Plasmodium Introduction 1- Most important parasitic disease affecting human. 2- Most common in...
19
Plasmodium Plasmodium Introduction Introduction 1- Most important parasitic disease affecting human. 2- Most common in Tropic –Subtropics mostly Africa, Asia & S. America 3- It is estimated that more than 300 million people suffer annually. 4- Number of Deaths more than 2 million per year mostly among children 5- Transmission of the disease is mainly by bite of female Anopheles . 6- Transmission in an area depends upon: infected cases “Gametocytes carriers” – Anopheles mosquito Vector (which require an optimum condition of humidity & temperature 20-30 ºC) – rainfall provides breeding places. DR. RAAFAT T. MOHAMED 7- Inhabitants in hyperendemic areas are repeatedly inoculated by Sporozoites through mosquito’s bite 8- Children are more susceptible in areas of high transmission than Adults 9- “Premunition ” a form of immunity sufficient to control but not to prevent infection develops which control infection in elders. 10- P. falciparum malaria infection is severe in immune & non-immune pregnant females.
-
Upload
lydia-henry -
Category
Documents
-
view
217 -
download
0
Transcript of Plasmodium Introduction 1- Most important parasitic disease affecting human. 2- Most common in...

Plasmodium Plasmodium
IntroductionIntroduction
1- Most important parasitic disease affecting human.2- Most common in Tropic –Subtropics mostly Africa, Asia & S. America3- It is estimated that more than 300 million people suffer annually.4- Number of Deaths more than 2 million per year mostly among children5- Transmission of the disease is mainly by bite of female Anopheles.6- Transmission in an area depends upon: infected cases “Gametocytes carriers” – Anopheles mosquito Vector (which require an optimum condition of humidity & temperature 20-30 ºC) –rainfall provides breeding places.
DR. RAAFAT T. MOHAMED
7- Inhabitants in hyperendemic areas are repeatedly inoculated by Sporozoites through mosquito’s bite8- Children are more susceptible in areas of high transmission than Adults9- “Premunition” a form of immunity sufficient to control but not to prevent infection develops which control infection in elders.10- P. falciparum malaria infection is severe in immune & non-immune pregnant females.

Plasmodium Plasmodium
DR. RAAFAT T. MOHAMED

Plasmodium Causes Human Malaria
Mal: bad aria: air
P.vivax: vivax or benign tertian malaria
P.ovale: ovale or ovale tertian malaria
P.malariae: malariae or quartan malaria
P.falciparum: falciparum or subtertian or malignant malaria
Most predominant
Tropics
Tropics
Temperate zones
Geographical Distribution
Presence of Malaria = Presence of Anopheline mosquito
DR. RAAFAT T. MOHAMED

Areas where malaria has disappeared or never existed Ø
Areas with limited risk +
Areas where malaria transmission occurs ++
Malaria Distribution all over the world
DR. RAAFAT T. MOHAMED
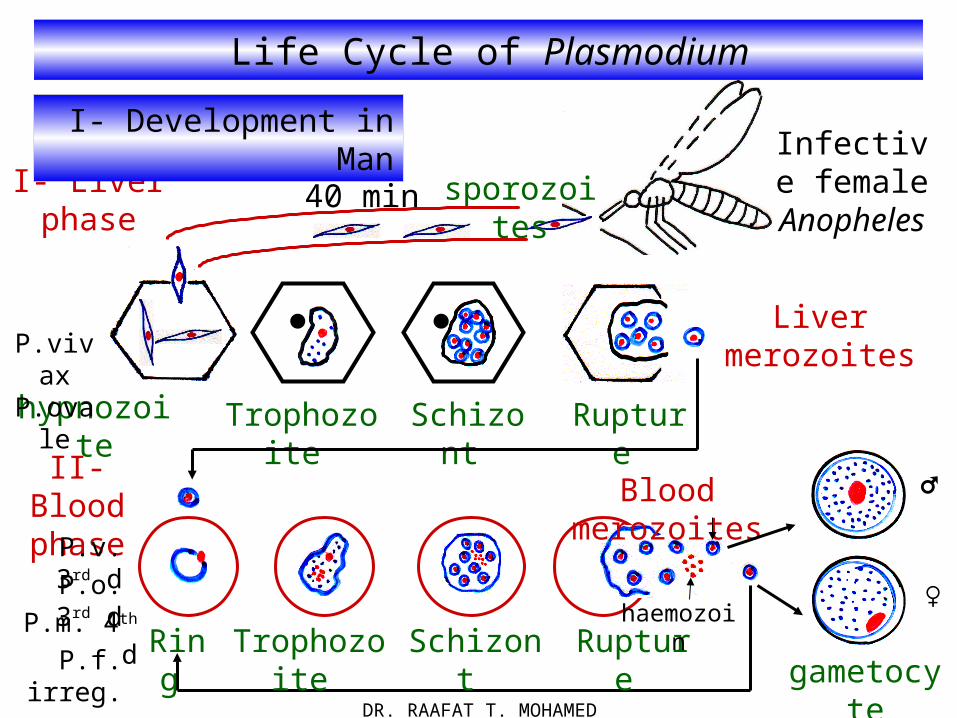
Life Cycle of Plasmodium
Infective female
Anopheles40 min
hypnozoite Trophozoite Schizont
Liver merozoites
I- Liver phase
Rupture
II- Blood phase Blood merozoites ♂
♀
gametocyteRing Trophozoite Schizont Rupture
P.vivax P.ovale
sporozoites
I- Development in Man
P.v. 3rd d
P.o. 3rd d
P.m. 4th d
P.f. irreg.
haemozoin
DR. RAAFAT T. MOHAMED

II- Development in Anopheles Mosquito gut
♂ and ♀ gametocytes
exflagellation
fusion
Zygote
♂ and ♀ gametes
Ookinete
Oocyst
Sporocyst
Sporozoites in salivary
gland
Sporogony
Reduction division
DR. RAAFAT T. MOHAMED
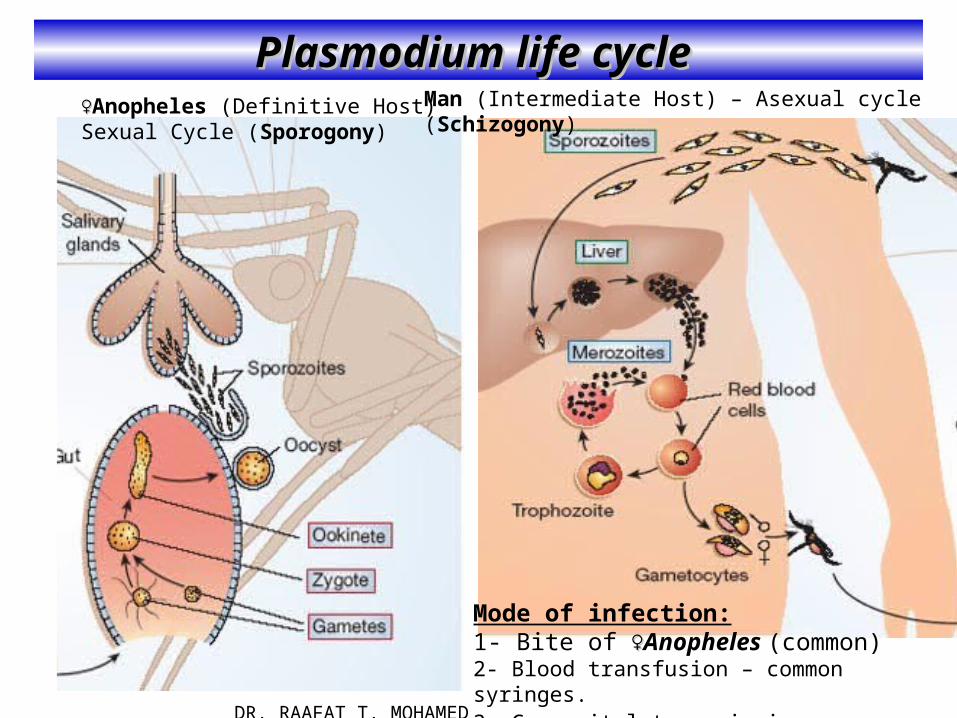
Plasmodium life cycle Plasmodium life cycle
DR. RAAFAT T. MOHAMED
♀♀Anopheles (Definitive Host)Sexual Cycle (Sporogony)
Man (Intermediate Host) – Asexual cycle (Schizogony)
Mode of infection:1- Bite of ♀♀Anopheles (common)2- Blood transfusion – common syringes.3- Congenital transmission.

Plasmodium life cycle Plasmodium life cycle
DR. RAAFAT T. MOHAMED

Plasmodium life cycle Plasmodium life cycle
28a_malaria_life_cycle_of_plasodium.swf plasmodium.swf
DR. RAAFAT T. MOHAMED
12

Some Stages of Malaria in Anopheles
Feeding female Anopheles Exflagellation showing microgametes
Oocysts on outside of mosquito stomachSporozoites from salivary gland
DR. RAAFAT T. MOHAMED

Exoerythrocytic Cycle
• Schizonts take 5-7 days to develop• formation of >10,000 merozoites• upon rupture of hepatocyte, released merozoites will invade R.B.Cs.
The final step involves the release of merozoites (green) into the bloodstream. The signal(s) that trigger the release remain unknown. Plasmodium merozoites are released by the formation of merozoite-filled vesicles (merosomes), which bud off from the infected hepatocytes into the sinusoidal lumen.
Nature Reviews Microbiology (2006): Nature Reviews Microbiology (2006): 4-8494-849DR. RAAFAT T. MOHAMED

Plasmodium (Ring form) Plasmodium (Ring form)
Early Trophozoite (Ring stage) :Thin loop of cytoplasm & a small chromatin dot enclosing a pale central vacuole (signet form) .In P falciparum P falciparum it appears like a pair of stereo-head phones. Also more than one ring in the Same RBCs (multiple infection). Accolè form (marginal ring).
DR. RAAFAT T. MOHAMED
P. falciparum
vivax
P malariae
ovale
falciparum
Accolè form
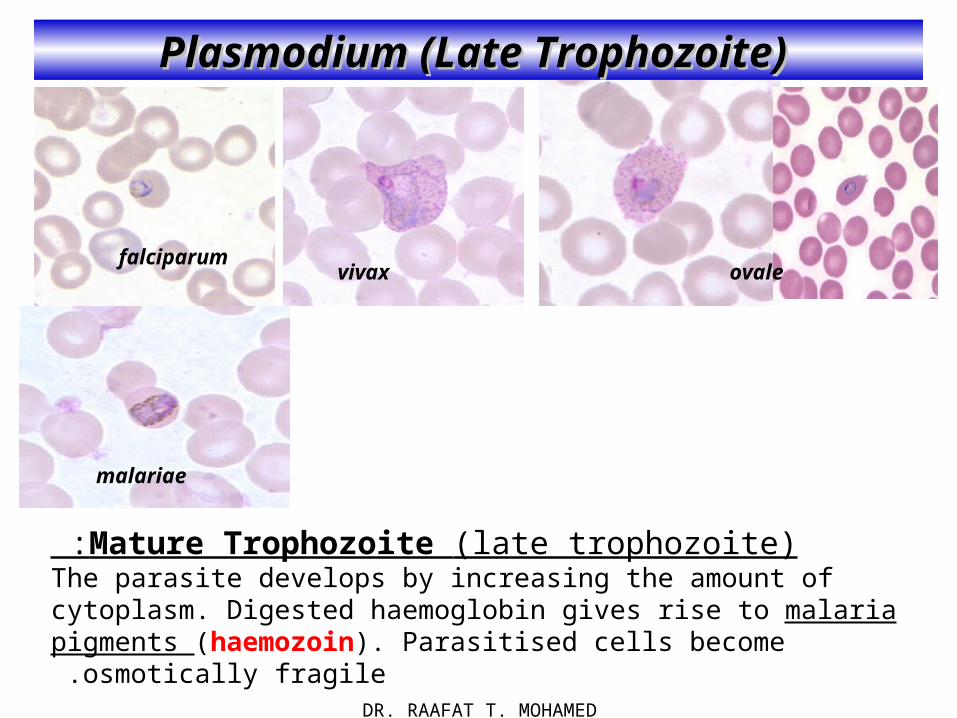
Plasmodium (Late Trophozoite) Plasmodium (Late Trophozoite)
Mature Trophozoite (late trophozoite) :The parasite develops by increasing the amount of cytoplasm. Digested haemoglobin gives rise to malaria pigments (haemozoin). Parasitised cells become osmotically fragile .
DR. RAAFAT T. MOHAMED
falciparumvivax ovale
malariae

Plasmodium (E. Schizont) Plasmodium (E. Schizont)
Erythroytic Schizont: The chromatin & cytoplasm break into fragments merozoites .
The pigments remains as a single mass in the center . The Schizont (mature stage of the parasite) eventually occupies the entire R.B.C
Rupture of E. Schizonts merozoites - malaria pigments - toxins into the blood stream: *Merozoites attack new R.B.Cs repeating the cycle. *Pigments (haemozoin) are engulfed by R.E.Cs. *Toxins (immunogenic) induce malarial paroxysm.Merozoites attack clean RBCs repeating the cycle
DR. RAAFAT T. MOHAMED
falciparum vivax
ovale
malariae

Plasmodium (Gametocytes) Plasmodium (Gametocytes)
Following repeated cycles Merozoites invade RBCs - develop into: *Microgametocytes (male gametocytes) & * Macrogametocytes ( female gametocyte).Gametocytes are infective to the female Anopheles .
DR. RAAFAT T. MOHAMED
falciparum vivax
ovalemalariae

Pathogenesis and Pathogenesis and Clinical PictureClinical Picture
1- Destruction of osmotically fragile infected R.B.C.s intra & extra-vascular haemolysis HAEMOLYTIC ANAEMIA.
2-Toxins activate the macrophage / monocyte series of cells which will stimulate sensitized T -lymphocytes to produce Cytokines FEVER.
3 -Merozoites - parasitized R.B.C.s -lysed R.B.C.s - toxins - pigments are cleared from the circulation by stimulation of the R.E.S. SPLENOMEGALY besides HEPATOMEGALY.
4-Destruction of immature Reticulocyte together with suppressed erythropoiesis decreased production of R.B.C.s ANAEMIA.
5- Enlarged spleen early destruction of RBCs (activation of the complement system) ANAEMIA
6 -Large number of circulating immune complexes 'C.LC.s' (takes place with P.malariae & P falciparum infections) deposit in the glomerular capillaries
acute glomerulopathy NEPHROTIC syndrome .
7- Parasite feeds on haemoglobin depletion of iron stores inappropriate haemoglobin metabolism ANAEMIA.
DR. RAAFAT T. MOHAMED

Pathogenesis and Pathogenesis and Clinical PictureClinical Picture
8- Haemolysis of R.B.C.s JAUNDICE
9 -Parasitised erythrocytes of P falciparum Cytoadhere to the endothelial surface of capillaries occludes the microcirculatory blood flow
PERNICIOUS syndrome as a result of Tissue Anoxia - Focal Necrosis - Hemorrhage - Oedema of vital organs 'multiorgan involvement‘.
1 -Paroxysms are repeated for few weeks or longer with decreasing intensity .The disease is self-limited (due to cytokine activity & Premunition). In between
attacks the patient may be exhausted but generally feels well . 2- RelapseRelapse of the infection may occur in both P. vivax & P.ovale after resolution of the primary infection (mainly due to Hypnozoites).
3- RecrudescenceRecrudescence of the infection may occur in both P.malariae & P falciparum (due to persistent low grade undetectable parasitaemia) flare up of the infection with recurrence of the clinical attack.
DR. RAAFAT T. MOHAMED

Pathogenesis and Pathogenesis and Clinical PictureClinical Picture
• paroxysms associated with synchrony of merozoites release
• between paroxysms temperature is normal and patient feels well
• falciparum may not exhibit classic paroxysms (continuous fever)
Subtertian malariatertian malariaquartan malaria
All species of Plasmodium will give rise to the following Clinical Picture:
1- FEVER1- FEVER 2- SPLENOMEGALY2- SPLENOMEGALY 3- HEPATOMEGALY3- HEPATOMEGALY
4- ANAEMIA4- ANAEMIA 5- JAUNDICE5- JAUNDICE.
three successive stages: Cold - Hot - Sweat
Cold stage : Shivering "chills"(O.5 - 1 hr.) followed by sharp rise in the temperature.Hot stage : High fever- headache - flushed face - rapid
pulse (1 - 4 hrs.) .Sweat stage : Sweat with drop of temperature (1- 4 hrs.) .
1- FEVER (PAROXYSM)1- FEVER (PAROXYSM)
DR. RAAFAT T. MOHAMED

Pathogenesis and Pathogenesis and Clinical PictureClinical Picture 22 - -ANAEMIAANAEMIA
Haemolytic anaemia Haemolytic anaemia - multifactorial due to rupture of R.B.C.s- deficient Hb.metabolism - suppressed erythropoiesis - early R.B.C.s destruction. *Severe in P falciparum (high parasitaemia "young & old RBCs" are infected). *Moderate in P vivax & P.ovale (moderate parasitaemia "young RBCs" are infected). *Mild in Pimalariae (mild parasitaemia "old RBCs" are infected).
33 - -SPLENOMEGALYSPLENOMEGALY
The Spleen: is enlarged - soft - tender *Mild to moderate "P vivax & P ovale".
*Marked enlargement "P malariae"(prolonged duration of infection "chronic" with repeated attacks that end up by hypersplenism .(
*Marked enlargement "P falciparum" (cytoadherence phenomenon).
44 - -JAUNDICEJAUNDICE
*Mild "P. vivax – P ovale – P malariae" (haemolysis of RBC). *Severe "P .falciparum'' (liver involved by cytoadherence)
DR. RAAFAT T. MOHAMED