PHYSICIAN MEMO - Mercy Medical Center · • A letter will be created and routed to the ordering...
11
-
Upload
trinhduong -
Category
Documents
-
view
217 -
download
0
Transcript of PHYSICIAN MEMO - Mercy Medical Center · • A letter will be created and routed to the ordering...


701 10th Street SE Cedar Rapids, IA 52403-1292 (319) 398-6011
PHYSICIAN MEMO
DATE: January 16, 2017
FROM: Laboratory and Pharmacy
SUBJECT: Changes to Heparin Therapeutic Range/Heparin Nomogram and Coagulation Reference Ranges Mercy Medical Center has purchased new, state of the art coagulation analyzers. This new instrumentation has resulted in new reference intervals for coagulation testing and to the heparin therapeutic range and heparin nomograms. Effective February 1st, 2017 the following changes will be made: New Reference Interval Current Reference Interval aPTT Reference Range 22.5-35.1 sec 24.7-31.0 sec Heparin Therapeutic Range 68-102 sec 48-65 sec aPTT Critical result >150 sec >120 sec Prothrombin Time (PT) 12.0-14.5 sec 9.6-11.5 sec Fibrinogin 216-488 mg/dL 196-400 mg/dL D-dimer <0.54 mg/L FEUs 0.19-0.52 mg/ L FEUs The cut-off level to exclude DVT will remain the same (0.5) In the heparin nomograms, dosing will remain the same. However, the aPTT ranges will change:
Current: New: Cardiac with Bolus Dosing: Cardiac No Bolus Dosing: DVT/PE Treatment
<32 seconds
<35 seconds
50 unit/kg bolus and increase rate by
4 units/kg/hr
Increase rate by 4 units/kg/hr
80 unit/kg bolus and increase rate by
4 units/kg/hr
32-40 35-51 25 unit/kg bolus and
increase rate by 2 units/kg/hr
Increase rate by 2 units/kg/hr
40 unit/kg bolus and increase rate by
2 units/kg/hr
41-47 52-67 Increase rate by
1 unit/kg/hr Increase rate by
1 unit/kg/hr Increase rate by
1 unit/kg/hr
48-65 68-102 THERAPEUTIC RANGE-NO
CHANGE THERAPEUTIC RANGE-NO
CHANGE
THERAPEUTIC RANGE- NO CHANGE
66-83 103-118 Decrease rate by
1 unit/kg/hr Decrease rate by
1 unit/kg/hr Decrease rate by
1 unit/kg/hr
84-102 119-134 Hold heparin infusion for 1 hour and decrease rate by
2 units/kg/hr
Hold heparin infusion for 1 hour and decrease rate by
2 units/kg/hr
Hold heparin infusion for 1 hour and decrease rate by
2 units/kg/hr
103-120 135-150 Hold heparin infusion for 2 hours and decrease rate by
4 units/kg/hr
Hold heparin infusion for 2 hours and decrease rate by
4 units/kg/hr
Hold heparin infusion for 2 hours and decrease rate by
4 units/kg/hr
>120 >150 Hold heparin infusion and
notify physician Hold heparin infusion and
notify physician Hold heparin infusion and
notify physician
*Bolus and rate increases/decreases dependent on patient weight For questions regarding aPTT testing, contact Julie Netser, MD at 398-6003 or [email protected]. For questions regarding heparin dosing, please contact Lauren Cumings at 398-6811 or [email protected].

Cedar Rapids Medical Education Foundation
Counting Medical Education Courses
February 2017
Page 1 of 1 2/3/2017
DATE TOPIC PRESENTOR(S)
Mon 2/6 1200 – CRMEF – PBLA Depression/Anxiety: Diagnosis and Differential
Diagnosis of Depression
Dr. Pramod Siddagunta
Tues. 2/7 1200 – CRMEF – PBLA Depression/Anxiety: Suicidality Assessment
Dr. David Byrne
Wed. 2/8 1200 – CRMEF – PBLA Depression/Anxiety: Psychotherapy in
depression, Adolescent Depression, Geriatric Depression
Drs. Ramya Maturu,
Sara Snitker, & BJ Willis
Thurs. 2/9 1200 – CRMEF – PBLA Depression/Anxiety: Seasonal Affective Disorder
Dr. Alex Efimov
Fri. 2/10 1200 – CRMEF – PBLA Depression/Anxiety: Nonpharmacological
Therapies for Depression
Dr. Christine Hawks
Tues. 2/28 1200 – CRMEF – Visiting Professor Program
Topic: Assessment of the Neonate with Heart Murmur
Speaker: Marcelo Auslender, MD
University of Iowa
ACCREDITATION * The Cedar Rapids Medical Education Foundation is accredited by the Iowa Medical Society (IMS) to provide continuing medical education for physicians.
+ The Cedar Rapids Medical Education Foundation designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit ™. Physicians should only claim credit commensurate with their participation in the activity.
CONFLICT OF INTEREST As a sponsor accredited by the Iowa Medical Society, the Cedar Rapids Medical Education Program must assure balance, independence, objectivity and scientific rigor in all its individually sponsored or jointly sponsored educational activities. All faculty participating in a sponsored activity are expected to disclose to the activity audience any significant financial interest or other relationship (1) with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in an educational presentation and (2) with any commercial supporters of the activity (significant financial interest or other relationship can include such things as grants, or research support, employee, consultant, major stock holder, member of speakers bureau, etc.) The intent of this disclosure is not to prevent a speaker with a significant financial or other relationship from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remains for the audience to determine whether the speaker’s interests or relationship may influence the presentation with regard to exposition or conclusion. Disclosure forms for each presenter are on file in the CME office. Participants interested in viewing copies may write the CME Office, including a self-addressed, stamped envelope. Please write to: Continuing Medical Education Office, Cedar Rapids Medical Education Foundation, 1260 2nd Avenue, SE, Cedar Rapids, IA 52403. DURING PRESENTATIONS THERE ARE OCCASIONALLY DISCUSSIONS OF UNAPPROVED USE OF FDA APPROVED DRUGS, DEVICES OR
TREATMENTS. THIS MUST BE DISCLOSED TO THE AUDIENCE DURING THE LECTURE.

Breast Cancer Risk Assessment at Mercy Medical Center
Beginning on March 1, 2017, Mercy Women’s Center will be offering a free breast cancer risk assessment at the time of a woman’s mammogram. This risk assessment involves answering a few questions which will be asked by the technologist. The information gathered will automatically populate an estimated risk for breast cancer using the Gail Breast Cancer Risk Assessment Model.
The Gail Breast Cancer Risk Assessment Model will estimate the 5 year risk and lifetime risk percentages for appropriate women. This includes women age 35 and older and women without a breast cancer history (including DCIS and LCIS). The Breast Cancer Risk Assessment percentages will be noted on the woman’s mammogram report if elevated. The American Cancer Society Guidelines for breast cancer screening recommends annual breast MRI if lifetime risk is greater than 20%. As all breast cancer risk models have limitations, we recommend reviewing family history with your patient.
If the woman’s estimated risk for breast cancer within the next 5 years is greater than 1.7% and/or lifetime risk for developing breast cancer is greater than 20%, this will automatically trigger the following:
• A letter will be created and routed to the ordering provider regarding the identified increased breast cancer risk for his/her patient with recommendation to discuss increased breast cancer risk with the patient.
• A letter will be mailed to the patient as well as routed to her MyChart (if applicable) informing her of being identified as having a higher than average risk for breast cancer with recommendation to discuss with the ordering provider.
You may want to consider a referral to the Hall-Perrine Cancer Center’s High Risk Breast Cancer Clinic. This clinic will provide your patient a detailed cancer risk assessment, discussion of options for management of breast cancer risk, and order high risk breast cancer screening if desired by the patient.
If you have any questions or concerns, please contact Stephanie Miller, Nurse Practitioner for the High Risk Breast Cancer Clinic at (319) 398-6737.
Sincerely,
Dr. Vincent Reid, MD, FACS Medical Director: Hall-Perrine Cancer Center
Dr. Laura Hemann, MD Medical Director: Mercy Women’s Center

MERCY MEDICAL CENTER Cedar Rapids, Iowa
APPLIES TO: Hospital Wide
Page 1 of 3
SUBJECT TITLE: Pre-Operative Testing STANDARD/REF #: NA
APPROVED BY: Medical Staff EFFECTIVE DATE: 12/6/2016
REQUIRED REVIEWERS: Medical Executive REVIEWED DATE: 12/6/2016
Anesthesia Preoperative Testing Guidelines 12-Lead
EKG (Within 1 month)
BMP INR, PT, PTT
Hgb, Hct,
Platelet
Hgb A1C (Within
90 Days)
Flex/Ext C Spine
(Within 12 months)
Serum HCG
*Major blood loss potential (See list below)
X
Known anemia if disease unstable or not done in past 6 months
x
EKG within 30 days if
Known coronary heart disease, PAD (peripheral or carotid disease), cerebrovascular disease (includes TIA), other significant structural (valve disease)
High risk surgery See ACC guidelines
X
Diuretic use if disease process unstable or no value within past 6 months
X
Lung or intracranial tumor X X
Digoxin use if disease process is unstable or no value in past 6 months
X
Suspect or Known Bleeding disorder X X X
End Stage Renal disease or Dialysis X (day of
OR)
X (day of OR)
Coumadin X (day of OR)
Diabetes X
Females age 10-55 unless hysterectomy
X
Liver Disease, severe or advanced only, and no value in past 6 months
X X
Steroid Use if disease process unstable or no value in past 6 months
X
Rheumatoid Arthritis or Downs Syndrome
X
MERCY MEDICAL CENTER Cedar Rapids, Iowa
APPLIES TO: Hospital Wide
Page 2 of 3
SUBJECT TITLE: Pre-Operative Testing STANDARD/REF #: NA
APPROVED BY: Medical Staff EFFECTIVE DATE: 12/6/2016
REQUIRED REVIEWERS: Medical Executive REVIEWED DATE: 12/6/2016
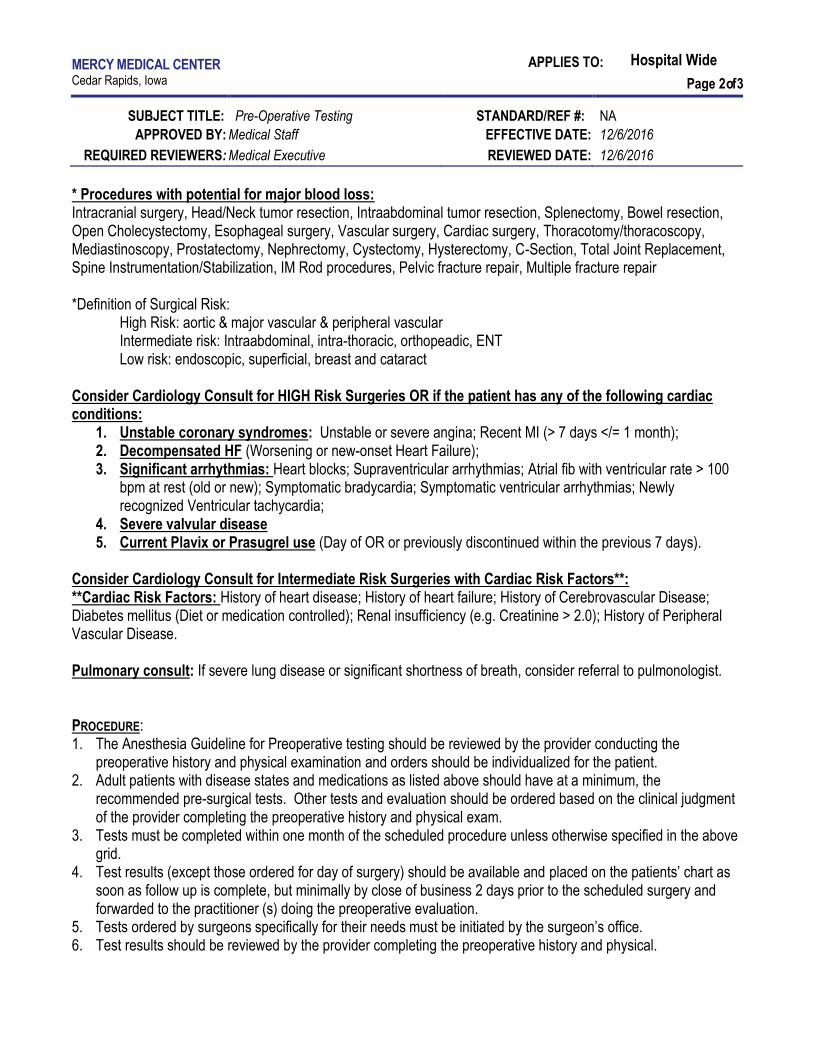
* Procedures with potential for major blood loss: Intracranial surgery, Head/Neck tumor resection, Intraabdominal tumor resection, Splenectomy, Bowel resection, Open Cholecystectomy, Esophageal surgery, Vascular surgery, Cardiac surgery, Thoracotomy/thoracoscopy, Mediastinoscopy, Prostatectomy, Nephrectomy, Cystectomy, Hysterectomy, C-Section, Total Joint Replacement, Spine Instrumentation/Stabilization, IM Rod procedures, Pelvic fracture repair, Multiple fracture repair *Definition of Surgical Risk: High Risk: aortic & major vascular & peripheral vascular Intermediate risk: Intraabdominal, intra-thoracic, orthopeadic, ENT Low risk: endoscopic, superficial, breast and cataract Consider Cardiology Consult for HIGH Risk Surgeries OR if the patient has any of the following cardiac conditions:
1. Unstable coronary syndromes: Unstable or severe angina; Recent MI (> 7 days </= 1 month); 2. Decompensated HF (Worsening or new-onset Heart Failure); 3. Significant arrhythmias: Heart blocks; Supraventricular arrhythmias; Atrial fib with ventricular rate > 100
bpm at rest (old or new); Symptomatic bradycardia; Symptomatic ventricular arrhythmias; Newly recognized Ventricular tachycardia;
4. Severe valvular disease 5. Current Plavix or Prasugrel use (Day of OR or previously discontinued within the previous 7 days).
Consider Cardiology Consult for Intermediate Risk Surgeries with Cardiac Risk Factors**: **Cardiac Risk Factors: History of heart disease; History of heart failure; History of Cerebrovascular Disease; Diabetes mellitus (Diet or medication controlled); Renal insufficiency (e.g. Creatinine > 2.0); History of Peripheral Vascular Disease. Pulmonary consult: If severe lung disease or significant shortness of breath, consider referral to pulmonologist.
PROCEDURE: 1. The Anesthesia Guideline for Preoperative testing should be reviewed by the provider conducting the
preoperative history and physical examination and orders should be individualized for the patient. 2. Adult patients with disease states and medications as listed above should have at a minimum, the
recommended pre-surgical tests. Other tests and evaluation should be ordered based on the clinical judgment of the provider completing the preoperative history and physical exam.
3. Tests must be completed within one month of the scheduled procedure unless otherwise specified in the above grid.
4. Test results (except those ordered for day of surgery) should be available and placed on the patients’ chart as soon as follow up is complete, but minimally by close of business 2 days prior to the scheduled surgery and forwarded to the practitioner (s) doing the preoperative evaluation.
5. Tests ordered by surgeons specifically for their needs must be initiated by the surgeon’s office. 6. Test results should be reviewed by the provider completing the preoperative history and physical.

MERCY MEDICAL CENTER Cedar Rapids, Iowa
APPLIES TO: Hospital Wide
Page 3 of 3
SUBJECT TITLE: Pre-Operative Testing STANDARD/REF #: NA
APPROVED BY: Medical Staff EFFECTIVE DATE: 12/6/2016
REQUIRED REVIEWERS: Medical Executive REVIEWED DATE: 12/6/2016
7. Test results from out of town or private labs must compare with those at Mercy regarding quality, type of test, and availability.
8. EKG tracings not done at Mercy must be of good quality and readable after transmission. 9. Chest x-rays from other facilities when read by a qualified radiologist are accepted. 10. Long term glycemic control and perioperative hyperglycemia are recognized risk factors for infectious
complications in diabetic surgical patients. To mitigate this risk a. A hemoglobin A-1c test within 90 days prior to elective procedures is recommended for all diabetics.
Consider delaying elective surgical procedure for patients with results greater than or equal to 8 until blood sugars are under adequate control.
b. Diabetic patients will have a finger stick glucose done at the time of arrival on the day of surgery. 11. Routine HCG testing is advised for all female patients undergoing anesthesia. All female patients age 10-55
(unless hysterectomy) will have HCG testing completed day of surgery unless a waiver is signed declining the test.
12. For cataract procedures, no testing is required unless the patient is scheduled for general anesthesia.
RELATED DOCUMENTS: REFERENCES: ACC/AHA 2014 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery

PRE-SURGICAL DIET
Mercy Medical Center
1/20/17 Effective immediately
Children (from age 6 months) and Adults:
No solid food or milk products, shakes or formulas (such as protein drinks or other liquids that
are not clear) after midnight the night before surgery.
Clear liquids only are permitted from midnight until 3 hours prior to scheduled surgery time.
Examples of clear liquids include, water, fruit juices without pulp, carbonated beverages, clear
tea, and black coffee with no cream. These liquids should not include alcohol.
No smoking the day of your surgery.
Infants (newborn to 6 months of age):
Infant formula or non-human milk permitted until 6 hours prior to surgery.
Breast milk permitted until 4 hours prior to surgery.
Clear liquids (water, Pedialyte, clear fruit juice without pulp) permitted until 3 hours prior to
surgery.
PLEASE NOTE THAT FAILURE TO FOLLOW THESE INSTRUCTIONS CAN CAUSE THE SURGERY TO BE
CANCELLED OR POST-PONED.

Colleagues, Friends & FamilyJoin us to celebrate the retirement of
Robert Silber, MD
Help us thank him for his service to our community and wish him
well as he begins a new journey as Associate Professor at the University
of Iowa Division of Gastroenterology.
Thursday, February 16, 2017
3 to 5 p.m.Lundy Pavilion at
Mercy Medical CenterGround Level

In this issueSleep Health: Health Cost & Sleep
Sleep Stages & Your Health
EISC & Sleep Seminars
Shift Work & Sleep
What’s Micro Sleep?
EISC Core Values To our patients, their families, and partners, we are committed to uphold the following values:
• Service that is unparalleled
• Listening and creating individualized treatment
• Excellence in quality, professional care
• Efficient and welcoming, with easy access
• Patient-centered, innovative & compassionate care
eiSleep.com
Produced by Eastern Iowa Sleep Center A Partnership: UnityPoint-St.Luke’s • Mercy Medical Center • Physicians’ Clinic of Iowa
Eastern Iowa Sleep Center600 7th St. SE, 2nd floorCedar Rapids, IA 52401Phone: 319-362-4433 / 877-361-4433 Fax: 319-362-4466 Office hours: 8am-4:30pm
1010 8th Ave.Belle Plaine, IA 52208Operation hours: 5:30pm-7:00am
Sleep Health Health Cost & SleepHealth care costs are everyone’s concern. Undiagnosed moderate to severe apnea in middle-aged adults may cause $3.4 billion in additional cost in the U.S. alone. Since the passage of the Affordable Care Act, health care payers, employers, providers and consumers have shown an increased commitment to health and health care quality. Sleep is recognized by the Centers for Disease Control and Prevention (CDC) as one of the pillars of healthy lifestyle, directly impacting every aspect of health and well-being.
Approximately 76% of congestive heart failures,
65% of strokes, 48% of type 2 diabetes sufferers and a wide
range of high blood pressure patients have Sleep-Disordered
Breathing such as Obstructive Sleep Apnea (OSA). OSA occurs when the muscles in the throat relax and the air way collapses during sleep. Air cannot get to the lungs and oxygen levels decrease. Take the Quick Test at eiSleep.com to see if you or someone you know are at risk. Visit your provider or visit a Sleep Medicine Physician
below to see if a sleep study is right for you.
Eastern Iowa Sleep Center – Take the Quick Test!Visit eiSleep.com and Take the Quick Test to get your sleepiness scale. Symptoms of sleep problems include excessive daytime sleepiness, snoring, morning headaches, waking up choking, restless sleep and if someone
has witnessed that you stop breathing for periods of time during your sleep. If you or someone you know experience any of these, visit your provider to see if Eastern Iowa Sleep Center (EISC) can help!
A. Peterson, M.D. S. Geisler, M.D. R. Struthers, M.D.Fellow, A.A.S.M. Diplomate, A.B.P.N.-S.M. Diplomate, A.B.P.N.-S.M.PCI Neurology/Sleep PCI Neurology/Sleep PCI Neurology/Sleep

When we sleep well, we wake up feeling refreshed and alert for our daily activi-ties. Sleep affects how we look, feel and perform on a daily basis, and can have a major impact on our overall quality of life.
To get the most out of our sleep, both quantity and quality are important. If sleep is cut short, the body doesn’t have time to complete all of the phases needed for muscle repair, memory consolidation and release of hormones regulating growth and appetite. Then we wake up less prepared to concentrate, make decisions, or engage fully in activities.
How does sleep contribute to all of these things?
Sleep architecture follows a pattern of alternating REM (rapid eye movement) and NREM (non-rapid eye movement) sleep throughout a typical night in a cycle that repeats itself about every 90 minutes.
What role does each state and stage of sleep play?
NREM (75% of night): As we begin to fall asleep, we enter NREM sleep, which is composed of stages 1-4:
Stage 1• Between being awake and falling
asleep, light sleep.
Stage 2• Onset of sleep, becoming disengaged
from surroundings, breathing and heart rate are regular, body temperature drops (so sleeping in a cool room is helpful).
Stages 3 and 4• Deepest and most restorative sleep,
blood pressure drops, breathing becomes slower, muscles are relaxed,
blood supply to muscles increases, tissue growth and repair occurs, energy is restored.
• Hormones are released, such as: growth hormone, essential for growth and development, including muscle development.
REM (25% of night): First occurs about 90 minutes after falling asleep and recurs about every 90 minutes, getting longer later in the night.
• Consolidates memory and learning, supports daytime performance, brain is active and dreams occur, eyes dart back and forth, body becomes immobile and relaxed as muscles are turned off.
Sleep helps us thrive by contributing to a healthy immune system, and can also balance our appetites by helping to regulate levels of the hormones ghrelin and leptin, which play a role in our feelings
of hunger and fullness. So when we’re sleep deprived, we may feel the need to eat more, which can lead to weight gain.
The one-third of our lives that we spend sleeping, far from being “unproductive,” plays a direct role in how full, energetic and successful the other two-thirds of our lives can be.
SleepSmartz
Sleep Stages & Your Health EISC & Sleep SeminarsEISC is available to present Sleep education. EISC offers seminars that fit all needs. Seminars can be given in any time frame (15 minutes to 45 minutes for example) and during var-ious shifts. EISC offers this education for free. Presentations can include: staff wellness in regards to Sleep; shift work concerns and understanding how poor Sleep increases health problems, the topics are endless. Questions? Call 319-362-4433. l
Shift Work & SleepSafety, Shift Work combined with Sleep issues are a concern for many. Operators of heavy equipment, drivers, fire fighters, police officers, healthcare providers and staff or other safety sensitive professions should pay careful attention to signs of sleepiness. Sleep problems and fatigue affect many of the nearly 15 million shift workers. The risk in-volved for workers and others around them if dozing off even for a brief moment (called a microsleep) could be detrimental in many ways. l
What’s Microsleep?Microsleep is when extreme drowsiness causes an episode of light sleep lasting 5 to 30 seconds. Several regions of the brain go to sleep involuntarily while areas controlling vision remain active. Fixed gaze or the eyelids start to droop, complete failure to respond and head nodding are signs that there is a loss of contact with reality – microsleep. l
eiSleep.com