
Pinguecula
11
PINGUECULA 1. Definition : Proliferation spot (yellow) on the conjunctiva bulbar near sclerocornea (cornea limbus), usually beside nasal and bilateral. (Dorland) Yellow – white, flat or slightly raised conjunctival lesion, usually in the inter-palpebral fissure adjacent to the limbus, but not involving the cornea (general ophthalmology) 2. Etiology and risk factors : Long exposed to dust , strong sun light, win, contact lens and another irritants. 3. Clinical sign and symptom : a. Usually asymptomatic unless inflammation occur (pingueculitis) b. Irritation c. Redness d. Uncomfortable feeling ( foreign body sensation ) e. Pain 4. Pathogenesis : Chronic exposure to solar radiation alteration of the collagen and elastic tissue of the conjunctival substansia propria pinguecula being formed tear film above it becomes thinner zone of dryness being inflamed vascular dilatation
-
Upload
agnes-lindrasari-jonathan -
Category
Documents
-
view
213 -
download
1
description
pinguecula
Transcript of Pinguecula

PINGUECULA
1. Definition :
Proliferation spot (yellow) on the conjunctiva bulbar near sclerocornea (cornea limbus), usually beside nasal and bilateral. (Dorland)
Yellow – white, flat or slightly raised conjunctival lesion, usually in the inter-palpebral fissure adjacent to the limbus, but not involving the cornea (general ophthalmology)
2. Etiology and risk factors :
Long exposed to dust , strong sun light, win, contact lens and another irritants.
3. Clinical sign and symptom :a. Usually asymptomatic unless inflammation occur (pingueculitis)b. Irritationc. Rednessd. Uncomfortable feeling ( foreign body sensation )e. Pain
4. Pathogenesis :
Chronic exposure to solar radiation alteration of the collagen and elastic tissue of the conjunctival substansia propria pinguecula being formed tear film above it becomes thinner zone of dryness being inflamed vascular dilatation allowing release of inflammation molecule irritative symptoms (pingueculitis)
Pinguecula formation is typically seen in older patients and is considered by most researchers to be a conjunctiva degenerative processes initiated by exposure to noxious environmental stimuli and ultraviolet radiation. The initial lesion is thought to result from the chronic action of solar radiation, which induces an alteration of the collagen and elastic tissue of the conjunctival substantia propria. Once a pinguecular elevation is formed, depending on its size, the tear film

may become thin and discontinuous in that zone, producing a bed of dryness. When the lesion is sufficiently affected by inflammation, vascular dilatation allows histamine, serotonin, bradykinin and prostaglandins to be released, producing the acute irritative symptoms that characterize pingueculitis. In severe cases, the conjunctival surface becomes sufficiently dry to cause microulceration of the surface epithelium. When this occurs, the eye attempts to cover the erosion, and this is the impetus for pterygium formation. New research has suggested that inflammatory cell infiltration may contribute to conjuctival inclucion cyst formation seen within pterygia, pingueculae, vernal conjuctivitides and pyogenic granuilomata.
5. treatment:- avoid the risk factors by wearing sunglasses, goggles, UV-blocking coatings- topical steroid :
o fluorometholone 0.25% o 1% rimexolone acetate o 0.12% prednisolone acetate suspension o 0.12% prednisolone sodium phosphate solution o 1% prednisolone acetate suspension o 1% prednisolone sodium phosphate solution
6. Differential diagnose :a. Pterygiumb. Pseudo pterygiumc. Conjuctival intraepithelial neoplasia ( CIN )

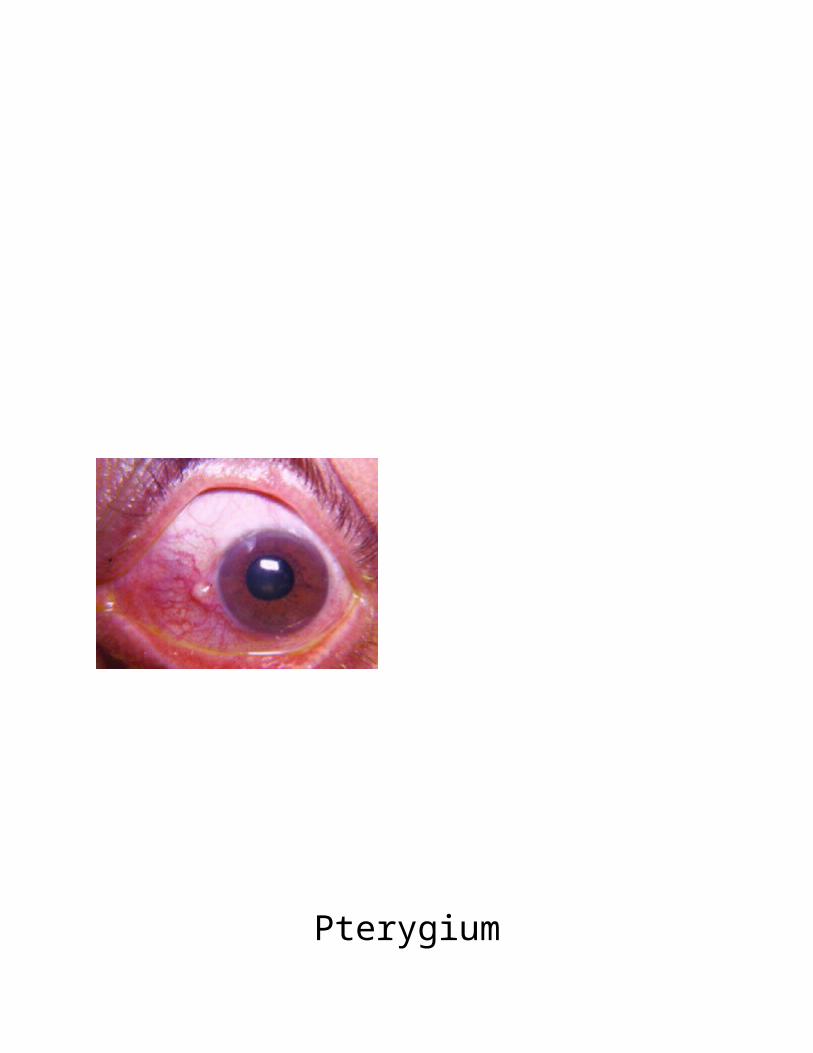
Pterygium
1. Definition :
Degenerative condition of the subconjunctiva tissue which proliferate as vascularized granulation tissue to invade the cornea, destroying as it does so the superficial layers of the stroma and bowman’s membrane, the whole being covered by conjunctiva epithelium
Wing – shaped fold of fibrovascular tissue arising from the intra – palpebral conjunctiva extending onto the cornea , usually nasal in location

2. Etiology and risk factors :
Most etiology and risk factor appear to be predominantly environmental in nature , namely, solar, and ultraviolet radiation, and also chronic irritation from airborne particulate matter, but some studies implicate hereditary factors.
a. Ultraviolet radiation :The major environmental risk factor for the development of pterygium is exposure to UV light. UV light absorbed by the cornea and conjunctiva results in cellular damage and subsequent proliferation of these cells.
b. Genetic factor :Several case reports have described clusters of family members with pterygium and a hospital-based case control study showed family history to be significant, suggesting a possible autosomal dominant inheritance pattern.
c. Other risk factorsDust , low humidity and micro-trauma from particular matter, dry eyes and human papillomavirus have also been implicated in pterygium.
3. Clinical symptom and sign :
A small, grey cornela opacity develops near the nasal limbus.
The conjunctiva overgrows the opacity and progressively encroaches onto the cornea in a triangular fashion
A deposit of iron (stocker line) may be seen in the corneal epithelium anterior to the advancing head of the pterygium
Ordinarily the condition is symptomless but vision becomes impaired if it progresses into the pupillary area of the cornea and may cause astigma or lead to blindness
If pterygium inflamed may cause red eye, watery, and feel uncomfortable in the eye
4. Pathogenesis :
The exact pathophysiological mechanisms underlying pterygium, its progression and recurrence are still being debated.
a. Degenerative versus proliferative disorders :

Pterygium has long been considered to be chronic degenerative condition because of the apparently degenerative appearance of its histophatology. Classically described as “elastotic degeneration” by light microscopists , pterygium tissue is characterized by abnormal subepithelial tissue containing altered collagen fibers that are demonstrable with elastin stain, which are purely degenerative processes caused by sun exposure. Clinically , there are also clear behavioral features of pterygium. Which suggest that it is proliferative growth disorder. A primary pterygium is locally invasive, growing towards the corneal apex. The link between UV radiation and cancer is well known, and UV light is able to induce mutations in solar keratosis and skin carcinomas. Pterygia have a high propensity for recurring aggressively after surgical excision and treatment modalities, therefore, mimic anti cancer treatment.
b. Limbal stem cell deficiency :
Limbal stem cells are now believed to be the ultimate source or regenerating corneal epithelium, via the supply of daughter transient amplifying cells that migrate cetripetally onto the cornea. In the presence of limbal deficiency, conjunctivalization of the cornea surface occurs. The classical sign or clinical hallmarks of limbal deficiency include conjunctival ingrowth , vascularization , chronic inflammation , destruction of basement membrane , and fibrous ingrowth. These sign are also the hallmark of pterygium and , therefore , many researchers today have suggested that pterygium is a manifestation of localized, interpalpebral limbal stem cell dysfunction or deficiency , perhaps as a consequence of UV light - related stem cell destruction.
c. Fibrovascular components of corneal invasion and pterygium recurrence :
Fibroblast isolated from pterygium tissue exhibit a transformed phenotype, growing much better in medium containing a low concentration of serum, compared to normal conjunctival fibroblast. Other studies show that the fibrovascular layer of a pterygium is the major of excessive cellular proliferation. It has also been found pterygial fibroblast express more matrix metalloproteinases . which are a family of extracellular matrix – degrading enzymes responsible for tissue degradation, wound healing and remodeling, and that these pterygium head fibroblasts respond to TGF – β signaling differently than do normal conjunctival tissues , over – expressing bFGF and IGF – II. These results may explain a pterygium’s propensity for sustained growth, invasion into corneal stroma, and fibrovascular and inflammatory responses .

5. Treatment : a. Protect eyes from sun , dust, and wind with sunglasses or gogglesb. Lubrication with artificial tears four to eight time per day to reduce ocular irritationc. If inflammation occur use topical steroidd. Surgical removal is indicated when :
- The pterygium progresses toward the visual axis- The patient is experiencing excessive irritation not relieved by the aforementioned
treatment- The lesion is interfering with contact lens wear
Pterygia can recur after surgical excision, bare sclera dissection with a conjunctiva auto-graft or amniotic membrane graft reduce the recurrence rate. Intra-operative application of an anti-metabolite (5-fluorouracil or mitomycin-C) also reduces recurrence.
Pseudo Pterygium
1. Definition :A conjunctivval scar attached to the cornea, superficially RESEMBLING a true pterygium but usually not firmly adherent to the underlying tissue (Dorland)
2. Etiology and Risk FactorsPseudipterygia occur following chemical injury, corneal ulceration, or other inflammatory problems in which the conjunctiva becomes scarred and drawn upon the cornea.
3. Pathogenesis :There is an adhesion of a fold of conjunctiva to a peripheral corneal ulcer or area of peripheral thinning , and is fixed only at its apex to the cornea. The fold can grow from any direction corresponding to the injury.
4. Sign and symptoms:

- A probe can pass beneath the fold- Vascular which occur looks like the vascularization on normal conjunctiva- Foreign body sensation
5. Treatment: surgically exsicion if the adherence to the cornea has occured
Discussion
Pinguecula is actually symptomless unless it is being inflamed. Inflammation causes vascular around the pinguecula become vasodilated. Common symptoms of eye irritation and inflammation may mimic pingueculitis. As in our patient, he felt uncomfortable on his eye, red eye, pain, and watery.
Triangular encroachment of the conjunctiva upon the cornea with numerous small opacities lying deeply in the neighbouring part of the cornea suggests pterygium. But in our eye examination, there is conjunctival injection on temporal of his right eye and yellow spot within it. So, we exclude this diagnosis.
Treatment should be administered while symptoms has being occurring. Topical corticosteroid can be given to our patient.
DAFTAR PUSTAKA
1. Tan DT, sao-bing lee, Jessica MA. Pterygium. In : Clinical Ophthalmology an asian perspective. Singapore: sunders Elsevier ; 2005 .p. 207 – 214
2. Kanski JJ. Clinical ophthalmology a systematic approach 5th ed. China : Elsevier ; 20033. Ehlers JP, chirag PS, editors. The wills eye manual. Baltimore : Lippincott Williams and wilkins ;
20084. Ilyas S, HHB Mailangkay , Hilman T, Raman RS, Monang S, Purbo SW, editor. Ilmu penyakit mata
untuk dokter umum dan mahasiswa kedokteran. Jakarta : sagung seto ;20025. Dorland’s illustrated medical dictionary. 30th ed. Philadelpia : sunders Elsevier ; 2003


















