Physical activity to maintain independence in older adults Marco Pahor, MD University of Florida...
44
Physical activity to maintain independence in older adults Marco Pahor, MD University of Florida Institute on Aging www.aging.ufl.edu
-
Upload
dana-waters -
Category
Documents
-
view
214 -
download
0
Transcript of Physical activity to maintain independence in older adults Marco Pahor, MD University of Florida...

Physical activity to maintain independence in older adults
Marco Pahor, MDUniversity of Florida Institute on Aging
www.aging.ufl.edu
• One of major goals of geriatric medicine: the prevention and management of disability in older persons
• Major limitation of geriatric medicine: no definitive Phase 3 RCT has proven that an intervention can prevent or delay the onset of major physical disability, such as mobility disability, in initially non-disabled older persons
Background

Adjusted % change in disability score
Ettinger et al. JAMA 1997
-10%
-5%
0%
5%
10%
15%Control
Resistance exercise
Aerobic exercise
Follow up (months)
0 1893
Exercise and Disability (FAST)Exercise and Disability (FAST)
P<.001 vs. control

FAST Physical exercise and ADL disability
010203040506070
0 3 6 9 12 15 18
Months
Pro
babi
lity
%
Control
Resistance
Aerobic
Penninx et al. Arch Intern Med 2001
P<.001 vs. control

Physical Disability
Time (months)
0 6 12 18
Sum
mar
y D
isab
ility
Sco
re
1.70
1.75
1.80
1.85
1.90
1.95
2.00
2.05
Healthy Lifestyle Control
Diet
Exercise
Diet + Exercise
*
ADAPT
Messier et al. Arthritis and Rheumatism 2004;50:1501
Extensive evidence from RCTs of limited size and duration and observational studies on the benefits of physical activity on several physiological measures:
• Walking speed, balance• Muscle strength• Body composition• Biomarkers
Efficacy of physical activity interventions

A Phase 3 RCT is needed
• Limited data on clinically relevant disability/mobility outcomes
• The observational evidence is not sufficient (reverse causality)
• Need for good risk / benefit data in older persons at high risk of disability

Refine key trial design benchmarks:• Primary outcome of major mobility disability
(inability to walk 400 m) • Sample size calculations• Recruitment, retention• Interventions: feasibility, safety & adherence• Internal validity: effects on the SPPB score and the
400 m walk speed• Secondary outcomes: ADL, major falls, CVD,
cognition, HRQL, health care services, CEA • Organizational infrastructure
LIFE-P Major goals

• A low SPPB score independently predicts mobility disability and ADL disability
• There is no definitive evidence from RCTs that changes in SPPB scores can be modified
• Objective: to assess the effect of a comprehensive physical activity (PA) intervention on the SPPB score and other physical performance measures
Background and objective
J Gerontol Biol Sci Med Sci 2006;61:1157
Inclusion criteria • 70-89 years• Sedentary lifestyle• Able to walk 400 m• SPPB score <9 • Completed a behavioral run-in • Gives informed consent, lives in study areaExclusion criteria• Medical conditions that raise concerns
regarding safety or adherence to a physical activity program
LIFE-P
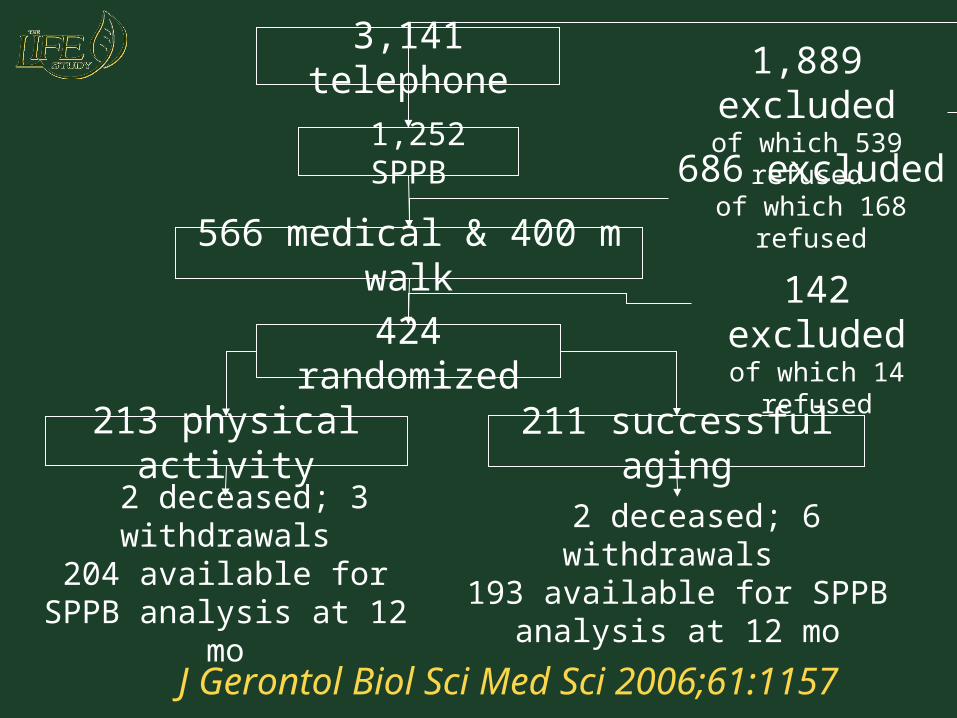
3,141 telephone1,889 excludedof which 539 refused
1,252 SPPB686 excluded
of which 168 refused566 medical & 400 m walk
424 randomized
213 physical activity 211 successful aging
142 excludedof which 14 refused
2 deceased; 3 withdrawals204 available for SPPB
analysis at 12 mo
2 deceased; 6 withdrawals 193 available for SPPB
analysis at 12 mo
J Gerontol Biol Sci Med Sci 2006;61:1157
Successful aging intervention
• Organized health workshops relevant to older adults (e.g., healthful nutrition, how to effectively negotiate the health care system, how to travel safely, etc.)
• Short instructor-led program (5-10 min) of upper extremity stretching exercises
• Group meeting once per week for weeks 1 - 24 and once per month for weeks 25 through the end of the study

Physical activity interventionCenter-based in a group setting with a systematic transition to home-based
exercise• Aerobic (walking)
• Strength (lower extremities)
• Balance
• Flexibility stretching• Behavioral counseling (group
and telephone)

8.58.7
7.57.98.0
6
7
8
9
10
0 6 12
Sco
re
Physical activitySuccessful aging
P<0.001
mo moMeans estimated from repeated measures ANCOVA adjusted for gender, field center and baseline values
LIFE-P SPPB score
J Gerontol Biol Sci Med Sci 2006;61:1157

• HRQL• 0.5 points= small meaningful change• 1.0 points= substantial meaningful change
• Disability outcomes over 4 years1 point = approximately 30% excess risk
of ADL or mobility disability
Theoretical clinical relevance of SPPB score
Perera et al. JAGS 2006;54:743
Guralnik et al. J Gerontol Med Sci 2000;55:M221

3556
4260
31
44
34
33
133102
128100
0%
20%
40%
60%
80%
100%
PA SA PA SA
Improve >=1pointNo change
Decline >=1point
SPPB changevs. baseline
6 monthP=0.004
12 monthP=0.03
Percent of participants who improved by >1 point, did not change, or declined by >1 point in the SPPB score from baseline to 6 and 12 mos.
NNT for improvement = 6 at 6 mos and 9 at 12 mos NNT for preventing decline = 10 at 6 and 12 mos
J Gerontol Biol Sci Med Sci 2006;61:1157
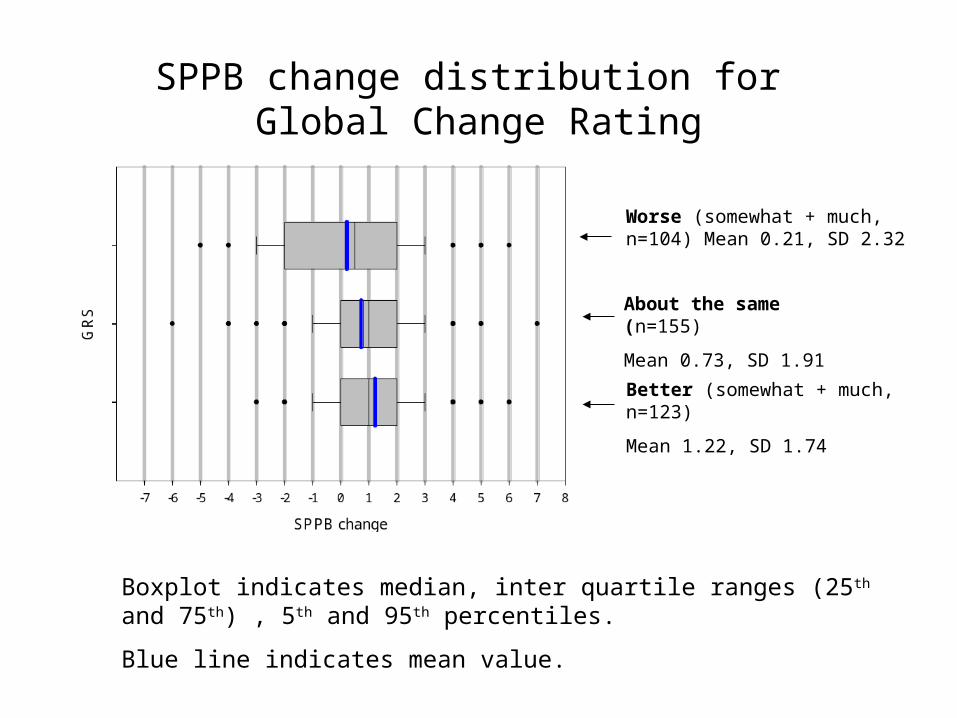
Worse (somewhat + much, n=104) Mean 0.21, SD 2.32
About the same (n=155)
Mean 0.73, SD 1.91
Better (somewhat + much, n=123)
Mean 1.22, SD 1.74
Boxplot indicates median, inter quartile ranges (25th and 75th) , 5th and 95th percentiles.
Blue line indicates mean value.
SPPB change distribution for Global Change Rating
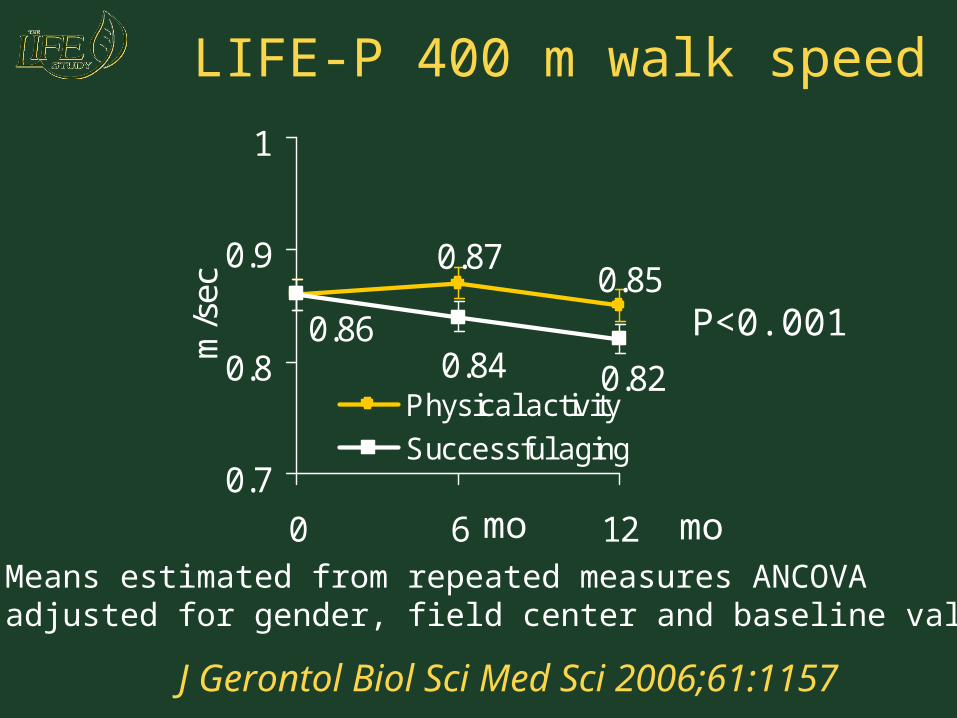
P<0.001
mo moMeans estimated from repeated measures ANCOVA adjusted for gender, field center and baseline values
LIFE-P 400 m walk speed
0.870.85
0.84 0.82
0.86
0.7
0.8
0.9
1
0 6 12
m/s
ec
Physical activity
Successful aging
J Gerontol Biol Sci Med Sci 2006;61:1157

Worse (somewhat + much, n=84) Mean -0.05, SD 0.11
About the same (n=146)
Mean -0.006, SD 0.11
Better (somewhat + much, n=115)
Mean 0.01, SD 0.14
Boxplot indicates median, inter quartile ranges (25th and 75th) , 5th and 95th percentiles.
Blue line indicates mean value.
Gait speed change* distribution for Global Change Rating
* Gait speed change among who completed 400m walk.

• Compared to SA, PA improved the SPPB score and 400 m walk speed
• Consistency among major subgroups
• Minimal loss to follow-up
• Excellent safety record
• An intervention that improves the SPPB performance may also offer benefit on more distal health outcomes, such as mobility disability
Conclusions

Cumulative hazard of time until major mobility disability
SA 211 PA 213
Number at risk
210213
191191
107125
2433
SA 0 PA 0
Cumulativeendpoints
1315
2823
3324
3426

LIFE main study Field Centers
CA
CO
LA FL
ILIN
NC
PACTMA
N = 2,000 - average FU = 4.5 yrs

• Will have important implications for public health prevention
• Will fill a critical gap in knowledge for practicing evidence-based geriatric medicine
• Will provide evidence regarding a broad spectrum of relevant health outcomes
• Will impact clinical practice and public health policy
• Will benefit individuals and society
LIFE Main study

Implementation of Physical Implementation of Physical Activity Interventions to Activity Interventions to
Improve Physical Function In Improve Physical Function In EldersElders
Part 2Part 2
The Durham VA GRECCThe Durham VA GRECC
Gerofit ProgramGerofit Program Facility-based exercise and health promotion Facility-based exercise and health promotion
program established in 1986 as a GRECC clinical program established in 1986 as a GRECC clinical demonstration project.demonstration project.
Developed in response to Veterans Health Care Developed in response to Veterans Health Care Amendment of 1983 mandating implementation Amendment of 1983 mandating implementation of preventive medicine in VA’s. Fitness of preventive medicine in VA’s. Fitness programming identified as a targeted area of programming identified as a targeted area of need.need.
Individually tailored to meet needs of older Individually tailored to meet needs of older veterans with chronic conditions and physical veterans with chronic conditions and physical impairments, many as a result of military service.impairments, many as a result of military service.

Veterans ages 65 and over have access to facility-based supervised exercise program (treadmills, stationary bicycles, stair machine, weight training machines, floor exercises, tai chi, water aerobics)
-Over 1200 patients referred -Average daily census + 60 patients
Referred by primary care providers and other health care specialists
Special consultative services available as needed
Telephone counseling offered to: -Patients who live too far to attend the facility-
based program - Patients under age 65

Key published clinical outcomesKey published clinical outcomes Veterans participating in Gerofit report significant Veterans participating in Gerofit report significant
improvements in exercise capacity, cardiovascular risk factors improvements in exercise capacity, cardiovascular risk factors and psychological well-being. JAGS (37):1989; J Appl Ger and psychological well-being. JAGS (37):1989; J Appl Ger (10):1991. (10):1991.
Examination of impact of burden of disease (no disease vs. 1 Examination of impact of burden of disease (no disease vs. 1
disease vs. 2 diseases) on exercise parameters and 5-year disease vs. 2 diseases) on exercise parameters and 5-year trajectories of performance. JAGS (44):1996.trajectories of performance. JAGS (44):1996.
Older veterans with chronic diseases experience a long-term Older veterans with chronic diseases experience a long-term beneficial mortality effect from participation in facility-based beneficial mortality effect from participation in facility-based program. JAGS (50):2002.program. JAGS (50):2002.
Older veterans enrolling in Gerofit have significantly poorer Older veterans enrolling in Gerofit have significantly poorer physical performance than national normative data. And, physical performance than national normative data. And, veterans participating in Gerofit for 6 months or more have veterans participating in Gerofit for 6 months or more have physical performance on par or higher than reported national physical performance on par or higher than reported national norms. JRRD (41):2004.norms. JRRD (41):2004.

Transition to Funded ResearchTransition to Funded Research
Aerobic vs. Axial/Aerobic Training: Improvement in Function Aerobic vs. Axial/Aerobic Training: Improvement in Function (PI: Morey, 1992-1995) (facility to home-based)(PI: Morey, 1992-1995) (facility to home-based)
Phoning for Function: Promoting Health After Cancer (PI: Phoning for Function: Promoting Health After Cancer (PI: Demark, 1997-2003) (home-based)Demark, 1997-2003) (home-based)
Improving Fitness and Function in Elders (LIFE 1) (PI: Morey, Improving Fitness and Function in Elders (LIFE 1) (PI: Morey, 2001-2004) (home-based)2001-2004) (home-based)
Learning to Improve Fitness and Function in Elders (LIFE 2) Learning to Improve Fitness and Function in Elders (LIFE 2) (PI: Morey, 2004-2008) (home-based)(PI: Morey, 2004-2008) (home-based)
RENEW: Reach Out to Enhance Wellness in Older Survivors RENEW: Reach Out to Enhance Wellness in Older Survivors (PI Demark 2004-2008) (home-based)(PI Demark 2004-2008) (home-based)

Aerobic vs. Axial/Aerobic Training: Aerobic vs. Axial/Aerobic Training: Improvement in FunctionImprovement in Function (facility to home-based) (facility to home-based)
Randomized clinical trial Randomized clinical trial •Three months of supervised exerciseThree months of supervised exercise• Followed by six months of home-based exerciseFollowed by six months of home-based exercise
with telephone follow-upwith telephone follow-up
Intervention (3 days per week)Intervention (3 days per week)• Axial/Aerobic group Axial/Aerobic group 20 minutes axial mobility exercises20 minutes axial mobility exercises 20 minutes aerobic exercise20 minutes aerobic exercise• Aerobic groupAerobic group 40 minutes aerobic exercise40 minutes aerobic exercise

Change in Aerobic CapacityChange in Aerobic Capacity
Findings:Findings:
Significant overall Significant overall improvement,improvement,
both groups, p=0.0001both groups, p=0.0001
0-3 mos.0-3 mos.
group*time interaction, group*time interaction, p=0.0014p=0.0014
(dose response) (dose response)
0-9 mos: p=0.070-9 mos: p=0.07
17
17.5
18
18.5
19
19.5
20
20.5
0 3 9
Axial/Aerobic
Aerobic
MonthsMonths
VVOO22 PPeeaakk ml/kg/minml/kg/min
Morey et al., J Geron Med Sci 1999 54A M335-M342.

Change in Physical FunctionChange in Physical Function
Findings:Findings:
Significant overall Significant overall improvement,improvement,
both groups, both groups, p=0.0016p=0.0016
0-3 mos. p=0.0040-3 mos. p=0.004
0-9 mos. p=0.680-9 mos. p=0.68
No between group No between group differencesdifferences
6567697173757779818385
0 3 9
Axial/Aerobic
Aerobic
MonthsMonths
PPhhyyss
FFuunnccttiioonn
ScoreScoreMorey et al., J Geron Med Sci 1999 54A M335-M342.

Secondary ImprovementsSecondary Improvements
• Health Related Quality of Life, p= Health Related Quality of Life, p= 0.00090.0009
• Total Number of Symptoms Reported, Total Number of Symptoms Reported, p=0.0001 p=0.0001
• Effect of Symptoms on Functional Effect of Symptoms on Functional Limitations, p=0.0001Limitations, p=0.0001
Morey et al., J Geron Med Sci 1999 54A M335-M342.

What did we learn and where do What did we learn and where do we go from here?we go from here?
Facility-based have more robust outcomes; Facility-based have more robust outcomes; but most people choose home-based but most people choose home-based exerciseexercise
How can we successfully apply these How can we successfully apply these approaches to home-based intervention?approaches to home-based intervention?
How can we assess/ enhance adherence?How can we assess/ enhance adherence?

Predictors of adherencePredictors of adherence
Number of Number of diseases diseases
Body mass index Body mass index Physical function Physical function PainPain **Weekend **Weekend
adherenceadherence0
10
20
30
40
50
60
70
80
90
1 3 5 7 9 11 13 15 17 19 21 23 25
Perc
ent A
dher
ent
AdherentsNon adherents
Weeks
Morey, et al. J Aging Phys Act 2003, 11,351-368

Functional Outcomes by Level of Functional Outcomes by Level of Adherence: SF-36 Physical FunctionAdherence: SF-36 Physical Function
50556065707580859095
100
0 3 9
AdherentNon-Adh
Findings:Findings:Change in physical Change in physical
function scores function scores between 3 and 9 between 3 and 9 months differed by months differed by level of adherence. level of adherence. (Chi sq. = 5.67, 1 df,(Chi sq. = 5.67, 1 df,
p= 0.017) p= 0.017)Adherents maintained Adherents maintained
gainsgains
Non adherents declined Non adherents declined to baseline functional to baseline functional score.score.
MonthMonthss
FFuunnccttiioonn

Project LIFE 1 And 2Project LIFE 1 And 2
Use state of the art counseling Use state of the art counseling methods to enhance adherencemethods to enhance adherence
Desire to include primary care Desire to include primary care providers as part of counseling teamproviders as part of counseling team
Needed to involve more functionally Needed to involve more functionally limited elderslimited elders

Project Life 1Project Life 1 Six-month feasibility trialSix-month feasibility trial
Primary care providers endorsed PA one-time in Primary care providers endorsed PA one-time in clinicclinic
Health counselor gave baseline PA counseling to Health counselor gave baseline PA counseling to everyone prior to randomizationeveryone prior to randomization
High intensity group had 3 months bi-weekly PA High intensity group had 3 months bi-weekly PA counseling and 3 months monthly PA counselingcounseling and 3 months monthly PA counseling

Project LIFE 1Project LIFE 1 One-time One-time
counseling had counseling had short-term benefit short-term benefit that was not that was not sustainedsustained
Patients valued Patients valued primary care primary care provider provider involvementinvolvement
More frequent More frequent telephone contact telephone contact was neededwas needed
0
5
10
15
20
25
Baselin
e
3 m
onth
6 m
onth
Physic
al A
ctivity F
requency
HighIntensity
AttentionControl
UsualCare
Morey, et al. J Aging Phys Act 2006 14 324-343
Project LIFE 2Project LIFE 2
12-month multi component PA trial 12-month multi component PA trial comparing counseling to usual carecomparing counseling to usual care• One-time in personOne-time in person• Provider endorsementProvider endorsement• Sustained telephone counselingSustained telephone counseling• Sustained provider endorsement by automated Sustained provider endorsement by automated
telephone messagingtelephone messaging• Mailed quarterly progress reportMailed quarterly progress report
Goal: 30 min 5 days/week aerobicGoal: 30 min 5 days/week aerobic
15 min strength training 3 days/wk15 min strength training 3 days/wk

Project LIFE 2Project LIFE 2 Counseling must be Counseling must be
sustainedsustained
It takes one year to get It takes one year to get close to recommended PA close to recommended PA guidelinesguidelines
Provider involvement is Provider involvement is highly acceptablehighly acceptable
These changes are These changes are accompanied by accompanied by improvements in physical improvements in physical functionfunction
Minutes of self reported exercise per week
0
50
100
150
0 3 6 12
Months
Rep
orte
d m
inut
es p
er
wee
k
Counsel
UC

From Physical Activity to From Physical Activity to Physical FunctionPhysical Function
Change in Physical Function by Change in Physical Activity Over Time (raw means + s.e.)
303540455055606570
Baseline 6 months
Ph
ysic
al F
un
ctio
n
Su
bsc
ale
SF
-36
Pooled data from several studies
>150 min/wk PA to < 150 min/wk
< 150 min/wk PA to > 150 min/wk
In an adjusted model, change in PA from < 150 min/wk to ≥ 150 min/wk or from ≥ 150 min/wk to < 150 min/wk resulted in a significant difference in PF (+ 6.4 points, p=0.006) controlling for age, race, gender, and baseline PA , baseline PF and trial.

Physical Activity to Physical Physical Activity to Physical FunctionFunction
Benefits are more easily achieved among Benefits are more easily achieved among adults of higher physical functionadults of higher physical function
Exercise modality is not crucial – any Exercise modality is not crucial – any exercise is better than being sedentaryexercise is better than being sedentary
Among more impaired adults and those Among more impaired adults and those with multiple morbidities results are more with multiple morbidities results are more tenuoustenuous

SummarySummary Change in physical function, physical Change in physical function, physical
performance is variableperformance is variable• Population under studyPopulation under study• Intensity of interventionIntensity of intervention• Specificity of trainingSpecificity of training
Measures sensitive to changeMeasures sensitive to change• Physical Function SubscalePhysical Function Subscale• Sickness Impact ProfileSickness Impact Profile• Gait SpeedGait Speed• Endurance walkEndurance walk
ConclusionsConclusions Physical activity interventions of diverse content Physical activity interventions of diverse content
can be implemented across multiple settingscan be implemented across multiple settings
Adherence to physical activity can be easily Adherence to physical activity can be easily identifiedidentified
Methods to address non-adherence need further Methods to address non-adherence need further studystudy
For questions relative to this presentation please For questions relative to this presentation please contact Miriam Morey at [email protected] Miriam Morey at [email protected]


















