Pulmonary hypertension dr md toufiqur rahman dm fcps frcp fesc faha fscai fapsic

16th Controversies& AdvancesIn The Treatment Of Cardiovascular Disease
Piecing Together the MACRA Puzzle:How the ACCand NCDRwill Help
MembersNavigate RadicalChangesAhea
Ralph Brindis , MD, MPH, MACC, FSCAI, FAHAClinical Professor of Medicine, UCSF
Dept. of Medicine & the Philip R. Lee Institute for Health Policy Studies
Senior Medical Officer, External Affairs,
ACC National Cardiovascular Data Registry
November 17, 2016

Disclosures
Senior Medica l Office r, NCDR

Message to Clinicians:Prepare for the Future

The Bridge to NowhereCholuteca Bridge, Honduras

What isYour Value & Worth?
The answer isnot monetary, but what isyour value andworth to...
1. Your Patients
2. Your Peers
3. Your Hospital System
4. The Payer(s)
5. The Government
We will be graded by them all.
Your data will be critical to your success—
real and perceived.

Clin ic ian Se lf-Awarenes s5 Rea lities over next 5 Years
1. Know your Personal Data!!!!
2. Certainty of Transparency & PublicReporting
3. Accountability for Patient & Peer Satisfaction
4. Accountability for Efficiency and Cost-Savings
5. Accountability for Demonstration of Value

- EHRs; meaningful use - ICD-10
- Value Based Purchas ing
- Efficiency metrics (= cut cos ts )
- Payment cuts
- Accountable Care Organiza tions- DOJ Fraud inves tiga tions
- Bundled payments (capita tion)
- Preauthoriza tion
- Phys ician Quality Reporting Sys tem (PQRS)
- Public Reporting
- Payer Programs
- Utiliza tion review
- Cla ims da ta profiling
- Episode groupers
- MOC / MOL- Certifica tion exams
- Coverage de te rmina tions
- Appropria teness auditing
- Hospita l employment
Health Care Environment 2016-2020
Merit Incentive Based Payment(MIPS)
Alternative Payment Models (APMs )Bundled Payments
Core Quality Measures CollaborativeCVQuality Measures

>2,500 hospitals>5,700 cardiologists>60 million clinical records

Name Disease or Device Facility SitesPatientRecords
PINNACLECoronary artery disease, heart failure,
atrial fibrillation, hypertension,diabetes, peripheral arterial disease
Outpatient 445 35,000,000
DiabetesDiabetes and
cardiometabolic careOutpatient 329 1,000,000
CathPCIPercutaneous coronary interventions
Diagnostic catheterizationsHospital/Free Standing 1,730 20,000,000
ICD Implantable cardioverter defibrillators Hospital 1,815 2,000,000
ACTION-GWTGAcute coronary syndrome
STEMI and NSTEMIHospital/EMS 1030 1,200,000
PVICarotid artery revascularization
Lower extremityHospital/Free Standing 214
350,000
(CAS& CEA)
IMPACTCongenital heart disease
Pediatric and AdultHospital 100 70,000
STS/ACCTVT Transcatheter Valve Therapy Hospital 470 75,000
LAAOLeft atrial appendage occlusion
proceduresHospital 159 1,500
AFAblation AFablation procedures Hospital 41 1,500

ACC/AHA/STS Sta tement on the Future of Regis triesand The Performance Measurement Ente rprise .
J Am Coll Cardiol; October 2015
TechnologyAssessment
ClinicalResearch
QualityImprovement
Clinical RegistriesNot Just Data

JACCDecember
2015
Involvement in the NCDRsuch asPINNACLEallowsclinicianstosubmit Physician Quality ReportingSystem to CMS. Additional NCDR-
related practice improvement programsare beingdeveloped toleverage NCDRregistriesto make it easier for the 21,881 unique
providersto successfully engage MACRA.

QCDRand MACRA
QCDR (CMS) certified regis tries :PINNACLE & Diabe tes Collabora tive Regis try
and hopefully CATHPCI coming year.GAPS: ICD, PVI and ACTION

2019 MIPSComposite Weighting
Quality60%
Resource Use (0%) will be incorporated into MIPS score(10%) in 2018 performance period
Advancing Care Information• Security Risk Analysis• E-Prescribing• Provide Patient Access• Send Summary of Care• Request/ Accept Summary of
Care• Bonus: Registry Reporting
Clinical PracticeImprovement
• Expanded Practice Access• Population Management• Care Coordination• Beneficiary Engagement• Patient Safety• Practice Assessment (ex.
MOC)• Patient-Centered Medical Home or
specialty APM
Quality•Most PQRS measures•QCDR (non-MIPS) measures•Bonus: “High-priority measures”
– Outcome, appropriate use,patient safety, efficiency,patient experience, carecoordination

Quality (60%)Full Credit
•6 quality measures, including 1 outcome measure or onespecialty measure set
•Points will be allocated based on performance against prior yearbenchmarks
•QCDRsapproved for group and individual level reporting
BonusPoints
•“High Priority Measures”– Outcome, appropriate use, patient safety, efficiency, patient experience,
care coordination
MIPS APM participants will report the quality measurerequirements of their program
High Priority Measures collected in NCDRRegistries:Outcomesand AUC
GAPS: PROMS-SAQ, Cost data
Can use MIPSand also non-MIPSmeasuresfrom NCDRQCDR(CMS) certified
and non-certified registries

Advancing Care Information (25%)
Full Credit
• Report 5 required measures for atleast 90 days
BonusPoints
• Submit up to 9 additionalmeasures for at least 90 days
– Clinical Data Registry Reporting
RequiredMeasures
Security Risk Analysis
E-Prescribing
Provide Patient Access
Send Summary of Care
Request/ AcceptSummary of Care
BonusPoints for QCDRreportingPINNACLE, Diabetes, next year CathPCI
Gaps: ICD, ACTION, PVI

Clinical Practice Improvement ActivitiesA KeyComponent of MIPS
Quality60%
Resource Use (0%) will be incorporated into MIPS score(10%) in 2018 performance period
Advancing Care Information• Security Risk Analysis• E-Prescribing• Provide Patient Access• Send Summary of Care• Request/ Accept Summary of
Care• Bonus: Registry Reporting
Clinical PracticeImprovement
• Expanded Practice Access• Population Management• Care Coordination• Beneficiary Engagement• Patient Safety• Practice Assessment (ex. MOC)• Patient-Centered Medical Home or
specialty APM
Quality•Most PQRS measures•QCDR (non-MIPS) measures•Bonus: “High-priority measures”
– Outcome, appropriate use,patient safety, efficiency,patient experience, carecoordination

Clinical Practice Improvement (15%)
Full Credit
• 4 medium-weighted activities or2 high-weighted activities
• At least 90 days of participationin each activity
Bonus Points
• None
Activity Weight
Participation in MOC Part IV Medium
Participation in CMMI Models such asthe Million HeartsRisk ReductionModel
Medium
Use of QCDRdata for ongoing practiceassessment and improvements
Medium
Use of decision support andstandardized treatment protocols
Medium
Activity Weight
Participation in a systematicanticoagulation program
High
Participating in CAHPS or othersupplemental questionnaire
High
A Strength of ACCand NCDR!!Development of Mobile APP

Clinical Practice Improvement ActivitiesA Mobile NewApproach
18
Da ta Driven Flexible Structure MobileIntegrated
Leverage ACC’s 8 inpatient and2 outpatient registries to selectareas for improvement
Registries provide ability totrack performance overtime
Incorporate ACC’s evidence-based strategies and toolkits andpromote best practice sharing
Programs include: Door2Balloon, Hospital-to-Home,SurvivingMI, ACC PatientNavigator
Access data and participate inclinical practice improvementactivities in a mobileenvironment
Flexible coaching format thatallows participant to constructan improvement activity toalign with local goals andobjectives rather than overlydirective
Guided self-assessment of goalachievement and personalengagement allow participantto reflect on skills andknowledge gained, andsustaining clinical practicegains for patient care

MobileAppOfferingOverview
19
• See My Data 1: Clinicians can access their dashboard to track andcompare their performance to national benchmarks and identify caregaps and areas of strength.
• Choose My Improvement: Convenient access to the ACC’s qualityinterventions as well as self-guided programs that allow clinicians toleverage insights and NCDR data in a self-guided clinical practiceimprovement activity. Provides access to a survey question instrument toprovide reflection on QI activities.
• Know MyProgress: See a summary of current quality improvementactivities, data review history, and status on all MOC activity: licensure,lifelong learning/ self-assessment, board certification and practice self-assessment.
• Submit My Activities2: Choose to have the ACC automatically submitclinical practice improvement activities based on NCDR data to multipleaccrediting boards and receive email confirming participation.
• Get My Alerts: Provides new data notifications, MOC reminders, whenthere is an opportunity for an MOC activity, when a practice has claimedyou as a physician as well as other helpful reminders.
• Learn More : Provides helpful resources for clinicians including MOC,reimbursement, quality improvement and PQRS reporting information.
Program components via a convenient, streamlined app as well as online within acc.org
ClinicalPractice
ImprovementApp
• Performance based on ACC registry participation (e.g. PINNACLE,CathPCI, ICD).
• Dashboard provide all metrics as well as recommended metric sets.

Data Driven“SeeMyData”
20
Save Metrics to Review and Track
Select Group of Metrics to ReviewCompare Performanceto Na tional Benchmarks
Prototype displayed, actual product may vary

Data Driven“SeeMyData”
21
Compare specific benchmarksto nationa l averages
Prototype displayed, actual product may vary

22
Prototype displayed, actual product may vary
Describe problem youimproved
Identify QI methodology
Flexible, yet Structured“MyClinical PracticeAssessment”

Flexible, yet Structured“MyClinical PracticeAssessment”
23
Prototype displayed, actual product may vary
Evaluate practiceassessment activities

IntegratedFutureReleases…
24

Member Survey:Clinical Practice Improvement App
• Do users understand the value proposition?– Yes, users very enthusiastic about having an easy to use tool for managing this
task, which they were not anxious to have to added to their workload
• Can users use the tools on the tool as intended?– Does the product help users identify opportunities for CPIAs,
create evidence, and track compliance with MACRA?• Users want help with defining a practice improvement activity and
understanding the types of evidence that would apply.
– Does App navigation work with minimal error/ recovery?– It appears to…. not thoroughly tested as the prototype was not interactive.
• Do users think the tool has useful content?– Users really liked NCDR data on their phone and said they would look at NCDR
data more often
• What are areas of confusion or frustration?– What would constitute a practice improvement activityand how a photograph would document it.
25
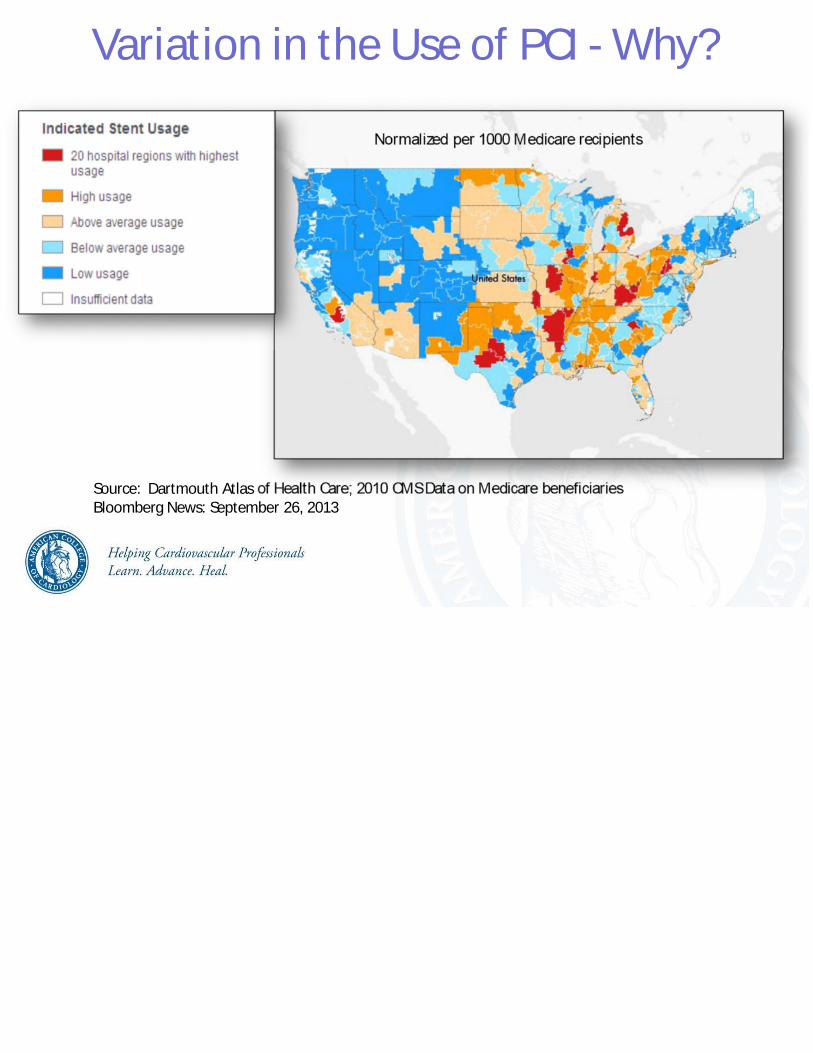
Variation in the Use of PCI - Why?
Source: Dartmouth Atlas ;Bloomberg News: September 26, 2013

California Elective PCI VariationCalif or nia Healt h Car e Foundat ion


PCI AUCMetrics

Top Reasonsfor which CADRevascularization isRarely Appropriate
1. Asymptomatic with 1 or 2 vessel disease• No or minimal anti-ischemic mediations• Low or intermediate risk findingson noninvasive study
2. Asymptomatic with 1 or 2 vessel disease• Maximal anti-ischemic medications• Low risk findingson noninvasive study
3. CCSClass I or II with 1 or 2 vessel disease• No or minimal anti-ischemic mediations• Low risk findingson noninvasive study

Chan PS et a l. J AMA 2011;306:53-61

Hospital Variation inNon-Acute PCI Inappropriateness
Chan, PS, e t.a l“Appropria teness of PCI”JAMA 2011;306:53-61.
Overa ll 11.6% Inappropria te


Study Population
Percutaneous coronaryinterventions between July 1, 2009and December 31, 2014 submitted
to NCDR CathPCIRegistry(n=3,604,365; 1561 hospitals)
Final Study Cohort(n=2,685,683; 766 hospitals)
Exclusions• Hospital did not participate in NCDR
CathPCI registry over the entire studyperiod (n=550,836; 583 hospitals)
• Hospital with an average of fewer than10 non-acute PCIs per year (n=273,167;212 hospitals)
• Second PCI if multiple PCIs in a singlevisit (n=94,679)

Trends in Indication for PCIPCIindication/ Year
Overall 2009* 2010 2011 2012 2013 2014
Overall, n 2,685,683 243,580 538,076 502,995 481,889 462,636 456,507
Acute, n(%)
2,047,853(76.3)
168,366(69.1)
377,540(70.2)
373,423(74.2)
380,331(78.9)
373,650(80.8)
374,543(82.0)
Non-acute, n(%)
397,737(14.8)
41,024(16.8)
89,704(16.7)
78,328(15.6)
66,849(13.9)
62,457(13.5)
59,375(13.0)
Non-mappablen (%)
240,093(8.9)
34,190(14.0)
70,832(13.2)
51,244(10.2)
34,709(7.2)
26,529(5.7)
22,589(4.9)
*Includes 6-months of data (July 1 to December 31, 2009)

2010 2014Absolute Change from
2014-2010
Patient Characteris tics # % # % # %
N 89,704 22.6 59,375 14.9 -30,329 -7.7
AnginaNo symptoms 26,313 29.3 12,890 21.7 -13,423 -7.6
CCS I or II 47,710 53.2 23,689 39.9 -24,021 -13.3
CCS III or IV 15,681 17.4 22,796 38.4 +7,115 +21.0No. of antianginal medications0 27,076 30.2 11,521 19.4 -15,555 -10.8
1 42,610 47.5 27,031 45.5 -15,579 -2.0
>=2 20,011 22.3 20,816 35.1 +805 +12.8
Stress test results (those with a test)Unavailable 10,328 18.4 4,708 11.2 -5,620 -7.2
Low or intermediate risk 33,468 59.5 23,475 55.6 -9,993 -3.9
High risk 12,460 22.2 14,018 33.2 +1,558 +11.0Multi-vessel CAD on angiography 39,231 43.7 28,192 47.5 -11,039 +3.8
Baseline CharacteristicsAmong PatientsUndergoing Non-acute PCI

0
20
40
60
80
100
Year
10
30
50
70
90
2009* 2010 2011 2012 2013 2014
*Includes July to December 2009
ropriate
certain
ppropriateNo
n-a
cute
PC
Is,%
Patient-level Trends inAppropriatenessof Non-acute PCI

0
20
40
60
80
100
Year
10
30
50
70
90
2009* 2010 2011 2012 2013 2014
*Includes July to December 2009
No
n-a
cute
PC
Is,%
50%relativereduction,p<0.001
Patient-level Trends inAppropriatenessof Non-acute PCI
propriate
certain
ppropriate

0
20
40
60
80
100
No
n-a
cute
PC
Iscl
ass
ifie
da
sin
ap
pro
pri
ate
,%
Year
10
30
50
70
90
2009* 2010 2011 2012 2013 2014
*Includes July to December 2009
Hospital-level Trends inInappropriate Non-acute PCIs
Median(IQR)
25.8(16.7-37.1)
24.3(15.2-33.3)
21.4(13.3-30.7)
17.0(9.1-26.8)
14.3(6.3-24.4)
12.6(5.9-22.9)

Appropriate Use Criteria

Professional Responsibility
JACC 2011; 57:1557-59
“Although this sounds onerous, is it not better for us to imposethese controls on ourselves than what is done currently by
payers to control costs and procedures.”

SMARTCare:Smarter Management And Resource Use
for Today’s Complex Care Delivery
Center for Medicare Medicaid InnovationProject Grant
Florida ChapterWisconsin Chapter
American College of Cardiology

• SMARTCare:Smarter Management And Resource Use for Today’s Complex Care Delivery
Appropriate Access to CareImproving QualityReducing Cost and Enhancing Value
Evidence-based GuidelinesTechnology at the point-of-careState-of-the-Art Data Analytics
By Improving the Science of Medicine
Improving the Outcomes of Medicine
A collaborative effort sponsored by theAmerican College of Cardiology to:
Reduce variation and cost while•Improving the quality of care in patients with established or potential CAD•Employing proven clinical software tools at the point of care

• Decrease imagingnot meeting AUCfor 12-15%to <8%• Decrease PCI not meeting AUCfrom 9-20%to <6%• Reduce the average rate of bleeding andcomplications to lessthan 2%
• Improve patient quality of life (based on the patientsurveys)
45

CMSBundled PaymentsProposed Model
• Mandated bundled payments for 3 episodesofcare announced August 2, 2016
• Acute MI
• CABG
• Hip or Femoral Fractures
• 5-year Demonstration Project for increasingparticipation/retention in cardiac rehab postCABG& MI– Beginning July 2017 in 98 randomly selected areas

MACRA andPopulation Health Management
JACCOctober 2016
Discussesthe need to focusonPopulation Health Management
and upcomingCV Bundled Payments

ACCMACRA WebsiteEducation and Communication to Members

ACCMACRA Website
Quality Payment Program Information– Merit-Based Incentive Payment System
– MIPS: Clinical Practice Improvement
– MIPS: Resource Use
– Advanced Alternative Payment Models
– Advanced APM Overview
Articles
ACCAction
Education and Meetings– 2017 Cardiovascular Summit
Resources
Videos

Message to Physicians
• Be aware of the changinglands cape– “You can run, but you can ’t hide ”
– Sticking your head in the sandwill not work
• Unders tand tha t th is will a ffec t yourprac tice and how you are pa id in the future
• Now is the time to ge t involved with your da ta– If you’re not a t the table , you’re on the menu