![Optimization of HILIC method for the analysis of bisoprolol …scindeks-clanci.ceon.rs/data/pdf/0004-1963/2014/0004...98 hydrochlorothiazide in tablet formulation [14, 15, 16], and](https://static.fdocuments.net/doc/165x107/6087a24e6dec0a790821a8e0/optimization-of-hilic-method-for-the-analysis-of-bisoprolol-scindeks-98-hydrochlorothiazide.jpg)
PIONEERING THE CHANGE IN HYPERTENSION …theblackcedar.com/downloads/3Bicedolol.pdf · Low-dose...
19
BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE Page | 1 BLACKCEDAR PHARMACEUTICALS LTD. PIONEERING THE CHANGE IN HYPERTENSION THERAPY IN NIGERIA WITH BICEDOLOL® Bisoprolol Fumarate 5mg & Hydrochlorothiazide 6.25mg HIGH EFFICACY - LOW DOSAGE With low-dose combination therapy BICEDOLOL® provides classic antihypertensive benefits of beta-blockers and diuretics without their dose- related side effects.
Transcript of PIONEERING THE CHANGE IN HYPERTENSION …theblackcedar.com/downloads/3Bicedolol.pdf · Low-dose...

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 1
BLACKCEDAR PHARMACEUTICALS LTD.
PIONEERING THE CHANGE IN HYPERTENSION
THERAPY IN NIGERIA WITH
BICEDOLOL® Bisoprolol Fumarate 5mg & Hydrochlorothiazide 6.25mg
HIGH EFFICACY - LOW DOSAGE
With low-dose combination therapy BICEDOLOL® provides classic
antihypertensive benefits of beta-blockers and diuretics without their dose-
related side effects.

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 2
TABLE OF CONTENT DRUG EVALUATION & RESEARCH RECOMMENDATION ...................................................................... 3
FIRST LINE TREATMENT IN HYPERTENSION ........................................................................................ 4
CLINICAL TRIALS ................................................................................................................................... 5
RESPONSE RATE UP TO 73% ................................................................................................................ 6
ADVERSE EVENTS COMPARABLE TO PLACEBO .................................................................................... 7
REDUCTION IN DIASTOLIC BLOOD PRESSURE ..................................................................................... 8
REDUCTION IN SYSTOLIC BLOOD PRESSURE ....................................................................................... 9
RESPONSE & SAFETY PROFILE VS. ACE INHIBITORS & CA-ANTAGONISTS ......................................... 10
LOWEST DISCONTINUATION RATES .................................................................................................. 11
EFFICACY REGARDLESS OF AGE, RACE OR GENDER .......................................................................... 12
NOTIFICATION DELIVERED BY NAFDAC ............................................................................................. 13
ABSTRACTS ........................................................................................................................................ 14
ABSTRACTS ........................................................................................................................................ 15
ABSTRACTS ........................................................................................................................................ 16
ABSTRACTS ........................................................................................................................................ 17
REFERENCES ...................................................................................................................................... 18
CONTACTS ......................................................................................................................................... 19
BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 3
DRUG EVALUATION & RESEARCH RECOMMENDATION
BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 4
FIRST LINE TREATMENT IN HYPERTENSION BICEDOLOL® is recommended by Drug Evaluation and Research (DER) and approved by NAFDAC for
the treatment of mild to moderate essential hypertension.
The combination & dosage in BICEDOLOL® is Recommended as a first line treatment in hypertension
by the American Joint National Committee on Prevention, Detection, Evaluation & Treatment of High
Blood Pressure.
It is recommended by NAFDAC’s Drug Evaluation & Research Unit for the treatment of mild to
moderate essential hypertension.
BLACKCEDAR PHARMACEUTICALS LTD is pioneering this change in Hypertension therapy in Nigeria
with BICEDOLOL®.
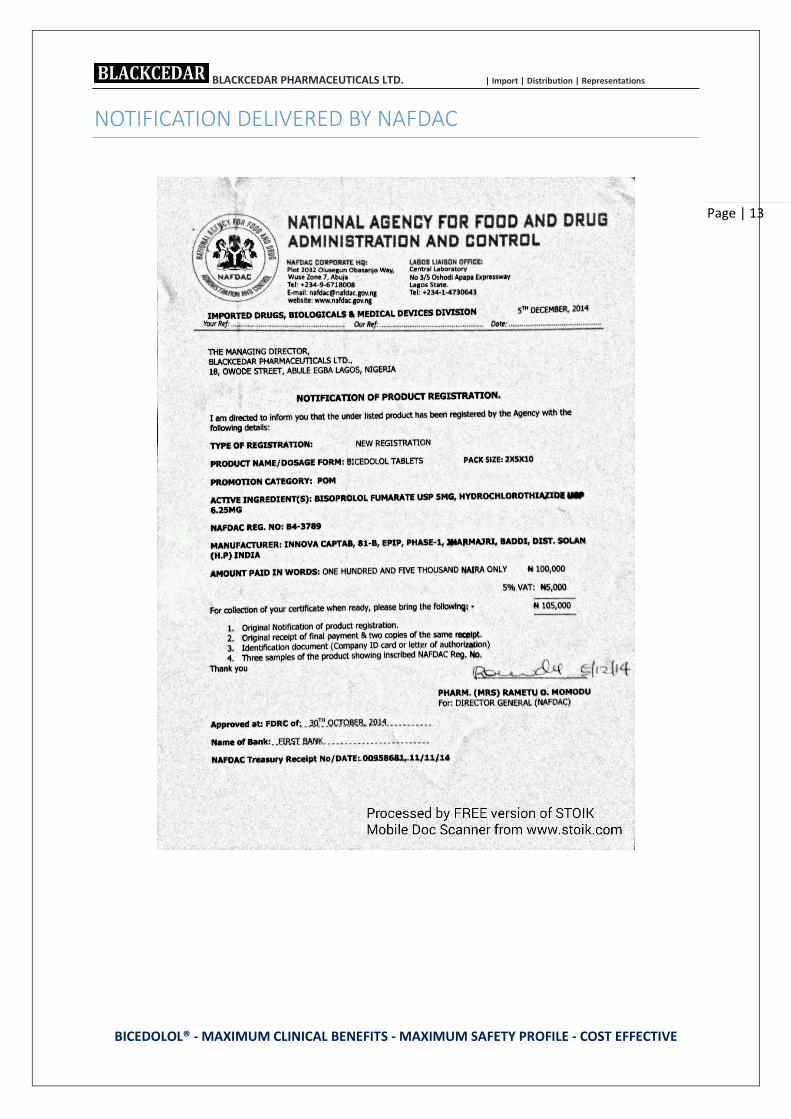
BICEDOLOL® was approved by NAFDAC in December 2014 for the treatment of hypertension.
HIGH EFFICACY Control of hypertension in up to 84% of patients
Effective in a broad range of patients regardless of age,
race or gender
Recommended by the JNC VI and other guidelines
Approved by NAFDAC as treatment of mild to moderate
essential hypertension
Approved by the FDA as first-line treatment of
hypertension
LOW RATE OF ADVERSE EVENTS Low-dose drug
Specifically developed to minimize dose-related side
effects
Side-effect profile comparable to placebo
MULTI-ACTIVE MODE OF ACTION Additive antihypertensive efficacy
Blood pressure reduction via different mechanisms
Metabolically neutral
IMPROVED COMPLIANCE Improvement in quality of life
Once-daily dosage (consistent 24 hour-efficacy)
Low discontinuation rates
Changes in Hypertension Therapy
Basic antihypertensive therapy with
high efficacy & low side effects
BICEDOLOL®

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 5
CLINICAL TRIALS
The US National Hypertension Trial with 12’629 patients confirmed positive data of BICEDOLOL®
(Bisoprolol Fumarate 5mg + HCTZ 6.25 mg) regarding efficacy, side-effects profile and quality of life in
actual clinical practice under usual care conditions.
Frishman et al, 1994-
Benetos et al, 2000 - 164
Papademetriou et al, 1998 - 75Neutel et al, 1996 -
Frishman et al,
Prisant et al , 1995 -
RANDOMIZED, DOUBLE BLIND TRIALS
Frishman et al , 1994 Benetos et al, 2000 Papademetriou et al, 1998
Neutel et al, 1996 Frishman et al , 1995 Prisant et al , 1995
BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 6
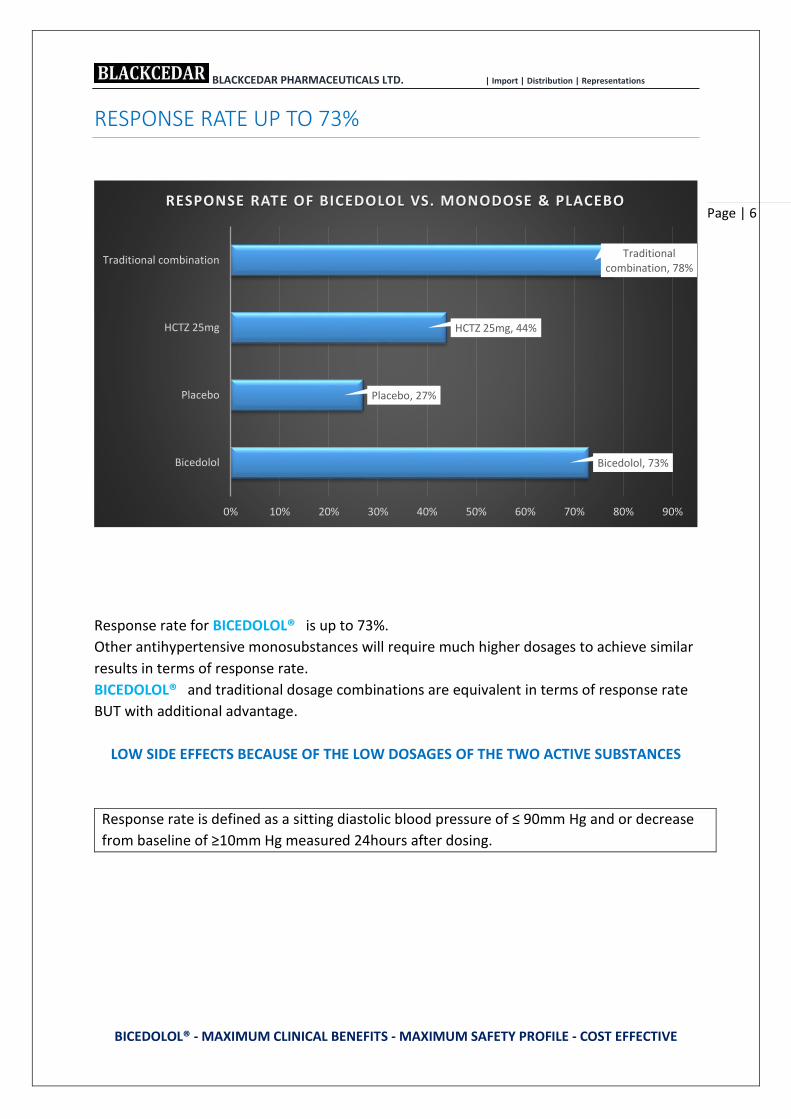
RESPONSE RATE UP TO 73%
Response rate for BICEDOLOL® is up to 73%.
Other antihypertensive monosubstances will require much higher dosages to achieve similar
results in terms of response rate.
BICEDOLOL® and traditional dosage combinations are equivalent in terms of response rate
BUT with additional advantage.
LOW SIDE EFFECTS BECAUSE OF THE LOW DOSAGES OF THE TWO ACTIVE SUBSTANCES
Response rate is defined as a sitting diastolic blood pressure of ≤ 90mm Hg and or decrease
from baseline of ≥10mm Hg measured 24hours after dosing.
Bicedolol, 73%
Placebo, 27%
HCTZ 25mg, 44%
Traditional combination, 78%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Bicedolol
Placebo
HCTZ 25mg
Traditional combination
RESPONSE RATE OF BICEDOLOL VS. MONODOSE & PLACEBO

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 7
ADVERSE EVENTS COMPARABLE TO PLACEBO
In all clinical trials including more than 14’000 patients BICEDOLOL® (Bisoprolol Fumarate 5mg
+ HCTZ 6.25mg) demonstrated a side-effect profile comparable to placebo on a minimum level.
0% 2% 4% 6% 8% 10% 12%
Bicedolol
Placebo
INCIDENCE OF ADVERSE EVENTSBICEDOLOL VS. PLACEBO
Rash Cough Diarrhea Bradycardia Dyspepsia Nausea Dizziness Asthenia Edema Headache

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 8
REDUCTION IN DIASTOLIC BLOOD PRESSURE
Therapy with BICEDOLOL® produced significant reductions from baseline sitting diastolic blood
pressure than placebo.
The mean reduction in SiDBP was also greater for patients taking BICEDOLOL® versus HCTZ alone in
a much higher dosage.
The low-dosed antihypertensive therapy with BICEDOLOL® results in a strong blood pressure
reduction with a side-effect profile comparable to placebo.
12.6
3.9
10.9
8.4 8.4
0
2
4
6
8
10
12
14
1
REDUCTION FROM BASELINE DIASTOLIC PRESSURE (mm Hg)
Bicedolol Placebo Bisoprolol 10mg Bisoprolol 2.5mg HCTZ 25mg
BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 9
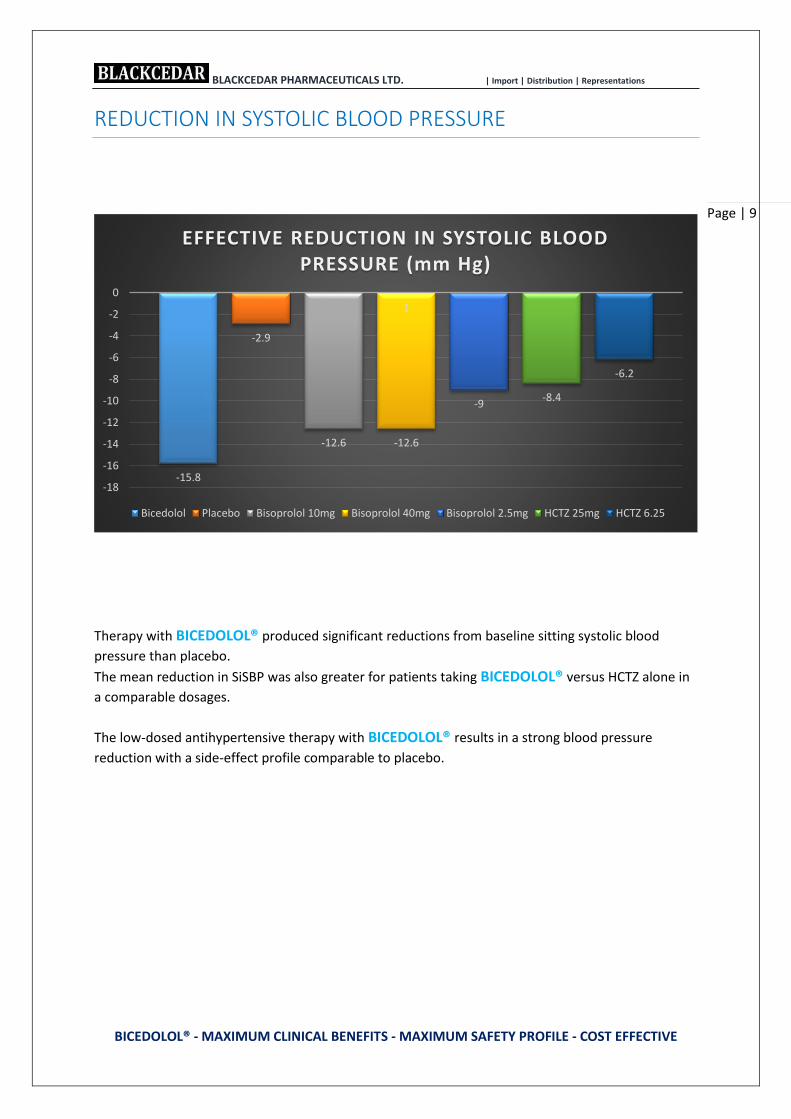
REDUCTION IN SYSTOLIC BLOOD PRESSURE
Therapy with BICEDOLOL® produced significant reductions from baseline sitting systolic blood
pressure than placebo.
The mean reduction in SiSBP was also greater for patients taking BICEDOLOL® versus HCTZ alone in
a comparable dosages.
The low-dosed antihypertensive therapy with BICEDOLOL® results in a strong blood pressure
reduction with a side-effect profile comparable to placebo.
-15.8
-2.9
-12.6 -12.6
-9-8.4
-6.2
-18
-16
-14
-12
-10
-8
-6
-4
-2
0
1
EFFECTIVE REDUCTION IN SYSTOLIC BLOOD PRESSURE (mm Hg)
Bicedolol Placebo Bisoprolol 10mg Bisoprolol 40mg Bisoprolol 2.5mg HCTZ 25mg HCTZ 6.25
BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 10
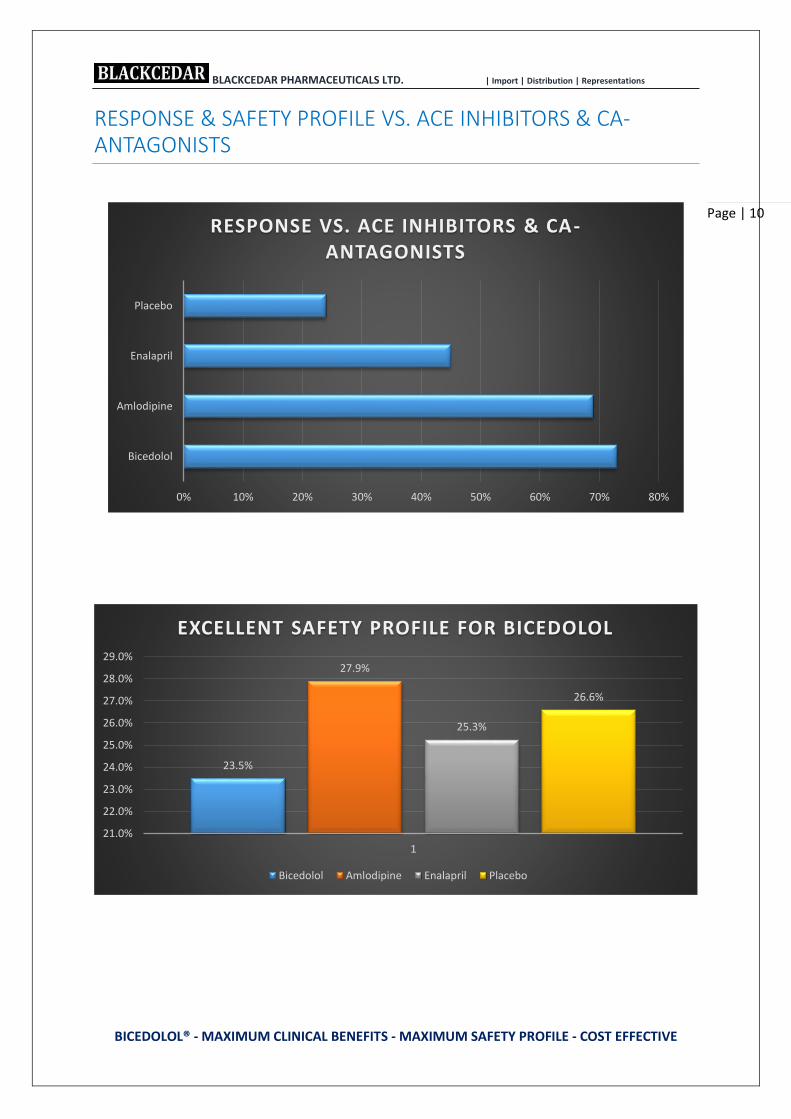
RESPONSE & SAFETY PROFILE VS. ACE INHIBITORS & CA-ANTAGONISTS
0% 10% 20% 30% 40% 50% 60% 70% 80%
Bicedolol
Amlodipine
Enalapril
Placebo
RESPONSE VS. ACE INHIBITORS & CA-ANTAGONISTS
23.5%
27.9%
25.3%
26.6%
21.0%
22.0%
23.0%
24.0%
25.0%
26.0%
27.0%
28.0%
29.0%
1
EXCELLENT SAFETY PROFILE FOR BICEDOLOL
Bicedolol Amlodipine Enalapril Placebo

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 11
LOWEST DISCONTINUATION RATES
Discontinuation rates for BICEDOLOL® were lowest in comparative studies vs Amlodipine, Enalapril
and placebo due to adverse events, lack of efficacy (Blood Pressure not controlled) as well as due to
other reasons.
A total of only 16.6% of patients who were treated with BICEDOLOL® discontinued therapy, 26.6% of
patients under Amlopdipine and 26.1% patiens under Enalpril.
Placebo treatment resulted in a discontinuation rate of 58.2%,including 41.8% due to lack of efficacy
(Neutel et al., 1996)
Discontinuation rates for BICEDOLOL® were also lower compared to ACE inhibitors due to adverse
events 7.1% for BICEDOLOL® vs. 9.5% for ACE inhibitors, due to lack of efficacy 2.7% vs. 5.6% and due
to administrative and other reasons 16.7% vs. 17.9%, in total 26.5% vs. 33.0% (Frishman, 1996)
0.0% 5.0% 10.0% 15.0% 20.0% 25.0% 30.0% 35.0% 40.0% 45.0%
Adverse Event
Lack of Efficiency
Others
LOWEST DISCONTINUATION RATE FOR BICEDOLOL
Placebo Enalapril Amlodipine Bicedolol

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 12
EFFICACY REGARDLESS OF AGE, RACE OR GENDER
AGE: BICEDOLOL® allows low-dose therapy in elderly patients, who are paricularly sensitive to the
effects of blood pressure manipulation and medication side effects as a result of the physiological
changs due to aging. Thus all age-groups may benefit from the low incidence of side effects of
BICEDOLOL®
RACE: BICEDOLOL® addresses the physiological mechanism of hypertension (low renin and volume
expansion) common among the black population, and therefore produces effects which are as high
as those observed in non-black population.
73%69%
81%
64%
86%
75% 73%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1
SIGNIFICANT EFFICACY REGARDLESS OF AGE, RACE OR GENDER
All patients <60 years >60 years Male Female Black Non Black
BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 13
NOTIFICATION DELIVERED BY NAFDAC

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 14
ABSTRACTS J Natl Med Assoc. 1996 Mar; 88(3):171-5. Saunders E1, Neutel J.
A new antihypertensive strategy for black patients: low-dose multi-mechanism therapy.
Abstract: Hypertension poses serious health risks for blacks because this population presents with earlier onset and more
severe forms of the disease than do nonblack. Although diuretics are the cornerstone of antihypertensive therapy In the
black population, investigators have expressed concern about adverse metabolic effects, such as hypokalaemia, produced
by the high doses of diuretics traditionally prescribed for blacks.
Recent evidence suggests that black patients may respond equally well to the new generation of cardio selective beta-
blockers and angiotensin-converting enzyme inhibitors, particularly when these agents are used together with a diuretic.
A new low-dose multi-mechanism agent that combines the cardio selective beta-blocker Bisoprolol Fumarate with
hydrochlorothiazide, a benzothiazine diuretic, is now available for first-line therapy for hypertension.
Results of two US multicentre trials--including a subset analysis of black patients--indicate that the once-daily agent is highly
effective in reducing diastolic and systolic blood pressure throughout a 24-hour period in both black and nonblack patients.
The agent is well tolerated in blacks and non-blacks and has a side-effect profile comparable to placebo. Because of its
efficacy and safety in black patients, Bisoprolol Fumarate/-hydrochlorothiazide is an appropriate therapeutic option for
first-line therapy of hypertension in the black population.
--------------------------------------------------------------------------------------------------------
Angiology. 2009 Oct-Nov; 60(5):601-7. doi: 10.1177/0003319708324926. Epub 2008 Nov 21.
Papadopoulos DP1, Papademetriou V.
Low-dose fixed combination of Bisoprolol/hydrochlorothiazide as first line for hypertension: a review of the rationale
and clinical evidence.
Abstract: Essential hypertension is a heterogeneous multifactorial disease. Data from the National Health and Nutritional
Examination Survey and from the World Health Organization have clearly demonstrated that, worldwide, less than 30% of
hypertensive patients are adequately controlled by our currently accepted blood pressure goals. Although monotherapy is
often unable to achieve blood pressure goals, the use of fixed low-dose combination drugs as alternative treatment seems
to be related to a better antihypertensive efficacy and higher response rates in the low range of doses as the result of
complementary mechanisms of antihypertensive effects. Indeed clinical trials have shown that initial low-dose combination
therapy is superior as compared with treatment by the stepped-care and the sequential monotherapy approach, while
recently, low-dose combination therapy for initial antihypertensive therapy instead of the stepped-care approach or of
sequential monotherapy has been recommended. This review summarizes the beneficial effect of low-dose bisoprolol/
hydrochlorothiazide combination in the treatment of patients with stage I and II hypertension
--------------------------------------------------------------------------------------------------------- Clin Cardiol. 1993 Oct; 16(10):732-6. ; Lewin AJ1, Lueg MC, Targum S, Cardenas P.
A clinical trial evaluating the 24-hour effects of bisoprolol/hydrochlorothiazide 5 mg/6.25 mg combination in patients
with mild to moderate hypertension.
Abstract: This study used 24-h ambulatory blood pressure (BP) monitoring to investigate the effectiveness of a novel low-
dose combination of bisoprolol/hydrochlorothiazide in adult patients with mild to moderate essential hypertension. Thirty-
six patients with stable mild to moderate hypertension (sitting diastolic BP 95-114 mmHg) after a placebo run-in phase
received oral bisoprolol/hydrochlorothiazide 5 mg/6.25 mg once daily for 4 weeks in a single-blind regimen. At office visits,
BP and pulse were measured with statistically significant reductions (p < 0.01) recorded after 2 and 4 weeks of treatment.
Twenty-four-h ambulatory BP monitoring at the completion of therapy revealed significant reductions (p < 0.01) in both
systolic and diastolic 24-h, daytime, and night-time BP, compared with the end of the placebo treatment phase. Systolic and
diastolic load were also reduced (p < 0.01). The combination was well tolerated, and overall quality-of-life questionnaire
scores indicated an improvement after bisoprolol/hydrochlorothiazide therapy (p = 0.02). No clinically significant changes
from baseline in laboratory parameters were observed; in particular, serum potassium was unchanged. This is the first
study to demonstrate the 24-h effectiveness of the bisoprolol/hydrochlorothiazide 5 mg/6.25 mg combination, using 24-h
ambulatory BP monitoring. In addition, antihypertensive therapy with low doses of bisoprolol/hydrochlorothiazide in
combination may improve tolerability

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 15
ABSTRACTS Arq Bras Cardiol. 1998 Oct; 71(4):601-8.
Efficacy and tolerance of the bisoprolol/hydrochlorothiazide combination in arterial hypertension
Luna RL1, Oigman W, Ramirez JA, Mion D, Batlouni M, da Rocha JC, Feitosa GS, Castro I, Chaves Júnior Hde C, God EM, Maia
LN, Ortega KC, Raineri AM.
PURPOSE: Multicentre, open and non-controlled study to evaluate the efficacy and the tolerability of a low-dose
combination of two anti-hypertensive agents: a cardio selective beta-blocker, Bisoprolol (2.5 and 5.0 mg) with 6.25 mg of
hydrochlorothiazide.
METHODS: One hundred and six patients in the stage I and stage II of the systemic hypertension (mild to moderate) were
given the Bisoprolol/hydrochlorothiazide combination once daily and the diastolic and systolic blood pressures were
monitored during the 8-week trial.
RESULTS: The Bisoprolol/hydrochlorothiazide combination reduced the initial mean values of systolic and diastolic blood
pressures, respectively, from the 157.4 mmHg and 98.8 mmHg to 137.3 mmHg and 87.4 mmHg. At the end of the treatment
period, 61% of the patients normalized blood pressure values (< 90 mmHg) and 22.9% of them had responded to the
treatment, resulting in a total response rate (normalized + responsive) of 83.9% of cases. Adverse events were described
only in 18.9% of the patients and dizziness and headache were the most common.
There were no clinically significant changes on plasma levels of potassium, uric acid, glucose, or in the lipid profile.
CONCLUSION: The combination of low dosages of Bisoprolol and hydrochlorothiazide may be considered an effective, well
tolerated and rational alternative for the initial treatment of the patients with mild to moderate hypertension
--------------------------------------------------------------------------------------------------------- Clin Ther. 1993 Sep-Oct;15(5):779-87.
Low-dose bisoprolol/hydrochlorothiazide: an option in first-line, antihypertensive treatment.
Zachariah PK1, Messerli FH, Mroczek W.
Abstract
Two recent, multicenter, double-blind, placebo-controlled studies established the efficacy and safety of low-dose
bisoprolol/hydrochlorothiazide (HCTZ) in patients with mild to moderate essential hypertension. Bisoprolol, a cardio
selective beta-blocker, was used in a dose of 2.5 mg, 5 mg, or 10 mg. HCTZ was used at a dose of 6.25 mg. This low-dose
compound was developed to minimize dose-related adverse effects. The addition of HCTZ to each of the doses of bisoprolol
was compared with monotherapy and placebo. Results of both studies demonstrated that this once-a-day, low-dose option
effectively reduced sitting diastolic and systolic blood pressure measured at the end of the 24-hour dosing period. Drug-
related adverse effects, including those generally associated with traditional beta-blocker therapy, were infrequent in
individuals who received the low-dose bisoprolol/HCTZ regimen. Dose-related side effects were minimized because of the
low doses of the two agents used together. There were no significant changes in mean total cholesterol, triglycerides, or
serum glucose with bisoprolol/HCTZ 6.25 mg therapy versus placebo (analysis of variance statistical methods). The
incidence of treatment-induced hypokalaemia with bisoprolol/HCTZ 6.25 mg was not significant; uric acid elevations were
minimized, and the incidence of hyperuricemia was significantly (P < 0.01) less with bisoprolol/HCTZ 6.25 mg than with 25
mg of HCTZ. Once-a-day dosing with the low-dose agent controlled (defined as a sitting diastolic blood pressure < or = 90
mmHg and/or a decrease from baseline > or = 10 mmHg) blood pressure in up to 80% of patients for a full 24 hours after
dosing

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 16
ABSTRACTS Trials. 2012 May 17; 13:59. doi: 10.1186/1745-6215-13-59.
Progress report on the first sub-Saharan Africa trial of newer versus older antihypertensive drugs in native black patients.
Odili AN1, Ezeala-Adikaibe B, Ndiaye MB, Anisiuba BC, Kamdem MM, Ijoma CK, Kaptue J, Boombhi HJ, Kolo PM, Shu EN,
Thijs L, Staessen JA, Omotoso BA, Kingue S, Ba SA, Lemogoum D, M'Buyamba-Kabangu JR, Ulasi II.
Abstract
BACKGROUND: The epidemic surge in hypertension in sub-Saharan Africa is not matched by clinical trials of
antihypertensive agents in Black patients recruited in this area of the world. We mounted the Newer versus Older
Antihypertensive agents in African Hypertensive patients (NOAAH) trial to compare, in native African patients, a single-pill
combination of newer drugs, not involving a diuretic, with a combination of older drugs including a diuretic.
METHODS: Patients aged 30 to 69 years with uncomplicated hypertension (140 to 179/90 to 109 mmHg) and ≤2 associated
risk factors are eligible. After a four week run-in period off treatment, 180 patients have to be randomized to once daily
Bisoprolol/hydrochlorothiazide 5/6.25 mg (R) or amlodipine/valsartan 5/160 mg (E).
To attain blood pressure <140/<90 mmHg during six months, the doses of Bisoprolol and amlodipine should be increased to
10 mg/day with the possible addition of up to 2 g/day α-methyldopa.
RESULTS: At the time of writing of this progress report, of 206 patients enrolled in the run-in period, 140 had been
randomized. At randomization, the R and E groups were similar (P ≥ 0.11) with respect to mean age (50.7 years), body mass
index (28.2 kg/m(2)), blood pressure (153.9/91.5 mmHg) and the proportions of women (53.6%) and treatment naïve
patients (72.7%). After randomization, in the R and E groups combined, blood pressure dropped by 18.2/10.1 mmHg,
19.4/11.2 mmHg, 22.4/12.2 mmHg and 25.8/15.2 mmHg at weeks two (n = 122), four (n = 109), eight (n = 57), and 12 (n =
49), respectively. The control rate was >65% already at two weeks. At 12 weeks, 12 patients (24.5%) had progressed to the
higher dose of R or E and/or had α-methyldopa added. Cohort analyses of 49 patients up to 12 weeks were confirmatory.
Only two patients dropped out of the study.
CONCLUSIONS: NOAAH (NCT01030458) demonstrated that blood pressure control can be achieved fast in Black patients
born and living in Africa with a simple regimen consisting of a single-pill combination of two antihypertensive agents.
NOAAH proves that randomized clinical trials of cardiovascular drugs in the indigenous populations of sub-Saharan Africa
are feasible
--------------------------------------------------------------------------------------------------------- J Clin Pharmacology. 1995 Feb; 35(2):182-8.
First-line therapy option with low-dose bisoprolol Fumarate and low-dose hydrochlorothiazide in patients with stage I
and stage II systemic hypertension.
Frishman WH1, Burris JF, Mroczek WJ, Weir MR, Alemayehu D, Simon JS, Chen SY, Bryzinski BS.
1Department of Medicine, Albert Einstein School of Medicine, Bronx, New York 10461, USA.
Abstract: This 30-center, randomized, double-blind, placebo-controlled, parallel-group study was designed to (1) establish
that 6.25 mg of hydrochlorothiazide (HCTZ) given once daily with 5 mg of Bisoprolol Fumarate can contribute to
antihypertensive effectiveness in patients with stage I and stage II (mild to moderate) systemic hypertension; and (2) assess
whether this formulation was more effective or possessed a safety advantage over standard monotherapy with Bisoprolol
or 25 mg of HCTZ. Results showed that HCTZ 6.25 mg contributed significantly to the antihypertensive effectiveness of
Bisoprolol 5 mg. Bisoprolol 5 mg/HCTZ 6.25 mg (B5/H6.25) produced significantly greater mean reductions from baseline in
sitting systolic and diastolic blood pressure (-15.8 mm Hg/-12.6 mm Hg) than Bisoprolol 5 mg alone (-10.0 mm Hg/-10.5 mm
Hg) and HCTZ 25 mg alone (-10.2 mm Hg/-8.5 mm Hg). A 73% response rate was achieved with the low-dose formulation
compared with 61% for the Bisoprolol 5 mg (B5) group and 47% for the HCTZ 25 mg (H25) group. B5/H6.25 was found to be
significantly more effective than B5 or H25 in all subgroups of patients, regardless of gender, race, age, or smoking history.
Antihypertensive effects were maintained during the 24-hour dosing interval. The incremental effectiveness of B5/H6.25
was not accompanied by an increase in the frequency or severity of adverse experiences; the incidence of adverse
experiences in the B5/H6.25 group was comparable to that in the placebo group. B5/H6.25 was shown to provide safety
advantages over H25, as shown by less hypokalaemia (< 1% with B5/H6.25 versus 6.5% with H25).

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 17
ABSTRACTS J Hypertens Suppl. 2002 Feb;20(1):S21-5.
Clinical results with bisoprolol 2.5 mg/hydrochlorothiazide 6.25 mg combination in systolic hypertension in the elderly.
Benetos A1, Adamopoulos C, Argyriadis P, Bean K, Consoli S, Safar M.
1IPC Center, Paris, France. [email protected]
Abstract: Hypertension in the elderly, especially systolic hypertension, has been recognized as a major cardiovascular risk
factor. Several international studies, using primarily diuretics and/or beta-blockers, have shown the benefits of
antihypertensive treatment in elderly patients in terms of cardiovascular morbidity and mortality reduction. However,
because the risk of side-effects is a major concern when treating the elderly, the use of low-dose combination treatments
may be of particular interest. A randomized, multicentre, double-blind, parallel group study was conducted to compare the
efficacy and safety of bisoprolol 2.5 mg/hydrochlorothiazide 6.25 mg (biso 2.5/HCTZ 6.25) (n = 84) versus amlodipine 5 mg
(n = 80) in subjects over 60years of age with isolated systolic hypertension. The effects of these two treatment strategies on
patients' quality of life were also assessed. After a two- to four-week placebo washout period, both drugs were
administered once daily and taken for 12 weeks. Blood pressure was measured 24 h after treatment administration. Systolic
blood pressure/diastolic blood pressure changes from baseline to week 12 were similar for both biso 2.5/HCTZ6.25 and
amlodipine (-20.0/-4.5 mmHg and -19.6/-2.4 mmHg, respectively). Overall adverse events for biso 2.5/HCTZ 6.25 and
amlodipine were 39% and 40%, respectively. Both treatments improved quality of life scores in the same way. This study
demonstrates comparable efficacy and tolerability of biso 2.5/HCTZ 6.25 and amlodipine. Low-dose combination of
bisoprolol and hydrochlorothiazide may be an appropriate alternative for elderly patients with systolic hypertension.

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 18
REFERENCES • BENETOS A, COSOLI S, SAFAVIANA, et al.: Efficacy, safety and effects on quality of life of
Bisoprolol/Hydrochlorothiazide versus Amlodipine in elderly patients with systolic hypertension. Am Heart J
2000; 140: e14.
• DE QUATTRO V, WEIR M. Bisoprolol Fumarate/Hydrochlorothiazide 6.25 mg: A new low-dose option for first-
line antihypertensive therapy. Advances in therapy 1993; 10 (5): 197-206.
• FRISHMAN WH, BRYZINSKI BS, COULSON LR, et al. A multifactorial trial design to assess combination therapy
in hypertension: Treatment with Bisoprolol and Hydrochlorothiazide. Arch Intern Med. 1994; 154: 1461-1468.
• FRISHMAN WH, BURRIS JF, MROCZEK WJ, et al. First-line therapy option with low-dose Bisoprolol Fumarate
and low-dose Hydrochlorothiazide in patients with stage I and stage II systemic hypertension. J Clin Pharmacol.
1995; 35: 182-188.
• FRISHMAN WH. ZIAC National Hypertension Trial Report. March 1996.
• HABIB GB. Reappraisal of heart rate as a risk factor in the general population. Eur Heart J 1999; 1 (Suppl H):
H2-H10.
• JNC VI/The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and
Treatment of High Blood Pressure, NIH Publications 1997; No. 98-4080.
• LEWIN AJ, LEUG MC, TARGUM S, et al. A clinical trial evaluating the 24-hour effects of Bisoprolol
5/Hydrochlorothiazide 6.25combination in patients with mild-to-moderate hypertension. Clin Cardiol. 1993; 16:
732-736.
• MOSER M, BLACK H. The role of combination therapy in the treatment of hypertension. Am J Hypertens
1998; 11: 73S-78S.
• NEUTEL JM, ROLF CN, VALENTINE SN, et al. Low-dose combination therapy as first line treatment of mild-to-
moderate hypertension: the efficacy and safety of Bisoprolol/6.25 HCTZ versus Amlodipine, Enalapril, and
placebo. Cardiovasc Rev Rep. 1996; 17: 33-45.
• PAPADEMETRIOU V, NEUTEL J, NARAVAN P, et al. Comparison of Bisoprolol and low dose
Hydrochlorothiazide combination with Losartan, alone or in combination with Hydrochlorothiazide, in the
treatment of hypertension: a double blind, randomized, placebo controlled trial. Cardiovasc Rev Rep.;
December 1998.
• PRISANT LM, WEIR MR, PAPADEMETRIOU V, et al. Low-dose drug combination therapy: An alternative first-
line approach to hypertension treatment. Am Heart J. 1995; 130: 359-366.
• PRISANT LM, NEUTEL JM, PAPADEMETRIOU V, et al. Low-dose combination treatment for hypertension
versus single-drug treatment - Bisoprolol/Hydrochlorothiazide versus Amlodipine, Enalapril, and placebo:
Combined analysis of comparative studies. Am J Ther .1998; 5: 313-321
• PRISANT LM, WEIRMR, FRISHMANWH, et al.: Self-reported Sexual Dysfunction in Men and Woman Treated
With Bisoprolol, Hydrochlorothiazide, Enalapril, Placebo, or Bisoprolol/Hydrochlorothiazide. J Clin
Hypertens.1999; 1:22-26.
• PRISANT LM, MOSERM: Hypertension in the Elderly. Arch Intern Med. 2000; 160: 283-289.
• WEIR MR, PRISANT LM, PAPADEMETRIOU V et al. Antihypertensive therapy and quality of life. Influence of
blood pressure reduction, adverse events and prior antihypertensive therapy. Am J Hypertens. 1996; 9: 854-
859.

BLACKCEDAR PHARMACEUTICALS LTD. | Import | Distribution | Representations
BICEDOLOL® - MAXIMUM CLINICAL BENEFITS - MAXIMUM SAFETY PROFILE - COST EFFECTIVE
Page | 19
CONTACTS
Contact us for any inquiries:
Country Director¦ +234 809 574 1998
Head of Sales & Marketing – Lagos territory¦ +234 809 574 1913
Medical Sales Rep. – Lagos Island¦ +234 809 574 1967
Medical Sales Rep. – Oyo State¦ +234 809 574 1972
Account & Administrative Coordinator¦ +234 809 574 1925
Swiss Rep. Office: +41 79 603 9042
www.theblackcedar.com
Registered Office
Blackcedar Pharmaceuticals Ltd.
18 Owode Street, Abule-Egba
Lagos, Nigeria
Representative Office
The Blackcedar GmbH
Hôtel-de-Ville 46
2300 La Chaux-de-Fonds
Switzerland


















