Planning & Investing now for future patient...
31
Planning & Investing now for future patient needs Private Hospitals Association Conference 2017 20 th June, 2017 Jim Breslin Secretary General Department of Health
Transcript of Planning & Investing now for future patient...

Planning & Investing now for future patient needs
P r i v a t e H o s p i t a l s A s s o c i a t i o n C o n f e r e n c e 2 0 1 7
20t h J u n e , 2 0 1 7
Jim BreslinSecretary General
Department of Health

The Health Outcomes Context

So here’s an extra 6 years…• Since 1990 life expectancy in Ireland has increased by:
– 6.3 years in total
– 6.9 for men
– 5.4 for women
• Irish life expectancy is now:
– 79 years for men(1 year above EU average)
– 83 years for women (at EU average)

Life expectancy at birth for Ireland and EU-28 by gender, 2000-2014Source: EurostatNote: Life expectancy figures for EU 28 available from 2002.
Life expectancy in Ireland and EU-28
70
72
74
76
78
80
82
84
86
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Life
exp
ect
ancy
in y
ear
sEU-28 Males EU-28 Females Ireland Males Ireland Females
Women =83 years Men =
79 yrs1 yr > EU

Reduction in Mortality Rates

Other Achievements
• Breast and Colorectal cancer improvements
• [5-Yr Relative Survival Rates 1998-2003 To 2008-2013 ]
• Breast Cancer – up from 75.8% to 81.5%
• Colorectal – up from 51% to 60.3%Meningitis C down from:130 cases (1999) to 6 (2014)
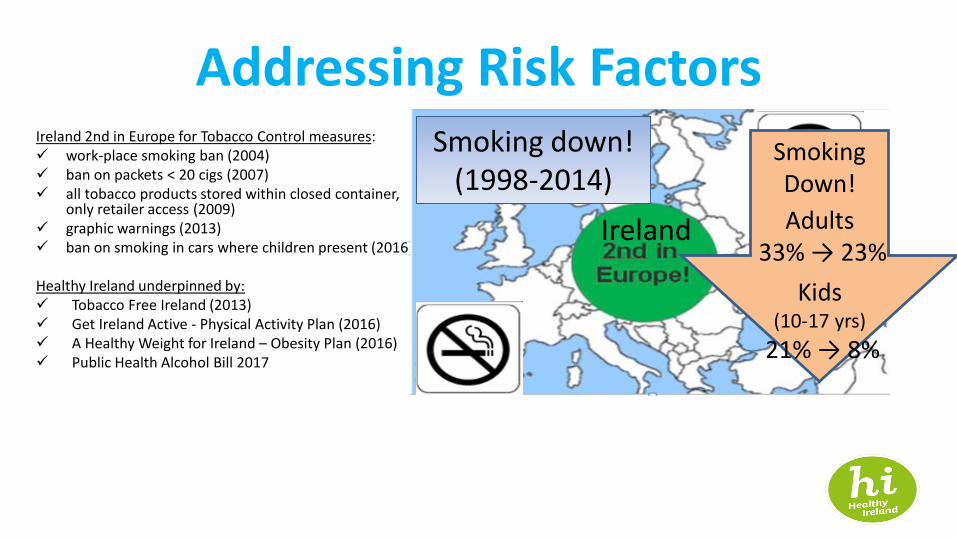
Addressing Risk FactorsIreland 2nd in Europe for Tobacco Control measures:✓ work-place smoking ban (2004)✓ ban on packets < 20 cigs (2007)✓ all tobacco products stored within closed container,
only retailer access (2009)✓ graphic warnings (2013)✓ ban on smoking in cars where children present (2016)
Healthy Ireland underpinned by:✓ Tobacco Free Ireland (2013)✓ Get Ireland Active - Physical Activity Plan (2016)✓ A Healthy Weight for Ireland – Obesity Plan (2016)✓ Public Health Alcohol Bill 2017
Ireland
Smoking down! (1998-2014)
Smoking Down!
Adults 33% → 23%
Kids(10-17 yrs)
21% → 8%

WHAT WE READ ABOUT
Good progress on outcomes, but overshadowed by significant strain on our health services. Why?

Health Service Productivity Improvement
• Inpatient & Day Cases
•54% increase in day case procedures - 558,813 to 860,763
•Inpatient procedures constant –approx 600,000 p.a. [above from 2006 – 2014]
•Cost per weighted unit of care fell from 2008 to 2014 by 19% (inpatient), 18.7% (day case)
•Day of Surgery Admission rate increased 9% - 2008-2014

But demographics and chronic illness require a major shift in our
model of health & social care

0%
5%
10%
15%
20%
25%
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
EU-28 Ireland
Percentage population growth since 2001: Ireland compared with EU average
Source: Eurostat
Demographic Backdrop

-5
0
5
10
15
20
25
Tho
usa
nd
sChanges over time in population 65+
Source: CSO
Change per annum in Population 65+, Ireland, 1950-2015

Projected population growth in the 65 years and older age group, Ireland compared with EU-28 average, 2013 to 2021Source: Eurostat
0
2.6%
5.7%
8.6%
11.6%
14.8%
17.8%
21.0%
24.1%
0%
5%
10%
15%
20%
25%
2013 2014 2015 2016 2017 2018 2019 2020 2021
EU-28 Ireland
Future Outlook – Older Population

0
5000
10000
15000
20000
25000
30000
35000
65-69 70-74 75-79 80-84 85+
2006 2011 2014
Increasing Number of Older People Requiring Emergency Admission
Source: Shelley/HIPE
Number of discharges of patients admitted as emergency

Chronic Illness• In 2010, 76% of deaths in Ireland were due to 3 major
conditions – cardiovascular disease (34%), cancer (30%) and respiratory disease (12%).
• c. 38% of Irish people 50+ have a chronic disease and 11% have more than one.
• As the number of older people increases this burden of chronic disease will grow, HSE estimates by 20% by 2020.
• Estimates project a 70% increase in cancer cases in females &

Chronic Illness• In 2011, 40% of all hospitalisations in patients 35 years+ related to 4
chronic diseases; cardiovascular disease, cancer, respiratory disease and diabetes (either as a direct reason for hospitalisation 19%, or a contributory factor 22%)
• 76% of all bed days used, either directly (46%) or as a contributory factor (30%), by patients with these 4 conditions
• 55% (€1.68 billion) of acute hospital budget is attributable to care of patients with these conditions, either directly or indirectly

WHO Principles for Management of Chronic Illness
• National focus on population directed disease prevention & health promotion
• Structured, planned care for patients with long-term chronic conditions
• Information systems and registers to plan and evaluate care
• Support and strengthen self-care
• Shared care that is integrated across organisational boundaries
• Supportive clinical decision systems
• Care that is delivered in the appropriate setting
• Multidisciplinary teams used to provide care
• Monitoring and evaluation framework for chronic disease programmes.

Population Health

GP ENROLLED POPULATION RISK STRATIFICATION CARE PLANNINGCARE DELIVERY AND
CO-ORDINATION
SHARED CARE PATHWAYS AND PROTOCOLS
Primary Care Acute Care Social Care
Case Manage
Disease Manage
Self -manage
Register • Clinical
• Social
• Risk
GP
Practice Nurse
Community Nurse Specialist
HSCP
Community Pharmacist
HSE Integrated Care Programme for Prevention & Management of Chronic Disease
Source: HSE National Clinical & Integrated Care Programmes

Ambulatory Care Sensitive Conditions
• Good quality primary care can help prevent the need for hospital admission
• Well established treatment guidelines for these conditions
• Significant differences between Ireland and other countries & between counties in Ireland
• Will never eliminate need for hospital treatment but there is potential to significantly improve hospitalisation rates and the standard of care for these conditions.

Ambulatory Care Sensitive Conditions
• Chronic obstructive pulmonary disease (COPD)– 381 hospitalisations per 100,000 population in 2014– 12,389 hospital stays consuming 107,467 bed-days – Equivalent of 300 acute beds– Slight increase in age standardised hospitalisation, 2005-2014
• Asthma– 41 hospitalisations per 100,000 population in 2014– 1,433 hospital stays consuming 6,953 bed-days – 25% reduction between 2005 and 2014
• Diabetes– 129 hospitalisations per 100,000 population in 2014

Healthy Ageing
Source: WHO Report on Ageing and Health, 2015

A RESPONSE TO LONG-TERM COMPLEX CARE
Integration is a fundamental principle of design rather than a system of delivery as a response to long term, complex care.
COMMUNITY DELIVERED It is community delivered but integrated across all agencies and services.
CORE ELEMENTS ARE
FUNDAMENTAL TO
INTEGRATED CARE
• Population stratification of risk (and case finding) • Anticipatory Care Planning (based on common assessment)• Care co-ordination by a case manager (with agreed care pathways)
LOCAL CONDITIONS Local conditions for Integrated care to flourish needs to be created from bottom up but incentivised from top down.
IMPLEMENTATION IS
TYPICALLY BY ‘PIONEERS’Implementation is typically by ‘pioneers’ leading on change model with dissemination and innovation as the lessons are scaled up
HSE Integrated Care Programme for Older People
Source: HSE National Clinical & Integrated Care Programmes

What does this mean for hospitals?
• Much of a hospital’s effort must be on prioritising activities and resources that will keep people out of hospital through ambulatory care, diagnostics, day hospitals, etc.
• Stronger partnerships with primary care & social care
• Evolution from episodic reactive response to supporting population health models of care which provide greater integration, continuity & coordination of care

What does this mean for hospitals?
• Effective management of unscheduled care will require prevention of admissions through partnering with primary and community care in addressing chronic conditions and frail elderly
• For elective and specialist we will need to continue to redesign national and regional clinical pathways to improve quality and efficiency


What does this mean for policy, programmes and practice generally?✓National focus on population directed disease
prevention & health promotion covering physical and mental health
✓Greater focus on population health and demographics in planning and delivering services
✓Support for self-care and primary care based strategies
✓Social care policy and service development to provide greater clarity on financing, entitlements, regulation and choice to support independence

What does this mean for policy, programmes and practice generally?✓Linkage between providers through greater
shared care across organisational boundaries
✓Multidisciplinary teams used to provide care
✓Supportive clinical decision systems
✓Outcomes-based monitoring and evaluation framework

What does this mean for Plans & Investment Strategies?
• Capacity review underway across primary, acute and continuing care services & across both public and private sectors
• Will identify current & future capacity constraints to 2030
• But based upon transitioning to a future-proofed model rather than simply extrapolating the current one
• The Capacity Review and the eHealth Strategy will inform decisions on the Government’s Mid Term Capital Review later this year

Thank you!







![Teresa M. [Breslin] DeLellis, PharmD, BCPS, BCGPatomalliance.org/.../2019/01/DeLellis_CV_11_2018.pdf · DeLellis 1 Teresa M. [Breslin] DeLellis, PharmD, BCPS, BCGP 1021 Woodland Pass](https://static.fdocuments.net/doc/165x107/5fba322bc915c30e9e04ab57/teresa-m-breslin-delellis-pharmd-bcps-delellis-1-teresa-m-breslin-delellis.jpg)