
PILOTING MALARIA POST MODEL IN MALARIA … · PILOTING MALARIA POST MODEL IN MALARIA PREVENTION AND...
32
PILOTING MALARIA POST MODEL IN MALARIA PREVENTION AND CONTROL (MPC) FOR MOBILE AND MIGRANT POPULATION (MMP) Nguyễn Quý Anh National Institute of Malariology Parasitology and Entomology (NIMPE)
Transcript of PILOTING MALARIA POST MODEL IN MALARIA … · PILOTING MALARIA POST MODEL IN MALARIA PREVENTION AND...
PILOTING MALARIA POST MODEL IN MALARIA PREVENTION AND CONTROL
(MPC) FOR MOBILE AND MIGRANT POPULATION (MMP)
Nguyễn Quý Anh National Institute of Malariology
Parasitology and Entomology (NIMPE)

1. Introduction • Vietnam is one of the countries which has successful malaria
prevention and control (MPC) program, malaria has been significantly decreased
• Malaria patients are mainly concentrated in provinces with a large number of mobile population, people sleeping on “ray”, seasonal and cross-border migrants
• The community healthcare network, especially the village health workers are insufficient and weak in malaria active areas, it’s hard to reach the migrants
• Interventions (access, active case detection, treatment, disease management, BCC) are needed among MMP for reduction of malaria and prevention of parasite and anti-drug parasite transmission
1. Introduction
• In 2014, WHO introduced the idea of piloting the malaria post model to enhance access to and provision of healthcare services for MMP
• This model was applied in 4 provinces: – Quảng Nam: conducted by the NIMPE – Bình Phước: conducted by the IMPE in HCM city – Đăk Nông and Gia Lai: conducted by the IMPE in
Quy Nhơn • Period: 1 year (depending on each IMPE)
2. Objectives
1. Build the “case detection, management and treatment” post model.
2. Strengthen the MPC measures for MMP. 3. Reduce malaria incidence among MMP.
3. Implementation
Post selection criteria - Villages with many malaria cases (Region 4, 5) - Villages with a large number of people working in
forest and sleeping on “ray” - Villages with seasonal migration - Villages with forest gates or areas where people
pass by on the way to forest.

3. Implementation
Staff selection criteria: - Age: 20-60 - Graduates from medical schools without job yet - Retired health workers - Agree to participate - Must be present daily at malaria post
4. Tasks of malaria post staff • MMP management • MPC propaganda • Case detection, diagnosis, treatment and
management • Involvement in the MPC activities in locality • Monthly, weekly reporting

4.1. MMP management
- Listing the village households - Monitoring the number of workers coming to the
village for long-term, short-term work - Monitoring the number of outbound migrants Working in forest Working on “ray” Sleeping on “ray” Working in other areas
Recording and weekly reporting

4.2. MPC propaganda - Involve in all village meetings for MPC
propaganda - Visit households for propaganda - Meet household owner and members for
propaganda - Meet people when working on “ray”: find out
whether they sleep there or not? whether they bring mosquito net or have one on “ray”?
- Distribute propaganda leaflets and posters - Encourage people to use mosquito net when
sleeping on “ray” or in the forest
4.3. Case detection, diagnosis, treatment and management
• Detect fever cases in the village • Take blood sample for testing (keep dry & send to
Commune health center (CHC) for identification of malaria parasite)
• Perform quick test • Provide treatment if results are positive Report to CHC, DHC when detecting patient Provide daily medicine (give medicine to patients at their
home or invite them to come for taking medicine) Investigate the case and fill in report form Check and monitor patient’s family members
• Record to monitor and weekly report to CHC
4.4. Reporting
• Report immediately to CHC, DHC whenever a case is detected
• Send microscopic blood sample to CHC • Weekly report to CHC • Involve in monthly CHC inter-departmental meeting • Fill in the report template and send to CHC/DHC

5. Equipment & materials
• Healthcare bag: each post is equipped with a healthcare bag, stethoscope, thermometer, clamp, cotton pack, etc.
• Microscopy slide, needle, alcohol (National) • Quick test (QTC-RAI project) • Communication materials (RAI project) • Long Lasting Insecticidal Nets - LLINs (awaiting
WHO mosquito nets)

OUTCOMES Site selection: Trà Cang, Trà Leng and Trà Dơn
• Trà Cang: Village No. 1, 5 and 7
• Trà Dơn: Village 2 • Trà Leng: Village 1, 2 and
3 Most people in the commune have malaria parasites Most of cases are people working in forest and sleeping on “ray” (80-90%)
Commune name Parasite in 2013
% parasite in village/commune
Trà Cang 311 Village 1 55 17,68 Village 5 113 36,33 Village 7 83 26,69 Trà Dơn 149 Village 2 104 69,80 Trà Leng 139 Village 1 39 28,06 Village 2 42 30.22 Village 3 44 31.65
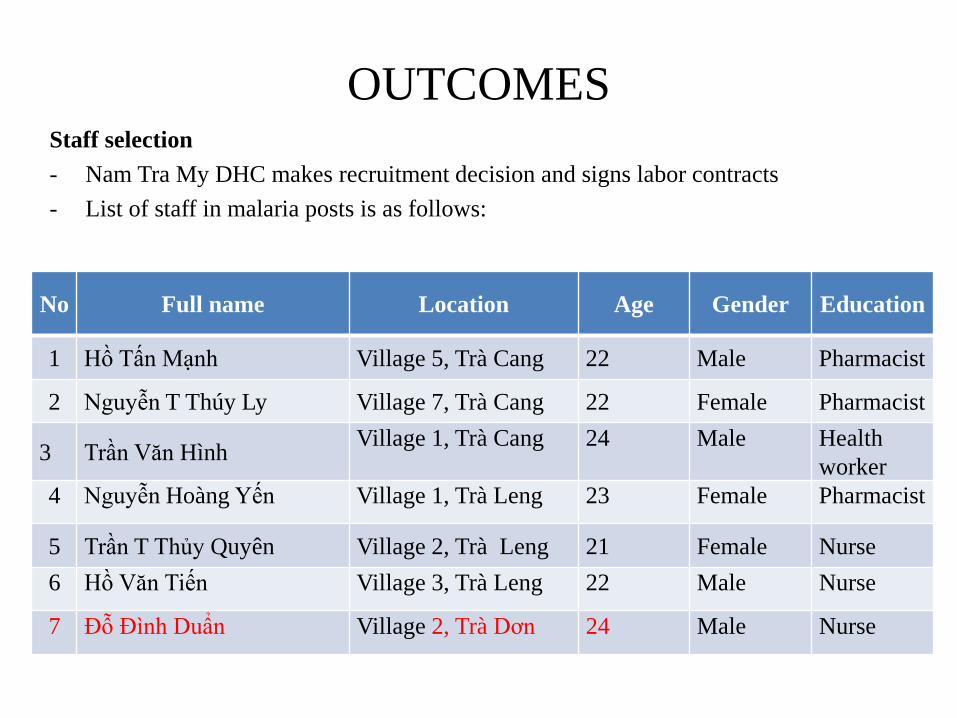
OUTCOMES Staff selection - Nam Tra My DHC makes recruitment decision and signs labor contracts - List of staff in malaria posts is as follows:
No Full name Location Age Gender Education
1 Hồ Tấn Mạnh Village 5, Trà Cang 22 Male Pharmacist
2 Nguyễn T Thúy Ly Village 7, Trà Cang 22 Female Pharmacist
3 Trần Văn Hình Village 1, Trà Cang 24 Male Health worker
4 Nguyễn Hoàng Yến Village 1, Trà Leng 23 Female Pharmacist
5 Trần T Thủy Quyên Village 2, Trà Leng 21 Female Nurse 6 Hồ Văn Tiến Village 3, Trà Leng 22 Male Nurse
7 Đỗ Đình Duẩn Village 2, Trà Dơn 24 Male Nurse

OUTCOMES Healthcare bag provision
OUTCOMES Training: - Treatment and diagnosis
guideline - Microscopy slide blood
sample taking method - Quick test method - Report template - Tasks of malaria post staff - Implementation at all
levels.

OUTCOMES Post activity implementation - Household survey - MPC propaganda - Taking household blood sample slide - Quick test for people with fever - Mosquito net distribution - Monthly report

OUTCOMES Household monitoring
Commune Location
No. of househol
ds
No. of family
members
Number of persons working in forest and sleeping on “ray”
Feb Mar Apr May
Trà Leng Village 1 122 485 449 478 478 385
Trà Leng Village 2 67 315 174 176 176 174
Trà Leng Village 3 205 912 828 929 1001 637
Trà Cang Village 3 186 796 812 834 837 983
Trà Cang Village 5 131 640 546 526 561 525
Trà Cang Village 7 108 491 409 314 586 431
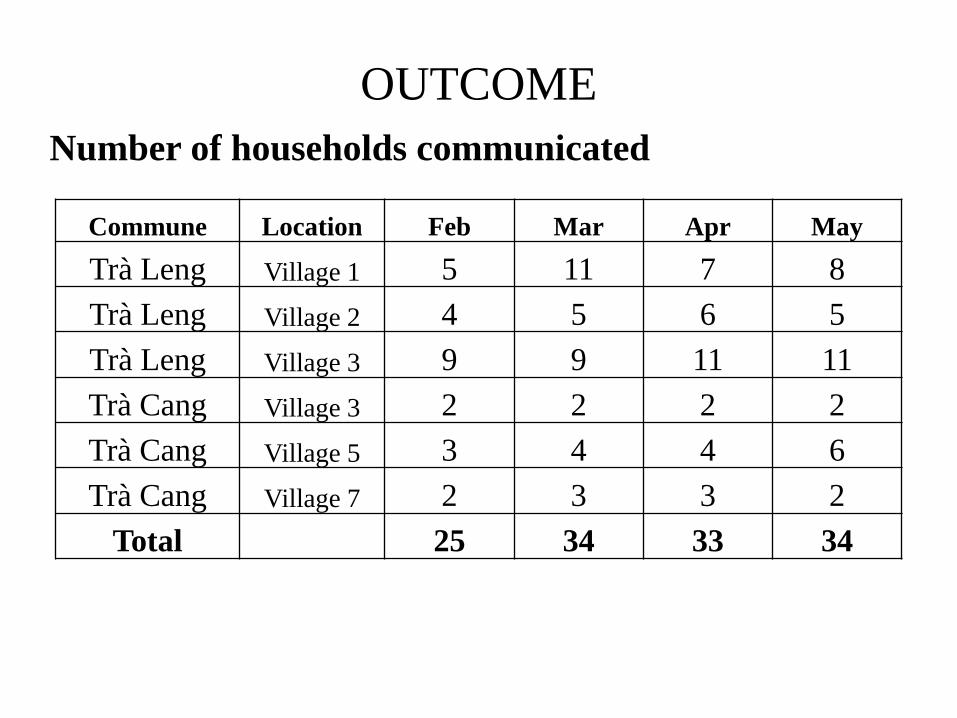
OUTCOME Number of households communicated
Commune Location Feb Mar Apr May
Trà Leng Village 1 5 11 7 8 Trà Leng Village 2 4 5 6 5 Trà Leng Village 3 9 9 11 11 Trà Cang Village 3 2 2 2 2 Trà Cang Village 5 3 4 4 6 Trà Cang Village 7 2 3 3 2
Total 25 34 33 34
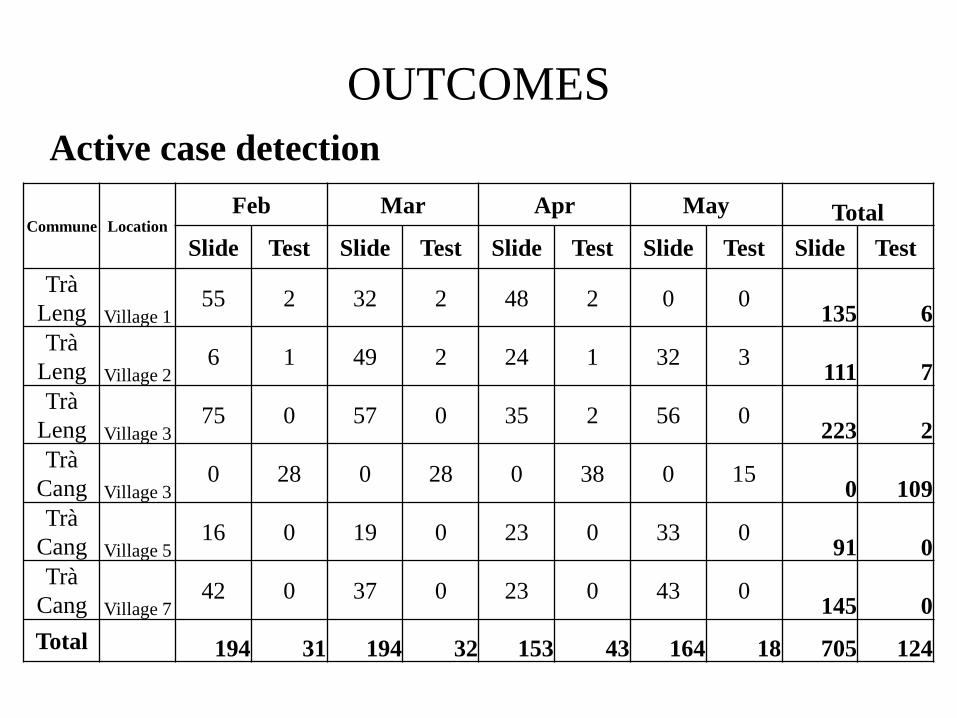
OUTCOMES Active case detection
Commune Location Feb Mar Apr May Total
Slide Test Slide Test Slide Test Slide Test Slide Test Trà
Leng Village 1 55 2 32 2 48 2 0 0 135 6
Trà Leng Village 2
6 1 49 2 24 1 32 3 111 7 Trà
Leng Village 3 75 0 57 0 35 2 56 0 223 2
Trà Cang Village 3
0 28 0 28 0 38 0 15 0 109 Trà
Cang Village 5 16 0 19 0 23 0 33 0 91 0
Trà Cang Village 7
42 0 37 0 23 0 43 0 145 0 Total 194 31 194 32 153 43 164 18 705 124
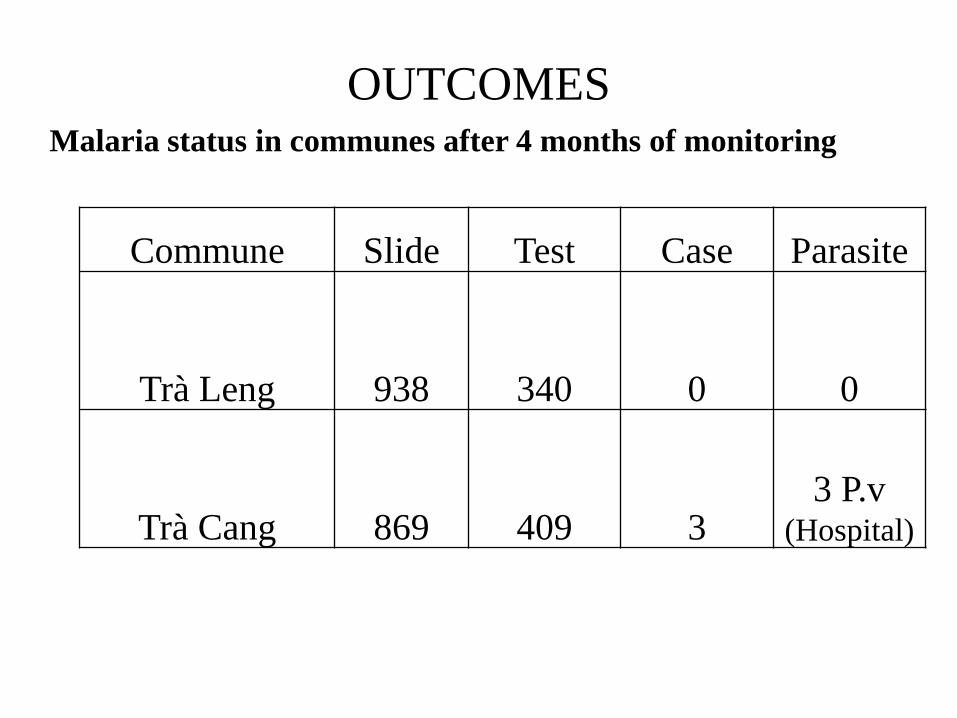
OUTCOMES Malaria status in communes after 4 months of monitoring
Commune Slide Test Case Parasite
Trà Leng 938 340 0 0
Trà Cang 869 409 3 3 P.v
(Hospital)

OUTCOMES Contribution of malaria posts in 4 month case detection
0
100
200
300
400
500
600
700
800
900
1000
Trà Leng Điểm SR Trà Cang Điểm SR
LamTest

OUTCOMES Monitoring at post - Central level: 1 time - Provincial level: 2 times - District level: 5 times - Commune level: monthly

No Malaria post Number of tests Positive (+) %
1 B Du. Ia Mla 41 5 12.20
2 Boi Jik. Ia Mla 39 0 0.00
3 B. Ma Nhe B Đất Bằng 37 12 32.43
4 B. Ma Nhe A. Đất Bằng 36 7 19.44
5 B. 12 households, Ia R Sai 77 2 2.60
6 B. E Nan Ia R Sai 71 3 4.23
7 B H Lang. Chư R Căm 36 0 0.00
8 B Du. Chư R Căm 54 5 9.26
Total 391 34 8.70
Malaria case detection in Krong Pa Gia Lai post
(8 malaria posts conducted by Quy Nhom IPME)

Month Test + Sleeping on “ray” + Working in
forest
Informal
migrants
+
12/2014 38 2 5.26 22 2 8 0 8 0
1/2015 83 0 0 49 0 23 0 11 0
2/2015 102 1 0.98 46 1 34 0 22 0
3/2015 109 2 1.83 43 2 54 0 12 0
4/2015 86 2 2.33 52 1 21 1 13 0
5/2015 110 2 1.82 91 2 7 0 12 0
528 9 1.70 303 8 147 1 78 0
Malaria case detection in Tuy Đức, Đăk Nông post
(8 malaria posts conducted by Quy Nhom IPME)

Active malaria case detection in Binh Phuoc
(9 malaria posts conducted by HCMC IPME)
Content
Đăk Ơ commune (3 posts)
Bù Gia Mập
commune (2 posts)
Đăk Nhau commune (4 posts)
Total (9 posts)
Number of quick test/slide 30/30 69/75 197/226 296/331
Number of positive case - P.falciparum - P.vivax - PH
9 3 5 1
14 7 5 2
21 9
12 0
44 19 22
3

6. Dicussion • Quang Nam is a province with a low number of MMP,
most migrants are seasonal, mobile, working in forest and sleeping on “ray”
• Malaria in the first 5 months of 2015 decreased considerably compared to the previous period.
• No communication materials • No WHO supported mosquito nets for malaria posts Severely affect evaluation of malaria post
performance

Advantages
• Provincial MPC center understands issues and gives timely instructions to DHC
• DHC enthusiastically implements: selecting staff, signing contracts, making payment.
• Quick test and microscopic slide are provided from QTC & National level
• Anti-malaria medicines (arterakin, cloroquin, primaquin) are also provided to posts from the national level

Disadvantages • All staff are new graduates and have no experience
of working with the community • Short duration training, not enough time to convey
information. • Weak communication skills • Post staff is NOT local people • Language barrier
Disadvantages • Working place is not suitable • Not being present 24/7 at post • Wide operation area (village-wide) • Local people have not been aware of post staff’s role • Small budget (not including social insurance, ect.) • Change of staff at post (turnover rate)

Conclussion 1. Malaria posts initially support CHC in active case
management 2. Proactively monitoring the number of people
working in forest and sleeping on “ray” every month
3. Not being able to manage malaria cases (communes do not manage malaria cases and do not require the post staff to monitor)
4. MPC communication is mainly direct communication
5. Support CHC to deliver and insecticide mosquito nets
Thank you!


















