Placental Transport in Pathologic Pregnancies
41
Placental Transport in Pathologic Pregnancies Gernot Desoye Clinic of Obstetrics and Gynaecology Medical University, Graz Note: for non-commercial purposes only
Transcript of Placental Transport in Pathologic Pregnancies

Placental Transport in
Pathologic Pregnancies
Gernot Desoye
Clinic of Obstetrics and Gynaecology
Medical University, Graz
Note: for non-commercial purposes only

Most Common Pregnancy Pathologies
• Diabetes (T1D, T2D, GMD)fetal overweight
• Fetal growth restriction (FGR)fetal underweight

Body Composition at Delivery
• Fat mass: 12 – 15 %
• Lean body mass: 85 – 88 %

LGA AGA SGA
Bo
dy
Fat
(%
)
NGTGDMP=0.002 P=0.002
Fetal Body Fat is Increased in GDM Independent of Body Weight
Petersen 1988; Catalano AJOG 2003; Durnwald AJOG 2004
NGT Col 2 Col 3
LGA AGA
Fat
Fre
e M
ass
(g)
P=0.0009 P=0.0008
LGA AGA

Padoan et al, AJOG 2004
Fetal Body Fat is Reduced in FGR
FGR:Fetal AC < 2 SD
Abnormal Doppler:
A. umbilicalis
A. uterina
Fat mass
Leanbodymass
AGA
FGR

Fetal Growth
• Fat Free Mass / Lean Body MassGenetics
• Fat MassIntrauterine Environment
Moulton J Biol Chem, 1923Sparks Sem in Perinat, 1989

Substrates Driving Fetal Fat Growth
• Glucose Insulin
• Lipids

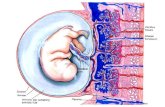
Placental Transport in Third Trimester
Glucose

Maternal-Fetal Glucose Relation is Linear
Biol Neonate 10: 227 (1966)

intervillousspace
fetalblood
ST ECCT
CT
EC
EC
ST
Pathways of Materno-Fetal Transport
Glucose:
* saturable* stereospecific* Na -indep.* GLUT1* mvm:bm ~ 3:1
* [gluc] >[gluc]m f

GLUT 1 in Term Placentas
Hahn et al, Cell Tiss Res 280, 1995

GLUT3
Term Placenta
Mol Hum Reprod 2001 7:1173 JCEM 1998 83:4097
GLUT4

Hyperglycemia in vitro induces GLUT1 translocation in
term human trophoblasts(Hahn et al., Diabetologia 43: 173, 2000)
Hyperglycemia in vitro downregulates glucose uptake
and GLUT1 in human term trophoblasts(Hahn et al., FASEB J 12: 1221, 1998)
Placental Glucose Transportersin vitro Regulation

external glucose [mM]
0 5 10 15 20 25
rate
[fm
ole
s/s
per
cel
l]
0
10
20
30
40
50 5.5 mmol/l glucose 25 mmol/l glucose
*
*
Hyperglycemia Downregulates Trophoblast Uptake of High Glucose Levels Only
Hahn et al, FASEB J 1998

D-g
luco
se(m
mol
.min
-1.to
tal p
lace
ntal
wei
ght-1
)
0
50
100
150
200
250
300 Control
Diet Insulin
GDM
Total Transplacental NetTransfer of Glucose Unaltered in GDM
Osmond et al, Diabetologia 2001
Maternal glucose: 8 mM

Transplacental Glucose Flux
• Depends on the MATERNAL-FETAL concentration gradient
• Is flow limited

onTransplacental Glucose Flux Depends
Maternal and Fetal Blood Flow
Illsley et al, Trophoblast Res. 2, 535, 1987

Placental Glucose Transport in FGR
• Maternal-fetal transfer is unaltered(Challis DE et al, Ped Res 47: 309, 2000)
• GLUT1 expression is unaltered(Jansson T et al, JCEM 77: 1554, 1993)

Placental Transport in Third Trimester
Lipids

Lipids
Apoproteins
Cholesterol/esters
Triglycerides
Phospholipids
Vitamins
• Free fatty acids
• Lipoproteins

Fetal Plasma
TAGPhospholipidsSphingolipidsCholesterol
Free fatty acid
Albumin Complex
FABP
Oxidation•Mitochondria•Peroxisome
Lipid resynthesis•TAG•Phospholipids•Sphingolipids•Cholesterol
Free fattyacid
Signal transduction• Gene regulation• Other biologicalactivity
Free fatty acid
MaternalPlasma
FATP
FAT/CD36
FABPpm
Diffusion
Albumin Complex
Albumin Binding Protein
Dissociation
FAT/CD36
FATP
Diffusion
EL Hydrolysis
Lipoprotein
Lipoprotein Receptor

Maternal circulation
Placenta
Fetal circulation
Placental Lipid Handling
Free fatty acid
Albumin Complex
Albumin Binding Protein
Dissociation
LP Hydrolysis
Lipoprotein
Lipoprotein Receptor
L
I
P
A
S
E

Triglyceride Lipase Gene Family
---Pancreatic LipasePL
--+/-Hepatic LipaseHL
--+Lipoprotein LipaseLPL
+++++++++Endothelial LipaseEL
ECTTFTlipase
Gauster et al, JCEM 92: 2256-63 (2007)

EL and LPL Localisation
Gauster et al, JCEM 92:2256 (2007)
EL LPL control

0.0
0.5
1.0
1.5
2.0
2.5
EL LPL
lipas
e / R
PL
30 m
RN
A c
op
ies
AGAFGR*
*
modified from Gauster et al, JCEM 92: 2256-63 (2007)
EL and LPL Expression is Alteredin FGR Placentas

Maternal circulation Placenta Fetal circulation
Placental Lipid Handling
Lipo-
ProteinsELHDL
LDL
HDL

PLTG
Lipid dropletsv
FA &FC pool
lipase
CE-hydrolase
Maternal circulation Placenta Fetal circulation
Pathways of PlacentalLipid Metabolism
SR-BI
HDL
HDL
CE
A-I
A-I
Selective pathway
?
?
?
LDLEndocytic pathway
LDL receptor CEACAT

LDLR mRNA expression in placenta
0
0,2
0,4
0,6
0,8
1
1,2
Rat
io L
DL
R/L
30 (
no
rmal
ised
)P < 0.05
LDL-R Expression in FGR and GDM
AGA GDMFGR1 2 + 3
Wadsack et al, AmJPhysiol 292: 476 (2007)

SR-BI Protein in FGR
Rat
io S
RB
-I/ ββ ββ
-act
inp
rote
inex
pr e
ssio
n(n
orm
aliz
ed)
AGA FGR 1 FGR 2+30.0
0.5
1.0
1.5
2.0
2.5 p=0.03
p=0.07
Wadsack et al, AmJPhysiol 292: 476 (2007)

SR-BI is Upregulated in Diabetes only at Term of Gestation
term of gestation
control T1D
[au
]
0.0
0.5
1.0
1.5
2.0
2.5 p=0.028
first trimester
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
control T1D
[au
]
control GDM
[au
]
0
1
2
3
4 p=0.002
T1D
GDM
Wadsack et al, unpublished

Placental SR-BI expression levels do not correlate with:
• Gestational age
• Fetal weight• Placental weight• Maternal BMI• Fetal BMI
• HDL
Correlation placental weight vs SR-BI over all groups
y = 0.6812x + 0.8884
R2 = 0.0399
0.00
0.50
1.00
1.50
2.00
2.50
3.00
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8
Placental weight [kg]
SR
-BI
arb
itra
ry u
nit
s
Correlation fetal weight vs SR-BI over all groups
y = 0.0938x + 0.9519
R2 = 0.0287
0.00
0.50
1.00
1.50
2.00
2.50
3.00
0 1 2 3 4 5
Fetal weight [kg]
SR
-BI
arb
itra
ry u
nit
s
Wadsack et al, unpublished

LDL-receptorrelated receptor
proteinLRP
apo E-binding protein
- APO-E VLDL- Chylomicron remnants
mainly expressed in:
liver, brain and placenta

n.s.
n.s.n.s.
AGA IUGR GDM1 2 + 3
LRP Expression in FGR and GDM
0.0
0.5
1.0
1.5
2.0
2.5
Rat
io L
RP
/L30
exp
ress
ion
(no
rmal
ized
to K
+)p= 0.03
n.s.
Wadsack et al, AmJPhysiol 292: 476 (2007)
FGR

Summary
• Transplacental glucose flux is dictated byconcentration gradient and blood flow
• Glucose transport is unaltered in GDM and FGR
• Lipid hydrolysis and uptake into trophoblast arereduced only in severe forms of FGR
• No information available about overall lipidtransport/transfer in FGR and GDM

Univ. Milano
I. Cetin V. CozziS. Tabano
Med. Univ. Graz
A. BlaschitzM. GausterT. HahnU. HidenI. LangC. Wadsack
Univ. San Pablo, Madrid
E. HerreraH. Ortega

Thank you !

Maternal-Fetal Glucose Gradientis Elevated in FGR vs AGA
AGA FGR0
0.2
0.4
0.6
0.8
1
1.2
1.4
mM
1 2 3
*
**
Marconi et al, Obstet Gynecol, 1996
Maternal glucose concentration is unchanged!

Maternal and Umbilical Cord Glucose in GDM
Radaelli BJOG, 116, 1729 (2009)
mother fetus
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
mm
ol/l
venous arterial
umbilical cordV - A
**

PLTG
Lipid dropletsv
FC poollipase
CE-hydrolase
Maternal circulation Placenta Fetal circulation
Pathways of PlacentalCholesterol Metabolism
Steroidproducts
SR-BI
HDL
HDL
CE
A-I
A-I
Selective pathway
?
?
?
LDLEndocytic pathway
LDL receptor CEACAT

LGA AGA SGA
Bo
dy
Fat
(%
)
NGTGDMP=0.002 P=0.002
NGT Col 2 Col 3
LGA AGA
Fat
Fre
e M
ass
(g)
P=0.0009 P=0.0008
Fat and Fat-free Mass
in Offspring of Women with GDM
Petersen 1988; Catalano AJOG 2003; Durnwald AJOG 2004

LGA AGA SGA
Bo
dy
Fat
(%
)
NGTGDMP=0.002 P=0.002
Fetal Body Fat is Increased in GDM Independent of Body Weight
Petersen 1988; Catalano AJOG 2003; Durnwald AJOG 2004