Plan B - GP Voicegpvoice.com.au/wp-content/uploads/2018/11/5_2018InjectablesInsulin... · Dr...
29
Plan B Dr Manoharan
Transcript of Plan B - GP Voicegpvoice.com.au/wp-content/uploads/2018/11/5_2018InjectablesInsulin... · Dr...

Plan B
Dr Manoharan

• Severe side effects from GLP1 • History of severe GI symptoms • History of severe pancreatitis • HbA1c still high despite GLP1 • HbA1c deteriorating after initially responding • HbA1c very high at oral failure • SMBG profile shows large excursion • Presented with symptomatic hyperglycaemia • Wants to go straight to insulin


The Injectables
Glucagon Like Peptide 1 Insulins

Insulin Defect

Insulin – what does it do?
• Increase peripheral glucose uptake: Muscles Adipose tissues
• Reduce gluconeogenesis: Hepatic Renal
• Increase protein synthesis & Inhibit proteolysis • Increase lipogenesis and inhibits lipolysis

Insulin development
• Initial insulins had to be given multiple times. • Animal insulins with longer half lives were used • Semi-synthetic insulins: Porcine insulin were converted into human insulin by
one amino acid substitution • Recombinant DNA human insulin was first used in 1978 • Protamine and/or Zinc added to increase half-life • Modification of the site of amino acids in the insulin changed the
pharmacokinetics - insulin analogues – rapid or basal • Newer insulins utilised chains of insulin molecules which resist degradation to
increase insulin duration of action and smoother pharmacodynamic profiles

Insulin types
Prandial Short-acting Rapid acting Basal Intermediate acting Long acting Ultra long acting Mix Basal + prandial

Insulins
Rapid acting
Lispro (Humalog®) Aspart (NovoRapid®) Glulisine (Apidra®)
Intermediate acting
NPH Determir
Long Acting
Glargine U100
Start: 5-15 mins Peak: 1 hour Last 3.5-4.5 hours
Start: 1-3 hours Last 12-16 hours
Start: 1-2 hours Peak: none Last ~24 hours
Ultra Long Acting
Start: 1-2 hours Peak: none Last >24 hours
Degludec Glargine U300
Short Acting Actrapid® Humulin R® Start: 30 mins Peak: 2-5 hour Last 6-8 hours

10
Limitations of premixed insulins and a basal-plus insulin regimen
1. Kruszynska YT, et al. Diabetologia. 1987; 30: 16–21. 2. Atkin S, et al. Ther Adv Chronic Dis. 2015; 6: 375–88.
Physiological insulin profile Bolus insulin Basal insulin Premixed insulin
Physiological insulin profile comprises a basal component with meal-related peaks1
Limitations of a basal-plus insulin regimen:2
• Burden of multiple injections • Complex titration schedule
Limitations of premixed insulins due to protamination:2
• Variability in glycaemic control • Incomplete 24-hour basal coverage • Need for re-suspension

WHAT’S THE DIFFERENCE BETWEEN TOUJEO (insulin glargine 300 units/mL) AND LANTUS (insulin glargine 100 units/mL)?
Toujeo is a formulation of insulin glargine containing 3-times the amount per mL as Lantus ● The same unit amount in one-third the volume1
The reduced surface area of the Toujeo depot provides: ● a more prolonged and sustained release of insulin glargine compared
with Lantus1-4
● more stable, predictable and prolonged activity profile than Lantus1-4
Lantus® Toujeo®
Reduction of volume by 2/3 Reduction of depot surface
Toujeo® Lantus®

TOUJEO: MORE STABLE AND PROLONGED ACTIVITY VS INSULIN GLARGINE 100 units/mL1,2
12
SMOOTH PROFILE AND STABLE ACTIVITY FOR AT LEAST 24 HOURS1,2
1. Becker RHA et al. Diabetes Care 2015; 38(4):637–43. 2. Toujeo Approved Product Information.
Pharmacodynamics Even steady-state profile
Prolonged duration of action
Pharmacokinetics Reduced fluctuation in
insulin exposure
Constant activity over 24 h
Adapted from Becker RHA et al. Diabetes Care 2015.1
Toujeo 0.4 units/kg (n=16)
Insulin glargine 100 units/mL 0.4 units/kg (n=17)
Glu
cose
infu
sion
rate
(m
g/kg
/min
)
Time after subcutaneous injection (h)
Presenter
Presentation Notes
This graph shows the glucose infusion rate of Lantus in type 1 diabetes.1 Superimposed on that is Toujeo, showing a smoother profile and stable activity with a prolonged duration of action (at least 24 h) compared with Lantus. The graph also reflects the pharmacokinetics with: insulin exposure demonstrated out to 32 h reduced fluctuation in insulin exposure.1 These results are from a double-blind, crossover study in 30 individuals with type 1 diabetes (n=30) using a euglycaemic clamp over 36 hours. Individuals were randomised to receive either Toujeo or Lantus at clinically relevant doses.1,2 References Becker RHA et al. Diabetes Care 2015; 38(4):637–43. Toujeo Approved Product Information.

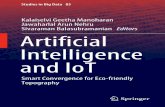
TOUJEO: SMOOTHER 24-H GLUCOSE PROFILE VS INSULIN GLARGINE 100 units/mL1
13
POOLED AVERAGE GLUCOSE PROFILES1
Insulin glargine 100 units/mL 1.6
mmol/L
Difference between minimum and maximum
values
Toujeo 0.8 mmol/L
Toujeo (n=30) Insulin glargine 100 units/mL (n=29)
1. Bergenstal RM et al. Diabetes Care 2017; 40(4):554–60.
Adapted from Bergenstal RM et al. Diabetes Care 2017.1
Mea
n (±
SE) g
luco
se
over
all (
mm
ol/L
)
Time (h)
Study Design: Exploratory, 16-week, exploratory, open-label, parallel-group, two-period cross-over study using continuous glucose monitoring in 59 individuals with type 1 diabetes. Individuals were randomised to receive either Toujeo or Lantus once-daily either morning or evening for 8 weeks before switching to the alternate schedule (morning or evening) for a further 8 weeks. The primary efficacy outcome of time in range (4.4–7.8 mmol/L) during the last 2 weeks of each treatment period, as measured by continuous glucose monitoring, was not met (p=0.73).
Presenter
Presentation Notes
This graph shows the glucose infusion rate of Lantus in type 1 diabetes.1 Superimposed on that is Toujeo, showing a smoother profile and stable activity with a prolonged duration of action (at least 24 h) compared with Lantus. The graph also reflects the pharmacokinetics with: insulin exposure demonstrated out to 32 h reduced fluctuation in insulin exposure.1 These results are from a double-blind, crossover study in 30 individuals with type 1 diabetes (n=30) using a euglycaemic clamp over 36 hours. Individuals were randomised to receive either Toujeo or Lantus at clinically relevant doses.1,2 References Becker RHA et al. Diabetes Care 2015; 38(4):637–43. Toujeo Approved Product Information.

“Mix” Insulins
Brand Intermediate Rapid
Novomix 30 Protamine 70% Aspart 30% Analogue
Humalog 25 Protamine 75% Lispro 25% Analogue
Humalog 50 Protamine 50% Lispro 50% Analogue
Mixtard 30/70 Isophane 70% Neutral 30% Human
Humulin 30/70 Isophane 70 Neutral 30% Human
Mixtard 50/50 Isophane 50% Neutral 50% Human
Analogues Novomix 30/70 Humalog 25/75 Humalog 50/50
Human Mixtard 30/70 Humulin 30/70 Mixtard 50/50

“Co-formulation”
Ultra-long acting + rapid acting insulin

16
A unique combination of a new ultra-long acting insulin (degludec) + the world’s number 1 prescribed bolus insulin (aspart)1-4
In the subcutaneous depot
Slow dissociation
Subcutis
Capillary
Rapid dissociation
degludec aspart
degludec di-hexamers
aspart hexamers
In the formulation
Ryzodeg® 70/30 = degludec (70%) + aspart (30%) existing separately in one formulation
1. Ryzodeg® 70/30 Product Information. 2. Internal calculations based on QuintilesIMS database. QuintilesIMS MMIDAS (Feb 2017) 3. Haahr H, Fita EG, Heise T. Clin Pharmacokinet. 2017; 56(4): 339-54. 4. Havelund S, et al. Pharm Res. 2015; 32: 2250-8
Presenter
Presentation Notes
Ryzodeg® 70/30is the first co-formulation. It is composed of 70% IDeg and 30% IAsp. The two insulins exist separately in the pen (IDeg as dihexamers and IAsp as hexamers). Upon injection into the subcutaneous space the IAsp hexamers rapidly dissociate and enter the blood stream, while IDeg forms multihexamer chains that slowly dissociate

17
Degludec and aspart exist separately in solution and the subcutaneous tissue1
1.00
0.90
0.80
0.70
0.60
0.50
0.40
0.30
0.20
0.10
0.00
4 5 6 7 8 9 10 11 12 13 14
degludec di-hexamer
aspart hexamer
Abs
orba
nce
units
Minutes
In solution In subcutaneous tissue
1. Havelund S, et al. Pharm Res. 2015; 32: 2250-8.
1.00
0.90
0.80
0.70
0.60
0.50
0.40
0.30
0.20
0.10
0.00
4 5 6 7 8 9 10 11 12 13 14
degludec multi-hexamer
Abs
orba
nce
units
Minutes
aspart monomer
Presenter
Presentation Notes
Size-Exclusion Chromatography Size-exclusion chromatography (SEC) was performed to characterize the association states for the individual basal and rapid-acting insulins, and for the combinations. Three SEC methods were used as in vitro models to simulate conditions in the pharmaceutical formulation (at high concentration of phenol and room temperature), the condition in the subcutaneous depot after injection (without phenol and at body temperature) and, finally, to evaluate a serial decrease in concentration of phenol and m-cresol, as expected to occur following subcutaneous injection. Furthermore, fractions of high and low molar mass were collected from the SEC eluents, and reverse-phase chromatography was used to measure the concentrations of the individual insulin within them. SEC method 1 was designed to simulate conditions in the pharmaceutical formulation (with the same phenol concentration), and was used to measure the percentage of oligomers of dihexamer, dihexamers, hexamers, and monomers with eluent of 16 mM phenol, 140 mM sodium chloride, 10 mM tris (hydroxymethyl) aminomethane (tris) pH 7.3, and 0.01% sodium azide at 23°C. The size-exclusion column used was ACQUITY UPLC® BEH200 (150*4.6 mm, d = 1.7 μm) from Waters Corporation, Milford, MA, USA. Ultraviolet detection wavelengths were at 286, 276 and 290 nm for methods 1–3, respectively. Injection volume was 20 μL and flow was 0.15 mL/min. SEC method 2 was designed to simulate conditions in the subcutaneous depot (in which phenol quickly dissipates), and was used to measure the percentage of multihexamer versus the hexamer–monomer fraction with a phenol-free eluent of 140 mM sodium chloride, 10 mM tris pH 7.3, 0.01% sodium azide, and 5% 2-propanol at 37°C. The concentrations of the individual insulin analogs in the multihexamer fraction and the hexamer–monomer fraction were determined by reverse-phase chromatography. A SymmetryShield RP18 (3.9*20 mm, d = 3.5 μm) column from Waters Corporation (Milford, MA, USA) was eluted with A: 10%(vol) acetonitrile 0.2 M sodium sulfate, 40 mM o-phosphoric acid adjusted to pH 3.6 with sodium hydroxide and B: 70%(vol) acetonitrile at a gradient of 20–54% at 1.4–5 min at 30°C, 1 mL/min, and detection at 276 nm. To avoid adsorption, 70 ppm polysorbate 20 was added to the fraction vials. For comparison, insulin detemir was combined with insulin aspart in the same proportions (volume 70:30) and stored for 4 weeks at 25°C. SEC method 2 was modified for the combination of insulin detemir and insulin aspart by dividing fraction collection between hexamer and dimer (since insulin detemir achieves its protracted absorption largely through reversible albumin binding rather than multihexamer formation). SEC method 1 was not employed for an insulin detemir and insulin aspart combination. This is because in the phenolic SEC eluent (similar to the pharmaceutical formulation), insulin detemir elutes as a hexamer [11, 15], as does insulin aspart, so the two insulin analogs (and any hybrid associations) would therefore be indistinguishable using this method. SEC method 3 was designed to simulate serial conditions at decreasing concentrations of the preservatives phenol and m-cresol, as will occur immediately after subcutaneous injection. These tests were made by mixing A: 16 mM phenol and m-cresol, 20 mM sodium chloride, 3 mM sodium dihydrogenphosphate pH 7.3, and 0.01% sodium azide, with B: 140 mM sodium chloride, 3 mM sodium dihydrogenphosphate pH 7.3, and 0.01% sodium azide at 37°C. Transformation of insulin degludec dihexamers to multihexamers, and of insulin aspart hexamers to monomers, was compared with human insulin. Abstract PURPOSE: To study the self-association states of insulin degludec and insulin aspart alone and combined in pharmaceutical formulation and under conditions simulating the subcutaneous depot. METHODS: Formulations were made of 0.6 mM degludec at 3 and 5 Zn/6 insulin monomers, and 0.6 mM aspart (2 Zn/6 insulin monomers). Self-association was assessed using size-exclusion chromatography (SEC) monitored by UV and orthogonal reverse-phase chromatography. RESULTS: Simulating pharmaceutical formulation, degludec eluted as dihexamers, whereas aspart eluted as hexamers and monomers. Combining degludec at low zinc with aspart increased dihexamer content, indicating hybrid hexamer formation. At high zinc concentration, however, there was no evidence of this. Simulating the subcutaneous depot by removing preservative, degludec eluted as multihexamers and aspart as monomers. Aspart was incorporated into the multihexamer structures when combined with degludec at low zinc, but there was no such interaction with high-zinc degludec. SEC using progressively diluted concentrations of phenol and m-cresol showed that dissociation of aspart into monomers occurs before the formation of degludec multihexamers. CONCLUSION: Insulins degludec and aspart can be combined without forming hybrid hexamers, but this combinability is dependent on zinc and preservative concentration, and requires that degludec is fully dihexameric before addition of aspart.

Short Acting Insulins
Start: 30 mins Peak: 2-5 hour Last 6-8 hours

Rapid Acting Insulins
Start: 5-15 mins Peak: 1 hour
Last 3.5-4.5 hours

Intermediate Acting Insulins
Start: 1-3 hours Peak: none
Last 12-16 hours

Long Acting Insulins
Start: 1-2 hours Peak: none
Last 20-24 hours

Ultra-Long Acting Insulins
Start: 1-2 hours Peak: none > 24 hours

What is the fuss with the new insulins?

24
Hypoglycaemia zone
Target zone
Average FPG
1 4 2 3 6 5 8 7 10 9 11 14 12 13 16 15 18 17 20 19 21 24 22 23 26 25 28 27 30 29
Day
FPG
(m
mol
/L)
54
90
36
18
144
108
126
162
180
198
216
72
FPG (m
g/dL)
3.0
5.0
2.0
1.0
8.0
4.0
6.0
7.0
9.0
10.0
11.0
12.0
Glucose variability predicts future risk of hypoglycaemia1
FPG, fasting plasma glucose. 1. Vora J & Heise T. Diabetes Obes Metab. 2013; 15: 701-12.
Presenter
Presentation Notes
Variability in blood glucose leads to patients experiencing periods of hyper- and hypoglycaemia.

Insulin + GLP1 agonist* or
SGLT2 inhibitors or
DPP4 inhibitors or
Pioglitazone
* Byetta only

What to watch for Hypoglycaemia
Weight gain
Lipodystrophy
Allergies to insulin

Insulin may be necessary when beta cells are gone
Insulins can either be
• short/rapid acting (prandial)
• Long/ultralong acting (basal)
• Mix insulin (basal + prandial)

Toujeo
Ryzodeg 70/30
Short acting
V-Go

Basal 10U at night? Prandial 10U at dinner?
Mix insulin 10U at dinner?