PLEASE LET TOM KNOW OF ANY ERRORS/ OTHER OPTIONS …
11
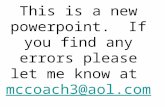
UNIVERSITY HOSPITAL, GEELONG FELLOWSHIP WRITTEN EXAMINATION WEEK 14– TRIAL SHORT ANSWER QUESTIONS Suggested answers PLEASE LET TOM KNOW OF ANY ERRORS/ OTHER OPTIONS FOR ANSWERS Please do not simply change this document - it is not the master copy ! Question 1 (18 marks) A 45 year man presents following a collapse. His observations are: BP 130/70mmHg Temp 36° O2 saturation 98% on room air a. State four (4) abnormal findings shown in this ECG.(4 marks) • Sinus tachycardia 100 bpm • STE: o 4mm in V1-2, “Downsloping” or “Coved” o Brugada sign (as this is followed by inverted Twave) • STD 2mm V4-V6, II, III, aVF • TW V1-2, aVL, biphasic in V3 b. What is the significance of this ECG for this patient? List two (2) points of significance. (2 marks) • In association with syncope is diagnostic of Brugada syndrome • Needs admission to monitored bed to monitor for malignant arrhythmia • High untreated mortality from VF (~ 10% / year) Type 1 (Coved ST segment elevation >2mm in>1 of V1-V3 followed by a negative T wave) is the only ECG abnormality that is potentially diagnostic. The other two types of Brugada are non-diagnostic but possibly warrant further investigation. Type 2 has >2mm of saddleback shaped ST elevation. Brugada type 3 can be the morphology of either type 1 or type 2, but with <2mm of ST segment elevation. c. What is the pathophysiological basis for this problem? (3 marks) • Mutation in a sodium channel gene (sodium channelopathy) • Either spontaneous or familial clustering (autosomal dominant) • Subendocardial fibrosis or replacement of myocardium with adipose d. List four (4) likely precipitating causes for this presentation. (4 marks) NB: ECG changes of Brugada syndrome can be transient and can be augmented or unmasked by multiple factors • Drugs: o Na Channel blockers/ CCB/ BBlockers o Nitrates o Cholinergic stimulation o Alcohol o Cocaine • Fever • Myocardial ischaemia • ↓K + • Post DCR • Alcohol • Hypothermia e. List four (4) other clinical features (Clinical features = Hx & Ex) that may also be associated with this problem. (4 marks) NB: To be Dx as “Brugada Syndrome”: 1) Brugada sign on ECG (Coved ST > 2mm in > 1 of V1-V3 followed by TWI) & 2) One of the following clinical criteria (or syncope as here) • VF • Polymorphic VT • FHx sudden cardiac death < 25 years old • Coved-type ECGS in family members • Inducible VT with flecainide or electrical stimulation • Nocturnal agonal respiration f. What is the specific treatment of choice for this problem? • AICD (or Quinidine if AICD CI eg neonate) “List” = 1-3 words “State”= short statement/ phrase/ clause
Transcript of PLEASE LET TOM KNOW OF ANY ERRORS/ OTHER OPTIONS …
UNIVERSITYHOSPITAL,GEELONG
FELLOWSHIPWRITTENEXAMINATIONWEEK14–TRIALSHORTANSWERQUESTIONSSuggestedanswersPLEASELETTOMKNOWOFANYERRORS/OTHEROPTIONSFORANSWERSPleasedonotsimplychangethisdocument-itisnotthemastercopy!
Question1(18marks)A45yearmanpresentsfollowingacollapse.Hisobservationsare:BP130/70mmHgTemp36°O2saturation98%onroomair
a. Statefour(4)abnormalfindingsshowninthisECG.(4marks)• Sinustachycardia100bpm• STE:
o 4mminV1-2,“Downsloping”or“Coved”o Brugadasign(asthisisfollowedbyinvertedTwave)
• STD2mmV4-V6,II,III,aVF• TWV1-2,aVL,biphasicinV3
b. WhatisthesignificanceofthisECGforthispatient?Listtwo(2)pointsofsignificance.(2marks)
• InassociationwithsyncopeisdiagnosticofBrugadasyndrome• Needsadmissiontomonitoredbedtomonitorformalignantarrhythmia• HighuntreatedmortalityfromVF(~10%/year)
Type1(CovedSTsegmentelevation>2mmin>1ofV1-V3followedbyanegativeTwave)istheonlyECGabnormalitythatispotentiallydiagnostic.TheothertwotypesofBrugadaarenon-diagnosticbutpossiblywarrantfurtherinvestigation.Type2has>2mmofsaddlebackshapedSTelevation.Brugadatype3canbethemorphologyofeithertype1ortype2,butwith<2mmofSTsegmentelevation.c. Whatisthepathophysiologicalbasisforthisproblem?(3marks)
• Mutationinasodiumchannelgene(sodiumchannelopathy)• Eitherspontaneousorfamilialclustering(autosomaldominant)• Subendocardialfibrosisorreplacementofmyocardiumwithadipose
d. Listfour(4)likelyprecipitatingcausesforthispresentation.(4marks)NB:ECGchangesofBrugadasyndromecanbetransientandcanbeaugmentedorunmaskedbymultiplefactors
• Drugs:o NaChannelblockers/CCB/BBlockerso Nitrateso Cholinergicstimulationo Alcoholo Cocaine
• Fever• Myocardialischaemia• ↓K+ • PostDCR• Alcohol• Hypothermia
e. Listfour(4)otherclinicalfeatures(Clinicalfeatures=Hx&Ex)thatmayalsobeassociatedwiththisproblem.(4marks)
NB:TobeDxas“BrugadaSyndrome”: 1)BrugadasignonECG(CovedST>2mmin>1ofV1-V3followedbyTWI)& 2)Oneofthefollowingclinicalcriteria(orsyncopeashere)• VF• PolymorphicVT• FHxsuddencardiacdeath<25yearsold• Coved-typeECGSinfamilymembers• InducibleVTwithflecainideorelectricalstimulation• Nocturnalagonalrespiration
f. Whatisthespecifictreatmentofchoiceforthisproblem?
• AICD (orQuinidineifAICDCIegneonate)
“List”=1-3words“State”=shortstatement/phrase/clause

Question2(12marks)A45yearoldmanisbroughtintoyouremergencydepartment,byambulance,withisolatedseverepaininhisrighthipafterafallfromhismotorbikeonehourearlier.HehasapasthistoryofIVDU.TheambulanceofficerswereunabletoobtainIVaccessandhaveprovidedpenthraneforanalgesiaalone.Hisambulancehandoverobservationsare:BP95/50mmHgHR130bpmRR24bpmOxygensaturations98%RAGCS15Hisprimarysurvey,includingaFASTscan,isnegative.Youarrangeatraumaseriesplainxray.
a. Statefive(5)stepsinyourinitialapproachtoprovisionofanalgesia.Includeanydrugdosesandroutes.(5marks) NB:HxIVDU
• Continuepenthrane/redosepenthraneifonlysingledosegiven• Inhalational:Nitrousoxide50/50• INfentanyl-anticipate>usualdosesneeded(usual1.5mcg/kgacceptto2mcg/kgrepeatsamedose
in10/60ifinadequate)• IMketamineafterHxtaken:2-3mg/kg,followedbyKetamine10-20mgIVwhenIVaccessobtained• IVnarcotic-morphinewhenIVaccessobtained-anticipatehighlevelsneeded-15-20mgtotal+.May
aggravatehypotension.Fentanyl25-50mcgtitratedabetteroption.
b. Statefive(5)abnormalfindingsshowninthisxray.(5marks)
• Comminuted # of R femur at junction of prox and mid 1/3 with 100% off ending andangulation.
• DislocatedRhip,likelyanteriorwithinfero-medialdisplacement• Transverse#Rpubicbone,symphysisnotwidened• #Rsuperiorpubicramus/acetabularfloorwithmedialdisplacement• metalandmaterialartifactRthigh
Hisinjuriesareconfirmedtobeisolatedtothoseshowninthehipxrayonly.Despiteyourinitialprovisionofanalgesia,hecontinuestocomplainofseverepain.
c. Statetwo(2)pointsinyouron-goingapproachtohisanalgesia.Includeanydrugdosesandroutes.(2marks)• Reduced#femurandlongitudinaltraction• FurtherIVketamine-10mgbolus/backgroundinfusion• FemoralnerveblockunderUSguidance(0.5%2-3mg/kg)
NB:givenHxIVDU-PCAisrelativelyCI

Question3(12marks)
a. Completethetabletodistinguishbetweentheinvestigativefeaturesofdiabeticketoacidosisandhyperosmolarnonketoticstate.(4marks)
Investigation Diabeticketoacidosis Hyperosmolarnonketoticstate
BSL
>11(rarely>30) BSLveryhigh(>33)
Osmo
N Hyperosmo>350mosm/L
Acidosis pH<7.3HCO3<15
Mildorabsent(mayhavemildLacticacidosis
Seketones ≥0.6mmol/L(usually>10mmol/L)
≤0.6
Ur:Cr
increased
b. Completethetabletodistinguishbetweenthemanagementofdiabeticketoacidosisand
hyperosmolarnonketoticstate.(8marks)
KeyManagementstep Diabeticketoacidosis Hyperosmolarnonketoticstate
Fluidrequirements ~5Ldeficitreplacedover24-48/24 Greatervolumesneeded-8-20L,slowIVreplacementover48-72/24
Insulinrate Requiredat0.1IU/kg/hrifBGL>15 Maynotberequired.Ifrequired,lowerdose0.05IU/kg/hr
K+replacement Initialrate10-20mmol/hrOftenlargedeficit
Deficitsvariable
VTEprophylaxis Notusu.clinicallyrelevant VTEmajorcauseofmorbidity/mortality
Rxunderlyingcause

Question4(12marks)
A65yearoldwomanpresentswithasevereheadache.Sheisotherwiseasymptomaticandtakesnoregularmedications.Herobservationsare:
BP 245/130mmHgHR 80 bpmRespiratoryrate 18 bpmTemperature 36 °COxygensaturation 100% roomairGCS 15
a. Listfour(4)keyexaminationfindingstoseekonyourexamination.Listwhyeachsignisimportant.(4marks)
Examinationfinding Whyisthissignimportant?
Papilloedema
↑ICP
Meningism-neckstiffness
↑ICP-SAH
CNIII
Suggestsaneurysm
Renalabruit
RAS
Renalmass
RCC
Adrenalmass
Cushingsyndromefeatures
LeadstopossibleunderlyingDx
Hypertensiveretinopathy EndorganeffectoflongstandingHT
LVF,4thheartsound
CCF
b. Listfour(4)drugoptionsforthemanagementofherbloodpressure.Foreachstateyourinitialdoseandroute.(8
marks)
Drugoption Dose/routeLabetolol(stroke,preeclampsia+withGTNindissection)
10-20mgIVbolusrepeatedevery10minuntiltargetBPobtainedthen1-2mg/mininfusion
Hydralazine 5-10mgbolusrepeated10minutely
GTN(ischaemia,LVF) 300-600mcgS/LFollowedbyinfusion5mcg/kg/hrtitratedtoresponse
Phentolamine(Phaeo) 1-5mgbolusestomaximum15mg
Nifedipine 60mgQIDPO
Morphine 2.5mgboluses5/60
Question5(12marks)
A6weekoldfemaleinfantpresentswithvomiting.a. Listsix(6)likelycausesofvomitinginthispatient.Statetheclinicalfeaturesthatwouldallowyoutodifferentiateeach
cause.(12marks)Causeofvomiting Distinguishingclinicalfeature/s
Overfeeding
Hx of overfeeding + absence of features of other seriouscause
Reflux
smallmilkpossetspostfeedsinwellinfant
Sepsis
Temperature,
Pyloricstenosis projectilenonbiliousvomitingpostfeeds,thenhungry,oliveshapedmass,visibleperistalsisR-L
Intussusception Intermittentepisodescryingandpallor,wellinbetween
Malrotation Distended abdo, distressed with pain, bilious vomiting,feedingissuessincebirth
NEC Prematurity
Metabolicdisorder FHxsame,FFT,↓BSL(98%have≥1episodeofhypo)DysmorphicSeizures
Infectivegastro rapid onsetdiarrhoea+/- vomiting, fever, abdominal pain,oftenhistorycontactwithanotherpersonwithsimilarSx
ClickontheimagebelowtoviewtheentirePDF(&print/saveifnecessary)
Question6(12marks)
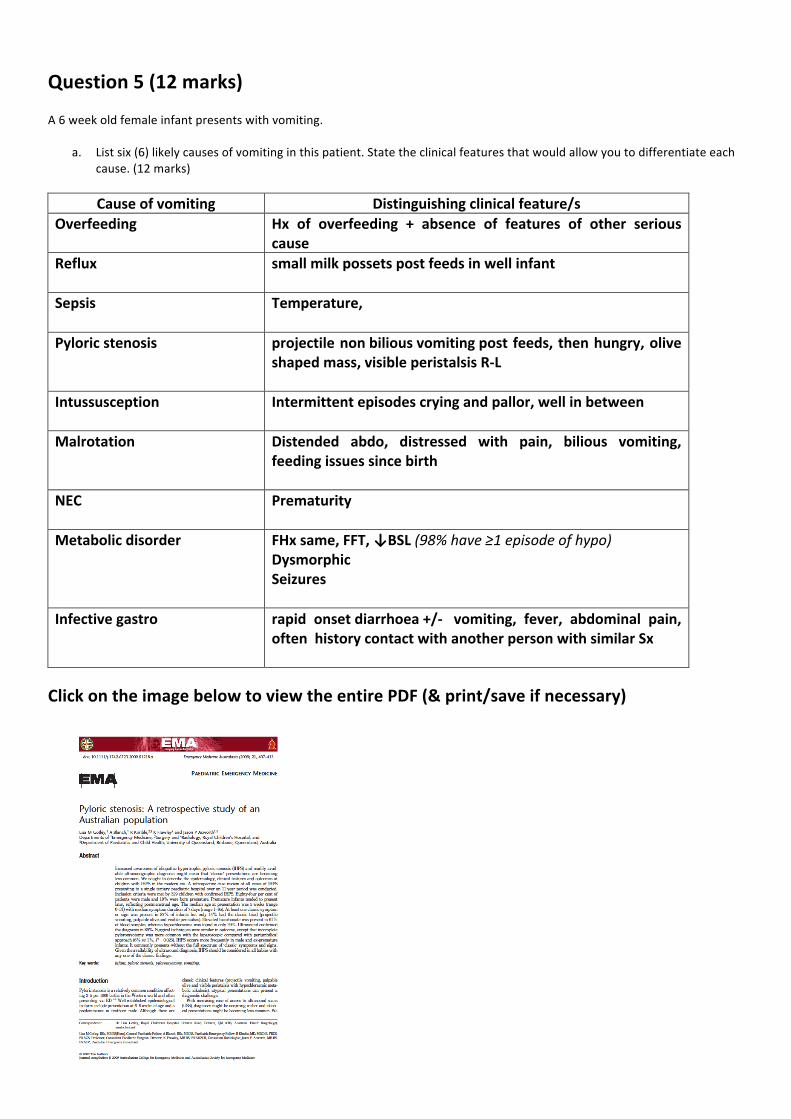
A23yearoldmanpresentedwithapainfulneckafterdivingintoapool.
a. Statethree(3)abnormalfindingsshowninhisx-ray.(3marks)
• #antC5-flexionteardrop• Anteriordisplacementoffracturefragment• Disruptionmiddlecolumn• STswellinganteriorly
b. Isthisinjurylikelytobestableorunstableandwhy?(2marks)
Stableorunstable Why?
Unstable • Ligamentousdisruptionhighlylikely-anteriorlongitudinal
• 2columnsinvolved-anterior&middlec. Listfour(4)physicalmethodsthatyoucouldutilisetoimmobilisethispatient.(4marks)
• RigidCxspinecollar• Sandbagsandtape• Foamhardblockandspinalboard• Strappinghead,thorax,abdo,pelvis• Vacuummattress
d. Ifthepatientistoremainnotintubated,listthree(3)othernon-physicalmeasurescouldyouemploytoensurespinalimmobility• Explaintoptandensureheisawaretoliestill• Analgesia• Antiemetic• Sedation
Question7(10marks)
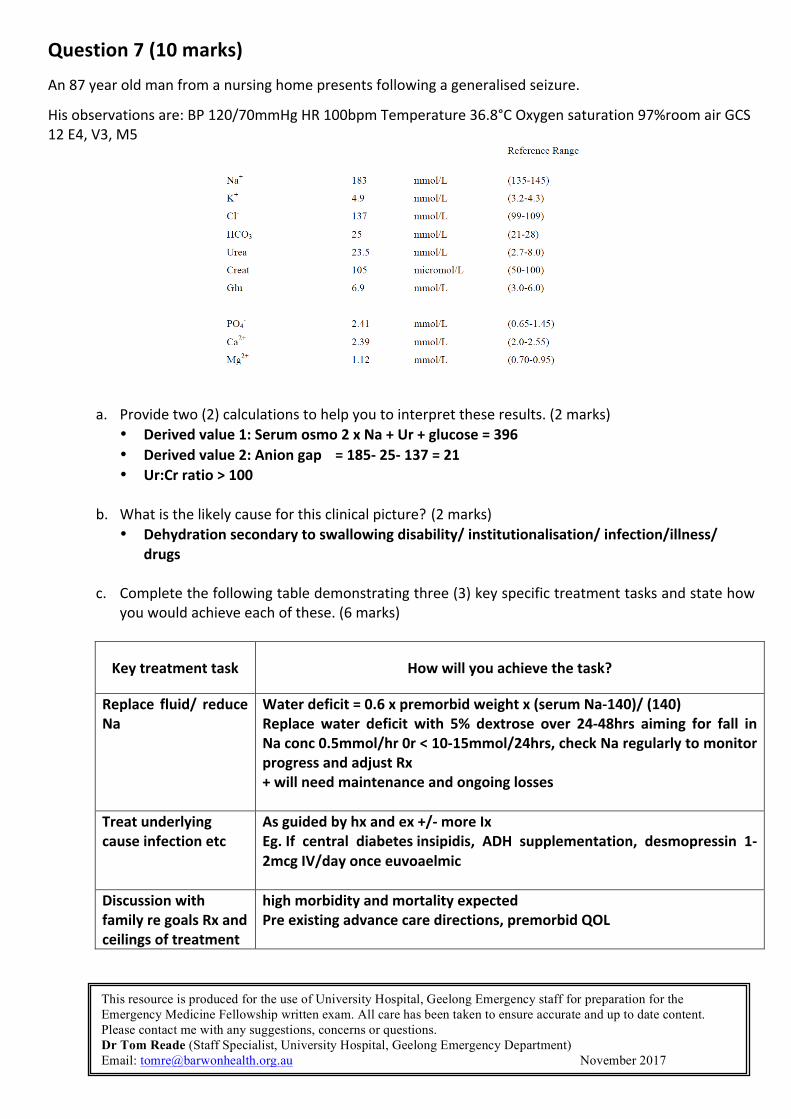
An87yearoldmanfromanursinghomepresentsfollowingageneralisedseizure.
Hisobservationsare:BP120/70mmHgHR100bpmTemperature36.8°COxygensaturation97%roomairGCS12E4,V3,M5
a. Providetwo(2)calculationstohelpyoutointerprettheseresults.(2marks) • Derivedvalue1:Serumosmo2xNa+Ur+glucose=396• Derivedvalue2:Aniongap =185-25-137=21• Ur:Crratio>100
b. Whatisthelikelycauseforthisclinicalpicture?(2marks)
• Dehydrationsecondarytoswallowingdisability/institutionalisation/infection/illness/drugs
c. Completethefollowingtabledemonstratingthree(3)keyspecifictreatmenttasksandstatehowyouwouldachieveeachofthese.(6marks)
Keytreatmenttask Howwillyouachievethetask?
Replace fluid/ reduceNa
Waterdeficit=0.6xpremorbidweightx(serumNa-140)/(140)Replace water deficit with 5% dextrose over 24-48hrs aiming for fall inNaconc0.5mmol/hr0r<10-15mmol/24hrs,checkNaregularlytomonitorprogressandadjustRx+willneedmaintenanceandongoinglosses
Treatunderlyingcauseinfectionetc
Asguidedbyhxandex+/-moreIxEg.If central diabetesinsipidis, ADH supplementation, desmopressin 1-2mcgIV/dayonceeuvoaelmic
DiscussionwithfamilyregoalsRxandceilingsoftreatment
highmorbidityandmortalityexpectedPreexistingadvancecaredirections,premorbidQOL
This resource is produced for the use of University Hospital, Geelong Emergency staff for preparation for the Emergency Medicine Fellowship written exam. All care has been taken to ensure accurate and up to date content. Please contact me with any suggestions, concerns or questions. Dr Tom Reade (Staff Specialist, University Hospital, Geelong Emergency Department) Email: [email protected] November 2017

Question8(12marks)
A4yearoldgirlpresentswithapainfulrighteyeforthelast1day.
a. Usingthetableprovided,listsix(6)clinicalfeaturesthatwoulddifferentiatebetweeninsectbite,
preseptalandorbitalcellulitis.(6marks)Clinicalfeature Insectbite Preseptalcellulitis Orbitalcellulitis
Source Bitewitnessed,visible
N N
Systemicfeatures(unwell,febrile,nauseated)
N Possible Verylikely
Opthalmoplegia/↓eyemovements
- - Present
Proptosis - - Possible(latesign)
Presenceofanteriorchanges-chemosis
- - Possible
↓VA N N Possible
RPAD - - Possible
b. Assumingthediagnosisisorbitalcellulitis, listthree(3)keymanagementpointsforthispatient.
Provideonejustificationforeachchoice.(6marks) Keymanagementpoint Justification
IVantibiotics-IVfluclox+ceftriaxone
InfectionwithseriouscomplicationsnecessitatingparenteralAbsCoverStaph,Strep,HInf
Analgesia Verypainfulcondition
Admit/disposition UrgentOpthalmologyconsultasmayrequireorbitaldecompressionifCTprovenabscess

Question9(18marks)a. Completethetable,listingsix(6)causesofneonataljaundice.Listeachcauseinthecharacteristictimeframefor
appearanceofjaundice.(4marks)Timetoonsetofjaundice Causeofneonataljaundice
<2days
• ABOincompatibility• Rhincompatibility• Bacterialsepsis• TORCHinfections• HaemolysisegG6PDdeficiency
2-3days • Physiological
3-7days• Bacterialsepsis• Toxoplasmosis• CMV
>1week
• Bacterialsepsis• Hepatitis• Congenitalbileductatresia• Congenitalhaemolyticanaemia• DruginducedHaemolyticanaemia• Rubella• Herpes• Hypothyroidism• Breastmilkjaundice
b. Listtwo(2)biochemicalfeaturesseenwithpathologicaljaundice.(2marks)• Conjugatedbilirubin• SeBili>13
c. Listthree(3)optionsforthemanagementofpathologicaljaundice.(3marks)
• Observe• Phototherapy• Exchangetransfusion
d. Define“ApparentLifeThreateningEvent”.(1mark)
• Anepisodethatisfrighteningtotheobserver,characterisedbysomecombinationof:o Apnoeao Colourchangeo Changeinmuscletoneo Chockingorgagging
e. Listthree(3)featuresofabenign“ApparentLifeThreateningEvent”.(3marks)
• Termchild• Previouslywell• Symptomstemporallyrelatedtofeeding
f. Listfive(5)investigationsthatareindicatedinapatientwhoshowsfeaturesofaserious“ApparentLifeThreatening
Event”.• FBE&diff• U+E• RBG• NPAforviruses/pertussis• ECG(espforQT)
Consideredinselectedcases:lactate,ammonia,acycamitineprofile,EEG,CTB,Holter,toxscreen,metabolicscreen

FromRCH:
ALTEDefinitionAnepisodethatisfrighteningtotheobserverandischaracterizedbysomecombinationof:
• Apnoea(centralorobstructive)• colourchange(cyanotic,pallid,orplethoric)• changeinmuscletone(usuallydiminishedbutmaybestiffening)• chokingorgagging
Insomecases,theobserverfearsthattheinfantwilldieorhasdied.Notes"ApparentLifeThreateningEvent(ALTE)"isnotadiagnosisbutratheradescriptionwhichencompassesabroadrangeofpresentationsdescribedinthedefinitionabove.Whileausefultermforclinicianstocollectivelydescribethesepresentations,itisatermwhichcanprovokeunnecessaryanxietyandalarminparents.Inwellover95%ofpatientswiththesepresentationsthecauseisphysiologicalorarelativelybenignpathologicalcondition(seebelow).Theterminologyshouldnotbeusedinfrontofparentsoronwrittenmaterialstheymightseewithoutcarefulthoughtandexplanation.ALTEisapresentationofinfancy,withhighestfrequencyinthefirst3monthsoflife.Approximately0.1%ofotherwise-healthytermbabieswillpresenttoanemergencydepartmentwithanALTE.ThereisnoprovenassociationbetweeninfantswithALTEpresentationsandSuddenInfantDeathSyndrome.Theepidemiologyisdifferent,andthereisnodocumentedincreasedriskofsubsequentSIDSinotherwisewellterminfantswhopresentwithanALTE.Theterm'near-missSIDS'shouldnotbeused.Whilethereisalonglistofpotentialcausesofsuchpresentations,extensiveinvestigationhasaverylowyieldandisunwarrantedinmostcases.Targetedtestingismoreappropriate.HistoryHistoryshouldbetaken,ideallyfirst-hand,frompersonswhoobservedtheinfantduringorimmediatelyaftertheevent.1.Descriptionofevent:
• Whatalertedthecaregivertoaproblem?• Behaviouralstate:awakeorasleep• Colourandcolourdistribution(cyanosis,pallor,plethora)• Tone-stiff,floppyornormal• Seizure-likeactivityorabnormalmovements,includingabnormaleyemovements
2.Circumstancesandenvironmentpriortoevent:• Relationshipoftheeventtofeedingandhistoryofvomiting• Sleepposition-prone/supine/side• Environment:natureandtypeofsleepingarrangement,chair,lounge,crib,carseat,bedaswelltype
ofbeddingandclothing3.RecentIllnessandFamilyHistory:
• Historyofcoryzaorotherupperorlowerrespiratorytractsymptomsininfantandfamilymembers• Relevantpastmedicalhistory(especiallyprematurity),immunisation• Socialfactorsincludingdrugsandmedicationtakenbycaregiverorgiventoinfant
4.Interventionsusedbycaregivers• Degreeofresuscitationrequired:gentle/vigorousstimulation,mouth-to-mouth/CPR
ExaminationAdetailedgeneralphysicalexaminationisrequired,bearinginmindthepossiblecauses.Payparticularattentionto:
• Neurologicalstateandfontanelle• Cardiorespiratoryexamination• Examineentireskinofbabyforevidenceofinjury• ConsiderfundoscopicexaminationifNAIsuspectedandconsultseniormedicalstaff(possible
ophthalmologyreview)• Abdomenformass,andinguinoscrotalabnormalities
Risk-assessmentThefollowingcriteriasuggestahigherriskofanunderlyingcauseormoreproblematiccourse:
• Agelessthan28days• Significantprematurity• Significantpriormedicalillness• Clinicallyunwelllooking.• Recurrenteventsbeforepresentation• Moresevere/prolongedALTEsymptoms
PossibleCausesItiscommonfornospecificdiagnosistobemadeafterevaluationandaperiodofobservation.Exaggeratedphysiologicalairwayprotectionreflexesisthemostcommonexplanation(readmore)OccasionallytheALTEisthefirstsignofadevelopingviralrespiratoryinfection,withmoretypicalcoryzalillnessorbronchiolitisappearinginsubsequentdays.Muchlesscommon,butpotentiallymoreseriouscausesinclude:
• Childabuse(shakenbaby,drugoverdose,Munchausenbyproxysyndromeorintentionalsuffocation)• Infection:Pertussis,pneumonia,meningitis,septicaemia• Airwayobstruction:congenitalabnormalities,infection,hypotonia• Abdominal:intussusception,strangulatedhernia,testiculartorsion• Metabolicproblems:hypoglycaemia,hypocalcaemia,hypokalaemia,otherinbornerrorsof
metabolism• Cardiacdisease:congenitalheartdisease,arrhythmias,vascularring,prolongedQT• Toxin/Drugs:accidentalornon-accidental• Neurologicalcauses:headinjury,seizures,infections,cerebralmalformationsetc.
InvestigationsInapreviously-wellterminfantwithaclearhistoryofALTEsymptomstemporallyrelatedtofeeding,thediagnosticyieldofinvestigationsisverylow.Investigationsforthisgroupareoftennotnecessary.Forpatientswithmoresevereepisodes,orthosewithoutthebenignclinicalpictureoutlinedabovethefollowinginvestigationsarereasonable:
• Fullbloodcountanddifferential• Urea&electrolytes,bloodglucose,• Nasopharyngealaspirateforviruses&pertussis.• ECG(measureQTinterval)
Iffebrile-alsofollowtheusualapproachtothefebrileinfantOtherinvestigationswhichmaybeconsideredinselectedcases:
• Investigationsforoccultfeaturesofnon-accidentalinjurysee• Metabolic:lactate,ammonia,acylcarnitineprofile• EEG• CThead• Holtermonitoring• Urinetoxicology/Metabolicscreen
InvestigationsforGastro-oesophagealrefluxareoftenunhelpfulseeManagementThismayincludeinitialresuscitation,and/ormanagementofanyidentifiedunderlyingaetiologyforthepresentation(egbacterialinfection,NAI)Needforadmission:Term-babieswithmoreminorpresentations(especiallyfeed-related),whoarewellonexamination,andwhoseparentscanbeappropriatelyreassuredandeducatedtoreturniftheyhavefurtherconcerns,maybedischargedwithrecommendationforearlyfollow-upwiththeirGPorapaediatrician.Inpracticemostbabieswiththispresentationareadmittedforobservation.Follow-upClosefollow-uppost-dischargeisrecommended,againlargelyforhelpingwithparentalanxiety.