
Platelet-Rich Plasma: The PAW Classification Systemorthodoc.aaos.org/WilliamFBennettMD/PRP_The PAW...
14
Level V Evidence Platelet-Rich Plasma: The PAW Classification System Jeffrey M. DeLong, B.Sc., Ryan P. Russell, M.A., and Augustus D. Mazzocca, M.S., M.D. Abstract: Platelet-rich plasma (PRP) has been the subject of hundreds of publications in recent years. Reports of its effects in tissue, both positive and negative, have generated great interest in the orthopaedic community. Protocols for PRP preparation vary wide!)' between authors and are often not well documented in the literature, making results difficult to compare or replicate. A classification system is needed to more accurately compare protocols and results and effectively group studies together for meta-analysis. Although some classification systems have been proposed, no single system takes into account the multitude of variables that determine the efficacy of PRP. In this article we propose a simple method for organizing and comparing results in the literature. The PAW classification system is based on 3 components: (1) the absolute number of Platelets, .(2) the manner in which platelet Activation occurs, and (3) the presence or absence of White cells. By analyzing these 3 variables, we are able to accurately compare publications. D espite the promising effects of platelet-rich plasma (PRP) therapy, most studies conducted have lacked accurate measurements and documentation of the PRP components and delivery methods used. This lack of standardization and consistency is prevalent throughout the literature and has frustrated attempts to compare results between articles. To determine the efficacy of PRP from system to system and patient to patient, the PRP components and the means by which they are delivered to the target tissue site should be identified and documented.1 Without these fundamental prerequisites, From the Medical University of South Carolina (J.M.D.), Charleston, South Carolina; and Department of Orthopaedic Sur- gery, University of Connecticut (R.P.R., A.D.M.), Farmington, Conneciicut, U.S.A. The authors report the following conflict of interest in relation to this article: A.D.M. received research support and is a consultant for Arthrex, Inc., Naples, Florida. Received March 20, 2012; accepted April 25, 2012. Address correspondence to Augustus D. Mazzccca, M.S., M.D., Department of Orthopaedic Surgery, University of Connecticut, Med- ical Arts and Research Building, Room 4017, 263 Farmington Ave, Farmington, CT 06034-4037,' U.S.A. E-mail: admazzocca@ yahoo, com © 2012 by the Arthroscopy Association of North America 0749-8063/12184/$36.00 http://dx.doi.Org/10.1016/j.anhro.2012.Q4.148 the evolution of PRP as a safe and effective treatment for orthopaedic disorders may not progress efficiently. IDENTIFYING CONTENT OF PRP Several essential factors exist that need to be identified to adequately determine the effects of PRP treatment. • The most essential factor is to ensure accurate and definitive concentration measurements of platelets. Without precise quantification of the cellular compo- nents, validation and accurate comparison of studies will remain extremely difficult, ultimately impeding dis- covery of optimum dosing. Many studies published in the recent literature lack this most basic requirement. • The presence or absence of platelet activators, as well as the type of activator used, is another important element requiring documentation. The way in which the platelets are applied to the tissue will undoubtedly affect the response of the tissue. For example, an exogenous platelet activator may be necessary to gen- erate a clot in certain procedures, whereas endogenous platelet activation without the use of an external clot- ting factor may be ideal in other indications. • Whether the administered PRP treatment includes highly concentrated leukocytes above baseline Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 28, No 7 (July), 2012: pp 99S-I009
Transcript of Platelet-Rich Plasma: The PAW Classification Systemorthodoc.aaos.org/WilliamFBennettMD/PRP_The PAW...

Level V Evidence
Platelet-Rich Plasma: The PAW Classification System
Jeffrey M. DeLong, B.Sc., Ryan P. Russell, M.A., and Augustus D. Mazzocca, M.S., M.D.
Abstract: Platelet-rich plasma (PRP) has been the subject of hundreds of publications in recent years.Reports of its effects in tissue, both positive and negative, have generated great interest in theorthopaedic community. Protocols for PRP preparation vary wide!)' between authors and are oftennot well documented in the literature, making results difficult to compare or replicate. A classificationsystem is needed to more accurately compare protocols and results and effectively group studiestogether for meta-analysis. Although some classification systems have been proposed, no singlesystem takes into account the multitude of variables that determine the efficacy of PRP. In this articlewe propose a simple method for organizing and comparing results in the literature. The PAWclassification system is based on 3 components: (1) the absolute number of Platelets, .(2) the mannerin which platelet Activation occurs, and (3) the presence or absence of White cells. By analyzingthese 3 variables, we are able to accurately compare publications.
Despite the promising effects of platelet-rich plasma(PRP) therapy, most studies conducted have lacked
accurate measurements and documentation of the PRPcomponents and delivery methods used. This lack ofstandardization and consistency is prevalent throughoutthe literature and has frustrated attempts to compareresults between articles. To determine the efficacy ofPRP from system to system and patient to patient, thePRP components and the means by which they aredelivered to the target tissue site should be identified anddocumented.1 Without these fundamental prerequisites,
From the Medical University of South Carolina (J.M.D.),Charleston, South Carolina; and Department of Orthopaedic Sur-gery, University of Connecticut (R.P.R., A.D.M.), Farmington,Conneciicut, U.S.A.
The authors report the following conflict of interest in relation tothis article: A.D.M. received research support and is a consultantfor Arthrex, Inc., Naples, Florida.
Received March 20, 2012; accepted April 25, 2012.Address correspondence to Augustus D. Mazzccca, M.S., M.D.,
Department of Orthopaedic Surgery, University of Connecticut, Med-ical Arts and Research Building, Room 4017, 263 Farmington Ave,Farmington, CT 06034-4037,' U.S.A. E-mail: admazzocca@yahoo, com
© 2012 by the Arthroscopy Association of North America0749-8063/12184/$36.00http://dx.doi.Org/10.1016/j.anhro.2012.Q4.148
the evolution of PRP as a safe and effective treatment fororthopaedic disorders may not progress efficiently.
IDENTIFYING CONTENT OF PRP
Several essential factors exist that need to be identifiedto adequately determine the effects of PRP treatment.
• The most essential factor is to ensure accurate anddefinitive concentration measurements of platelets.Without precise quantification of the cellular compo-nents, validation and accurate comparison of studieswill remain extremely difficult, ultimately impeding dis-covery of optimum dosing. Many studies published inthe recent literature lack this most basic requirement.
• The presence or absence of platelet activators, as wellas the type of activator used, is another importantelement requiring documentation. The way in whichthe platelets are applied to the tissue will undoubtedlyaffect the response of the tissue. For example, anexogenous platelet activator may be necessary to gen-erate a clot in certain procedures, whereas endogenousplatelet activation without the use of an external clot-ting factor may be ideal in other indications.
• Whether the administered PRP treatment includeshighly concentrated leukocytes above baseline
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 28, No 7 (July), 2012: pp 99S-I009
PRESIDENTIAL ADDRESS 997
cepted the responsibility to transfer the orb with pas-sion and determination, ensuring an even brighter andstronger future for those that follow.
I'll share a few final thoughts in closing.-A numberof individuals have come up to me and stated withconfidence that, "one of the best days of your life isthe day you become immediate past president!" Withone exception, nothing could be further from the truthfor me. This has been the most enjoyable and reward-ing year of my professional career. The opportunity towork with colleagues of great talent and a desire togenuinely contribute to the betterment of the organi-zation has been truly inspiring. What more could oneask for than to roll up your sleeves daily with friendswho want nothing more than to serve our organizationwell? I mentioned one exception—my stepping downmeans that Dr. Nick Sgaglione assumes the presi-dency of The Arthroscopy Association of NorthAmerica. I could not be more excited for his tenure.He is a man of immense talent, great character, and isone of the most outstanding natural leaders I have evermet. Dr. Thomas Byrd will follow Nick and is a man
wise beyond his years, respected throughout the worldfor his contributions to hip arthroscopy, and is theepitome of a "Southern Gentlemen." This organiza-tion could not be in better hands.
So, I am able to stand before you today and makethree statements with great certainty. First, the LadyAANA is in robust and radiant health. Secondly, thetrade winds are fair for the continued exploration foreducational treasures. Finally, there is no finer groupof individuals to transfer the golden orb of AANA'sculture to the next generation of young orthopaedicsurgeons than those of you sitting in this audiencetoday!
I offer my sincere thanks to you for the opportunityto serve as your president this past year.
RICHARD L. ANGELO, M.D.
Address correspondence and reprint requests to Richard L. Angela,M.D., 12911 120th Ave NE, Bldg H, Suite 210, Kirldand, WA 98034.E-mail: [email protected].
PLATELET-RICH PLASMA CLASSIFICATION 999
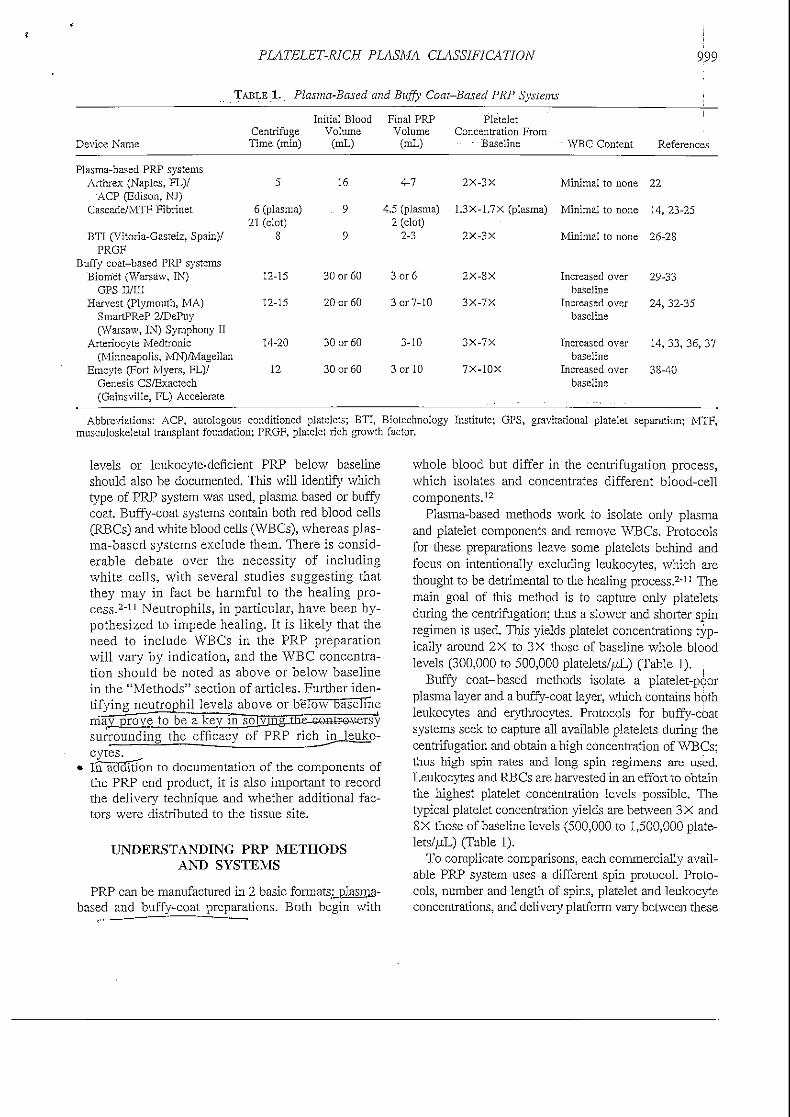
TABLE 1. Plasma-Based and Buffy Coat-Based PRP Systems
Device Name
Plasma-based PRP systemsArthrex (Naples, FL)/
ACP (Edison, NJ)Cascade/MTF Fibrinet
BTI (Vitoria-Gasteiz, Spain)/PRGF
Buffy coat-based PRP systemsBiomet (Warsaw, IN)
GPS II/IIIHarvest (Plymouth, MA)
SmartPReP 2/DePuy(Warsaw, IN) Symphony II
Arteriocyte Medtronic(Minneapolis, MN)/Magellan
Emcyte (Fort Myers, FL)/Genesis CS/Exactech(Gainsville, FL) Accelerate
CentrifugeTime (min)
5
6 (plasma)21 (clot)
S
12-15
12-15
14-20
12
Initial BloodVolume
(mL)
16
9
9
30 or 60
20 or 60
30 or 60
30 or 60
Final PRPVolume
(mL)
4-7
4.5 (plasma)2 (clot)
2-3
3 or 6
3 or 7- 10
3-10
3 or 10
PlateletConcentration From
• Baseline
2X-3X
1.3X-1.7X (plasma)
2X-3X
2X-SX
3X-7X
3X-7X
7X-10X
WBC Content
Minimal to none
Minimal to none
Minimal to none
Increased overbaseline
Increased overbaseline
Increased overbaseline
Increased overbaseline
References
22
14, 23-25
26-28
29-33
24, 32-35
14, 33, 36, 37
3S-40
Abbreviations: ACP, autologous conditioned platelets; BTI, Biotechnologymusculoskeletal transplant foundation; PRGF, platelet rich growth factor.
Institute; GPS, gravitational platelet separation; MTF,
levels or leukocyte-deficient PRP below baselineshould also be documented. This will identify whichtype of PRP system was used, plasma based or buffycoat. Buffy-coat systems contain both red blood cells(RBCs) and white blood cells (WBCs), whereas plas-ma-based systems exclude them. There is consid-erable debate over the necessity of includingwhite cells, with several studies suggesting thatthey may in fact be harmful to the healing pro-cess.2'11 Neutrophils, in particular, have been hy-pothesized to impede healing. It is likely that theneed to include WBCs in the PRP preparationwill vary by indication, and the WBC concentra-tion should be noted as above or below baselinein the "Methods" section of articles. Further iden-tifying neutrophil levels above or below bas'elmem'a^proye^to be a key IFl;gJvjn.gI^surrounding the efficacy of PRP richjr^ieukp-cytes.
• IiTa33ItIon to documentation of the components ofthe PRP end product, it is also important to recordthe delivery technique and whether additional fac-tors were distributed to the tissue site.
UNDERSTANDING PRP METHODSAND SYSTEMS
PRP can be manufactured in 2 basic formats: plasma-based and buffy-coat preparations. Both begin with
whole blood but differ in the centrifugation process,which isolates and concentrates different blood-cellcomponents.12
Plasma-based methods work to isolate only plasmaand platelet components and remove WBCs. Protocolsfor these preparations leave some platelets behind andfocus on intentionally excluding leukocytes, which arethought to be detrimental to the healing process.2"11 Themain goal of this method is to capture only plateletsduring the centrifugation; thus a slower and shorter spinregimen is used. This yields platelet concentrations typ-ically around 2X to 3X those of baseline whole bloodlevels (300,000 to 500,000 platelets//^) (Table 1).
Buffy coat-based methods isolate a platelet-poorplasma layer and a buffy-coat layer, which contains bothleukocytes and erythrocytes. Protocols for buffy-coatsystems seek to capture all available platelets during thecentrifugation and obtain a high concentration of WBCs;thus high spin rates and long spin regimens are used.Leukocytes and RBCs are harvested in an effort to obtainthe highest platelet concentration levels possible. Thetypical platelet concentration yields are between 3 X and8X those of baseline levels (500,000 to 1,500,000 plate-lets//^) (Table 1).
To complicate comparisons, each commercially avail-able PRP system uses a different spin protocol. Proto-cols, number and length of spins, platelet and leukocyteconcentrations, and delivery platform vary between these
1000 J. M. DELONG ET AL.
devices, making no 2 PRP products identical (Table 1).These variances lead to different amounts of. anabolicand catabolic proteins released to the target tissues afterinjection.13 For instance, Castillo et al.14 tested 3 differ-ent PRP separation systems, and each system yielded asimilar platelet concentration (approximately 600,000platelets//xL) and RBC, active transforming growth fac-tor (TGF) j3I, and fibrinogen levels. However, eachsystem produced significantly different levels of platelet-derived growth factor (PDGF) AB, PDGF-BB, vascularendothelial growth factor (VEGF), and WBC concentra-tion. Although the effects of these bioactive factors ontissue were not tested, it is possible that these variationscould result in considerable and dramatically distincteffects on healing.12 Lack of standardization of PRPpreparations may therefore lead to inconsistent results inthe literature.15
Additives also alter the content and effect of PRP.For example, anticoagulants and local jmesthetics alterthe pH of PRP; understanding the effect of this alter-ation on tissue response is important. Variations in pHhave been shown to affect in vitro proliferation, andconsideration must be given to the desired responsebefore choosing to mix PRP with an additive.16*17
Local anesthetics, in particular, appear to jjroduce anegative; effect_6ii~PRPjre^ment in_yitro _and_ shouldie avoided when possible.17-18
PRP can even be altered by the metals used in medicaldevices or implants as well as the centrifuge material.Tanaka et al.19 studied the effects that various metals hadon platelet adhesion. The study found that platelet adhe-sion and aggregation can both be inhibited and enhancedby different types of metal. Test tube materials are alsoimportant. Michelson20 reported in his comprehensivebook on platelets that polypropylene .tubes are.superior toeither polystyrene or polycarbonate when used.for plate-let preparation and/or storage. In addition, he noted thatuncoated glass may artificially activate platelets and af-fect results.20 A study conducted by Grottum et al.21
determined the effect of polystyrene particles on PRP.Incubation of PRP with polystyrene particles inducedsurface contact between platelets and particles, uptake ofparticles, and changes in platelet morphology. After in-jection into rabbits, Grottum et al, identified increasedplatelet aggregation, which may have resulted from areduction in platelet surface charge due to interactionwith polystyrene.21 For these reasons, it is imperativethat the protocol chosen to manufacture PRP in eachstudy be strictly adhered 'to, and materials cannot bereefy substituted.
UNDERSTANDING CELLULAR COMPONENTS
Platelet Concentration
Few studies have compared the healing effects ofdifferent PRP platelet concentrations for the sameindication.14*41 This may prove to be the most signif-icant aspect in identifying the true effectiveness ofPRP and in choosing the proper protocol.
Low: Less Than IX (Less Than Baseline): Plate-let concentrations below baseline may not allow for asufficient cellular response.42 Often used as a control,platelet-poor plasma has only shown the sk'ghtest benefit.
Moderate: Greater Than Ix to Less Than 4x(Greater Than Baseline to 750,000 platelets//*!,):Plasma-based PRP systems typically produce plateletconcentrations between baseline and 3X baseline. Theabsolute platelet number obtained by this method isgenerally equal to or less than 750,000 platelets/jtL.
In vitro, in vivo, and clinical studies have beenconducted and published by Anitua and Sanchez, aswell as their colleagues, showing jhe.effectivenessof PRP with a platelet concentration of 2X to3 X .26.23.43-49 Sanchez et al.28 injected exogenouslyactivated PRP with a 3X platelet concentration intosurgically repaired human Achilles tendons. Theyfound significant improvement and an earlier return tosports as compared with the control group. The sameresearchers performed an uncontrolled retrospectivecase study in which they treatedj_6 aseptic nonunionsintraoperatively with a moderate PRP platelet concen-tration (2X to 3X) with a bone, allograft and anautologous fibrin membrane. All subjects went on tobony union.47 Another study showed enhanced tendongraft ligamentization during anterior cruciate ligamentsurgery.41 Histology at the 6- and 24-month marksshowed increased connective tissue remodeling whencompared with the untreated grafts.
Anitua-and Sanchez are not the only researchers whohave"shown positive-responses'to PRP in the 2X to 3Xbaseline range. Graziani et al.50 evaluated the effect of ,PRP on the function of osteoblasts and fibroblasts^Aftera 72-hour incubation period, the 2.5X (approximately55MjOO_piatelets//xL') PPJ^grnup-resulted in a-statisti-cal 1 y-sigfiincantrfncrectsti in cblr count[orrosteubl;ibU> and
control. The authors concluded, that a platelet concentra-tion gf 2,5X^y-ialded-ep^rmal rcsnlteT-feraddition. Torri-celli et al.51 evaluated the effect of PRP for the treatmentof musculoskeletal overuse injuries in competitionhorses. With the placebo effect nullified, they found thatPRP with a platelet concentration of 750,000 plate-

PLATELET-RICH PLASMA CLASSIFICATION 1001
lets/,uL accelerated healing and allowed an earlier returnto competition.
High: 4X to 6x (>750,000 to 1,800,000 platelets/juiL): Literature suggests that successful buffy coat-based PRP treatments typically produce platelet con-centrations greater than 3 X and primarily in the 4X to6X range.14-24*32 The absolute platelet number is gen-erally greater than 750:000 to 1,800,000 platelets/^L.Successful reports in this range include that of He etal.,52 who found accelerated bone healing with PRPplatelet concentrations of approximately 4X to 5Xversus controls in patients who underwent transforma-tional lumbar interbody fusions. An in vivo rabbitstudy conducted by Weibrich et al.^ analyzed theeffect of platelet count in PRP on boae_r&gsneration.They found significant bone regeneration with a plate-let concentration up to 6X (1,729,000 platelets//xL).Giusti et al.54 studied endothelial cells and found thatthe optimal concentration for cell proliferation was
_ _Super: Greater Than 6x (>1,800,000 platelets/
:- Concenfaations— too— h-igb__-rriay h^dgjrjmeiital-Overwhelming the healing milieu with an excessiveamount of platelets may lead_tojirjoj}tasis, growth faster
•preceptor downregulation, and receptor desensitization,whicrTrnay result in a paradoxical inhibitory effect.42™5
Several studies have shown this. ..Weibrich et al.53
showed that highly concentrated platelets (6X to 11X)( I,845,000jo_3.2n0.n00 platelets/uLlJiad-aiLinhibitorveffect on osteoblast activity when compared wjth lowerconcentrations. In a study on alveolar bone cells, Choi etal.56 concluded -that. .the. high, concentration of plateletsused may have resulted in adverse effects on bonegrowth.
Platelet Count
A single individual's platelet count can vary con-siderably on different days.18 There is also a- signifi-cant variation in platelet count-between individuals.For example, the normal platelet count varies between150000 and 350,000 platejels/j^L. An individual witha low normal count receiving PRP with a concentra-tion of 1 million platelets//xL would see an approxi-mate 6.5 X increase. Arnndividual with a high normalcount receiving PRP with a concentration of 1 million
would seean approximate 3X increase.Variations in an inch victual's baseline platelet countlead to inconsistency in quantifying a "fold" increase,making PRP products different between both individ-uals and treatments, even when identical protocols areused. For this reason, documenting both the absolute
number of platelets per microliter contained in thePP^_ preparation., and Jhe. individual's own plateletcount on the day of treatment is important in compar-ing effectiveness.- • - .. . ......
Centrifugation force, duration, and frequency arealso important elements that may result in varyingplatelet concentrations and alteration of platelet mor-phology.57 Jo et al.58 determined optimum PRP gelformation by varying time and gravitational forcesduring centrifugation. The optimal conditions werefound to be 900g for 5 minutes and 1,500# for 15minutes for the separating centrifugation step and thecondensing centrifugation step, respectively. In addi-tion, Barrett and Erredge59 found that the number ofcentrifugations varied platelet capture significantly.They determined that a single centrifugation spin pro-duced 1,254,000 platelets//xL whereas a double spinproduced 2,017,000 platelets//uL.
The process for measuring platelet count may con-tribute to variation as well. Most hematology analyzersystems are designed to operate in ranges found withinwhole blood, and PRP may exceed the upper limit ofthe linear range of platelets that can be counted. Inaddition, adequate resuspension of the PRP and propersample preparation are required for accurate plateletcounts. Platelet clumping or lack of even distributionmay result in inaccuracies.1 (
Woodell-May et al.1 determined the average plateletcount to be significantly less when samples were mea-sured immediately after preparation of the PRP thanwhen samples were resuspended on a rocker (P < .05).This study suggests that for accurate platelet counts to beachieved, the_entire PRP sample must be remove^ andallowed to sit on a rocker for ajjeast 5 minutes beforecounting. Furthermore, this study recommends usingmanual mode in the hematology analyzer because auto-matic counting .modes are. more Jikely to allow the sam- 'pie to settle, reducing the absolute platelet count.32
Leukocyte Content
The effect of highly concentrated WBCs containedwithin PRP preparations60 has been hotly debated. PRPsystems that use a buffy coat contain an increased concen-tration of WBCs above baseline levels, whereas plasma-based methods do not. Although normal levels of WBCshave a positive immunomodulatory effect, heightenedlevels in some PRP preparations may have a deleteriousimpact. Literature suggests that excessive leukocytes,specifically neutrophils, may be contributing to theseundesired results.zrn~Ho\*t'everrth'5"efficaciy
treatments still remains unclear and may be
1002 J. M. BELONG E
dependent on indication. PRP used to treat opewounds and prevent infection may rcauirejjupraiigf-mal WBC levelg,61-64 whereas^PRP used to minimize
WBCcontent should always be documented in any classifi-cation system.
UNDERSTANDING DELIVERY METHOD
Activation Methods
Platelets can be activated endogenously or throughthe addition of an exogenous clotting factor to anycommercially available system. Each type of activatormay produce varying effects and significantly influ-ence growth factor kinetics. Accurately documentingthe deliver}' method and activation scheme used isanother key to a successful classification system.
Exogenous: Exogenous activation results in rapidcoagulation of platelets and quick clot formation. Forthis reason, clots formed in this manner are best ap-plied manually to the tissues, rather than administeredby injection. They often can be sutured to repairs.Proposed benefits of a preformed clot include theability to more accurately localize growth factor re-lease, as well as decreased diffusion when used intra-articularly. Advocates of preclotted PRP also theorizea more sustained growth factor release because growthfactors are thought to elute from the clot slowly overthe span of several days. The effect of exposure of theclot to synovial fluid has not been well documented,and it is possible that the clot is quickly dissolved inthe joint.66-67
Endogenous: The addition of external clotting fac-tors to PRP may not be needed to significantly activateplatelets. Not only will tissue collagen cause activa-tion of platelets but simple_agitation jjf p]atelets? suchas centrifugation, as well as needle-induced bleedingduring PRP injection, may provide the appropriateendogenous clotting factors needed for activation. En-dogenous activation has the potential for slower ag-gregation of platelets and release of growth factors byallowing collagen within the tissue to operate as theactivator providing a natural release pattern.68 Clotformation occurring after injection provides the ben-efit of administration through a needle and may allowa more precise delivery to, and within, the targettissue.
Platelet Activators
Thrombin: Thrombin causes rapid aggregation ofplatelets. Rapid activation may lead to excessive con-
densing of the fibrin matrix and significant retraction.of cloTs, which m^nilTiriierior with respect to cellmigration and growth factor enmeshment when com-pared with less condensed physiological activa-tion.69'72 A rapid activation may also lead to a de-crease in the total amount of growth factors availableat the tissue site over time.short half-life minutes d-will^&^ade-beforeadditional tissue receptors become available if they arenot immediately .used upon release from a platelet.68-73
Additional potential negative effects include an immune-
tion against bovine-derived thrombin.68
CatctmTTT^hloride: Calcium chloride has beenadded exogenously to PRP preparation in lieu of bo-vine thrombin and may result in the formation of a lesscondensed fibrin matrix. The fibrin matrix may pro-vide a trapping mechanism for platelets, resulting insmaller amounts of thrombin formation endogenously,allowing a slower release of growth .factors over a7-day period, which may enhance cell migration andhealing .7^-74;?? Injections. containing-cakJAjm-Gbloadehave a low pH amTcause significantLpaJn and a burn-ing . sensation .to the . patient.
Calcium Chloride Plus Thrombin: Calcium chlo-ride is a citrate inhibitor and allows the plasma tocoa^uiaLe^_an.dJ±LrQnibin causes fibrin to polymerizeinto, an insoluble gel: platelets then degranulate andrelease growth factors.57 When calcium chloride andthrombin are combined with PRP a gel or _ .scaffoldmatrix is produceo7~TEs^^nmy^)ffer_the benefit of a
Type I Collagen: Endogenous type I collagen hasbeen found to be equally effective as thrombin inactivating platelets and stimulating the release ofgrowth factors. In an in vitro study of PRP fromhuman donors, clotting was performed with type Icollagen or bovine thrombin. Type I collagen resultedin similar release of PDGF and VEGF but a moreextended and overall greater release of TGF-/3 thanthrombin. Clots formed by use of type I collagen alsoexhibited far less retraction than those formed withbovine thrombin. In addition, both type I collagen andbovine thrombin stimulated similar release of PDGF andVEGF between days 1 and 10, whereas thrombin re-sulted in a greater release of TGF-/3 during days 1 to 5 .7S
Delivery Technique
The technique used during delivery of PRP is an-other fundamental variable that should be understoodand addressed. Individual tissues may have ideal an-
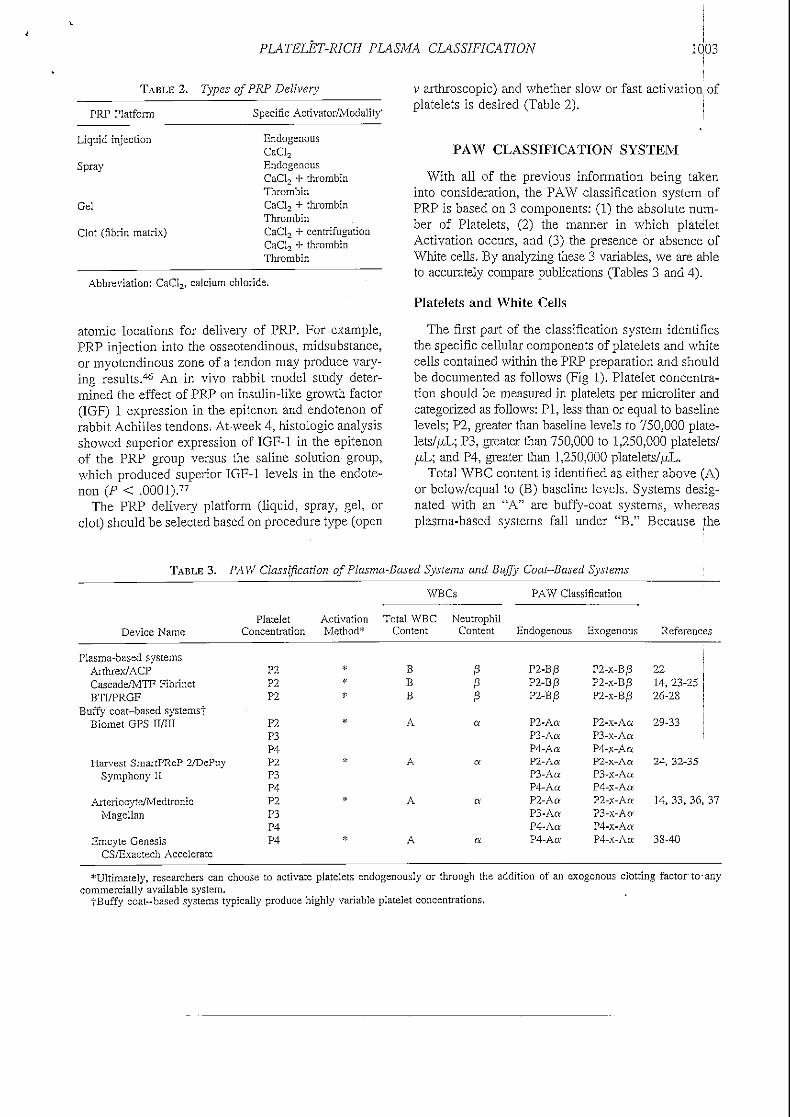
PLATELET-RICH PLASMA CLASSIFICATION 1003
TABLE 2. Types ofPRP Delivery
PRP Platform Specific Activator/Modality'
Liquid injection
Spray
Gel
Clot (fibrin matrix)
EndogenousCaCI2
EndogenousCaCl2 + thrombinThrombinCaCl2 + thrombinThrombinCaCl2 + centrifugationCaCl2 + thrombinThrombin
Abbreviation: CaCU. calcium chloride.
atomic locations for delivery of PRP. For example,PRP injection into the osseotendinous, midsubstance,or myotendinous zone of a tendon may produce vary-ing results.46 An in vivo rabbit model study deter-mined the effect of PRP on insulin-like growth factor(IGF) 1 expression in the epitenon and endotenon ofrabbit Achilles tendons. At-week 4, histologic analysisshowed superior expression of IGF-1 in the epitenonof the PRP group versus the saline solution group,which produced superior IGF-1 levels in the endote-non (P < .0001).77
The PRP deliver}' platform (liquid, spray, gel, orclot) should be selected based on procedure type (open
y artriroscopic) and whether slow or fast activation ofplatelets is desired (Table 2).
PAW CLASSIFICATION SYSTEM
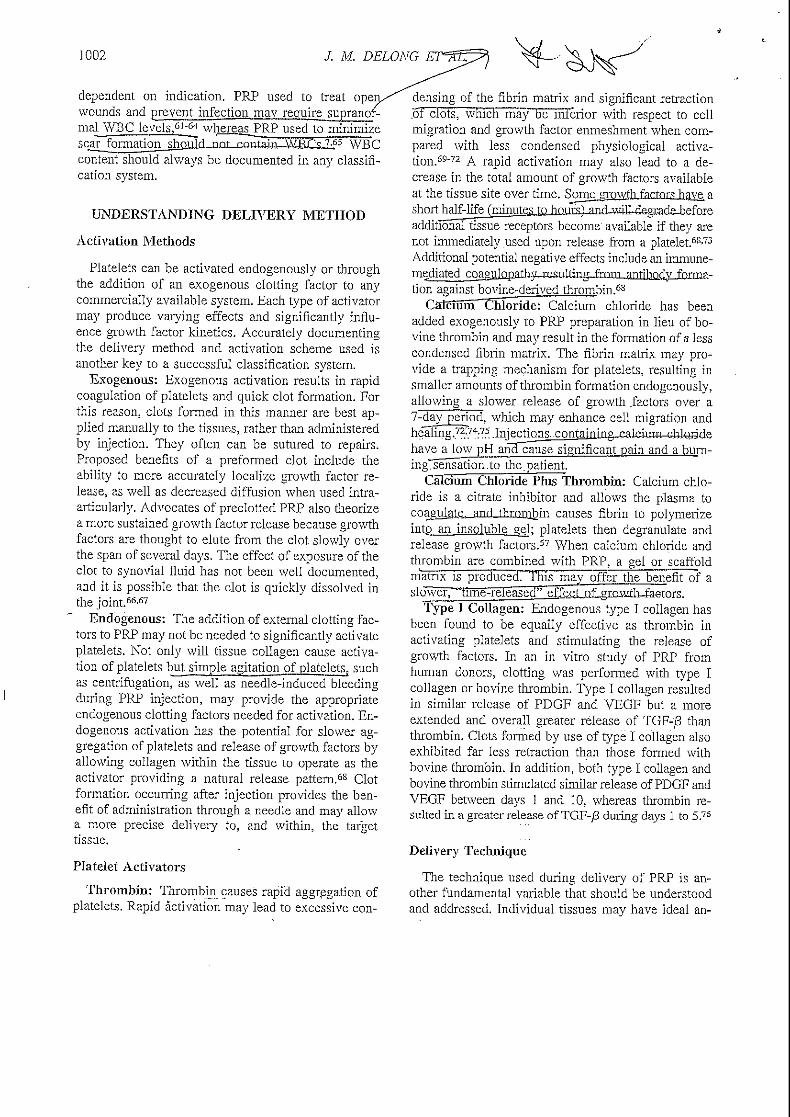
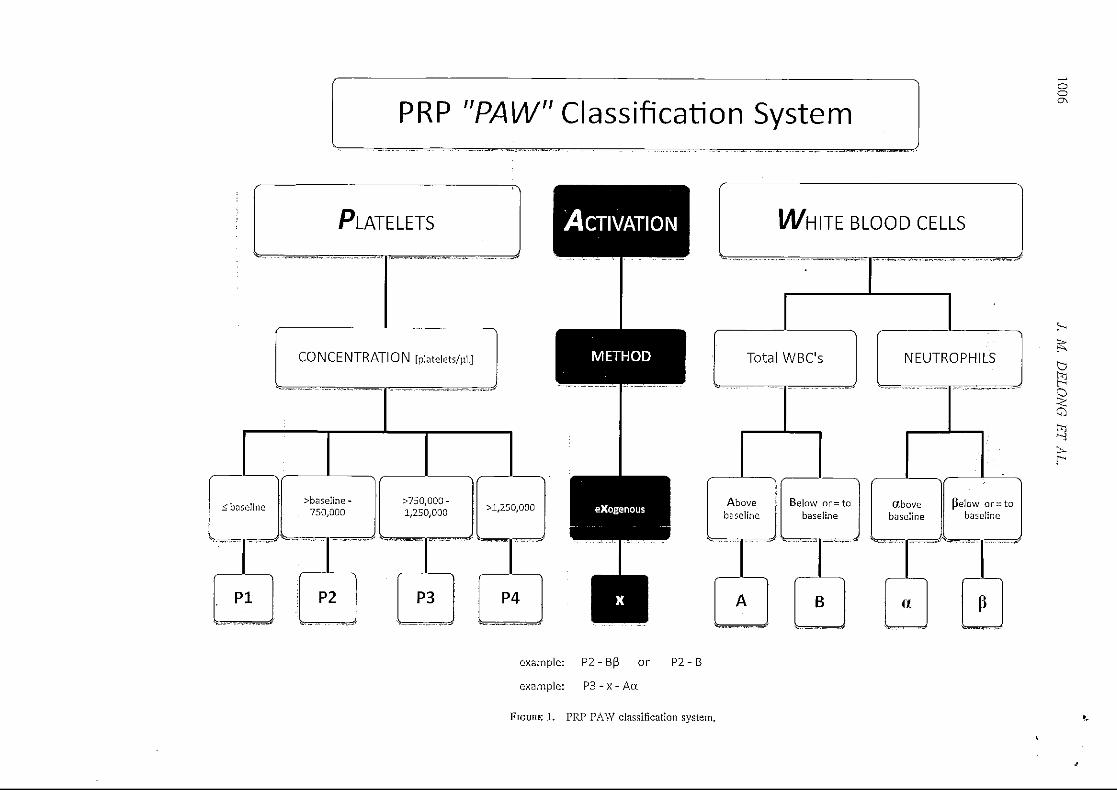
With all of the previous information being takeninto consideration, the PAW classification system ofPRP is based on 3 components: (1) the absolute num-ber of Platelets, (2) the manner in which plateletActivation occurs, and (3) the presence or absence ofWhite cells. By analyzing these 3 variables, we are ableto accurately compare publications (Tables 3 and 4).
Platelets and White Cells
The first part of the classification system identifiesthe specific cellular components of platelets and whitecells contained within the PRP preparation and shouldbe documented as follows (Fig 1). Platelet concentra-tion should be measured in platelets per microliter andcategorized as follows: PI, less than or equal to baselinelevels; P2, greater than baseline levels to 750,000 plate-lets/juL; P3, greater than 750,000 to 1,250,000 platelets/juL; and P4, greater than 1,250,000 platelets/pL.
Total WBC content is identified as either above (A)or below/equal to (B) baseline levels. Systems desig-nated with an "A" are buffy-coat systems, whereasplasma-based systems fall under "B." Because the
TABLE 3. PAW Classification of Plasma-Based Systems and Buffy Coat-Based Systems
WBCs PAW Classification
Device NamePlatelet Activation Total WBC Neutrophil
Concentration Method* Content Content Endogenous Exogenous References
Plasma-based systemsArthrex/ACPCascade/MTF FibrinetBTI/PRGF
Buffy coat-based systemsfBiomet GPS II/III
Harvest SmartPReP 2/DePuySymphony II
Arteriocyte/MedtronicMagellan
Emcyte GenesisCS/Exactech Accelerate
P2P2P2
P2P3P4P2P3P4P2P3P4P4
* B /3 P2-B0* B /3 P2-Bj3'* B p P2-B/3
* A a P2-AaP3-AaP4-Aa
* A a P2-AaP3-Aa:P4-Aa
* A a P2-A«P3-AaP4-Ao;
* A a P4-Aa
P2-X-B/3P2-X-B/3P2-X-B/3
P2-x-AaP3-x-AaP4-x-AaP2-x-Aa
P3-x-AaP4-x-AaP2-x-AaP3-x-AaP4-x-AaP4-x-Aa
2214, 23-2526-2S
29-33
24, 32-35
14, 33, 36, 37
38-40
""Ultimately, researchers can choose to activate platelets endogenously or through the addition of an exogenous clotting factor to-anycommercially available system.
|Buffy coat-based systems typically produce highly variable platelet concentrations.
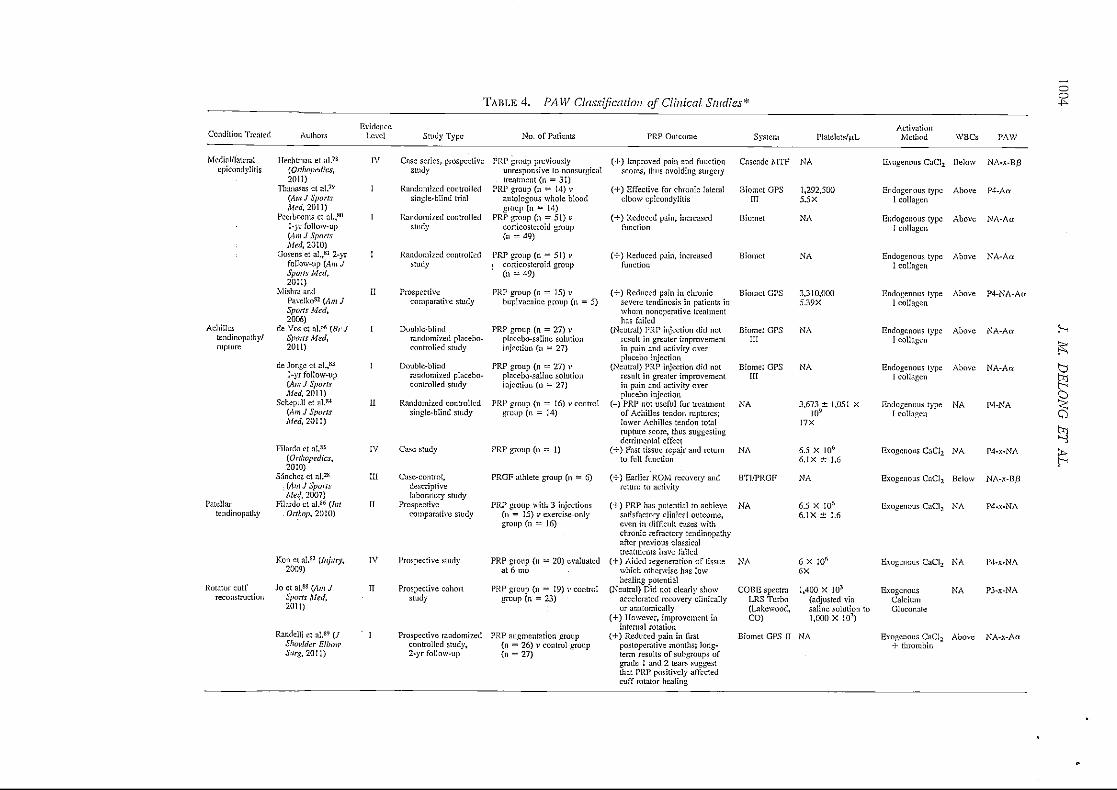
TABLE 4. PAW Classification of Clinical Studies*
Condition Treated
Medial/lateralepicondylitis
Achillestendinopflthy/rupture
Patellartendinopathy
Authors
Hechtman et al.7S
{Orthopedics,2011)
Thanasas ct al 79
(Am J SportsAM/, 2011)
Peerbooms el a I.,80
1-yr follow-up(Am J SportsMed, 2010)
Gosens et al.,31 2-yrfollow-up (Am JSports Med,2011}
Mishra andPavelko81 (Am JSports Med,2006)
de Vosetal.*6 (BrJSpans Med,2011)
de Jnngc ct al.,83
1-yr follow-up(Am J SportsMed, 2011)
Schepull et al «(Am J SporlsAM;, 201 1)
Filardo ct al.85
(Orthopedics,2010)
Sanchez ct al.38
(Am J SportsMed. 2007)
Filardo ct al.86 (In!.Onhop, 2010}
EvidenceLevel Study Type
IV Case series, prospectivestudy
1 Randomized controlledsingle-blind trial
1 Randomized controlledStudy
I Randomized controlledStudy
II Prospectivecomparative study
I Double-blindrandomized placebo-controlled study
I Double-blindrandomized placebo-control led study
II Randomized controlledsingle-blind study
IV Case study
III Case- control,descriptivelaboratory study
11 Prospectivecomparative study
No. of Patients
PRP group previouslyunresponsive to nonsurgicaltreatment (n = 31)
PRP group (n = 14) vautologous whole bloodgroup (n = 14)
PRP group (n = 51) vcortices leroid group(n = 49)
PRP group (n = 51) i-i corti co steroid group
(n = 49)
PRP group (n = 15) vbupivacainc group (n = 5)
PRP group (n = 27) vplacebo-saline solutioninjection (n = 27)
PRP group (n = 27) vplacebo-saline solutioninjection (n — 27)
PRP group (n = 16) v controlgroup (n = 14)
PRP group (11= 1}
PRGF athlete group (n = 6)
PRP group with 3 injections(n = 15) v exercise-onlygroup (n = 16)
PRP Outcome
(+) Improved pain and functionscores, thus avoiding surgery
(+) Effective for chronic lateralelbow epicondylilis
(+) Reduced pain, increasedfunction
(•I-) Reduced pain, increasedfunction
(+) Reduced pain in chronicsevere tendinosis in patients inwhom nonoperative treatmenthas failed
(Neutral) PRP injection did notresult in greater improvementin pain and activity overplacebo injection
(Neutral) PRP injection did notresult in greater improvementin pain and activity overplacebo injection
(-} PRP not useful for treatmentof Achilles tendon ruptures;lower Achilles tendon totalrupture score, thus suggestingdetrimental effect
(+) Fast tissue repair and returnto full function
(•f) Earlier ROM recovery andreturn to activity
(+) PRP has potential to achievesatisfactory clinical outcome.even in difficult cases with
System
Cascade MTF
Biomct GPSIII
Biomel
Biomct
Biomct GPS
Biomel GPSIII
Biomel GPSIII
NA
NA
BTI/PRGF
NA
PlaleletsVL
NA
1,292.5005.5 X
NA
NA
3,310,0005.39X
NA
NA
3,673 ± 1,051 x10"
17X
6.5 X I06
6.1X ± 1.6
NA
6.5 X 10s
6.1X ± 1.6
ActivationMethod
Exogenous CaClj
Endogenous typeI collagen
Endogenous typeI collagen
Endogenous typeI collagen
Endogenous type1 collagen
Endogenous typeI collagen
Endogenous type1 collagen
Endogenous typeI collagen
Exogenous CaG2
Exogenous CaCl2
Exogenous CaCl2
WBCs
Below
Above
Above
Above
Above
Above
Above
NA
NA
Below
NA
PAW
NA-x-B/J
P4-Aa
NA-Aa
NA-Art
P4-NA-A«
NA-Aor
NA-An
P4-NA
P4-X-NA
NA-x-B/3
P4-X-NA
OO-P-
st=-fSj
bt~-<p-SQhi
t̂^t— <
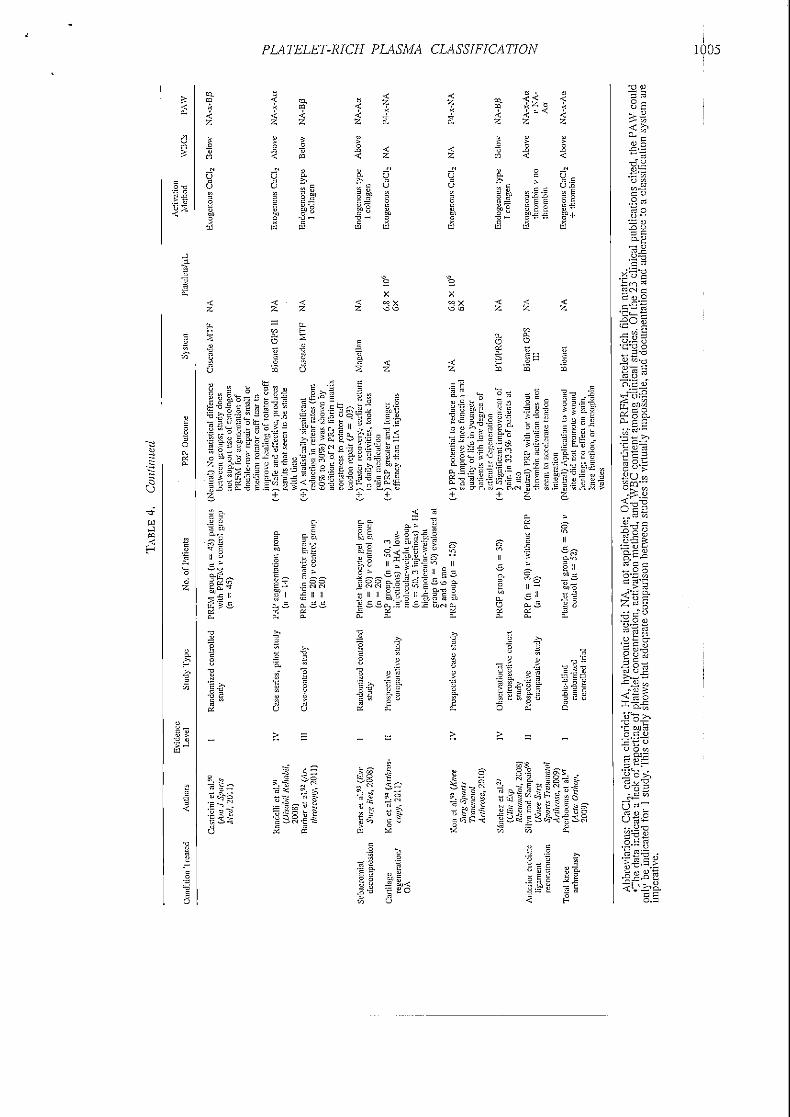
Kon et al.sj (Injury,2009)
Rotator cuff Jo et al.8S (/1m Jreconstruction Sports Med,
2011)
Randelli et al.89 (JShoulder Elbow
IV Prospective study PRP group {n = 20) evaluatedat 6 mo :
II Prospective cohon PRP group (n = 19) v controlstudy group (n = 23) -
I Prospective randomized PRP augmentation groupcontrolled study, (n = 26) v control group2-yr follow-up (n = 27)
chronic refractory tcndinopathyafter previous classicaltreatments have failed
(4-) Aided regeneration of tissuewhich otherwise has lowhealing potential
(Neutral) Did not clearly showaccelerated recovery clinicallyor anatomically
(+) However, improvement ininternal rotation
(+) Reduced pain in firstpost opera live months; long-term results of subgroups ofgrade 1 and 2 tears suggestthat PRP positively affectedcuff rotator healing
NA
COBE spectraLRS Turbo(Lake wood,CO)
6 X I0r'fix
1,400 X I03
(adjusted viasaline solution to1,000 X 103)
Exogenous CaCl2 NA 1'4-x-NA
Biomet GPS II NA
ExogenousCalciumGluconnle
Exogenous CaCl2
4- thrombin
NA P3-X-NA
Above NA-x-Aa
PLATELET-RICH PLASMA CLASSIFICATION 1005
^ ^ U os- fl 6= # L. CL
.^.25 ™ e S P S^ ~ •— ^-« -— E ^- ?
C 3,s c*H tQ
61) "g"
t: 3U C CT'^ C CU
•i
PRP "PAW" Classification Systemooo\S
ACTIVATION
METHOD
exogenous
M/HITE BLOOD CELLS
Total WBC's NEUTROPHILS
Abovebaseline
Below or-tobaseline
abovebaseline
pelow or=tobaseline
B
b
example: P 2 - B P or P2 - B
example: P 3 - x - A a
FIGURE 1. PRP PAW classification system.

PLATELET-RICH PLASMA CLASSIFICATION 1007
inclusion or exclusion of neutrophils willbecome animp ortant variableLa_gubcategory for neujroghtl counthag been createdlbr^sYstems that concentrate WBCs.If neutrophils are included in the buffy coat then_a(abp_ye) is added. If neutrophils are filtered out,J_hen /3fbelov.0 is ad4&l Thf»Tftfnr&-hiifly=f:nat systems ..willhave a designation of either Aa or A/3 in our system.
For example, a PRP preparation consisting oF900,000 platelets//nL with a total WBC and neutrophilcontent above baseline levels will be documented as
Activation Method
Ultimately, researchers can choose to activate plate-lets endogenously or through the addition of an exog-enous clotting factor to any commercially availablesystem. Endogenous activation is not given a desig-nation. However, if an exogenous external activator isused, it is documented with an x. Combining thepreviously described PRP preparation with this acti-vation method will provide the complete classifica-tion: either P3-Aa for endogenous activation or P3-x-Aa for exogenous activation.
CONCLUSIONS
PRP continues to occupy both orthopaedic literatureand the lay press, and more funding is being dedicatedto unraveling its mysteries; a simple method for com-paring published data based on the content of PRPneeds to be established. Our system offers a simple,effective method for quickly documenting the cellularcomponents and activation method used. The acronymPAW serves as a pneumonic for Platelets, Activation,and White cells, and the subcategories are thought-fully organized to enhance recall. Using a classifica-tion system will speed the process of identifying theoptimal PRP preparation for each indication and allowother investigators to replicate published data or per-form meta-analyses.
Acknowledgment: The following individuals are ac-knowledged for their substantial contribution in the devel-opment of the classification system: Bryan T. Hanypsiak,M.D., David O. Shepard, M.B.A., C.T.B.S., and Brandon L.Roller, M.D. All are employees of Arthrex, Naples, Florida.
REFERENCES
1. Woodell-May JE, Ridderman DN, Swift MJ, Higgins J. Pro-ducing accurate platelet counts for platelet rich plasma: Vali-
dation of a hematology analyzer and preparation techniquesfor counting. / Craniofac Surg 2005; 16:749-759. i
2. Brickson S, Ji LL, Schell K, Olabisi R, St Pierre Schneider B,Best TM. Ml/70 attenuates blood-borne neutrophil oxidants,activation, and myofiber damage following stretch injury.JAppl Physiol 2003;95:969-976.
3. Crinnion IN, Homer- Vanniasinkam S, Parkin SM, Gough MJ.Role of neutrophil-endothelial adhesion in skeletal musclereperfusion injury. Br J Surg 1996;83:251-254.
4. Diegelmann RF, Evans MC. Wound healing: An overview ofacute, fibrotic and delayed healing. From Biosci 2004;9:283-289.
5. Dovi JV, He LK, DiPietro LA. Accelerated wound closure inneutrophil-depleted mice. J Leukoc Biol 2003:73:448-455.
6. Gr0gaard B, Gerdin B, Reikeras 0. The polymorphonuclearleukocyte: Has it a role in fracture healing? Arch OrthopTrauma Surg 1990;109:2fi8-271.
7. Martin P, Leibovich SJ. Inflammatory cells during woundrepair: The good, the bad and the ugly. Trends Cell Biol2005; 15:599-607.
S. Schneider BS, Tiidus PM. Neutrophil infiltration in exercise-injured skeletal muscle: How do we resolve the controversy?Sports Med 2007;37:837-856.
9. Simpson DM, Ross R. The neutrophilic leukocyte in woundrepair. A study with antineutrophil serum. / din Invest 1972;51:2009-2023.
10. Toumi H, Best TM. The inflammatory response: Friend orenemy for muscle injury? Br J Sports Med 2003;37:284-286.
11. Tidball JG. Inflammatory processes in muscle injury and re-pair. Am J Physiol Regul Integr Comp Physiol 2005;288:R345-R353.
12. Redler LH, Thompson SA, Hsu SH, et al. Platelet-rich plasmatherapy: A systematic literature review and evidence for clin-ical use. Phys Spans Med 201 1;39:42-51.
13. Kon E. PRP for the treatment of cartilage defects. Presented atthe AAOS (American Academy of Orthopaedic Surgeons)Now 201 1 PRP Forum, San Diego, CA, February 14, 201 1.
14. Castillo TN, Pouliot MA, Kim HI, Dragoo JL. Comparison ofgrowth factor and platelet concentration from commercialplatelet-rich plasma separation systems. Am J Sports Med2011;39:266-271.
15. Kon E, Filardo G, Di Martino A, Marcacci M. Platelet-richplasma (PRP) to treat sports injuries: Evidence to support itsuse. Knee Surg Sports Traumata! Arthrosc 2011;19:516-527.
16. Wahlstrb'm O, Linder C, Kalen A, Magnusson P. Variation ofpH in lysed platelet concentrates influence proliferation andalkaline phosphatase activity in human osteoblast-like cells.
17. Borg T, Modig J. Potential anti-thrombotic effects of localanesthetics due to their inhibition of platelet aggregation. AdaAnaesthesiol Scand 200 S;29:73 9-742.
18. Mazzocca AD, McCarthy MB, Chowaniec DM, et al. Platelet-rich plasma differs according to preparation method and hu-man variability. J Bone Joint Surg Am 2012;94:308-316.
19. Tanaka Y, Kurashima K, Saito H, et al. In vitro short-terrnplatelet adhesion on various metals. J Artif Organs 2009;12:182-186.
20. Michelson AD. Platelets. Ed 2. San Diego: Elsevier/AcademicPress; 2007.
21. Grottum KA, Jorgensen L, Jeremic M. Decrease in plateletsurface charge during phagocytosis of polystyrene latex parti-cles or thorium dioxide. Scand J Haematol 1972;9:83-96.
22. Arthrex. ACP: Autologous conditioned plasma double syringesystem. Brochure LB0810F. Naples, FL: Arthrex, 2011.
23. Cascade Medical/MTF. Releasing the power of growth factorhealing. Brochure 408-5M 506TC4. Edison, NJ: CascadeMedical/Musculoskeletal Transplant Foundation, 2008.
24. Leitner GC, Gruber R, Neumiiller J, et al. Platelet content and

1008 J. M, DELONG ET AL.
growth factor release in platelet-rich plasma: A comparison of 45.four different systems. Vox Sang 2QQ5;91:135-139.
25. Mazzucco L, Balbo V, Cattana E, Guaschino R, Borzini P. Notevery PRP-gel is born equal. Evaluation of growth factoravailability for tissues through four PRP-gel preparations: Fi-brinet, RegenPRP-Kit, Plateltex, and one manual procedure. 46.Vac Sons 2009;97:IIO-IIS.
26. Anitua E, Aguirre JJ, Algorla J, et al. Effectiveness of autol-ogous preparation rich in growth factors for the treatment of 47.chronic cutaneous ulcers. / Blamed Mater Res B Appi Biam-ater 2008:84:415-421.
27. Sanchez M, Anitua E, Azofra J, Aguirre JJ, Andia I. Intra-ardcular injection of an autologous preparation rich in growth 48.factors for the treatment of knee OA: A retrospective cohortstudy, din Exp Rheumatol 20QS;26:91Q-913.
28. Sanchez M, Anitua E, Azofra J, Andia I, Padilla S, Mujika I. 49.Comparison of surgically repaired Achilles tendon tears usingplatelet-rich fibrin matrices. Am J Sports Med 2Q07;35:245-251. 50.
29. Biomet. GPS III platelet separation system process steps. Bro-chure BB10001.0. Warsaw, IN: Biomet, 2009.
30. Biomet. GPS III platelet separation system. BrochureBB10003.0. Warsaw, IN: Biomet, 2007. 51.
31. Eppley BL, Woodell JE, Higgins J. Platelet quantification andgrowth factor analysis from platelet-rich plasma: Implicationsfor wound healing. Plast Reconstr Surg 2004;114:1502-150S. 52.
32. Kevy SV, Jacobson MS. Comparison of methods for point ofcare preparation of autologous platelet gel. J Extra CorporTechnal 2QQ4;36:2S-35. 53.
33. Roukis TS, Zgonis T, Tiernan B. Autologous platelet-richplasma for wound and osseous healing: A review of theliterature and commercially available products. Adv Ther 54.2Q06;23:21S.
34. Harvest Technologies. Developing technologies for accelerat-ing healing, naturally. Brochure SL 021/0106. Plymouth, MA: 55.Harvest Technologies, 2000.
35. Sclafani AP, Romo TR, Ukrainsky G, et al. Modulation ofwound response and soft tissue ingrowth in synthetic andallogeneic implants with platelet concentrate. Arch Facial 56.Plast Surg 2QQ5;l;\63-\69.
36. Christensen K, Vang S, Brady C, et al. Autologous platelet gel:An in vitro analysis of platelet-rich plasma using multiplecycles. / Extra Corpor Techno! 2006;38:249-253. 57.
37. Medtronic. Magellan autologous platelet separator. BrochureUC200502505. Minneapolis, MN: Medtronic, 2005.
38. Exactech. Accelerate concentrating system platelet rich plasma 58.preparation guide. Brochure 713-06-00 Rev B. Gainesville,FL: Exactech, 2010.
39. Exactech. Analysis of Accelerate platelet concentrating sys-tem: Preparation of concentrated platelet product. Brochure 59.713-06-81. Gainesville, FL: Exactech, 2010.
40. Exactech. Accelerate PRP sport preparation technique. Bro- 60.chure 713-08-00 Rev B. Gainesville, FL: Exactech, 2010.
41. Sanchez M, Anitua E, Andia I. Poor standardization in plate-let-rich therapies hampers advancement. Arthroscopy 2010;26:725-726. 61.
42. Haynesworth SE, Kadiyala S, Liang LN, et al. Mitogenicstimulation of human mesenchymal stem cells by plateletrelease suggest a mechanism for enhancement of bone repairby platelet concentrates. Presented at the 4Sth Meeting of the 62.Orthopedic Research Society, Boston, MA, 2002.
43. Anitua E, Andia I, Sanchez M, et al. Autologous preparationsrich in growth factors promote proliferation and induce VEGF 63.and HGF production by human tendon cells in culture. J Or-thop Res 2005;23:2Sl-286.
44. Anitua E, Orive G, Pla R, Roman P, Serrano V, Andia I. Theeffects of PRGF on bone regeneration and on titanium implant 64.osseointegration in goats: A histologic and histomorphometricstudy. J Blamed Mater Res A 2Q09;91:15S-165.
Anitua E, Sanchez M, Nurden AT, et ah Platelet-released•growth factors enhance the secretion of hyaluronic acid andinduce hepatocyte growth factor production by synovia! fibro-blasts from arthritic patients. Rheumatology .(.Oxford] 2007 ;46:1769-1772.Anitua' E, Sanchez M, Zalduendo MM, et al. Fibroblasticresponse-to -treatment with different preparations rich ingrowth factors. Ce//'/)ro/i/'2009;42:162-170, - ...Sanchez M, Anitua E, Azofra J, Prado R, Muruzabal F, AndiaI. Ligamentization of tendon grafts treated with an endogenouspreparation rich in growth factors: Gross morphology andhistology. Anhroscopy 2010;26:470-4SO.Sanchez M, Anitua E, Cugat R, et al. Nonunions treated withautologous preparation rich in growth factors. J OrthopTrauma 2009;23:52-59.Sanchez M, Azofra J, Anitua E, et al. Plasma rich in growthfactors to treat an articular cartilage avulsion: A case report.Med Set Sports Exerc 2003;35:1648-1652.Graziani F, Ivanovski C, Cei S, Ducci F, Tonetti M, GabrieleM. The in vitro effect of different PRP concentrations onosteoblasts and fibroblasts. Clin Oral Implants Res 2QQ6;17:212-219.Torricelli P, Fini M, Filardo G, et al. Regenerative medicinefor the treatment of musculoskeletal overuse injuries in com-petition horses. Int Orthop 2011;35:1569-1576.He HT, Majd ME, Holt RT, et al. Do autologous growthfactors enhance transforaminal lumbar interbody fusion? EurSpine J2003;12:400-407.Weibrich G, Hansen K, Kleis W, Buch R, Hitzler WE. Effectof platelet concentration in platelet-rich plasma on peri-im-plant bone regeneration. Bone 2004;34:665-671.Giusti I, Rughetti A, D'Ascenzo S, et al. Identification of anoptimal concentration of platelet gel for promoting angiogen-esis in human endothelial cells. Transfusion 2009;49:771-778.Gruber R, Varga F, Fischer MB, Watzek G. Platelets stimulateproliferation of bone cells: Involvement of platelet-derivedgrowth factor, microparticles and membranes. Clin Oral Im-plants Res 2002; 13:529-535.Choi BH, Zhu SJ, Kim BY, et al. Effect of platelet-rich plasma(PRP) concentration on the viability and proliferation of alve-olar bone cells: An in vitro study. In! J Oral Maxillofac Surg2005;34:420-424.Nikolidakis D, Jansen JA. The biology of platelet-rich plasmaand its application in oral surgery: Literature review. TissueEng Part B Rev 2008; 14:249-258.Jo CH, Roh YH, Kim JE, et al. Optimizing platelet-rich plasmagel formation by varying time and gravitational forces duringcentrifugation. J Oral Implanto! in press, available online 11April, 2011.Barrett S, Erredge S. Growth factors for chronic plantar fas-ciitis. Podiatry Today 2004; 17:37-42.Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classifi-cation of platelet concentrates: From pure platelet-rich plasma(P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). TrendsBiotechnol 2009;27:15S-167.Saad Setta H, Elshahat A, Elsherbiny K, Massoud K, Safe I.Platelet-rich plasma versus platelet-poor plasma in the man-agement of chronic diabetic foot ulcers: A comparative study.Int Wound/2011;8:307-312.Rappl LM. Effect of platelet rich plasma gel in a physiologi-cally relevant platelet concentration on wounds in persons withspinal cord injury. Int Wound J 2011;8:187-195.Frykberg RG, Driver VR, Carman D, et al. Chronic woundstreated with a physiologically relevant concentration of plate-let-rich plasma gel: A prospective case series. Ostoiny WoundManage 2010;56:36-44.Moojen DJ, Everts PA, Schure RM, et al. Antimicrobial ac-tivity of platelet-leukocyte gel against Staphylococcus aureus.J Orthop Res 200S;26:404-410.
PLATELET-RICH PLASMA CLASSIFICATION 1009
65. Martin P, D'Souza D, Martin J, et al. Wound healing in thePU.l null mouse—Tissue repair is not dependent on inflam-matory cells. CHIT Biol 2003;13:1122-112S.
66. de Vos RJ, Weir A, van Schie HT, Verhaar JA, Weinans H,van Schie HT. No effects of PRP on ultrasonographic tendonstructure and neovascularisation in chronic midpoint Achillestendinopathy. Br J Sports Med 2011;45:387-392.
67. Mishra A, Woodall J, Vieira A. Treatment of tendon andmuscle using platelet-rich plasma. Clin Sports Mad 2009;28:113-125.
68. Harrison S, Vavken P, Kevy S, Jacobson M, Zurakowski D,Murray MM. Platelet activation by collagen provides sustainedrelease of anabolic cytokines. Am J Sports Med 2011;39:729-734.
69. Mosesson MW, Siebenlist KR, Meh DA. The structure andbiological features of fibrinogen and fibrin. Ann N Y Acad Sci2001:936:11-30.
70. Alsousou J, Thompson M, Hulley P, Noble A, Willett K. Thebiology of platelet-rich plasma and its application in traumaand orthopaedic surgery: A review of the literature. J BoneJoint Surg Br 2009;91:9S7-996.
71. Dohan DM, Choukroun J", Diss A, et al. Platelet-rich fibrin(PRF): A second-generation platelet concentrate. Part I: Tech-nological concepts and evolution. Oral Surg Oral Med OralPathol Oral Radial Endod 2006;101:e37-e44.
72. Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, RodeoSA. Platelet-rich plasma: From basic science to clinical appli-cations. Am J Spans Med 2009;37:2259-2272.
73. Sir SC, Esaki J, Marui A, et al. Angiogenic properties ofsustained release platelet-rich plasma: Characterization in-yitro and in the ischemic hind limb of the mouse. J Vase Surg2009;50:S70-S79.e2.
74. Baton! G, Maisetta G, Brancatisano FL, Esin S, Campa M. Useof antimicrobial peptides aaainst microbial biofilms: Advan-tages and limits. Curr MetTchem 2011;18:256-279.
75. Carrol RJ, Araoczky SP, Graham S, et al. Characterization ofautologous growth factors. Cascade® platelet-rich fibrin ma-trix (PRFM). Edison, NJ: Musculoskeletai Transplant Foun-dation, 2005.
76. Fufa D, Shealy B, Jacobson M, Kevy S, Murray MM. Acti-vation of platelet-rich plasma using soluble type I collagen.J Oral Maxllhfac Surg 200S;66:684-690.
77. Lyras DN, Kazakos K, Georgiadis G, et al. Does a singleapplication of PRP alter the expression of IGF-I in the earlyphase of tendon healing? J Foot Ankle Surg 2011;50:276-282.
78. Hechtman KS, Uribe JW, Botto-vanDemden A, Kiebzak GM.Platelet-rich plasma injection reduces pain in patients withrecalcitrant epicondylitis. Orthopedics 2011;34:92-92.
79. Thanasas C, Papadirnitriou G, Charalambidis C, Paraskevo-poulos I, Papanikolaou A. Platelet-rich plasma versus autolo-gous whole blood for the treatment of chronic lateral elbowepicondylitis: A randomized controlled clinical trial. Am JSports Med 2011;39:2130-2134.
50. Peerbooms JC, Sluimer J, Bruijn DJ, Gosens T. Positive effectof an autologous platelet concentrate in lateral epicondylitis ina double-blind randomized controlled trial: Platelet-richplasma versus corticosterold injection with a 1-year follow-up.Am J Sports Med 2010;38:255-262.
51. Gosens T, Peerbooms JC, van Laar W, den Oudsten BL.Ongoing positive effect of platelet-rich plasma versus cortico-
steroid injection in lateral epicondylitis: A double-blindrandomized controlled trial with 2-year follow-up. Am J SportsMed 2011;39:1200-1208.
82. Mishra A, Pavelko T. Treatment of chronic elbow tendinosiswith buffered platelet-rich plasma. Am J Sports Med 2006;34:1774-1778.
83. de Jonge S, de Vos RJ, Weir A, et al. One-year follow-up ofplatelet-rich plasma treatment in chronic Achilles tendinopa-thy: A double-blind randomized placebo-controlled trial. Am JSports Med 2011;39:1623-1629.
84. Schepull T, Kvist J, Norrman H, Trinks M, Berlin G, Aspen-berg P. Autologous platelets have no effect on the healing ofhuman Achilles tendon ruptures: A randomized single-blindstudy. Am J Sports Med 2011:39:38-47.
85. Filardo G, Presti ML, Kon E, Marcacci M. Nonoperativebiological treatment approach for partial Achilles tendon le-sion. Orthopedics 2010;33:120-123.
86. Filardo G, Kan E, Delia Villa S, Vincentelli F, Fornasari PM,Marcacci M. Use of platelet-rich plasma for the treatment ofrefractor;'jumper's knee. Int Orthop 2010;34:909-915.
87. Kon E, Filardo G, DelcogHano M, et al. Platelet-rich plasma:New clinical application: A pilot study for treatment of jump-er's knee. Injury 2009:40:598-603.
88. Jo CH, Kim JE, Yoon KS, et al. Does platelet-rich plasmaaccelerate recovery after rotator cuff repair? A prospectivecohort study. Am J Sports Med 2011;39:2082-2090.
89. Randelli P, Arrigoni P, Ragone V, Aliprandi A, Cabitza P.Platelet rich plasma in arthroscopic rotator cuff repair: Aprospective RCT study, 2-year follow-up. J Shoulder ElbowSurg 2011;20:51S-52S.
90. Castricini R, Longo UG, De Benedetto M, et al. Platelet-richplasma augmentation for arthroscopic rotator cuff repair: Arandomized controlled trial. Am J Sports Med 2011;39:25S-265.
91. Randelli PS, Arrigoni P, Cabitza P, Volpi P, Maffulli N.Autologous platelet rich plasma for arthroscopic rotator cuffrepair. A pilot study. Disabil Rehabll 200S;30:1584-1589;
92. Barber FA, Hrnack SA, Snyder SJ, Hapa O. Rotator cuff repairhealing influenced by platelet-rich plasma construct augmen-tation. Arthroscopy 2011;27:1029-I035. •
93. Everts PA, Devilee RJ, Brown Mahoney C, et al. Exogenousapplication of platelet-leukocyte gel during open subacromialdecompression contributes to improved patient outcome. Aprospective randomized double-blind study. Eur Surg Res200S;40:203-210.
94. Kon E, Mandelbaum B, Buda R, et al. Platelet-rich plasmaintra-articular injection versus hyaluronic acid viscosupple-mentation as treatments for cartilage pathology: From earlydegeneration to osteoarthritis. Arthroscopy 2011;27:1490-1501.
95. Kon E, Buda R, Filardo G, et al. Platelet-rich plasma: Intra-articular knee injections produced favorable results on degen-erative cartilage lesions. Knee Surg Sports Traumatol Arthrosc2010:18:472-479.
96. Silva A, Sampaio R. Anatomic ACL reconstruction: Does theplatelet-rich plasma accelerate tendon healing? Knee SurgSports Traumatol Arthrosc 2009; 17:676-652.
97. Peerbooms JC, de Wolf GS, Colaris JW, Bniijn DJ, VerhaarJA. No positive effect of autologous platelet gel after totalknee arthroplasty. Ada Orthop 2009:80:557-562.
Systematic Review
Open Capsular Shift and Arthroscopic Capsular Plication forTreatment of Multidirectional Instability
Mark E. Jacobson, M.D., Michael Riggenbach, MX)., Adam N. Wooldridge, B.A., B.S., andJulie Y. Bishop, M.D.
Purpose: To compare the results of open inferior capsular shift with arthroscopic capsular plicationfor multidirectional instability in patients without a Bankart lesion. We hypothesized that there is nodifference with regard to the specific clinical outcomes evaluated, including recurrent instability,range of motion, return to sport, and complications. Methods: We conducted a comprehensiveliterature search. Databases searched included PubMed from 1966 to 2010, the Cochrane Databaseof Systematic Reviews and Controlled Trials, CINAHL (Cumulative Index to Nursing and AlliedHealth Literature) from 1982 to 2010, and SPORTDiscus from 1975 to 2010. Limits included Englishlanguage, human subjects, and title. Results: We found 7 articles with a total of 197 patients (219shoulders) that met our inclusion criteria. The data did not clearly show open treatment to be superiorto,arthroscopic treatment. No study reported a consistent loss of greater than 40° of external rotation.No technique showed significantly less external rotation loss over the other. Whereas there was aslight trend toward increased return to sport for patients treated arthroscopic ally, no clear conclusioncan be drawn given the variability of reporting in the reviewed studies. Analysis of complicationsshows that both procedures are reliably safe with minimal complications. Conclusions: When one isevaluating patients with traumatic or atraumatic onset of shoulder instability in 2 directions and nostructural lesions, arthroscopic capsular plication yields comparable results to open capsular shiftwith regard to recurrent instability, return to sport, loss of external rotation, and overall complica-tions. Level of Evidence: Level IV, systematic review of Level IV studies.
In 1980, Neer and Foster1 coined the term "mul-tidirectional instability" (MDI) and proposed
specific surgical treatment to patients in whom con-servative management has failed. In this classicarticle they report preliminary results of the inferiorcapsular shift as a means to address the patulous
From the Division of Shoulder Surgery, Department of Ortho-paedics, The Ohio State University, Columbus, Ohio, U.S.A.
The authors report that they have no conflicts of interest in theauthorship and publication of this article.
Received September 30, 2011; accepted December 6, 20] 1.Address correspondence to Julie Y. Bishop, M.D., Department of
Orthopaedics, The Ohio State University Medical Center, 2050Kenny Kd. Ste 3300, Columbus, OH 43221, U.S.A. E-mail: Julie, bishop @osumc. edu
© 2012 by the Arthroscopy Association of North America0749-8063/1162 7/$36.00doi:10.1016/j.arthro.201L12,006
inferior capsule that they believed to be the respon-sible pathology. Although open inferior capsularshift remains the standard in surgical treatment ofMDI, multiple alternative procedures have been de-veloped. In 1993, Duncan and Savoie2 first reportedpreliminary results of arthroscopic capsular plica-tion.
In all patients presenting with MDI, a regimentedcourse of physical therapy directed at strengtheningof scapular stabilizers, the rotator cuff, and thedeltoid is warranted.1*3-4 Burkhead and Rockwood4
reported good or excellent results in 88% of patientswith atraumatic instability treated with an exerciseprogram; however, more recent results have beenless encouraging, at 30% to 61%.3'5 If these recentreports more adequately represent our current pa-tient population and its expectations, it is reason-
1010 Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 28, No 7 (July), 2012: pp 1010-1017


















