
PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
108
PHYSIOLOGY / PATHOLOGY OF THE PUL MONAR Y SYSTE M Michael Guerra, PA!C, MS 1
Transcript of PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 1/108
PHYSIOLOGY / PATHOLOGYOF
THE PULMONARY SYSTEM
Michael Guerra, PA!C, MS
1
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 2/108
Contact MePlease feel free to contact me if you have any questionsor comments about today’s lecture.
2
2

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 3/108
Objectives
Part 1
• Understand normal pulmonary physiology
• Ventilation: transport of gas to alveoli
• Respiration: alveolar-capillary gas exchange• Pulmonary Defense mechanisms
3
3
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 4/108
Objectives
Part 2
• Understand common pathology affectinglungs
• Gas transport problems
• Gas exchange problems
• Pulmonary Defense mechanism failures
4
4
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 5/108
Function of Pulmonary System
• Provides O2
• Eliminates CO2
• Regulate H+ concentration (body pH)
• Phonation
• Defense
• Controls enzymes
• Dissolves blood clots
5
5

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 6/108
Anatomy of AirwaysConducting airways
• Upper airways
• Nasopharynx
• Oropharynx
Larynx
• Connects upper and lowerairways
Lower airways
• Trachea
• Bronchi
• Terminal bronchioles
• Alveoli 6
6

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 7/108
Airway Anatomy
• Upper Airway
• Transition
• Lower Airway
7
7

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 8/108
Conducting Airways
• Defenses: cough, sneeze, mucocilliary
elevator traps and eliminates microbes,chemicals foreign matter
• Warms and humidifiers air
• Low resistance pathway to alveoli
8
8

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 9/108
Conducting Airways
• Defenses: cough, sneeze, mucocilliary
elevator traps and eliminates microbes,chemicals foreign matter
• Warms and humidifiers air
• Low resistance pathway to alveoli
8
8

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 10/108
Ventilation -vs- Respiration
Conducting Airways (ventilation)
• Trachea, bronchi, bronchioles, terminal
bronchioles
Airways that exchange gases (respiration)
• Respiratory bronchioles• Alveolar ducts
• Alveoli9
9

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 11/108
Histology of Airways
• MOST airway
resistance is in larger
(non-respiratory)
conducting airways
• Respiratory (small)
airways offer LEASTairway resistance--
why?
10
10

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 12/108
Ventilation
• Movement of gas or air into and outof the lungs (your text definition)
• Not necessarily reflected in observedresp. rate
1) Provides O2 for respiration2) Eliminates CO2 fromrespiration
11
11
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 13/108
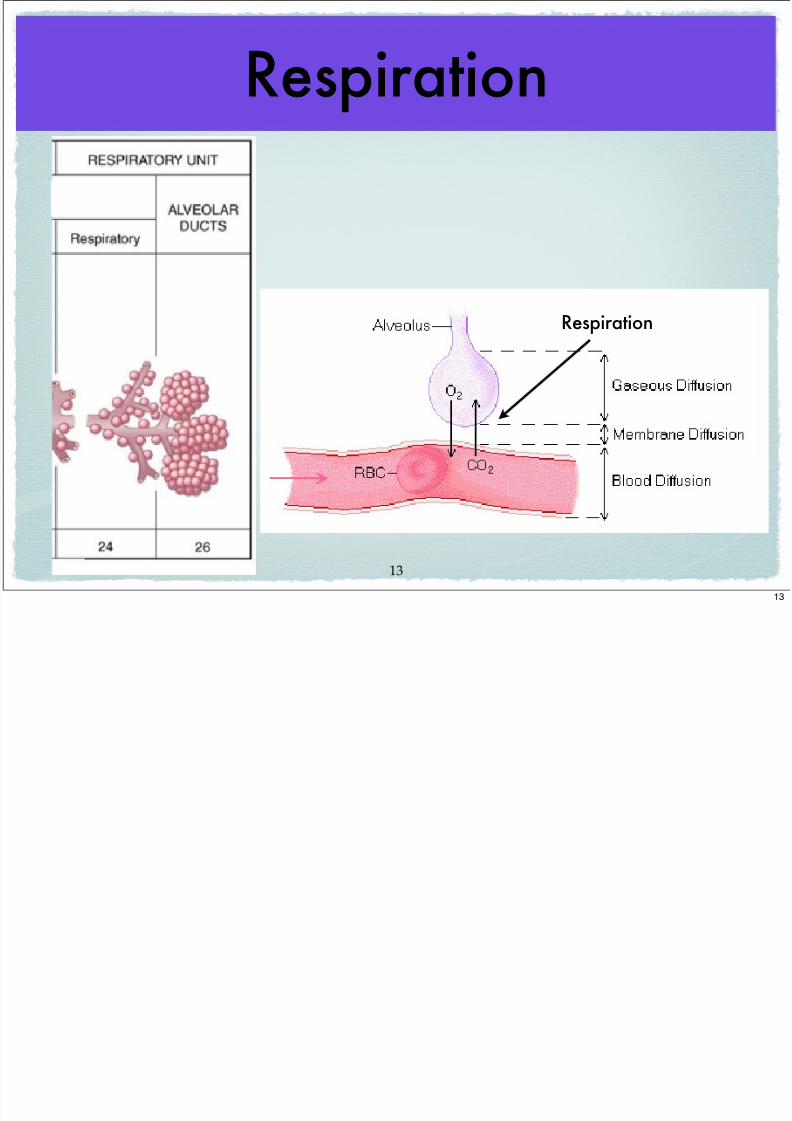
Respiration
• The exchange of oxygen and carbon
dioxide during cellular metabolism (your
text definition)
• Occurs in the “Respiratory Bronchioles”
and Alveoli
12
12
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 14/108
Respiration
Respiration
13
13
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 15/108
The Alveoli
• 300 million: surface area = tennis court
• Type 1 Alveolar cells: epithelial, flat onecells
• Type 2 Alveolar cells: thicker, surfactantproducing cells
14
14
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 16/108
Alveoli Histology
15

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 17/108
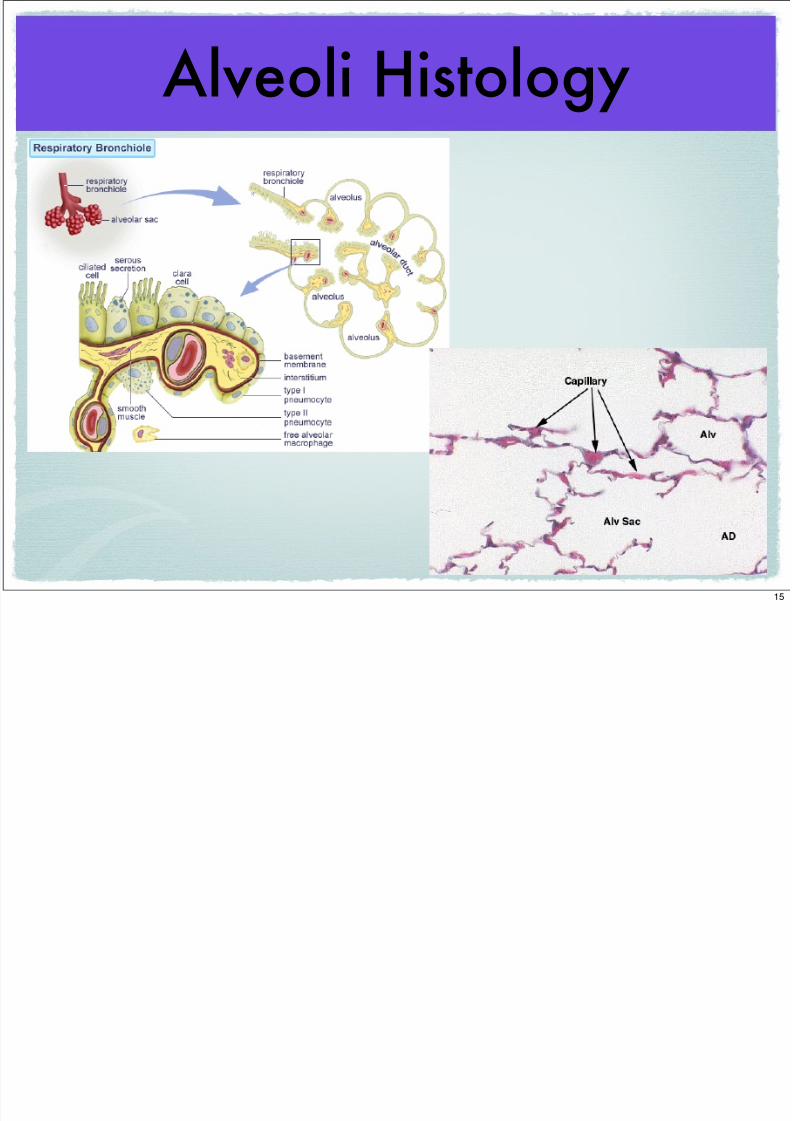
Alveoli Histology
alveolar air : alveolar capillary separated by 0.2 microns
15
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 18/108
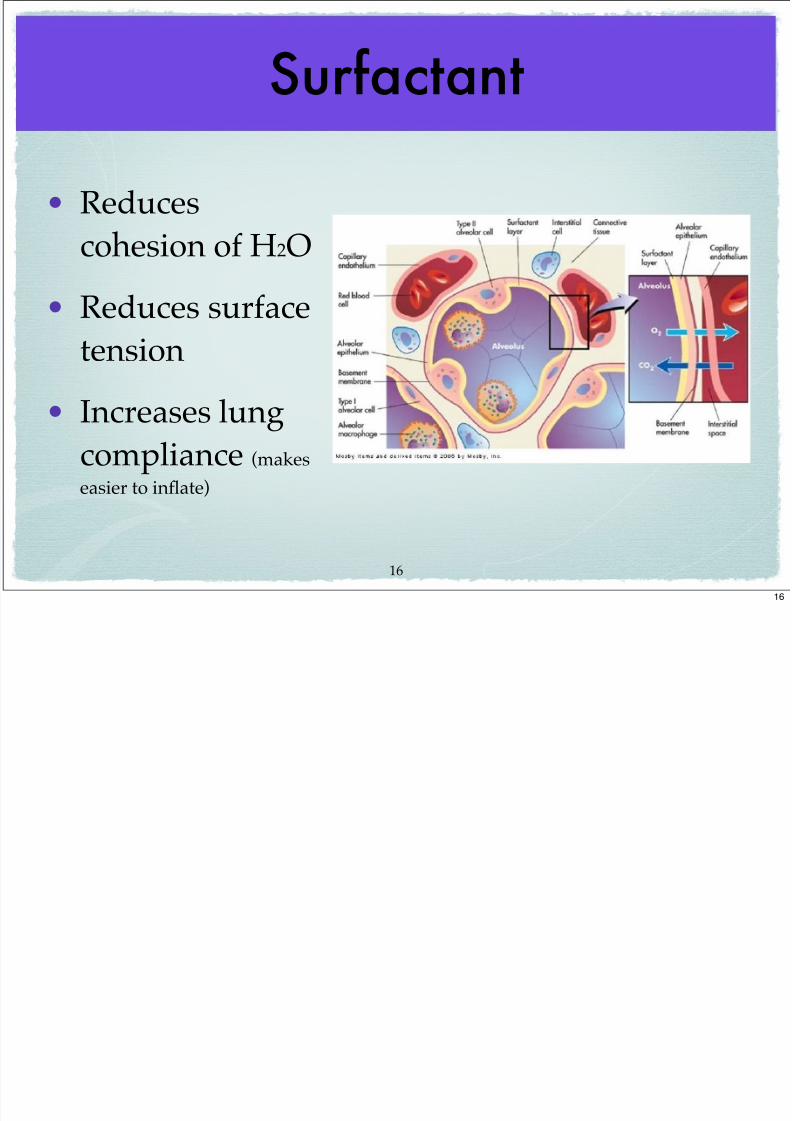
Surfactant
• Reduces
cohesion of H2O
• Reduces surface
tension
• Increases lungcompliance (makes
easier to inflate)
16
16
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 19/108
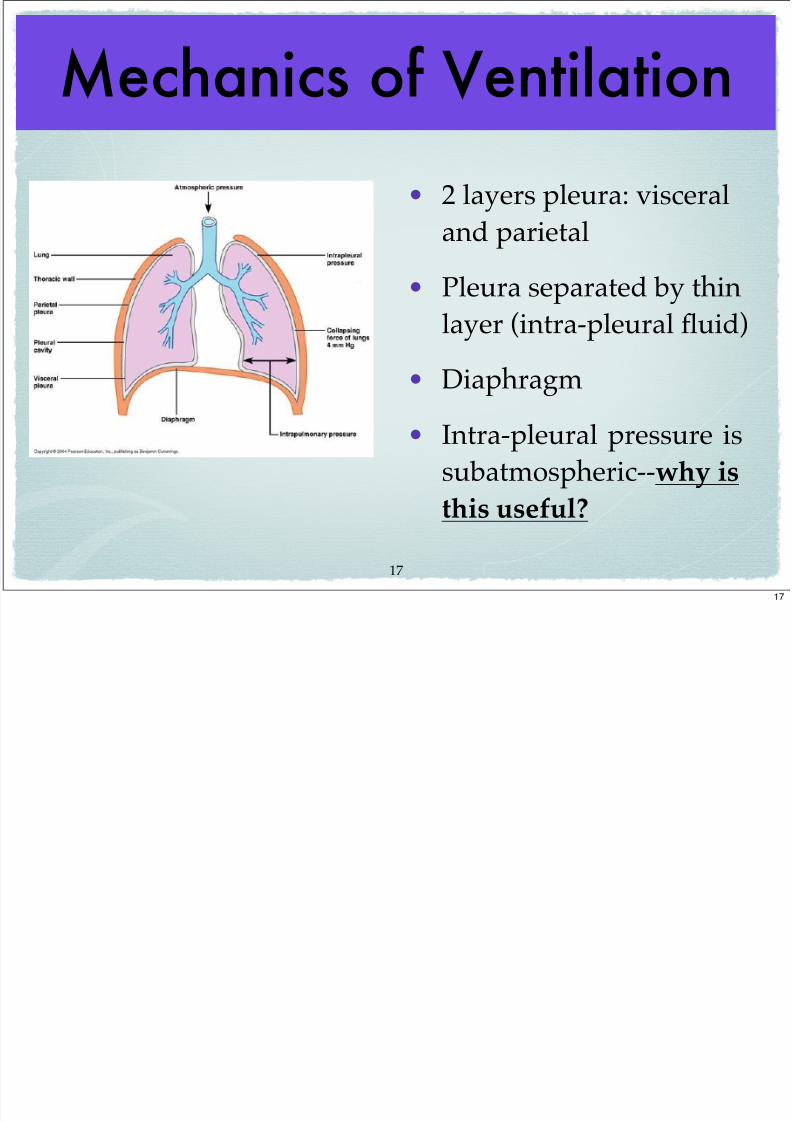
Mechanics of Ventilation
• 2 layers pleura: visceral
and parietal
• Pleura separated by thinlayer (intra-pleural fluid)
• Diaphragm
• Intra-pleural pressure is
subatmospheric--why is
this useful?
17
17

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 20/108
Ventilation Physiology• Air moves from high (gas in mouth) to low (gas
in alveoli) pressure
• Flow is proportional to change in pressure
between high and low points
• Flow is inversely proportional to airway
resistance (most affected by diameter of airways)
• Pressures in lungs are at atmosphericpressure (760 mmHg at sea level)
18
18

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 21/108
Boyle’s Law
• Volume of a container
and Pressure within
that container are
inversely related (at
constant temp.)
• Lung expansion (inc.volume container) will
decrease pressure of
gas in lungs19
expiration
inspiration
19

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 22/108
Boyle’s Law
• Volume of a container
and Pressure within
that container are
inversely related (at
constant temp.)
• Lung expansion (inc.volume container) will
decrease pressure of
gas in lungs19
expiration
inspiration
19
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 23/108
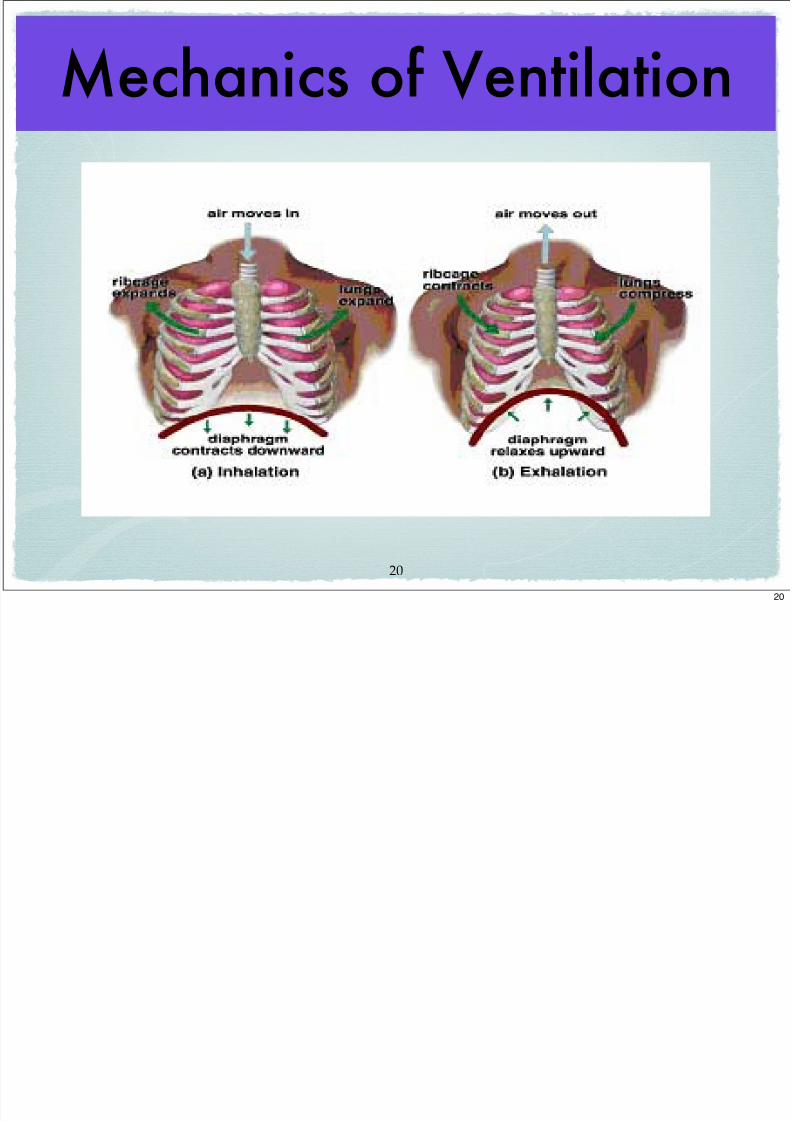
Mechanics of Ventilation
20
20

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 24/108
Elasticity / Compliance(opposing forces)
• Compliance
(stiffness) is a
measure of lungand chest
distensibility
• Elasticity is a
measure of recoil
property of lungs(think rubber band) 21
21

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 25/108
Pneumothorax
• Elastic recoil of lung will collapse if sub-
atmospheric intrapleural pressure is lost
22
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 26/108
Pulmonary Circulation• Hypoxic vasoconstriction (low PAO2)
• Blood is shunted to well-ventilated portions of
the lungs
• Better ventilation-perfusion matching
• Excessive pulmonary hypoxia all segments of
the lungs--may result in vasoconstriction and
pulmonary hypertension
• Acidemia also causes pulmonary artery
constriction
23
23
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 27/108
Neurolgy of Ventilation
Neurochemical control
• Lung receptors
• Irritant receptors
• Stretch receptors
• J-receptors
Chemoreceptors
• Central chemoreceptors
24
24
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 28/108
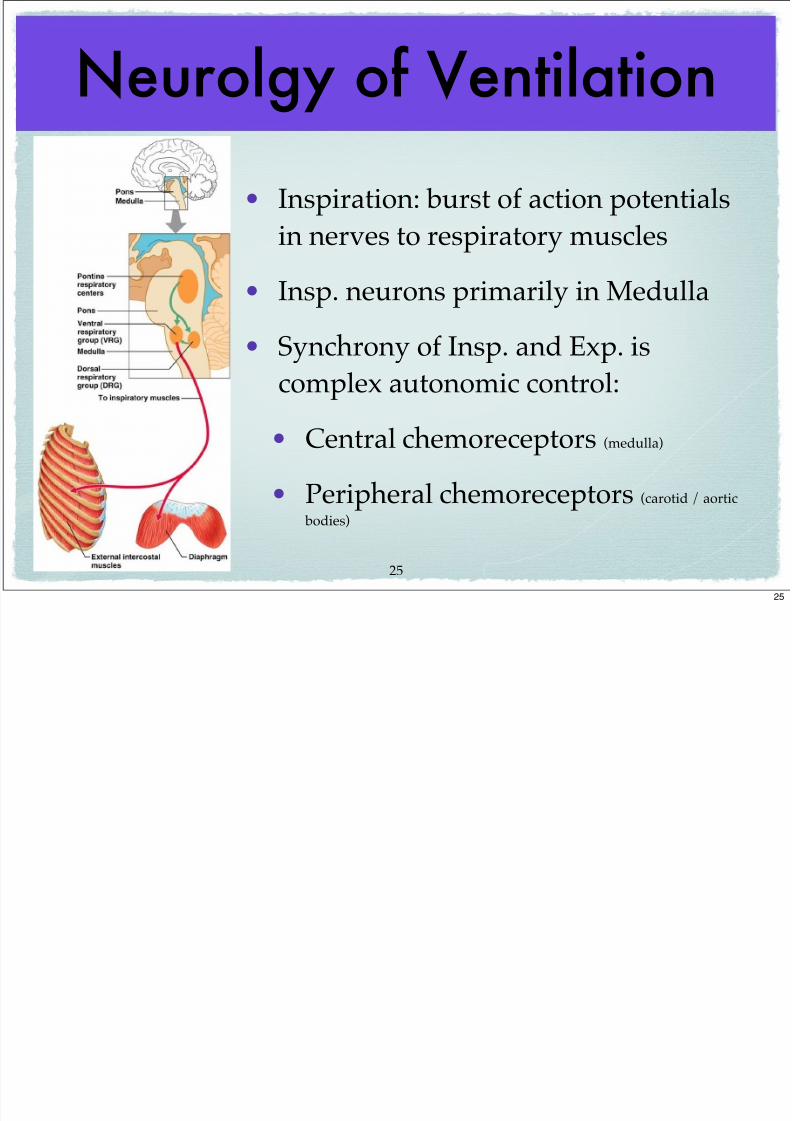
Neurolgy of Ventilation
• Inspiration: burst of action potentials
in nerves to respiratory muscles
• Insp. neurons primarily in Medulla
• Synchrony of Insp. and Exp. is
complex autonomic control:
• Central chemoreceptors (medulla)
• Peripheral chemoreceptors (carotid / aortic
bodies)
25
25

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 29/108
Summary of Inspiration• Diaphragm and inspiratory muscles contract
• Thorax expands
• Increase pressure gradient: mouth > lungs
• Pressure in lungs becomes
subatmospheric
• Lungs expand
• Air flows into alveoli
IN
26

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 30/108
Summary of Expiration
• Diaphragm and inspiratory muscles STOP
contracting
• Thorax contracts
• Increase pressure gradient: lungs > mouth
• Lungs recoil (due to elasticity)• Air flows out of alveoli
OUT
27
h

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 31/108
Atmospheric Gases
28
21%
78%
Earth Barometric Pressure = 760mmHg (sea level)
28

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 32/108
Dalton’s Law of Partial Pressure
159mmHg
592mmHg
Earth Barometric Pressure = 760mmHg (sea level)
29
29
Al l G
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 33/108
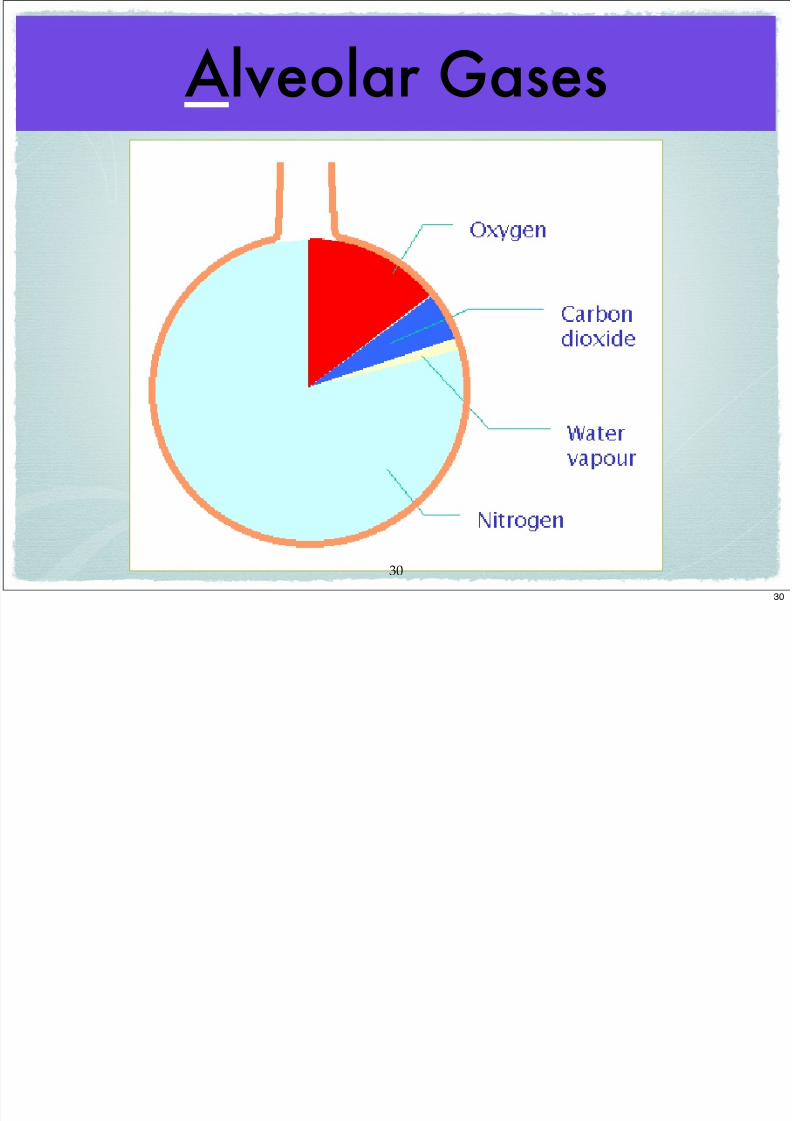
Alveolar Gases
30
30
R i i

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 34/108
Respiration
31
31
A G di t

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 35/108
A-a Gradient(Alveolar-arterial Gradient)
• Reflects difference between Alveolar
oxygen and arterial blood oxygen
• Average is 5-10mmHg
• e.g. 105 PAO2– 95 PaO2• = A-a gradient of 10mmHg A=105
a=9532
32
F ff i R i i
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 36/108
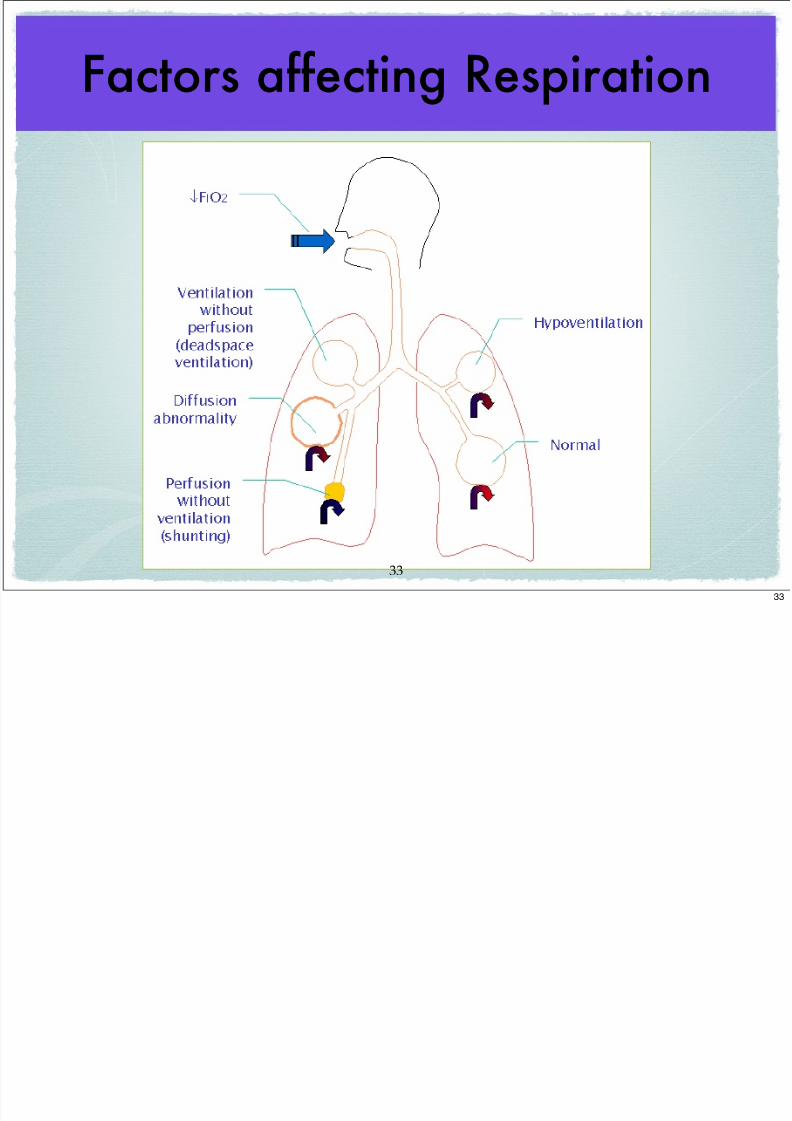
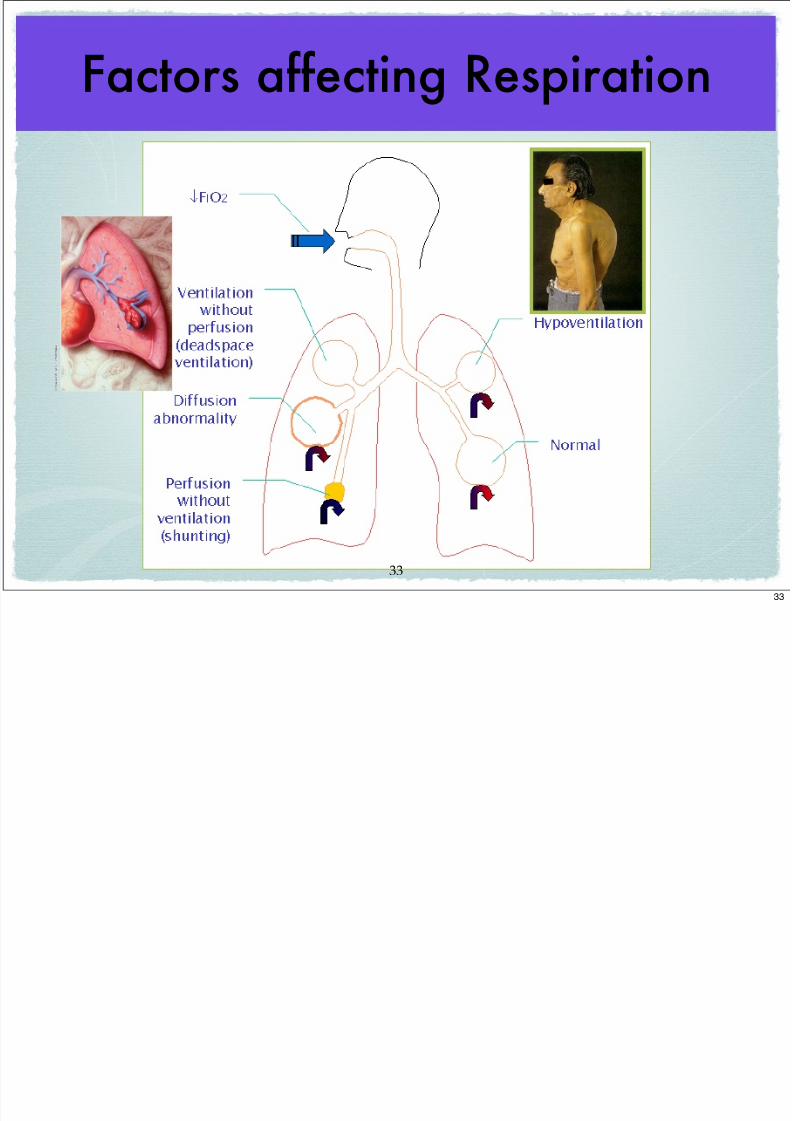
Factors affecting Respiration
33
33
F ff i R i i
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 37/108
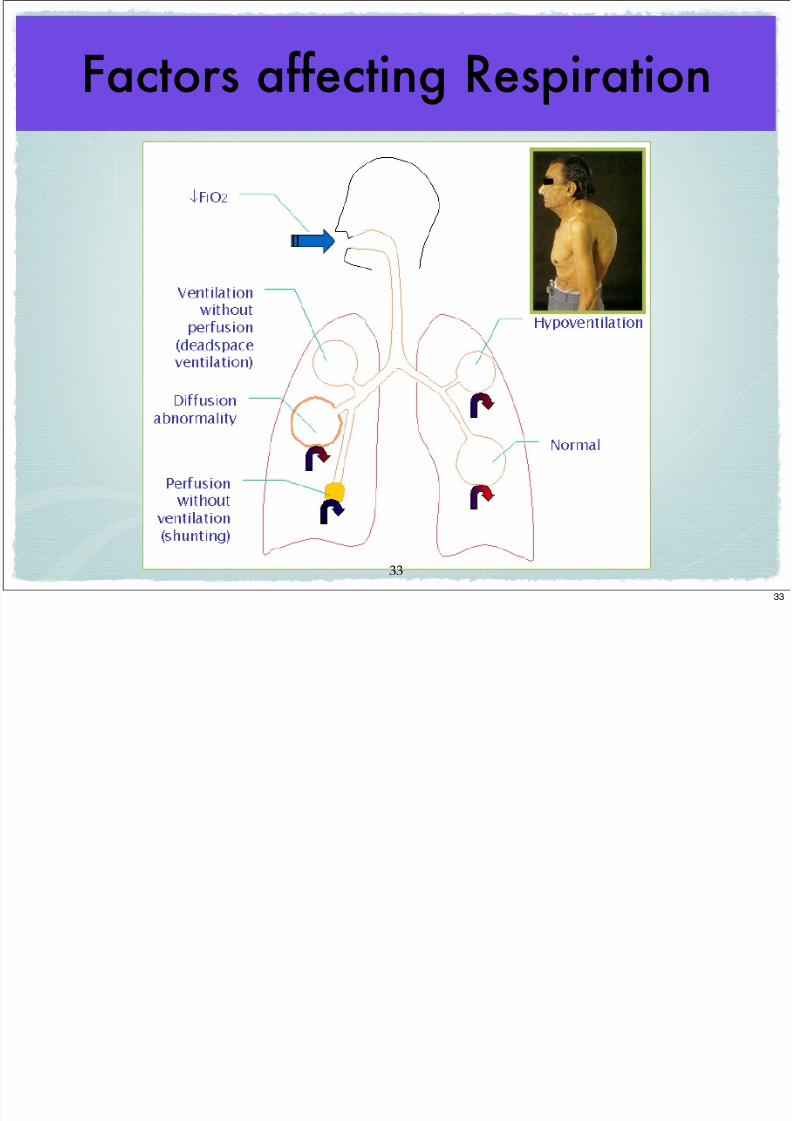
Factors affecting Respiration
33
33
F ff i R i i
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 38/108
Factors affecting Respiration
33
33
Al l O2

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 39/108
Alveolar O2
• Factors that result in changes in PAO2
are:
• PACO2
• Inspired Oxygen concentration (room air
versus enriched O2)• Ventilation
34
34
Al l CO2
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 40/108
Alveolar CO2
• Factor which results in changes inPACO2 is:
• Ventilation
35
35
H i
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 41/108
Hypoxemia (low arterial O2)
• Resting PaO2 normally > 70mmHg
• A PaO2 of 60mmHg is lower limit of safety
• Decreases in PaO2 occur with:
• aging
• Intracardiac shunt
• Intrapulmonary shunt
• V/Q mismatch
• Alveolar hypoventilation (high CO2)36
36
C f H i

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 42/108
Causes of Hypoxemia
• 1) Decreased O2 content (think high altitude)
• 2) V/Q (ventilation/perfusion) mismatch)
• 3) Shunt (R to L)
• 4) Diffusion problem
• 5) Hypoventilation (this means HIGH CO2 NOT
decreased resp. rate--think COPD)
37
37
C Hi h t i l CO2
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 43/108
Causes High arterial CO2• Anything that impairs normal
ventilation
• Acute and chronic respiratory failure
• Respiratory arrest
• COPD
• Neuromuscular diseases
• V/Q mismatching
38
38
O h l bi Di i ti C

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 44/108
Oxyhemoglobin-Dissociation Curve
Many
reasons for normal
curve to
shift leftleft or rightright
Carbon Monoxide poisoning
Fever
39
39
Causes of Low arterial CO2
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 45/108
Causes of Low arterial CO2
• Anything that increases ventilation
• Acute anxiety (hyperventilation)
• Compensatory responses to: Metabolic
problems
• Hypoxemia (think asthma andpneumonia)
40
40
Review Questions

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 46/108
Review Questions1) Surfactant is produced by type 2 alveolar cells, and allows alveoli to inflate at
LOWER intra-pulmonary gas pressure.
• a) TRUE
• b) FALSE
2) A patient in DKA (Diabetic Ketoacidosis) presents with a RR of 40 breaths per
minute. Given this information, you may assume this patient has:
• a) hypoxemia
• b) hypoventilating
• c) an arterial CO2 that is likely high
• d) an arterial CO2 that is likely low
41
41
Review Questions
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 47/108
Review Questions
3) BOTH O2 and CO2 have similar diffusion coefficients (diffuse through alveoli to
capillary with equal ease).
• a) TRUE
• b) FALSE
4) Premature birth (before development of type 2 cell development) will result in an
infant with:
• a) increased lung compliance
• b) decreased lung compliance
• c) no impairment of normal lung compliance
42
42
Review Questions
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 48/108
Review Questions
5) Elasticity of the lungs is DECREASED in patients with advanced emphysema.
• a) TRUE
• b) FALSE
6) The MOST influential factor influencing ventilation in otherwise healthy humans
is:
• a) peripheral chemoreceptors
• b) central chemoreceptors
• c) J-receptors
• d) Lung stretch receptors
43
43
Review Questions
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 49/108
Review Questions7) Diaphragmatic relaxation and the lung recoil account for expiration while breathing normally at rest.
• a) TRUE
• b) FALSE
8) The partial pressure of oxygen varies according to barometric pressure (BP) of the
surrounding atmosphere. What would be the approximate partial pressure of O2 at a
BP of 600mmHg.
• a) about 160mmHg
• b) about 200mmHg
• c) about 126mmHg
• d) about 760mmHg
44
44
Review Questions

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 50/108
Review Questions9) Ventilation is the single MOST important factor regarding changes in Alveolar
CO2.
• a) TRUE
• b) FALSE
10) Arterial PaO2 in a blood gas sample is noted to be 59mmHg. You correctly
conclude that the corresponding O2 saturation (think dissociation curve) is about:
• a) 100%
• b) 90%
• c) 80%
• d) 70%
45
45
BREAK!

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 51/108
BREAK!
46
46
Pulmonary Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 52/108
y p y gy(when things go wrong)
Michael Guerra, PA!C, MS
47
47
Definitions
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 53/108
Definitions
Dyspnea: subjective sense of SOB oruncomfortable breathing
• Subjective: the patient tells you they feel(not
the clinician’s perception)
• Many etiologies
• Mechanism unclear: possibly due to changesin chest wall / lungs / chemoreceptors:
afferents stimulate CNS DYSPNEA
48
48
Definitions

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 54/108
Definitions
• Hypoxemia: low arterial blood oxygen
• Hypoxia : low cellular oxygen (mitochondria)
• Hypercapnia: elevated arterial CO2 (hypoventilation)
• Hypocapnia: low arterial CO2 (hyperventilation)
• Atelectasis: alveolar collapse
• compression vs absorption
49
49
Definitions
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 55/108
Definitions• Orthopnea: dyspnea associated with position of lying
down (many causes)
• PND (Paroxysmal Nocturnal Dyspnea): acute
positional (lying) dyspnea; often awakens pt. from sleep(think CHF)
• Hypoventilation: inadequate alveolar ventilation
(elevated CO2)
• Hyperventilation: excessive alveolar alveolar
ventilation (low CO2)
5050
Definitions

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 56/108
Definitions
• Cyanosis: bluish skin discoloration due
to desaturated hemoglobin.
• Desaturate 5g of available Hb todemonstrate clinical cyanosis
• Many etiologies
• LATE objective evidence ofhypoxemia
5151
Definitions
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 57/108
Definitions
• Cyanosis: bluish skin discoloration due
to desaturated hemoglobin.
• Desaturate 5g of available Hb todemonstrate clinical cyanosis
• Many etiologies
• LATE objective evidence ofhypoxemia
Can a patient be cyanotic and NOT have hyoxemia?
5151
Cough
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 58/108
CoughAcute: (< 3 wks duration);
• is usually inflammatory; URI, pneumonia, acute
asthma attack
Chronic: ( > 3wks duration);
• in non-smokers usually post-nasal drainage
• in smokers usually chronic bronchitis• also think about: GERD, CHF, Asthma, CA,
• Drugs: ACE and Beta Blockers
5252
Pulmonary Pain

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 59/108
Pulmonary PainMay originate in parietal pleura, airways or chest wall
• 1) Pleural pain: worse with respiratory motion (pleurodynia)
• acute pleurisy, PE or infarct
• 2) Airways: central or global chest pain
• acute bronchitis and pneumonia
• 3) Chest Wall: soft tissue, muscle, rib
• often reproducible on PE (costochondritis)
5353
Digital Clubbing
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 60/108
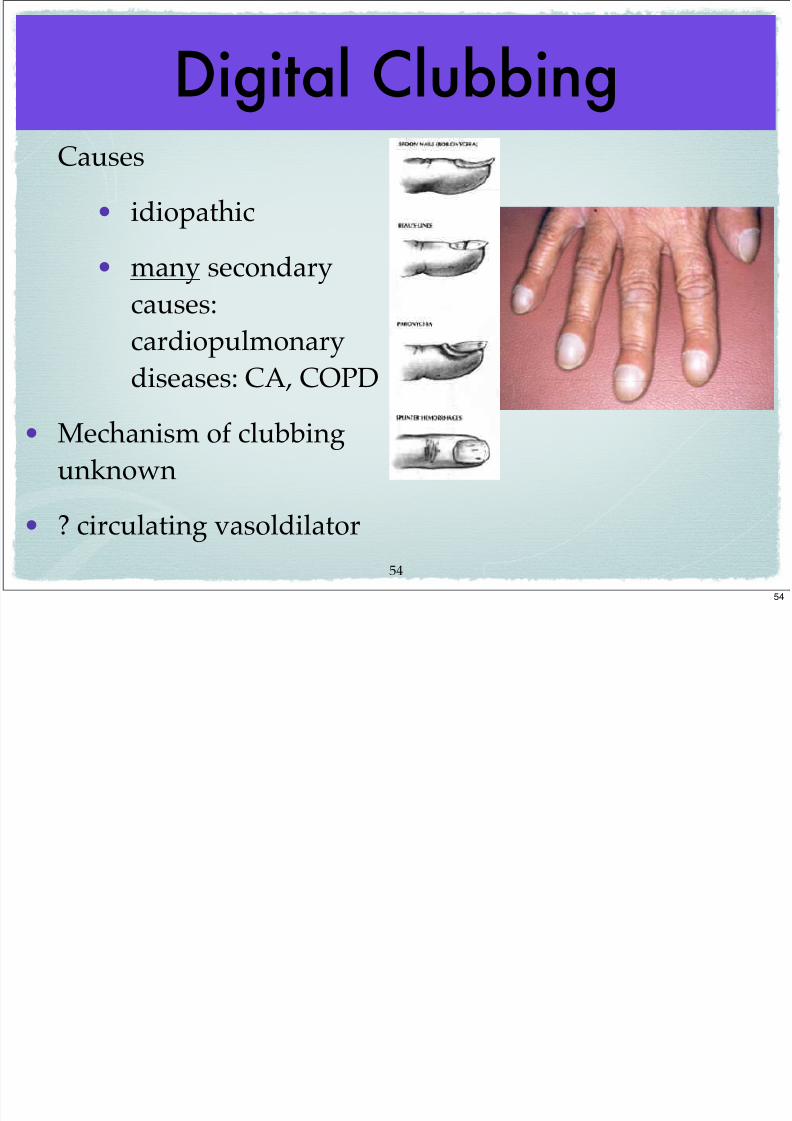
Digital ClubbingCauses
• idiopathic
• many secondary
causes:cardiopulmonary
diseases: CA, COPD
• Mechanism of clubbingunknown
• ? circulating vasoldilator
5454
Lung Pathology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 61/108
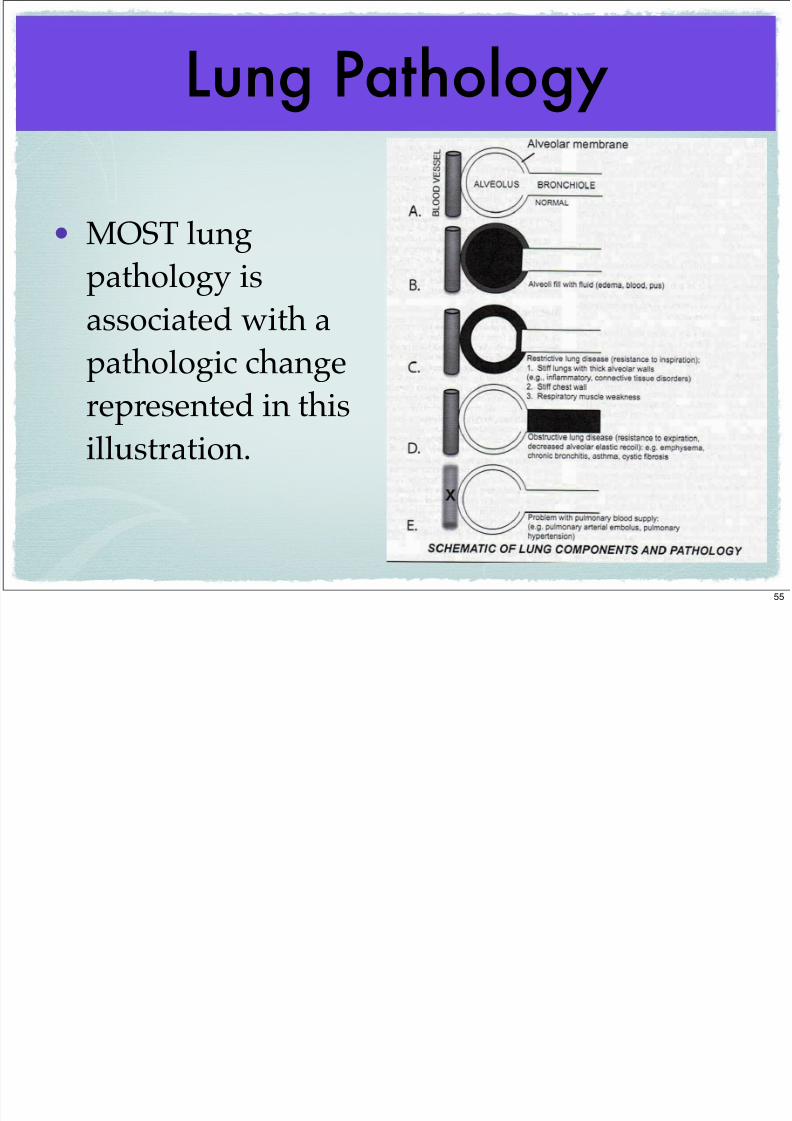
Lung Pathology
• MOST lung
pathology is
associated with a
pathologic change
represented in this
illustration.
55
Acute Pulmonary Disease
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 62/108
y
• Bronchitis
• Bronchiolitis• Pneumonia
• Pulmonary Embolism (PE)
• Pulmonary Edema
5656
Bronchitis / Bronchiolotis

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 63/108
/Bronchiolotis (“happy wheezers”)
• Inflammatory obstruction of the small airways
• Most common in children
• Occurs in adults with chronic bronchitis, in association with a viralinfection, or with inhalation of toxic gases
• Acute Bronchitis
• acute bronchial inflammation; usually viral and SELF LIMITED
• cough, chest discomfort, fever: often follows URI (cold)
• unlike pneumonia, no signs lung consolidation--would you expect pt.
to c/o dyspnea?
5757
Pneumonia (CAP)
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 64/108
( )
Pneumonia Facts
• 7th leading cause death• MOST common lethal infection US
• About 5 million cases annually
• 1 million hospitalizations annually
5858
Pneumonia Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 65/108
p y gy
Routes of Infection
• 1) Aspiration• 2) Inhalation
• 3) Hematogenous
• 4) Direct Inoculation
59
Pneumonia Pathophysiology

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 66/108
p y gy
Routes of Infection
• 1) Aspiration• 2) Inhalation
• 3) Hematogenous
• 4) Direct Inoculation
59
Pneumonia Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 67/108
Routes of Infection
• 1) Aspiration
• 2) Inhalation
• 3) Hematogenous
• 4) Direct Inoculation
59
Pneumonia Microbiology

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 68/108
gy
2) H. Influenza
3) Morexella
4) Staphylcoccus5) Klebsiella
6) Pseudomonas
7) Pneumocystis jiroveci
8) T.B.
60
Pneumonia Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 69/108
1) Pneumococcus Pneumonia (Strep. Pneumoniae)
• Encapsulated bacteria
• Many strains (>80)
• Virulence related to capsule strain
• Antibiotic resistance related to PBPon capsule (polysaccharide)
61
Pneumonia Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 70/108
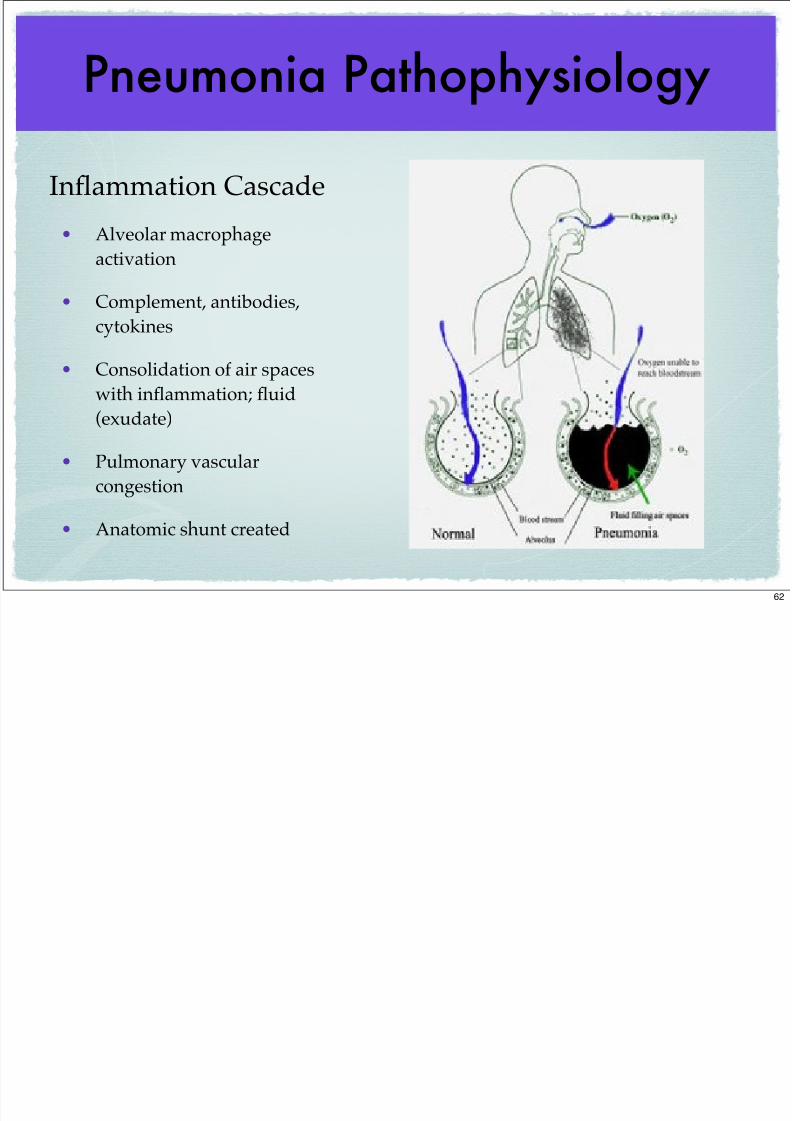
Inflammation Cascade
• Alveolar macrophage
activation
• Complement, antibodies,cytokines
• Consolidation of air spaces
with inflammation; fluid
(exudate)
• Pulmonary vascular
congestion
• Anatomic shunt created
62
Pneumonia Presentation
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 71/108
• Cough (rusty / bloody
sputum--think Pneumococcus)
• Fever / Chills
• Dyspnea
• Chest Pain
63
Pneumonia PE Findings
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 72/108
Signs of consolidation:
• Rales (crackles)
• Egophony
• Bronchial breath sounds
• Fremitus• Dullness to percussion
64
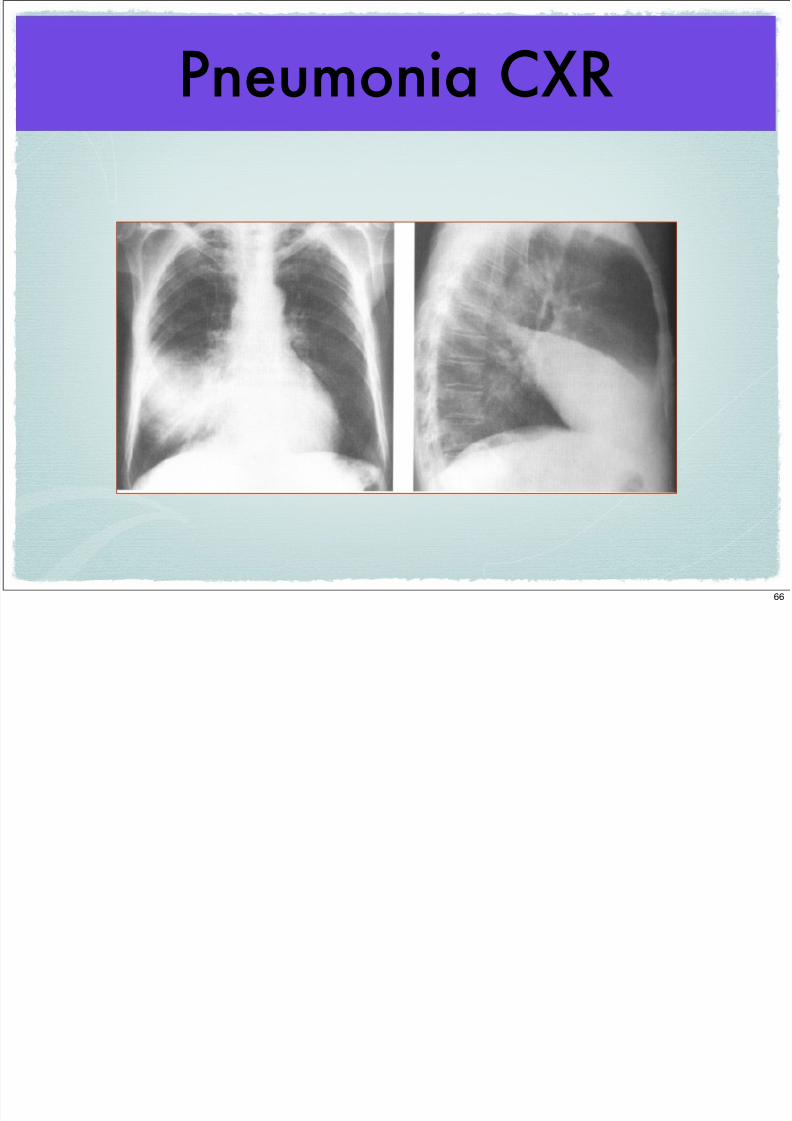
Pneumonia CXR

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 73/108
65
Pneumonia CXR
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 74/108
66
Pulmonary Embolism (PE)
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 75/108
• Acute blood clot in pulmonary vessel(s)
• Most common cause: DVT (deep vein thrombosis) from thigh
• Embolism may be: Blood, air, fat or tissue
Pathophysiology:
• occlusion of pulmonary circulation
• hypoxic vasoconstriction / inflammation
• atelectasis
• V/Q mismatch
• arterial hypoxemia
• clinical manifestations--death
6767
Acute PE

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 76/108
• Acute dyspnea
• Tachycardia
• Tachypnea
• Chest pain
• Low PaO2• Can be difficult Dx to make!
6868
Acute Pulmonary Edema

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 77/108
• Excess lung water (edema)
• Acute CHF (left heart failure) most common cause
• ARDS (Adult Resp. Distress Syndr.)
• capillary injury
• increased capillary permeability (leaky)• edema
6969
Pulmonary Edema Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 78/108
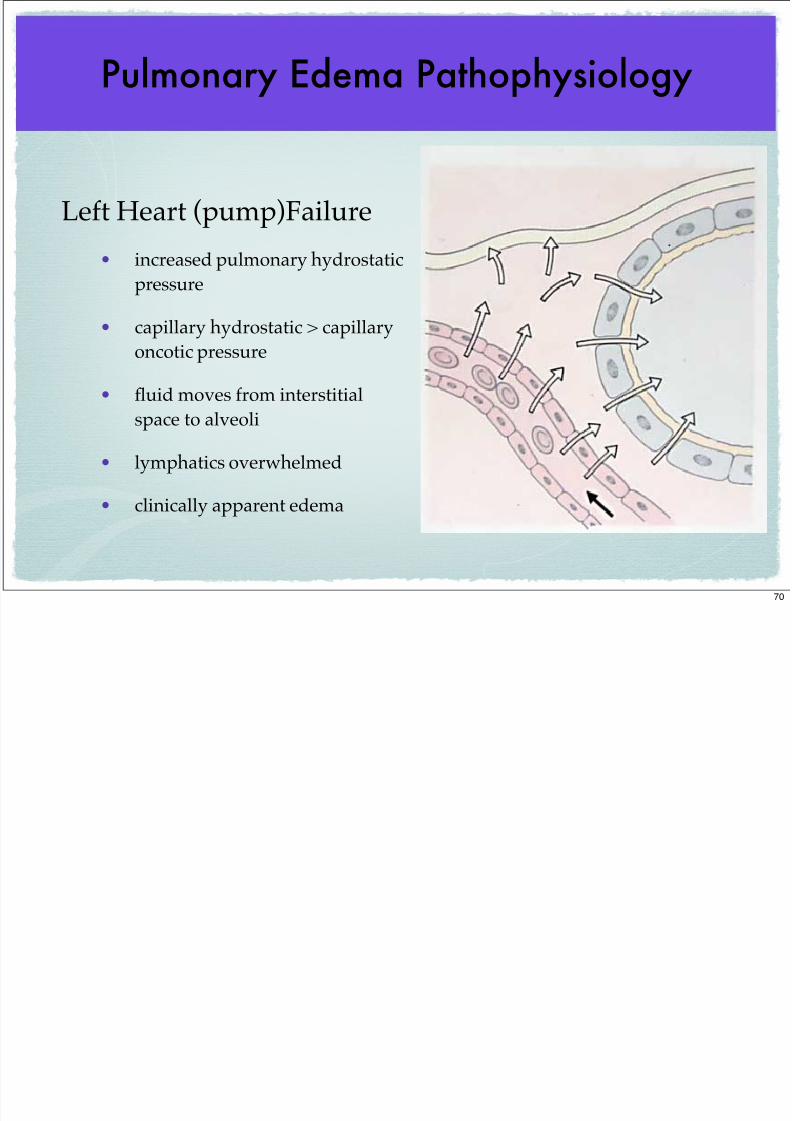
Left Heart (pump)Failure
• increased pulmonary hydrostatic
pressure
• capillary hydrostatic > capillary
oncotic pressure
• fluid moves from interstitial
space to alveoli
• lymphatics overwhelmed
• clinically apparent edema
70
Pulmonary Edema Presentation
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 79/108
• PND (Paroxysmal Nocturnal Dyspnea)
• Orthopnea
• Cough / wheezing (“cardiac asthma”)
• Exertional dyspnea
• Hypoxemia
71
SUMMARY ALGORITHMPulmonary Edema

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 80/108
72
Acute Pulmonary Edema

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 81/108
73
73
ARDS
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 82/108
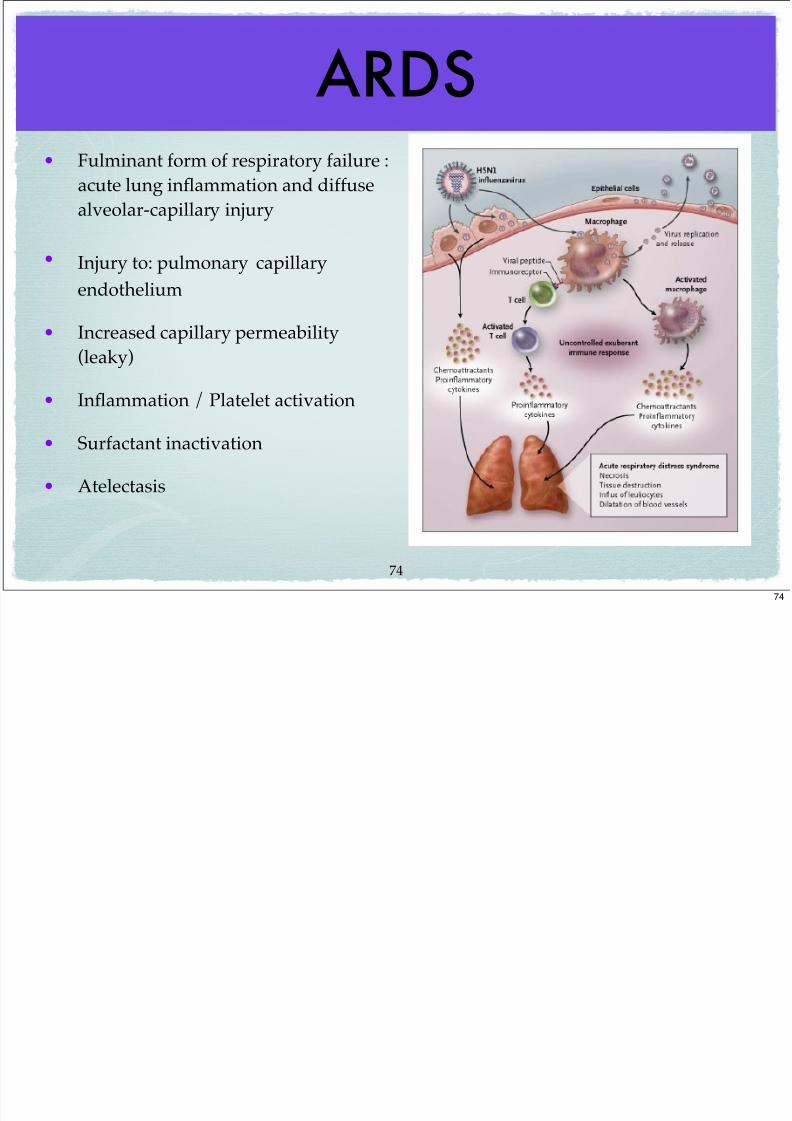
• Fulminant form of respiratory failure :acute lung inflammation and diffuse
alveolar-capillary injury
• Injury to: pulmonary capillary
endothelium
• Increased capillary permeability
(leaky)
• Inflammation / Platelet activation
• Surfactant inactivation
• Atelectasis
74
74
ARDS Presentation

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 83/108
• Tachypnea
• Severe dyspnea
• Hypoxemia (unresponsive to
enriched O2 delivery)
• Decreased lung compliance
• Hypoventilation
• Decreased cardiac output
Death
75
Pleural Disease
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 84/108
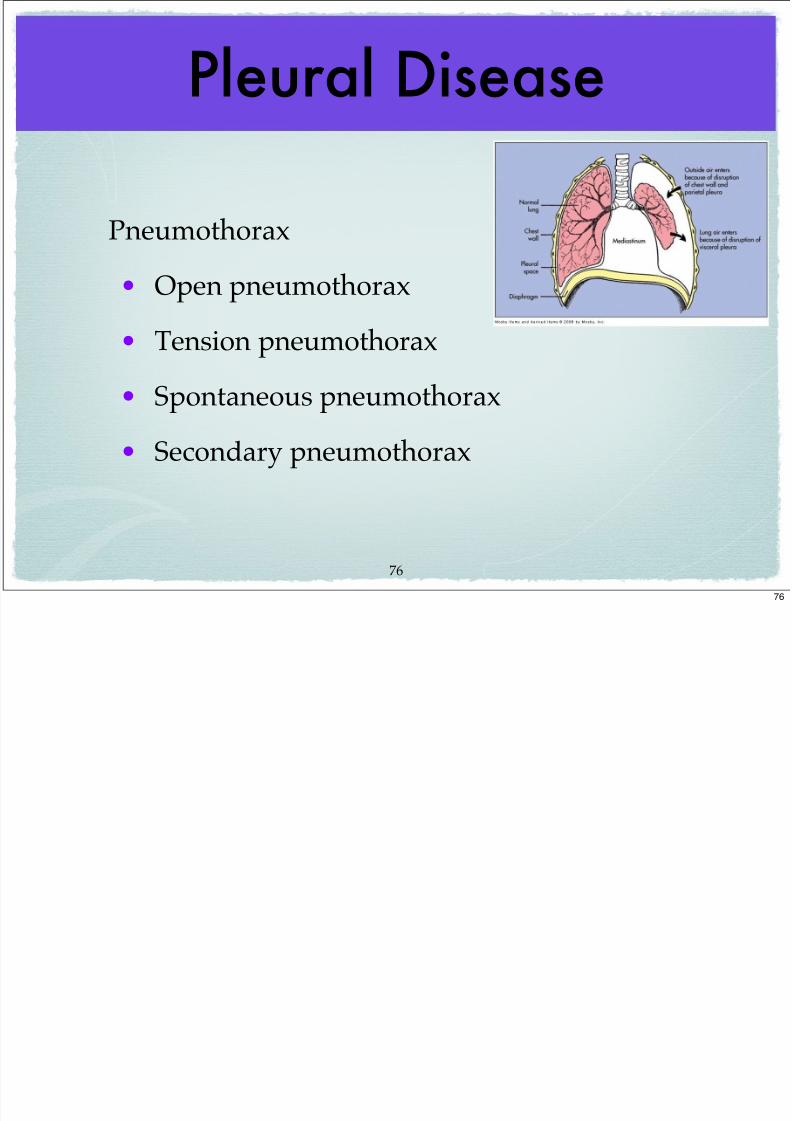
Pneumothorax
• Open pneumothorax
• Tension pneumothorax
• Spontaneous pneumothorax
• Secondary pneumothorax
76
76
Acute Pneumothorax

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 85/108
Spontaneous Pneumothorax
• pleural integrity (parietal or visceral is violated)
• normal sub-atmospheric intrapleural pressure is
lost
1) OPEN Pneumothorax
• pleural space openly communicates withexternal environment and barometric pressure
between pleura and environment are equal
77
77
Acute Pneumothorax

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 86/108
2) TENSION Pneumothorax
• one way-valve flap: airflow into pleural space
during inspiration BUT closed during expiration
• “tension” created by increasing pleural pressures
with each breath
• cardiovascular compromise / mediastinal shift due
to unilateral increase in tension
• life-threatening emergency requires immediate relief
78
78
Open Pneumothorax

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 87/108
79
79
Tension Pneumothorax

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 88/108
80
Pleural Disease

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 89/108
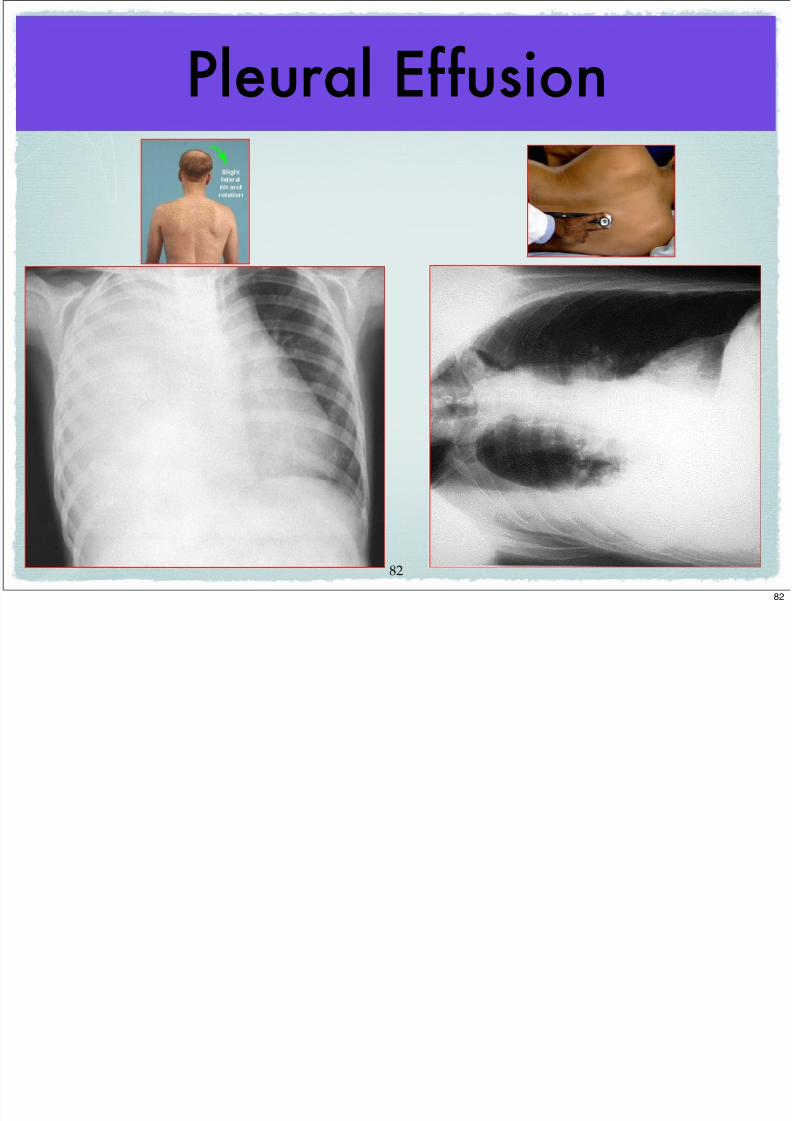
Pleural effusion
• fluid in pleural space
1) Transudative effusion (watery): CHF, orhypoproteinemia (liver/kidney disease)
2) Exudative effusion (less watery& higher
protein content): inflammatory diseases,infections, malignancies
81
81
Pleural Effusion
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 90/108
82
82
Pleural Disease

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 91/108
• Pleurisy: pain associated with respiratory
motion; secondary to acute inflammation
within pleura• Hemothorax (blood in pleural space): secondary to
ruptures intrathoracic aneurysm--usually fatal)
• Empyema (pus within pleural space): secondary toinfections--bacterial pneumonia, lung abscesses
83
83
Chronic Pulmonary Disease(COPD)
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 92/108
• Asthma
• Bronchiectasis (chronic dilated airways)
• Chronic Bronchitis
• Emphysema
• Pulmonary Fibrosis
84
84
Asthma
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 93/108
• Chronic inflammatory airway disorder
characterized by: hyper-bronchial
reactivity reversible bronchospasm• genetic predisposition strong
• clinically presents as dyspnea, wheezing and
cough
85
Asthma Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 94/108
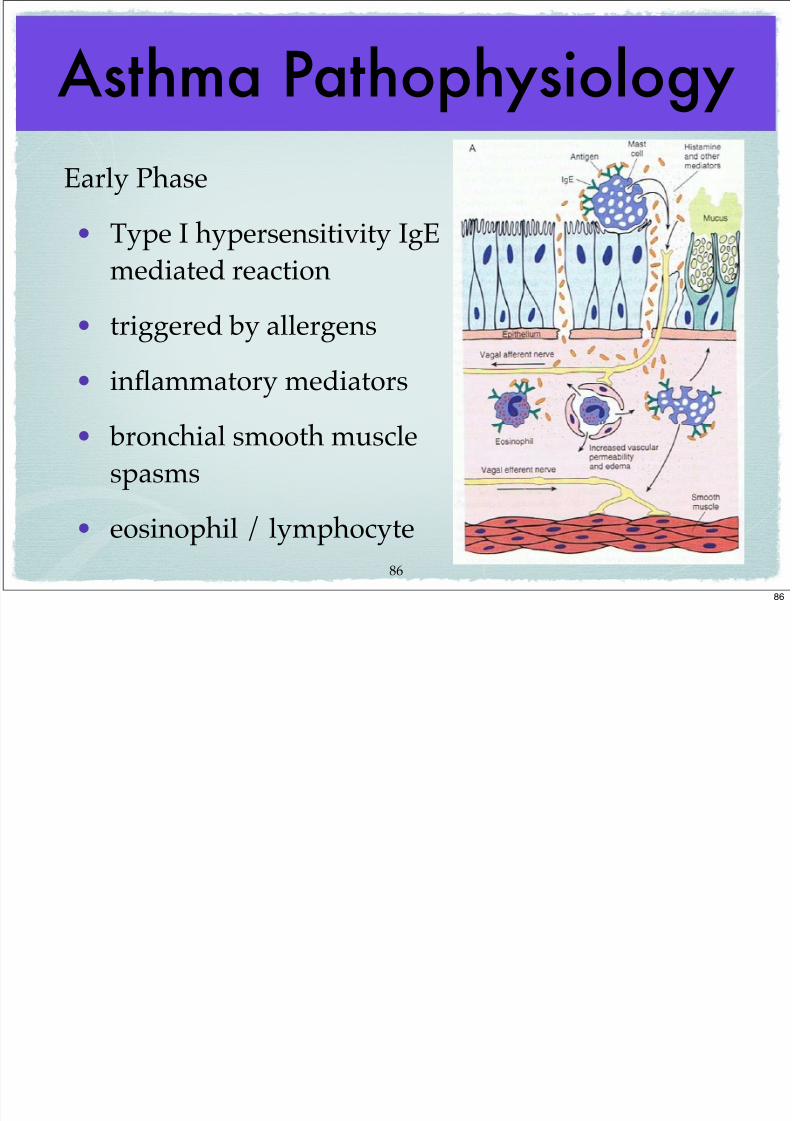
Early Phase
• Type I hypersensitivity IgE
mediated reaction
• triggered by allergens
• inflammatory mediators
• bronchial smooth musclespasms
• eosinophil / lymphocyte
86
86
Asthma Pathophysiology
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 95/108
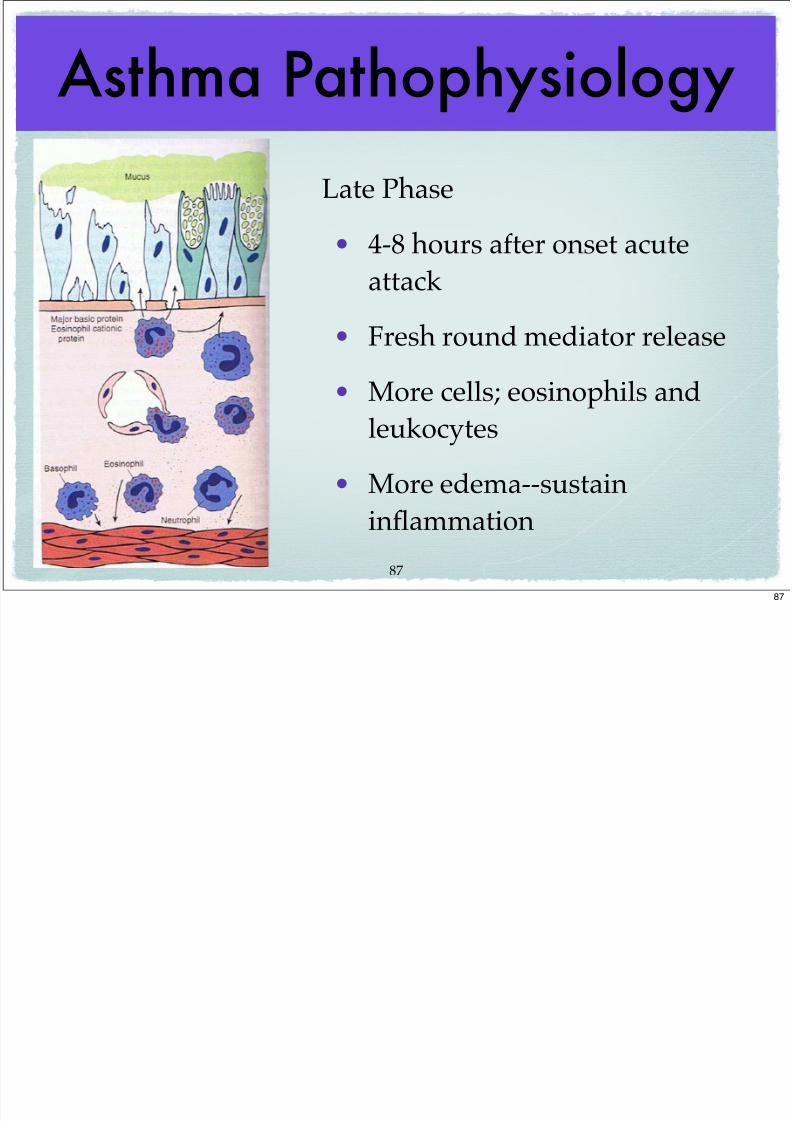
Late Phase
• 4-8 hours after onset acute
attack
• Fresh round mediator release
• More cells; eosinophils and
leukocytes
• More edema--sustain
inflammation
87
87
Asthma Presentation
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 96/108
• Acute dyspnea / cough
• Accessory muscle use
• Prolonged expiration (why?)• Thick mucus
• Decrease O2 saturation (pulse oximetry)
• What would you expect the arterial CO2 to
be during acute attack?88
88
Asthma Pathophysiology

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 97/108
• Airway obstruction (bronchospasm, edema) leads to
increasing airway resistance: if airway
diameter decreases by 1/2, resistanceincreases by factor of 16!
• Hyperinflation, air trapping, V/Q
mismatching hypoxemia
89
Chronic Bronchitis

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 98/108
• Hypersecretion of
mucus /chronic
productive cough for at
least 3 mos. /yr. and forat least 2 consecutive
years
• Inspired irritants,smoking major causes
• Smoking #1
90
Chronic Bronchitis
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 99/108
• Mucus hypersecretion leads to hypertrophy
mucus glands (goblet cell metaplasia in bronchial epithelium)
• Chronic obstruction
• Recurrent infections
• Hypoventilation--Hypoxemia--Death
91
Emphysema
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 100/108
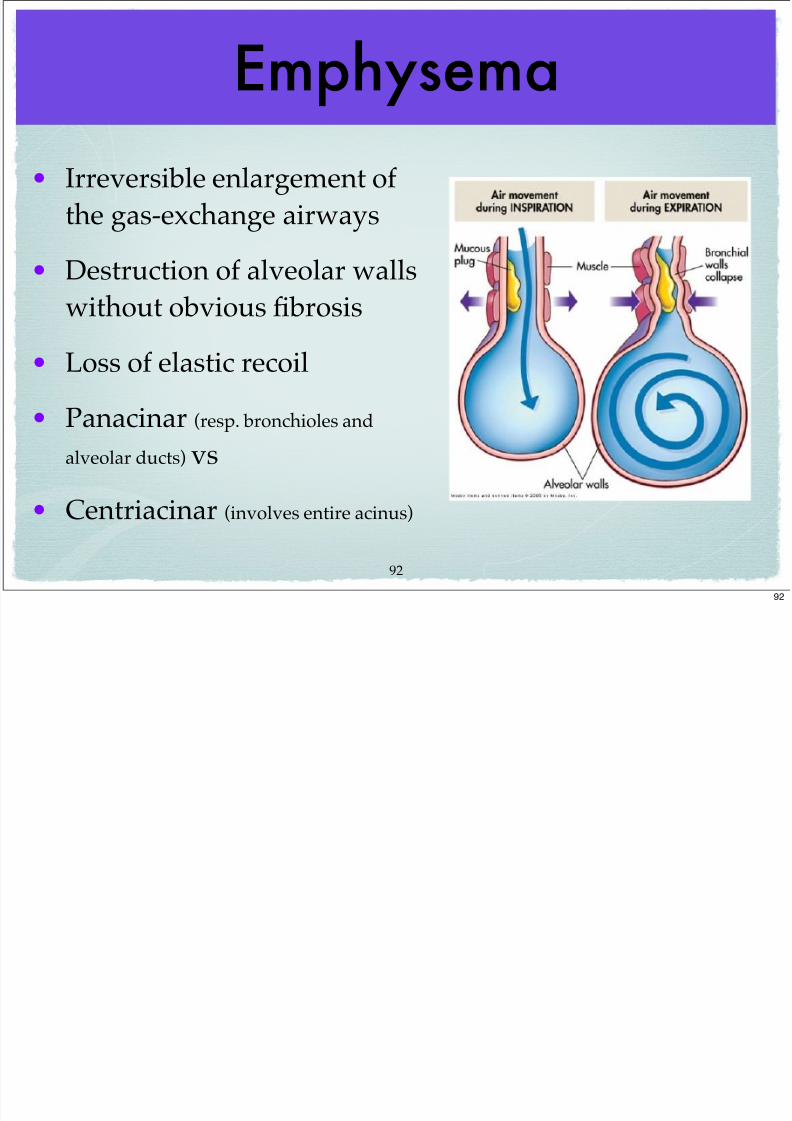
• Irreversible enlargement ofthe gas-exchange airways
• Destruction of alveolar walls
without obvious fibrosis
• Loss of elastic recoil
• Panacinar (resp. bronchioles and
alveolar ducts) vs
• Centriacinar (involves entire acinus)
92
92
Emphysema Cascade
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 101/108
• Chronic airway Inflammation (tobacco toxins)
• alpha-1 Antitrypsin inhibition (protects against
proteases) inhibited by smoking
• Destruction of elastin
• Loss of elastic recoil
• Hyperinflation (air trapping)
• Destruction alveoli / capillaries
• Hypoventilation
93
93
Emphysema

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 102/108
• Dyspnea with activity (early)
• Dyspnea at rest (late)
• Accessory muscledevelopment
• Barrel chest appearance
• Prolonged expiration (why?)
94
94
Pulmonary Hypertension(arterial)
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 103/108
• Mean pulmonary artery pressure 5-10 mm Hg above normal or above 20 mm
Hg (your text definition)
• pulmonary arterial vasoconstriction and remodeling of vessels
Causes:
• 1) COPD and interstitial disease
• 2) Pulmonary Embolism (recurrent)
• 3) Heart disease with L to R shunting
• 4) Idiopathic (uncommon)
• Exertional dyspnea, fatigue, JVD, and Right Ventric. Hypert. (on chest x-
ray)95
95
Cor Pulmonale
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 104/108
• Caused by chronic pulmonary
hypertension / pulmonary disease
• Think of it as Right-sided Heart Failure
• Chest pain, exertional dyspnea, JVD,
RVH
96
96
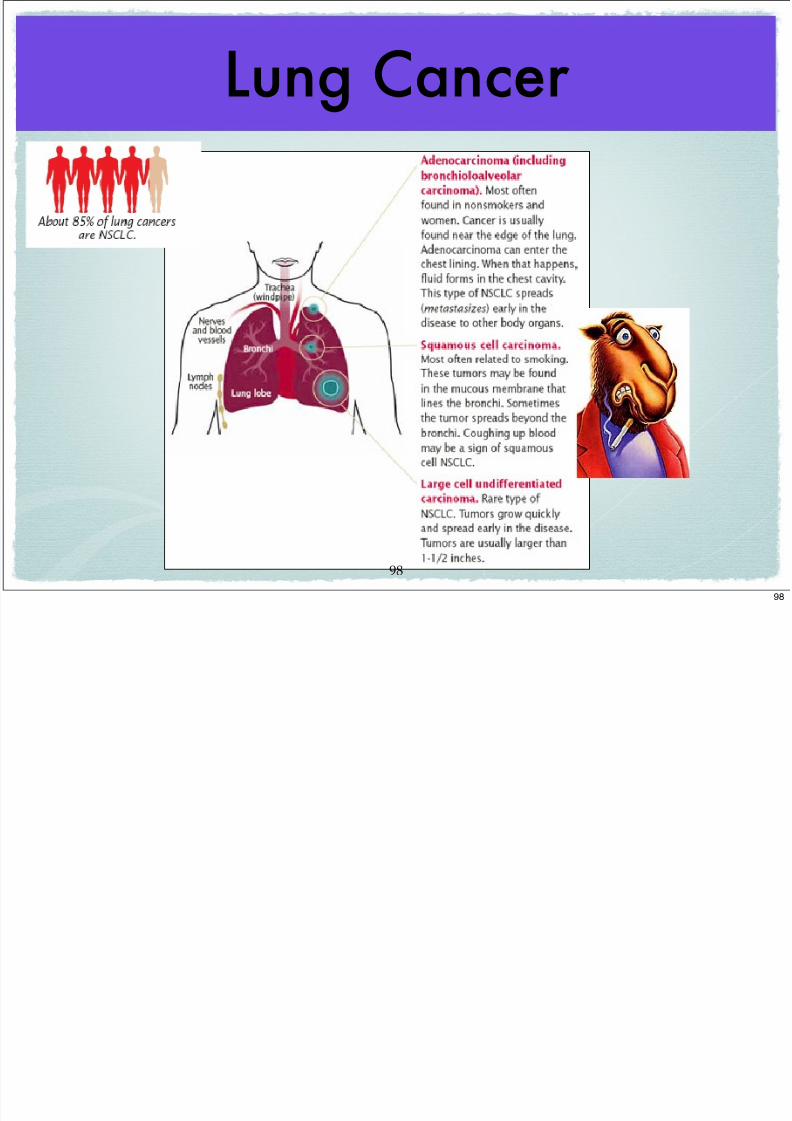
Lung Cancer

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 105/108
• Leading cause of cancer death men / women
• MOST common Cancer worldwide
• Bronchogenic is MOST common type
1) Non-Small cell carcinoma (NSCLC)
• Adenocarcinoma (located in parenchyma--now is #1--why?)
• Squamous (located in central bronchial epithelium #2)
• Large cell carcinoma
2) Small cell carcinoma (SCLA)
3) Other Lung cancers (sm. %)
97
97
Lung Cancer
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 106/108
98
98
Lung Cancer

7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 107/108
• Cough
• Weight loss
• Hemoptysis
• Wheezing
• Chest pain• Recurrent pneumonia
99
99
7/22/2019 PHYSIOLOGY / PATHOLOGY OF THE PULMONARY SYSTEM
http://slidepdf.com/reader/full/physiology-pathology-of-the-pulmonary-system 108/108
100
100


















