PLEURAL TUM:OURS · t AsinCa,e8 nitrogen mustard; radiotherapy Thoracoscopy; radiotherapy Survival...
9
Thorax (1962), 17, 111. PLEURAL TUM:OURS BY B. T. LE ROUX From the Department of Clinical Surgery, University of Edinburgh (RECEIVED FOR PUBLICATION NOVEMBER 27, 1961) The commonest pleural tumour is a metastasis, and the commonest source of such a metastasis is a primary tumour in the lung. Primary pleural tumours are not only rare but their origin from the pleura is disputed. The purpose of this paper is to outline the clinical behaviour of pleural metastases and to compare this with the natural history of the group of tumours believed to be of pleural or subpleural origin in order to establish that, on clinical grounds, there is justification for distinguishing the latter group from metastases. A further purpose is to draw attention in one group of pleural tumours to the absence of corre- lation between the histological assessment of malignancy and prognosis. During a ten-year period when 3,000 patients investigated in the Regional Thoracic Unit in Edinburgh were found to have a bronchial carcinoma, 220 of these were shown at thoraco- scopy, thoracotomy, or necropsy to have pleural metastases, as distinct from pleural invasion in continuity with either the primary tumour or mediastinal glandular metastases. The incidence of pleural metastases may well be higher in this series, since a number of patients with extra- thoracic extension of tumour were not submitted to either thoracoscopy or thoracotomy and later died at home without necropsy. Of the 220 patients with pleural metastases from bronchial carcinoma 80% had died within six months of the diagnosis having been established, and none survived a year. In the experience of this unit pleural metastases are common, although relative to bronchial carcinoma much less common, from primary tumours in the breast (27 cases) and in the kidney (10 cases). The number of cases of pleural metastases from breast carcinoma quoted is not a true reflection of the incidence of mammary tumours metastasizing to the pleura, since only those patients severely dyspnoeic because of the rapid recurrence of pleural effusion, and therefore requiring pleural intubation, or those in whom the diagnosis was in doubt and who therefore required thoracoscopy, were referred to this unit. During the period when 3,000 patients with bronchial carcinoma were investigated, 3,500 patients with primary mammary carcinomata were seen in the Department of Radiotherapy in Edin- burgh (McWhirter, 1960). Both these figures are thought to represent fairly accurately the incidence of bronchial and mammary carcinoma during this period in this region. The introduction of nitrogen mustard into the pleural space, various forms of hormone therapy, and the ablation of various endocrine glands prolonged survival for as long as two years in some patients with pleural metastases from mammary carcinoma, but most had died within a year of their first being seen in the Thoracic Unit. Three of the ten patients with pleural metastases from primary renal carcinoma had undergone nephrectomy before they presented with pleural effusions; in the remaining seven, investigation of a pleural effusion established the diagnosis of pleural metastases from an unsuspected renal primary. All died within a year of the diagnosis of pleural metastasis having been established. Examples of metastases in the pleura from osteogenic sarcoma (three cases), uterine adeno- carcinoma (three cases), and prostatic carcinoma (two cases), and one example each of metastases from melanoma of the eye, uterine sarcoma, carcinoma of the cervix uteri, ovarian carcinoma, rectal carcinoma, and testicular seminoma, were encountered. All these patients, in common with those with primary tumours in the lung, breast, or kidney, presented with the clinical features of a pleural effusion and without other evidence of dissemination from the primary tumour. All except the two patients with prostatic tumours and the patient with a seminoma were known to have an extrathoracic tumour at the time of investigation of the pleural effusion. Three of 700 patients with a primary tumour in the proximal alimentary tract (Le Roux, 1961) had pleural metastases as distinct from pleural invasion. None of these 17 patients survived a year from copyright. on November 29, 2020 by guest. Protected by http://thorax.bmj.com/ Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. Downloaded from
Transcript of PLEURAL TUM:OURS · t AsinCa,e8 nitrogen mustard; radiotherapy Thoracoscopy; radiotherapy Survival...

Thorax (1962), 17, 111.
PLEURAL TUM:OURSBY
B. T. LE ROUXFrom the Department of Clinical Surgery, University of Edinburgh
(RECEIVED FOR PUBLICATION NOVEMBER 27, 1961)
The commonest pleural tumour is a metastasis,and the commonest source of such a metastasisis a primary tumour in the lung. Primary pleuraltumours are not only rare but their origin fromthe pleura is disputed. The purpose of this paperis to outline the clinical behaviour of pleuralmetastases and to compare this with the naturalhistory of the group of tumours believed to beof pleural or subpleural origin in order to establishthat, on clinical grounds, there is justification fordistinguishing the latter group from metastases.A further purpose is to draw attention in onegroup of pleural tumours to the absence of corre-lation between the histological assessment ofmalignancy and prognosis.During a ten-year period when 3,000 patients
investigated in the Regional Thoracic Unit inEdinburgh were found to have a bronchialcarcinoma, 220 of these were shown at thoraco-scopy, thoracotomy, or necropsy to have pleuralmetastases, as distinct from pleural invasion incontinuity with either the primary tumour ormediastinal glandular metastases. The incidenceof pleural metastases may well be higher in thisseries, since a number of patients with extra-thoracic extension of tumour were not submittedto either thoracoscopy or thoracotomy and laterdied at home without necropsy. Of the 220patients with pleural metastases from bronchialcarcinoma 80% had died within six months ofthe diagnosis having been established, and nonesurvived a year.
In the experience of this unit pleural metastasesare common, although relative to bronchialcarcinoma much less common, from primarytumours in the breast (27 cases) and in the kidney(10 cases). The number of cases of pleuralmetastases from breast carcinoma quoted is nota true reflection of the incidence of mammarytumours metastasizing to the pleura, since onlythose patients severely dyspnoeic because of therapid recurrence of pleural effusion, and thereforerequiring pleural intubation, or those in whomthe diagnosis was in doubt and who therefore
required thoracoscopy, were referred to this unit.During the period when 3,000 patients withbronchial carcinoma were investigated, 3,500patients with primary mammary carcinomata wereseen in the Department of Radiotherapy in Edin-burgh (McWhirter, 1960). Both these figures arethought to represent fairly accurately the incidenceof bronchial and mammary carcinoma during thisperiod in this region. The introduction ofnitrogen mustard into the pleural space, variousforms of hormone therapy, and the ablation ofvarious endocrine glands prolonged survival foras long as two years in some patients with pleuralmetastases from mammary carcinoma, but mosthad died within a year of their first being seen inthe Thoracic Unit.Three of the ten patients with pleural metastases
from primary renal carcinoma had undergonenephrectomy before they presented with pleuraleffusions; in the remaining seven, investigation ofa pleural effusion established the diagnosis ofpleural metastases from an unsuspected renalprimary. All died within a year of the diagnosisof pleural metastasis having been established.Examples of metastases in the pleura fromosteogenic sarcoma (three cases), uterine adeno-carcinoma (three cases), and prostatic carcinoma(two cases), and one example each of metastasesfrom melanoma of the eye, uterine sarcoma,carcinoma of the cervix uteri, ovarian carcinoma,rectal carcinoma, and testicular seminoma, wereencountered. All these patients, in common withthose with primary tumours in the lung, breast, orkidney, presented with the clinical features of apleural effusion and without other evidence ofdissemination from the primary tumour. Allexcept the two patients with prostatic tumoursand the patient with a seminoma were known tohave an extrathoracic tumour at the time ofinvestigation of the pleural effusion. Three of 700patients with a primary tumour in the proximalalimentary tract (Le Roux, 1961) had pleuralmetastases as distinct from pleural invasion.None of these 17 patients survived a year from
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

B. T. LE ROUX
TABLE IPRIMARY PLEURAL TUMOURS
RadiographicFeatures
aose Age Sex Symptoms Single0. Peri- Pleural
pheral ShadowOpacity
1 63 M Cough, 10yr.;dyspnoea4 yr.; jointpains, 1 yr.
2 3 M Cough; lossof weight;dyspnoea andlassitude
3 52 M None:M.M.R.
4 53 F Cough-
OtherSignificantFeatures
Macro-scopic
Treatment Featuresof thePleura
Abnormal radiograph Resection of 1,800 g. Normal4 yr. pre-op. Hyper- tumour with liga-trophic pulmonary tion of slenderosteoarthropathy avascular pedicle
of visceral pleuraLeft chest bulged; Pneumonectomy ,,
gross mediastinal with resection ofshift to right tumour
Abnorma9 yr. be
5 64 F None:M.M.R.
6 58 F Dyspnoea
7 39 F None:M.M.R.
8 52 M Dyspnoeaincreasing4 yr.
9 42 M Dyspnoea andpain increas-ing 3 yr.
10 56 M None;M.M.R.
It 76 M Dyspnoeaincreasingover I yr.
12 58 M DyspnoeaincreasingI yr.
13 66 M IncreasingdyspnoeaI yr.
14 58 M Increasingdyspnoea2 yr.
15 46 M Dyspnoea andpain increas-ing over 2 yr.
16 65 M Dyspnoea andpain increas-ing over I yr.
W.R. posi
- Enucleation oftumour fromoblique fissure
LI radiograph Tumour in obliqueefore fissure; apical
lower segment andposterior segmentresected
- Tumour in obliquefissure; apicallower segment andposterior segmentresected
itive Pneumonectomy
-- Tumour 7 cm. indiameter pedicledon apical segment;pedicle 5 mm. indiameter
+ Lumps on parietal Pleurectomy;pleura seen on radio- radiotherapygraph after induc-tion of pneumo-thorax
As in Case 8 Thoracoscopy;
t AsinCa,e8
nitrogen mustard;radiotherapy
Thoracoscopy;radiotherapy
Survival fromTime of
Histology Investigation (yr.)
Fibroma
Fibro-sarcoma
Alive Dead
It -
14 -
.. ,, 4 -
Fibroma 6
5 -
Fibro-sarcoma
Opera-tivedeath
13 -
Large Meso-nodules thelioma
,, S
5Smallnodules
+-4
- Thoracoscopy;pleurectomy;radiotherapy;mustine
- Pleuropneumonec-tomy
- Pleurectomy
-+- Frozen chest
+ Frozen chest
Pleuropneumonec-tomy;radiotherapy
Pleurectomy
Thick Ipleuradevoid ofnodules
Obliter-atedpleuralspace
- 3
Mesothe-Iioma orfibro-sarcomaMeso-thelioma
1I
1 -
1,. - 4
, ,, ,,I- Post-opera-tivedeath
112
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

PLEURAL TUMOURS
the time of investigation of the pleural lesion.The appearances at thoracoscopy in many of thepatients found to have pleural metastases weresimilar to those found in patients referred to laterin this paper as having large nodular meso-thelioma. In none was the appearance atthoracoscopy similar to that found in the smallnodular mesothelioma, and in none was thepleural space obliterated.During the same ten-year period 16 patients
investigated in this unit have been found to havetumours which have been called primary pleuraltumours. In nine of these patients the radio-graphic abnormality was a pleural shadowsuggestive of a pleural effusion, and in all thesethe diagnosis of pleural mesothelioma was madeon histological grounds, with the diagnosis offibrosarcoma offered as an alternative in one. Inthe remaining seven patients the radiographicabnormality was a single well-circumscribedperipheral opacity; in three of these the diagnosisof fibrosarcoma was made, and in four of fibroma.Details relating to these 16 patients are shown inTable I.
CASE REPORTSCase 1 (Figs. 1 and 2) is similar to many reported
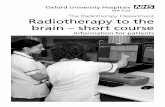
examples of pleural fibroma (e.g., Thomas and Drew,1953), and it is the only example in the present seriesof a patient with hypertrophic pulmonary osteo-arthropathy. The diagnosis of fibroma was madepre-operatively on the basis of the changes in thejoints; joint pain had disappeared by the time thepatient was able intelligently to answer questions onthe evening of the day of operation, and his fingerswere normal three months later. This patient hadbeen found to have an abnormal chest radiographfour years before thoracotomy. At thoracotomy thetumour was found to be attached by a slenderavascular pedicle to the apical segment of the leftlower lobe.
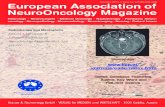
Case 2 (Fig. 3) is unusual because of the age ofthe boy (he was 3 years old at the time of thoraco-tomy) and the size of the tumour, which occupied theleft hemithorax and encroached on the right. Aconfident histological diagnosis of fibrosarcoma wasmade, and the boy is well 14 years later. In Case 3(Fig. 4) the unusual feature was the macroscopicappearance of the tumour, which lay in the obliquefissure between middle and lower lobes. The tumourshelled out of the fissure without the sacrifice of anypulmonary tissue, and during manipulation it dis-integrated into six small spherical lumps, each wellcircumscribed and free from its neighbour, the largestthe size of a golf-ball and the smallest the size of apea. The appearance was likened at the time ofresection to a nest containing eggs of different sizes.Each separate tumour had the same histologicalfeatures, called sclerosing fibrosarcoma.
FIG. 1
FIG. 2
FIGS. 1 and 2.-Case 1. P.A. and lateral views showing a largeintrathoracic fibroma in a patient with hypertrophic pulmonaryosteoarthropathy.
113
WW, Vr4w.. M.
1 i:,
;il
e!QL
I
.4-4!
Z,1:
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

114 B. T. LE ROUX
. w~~~~~~~~~~~~~~~~~~~~~~~~~~1 ......I.
FIG. 3.-Case 2. A large left intrathcracic fibrosarcoma displacingthe mediastinum to the right in a boy of 3 years.
FIG. 4.-Case 3. A "nest" of fibrosarcomata in the oblique fissure.
[to.... . . .. X. ..
FIG.S
Fic,s. S and 6.-Case 4. A P.A. view and a tomogram ot a fibromain the oblique fissure.
FIG. 6
im
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

PLEURAL TUMOURS
FIG. 7.-Case 5. Another example ofa fibroma in the oblique fissure.
Case 4 (Figs. 5 and 6) and Case 5 (Fig. 7) weresimilar. In each at thoracotomy a lump lay buriedin the oblique fissure between the apical segment ofthe right lower lobe and the posterior segment of theupper lobe, and in each these segments were resectedwith the lump. Dissection of the operative specimenshowed a tumour in the fissure displacing but notinvading lung. In neither was the fissure welldeveloped, and in each resection was undertaken inthe belief that the tumour was pulmonary andprobably an adenoma. In both resection wasconservative because of a limited respiratory reserve;a less conservative resection would have meantpneumonectomy. Case 6 is one of the two operativedeaths in this series. Thoracotomy was undertakenbecause of a lobulated opacity 7 cm. in diameter inthe periphery of the right lung. without pre-operativelead to the diagnosis. Haemorrhage from the azygosvein contributed to death. The fibroma was describedas subpleural in origin, compressing but not invadingthe subtended lung. The operative findings in Case 7were similar to those in Case 1, and this is anotherexample of long survival following resection of atumour called by the examining pathologist afibrosarcoma.Case 8 (Fig. 8) and Case 9 (Fig. 9) are examples of
pleural mesotheliomata visible on plain films of thechest as large parietal pleural nodules after replace-ment of a pleural effusion with air. The noduleswere all larger than a centimetre in diameter and, incomparison with the small nodular mesothelioma.relatively few in number and scattered over a rela-tively limited area; the nodules were confined to theparietal pleura in these two examples, and the pleuralsurface of the nodules was ulcerated. This macro-
I
FIG. 8
.......P....'.............. ....
FIG. 9
FIGS. 8 and 9.-Cases 8 and 9. Two examples of large nodularmesotheliomata visible on the parietal pleura after replacementof a pleural effusion with air.
115
PP
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

B. T. LE ROUX
FIG. 10 FIG. 11
FIGS. 10 and 11.-Case 10. P.A. and lateral views showing a large nodular mesothelioma visible after the aspiration of pleural liquidwithout a pneumothorax.
FIG. 12a FIG. 12b
FIG. 12.-Case 12. P.A. views of the chest (a) before and (b) after the aspiration of pleural liquid in a patient with a small nodularmesothelioma.
116
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

PLEURAL TUMOURS
scopic appearance is indistinguishable from that ofpleural metastases from any of the sources mentionedearlier. The large nodules on the parietal pleura inCase 10 were visible on plain films after thoracentesisin the absence of a pneumothorax (Figs. 10 and 11).In Cases 8 and 9 death from progress of diseaseoccurred more than five years after the onset ofsymptoms, and in one case hepatic metastases werefound at necropsy. Case 10 is unusual in that thepatient presented because of an abnormal massradiograph; he is well five years after investigation,with certainly no increase in the size of the opacitiesand possibly a little shrinkage of the lesionsradiographically after radiotherapy.
Cases 11, 12, and 13 are examples of patientspresenting with pleural effusions and found to havemultiple, small, smooth, non-ulcerating parietal pleuraltumours, all roughly the same size, none larger than3 or 4 mm., scattered thickly over the pleural surface,with involvement of the diaphragmatic andmediastinal pleurae but with very little involvement ofthe visceral pleura. The chest radiographs fromCase 12 before (Fig. 12a) and after (Fig. 12b)aspiration of the effusion are typical of these threecases; the film made after thoracentesis would passas normal. This patient died three years afterpleurectomy, from recurrence of tumour and frommetastases. A year before death, pain in the backprompted further radiographic studies and vertebraldestruction was seen. At necropsy extensive recur-rence of tumour in the pleural space and hepatic andvertebral metastases were found. The histologicalappearances of the metastases were similar to thoseof the original operative specimen. Long survivalfrom the onset of symptoms (e.g., Case 11, this patientnow being 81 years old) is one feature whichdistinguishes this group of pleural tumours frompleural metastases. The examining pathologists wereunable to decide whether Case 13 was an example ofpleural mesothelioma or fibrosarcoma.
In Case 14 the parietal pleura was 1 cm. thick butdevoid of nodules. The last two patients (Cases 15and 16) both presented with pain in the chest anddyspnoea; in each the hemithorax was immobile andshrunken, and there was a dense pleural shadow withan obliterated pleural space. In Case 15 the diagnosisof mesothelioma was made from the histologicalexamination of a nodule removed with the scalenepad; the nodule was adjacent to, but not invading,a lymph gland. This patient died four years afterpleuropneumonectomy, undertaken because of paindespite the evidence of extrathoracic extension oftumour; at necropsy the hemithorax on the side ofpneumonectomy was filled with tumour and the heartwas encased in a mass of intrapericardial tumour,death being directly related to cardiac constriction.This patient survived six years from the onset ofsymptoms and four years from the demonstration ofextrathoracic extension of tumour. Case 16, theother operative death, demonstrates the hazard of anextenisive pleural resection, with concomitant air leaks
from the lung, in a patient with a limited respiratoryreserve; multiple persisting fistulae contributed to thispatient's death on the eighth post-operative day fromrespiratory insufficiency.Of these 16 patients, therefore, seven had a
single peripheral spherical radiographic opacity;six of these seven are alive four to 14 years afteroperation, and one died from operation (fromhaemorrhage unrelated to the tumour); the histo-logical diagnosis in three of the six survivors wasfibrosarcoma; and none has evidence of tumourrecurrence. In nine of the 16 patients the radio-graphic abnormality was a pleural shadow-aneffusion in seven and thickened pleura with anobliterated pleural space in two. In these ninepatients the pleura was diffusely tumorous, leastdiffusely where the nodules of tumour werelargest, and the histological diagnosis of meso-thelioma was offered in all of them, with fibro-sarcoma as an alternative in one (with smallnodules). In two patients the diagnosis ofmesothelioma was qualified by the descriptive termpapillary, in two others mucus-secreting, and inone each cuboidal, pleomorphic, and solid. Intwo mesothelioma was unqualified. Wide varia-tion in the histological structure of diffusemalignant pleural mesothelioma is well recognized.Five of these nine patients have died, one inrelation to operation and four one to four yearsafter operation but four to six years after theonset of symptoms. Four are alive, two of thesefive years after investigation. Extrathoracicmetastases were found in one patient duringinvestigation and in two others at necropsy. Longsurvival is therefore a feature of most of thesepatients, in comparison with short survival ofpatients with metastatic tumours in the pleura.
DISCUSSIONKlemperer and Rabin (1931) distinguished two
groups of primary pleural tumours, a fibromatousgroup which they believed had their origin fromthe tissues deep to the superficial lining cells ofthe pleura, and a group called mesothelioma,which arose from the surface lining cells of thepleura. Clagett, McDonald, and Schmidt (1952)recognized these two groups of tumours, distin-guishable by the circumscription of the one andthe diffuseness of the other; they believed thatthese two groups of tumours had nothing incommon except their supposed origin from thepleura, but since both must have a mesothelialorigin, they subscribed to and acknowledged thevalue of the terms "localized fibrous " and" diffuse malignant " mesothelioma. That the
117
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

B. T. LE ROUX
localized fibrous mesothelioma, for which synony-mous terms are pleural fibroma, intrathoracicfibroma, and benign localized mesothelioma, isoften malignant is clear from the reports in theliterature of recurrence of these tumours afterresection and their development of invasiveproperties. Kerr and Nohl (1961) report sixexamples of recurrence of localized fibroustumours previously called benign, and Clagettet al. (1952) and Ehrenhaft, Sensenig, and Law-rence (1960) also report examples of recurrenceafter resection of pleural fibromata. All theseauthors comment on the histological similaritybetween the original tumour and the recurrence.The rather sweeping generalization that fibromais the diagnosis of the intellectually destitute wasgleaned when one was an undergraduate. Thesource of this aphorism is forgotten, but itsmessage is valid-every fibroma is a potentialfibrosarcoma.The localized tumours, comprising the first
seven cases in this series, cannot therefore becalled benign tumours, but their behaviour makesthem relatively benign. The diagnosis of fibromaor fibrosarcoma in this type of tumour dependsmore on the histologist than on the histology. Thelocalized fibrous mesothelioma may have histo-logical features which necessitate calling it asarcoma, and resection may yet allow of longsurvival without recurrence, or may have histo-logical features which suggest benignity andresection may be followed by recurrence. Templeand Jones (1954) emphasize that the differencebetween the highly cellular anaplastic fibrosar-coma and the densely fibrous and apparentlybenign growth is one only of degree. In one ofthe nine diffuse tumours called mesothelioma thediagnosis of fibrosarcoma was suggested as analternative. This implies an overlap between thetwo groups. This overlap has been emphasizedby McCaughey (1958) and by Kahn, Glay, andMadore (1959). If in fact the " pleural " fibromaarises from subpleural tissues and the meso-thelioma from the layer of serosal cells comprisingthe pleural membrane, then such an overlap isacceptable on embryological grounds; thecoelomic epithelium and the underlying mesen-chyme are both derived from mesoderm and arenot separated by a basement membrane. The viewof Stout and Murray (1942) that intrathoracicfibroma is a localized form of pleural meso-thelioma is widely accepted in the North Americanliterature, and the application of the term meso-thelioma to the localized fibrous growth empha-sizes its potential malignancy. The behaviour ofthe diffuse mesothelioma is that of a slow-growing
malignant tumour, the course of which is littleinfluenced by any surgical procedure, and claimsof prolongation of life by surgical removal ofthese tumours must be judged with the knowledgethat long survival is common in the absence ofsurgical intervention. The value of resection ofmesotheliomata seems purely palliative, achievingpalliation in one of three ways-by limiting thereaccumulation of pleural liquid, by relievingpain, or, when accompanied by pulmonary resec-tion, by providing space in which the tumour maypursue its growth for a longer period with lessinterference with vital structures. The pain pro-duced by diffuse mesothelioma is constant andgnawing in character, suggestive of nerve involve-ment rather than pleural irritation. Barrett andElkington (1938) reported examples of pleuralmesothelioma with neurological abnormalities-paralysis and sensory loss in the distribution ofintercostal nerves on the side of the tumour andsuggested that nerves were involved by the tumourposteriorly, where the anterior primary ramus liesin direct relation to parietal pleura, unprotectedby rib.
Willis (1953) denies the existence of meso-theliomata as an entity, but whatever doubts theremay be on histological grounds, the clinicalbehaviour of this group of tumours is differentfrom that of pleural metastases, and long survivalof many patients with mesotheliomata is thedistinguishing feature.For simplicity it seems justifiable to attribute
to the pleura only one tumour, and that is malig-nant, a sarcoma. This tumour behaves in one oftwo ways, with an overlap between these twomodes of behaviour: (1) When it is single andlocalized it usually, but not always, arises in rela-tion to the visceral pleura. It is often associatedwith the clinical syndrome of hypertrophicpulmonary osteoarthropathy (Thomas and Drew,1953) and with episodes of chills and fever(Ehrenhaft et al., 1960). The histological featuresare often those of fibrous tissue only, and yetrecurrence of these tumours after resection is notuncommon. (2) When the sarcoma has a morediffuse origin from the pleura it is usually mostwidely disseminated in relation to the parietalpleura, presents because it produces dyspnoea frompleural effusion, and sometimes pain, has a variablehistological pattern sometimes indistinguishablefrom the first group, and is frequently associatedwith long survival despite its more clearly defin-able malignant clinical and histological charac-teristics. The clinical behaviour of both groupsmerges, but is clearly different from that of pleuralmetastases from other malignant tumours.
11 8
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from

PLEURAL TUMOURS
SUMMARY
The clinical behaviour of pleural metastases,based on 274 cases, is outlined and compared withthe behaviour in 16 cases of tumours believed tobe primarily pleural. It is suggested that the onlyprimary pleural tumour is a sarcoma, which maybe circumscribed or may involve the pleuradiffusely. Typical examples of these two varietiesof sarcoma behave in a recognizable way whichserves to distinguish them, but there is consider-ablz overlap histologically. Pleural sarcoma isa slow-growing tumour associated with longsurvival, and differs from metastatic pleuraltumours which usually result in death within ayear.
REFERENCESBarrett, N. R., and Elkington, J. St. C. (1938). Brit. J. Surg., 26, 314.Clagett, 0. T., McDonald, J. R., and Schmidt, H. W. (1952). J.
thorac. Surg., 24, 213.Ehrenhaft, J. L., Sensenig, D. M., and Lawrence, M. S. (1960). Ibid.,
40, 393.Kahn, D. S., Glay, A., and Madore, P. (1959). Ibid., 38, 225.Kerr, W. F., and Nohl. H. C. (1961). Thorax, 16, 180.Klemperer. P., and Rabin, C. B. (1931). Arch. Path. Lab. Med., 11,
385.Le Roux, B. T. (1961). Thorax, 16, 226.McCaughey, W. T. E. (1958). J. Path. Bact., 76, 517.McWhirter, R. W. (1960). Personal communication.Stout, A. P., and Murray, M. R. (1942). A-ch. Path. Lab. Mled., 34,
951.Temnple, L. J., and Jones, G. Penrhyn (1954). Thorax, 9, 112.Thomas, Sir Clement Price, and Drew, C. E. (1953). Ibid., 8, 180.Willis, R. A. (1953). Pathology of Tumours, 2nd ed. Butterworth,
London.
119
copyright. on N
ovember 29, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.17.2.111 on 1 June 1962. D
ownloaded from