Physiology 441 The Urinary System, Chp. 14 Text: Human Physiology (Sherwood), 6 th Ed. Julie Balch...
40
Physiology 441 The Urinary System, Chp. 14 Text: Human Physiology (Sherwood), 6 th Ed. Julie Balch Samora, MPA, MPH [email protected] 293-3412, Room 3145
-
Upload
anthony-houston -
Category
Documents
-
view
216 -
download
0
Transcript of Physiology 441 The Urinary System, Chp. 14 Text: Human Physiology (Sherwood), 6 th Ed. Julie Balch...

Physiology 441
The Urinary System, Chp. 14
Text: Human Physiology (Sherwood), 6th Ed.
Julie Balch Samora, MPA, MPH
293-3412, Room 3145
The Urinary System
• The Kidneys (form the urine)
• Renal Pelvis (into which urine is drained)
• Ureters (carry to urinary bladder)
• Bladder (stores urine)
• Urethra (tube which allows elimination of urine to external environment)


The Nephron
• The functional unit of the kidney
• Each nephron has two components– Vascular component– Tubular component
• Renal cortex- outer region (granular)
• Renal medulla- inner region, made up of triangles (renal pyramids)

Vascular Part of the Nephron
• The glomerulus- (a ball of capillaries) filters H2O and solute from blood
• Afferent arterioles (come from renal artery)- one supplies each nephron and delivers blood to glomerulus
• Efferent arterioles (come from glomerular capillaries)- unfiltered blood leaves glomerulus
• Peritubular capillaries- supply renal tissue with blood (exchanges w/ tubules)
Tubular Part of the Nephron• Bowman’s capsule- collects glomerular filtrate• Proximal tubule- uncontrolled reabsorption and
secretion of selected substances• Loop of Henle – establishes an osmotic gradient
in order to concentrate urine to appropriate amt• Distal tubule- controlled reabsorption and
secretion occur here• collecting duct (tubule)- variable, controlled
reabsorption of Na+ and H2O, and secretion of K+ and H+ (fluid leaving here is urine-enters renal pelvis)


Juxtaglomerular apparatus (JGA)
• The ascending limb of Henle passes through a fork formed by the afferent and efferent arterioles of the same nephron.
• The vascular and tubular cells at this juncture are both specialized to form the JGA.
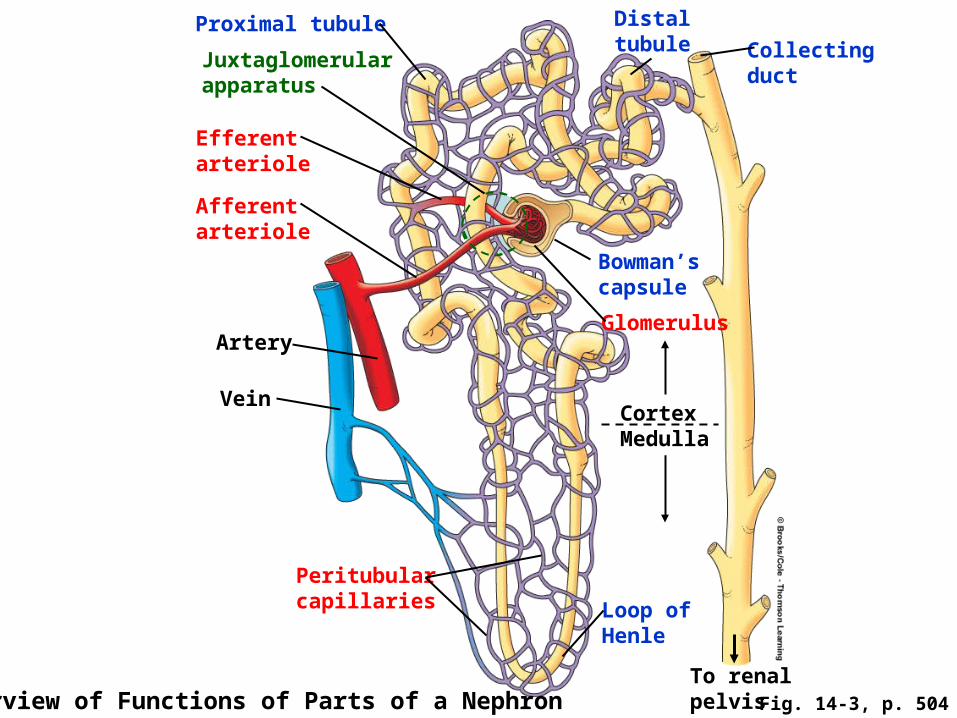
Proximal tubule Distaltubule Collecting
duct
Bowman’scapsule
Glomerulus
CortexMedulla
Loop of Henle
To renalpelvis Overview of Functions of Parts of a Nephron
Peritubularcapillaries
Vein
Artery
Afferentarteriole
Efferentarteriole
Juxtaglomerularapparatus
Fig. 14-3, p. 504

Location of Nephron Matters!
• All nephrons originate in the cortex, but where glomeruli lie and length of loops of henle designate type of nephron
• Cortical (80%) - glomeruli in outer cortex- hairpin loops barely reaches medulla
• Juxtamedullary (20%) - glomeruli in inner layer of cortex, next to medulla- hairpin loop goes through the entire depth of medulla- peritubular capillaries form vasa recta

Proximaltubule
Distaltubule
Distaltubule Glomerulus
Bowman’scapsule
Proximaltubule
Loop of Henle
Other nephrons emptying intothe same collecting duct
Collectingduct
Ascendinglimb ofloop ofHenle
To renalpelvis
Vasa recta
Descendinglimb ofloop ofHenle
Medulla
Cortex
Fig. 14-5, p. 505

The Kidneys Multiple Roles
• Play a major role in maintaining homeostasis• Maintain water balance• Regulate the quantity and concentration of ECF
ions• Regulate the plasma volume• Regulate pH by controlling elimination of acid
and base in urine • Maintain osmolarity• Regulate the concentration of plasma
constituents (e.g. electrolytes and water)

The Kidneys Multiple Roles
• Remove Toxic Metabolic Wastes
• Excreting foreign compounds
• Secreting erythropoietin
• Producing renin (imp. in salt handling)
• Converting Vitamin D into its active form

Basic Renal Processes
• Glomerular filtration• Tubular reabsorption• Tubular secretion
Urine results from these three processes.

Glomerular Filtration
• The first step in urine formation
• Blood flows through the glomerulus, allowing protein-free plasma to be filtered through the glomerular capillaries into Bowman’s capsule.
• ~20% of plasma entering the glomerulus is filtered
• 125 ml/min filtered fluid

Tubular Reabsorption
• Movement of substances from tubular lumen back into the blood
• Reabsorbed substances are therefore not lost in the urine, but are carried by the peritubular capillaries to the venous system
• Most of the filtered plasma is reabsorbed

Tubular Secretion
• The selective transfer of substances from the peritubular capillary into the tubular lumen.
• Allows for rapid elimination of substances from the plasma via extraction of the 80% of unfiltered plasma in peritubular capillaries and adding it to the substances already in tubule as result of filtration

Urine Excretion
• The elimination of substances from the body in the urine
• All plasma constituents filtered or secreted, but not reabsorbed remain in the tubules and pass into the renal pelvis to be excreted as urine and eliminated from the body

Renal Processes 1

Glomerular Filtration
• Fluid filtered from the glomerulus into Bowman’s capsule passes through 3 layers: – the glomerular capillary wall– the basement membrane
• Collagen• Glycoproteins- negative charge
– the inner layer of Bowman’s capsule• Podocytes• Filtration slits

Layers of Glomerulus Membrane

What Drives Filtration?
How does fluid move from the plasma across the glomerular membrane into Bowman’s capsule?
• No active transport mechanisms• No local energy expenditureSimple passive physical forces accomplish
filtration- Filtration occurs throughout the length of
the capillaries

Forces involved in Filtration
• Glomerular capillary blood pressure (favors filtration)
• Plasma-colloid osmotic pressure (opposes filtration)
• Bowman’s capsule hydrostatic pressure (opposes filtration)

Glomerular Capillary Blood Pressure
• Fluid pressure exerted by the blood within the glomerular capillaries
• Glomerular capillary pressure is significantly higher than other capillary blood pressures– This is due to the larger diameter of the afferent
arteriole compared with the efferent arteriole
• Blood pressure does not fall along the length of this capillary, which pushes fluid out of the glomerulus into Bowman’s capsule– (pressure build-up in glom. Cap. ~ 55mmHg)

Pressure opposing filtration
• Plasma-colloid oncotic pressure- caused by the unequal distribution of plasma proteins across the glomerular membrane– (~30mmHg)
• Bowman’s capsule hydrostatic pressure- the pressure exerted by the fluid in this initial part of the tubule- tends to push fluid out of Bowman’s capsule– (~15mmHg)


Net Filtration Pressure
• Force favoring filtration (glomerular capillary blood pressure of 55 mmHg) minus forces opposing filtration (plasma colloid osmotic pressure of 30 mmHg & Bowman’s capsule pressure of 15 mmHg) =
• 55 – (30 + 15) = 10 mmHg

Glomerular Filtration Rate• Depends on
– The net filtration pressure– How much glomerular surface area is available for
penetration– How permeable the glomerular membrane is
GFR = Kf x net filtration pressure
Where (Kf)= filtration coefficient (a product of the above two glomerular properties)
- Roughly 125 ml/min in males

GFR
• Changes in GFR primarily result from changes in the glomerular capillary blood pressure
• As glomerular capillary blood pressure ↑, the net filtration pressure ↑, as does GFR
• If afferent arteriolar resistance ↑, GFR ↓

Mechanisms to Regulate GFR
• Autoregulation (prevent spontaneous changes in GFR) – Involves myogenic and tubuloglomerular
feedback mechanisms
• Extrinsic sympathetic control (long-term regulation of arterial BP)– Mediated by the sympathetic nervous system– Can override autoregulatory mechanisms

Autoregulation Myogenic mechanism
• Response to changes in pressure within the nephron’s vascular component
• Arterioles contract inherently in response to the stretch accompanying ↑ pressure. Vessel automatically constricts, which helps limit blood flow into glomerulus despite increased systemic pressure
• Opposite reaction occurs when smooth muscles sense a drop in pressure

Autoregulation Tubuloglomerular feedback
• Juxtaglomerular apparatus– the combination of tubular and vascular cells where
the tubule passes through the angle formed by the afferent and efferent arterioles as they join the glomerulus
• Smooth muscle cells within the afferent arteriole form granular cells
• Specialized tubular cells in this region known as macula densa- sense changes in salt level of tubular fluid


Importance of Autoregulation of GFR
• The myogenic and tubuloglomerular feedback mechanisms work in tandem to autoregulate GFR within a MAP range of 80-180 mmHg
• Autoregulation greatly blunts the direct effect that changes in arterial pressure might otherwise have on GFR and preserves water and solute homeostasis and allows waste excretion to carry on as usual

Extrinsic Sympathetic Control
• GFR can be changed purposefully, even when MAP is within the autoregulatory range
• GFR is reduced by the baroreceptor reflex response to a fall in blood pressure (the SNS causes vasoconstriction in most arterioles as a compensatory mechanism to ↑ TPR)
• Afferent arterioles innervated with sympathetic vasoconstrictor fibers much more than are the efferent aa.
• ↓ GFR causes ↓ urine output, conserving some water and salt, helping to restore plasma volume to normal

Baroreceptor Reflex Influence on the GFR in Long-term Regulation ofArterial Blood Pressure

Filtration Fraction
• The Percentage of Renal Plasma Flow that is Filtered
• FF = GFR/RPF
• Roughly 20%