physiology
31
Biology 204: Introduction to Physiology Cardiac Physiology II
Transcript of physiology

Biology 204: Introduction to Physiology
Cardiac Physiology II

Cardiac cycle. Figure 9-17 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 316.

Ventricular filling profiles during normal and rapid heart rates. Figure 9-18 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 318.

Comparison of laminar and turbulent flow.Figure 9-19 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 319.

From Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 319.
Normal heart sounds
Normal sounds and sounds of late aortic stenosis, mitral stenosis, and aortic insufficiency from University of Washington Department of Medicine Advanced Physical Diagnosis: Learning and Teaching at the Bedside, Edition 1 http://depts.washington.edu/~physdx/heart/demo.html

From Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 321.

Heart rate
Parasympatheticactivity
Sympatheticactivity(and epinephrine)
Autonomic control of SA node activity and heart rate. Figure 9-20b from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 322.

Thresholdpotential
Thresholdpotential
= Inherent SA node pacemaker activity= SA node pacemaker activity on parasympathetic stimulation= SA node pacemaker activity on sympathetic stimulation
Autonomic control of SA node activity and heart rate. Figure 9-20a from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th
ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 322.

Stroke volume
Strength ofcardiac contraction
Extrinsiccontrol
Intrinsic control
End-diastolicvolume
Intrinsic control
Venous return
Sympathetic activity(and epinephrine)
Intrinsic and extrinsic control of stroke volume.Figure 9-21 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th
ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 322.

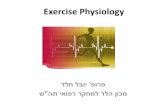
Intrinsic control of stroke volume (Frank–Starling curve). Figure 9-22 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 323.

Effect of sympathetic stimulation on stroke volume. (a) Normal stroke volume. (b) Stroke volume during sympathetic stimulation. (c) Stroke volume with combination of sympathetic stimulation and increased end-diastolic volume. Figure 9-23 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th
ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 324.

Shift of the Frank–Starling curve to the left by sympathetic stimulation.Figure 9-24 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 324.

Cardiac output
Heart rate Stroke volume
Parasympatheticactivity
Sympatheticactivity (andepinephrine)
End-diastolicvolume
Venous return
Extrinsiccontrol
Intrinsic control
Intrinsic control
Control of cardiac output.Figure 9-25 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th
ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 325.

Shift of the Frank–Starling curve downward and to the right in a failing heart.Figure 9-26a from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 326.

Coronary blood flow. Figure 9-27 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 327.

Vasodilation of coronary vessels
Adenosine
Blood flow to cardiac muscle cells
Oxygen available to meet oxygen need
Metabolic activity of cardiac muscle cells( oxygen need)
Stepped art
Matching of coronary blood flow to the O2need of cardiac muscle cells.Figure 9-28 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 327.

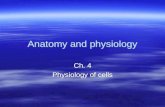
ARTERY WALL is built up of several layers, whose precise composition varies with the particular artery. A segment of a major elastic artery of the type of the human aorta is diagrammed. Benditt, Earl P. The origin of atherosclerosis. Scientific American 236(2): 74–85, February 1977. Offprint No. 1351.

ATHEROSCLEROTIC INNER SURFACE of an artery is seen at about two and a half times natural size in this photograph of a human aorta segment that has been slit open. The plaques are seen to be discrete lumps that bulge into the lumen of the dissected artery. Benditt, Earl P. The origin of atherosclerosis. Scientific American 236(2): 74–85, February 1977. Offprint No. 1351.

GENESIS OF A PLAQUE as proposed by the monoclonal hypothesis is traced in these highly schematic drawings. The process begins in the inner media. There are two cell types. A single cell (dark color) has undergone a mutation that gives it a selective advantage, and some stimulus causes the mutated cell to divide (1). Its daughter cell migrates into the intima (2). The progeny of the mutated cell, having a selective advantage and perhaps somehow freed of some curb on proliferation, continue to multiply, thickening the intima (3, 4) and eventually forming a lumpy plaque (5) all of whose cells are progeny of the original cell that mutated. The last drawing (6) shows, by way of contrast, a polyclonal plaque, which is the kind that would arise from the migration and proliferation of many cells of both cell types. Benditt, Earl P. The origin of atherosclerosis. Scientific American 236(2): 74–85, February 1977. Offprint No. 1351.

ADVANCED MONOCLONAL PLAQUE is often ulcerated at the surface where endothelial and smooth-muscle cells have died. The interior is filled with fatty debris, the result of cell death and degeneration as well as of migration of cholesterol and lipoproteins into the plaque. Benditt, Earl P. The origin of atherosclerosis. Scientific American 236(2): 74–85, February 1977. Offprint No. 1351.

Collagen-richsmooth musclecap of plaque
Normal bloodvessel wall
Lipid-rich coreof plaque
Endothelium
Plaque
Atherosclerotic plaque. Figure 9-29 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 328.

Blood flow
Thrombus
Blood flow
Embolus
Consequences of thromboembolism. (a) A thrombus may enlarge gradually until it completely occludes the vessel at that site. (b) A thrombus may break loose from its attachment, forming an embolus that may completely occlude a smaller vessel downstream. Figure 9-30a,b from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 330.

ATHEROSCLEROTIC PLAQUE narrows the lumen, or passageway, of a human coronary artery, enlarged 19 diameters in this photomicrograph made by the author. The plaque is a thickening of the artery wall composed mainly of connective tissue and smooth-muscle cells, with a region of cellular and fatty debris (lighter gray areas).
THROMBUS that formed just downstream of the narrowing caused by an atherosclerotic plaque blocked a coronary artery, shutting off the blood flow to part of the heart muscle and leading to a fatal heart attack. The darker regions of the throm-bus are composed of red blood cells and the lighter regions contain white blood cells and platelets.
Benditt, Earl P. The origin of atherosclerosis. Scientific American 236(2): 74–85, February 1977.

Consequences of thromboembolism. (c) Scanning electron micrograph of a vessel completely occluded by a thromboembolic lesion. Figure 9-30c from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 330.

Extent of myocardial damage as a function of the size of the occluded vessel. Figure 9-31 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 6th ed. Belmont CA: Thomson Brooks/Cole, 2007, p. 331.

NORMAL EKG PATTERN:
MYOCARDIAL INFARCTION:
VENTRICULAR FIBRILLATION:Adapted from Figure 9-20 from Sherwood, Lauralee. Human Physiology: From Cells to Systems. 5th ed. Belmont CA: Brooks/Cole—Thomson Learning, 2004, p. 319.

HO
Cholesterol

LOW-DENSITY LIPOPROTEIN (LDL), MAJOR CHOLESTEROL CARRIER in the blood-stream, is a spherical particle with a mass of three million daltons and a diameter of 22 nanometers (millionths of a millimeter). Its core consists of some 1,500 cholesteryl esters, each a cholesterol molecule attached by an ester linkage to a long fatty acid chain. The oily core is shielded from the aqueous plasma by a detergent coat composed of 800 molecules of phospholipid, 500 molecules of unesterified cholesterol and one large protein molecule, apoprotein B-100. When blood cholesterol is elevated, increasing the risk of atherosclerosis, the reason is almost always an increase in circulating LDL. From Brown, Michael S. & Joseph L. Goldstein. How LDL receptors influence cholesterol and atherosclerosis. Scientific American251(5): 58–66, November 1984. Offprint No. 1555.

RANGE OF LDL LEVELS in "normal" adults in Western industrial societies, indicated by the curve, is compared with the range in adult animals and human infants and with the levels seen in FH patients. Levels in the shaded region of the chart are above the threshold associated with accelerated atherosclerosis; more than half of the adults have LDL levels above the threshold. The LDL level is inversely associated with the number of LDL receptors (color). Brown, Michael S. & Joseph L. Goldstein. How LDL receptors influence cholesterol and atherosclerosis. Scientific American251(5): 58–66, November 1984. Offprint No. 1555.

LDL RECEPTOR, a glycoprotein embedded in the plasma membrane of most body cells, was purified from the adrenal gland by Wolfgang J. Schneider in the authors' laboratory. David W. Russell and Tokuo Yamamoto cloned complementary DNA derived from its messenger RNA. The DNA's nucleotide sequence was determined and from it the 839-amino-acid sequence of the receptor's protein backbone was deduced. Sites of attachment of sugar chains to nitrogen (N) and oxygen (0) atoms were identified, as was a stretch likely to traverse the membrane. The actual shape of the receptor is not yet known; the drawing is a highly schematic representation. Brown, Michael S. & Joseph L. Goldstein. How LDL receptors influence cholesterol and atherosclerosis. Scientific American251(5): 58–66, November 1984. Offprint No. 1555.

O
OO
HO O
Lovastatin
HO
O
OOH
HOCOO-
Prevastatin