care Policy Evaluation 10
Implementation of new policies should also consider ethical implications that might need
to be addressed. Government regulations that dictate what children can and can’t eat at school
will have some individuals thinking that the government is overreaching its power over its
citizens (Kass, Hecht, Paul & Birnback, 2014). In order to address this issue, operational
planning that presents evidence based data to the public will play an important role in the
acceptance of the new policy (Kass et al, 2014). Perceived burdens to the public should also be
kept at a minimum by using opt-out strategies and financial disclosures (Kass et al, 2014). By
allowing public transparency into the cost-benefit analysis of implementing the new policies
individuals can make an educated decision as to support or oppose the policy.
Evaluate the short-term and long-term effects of proposed policy reforms in the health care system Healthy, Hunger-Free Kids Act of 2010 (Parthenia)
Improving child nutrition is the focal point of the Healthy, Hunger-Free Kids Act of
2010. The legislation authorizes funding and sets policy for USDA's core child nutrition
programs: the National School Lunch Program, the School Breakfast Program, the Special
Supplemental Nutrition Program for Women, Infants and Children (WIC), the Summer
Food Service Program, and the Child and Adult Care Food Program (United States Department
of Agriculture, 2014). The Healthy, Hunger-Free Kids Act of 2010 allows USDA, for the first
time in over 30 years, the opportunity to make real reforms to the school lunch and breakfast
programs by improving the critical nutrition and hunger safety net for millions of children.
(United States Department of Agriculture, 2014).
This proposed rule would require all local educational agencies participating in the
National School Lunch Program and/or the School Breakfast Program to meet expanded local
schools wellness policy requirements consistent with the new requirements set forth in section

Health Care Policy Evaluation 11
204 of the Healthy, Hunger-Free Kids Act of 2010 (United States Department of Agriculture,
2010).
This proposed rule would establish the framework for the content of the local school
wellness policies, ensure stakeholder participation in the development of such policies, and
requires periodic assessment of compliance and reporting on the progress toward achieving the
goals of the local school wellness policy (United States Department of Agriculture, 2010). It
would also require local educational agencies, as part of the local school wellness policy, to
implement policies for the marketing of foods and beverages on the school campus during the
school day consistent with nutrition standards for Smart Snacks (United States Department of
Agriculture, 2010). The provisions of this proposed rulemaking would ensure local educational
agencies establish and implement local school wellness policies that meet minimum standards
designed to support a school environment that promotes sound nutrition and student health,
reduces childhood obesity, and provides transparency to the public on school wellness policy
content and implementation. (United States Department of Agriculture, 2010).
Policy makers, public health officials, and parents are concerned about the implications
of the increasing rate of childhood obesity in the U.S. such as behavioral, social, and
environmental risk factors contribute to childhood obesity. Research demonstrates that if the
trend is not reversed, childhood obesity will suffer from a number of health complications and
society will deal with rising healthcare costs (Letsmove.gov, 2010). Communities that have
already implemented the comprehensive approach promoted by the ecological framework have
seen a reduction in childhood obesity rates. (Crawford et al, 2013).

Health Care Policy Evaluation 12
Social factors influence children’s risk of becoming obese. Social factors include race,
ethnicity, gender, class, and relationships with parents, siblings, and peers. Research shows that
family structure influences the risk for obesity. (Crawford et al, 2013).
Class and race also play a role in childhood obesity. Health disparities exist among
African Americans, Hispanics, American Indians, and other minority groups (Caprio et al, 2008).
Children in these racial minority groups experience higher rates of obesity than white children.
Researchers found that after adjusting for socioeconomic status and behavioral factors, African
American children and Hispanic children are 27% more likely to become obese than white
children. Children living in poverty are 69% more likely to be obese. (Caprio et al, 2008).
Schools play a critical role in promoting student health, preventing childhood obesity,
and combating problems associated with poor nutrition and physical inactivity. To formalize and
encourage this role, section 204 of the Child Nutrition and WIC Reauthorization Act of 2004
(Pub. L. 108-265), required each local educational agency (LEA) participating in the National
School Lunch Program (NSLP) and/or the School Breakfast Program (SBP) to establish a local
additional stakeholders into the development, implementation, and review of local school
wellness policies; and requires public updates on the content and implementation of the wellness
policies. (United Stated Department of Agriculture, 2014).
According to Capretta & O’Grady (2012), if policy fails to reduce childhood obesity,
American society will face serious consequences over the next 20 years. In the short term, these
consequences include increased child obesity diagnosis rates, increased risk for obesity-related
illness, and diminished academic performance. Children will also suffer increased risk for at
least one additional illness such as cardiovascular disease, elevated total cholesterol,
Health Care Policy Evaluation 13
triglycerides, insulin, or blood pressure. Obese children often perform poorly academically due
to compromised physical and cognitive functioning (Capretta & O’Grady, 2012).
While the short-term effects of obesity are seen in the school systems, long term
implications exist because obese children are more likely to become obese adults. Adult obesity
increases costs for health care systems and creates an unhealthy labor force. (Crawford et al,
2013). Public insurance programs such as Medicare and Medicaid will be expected to cover
most of these costs. The economic implications for obese adults in the workforce are increased
absenteeism and loss of productivity (Crawford et al, 2013)
People argue that the component for childhood obesity is parents often do not have the
information to make healthy food choices for their children and children’s choices are often
dependent on those around them (Crawford et al, 2013). Parents argue that the cost to shopping
for health foods are more expensive and it is easier to get unhealthy foods that healthy foods.
Society has made eating unhealthy convenient because we promote unhealthy behaviors. This
includes an abundance of fast food restaurants in the U.S. Therefore policy interventions should
address this market failure by affecting the factors that contribute to childhood obesity (Crawford
et al, 2013).
In public health, especially with obesity, the public, private, and non-profit sectors are
essential for scalable and sustainable interventions (Crawford et al, 2013). The public sector
includes major policy factors such as local, state, and federal levels of government as well as
public schools and public universities. Private sector actors include the business community and
industries (Crawford et al, 2013).

Health Care Policy Evaluation 14
The non-profit sector has the potential to mobilize and conduct large-scale programs. For
successful policy interventions, cooperation between the public, private, and non-profit sectors is
essential for political feasibility. (Crawford et al, 2013). The public sector can set the agenda and
provide funding. The non-profit sector is able to plan and develop large-scale programs while
private sector buy-in can promote long-term sustainable interventions in which this policy will
and can implement (Crawford et al, 2013).
Analyze Operational Recommendations and Strategic Implications of the Proposed
Health Care System (Robbin)
Childhood obesity has become the national health crisis epidemic, globally. One in every
three children (31.7) is overweight or obese for children ages 2 to 19 years of age. This issue has
become very forcibly especially when it can become life threatening outcome for most obese
individuals. In the United States, Obesity has caused 112,000 deaths and it poses a substantial
cost. There are many recommendations made in regards to this policy, one recommendation is
developing a school based program to address complex issues such as childhood obesity, this
requires the best practice guideline and evidence based intervention. There is very little evidence
or literature that supports school based intervention. Therefore, it becomes necessary for the
system to look at the national guidelines and recommendation for intervention based
programming.
Section 9A of the NSLA, 42u.s.c. 1758B, added by the HHFKA, requires LEA’s to
establish and local school wellness polices for all schools under the jurisdictions (United States
Department of Human Services, 2011). All nutrition guideline must be consistent because the
school plays a very important role in advocating student’s health, preventing child obesity, and
combating problems with kid’s poor nutrition habits. In 2004, the legislation placed the
Health Care Policy Evaluation 15
responsibility of developing a local school wellness policy at the local level; therefore all school
under the jurisdiction of the LEA will be able to address the obesity issues (United States
Department of Human Services, 2011). The United States Department of Health and Humans
Services have designed, Healthy People 2020 which is a 10 year health specification that will
contribute to the guidelines for program development and evaluation. What these benchmarks
willful do is encourage collaboration across sectors, guide others toward making informed health
decisions and measure the impact of prevention activities (United States Department of Health
and Human Services, 2011).
One guideline is to partner with families and community members in the development and
implementation of health eating and physical activity policies, practices, and programs
Encourage communication between schools, families and community members to
promote the adoption of healthy eating and physical activities behaviors among students
(United States Department of Health and Human Services, 2011).
Involve families and community leaders on the school health council (United States
Department of Health and Human Services, 2011).
Develop and implement strategies for motivating families to participate in school-based
programs and activities that promote healthy eating and physical activity (United States
Department of Health and Human Services, 2011).
Access community resources to help provide healthy eating and physical activity
opportunities for students (United States Department of Health and Human Services,
2011).
Demonstrate cultural awareness in healthy eating and physical activity practices
throughout the school (United States Department of Health and Human Services, 2011).

Health Care Policy Evaluation 16
The federal and state provides the largest portion of infrastructure for combating childhood
obesity. The two federal agencies that actually provide the oversight and regulation for school
health and nutrition are a listed: CDC and USDA (Sinott, 2011). The CDC is responsible for
developing strategies to improve the health of the helpless population such as children and
adults. One example of the CDC strategy is CSHP (Coordinated School Health Program) (Sinott,
2011). These are some strategies to improve the effectiveness and efficiency of SNAP. These
strategies are based upon literature review, expert’s recommendations, and prior experiences in
communities and states.
Changing one’s behavior is difficult, and changing a population of American behavior is
even more difficult because you a dealing with the nation as a whole. Research state that the
national data corroborates most children who come to after school programs are already hungry
(Sinott, 2011). Most of them do not have a hot meal awaiting them at home. Therefore, the main
goal of these programs is to expand the number of after school snacks and meals served in after
school programs. In 2010, the Healthy Hunger Free Act developed a federally funded after
school meal reimbursement program in all 50 states (Hungerfreemn.org, 2013). These proposed
strategies are to indicate the future we want for our children and its burden to healthcare.
Strategies are as indicated:
To improve access to health foods-set guideline requires SNAP vendors to carry
healthier options. If we improve our selection of healthier foods, it gives the participant
choices and it improves the food environment (Hungerfreemn.org, 2013).
Incentivizing purchases of healthy foods (fruits and vegetables)-research show this is
a monetary incentives that is more effective strategy in encouraging healthier food

Health Care Policy Evaluation 17
consumption and it improves dietary behavior. Accept the SNAP benefits at the Farmer’s
market and allow online purchases using SNAP benefits (Hungerfreemn.org, 2013).
Restrict options for unhealthy foods.
Public Health approaches to expand SNAP Outreach-the USDA indicates this is the
most important aspect in the nation in regards to improving diets of low income
Americans. One-one or group education sessions to adopting multimedia approaches
which include social marketing campaign to reach the larger numbers, in using advancing
technology such as smart phones to deliver and evaluate nutrition education
(Hungerfreemn.org, 2013).
Health system analysis seeks to understand the determinants of health system performance
and to develop better policies and strategies for reform that improve that performance (Berman
& Bitran, 2011). The health system analysis involves gathering data on health system it is
recommended there is a great need for some development of collaborative learning resources by
World Bank and its partners (Berman & Bitran, 2011). Very few countries have taken it upon
themselves to cost out their recommendations because of the lack of information on
implementation costs limits the reader to judge the feasibility of what is recommended.

Health Care Policy Evaluation 18
Table 1. From Problems to Causes to Solution
The main problems Problems 1: Low health status and unequal access to health services, clean water, sanitation, and education Problems 2: Low level of public spending on health, and available resources are not allocated efficiently and equitably Problem 3: Poor incentive for managers and providers in public provision health Problems 4: Delivery of health care is fragmented Problems 5: Potential of private sectors is not fully realized Cause 1: not all who are getting treated, particularly poor? Large segment of population lack adequate health insurance in some form of financial protection
Main recommendation: offering compulsory universal social health insurance (health fund) with optional supplemental private insurance
Cause 2: Primary health care system is underfunded and ineffective. Many health centers are understaffed, and huge gap in the distribution of health personnel
Staffing rural health facilities Strengthening delivery of primary care services Adopting the concept and practice of family practice of family medicine
Cause 3: general hospital are inefficiently run
Reorganizing public hospital and provide greater autonomy
Cause 4: There is little to no coordination between ministry of health and ministry of labor, who control most financing and provision of healthcare.
Consolidating and redefining institutional responsibilities role in policy formulation and regulatory oversight and MOL
Epidemiological surveillance and data collection Quality assurance and control
Cause 5: There is an inequitable distribution of public expenditures on health, and little is spent on preventive care/maternal and child health
Developing a package of essential services (maternal and child oriented) and target public spending
Target the delivery to the poor and underserved regions World Bank Data, 2003

Health Care Policy Evaluation 19
Conclusion
Childhood obesity is a problem that can be addressed through multi-disciplinary
collaboration from the community and other governmental agencies. Research and empirical
evidence has demonstrated that unhealthy behaviors associated with the types of food chosen by
school aged children has resulted in chronic conditions that has proven more costly to treat.
Initiatives that involve education, community outreach programs, changes in advertising, and
incentives has shown to change behaviors that improve the health of children and the
community.

Health Care Policy Evaluation 20
References
Berman, P. & Bitran, R. (2011). Health System Analysis for Better Health System
Strengthening. Retrieved on March 8, 2015, from http://worldbank.org.
Brownson, R. C., Chriqui, J. F., & Stamatakis, K. A. (2009). Understanding evidence- based
public health policy. American Journal of Public Health, 99(9), 1576-1583.
Burkitt, Laurie. (2014). As Obesity Rises, Chinese Kids Are Almost as Fat as Americans.
Retrieved from: http://blogs.wsj.com/chinarealtime/2014/05/29/as-obesity-rises-chinese-
kids-are-almost-as-fat-as-americans/.
Capretta, James C. MA & O’Grady, Michael J. PhD. 2012, Assessing the Economics of Obesity
and Obesity Interventions. Retrieved from:
http://obesitycampaign.org/documents/StudyAssessingtheEconomicsofObesityandObesit
yIntervention.pdf
Crawford, Loren, Howard, Jenna, Karmali, Ruchir, Pjecha, Matthew, & Santoro, Hannah (2013).
Childhood Obesity and Possible Policy Interventions. Georgia Tech University.
Retrieved from: http://policychallengeusa.org/uploads/3/1/5/9/3159875/2013_challenge_-
_memo_-_georgia_tech.pdf
Caprio, S., Daniels, S. R., Drewnowski, A., Kaufman, F. R., Palinkas, L. A., Rosenbloom, A., L.,
& Schwimmer, J. B. (2008). Influence of Race, Ethnicity, and Culture on Childhood
Obesity: Implications for Prevention and Treatment. A consensus statement of Shaping
America’s Health and the Obesity Society. Diabetes Care. 31(11), 2211-2221. Doi:
Health Care Policy Evaluation 21
10.2337/dc08-9024. Retrieved from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2571048/
Feeg, V.D. (2004). Combating Childhood Obesity: A Collective Effort. Pediatric Nursing. pp.
361-362.
Foltz, J. L., May, A. L., Belay, B., Nihiser, A. J., Dooyema, C. A., & Blanck, H. M. (2012).
Population-level intervention strategies and examples for obesity prevention in
children. Annual Review of Nutrition, 32, 391-415.
Garcia, R., & Fenwick, C. (2009). Social Science, Equal Justice, and Public Health Policy:
Lessons from Los Angeles. Journal of Public Health Policy. Pp. S26-S32.
Doi:10.1057/jphp.2008.58.
Hungerfreemn.org (2013). Hunger-Free Minnesota 2013 in Review. Retrieved on March 9,
2015, fromhttp://www.hungerfreemn.org/.../Hunger-Free-Minnestoa-2013-Year-in-
Review.pdf.
Kass, N., Hecht, K., Paul, A., & Birnbach, K. (2014). Ethics and obesity prevention: Ethical
considerations in 3 approaches to reducing consumption of sugar-sweetened beverages.
American Journal of Public Health, 104(5), 787-795. Retrieved from
http://search.proquest.com.library.capella.edu/docview/1524713423?accountid=2796.
Letsmove.gov. (2010). White House Task Force on Childhood Obesity Report to the President
Solving the Problem of Childhood Obesity within a Generation (2010). Retrieved
from:<http:www.letsmove.govsitesletsmove.govfilesTaskForce_on_Childhood_Obesity_
May2010_FullReport.pdf>.

Health Care Policy Evaluation 22
Mortazavi, M. D. (2011). Are food subsidies making our kids fat? Tensions between the
Healthy hunger-free kids act and the farm bill. Washington and Lee Law Review, 68(4),
1698-1735.
Patel, A. I., & Hampton, K. E. (2011). Encouraging consumption of water in school and
Child care settings: access, challenges, and strategies for improvement.
Government, Politics, and Law, 101 (8), 1370-1379.
Policy Consideration for Improving the Supplemental Nutrition Assistance Program: Making A
Case for Increasing the Burden of Obesity (2011). School of Nutrition & Health
Promotion. Retrieved on March 9, 2015, from
http://www.azdhs.gov/phs/nupao/Documents/SNAP_White_Paper_12_14_11.pdf
Proposed Rule on Local School Wellness Policy-Food (2014). Food and Nutrition Service.
79(38), p10693-10706.
Sinnott, C.H. (2011). The Impact of Childhood Obesity, Poor Nutrition and Inactivity on Public
School System. Lerner Center for Public Health Promotion. Retrieved on March 8, 2015,
from http://www.lernercenter.syr.edu/.../Impactof %20of%20child.
Terry-McElrath, Y. M., O'Malley, P. M., & Johnston, L. D. (2014). Accessibility over
availability: associations between the school food environment and student fruit and
green vegetable consumption. Childhood Obesity, 10(3), 241-250.
http://online.liebertpub.com.library.capella.edu/doi/pdfplus/10.1089/chi.2014.0011.

Health Care Policy Evaluation 23
Turner, L.R., & Chaloupka, F.J. (2012). Student access to competitive foods in elementary
schools: Trends over time and regional differences. Archives of Pediatrics & Adolescent
Medicine, 166(2), 164-169. Retrieved from
http://archpedi.jamanetwork.com.library.capella.edu/article.aspx?articleid=1107696.
United States Department of Agriculture (USDA) Food and Nutrition Service (2014).
Implementation Plan: Health, Hunger-Free Kids Act of 2010. Retrieved from:
http://www.fns.usda.gov/sites/default/files/implementation_actions.pdf.
United States Department of Agriculture. (2010). Healthy, Hunger-Free Kids Act of 2010. 111th
Congress. 2009–2010. Retrieved from http://www.fns.usda.gov/school-meals/healthy-
hunger-free-kids-act.
Warraich, H.J., Javed, F., Faraz-ul-Hag, M., Khawaja, F.B., & Saleem, S. (2009). Prevalence of
Obesity in School-Going Children of Karachi. Plos ONE 4(3), 1-6.
Doi;10.1371/journal.pone.0004816. Retrieved from Capella University Library.
Wootan, M. G., D.Sc. (2012). The healthy, hunger-free kids act: One year later. NASN School
Nurse, 27(1), 18-9. Retrieved from
http://search.proquest.com.library.capella.edu/docview/993921366?accountid=27965.