mcaa.gov.mnAuthor Tricom LLC Created Date 2/21/2018 1:30:57 PM

Cancer Therapy: Clinical
Phase I Study of a Poxviral TRICOM-BasedVaccine Directed Against the TranscriptionFactor BrachyuryChristopher R. Heery1, Claudia Palena1, Sheri McMahon2, Renee N. Donahue1,Lauren M. Lepone1, Italia Grenga1, Ulrike Dirmeier3, Lisa Cordes2, Jenn Mart�e2,William Dahut2, Harpreet Singh2, Ravi A. Madan2, Romaine I. Fernando1,Duane H. Hamilton1, Jeffrey Schlom1, and James L. Gulley2
Abstract
Purpose: The transcription factor brachyury has beenshown in preclinical studies to be a driver of the epithe-lial-to-mesenchymal transition (EMT) and resistance totherapy of human tumor cells. This study describes thecharacterization of a Modified Vaccinia Ankara (MVA)vector–based vaccine expressing the transgenes for brachy-ury and three human costimulatory molecules (B7.1, ICAM-1, and LFA-3, designated TRICOM) and a phase I studywith this vaccine.
Experimental Design: Human dendritic cells (DC) wereinfected with MVA-brachyury-TRICOM to define their abilityto activate brachyury-specific T cells. A dose-escalation phase Istudy (NCT02179515) was conducted in advanced cancerpatients (n ¼ 38) to define safety and to identify brachyury-specific T-cell responses.
Results: MVA-brachyury-TRICOM-infected human DCs acti-vated CD8þ and CD4þ T cells specific against the self-antigenbrachyury in vitro. No dose-limiting toxicities were observeddue to vaccine in cancer patients at any of the three dose levels.One transient grade 3 adverse event (AE) possibly relatedto vaccine (diarrhea) resolved without intervention and didnot recur with subsequent vaccine. All other AEs related tovaccine were transient and �grade 2. Brachyury-specific T-cellresponses were observed at all dose levels and in most patients.
Conclusions: The MVA-brachyury-TRICOM vaccine directedagainst a transcription factor known to mediate EMT can beadministered safely in patients with advanced cancer and canactivate brachyury-specific T cells in vitro and in patients. Furtherstudies of this vaccine in combination therapies arewarranted andplanned. Clin Cancer Res; 23(22); 6833–45. �2017 AACR.
IntroductionBrachyury was first identified as an embryonic transcription
factor of the T-box family that regulates the formation of theposterior mesoderm in the developing murine embryo, a pro-cess that involves the conversion of epithelial layers intomesenchymal cells (1). Subsequent studies have found thatbrachyury is absent in most normal adult human tissues, withthe exception of low levels found in normal testis, thyroid,and a subset of B cells (2, 3). High levels of brachyury have
been found, however, in the primary and/or metastatic sites ofnon–small cell lung cancer (NSCLC) and small cell lung cancer(4, 5), colon (6), hepatocellular (7), prostate (8), and breastcarcinomas (9), including triple-negative breast cancer (TNBC;ref. 10). High levels of brachyury are also characteristic ofchordoma (11, 12), a rare tumor type thought to originatefrom remnants of the notochord where brachyury is normallyfound in the human embryo.
We and others have now characterized the role of brachyuryin the biology of epithelial tumors and demonstrated its abilityto induce the process of carcinoma mesenchymalization(13), i.e., a phenotypic conversion of tumor cells from anepithelial to a mesenchymal-like phenotype (also designatedas an epithelial–mesenchymal transition, or EMT; refs. 14, 15).Tumor cells undergoing this phenotypic transition exhibitenhanced motility and invasiveness in vitro, a propensity tometastasize in vivo, and features of tumor stemness (16), includ-ing resistance to a range of therapeutics such as chemotherapy,radiotherapy, small molecule therapies, and, potentially, immu-notherapy (17–20). In agreement with a role for brachyury inthe progression of carcinomas, multiple studies have nowshown that the level of brachyury in the primary tumor corre-lates with poor patient prognosis in carcinomas of the lung (21),colon (6), breast (9), triple-negative breast (10), and gastroin-testinal stromal tumor (22). Brachyury expression has also beenshown to be correlated with advanced-stage prostate cancer (8).
1Laboratory of Tumor Immunology and Biology, Center for Cancer Research,National Cancer Institute, National Institutes of Health, Bethesda, Maryland.2Genitourinary Malignancies Branch, Center for Cancer Research, NationalCancer Institute, National Institutes of Health, Bethesda, Maryland. 3BavarianNordic GmbH, Martinsried, Germany.
C.R. Heery and C. Palena contributed equally to this article.
J. Schlom and J.L. Gulley contributed equally to this article.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: J.L. Gulley, National Cancer Institute, 10 Center Dr.,13N240, Bethesda, MD 20892; Phone: 301-480-7164; Fax: 301-480-6288; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-17-1087
�2017 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 6833
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

In addition to having a tumor-restricted pattern of expressionand a relevant role in several aspects of tumor progression,brachyury has been shown to be an immunogenic target. Utilizing9-mer peptides of the brachyury protein, for example, brachyury-specific CD8þ T cells have been expanded in vitro from the bloodof cancer patients. These brachyury-specific CD8þ T cells wereutilized in cytotoxic assays for effective lysis of human tumor cellsthat endogenously express brachyury (23, 24). These combinedproperties, i.e., tumor-restricted expression, relevant function intumor progression, and immunogenicity, make the self-antigenbrachyury a potential target for immunotherapy-mediatedapproaches against cancer.
Here, we describe the preclinical work that led to the develop-ment of a recombinant brachyury-specific poxviral vaccine and thephase I clinical trial of this agent. This poxviral platform, whichencodes the transgenes for the target antigen(s) as well as a triad ofhuman T-cell costimulatorymolecules (TRICOM: B7.1, LFA-3, andICAM-1; ref. 25), has been previously evaluated across multipleclinical trials (26–32). The vaccine in this brachyury-TRICOMclinical trial (NCT02179515) differs from the previous generationof TRICOM-based vaccines in that the priming vector is not vacci-nia virus, but a replication-incompetent form of vaccinia desig-nated Modified Vaccinia Ankara (MVA). MVA has an improvedsafety profile compared with vaccinia, and its inability to replicateallows MVA to be administered more than once without a signif-icant host-neutralizing immune response (33–38). This dose-escalation phase I study was conducted to demonstrate the safetyofMVA-brachyury-TRICOMand to determine its ability to generatebrachyury-specific CD4þ or CD8þ T cells in patients with advancedcancer. Future phase II studies of this vaccine will be based on thepreclinical rationale of vaccine studies in combination with check-point inhibitor mAbs, immune modulators, inhibitors of immu-nosuppressive entities, and combinations of these (39–43).
Materials and MethodsPreclinicalVaccine construct. MVA-brachyury-TRICOM vaccine comprisesMVA, a strain of vaccinia that lacks replication capacity despite
maintaining the ability to infect human cells and express trans-genes, and the transgenes for brachyury and the triad of humancostimulatory molecules (B7.1, LFA-3, and ICAM-1; ref. 44). Thevaccine was developed as part of a Cooperative Research andDevelopment Agreement (CRADA) between the National CancerInstitute (NCI) and Bavarian Nordic.
Culture and infection of human DCs. Peripheral blood mononu-clear cells (PBMC) were separated from heparinized blood ofnormal donors obtained from the NIH Blood Bank by centrifu-gation on a Ficoll density gradient (Lymphocyte SeparationMedium, LSM; MP Biomedicals). For preparation of dendriticcells (DC), PBMCswere resuspended in AIM-Vmedium (Thermo-Fisher) and allowed to adhere to the surface of T-150 flasks(Corning) for 2 hours at 37�C. The nonadherent cell fraction wasremoved with a gentle rinse. Adherent cells were cultured for 6days in AIM-V medium containing 100 ng/mL of recombinanthuman GM-CSF and 20 ng/mL of recombinant human IL4(Peprotech). The culture medium was replenished every 3 days.On day 6, DCs (1 � 106) were incubated with MVA-brachyury-TRICOMor a controlMVA empty vector [MVA-wild type (WT)] orMVA-TRICOM (devoid of the brachyury transgene), for 1 hour at37�C in 1 mL of Opti-MEM medium (ThermoFisher) at a mul-tiplicity of infection (MOI) of 10:1. Infected DCs were subse-quently suspended in 10 mL of fresh, warmed RPMI-1640 medi-um (ThermoFisher) containing 10% FBS and cultured for 24hours prior to analysis.
Flow cytometric analysis. Infected DCs were washed with cold PBS1� and stained for 40minutes at 4�Cusing phycoerythrin-labeledantibodies against human B7.1 (CD80), ICAM-1 (CD54), andLFA-3 (CD58), or a control isotype IgG (BD Biosciences). Fol-lowing staining, cells were washed and resuspended in PBS 1�and analyzed using a FACSCalibur cell analyzer (BD Biosciences)and FlowJo 9.9 software (FlowJo, LLC). Results are shown inpercent positive cells for each marker and mean fluorescenceintensity (MFI).
Western blot. Protein lysates from uninfected DCs and DCsinfected with 10 MOI of the MVA-WT or MVA-brachyury-TRICOMvectors were preparedwith RIPA lysis buffer (Santa CruzBiotechnology) supplemented with 1 mmol/L phenylmethane-sulfonyl fluoride (Sigma-Aldrich). Protein lysates (20 mg) wereresolved on SDS-PAGE and transferred onto nitrocellulose mem-branes using a standard Western blot protocol. Membranes wereprobed overnight at 4�C with a primary rabbit mAb againstbrachyury (MAb 54-1; ref. 3), followed by 1-hour incubationwith a secondary anti-rabbit antibody conjugated with IRDye.Membranes were imaged using the Odyssey Infrared ImagingSystem (LI-COR Biosciences).
Immunofluorescence. DCs were grown on glass coverslipsand infected by direct addition of 10 MOI of the MVA-WTor MVA-brachyury-TRICOM vectors in 1 mL Opti-MEM medi-um. After a 1-hour infection, warmed RPMI-1640 mediumcontaining 10% FBS was added for an additional 24-hourculture. Cells were fixed with 3% paraformaldehyde, per-meabilized with 0.05% Triton X-100, and blocked with PBScontaining 10% goat serum and 1% BSA. Coverslips wereincubated overnight with anti-brachyury MAb 54-1, followedby incubation with an AlexaFluor-488–conjugated secondary
Translational Relevance
Transcription factors such as brachyury are known toplay animportant role in the processes of epithelial-to-mesenchymaltransition (EMT), stemness, and resistance to therapy ofhuman cancer cells. We describe here the generation of avector-based vaccine expressing the transgenes for brachyuryand three humanT-cell costimulatorymolecules. The ability ofthis vaccine to activate CD8þ and CD4þ T cells specific againstthe self-antigen brachyury, both in vitro and in advanced cancerpatients in the absence of a dose-limiting toxicity, provides therationale to target the EMT process in subsequent phase IIstudies in combinationwith checkpoint inhibitormonoclonalantibodies and other immune modulators. Distinct fromtargeting a tumor-associated antigenor a neoepitope, targetingthe process of tumor cells undergoing mesenchymalizationrepresents a unique strategy tominimize tumor disseminationand, more importantly, to prevent the emergence of tumorresistance to therapies.
Heery et al.
Clin Cancer Res; 23(22) November 15, 2017 Clinical Cancer Research6834
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

antibody (ThermoFisher) and staining with DAPI (Thermo-Fisher). Coverslips were mounted using Fluorogel (ElectronMicroscopy Sciences) and imaged utilizing a fluorescencemicroscope (Leica Microsystems). Percentage of DCs expressingbrachyury was calculated as the average of brachyury-positivecells relative to the total number of DAPI-positive nucleicounted from two 20� fields.
Activation of brachyury-specific T cells. For activation of brachyury-specific CD8þ T cells, DCswere prepared fromPBMCs of a normaldonor and infected on day 6 with 10 MOI of MVA-brachyury-TRICOM, MVA-WT, or MVA-TRICOM (encoding for the threecostimulatory molecules but not brachyury), for 1 hour at 37�C.Cells were then cultured in serum-containing medium for anadditional 24-hour period. Allogeneic, brachyury-specific CD8þ Tcells (1� 105 T cells, generated against a brachyury-specific 9-merpeptide, designated as Tp2; ref. 23) were stimulated with irradi-atedDCs at a T-cell:DCs ratio of 10:1. After 24hours, supernatantswere collected and evaluated for IFNg production by ELISA;background observed with T cells only was subtracted from thevalues observed with MVA-WT-, MVA-TRICOM-, and MVA-bra-chyury-TRICOM-infected DCs.
For activation of autologous brachyury-specific T cells, DCswere prepared from PBMCs of four normal donors and infectedwith MVA-brachyury-TRICOM, as indicated above. AutologousPBMCs were stimulated with irradiated MVA-brachyury-TRI-COM–infected DCs at a PBMC:DC ratio of 10:1. After 3 days,IL2 (20 U/mL) was added to the culture; each stimulation cyclelasted 7 days. At the end of two stimulation cycles (IVS2), CD4þ
T cells were isolated by negative selection with magnetic beads(Miltenyi) and assayed for proliferation in response to autologousPBMCs pulsed with control HSA protein or a recombinant,purified His-brachyury protein. Proliferation of CD4þ T cells wasmeasured on day 5 by [3H]-thymidine incorporation. Productionof IFNg was evaluated with total T cells stimulated for two IVS asindicated above, and subsequently activated in the presence ofautologous DCs pulsed with control HSA or His-brachyury pro-tein. Supernatantswere collected at 72 to 96hours and assayed forIFNg production by ELISA.
Detection of brachyury-specific T cells. PBMCs from patientsenrolled in the clinical trial were separated by Ficoll–Hypaquedensity gradient separation, washed 3 times, and cryopreservedin 90% heat-inactivated human AB serum and 10% DMSO inliquid nitrogen at a concentration of 1 � 107 cells/mL untilassayed. Analysis of antigen-specific responses following therapywas assessed by intracellular cytokine staining following a periodof in vitro stimulation (IVS) with overlapping 15-mer peptidepools encoding the tumor-associated antigen (TAA) brachyury aspreviously described (45). The TAA peptide pool was designed tocontain a brachyury agonist epitope that had been previouslyidentified (24). Peptide pools encoding for HLA and CEFT(a mixture of peptides of cytomegalovirus, EBV, influenza, andtetanus toxin) served as negative and positive controls, respec-tively. Peptide mixes were purchased from JPT, reconstituted inDMSO, and utilized immediately.
Cryopreserved PBMCs from patients before therapy and ondays 28 (post I cycle of vaccine), 56 (post II cycles of vaccine),84 (post III cycles of vaccine), and at a late time point(days 168–190, where available) were assayed as previouslydescribed (45). Using a BD LSR-II flow cytometer equipped
with a UV, violet, blue, and red laser, 3 � 105 events in the livegate were acquired. FCS files were analyzed with FlowJo V.9.7for Macintosh (TreeStar). Nonviable cells were excluded, andfluorescence minus one controls were used for gating. Theabsolute number of CD4þ or CD8þ T lymphocytes producingcytokine or positive for CD107a was calculated per 1� 106 cellsplated at the start of the IVS. The background signal (obtainedwith the HLA peptide pool) and any value obtained priorto vaccination were subtracted from those obtained aftervaccination ([post-brachyury – post-HLA] – [pre-brachyury– pre-HLA]). An antigen-specific immune response to brachy-ury was scored as positive if a patient had more than 250 CD4þ
or CD8þ T cells that produced IFNg , TNF, IL2, or were positivefor CD107a at the end of the stimulation assay per 1 � 106 cellsthat were plated at the start of the assay.
Immunoassay for brachyury-specific antibodies. Serum sampleswere collected from patients enrolled in the clinical trial in serumseparator tubes, spun down, and stored at �80�C. Immulon4HBX 96-well plates (Thermo Scientific) were coated with 1mg/mL of a purified, recombinant brachyury protein or 5% BSAin PBS for 4 hours at room temperature. Assay plates were washedtwice with PBS and blocked for 3 hours at room temperature with5% BSA in PBS. Serum collected from patients before vaccinationand on days 28, 56, and 84 after vaccination was added at a 1:100dilution in PBS with 1% BSA. Following overnight incubation at4�C, plates were washed 4 times with PBST buffer (PBSþ 0.05 %Tween-20). A secondary horseradish peroxidase–labeled anti-human IgG antibody (BD Biosciences) was added at 1:6,000dilution in PBS with 1% BSA. After a 1-hour incubation at roomtemperature, plates were washed 4 times with PBST; SureBlueTMB Microwell Peroxidase Substrate (KPL) was added, and colorwas allowed to develop for 30 minutes in the dark at roomtemperature. The reaction was stopped utilizing TBM stop solu-tion (KPL), and absorbance was read at 405 nm. Titer was definedas the maximum dilution where the absorbance at 450 nm wastwice that obtained from the same sample on the control BSAplate at a 1:50 dilution of sera.
Statistical analysis. Data were analyzed using GraphPad Prism(GraphPad Software). Mean comparisons among groups wereconducted by one-way ANOVA; multiple comparison analysisused the Tukey test. Graphs depict the mean � SD from replicatemeasures for each group.
Clinical trialPatients. Eligibility for the trial required patients to be >18 yearsof age with evaluable (not necessarily measurable) metasta-tic or unresectable locally advanced solid tumors, includingchordoma, and good Eastern Cooperative Oncology Groupperformance status (0–1). Patients must have completed atleast one line of standard therapy (if one existed) at least4 weeks prior to enrollment, with resolution of any grade�2 adverse events (AEs) from prior therapy and could not beeligible for curative therapy. Patients with resected metastaticdisease at high risk of recurrence were eligible. Essentiallynormal organ function and barrier contraception and/or absti-nence was required. During dose escalation, no other cancertreatment was allowed. Exclusion criteria included chronicinfection, including hepatitis B or C and HIV, altered mentalstatus, autoimmune disorders of clinical significance,
Phase I Trial of MVA-Brachyury-TRICOM
www.aacrjournals.org Clin Cancer Res; 23(22) November 15, 2017 6835
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

concurrent systemic corticosteroid use, untreated central ner-vous system metastases, history of allergic reaction to compo-nents of vaccine, serious uncontrolled medical issues, andpregnancy.
Trial design and oversight. The trial was a phase I dose-escalationstudy to demonstrate the safety and immunogenicity of MVA-brachyury-TRICOM in patients with advanced solid malignan-cies. Three vaccine dose levels (DL) were evaluated. Doseswere administered subcutaneously. Each injection site received5 � 108 plaque-forming units (PFU). At increasing DLs, one, two,and four injection sites were given per dose to make total PFUdelivery 5 � 108, 1 � 109, and 2 � 109 at DLs 1, 2, and3, respectively. After safety was established, expansion of the twohighest doses for further safety and immune response analysis wasconducted. In these cohorts, eligibility was modified to allowpatients receiving specific standard therapies. Patients withEGFR-mutated lung cancer who were being treated with erlotinibfor at least 3 months with ongoing response or stable disease wereallowed to continue erlotinib and enter the study. Patients withERþ breast cancer could continue hormonal therapy. Patients withHer2þ breast cancer could continue onmaintenanceHer2-directed
therapy. Finally, patients with colorectal cancer who had complet-ed front-line combination chemotherapy and were on mainte-nance capecitabine and/or bevacizumab were eligible
The trial was run in accordance with the Declaration ofHelsinki after approval by the Scientific Review Committeeand Institutional Review Board (IRB) of the Intramural Nation-al Cancer Institute (NCI) and the Center for Cancer Research,NCI. NCI sponsored this study. Ongoing safety monitoringwas conducted by the IRB and the Intramural Data SafetyMonitoring Board. All serious AEs were reported to the FDAfor review per guidelines. Informed consent was obtained fromeach participant, including consent for treatment, primary andsecondary endpoints, and correlative studies.
ResultsIn vitro studies
The ability of the MVA-brachyury-TRICOM vector to infecthuman DCs in vitro was first evaluated. As shown in Fig. 1A,whereas human DCs endogenously express costimulatory mole-cules, expression of the encoded human costimulatory moleculetransgenes B7.1, ICAM-1, and LFA-3 was markedly enhanced in
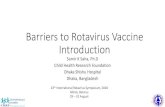
Figure 1.
A, Flow cytometric analysis of CD80 (B7.1), CD54 (ICAM-1), and CD58 (LFA-3) expression in human DCs infected with indicated vectors (10 MOI, 24 hours).Shown is the percent-positive cells for each marker and the MFI. B, Western blot analysis of brachyury expression in protein lysates of indicated DCcultures. GAPDH is used as a loading control protein for each sample. C, Immunofluorescence analysis of brachyury expression in indicated DC cultures;green corresponds to brachyury, and blue corresponds to DAPI-stained nuclei. Magnification, �20.
Heery et al.
Clin Cancer Res; 23(22) November 15, 2017 Clinical Cancer Research6836
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

MVA-brachyury-TRICOM–infected cells versus control MVA-WT–infected cells. Expression of the encoded brachyury protein wasalso observed in MVA-brachyury-TRICOM–infected human DCs,and compared with uninfected and control MVA-WT–infectedcells (Fig. 1B). Immunofluorescent analysis demonstrated expres-sion of brachyury protein in 63% � 11% of DCs infected withMVA-brachyury-TRICOM (Fig. 1C).
MVA-brachyury-TRICOM–infected human DCs were subse-quently used in vitro as antigen-presenting cells (APC) to stim-ulate HLA-A2–restricted, brachyury-specific human CD8þ
T cells. Brachyury-specific T cells were generated against a 9-mer
epitope of brachyury (Tp2, WLLPGTSTL), as previouslydescribed (23). DCs generated from PBMCs of an HLA-A2þ
healthy donor were infected with MVA-WT, MVA-TRICOM, orMVA-brachyury-TRICOM, subsequently irradiated, and used asAPCs for stimulation of brachyury-specific CD8þ T cells. Ascontrol, a recombinant vector encoding for the three costimu-latory molecules (MVA-TRICOM) and not the target brachyurywas used. As shown in Fig. 2A, MVA-brachyury-TRICOM–
infected DCs efficiently stimulated brachyury-specific CD8þ
T cells to secrete high levels of IFNg , compared with the levelsobserved with control-infected DCs.
Figure 2.
A, DCs infected with 10 MOI of MVA-WT, MVA-TRICOM, or MVA-brachyury-TRICOM vectors were used for stimulation of allogeneic, brachyury-specific CD8þ
T cells generated against a brachyury-specific 9-mer peptide. After 24 hours, supernatants were collected and evaluated for IFNg production by ELISAassay. Shown are the IFNg levels (pg/mL) after subtraction of background in response to T cells only. One-way ANOVA, P ¼ 0.0036. Shown P valuesfor comparison between indicated groups were calculated by the Tukey multiple comparisons test. B, DCs infected with 10 MOI of MVA-brachyury-TRICOM vector were used for stimulation of autologous PBMCs, as described in detail in the Materials and Methods section. Following two cycles ofstimulation, CD4þ T cells were isolated and stimulated in the presence of autologous PBMCs pulsed with control HSA protein or a recombinant,purified His-brachyury protein. Shown is the proliferation of CD4þ T cells measured as [3H] thymidine incorporation (cpm ¼ counts per minute) for tworepresentative donors. One-way ANOVA, P ¼ 0.0046 (top) and P ¼ 0.004 (bottom). C, Supernatants from autologous T cells were collected at 72 to96 hours and assayed for IFNg production by ELISA. One-way ANOVA, P ¼ 0.0329 (top) and P ¼ 0.0007 (bottom). In all panels, P values forcomparison between indicated groups were calculated by the Tukey multiple comparisons test.
Phase I Trial of MVA-Brachyury-TRICOM
www.aacrjournals.org Clin Cancer Res; 23(22) November 15, 2017 6837
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

In additional experiments, the ability of MVA-brachyury-TRICOM-infected DCs to stimulate autologous brachyury-specific T cells was also investigated. DCs prepared fromPBMCs of several normal donors were infected with MVA-brachyury-TRICOM and used as APCs for IVS of autologousPBMCs. At the end of two cycles of stimulation (IVS2), CD4þ
T cells were isolated and assayed for proliferation in responseto autologous PBMCs pulsed with control HSA protein orpurified His-brachyury protein. As shown in Fig. 2B for tworepresentative donors, CD4þ T cells generated in responseto MVA-brachyury-TRICOM-infected DCs efficiently pro-liferated in response to brachyury versus control HSA protein.Overall, proliferation of autologous CD4þ T cells was observedin 3 of 5 donors evaluated. Production of IFNg by totalT cells stimulated for two IVS with autologous MVA-brachy-ury-TRICOM-infected DCs was also evaluated. As shown inFig. 2C for two donors, autologous T cells stimulated withMVA-brachyury-TRICOM released IFNg in response to brachy-ury but not control HSA (Fig. 2C). Overall, 2 of 5 normaldonors evaluated showed IFNg production in response tobrachyury protein following stimulation with autologous,MVA-brachyury-TRICOM-infected DCs.
Altogether, these results demonstrated that MVA-brachyury-TRICOM is able to efficiently infect and direct the expressionof the encoded transgenes, brachyury, B7.1, ICAM-1, and LFA-3 in human DCs. More importantly, the results demonstratedthat the antigen brachyury encoded by the virus is beingprocessed and presented in the surface of infected DCs in thecontext of MHC-class I and II molecules, leading to theeffective activation of brachyury-specific CD8þ and CD4þ
T cells, respectively.
Patient demographicsIn total, 38 patients (Table 1) were enrolled on the study
between July 2014 and March 2015 (DL1, n ¼ 3; DL2, n ¼ 17;DL3; n ¼ 18). On DL2 and DL3, 1 and 2 patients, respectively,were not evaluable for safety or immune responses and replac-ed. Patient baseline characteristics are shown in Table 1. In theexpansion cohorts, 13 patients remained on maintenancestandard therapy for colorectal cancer, EGFR-mutated lungcancer, and ERþ breast cancer. Median age at enrollment was60 (range, 35–86), with 53% (n ¼ 20) female. Excluding thepatients on maintenance therapy at enrollment (n ¼ 13 total),23 of 25 patients had evidence of progressing disease (byimaging, symptoms, or serum markers) within 3 months priorto enrollment on study and had received multiple lines of priortherapy (median, 3; range, 0–8, Table 1).
SafetyMVA-brachyury was well tolerated with no dose-limiting
toxicities (Table 2). The MTD was not reached. Two deathsoccurred on study, both due to complications of rapid diseaseprogression unrelated to vaccine. Two other serious AEsoccurred, a hip fracture caused by a fall and a colonic obstruc-tion due to disease progression. No serious AE was related tovaccine. AEs occurring in >2 unique patients included injection-site reaction (78.9%), flu-like symptoms (39.5%), fever(21.1%), and diarrhea (7.9%). One grade 3 AE, diarrhea, wasrelated to vaccine and resolved without intervention after48 hours. All other AEs related to vaccine were grade 1 or 2with short duration.
Clinical activity and outcomesMost (34/38) patients on study completed all three doses of
therapy. Four patients did not complete therapy due to progres-sion (n ¼ 3) or death (n ¼ 1). Two patients died on study. Onepatient with colon cancer died due to rapid disease progression 36days after her third dose. The other patient had cholangiocarci-noma and refused treatment when she had sepsis presumablyrelated to common bile duct stent infection, but workup andtreatmentwere stopped based on the patient's pre-existingwishes.She received two vaccinations and died 5.5 weeks after startingtreatment. Twenty-one patients had progressive disease as theirbest response, and 17 had stable disease. As there were only threevaccines offered on study, 13 patients elected to pursue differenttreatments or to participate in a different clinical trial, and fourwithdrew due to logistical concerns.
The most notable clinical outcomes were in the 4 patientswith metastatic EGFR-mutated lung cancer in the expansioncohort who enrolled on study while on maintenance erlotinib.Patients 11, 28, 34, and 36 (Table 1) had three, one, two, andfour prior therapies, respectively, going on the vaccine study.All had been treated with erlotinib for at least 3 months and
Table 1. Demographic characteristics of enrolled patients
Doselevel
Patientnumber Age
Cancerdiagnosis
Number ofprior treatments
1 1 60 Chordoma 11 2 58 Ovarian Ca 11 3 65 Chordoma 1
2 4 65 Chordoma 12 5 58 Chordoma 32 6 84 Pancreatic Ca 12 7 54 Colon Ca 42 8 48 Chordoma 02 9 42 Chordoma 22 10 69 Chordoma 12 11 64 Lung Caa 22 15 44 Breast Caa 22 17 64 Colon Caa 52 18 72 Breast Caa 22 20 47 Colon Caa 32 22 75 Prostate Ca 12 23 60 Colon Ca 42 24 60 Colon Caa 32 25 69 Breast Ca 32 31 53 Chordoma 2
3 12 65 Pancreatic Ca 33 13 65 Cholangiocarcinoma 23 14 57 Colon Ca 23 16 59 Chordoma 23 19 65 Prostate Ca 33 21 53 Chordoma 23 26 35 Colon Caa 53 27 51 Breast Caa 23 28 60 Lung Caa 13 29 60 Prostate Ca 23 30 60 Chordoma 03 32 51 Colon Caa 53 33 50 Colon Ca 23 34 86 Lung Caa 13 35 57 Chordoma 33 36 54 Lung Caa 33 37 82 Chordoma 03 38 79 Breast Caa 1aPatient who was on a maintenance therapy at the time of enrollment. Thatmaintenance therapy is included in the number of prior treatments and wascontinued on study. Ca ¼ cancer.
Heery et al.
Clin Cancer Res; 23(22) November 15, 2017 Clinical Cancer Research6838
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

had achieved an objective radiographic response or stabledisease at the time of vaccine study enrollment. It is interestingto note that all 3 of the patients treated at DL3 had progression-free survival more than double the median that was seen inprior trials (Fig. 3; ref. 46). Although it is acknowledged thatthere is intrinsic ascertainment bias in this very small subset ofpatients, the safety seen with this combination opens thepossibility of a clinical endpoint study of erlotinib with orwithout vaccine.
Identification of brachyury-specific T cellsOf the 38 patients enrolled on study, sufficient PBMCs were
available from 34 patients to analyze brachyury-specific CD4þ
and CD8þ T-cell responses. PBMCs were examined beforetherapy and after cycle I (day 28, n ¼ 34), cycle II (day 56,n ¼ 34), and cycle III of vaccine (day 84, n ¼ 32), as well as at alater time point (days 168–190, n ¼ 10). The FACS-based assayfor T cells expressing the type I cytokines IFNg , IL2, TNFa, and/or the degranulation marker CD107a following stimulationwith overlapping peptide pools is described in detail in theMaterials and Methods section. All assays for a given patient'ssamples before and after vaccine were performed in the samecontrolled experiment.
Including all DLs and all cancer types, 28 of 34 (82%)patients developed brachyury-specific CD4þ and/or CD8þ
T-cell responses after vaccination (Table 3). Of the 28 patientswho developed brachyury-specific responses, 20 (71%) dis-played T cells that were positive for the degranulation markerCD107a, which identifies tumor-lytic cells (47). The inductionof brachyury-specific T-cell responses was rapid, with responsesdeveloping in 17 patients after a single vaccination and in9 patients after two vaccinations. The development of poly-functional brachyury-specific T cells was seen at all DLs, with2 of 3 (66%) patients developing brachyury-specific T cellsafter vaccination at DL1, 12 of 15 (80%) patients at DL2, and14 of 16 (88%) patients at DL3. Brachyury-specific T-cellstimulation persisted for at least two consecutive cycles in0 of 3 patients at the lowest DL, 5 of 15 in the second DL,and 8 of 16 patients at the highest DL. Brachyury-specific T-cellstimulation was observed at >1 timepoint (nonconsecutive) in0 of 3 patients at the lowest DL, 8 of 15 in the second DL, and10 of 16 patients in the highest DL.
Three of the 4 patients with EGFR-mutated NSCLC, whoreceived maintenance erlotinib while on study, developed bra-chyury-specific T-cell responses. The responses in these 3 patientswere noted in both the CD4þ and CD8þ T-cell compartments andincluded the production ofmultiple cytokines aswell as positivityfor the degranulation marker CD107a. As noted previously, allvalues shown in Table 3 are background subtracted for any priorbrachyury-specific T cells as well as responses to the HLA controlpeptides.
Fourteen of 34 patients (41%) had detectable levels ofbrachyury-specific T-cell responses prior to therapy. Thesepre-existing brachyury-specific T cells were noted in 8 of 23patients (35%) with various types of carcinoma, and 6 of 11patients (55%) with chordoma. Of the 14 patients with pre-existing brachyury-specific T-cell responses, only 10 (71%)developed enhanced brachyury-specific T-cell responses aftervaccination. Of the 20 patients who had no detectable level ofbrachyury-specific T cells prior to vaccination, 18 (90%) devel-oped brachyury-specific T cells after vaccination (Table 4).Ta
ble
2.AEprofile
ofMVA-brachyu
ry-TRICOM Grade1
Grade2
Grade3
AllGrades
CTC
term
Num
ber
of
distinc
tpatients
%ofall
patients
(n¼
38)
Num
ber
of
even
ts
Eve
nts
as%
of
doses
given
(n¼
107)
Num
ber
of
distinc
tpatients
%ofall
patients
(n¼
38)
Num
ber
of
even
ts
Eve
nts
as%
of
doses
given
(n¼
107)
Num
ber
ofdistinc
tpatients
%ofall
patients
(n¼
38)
Num
ber
of
even
ts
Eve
nts
as%
of
doses
given
(n¼
107)
Num
ber
of
distinc
tpatients
%ofall
patients
(n¼
38)
Num
ber
of
even
ts
Eve
nts
as%
of
doses
given
(n¼
107)
Aspartate
aminotran
sferase
increa
sed
12.6
10.9
00
00
00
00
12.6
10.9
Diarrhe
a2
5.3
32.8
00
00
12.6
10.9
37.9
43.7
Fatigue
12.6
10.9
00
00
00
00
12.6
10.9
Fev
er7
18.4
98.4
12.6
10.9
00
00
821.1
109.3
Flu-likesymptoms
1539
.523
21.5
00
00
00
00
1539
.523
21.5
Hea
dache
12.6
10.9
00
00
00
00
12.6
10.9
Injection-site
reaction
2155
.332
29.9
1950
.026
24.3
00
00
3078
.958
54.2
Pruritus
12.6
10.9
00
00
00
00
12.6
10.9
Rashacne
iform
12.6
10.9
00
00
00
00
12.6
10.9
Phase I Trial of MVA-Brachyury-TRICOM
www.aacrjournals.org Clin Cancer Res; 23(22) November 15, 2017 6839
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

Anti-brachyury antibodiesThree of 34 patients (9%) displayed low levels of antibodies
reactive to brachyury at baseline, using the criteria defined inthe Materials and Methods section. A positive brachyury anti-body titer consisted of an absorbance to brachyury protein thatwas twice that obtained with the negative control protein BSA.One of these patients developed a very slight increase in titerafter three cycles of vaccine. In addition, 4 of 31 patients (13%)who had undetectable levels of antibodies reactive to brachyuryat baseline developed barely detectable levels of titer followingvaccination.
DiscussionThe phenomenon of carcinoma mesenchymalization is now
recognized as an important step during the progression ofcarcinomas toward metastatic disease. Clinical evidence of theassociation of this phenomenon with tumor progressionincludes, for example, the observation that mesenchymal-cir-culating tumor cells in breast cancer patients positively asso-ciate with disease progression and failure to therapy (48).Distinct from targeting a TAA or a neoepitope, targeting theprocess of tumor cells undergoing mesenchymalization repre-sents a unique strategy to minimize tumor dissemination and,more importantly, to prevent the emergence of tumor resis-tance to therapies. One potential strategy to target the phe-nomenon of mesenchymalization is immunotherapy. Thetranscription factor brachyury has been extensively character-ized in previous studies (9, 14, 17, 49) in terms of (i) its abilityto drive carcinoma cells into a mesenchymal-like invasivephenotype (mesenchymalization); (ii) its ability to promotethe acquisition of tumor resistance to a range of anticancertherapies; (iii) its tumor-restricted pattern of expression withminimal expression in normal adult tissues; and (iv) itsimmunogenicity. Due to the location of transcription factorsin the cell nucleus and their lack of a hydrophobic groove, theyhave been characterized as "non-druggable" or difficult totarget by other types of therapeutics. However, prior studiesand those reported here demonstrate that the breakdown ofbrachyury in the cytoplasm can lead to the generation ofbrachyury peptide MHC complexes in DCs capable of activat-ing brachyury-specific T cells. Prior studies (23) have shown
that brachyury-specific T cells can lyse human tumor cellsendogenously expressing brachyury. These findings make bra-chyury a potential vaccine target to eradicate cells undergoingmesenchymalization via an immune-mediated approach. Priorstudies (28, 50) have also demonstrated that cancer patientsreceiving either carcinoembryonic antigen (CEA)- or prostate-specific antigen (PSA)-based vaccines develop postvaccinationT-cell responses to brachyury, probably due to cross-presenta-tion of brachyury to APCs as a consequence of some tumor celldestruction. These findings further demonstrated the immu-nogenicity of brachyury in humans.
Here, we demonstrated the ability of MVA-brachyury-TRI-COM to successfully infect human DCs in vitro and to direct theexpression of brachyury and encoded costimulatory molecules,leading to the activation of both CD8þ and CD4þ T cellsspecific against brachyury, a self-antigen. The experiment withallogeneic T cells as presented in Fig. 2A was meant only topreliminarily evaluate whether human DCs infected with MVA-brachyury-TRICOM could correctly process and present brachy-ury peptides in the context of MHC class I to a previouslyestablished brachyury-specific T-cell line. Activation of autol-ogous T cells was conducted with normal donors, and the dataare presented in Fig. 2B and C, where we demonstrate thatMVA-brachyury-TRICOM-infected DCs can activate brachyury-specific T cells, as denoted by the proliferation and/or IFNgproduction in response to brachyury protein. These experi-ments were conducted in a strictly autologous setting. More-over, the data presented in Table 3 regarding activation ofcancer patients' blood in response to brachyury-specific peptidestimulation in vitro indicate that MVA-brachyury-TRICOM isable to infect APCs in the vaccinated patients, and that thebrachyury protein is being expressed, correctly processed, andpresented by those APCs in an autologous fashion to thepatients' T cells, resulting in expansion of brachyury-specificimmune responses, both CD4 and CD8, in >80% of vaccinatedpatients. The preclinical studies generated the rationale for thephase I trial of MVA-brachyury-TRICOM. MVA has been select-ed here as a vector due to its infectivity of human DCs and itsincapacity to replicate in mammals and its ability to inducesimilar levels of cellular immune responses to self-antigens andantitumor activity as vaccinia (51). MVA has demonstratedsafety in immunosuppressed patients and is being stockpiled
Figure 3.
Progression-free survival on combination of vaccine and erlotinib. Patient 11 was treated on vaccine DL2, with time on vaccine of 15.9 months, for a totalof 21.5 months on erlotinib. Patients 28, 34, and 36 were treated on vaccine DL3. Patient 28 was on vaccine study for 21.8þ months, and total time onerlotinib was 41.9þmonths at the time of data lock for this publication. Patient 34 was on vaccine for 19.8 months, and total time on erlotinib was 35.0 months.Patient 36 was on vaccine study for 20þ months, with a total time on erlotinib of 32þ months at the time of data lock for this publication.
Heery et al.
Clin Cancer Res; 23(22) November 15, 2017 Clinical Cancer Research6840
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

Table
3.Dev
elopmen
tofbrachyu
ry-specificT-cellresponses
byintracellularcytokine
staining
Clin
ical
characteristics
Cycle
ICycle
IICycle
III
Late
Dose
leve
l
CD4
CD8
CD4
CD8
CD4
CD8
CD4
CD8
Any
post
Pt
Can
cer
CD107a
IFNg
IL2
TNF
CD107a
IFNg
IL2
TNF
CD107a
IFNg
IL2
TNF
CD107a
IFNg
IL2
TNF
CD107a
IFNg
IL2
TNF
CD107a
IFNg
IL2
TNF
CD107a
IFNg
IL2TN
FCD107a
IFNgIL2TN
F
Carcino
ma
2Ova
rian
10
00
00
00
00
00
00
00
00
00
00
017
00/1
(0%)
15Breast
20
06
00
471
0894
2,121
00
194
00
0458
00
00
00
00
00
00
00
00
7/10
(70%)
18Breast
20
070
00
079
00
075
00
00
00
029
00
00
320
00
98
00
00
025
Breast
2603
948
035
50
395
0217
1,77
1134
022
50
268
67
382
0835
3,480
767
00
29104
7Colon
20
80
00
096
00
00
00
00
00
00
00
00
017
Colon
20
00
389
00
0446
00
00
0191
00
87
00
00
00
028
50
44
00
135
045
23Colon
20
00
00
00
00
00
00
00
560
00
00
00
024
Colon
20
00
00
366
00
00
00
00
00
00
00
00
00
11Lu
ng2
1,22
84,524
1,1201,30
071,107
15,652
45
8,323
00
00
00
00
0217
046
00
00
00
00
00
00
6Pan
crea
tic
20
00
00
00
00
540
00
00
022
Prostate
20
00
00
00
00
00
03,400
654
02,55
80
02,55
70
00
00
27Breast
30
00
136
00
00
025
60
380
00
00
0121
00
0108
011/12(92%
)38
Breast
30
00
00
00
00
00
5,58
10
735
08,763
39,149
23,0085,24
046,867
19,438
2,608
010,472
14Colon
319
0128
01,858
335
0633
00
102
03,76
239
10
1,28
60
00
00
00
00
388
140
00
289
00
26Colon
30
00
00
0162
030
42,150
02,50
03,086
96
01,25
90
929
0973
022
30
032
Colon
30
516
051
023
00
00
00
0188
00
169
110
687
00
00
33Colon
3463
0146
00
00
00
00
00
00
02,461
196
00
6,971
00
028
Lung
30
00
00
00
00
370
00
122
023
5857
265
00
4,417
507
078
834
Lung
30
00
00
00
00
00
00
00
00
00
00
00
036
Lung
31,039
250
1,55
11,825
2,894
411
02
00
00
00
00
00
00
0182
069
12Pan
crea
tic
3404
074
00
00
027
134
80
479
1,982
010
148
00
00
00
00
19Prostate
30
00
00
00
00
039
40
00
00
00
1,686
00
030
10
29Prostate
30
021
00
00
00
0128
01,116
00
0607
058
01,27
60
00
Cho
rdoma
1Cho
rdoma
10
0415
02,125
00
718
00
00
0177
00
00
00
00
5129
2/2(100%)
3Cho
rdoma
10
308
0112
00
340
00
00
00
00
00
083
00
49
043
00
300
00
04
Cho
rdoma
228
00
0695
00
00
00
00
1,59
220
70
804
00
00
00
00
00
00
00
053
55/5(100%)
5Cho
rdoma
20
00
00
00
0838
193
38112
1,148
00
442
00
00
00
60
00
030
011
730
8Cho
rdoma
2216
00
00
749
01,640
00
00
0120
0120
382
00
05,27
823
90
302
9Cho
rdoma
20
00
00
253
00
00
268
00
173
00
00
206
00
46
00
10Cho
rdoma
253
80
00
00
00
00
00
00
00
488
00
03,955
024
00
00
00
00
016
Cho
rdoma
30
036
01,30
90
00
024
854
635
6,327
2,079
141
01,32
4677
032
35,76
10
00
0159
0126
00
370
3/4(75%
)21
Cho
rdoma
30
00
560
00
00
1,640
240
1,56
69,455
5730
71,55
430
Cho
rdoma
30
00
00
00
00
00
00
00
00
00
96
00
00
37Cho
rdoma
30
00
00
00
00
00
00
00
1,629
00
280
552
00
03,655
NOTE:A
bsolute
number
ofC
D4orCD8Tcells
producingcytokine
orpositive
forCD107a
per
1�10
6cells
platedat
startofIVS.N
umbersinboldan
dgrayarethose
positive
afterve
rsus
before
vaccination.Grayindicates
apatient
mee
ting
defi
nedim
mun
eresponsecriteria.
Phase I Trial of MVA-Brachyury-TRICOM
www.aacrjournals.org Clin Cancer Res; 23(22) November 15, 2017 6841
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

as the "safe" anti-smallpox vaccine by the United States andother countries (52, 53). This clinical trial demonstrates thatthe MVA-brachyury-TRICOM vaccine can generate both CD8þ
and CD4þ brachyury-specific T cells in advanced cancer patientswithout serious treatment-related AEs.
The FACS-based assay used in the current study to measure thedevelopment of antigen-specific T-cell responses employed over-lapping peptide pools that span the entire sequence of the TAA,and assessed for the production of cytokines and the degranula-tionmarker CD107a. Due to the low number of T cells specific forbrachyury that can be stimulated in vitro in our experimentalsystem with normal donors, unfortunately, we have been unableto perform a lytic assay with brachyury-positive tumor cells or
peptide titrations to evaluate functional avidity. However, it isimportant to point out that the expression of CD107a, amarker oflytic effector function in T cells of patients vaccinated with MVA-brachyury-TRICOM following in vitro restimulation with brachy-ury-specific peptides, would indicate that the effector T cells havelytic potential and are presumed to be of high avidity. Mostpatients (82%) were shown to develop brachyury-specific T cellsafter vaccination, demonstrating the immunogenicity of thisantigen. In addition, we observed a trend indicating a potentialdose response, resulting in the highest dose being selected for usein future phase II trials. One concern is the observation thatbrachyury-specific immune responses were not maintained formost patients during the trial. Previous studies have shown that
Table 4. Baseline pre-existing brachyury-specific T-cell responses by intracellular cytokine staining assay
CD4 CD8Pt Cancer Dose level CD107a IFNg IL2 TNF CD107a IFNg IL2 TNF
Carcinoma2 Ovarian 1 PRE15 Breast 218 Breast 225 Breast 27 Colon 217 Colon 223 Colon 2 PRE PRE24 Colon 211 Lung 26 Pancreatic 2 PRE PRE22 Prostate 2 PRE PRE PRE27 Breast 338 Breast 3 PRE PRE PRE PRE PRE14 Colon 3 PRE26 Colon 3 PRE PRE32 Colon 3 PRE33 Colon 328 Lung 334 Lung 336 Lung 312 Pancreatic 319 Prostate 329 Prostate 3
Baseline responseDeveloped responseYes No
YES: 8/23 (35%) 5/8 (63%) 3/8 (37%)NO: 15/23 (65%) 13/15 (87%) 2/15 (13%)
CD4 CD8Pt Cancer Dose level CD107a IFNg IL2 TNF CD107a IFNg IL2 TNFChordoma1 Chordoma 1 PRE3 Chordoma 14 Chordoma 2 PRE PRE5 Chordoma 28 Chordoma 2 PRE PRE9 Chordoma 210 Chordoma 2 PRE PRE PRE16 Chordoma 321 Chordoma 330 Chordoma 3 PRE PRE37 Chordoma 3 PRE
Baseline responseDeveloped response
Yes NoYES: 6/11 (55%) 5/6 (83%) 1/6 (17%)NO: 5/11 (45%) 5/5 (100%) 0/5 (0%)
Heery et al.
Clin Cancer Res; 23(22) November 15, 2017 Clinical Cancer Research6842
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

the repeated use of a vaccinia or MVA vector for priming andsubsequent boosting is not as efficient as a diversified prime andboost approach employing vaccinia or MVA followed by a non-replicative avipox or fowlpox vector to elicit antigen-specificimmune responses both in preclinical (51, 54, 55) and clinicalstudies (56, 57). In this regard, a fowlpox vector encoding forbrachyury and TRICOM has now been developed (rF-brachyury-TRICOM) that will be used for boosting of immune responsesfollowing MVA-brachyury-TRICOM priming in subsequent stud-ies (Supplementary Fig. S1). This vector was not available at thetime of this study. A trial of MVA-brachyury-TRICOM vaccine isplanned in which booster doses of rF-brachyury-TRICOM will beemployed. Recombinant fowlpox vectors have been evaluated inmultiple prior clinical studies with an excellent safety profile.Their inability to replicate in mammalian cells also results inminimal host vector-neutralizing immunity and the ability toadminister multiple booster vaccinations.
Because this trial administered only three doses of MVA-bra-chyury-TRICOM, clinical outcomes were difficult to assessbecause most patients opted for alternative therapy once vacci-nation was complete. In the case of EGFR-mutated NSCLC, wewere able to enroll 4 patients who had already responded or hadstable disease for at least 3 months on erlotinib. Among thosepatients, there was preliminary evidence of safety of the combi-nation. Furthermore, although the numbers of patients treated arevery small, it is interesting to note that the time on studywas 15.9,19.8, 20.0þ, and 21.8þ months with a total time on erlotinib of21.5, 35.0, 32.0þ, and 41.9þmonths at the time of data lock forthis article, which compares favorably with the 11- to 12-monthprogression-free survival typically seen with erlotinib. Althoughthere are insufficient numbers of patients to draw any conclu-sions, the safety of the combination, along with preclinical find-ings (42) demonstrating that human tumor cell lines bearing theEGFR mutation can be rendered more susceptible to brachyury-specific T-cell lysis by treatment with erlotinib, provides rationalefor a future combination study in NSCLC.
A prior trial of a recombinant yeast-brachyury–targeting vac-cine demonstrated immunogenicity, safety, and generation ofbrachyury-specific T cells, without evidence of autoimmune tox-icity (45). Preclinical murine studies (58) have shown that boththe recombinant yeast vaccine (yeast-CEA) and the recombinantpoxviral vaccine (CEA-TRICOM) platforms generate immuneresponses directed against different CEA epitopes, most likelydue to differences in antigen processing by the two diverse vaccineplatforms. Those studies also showed that each vaccine platformgenerated a unique TCR repertoire and host cytokine profile. Theuse of both vaccines in combination also resulted in greater
antitumor activity than the use of either one alone. One goal ofpotential future clinical studies would be to employ both MVAand yeast-brachyury vaccine platforms either as combinationtherapy or in a temporal manner.
The safety and immunogenicity demonstrated with the MVA-brachyury-TRICOMvector describedhere in advanced anddiversecancer populations in this phase I study provide the evidence forthe use of this vaccine in combination immunotherapy studies inmore homogeneous and perhaps less advanced cancer settings.One obvious direction is the use of this vaccine in combinationwith anti–PD-1/PD-L1 checkpoint inhibitor mAbs in patientswith so-called "cold tumors." Other settings may involve the useof this vaccine in the adjuvant setting to attack the metastaticprocess, in combination with erlotinib in patients with EGFR-mutated NSCLC, or in combination with immune modulators orinhibitors of immunosuppressive entities.
Disclosure of Potential Conflicts of InterestC.R. Heery is an employee of Bavarian Nordic. No potential conflicts of
interest were disclosed by the other authors.
Authors' ContributionsConception and design: C.R. Heery, C. Palena, W. Dahut, J. Schlom, J.L. GulleyDevelopment of methodology: C.R. Heery, C. Palena, R.N. Donahue,U. Dirmeier, D.H. HamiltonAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): C.R. Heery, C. Palena, S. McMahon, R.N. Donahue,L.M. Lepone, I. Grenga, L. Cordes, W. Dahut, H. Singh, R.A. Madan,R.I. Fernando, D.H. Hamilton, J. Schlom, J.L. GulleyAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): C.R. Heery, C. Palena, R.N. Donahue, J. Mart�e,W. Dahut, R.I. Fernando, J. Schlom, J.L. GulleyWriting, review, and/or revision of the manuscript: C.R. Heery, C. Palena,R.N. Donahue, L. Cordes, W. Dahut, R.A. Madan, J. Schlom, J.L. GulleyAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): C.R. Heery, J.L. GulleyStudy supervision: C.R. Heery, C. Palena, J. Schlom, J.L. GulleyOther (generation of recombinant vaccine construct): U. Dirmeier
Grant SupportThis study was supported by the Intramural Research Program of the Center
for Cancer Research, National Cancer Institute (NCI), NIH, and a CRADAbetween the NCI and Bavarian Nordic.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received April 16, 2017; revised June 11, 2017; accepted August 24, 2017;published OnlineFirst August 30, 2017.
References1. Herrmann BG, Labeit S, Poustka A, King TR, Lehrach H. Cloning of the T
gene required in mesoderm formation in the mouse. Nature 1990;343:617–22.
2. Hamilton DH, Litzinger MT, Fernando RI, Huang B, Palena C.Cancer vaccines targeting the epithelial-mesenchymal transition:tissue distribution of brachyury and other drivers of the mes-enchymal-like phenotype of carcinomas. Semin Oncol 2012;39:358–66.
3. Hamilton DH, Fernando RI, Schlom J, Palena C. Aberrant expressionof the embryonic transcription factor brachyury in human tumorsdetected with a novel rabbit monoclonal antibody. Oncotarget 2015;6:4853–62.
4. Roselli M, Fernando RI, Guadagni F, Spila A, Alessandroni J, Palmirotta R,et al. Brachyury, a driver of the epithelial-mesenchymal transition, isoverexpressed in human lung tumors: an opportunity for novel interven-tions against lung cancer. Clin Cancer Res 2012;18:3868–79.
5. Miettinen M, Wang Z, Lasota J, Heery C, Schlom J, Palena C. Nuclearbrachyury expression is consistent in chordoma, common in germ celltumors and small cell carcinomas, and rare in other carcinomas andsarcomas: an immunohistochemical study of 5229 cases. Am J Surg Pathol2015;39:1305–12.
6. Kilic N, Feldhaus S, Kilic E, Tennstedt P, Wicklein D, Wasielewski R, et al.Brachyury expression predicts poor prognosis at early stages of colorectalcancer. Eur J Cancer 2011;47:1080–5.
Phase I Trial of MVA-Brachyury-TRICOM
www.aacrjournals.org Clin Cancer Res; 23(22) November 15, 2017 6843
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

7. Du R, Wu S, Lv X, Fang H, Wu S, Kang J. Overexpression of brachyurycontributes to tumor metastasis by inducing epithelial-mesenchymaltransition in hepatocellular carcinoma. J Exp Clin Cancer Res 2014;33:105.
8. Pinto F, Pertega-Gomes N, Pereira MS, Vizcaino JR, Monteiro P, Henri-que RM, et al. T-box transcription factor brachyury is associated withprostate cancer progression and aggressiveness. Clin Cancer Res 2014;20:4949–61.
9. Palena C, Roselli M, Litzinger MT, Ferroni P, Costarelli L, Spila A, et al.Overexpression of the EMT driver brachyury in breast carcinomas: associ-ation with poor prognosis. J Natl Cancer Inst 2014;106.
10. HamiltonDH,RoselliM, Ferroni P,Costarelli L,Cavaliere F, TaffuriM, et al.Brachyury, a vaccine target, is overexpressed in triple-negative breast cancer.Endocr Relat Cancer 2016;23:783–96.
11. Tirabosco R, Mangham DC, Rosenberg AE, Vujovic S, Bousdras K, Pizzo-litto S, et al. Brachyury expression in extra-axial skeletal and soft tissuechordomas: a marker that distinguishes chordoma from mixed tumor/myoepithelioma/parachordoma in soft tissue. Am J Surg Pathol 2008;32:572–80.
12. Vujovic S, Henderson S, Presneau N, Odell E, Jacques TS, Tirabosco R, et al.Brachyury, a crucial regulator of notochordal development, is a novelbiomarker for chordomas. J Pathol 2006;209:157–65.
13. Thiery JP.Epithelial-mesenchymal transitions in tumour progression. NatRev Cancer 2002;2:442–54.
14. Fernando RI, Litzinger M, Trono P, Hamilton DH, Schlom J, Palena C. TheT-box transcription factor Brachyury promotes epithelial-mesenchymaltransition in human tumor cells. J Clin Invest 2010;120:533–44.
15. Savagner P.Epithelial-mesenchymal transitions: from cell plasticity toconcept elasticity. Curr Top Dev Biol 2015;112:273–300.
16. Nieto MA, Cano A. The epithelial-mesenchymal transition under control:global programs to regulate epithelial plasticity. Semin Cancer Biol2012;22:361–8.
17. Huang B, Cohen JR, Fernando RI, Hamilton DH, Litzinger MT, Hodge JW,et al. The embryonic transcription factor Brachyury blocks cell cycleprogression and mediates tumor resistance to conventional antitumortherapies. Cell Death Dis 2013;4:e682.
18. Larocca C, Cohen JR, Fernando RI, Huang B, Hamilton DH, Palena C. Anautocrine loop between TGF-beta1 and the transcription factor brachyurycontrols the transition of human carcinoma cells into a mesenchymalphenotype. Mol Cancer Ther 2013;12:1805–15.
19. Hamilton DH, Huang B, Fernando RI, Tsang KY, Palena C. WEE1 inhibi-tion alleviates resistance to immune attack of tumor cells undergoingepithelial-mesenchymal transition. Cancer Res 2014;74:2510–9.
20. David JM, Hamilton DH, Palena C. MUC1 upregulation promotesimmune resistance in tumor cells undergoing brachyury-mediated epithe-lial-mesenchymal transition. Oncoimmunology 2016;5:e1117738.
21. Haro A, Yano T, KohnoM, Yoshida T, Koga T, Okamoto T, et al. Expressionof Brachyury gene is a significant prognostic factor for primary lungcarcinoma. Ann Surg Oncol 2013;20:S509–16.
22. Pinto F, Campanella NC, Abrahao-Machado LF, Scapulatempo-Neto C, deOliveira AT, BritoMJ, et al. The embryonic brachyury transcription factor isa novel biomarker of GIST aggressiveness and poor survival. Gastric Cancer2016;19:651–9.
23. Palena C, Polev DE, Tsang KY, Fernando RI, Litzinger M, Krukovskaya LL,et al. The human T-box mesodermal transcription factor Brachyury is acandidate target for T-cell-mediated cancer immunotherapy. Clin CancerRes 2007;13:2471–8.
24. Tucker JA, Jochems C, Boyerinas B, Fallon J, Greiner JW, Palena C, et al.Identification and characterization of a cytotoxic T-lymphocyte agonistepitope of brachyury, a transcription factor involved in epithelial tomesenchymal transition and metastasis. Cancer Immunol Immunother2014;63:1307–17.
25. Madan RA, Bilusic M, Heery C, Schlom J, Gulley JL. Clinical evaluationof TRICOM vector therapeutic cancer vaccines. Semin Oncol 2012;39:296–304.
26. Gulley JL, Arlen PM, Tsang KY, Yokokawa J, Palena C, Poole DJ, et al. Pilotstudy of vaccination with recombinant CEA-MUC-1-TRICOM poxviral-based vaccines in patients with metastatic carcinoma. Clin Cancer Res2008;14:3060–9.
27. Mohebtash M, Tsang KY, Madan RA, Huen NY, Poole DJ, Jochems C,et al. A pilot study of MUC-1/CEA/TRICOM poxviral-based vaccine in
patients with metastatic breast and ovarian cancer. Clin Cancer Res2011;17:7164–73.
28. Madan RA, Mohebtash M, Arlen PM, Vergati M, Rauckhorst M, SteinbergSM, et al. Ipilimumab and a poxviral vaccine targeting prostate-specificantigen in metastatic castration-resistant prostate cancer: a phase 1 dose-escalation trial. Lancet Oncol 2012;13:501–8.
29. Heery CR, Madan RA, Stein MN, Stadler WM, Di Paola RS, Rauckhorst M,et al. Samarium-153-EDTMP (Quadramet(R)) with or without vaccine inmetastatic castration-resistant prostate cancer: a randomized phase 2 trial.Oncotarget 2016;7:69014–23.
30. Kantoff PW, Schuetz TJ, Blumenstein BA,Glode LM, BilhartzDL,WyandM,et al. Overall survival analysis of a phase II randomized controlled trial of aPoxviral-based PSA-targeted immunotherapy in metastatic castration-resistant prostate cancer. J Clin Oncol 2010;28:1099–105.
31. Gulley JL, Arlen PM, Madan RA, Tsang KY, Pazdur MP, Skarupa L, et al.Immunologic and prognostic factors associated with overall survivalemploying a poxviral-based PSA vaccine in metastatic castrate-resistantprostate cancer. Cancer Immunol Immunother 2010;59:663–74.
32. Arlen PM, Skarupa L, Pazdur M, SeetharamM, Tsang KY, Grosenbach DW,et al. Clinical safety of a viral vector based prostate cancer vaccine strategy.J Urol 2007;178:1515–20.
33. Moorthy VS, McConkey S, Roberts M, Gothard P, Arulanantham N,Degano P, et al. Safety of DNA andmodified vaccinia virus Ankara vaccinesagainst liver-stage P. falciparum malaria in non-immune volunteers.Vaccine 2003;21:1995–2002.
34. AmatoRJ,HawkinsRE, KaufmanHL, Thompson JA, TomczakP, Szczylik C,et al. Vaccination of metastatic renal cancer patients with MVA-5T4: arandomized, double-blind, placebo-controlled phase III study. Clin Can-cer Res 2010;16:5539–47.
35. Ramlau R, Quoix E, Rolski J, Pless M, Lena H, Levy E, et al. A phase IIstudy of Tg4010 (Mva-Muc1-Il2) in association with chemotherapy inpatients with stage III/IV Non-small cell lung cancer. J Thorac Oncol2008;3:735–44.
36. Scholl SM, Balloul JM, Le Goc G, Bizouarne N, Schatz C, Kieny MP, et al.Recombinant vaccinia virus encoding human MUC1 and IL2 as immu-notherapy in patients with breast cancer. J Immunother 2000;23:570–80.
37. von Sonnenburg F, Perona P, Darsow U, Ring J, von Krempelhuber A,Vollmar J, et al. Safety and immunogenicity ofmodified vaccinia Ankara asa smallpox vaccine in people with atopic dermatitis. Vaccine 2014;32:5696–702.
38. Zitzmann-Roth EM, von Sonnenburg F, de la Motte S, Arndtz-WiedemannN, vonKrempelhuber A,UeblerN, et al. Cardiac safety ofmodified vacciniaankara for vaccination against smallpox in a young, healthy study popu-lation. PLoS One 2015;10:e0122653.
39. Kwilas AR, Ardiani A, Dirmeier U, Wottawah C, Schlom J, Hodge JW. Apoxviral-based cancer vaccine the transcription factor twist inhibits pri-mary tumor growth and metastases in a model of metastatic breast cancerand improves survival in a spontaneous prostate cancermodel. Oncotarget2015;6:28194–210.
40. Kwilas AR, Ardiani A, Gameiro SR, Richards J, Hall AB, Hodge JW.Androgen deprivation therapy sensitizes triple negative breast cancer cellsto immune-mediated lysis through androgen receptor independent mod-ulation of osteoprotegerin. Oncotarget 2016;7:23498–511.
41. Fernando RI, Hamilton DH, Dominguez C, David JM, McCampbell KK,Palena C. IL-8 signaling is involved in resistance of lung carcinoma cells toerlotinib. Oncotarget 2016;7:42031–44.
42. Dominguez C, Tsang KY, Palena C. Short-term EGFR blockade enhancesimmune-mediated cytotoxicity of EGFRmutant lung cancer cells: rationalefor combination therapies. Cell Death Dis 2016;7:e2380.
43. Hamilton DH, Griner LM, Keller JM, Hu X, Southall N, Marugan J, et al.Targeting estrogen receptor signaling with fulvestrant enhances immuneand chemotherapy-mediated cytotoxicity of human lung cancer. ClinCancer Res 2016;22:6204–16.
44. Hodge JW, Sabzevari H, Yafal AG, Gritz L, Lorenz MG, Schlom J. A triad ofcostimulatory molecules synergize to amplify T-cell activation. Cancer Res1999;59:5800–7.
45. Heery CR, Singh BH, Rauckhorst M, Marte JL, Donahue RN, Grenga I, et al.Phase I trial of a yeast-based therapeutic cancer vaccine (GI-6301) targetingthe transcription factor brachyury. Cancer Immunol Res 2015;3:1248–56.
46. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al.Erlotinib versus standard chemotherapy as first-line treatment for
Heery et al.
Clin Cancer Res; 23(22) November 15, 2017 Clinical Cancer Research6844
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

European patients with advanced EGFR mutation-positive non-small-celllung cancer (EURTAC): a multicentre, open-label, randomised phase 3trial. Lancet Oncol 2012;13:239–46.
47. Rubio V, Stuge TB, Singh N, Betts MR, Weber JS, Roederer M, et al. Ex vivoidentification, isolation and analysis of tumor-cytolytic T cells. Nat Med2003;9:1377–82.
48. Yu M, Bardia A, Wittner BS, Stott SL, Smas ME, Ting DT, et al. Circulatingbreast tumor cells exhibit dynamic changes in epithelial andmesenchymalcomposition. Science 2013;339:580–4.
49. Hamilton DH, David JM, Dominguez C, Palena C. Development ofcancer vaccines targeting brachyury, a transcription factor associatedwith tumor epithelial-mesenchymal transition. Cells Tissues Organs2017;203:128–38.
50. Bilusic M, Heery CR, Arlen PM, Rauckhorst M, Apelian D, Tsang KY, et al.Phase I trial of a recombinant yeast-CEA vaccine (GI-6207) in adults withmetastatic CEA-expressing carcinoma. Cancer Immunol Immunother2014;63:225–34.
51. Hodge JW, PooleDJ, AartsWM,Gomez Yafal A,Gritz L, Schlom J.Modifiedvaccinia virus ankara recombinants are as potent as vaccinia recombinantsin diversified prime and boost vaccine regimens to elicit therapeuticantitumor responses. Cancer Res 2003;63:7942–9.
52. Earl PL, Americo JL, Wyatt LS, Eller LA, Whitbeck JC, Cohen GH, et al.Immunogenicity of a highly attenuated MVA smallpox vaccine and pro-tection against monkeypox. Nature 2004;428:182–5.
53. Meyer H.Summary report on first, second and third generation smallpoxvaccines. Geneva: World Health Organisation; 2013. p. 1–33.
54. Hodge JW, McLaughlin JP, Kantor JA, Schlom J. Diversified prime andboost protocols using recombinant vaccinia virus and recombinant non-replicating avian pox virus to enhance T-cell immunity and antitumorresponses. Vaccine 1997;15:759–68.
55. Hodge JW, Higgins J, Schlom J. Harnessing the unique local immu-nostimulatory properties of modified vaccinia Ankara (MVA) virus togenerate superior tumor-specific immune responses and antitumoractivity in a diversified prime and boost vaccine regimen. Vaccine2009;27:4475–82.
56. Marshall JL, Hoyer RJ, Toomey MA, Faraguna K, Chang P, Richmond E,et al. Phase I study in advanced cancer patients of a diversified prime-and-boost vaccination protocol using recombinant vaccinia virus and recom-binant nonreplicating avipox virus to elicit anti-carcinoembryonic antigenimmune responses. J Clin Oncol 2000;18:3964–73.
57. KaufmanHL,WangW,Manola J, DiPaola RS, Ko YJ, SweeneyC, et al. PhaseII randomized study of vaccine treatment of advanced prostate cancer(E7897): a trial of the Eastern Cooperative Oncology Group. J Clin Oncol2004;22:2122–32.
58. Boehm AL, Higgins J, Franzusoff A, Schlom J, Hodge JW. Concurrentvaccination with two distinct vaccine platforms targeting the same antigengenerates phenotypically and functionally distinct T-cell populations.Cancer Immunol Immunother 2010;59:397–408.
www.aacrjournals.org Clin Cancer Res; 23(22) November 15, 2017 6845
Phase I Trial of MVA-Brachyury-TRICOM
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087

2017;23:6833-6845. Published OnlineFirst August 30, 2017.Clin Cancer Res Christopher R. Heery, Claudia Palena, Sheri McMahon, et al. Against the Transcription Factor BrachyuryPhase I Study of a Poxviral TRICOM-Based Vaccine Directed
Updated version
10.1158/1078-0432.CCR-17-1087doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2017/08/30/1078-0432.CCR-17-1087.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/23/22/6833.full#ref-list-1
This article cites 56 articles, 17 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/23/22/6833.full#related-urls
This article has been cited by 5 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/23/22/6833To request permission to re-use all or part of this article, use this link
on March 22, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2017; DOI: 10.1158/1078-0432.CCR-17-1087





![Tricom India LtdCorporate Office: COMPANY BACKGROUND Tricom House, Gandhi Estate, Tricom India Ltd [Tricom Finance Ltd (TFL)], promoted by Mr W M Bhagat, Mr V Srinivas and Associates](https://static.fdocuments.net/doc/165x107/5ffd69bd12546b4a865f5f48/tricom-india-ltd-corporate-office-company-background-tricom-house-gandhi-estate.jpg)