Lip repositioning with a myotomy of the elevator muscles ...

Ping-hong ZHOU, MD
Endoscopy Center, Zhongshan Hospital
Fudan University, Shanghai, China
How I Do It?
Per-oral Endoscopic Myotomy (POEM)

Prof. Pinghong ZHOU
Zhongshan Hospital, Fudan University, Shanghai, China
Per-oral Endoscopic Myotomy (POEM)
Disclosure of Interest: Nothing to Disclose
The 2nd World Congress on
CONTROVERSIES IN GASTROENTEROLOGY

Treatment
No curative option!
Objective
Reduction of the gradient across the LES for
relieving symptoms
improving esophageal emptying
preventing development of megaesophagus
Pharmacological treatment Disruption of the LES
Endoscopic botox injection
Calcium channel blockers Surgical
myotomy
Pneumatic
dilation
Endoscopic
myotomy

History of POEM
NOTES has inspired endoscopists to creat less invisive treatment even for achalasia.
Pasricha et al. performed submucosal endoscopic esophageal
myotomy on 4 pigs and found it feasible, safe and effective.
It provided experimental evidence for peroral endoscopic
myotomy later on.
Pasricha et al. Endoscopy, 2007

Inoue,et al. Endoscopy 2010; 42: 265–271
Inoue et al. reported a novel endoscopic
surgery: peroral endoscopic myotomy
(POEM) for treating esophageal achalasia
Significant improvement in dysphagia
score (preop 10 ↓to 1.3 postop (P<0.001)
Improvement in LES pressure (mean
preop 52.4mmHg ↓19.9mmHg postop
(P<0.001)
It is a milestone event of tunnel
endoscopic surgery

July 2010, Hongkong

• First case (16-Aug-2010)
• Operative time: 85 minutes


POEM - Clinical setting
Gastroscope with jet system
Hook, TT Knife (Olympus, Japan)
Hybrid Knife (T-type, ERBE, Germany)
Distal attachment: transparent cap
Diathermy: VIO 300D (ERBE, Germany)
Forced Coag, Effect 2,45W, 3-2-4
CO2 insufflation
Instruments

Preparation of esophageaus

POEM - Clinical setting
All performed under GA

Tips for POEM procedure
When coagulating the blood vessel, the coagulation forceps are suggested
to be close to the muscular side to avoid mucosal injury

Tips for POEM procedure
The fibrosis at the EGJ is common for pre-treatment patients
Sufficient submucosal cushion is important to prevent mucosal rupture

Judgement of EGJ
1)Length of insertion; 2)Resistance of gastroscopy;
3)Typical vessels; 4)Color change in cardia mucosa

Bleeding during myotomy


Presidental plenary session, DDW, 2012, San Diego
Water-jet assisted POEM in comparison to conventional
myotomy technique for treatment of esophageal achalasia
www.asge.org/ddw

Water-jet assisted POEM lead to significantly shorter
operation time, lower bleeding rate and a lower frequency
of usage of coagulation forceps
The water-jet assisted procedure simplifies the POEM
procedure and makes it safer
“push and pull” technique
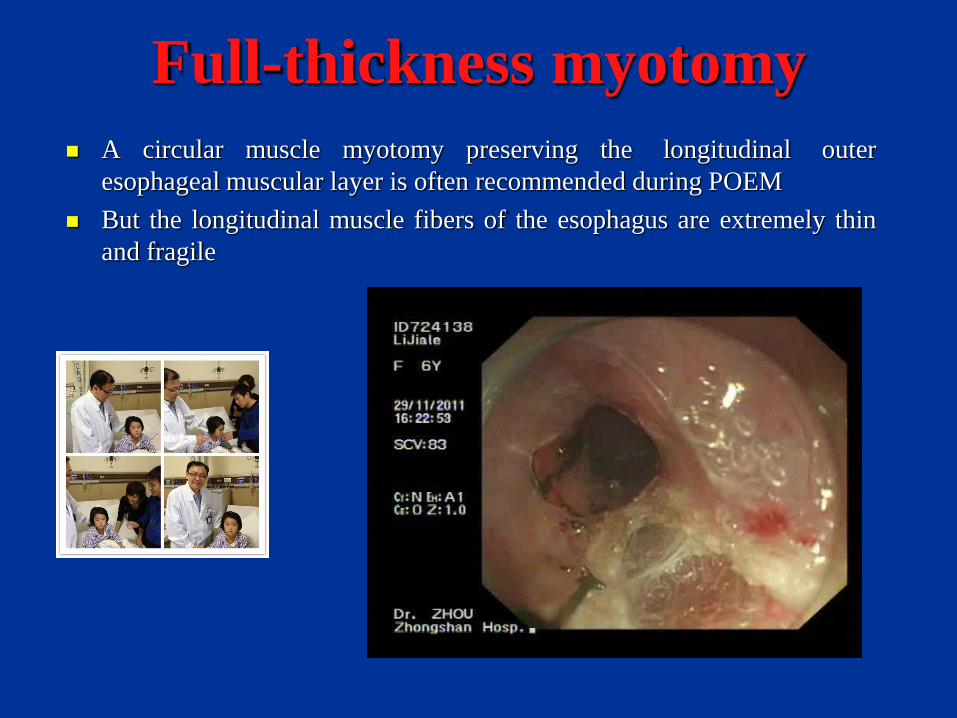
Full-thickness myotomy
A circular muscle myotomy preserving the longitudinal outer
esophageal muscular layer is often recommended during POEM
But the longitudinal muscle fibers of the esophagus are extremely thin
and fragile

Full-thickness myotomy
Zhou PH et al. J Am Coll Surg, 2013
Reduced the procedure time
Did not increase the procedure-
related adverse events
Did not increase clinical reflux
complications

UEG Week 2012, Amsterdam

Familiari Zhou V. Rentile Maselli Charton
Patients 22 46* 69 8 21
Success 91% 93% 96% 100% 95%
Major complications 0 0 0 0 0
GERD occurrence 0 1 18% 0 31%
*
Paediatric N = 21
Prior LM N = 12
Sigmoid type N = 13
Results presented at the UEGW 2012

Reasons for operation failure
Incomplete myotom
Healing of myotomy edges by fibrosis
Hypertensive fundoplication
Esophageal diverticula
Gastro-esophageal reflux disease
POEM for failed HM

Controversy exists regarding the therapy of failed HM
Peroral endoscopic myotomy (POEM)
Pneumatic dilation was associated with unpredictable
outcomes and significant complications
Laparoscopic remyotomy was still an invasive procedure
with an increased risk of failure and complications
POEM may offer another option for failed HM
Subsequent POEM may be more challenging
because of scars and tissue adhesions
No systematic data HM have yet been published
Management of failed HM

The patient once had thoracoscopic HM 10 years ago, but the symptom was
recurrent due to imcomplete myotomy around the cardia
POEM was performed at the opposite side of the esophagus
POEM seems to a promising new treatment for
failed HM resulting in short-term symptom relief
in > 90% of cases
Previous HM may make subsequent endoscopic
remyotomy more challenging, but does not
influence subsquent POEM procedure

POEM for sigmoid type
The S type was considered to be the advanced stage of
achalasia
The esophageal lumen was dilated, tortuous and stored
with lot of effusion

Strategy for S type
Treatment of S type is still controversial
POEM may offer another option for S type
Interventional treatments (balloon dilation, botox et al.) are ineffective
Esophagectomy has historically been considered as standard treatment
Some recommend a myotomy as the first step
several studies have examined successful treatment of achalasia with
laparoscopic Heller myotomy
A new way of myotomy
Less invasive
Effective in primary cases

It is very difficult and time-consuming to make the tunnel for sigmoid type achalasia
S type POEM difficulties
Easy to be lost in the tunnel
Tortuous lumen
fibrosis in SM layer
thickened and disordered muscle fiber

During follow-up, the esophageal lumen is still dilated,
but no more effusion
Clips sometimes remains and cardia is loose

31
Gentleman, 98 years old
Severe fibrosis in sm layer

Child, 3 years old

Child, 2 years old


POEM was performed in another hospital 4 monthes ago, but dysphagia
was not relieved due to imcomplete myotomy around the cardia
Thorough myotomy was achieved by Hybrid Knife
Re-myotomy after POEM

Gas-related complications
Pneumothorax
Small-caliber thoracic tube
Pneumoperitoneum
Puncture with 20G needle
Subcutaneous emphysema
mediastinal emphysema

Delayed bleeding
Zhou PH et al. GIE, 2013
Early manifestations Hematoma on CT scan
Progressive retrosternal pain
Vomited fresh blood
Hemostasis Emergency endosopy
Sengstaken–Blakemore tube

Orlando, 2013 DDW

Delayed bleeding in the submucosal tunnel
Vomiting of fresh blood and progressive retrosternal pain were the major early
manifestations
Emergency endoscopic diagnosis and hemostasis should be taken as early as possible
A Sengstaken–Blakemore tube is particularly effective for hemostasis by compression

Esophageal leakage
Clinical signs
Chest CT scan
Endoscopy
chest pain continuous high fever dyspnea
pleural effusion
mediastinal emphysema pneumonia and segmental atelectasis of the lungs
esophageal leakage

GI tract leakage
Metallic clips falling off from entry of the tunnel and endoscopic observation
revealing orificium fistulae which were successfully clipped with metallic clips
A satisfactorily healing was seen at 2-3 weeks follow-up endoscopy

42
Sealant Pocrine Fibrin Kit (fibrinogen+thrombin)

43

44
String suture with endoloop and meatllic clips

45

Day 3 after Procedure
• Body Temperature: 39.1 ℃
• Gastroscopy: leakage of mucosa in EGJ
purulent secreta in tunnel
• Washing the tunnel with NS
• Position: semireclining
• NGT drainage
• Antibiotics and PPI
Retroperitoneal Infection

• Body Temperature: 38.5 ℃
• Complain of pain at right lower back
• CT Scan
• Drainage of the retroperitoneal abscess
Day 10 after Procedure

Discharged: Day 29

promises to be
• as effective as laparoscopic myotomy (LM) or
pneumatic dilation (PD)
• less invasive than LM (no injury of surrounding tissue)
• at least as safe as PD
• more durable than PD
could be effective in failures or predictable negative outcome
of LM or PD
Current Status

Summary
When, whom, how long and which direction for POEM ?
POEM allows myotomy in any direction and any length
POEM for achalasia type I-III
POEM for tortuous achalasia
POEM for children
POEM for failure after surgery
Re-myotomy for failure after POEM
POEM for EVERYBODY !
is still investigational


53