Phase 1 First-in-Human Trial of AMV564, a Bivalent ... · 0.5 – 50 mcg. 100 mcg. 150 mcg. 200...
15
Phase 1 First-in-Human Trial of AMV564, a Bivalent Bispecific (2:2) CD33/CD3 T-Cell Engager, in Patients with Relapsed/Refractory Acute Myeloid Leukemia (AML) Peter Westervelt, MD, PhD 1 , Jorge E. Cortes , MD 2 , Jessica K. Altman 3 , Meixiao Long, MD 4 , Vivian G. Oehler, MD 5,6 , Ivana Gojo, MD 7 , Jeanmarie Guenot, PhD 8 , Patrick Chun, MD 8 and Gail J. Roboz, MD 9 1 Division of Oncology, Washington University School of Medicine, Saint Louis, MO; 2 Georgia Cancer Center, Augusta University, Augusta, GA; 3 Northwestern University, Chicago, IL; 4 Division of Hematology, Department of Internal Medicine, Ohio State University Hospital, Columbus, OH; 5 Division of Hematology, Department of Medicine, University of Washington, Seattle, WA; 6 Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA; 7 Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University, Baltimore, MD; 8 Amphivena Therapeutics, Inc, South San Francisco, CA; 9 Division of Hematology and Oncology, Weill Cornell Medical College of Cornell University, New York ASH 61 st Annual Meeting and Exposition December 7-10, 2019. Orlando, FL
Transcript of Phase 1 First-in-Human Trial of AMV564, a Bivalent ... · 0.5 – 50 mcg. 100 mcg. 150 mcg. 200...
Phase 1 First-in-Human Trial of AMV564, a Bivalent Bispecific (2:2) CD33/CD3 T-Cell Engager, in Patients with Relapsed/Refractory
Acute Myeloid Leukemia (AML)
Peter Westervelt, MD, PhD1, Jorge E. Cortes, MD2, Jessica K. Altman3, Meixiao Long, MD4, Vivian G.Oehler, MD5,6, Ivana Gojo, MD7, Jeanmarie Guenot, PhD8, Patrick Chun, MD8 and Gail J. Roboz, MD9
1Division of Oncology, Washington University School of Medicine, Saint Louis, MO; 2Georgia Cancer Center, Augusta University, Augusta, GA;
3Northwestern University, Chicago, IL; 4Division of Hematology, Department of Internal Medicine, Ohio State University Hospital, Columbus, OH;
5Division of Hematology, Department of Medicine, University of Washington, Seattle, WA; 6Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA;
7Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University, Baltimore, MD; 8Amphivena Therapeutics, Inc, South San Francisco, CA;
9Division of Hematology and Oncology, Weill Cornell Medical College of Cornell University, New York
ASH 61st Annual Meeting and ExpositionDecember 7-10, 2019. Orlando, FL
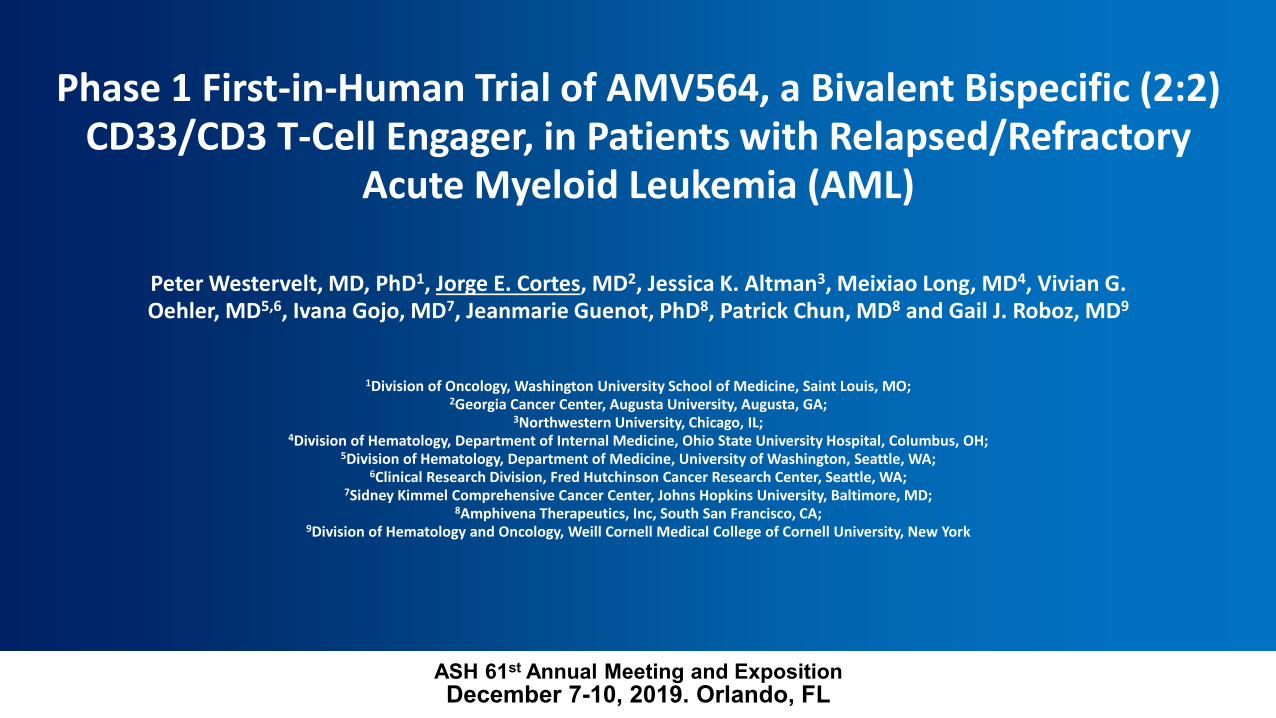
AMV564: A Bivalent, Bispecific CD33/CD3 T-cell Engager
AMV564: Binding Sites & Mechanism of Action
• CD33 Expressed on AML blasts
• EC50 4 - 8 pM for target-dependent killing of AML cell lines
AMV564: Selectivity
2 CD33 Binding Sites
2 CD3 Binding Sites
1Amphivena Therapeutics, Inc. https://amphivena.com/amv564/2Chen X, et al. Induction of myelodysplasia by myeloid-derived suppressor cells. J Clin Invest. 2013;123(11):4595-611.
AMV564Selectivity for CD33-signaling/clustered
Monovalent T-cells engagerscannot distinguish cell types

0.5 – 50 mcg
100 mcg
150 mcg
200 mcg
250 mcg
3+3 DESIGN(14 Days Continuous IV Infusion on a 28 Day cycle)
AMV564-101 Phase 1 Clinical Study Design: Relapsed/Refractory AML
450 mcg
300 mcg
Key Eligibility Criteria • Age ≥ 18 years• Relapsed or refractory
disease• 1-3 prior induction/salvage
regimens • Secondary AML • ECOG 0-2• Normal renal/hepatic
function
Status at cutoff date of 11/1/2019• 41 patients dosed• 11 dose cohorts
explored to date• Lead-in dosing for
450mcg cohort: 15mcg 30mcg 100mcg150mcg 300mcg target dose

AMV564-101 Phase 1 Clinical Study Design: Relapsed/Refractory AML
• Key Objectives− To characterize the safety and tolerability, including dose-limiting toxicity (DLT), of
AMV564 administered by CIV infusion− To identify the maximum tolerated dose (MTD) and recommended Phase 2 dose
(RP2D) of AMV564− To evaluate preliminary efficacy of AMV564 administered at the RP2D
• Additional objectives− To characterize the pharmacokinetics (PK), pharmacodynamics (PD), and
immunogenicity of AMV564 when administered by CIV infusion− To evaluate predictive biomarkers of response or resistance to AMV564 − To investigate the immunoregulatory activity of AMV564, including measures of T-
cell function and profiling of T-cell subpopulations
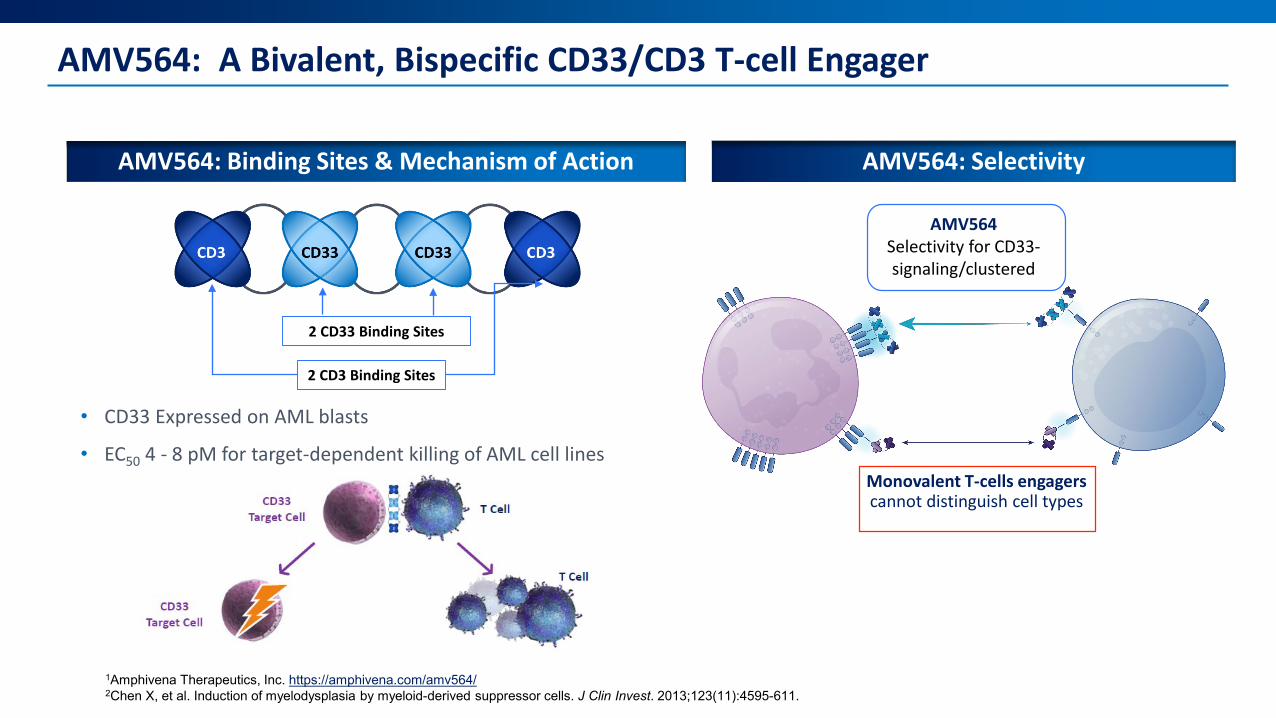
AMV564-101: DemographicsPatient Demographics N=41Median age, year (range), n (%)Age >65
71.3 (24.2 to 84.6)28 (68.3)
ECOG score, n (%)012
7 (17.1)29 (70.7)5 (12.2)
AML Classification, n (%)AML with Myelodysplasia Related ChangesAML, Not Otherwise SpecifiedAML with Recurrent Genetic AbnormalitiesTherapy Related Myeloid Neoplasm
20 (48.8)12 (29.3)7 (17.1)2 (4.9)
Number of prior AML regimen, n (%)a
123 >3
13 (31.7)12 (30.0)9 (22.5)6 (15.0)
Prior AML TherapyAnthracyline based therapyHypomethylating agent therapyPrior high dose cytarabine (≥1000 mg/m2)a, n (%)
20 (50.0)25 (62.5)13 (31.7)
Prior allogeneic transplant, n (%) 3 (7.3)MRC cytogenetic risk group, n (%)UnfavorableIntermediateFavorable
22 (53.7)17 (41.5)1 (2.4)
aN=40

AMV564-101 Treatment-Emergent Adverse Events (> 20% Patients) and Grade 3+ AEs
Adverse Event, n (%) Total Safety Evaluable, (N=41)TEAE > 20% Grade 3+
Pyrexia 20 (48.8) 1 (2.4)Nausea 19 (46.3)Oedema peripheral 18 (43.9) 1 (2.4)Cytokine release syndrome 16 (39.0)Headache 15 (36.6) 1 (2.4)Diarrhoea 14 (34.1) 3 (7.3)Cough 14 (34.1)Febrile neutropenia 13 (31.7) 11 (26.8)Fatigue 12 (29.3)Constipation 12 (29.3)Vomiting 12 (29.3)Hypokalaemia 10 (24.4) 2 (4.9)Hypotension 10 (24.4) 3 (7.3)Rash 9 (22.0)Hypomagnesaemia 9 (22.0)Insomnia 9 (22.0)
• No Dose-Limiting Toxicity through 450 mcg/day• Infusion related Adverse Events (n=2; Grade 2)• AEs leading to discontinuation (n=2): septic shock (n=1; 150 mcg/d) and myocarditis (n=1; 250 mcg/d)
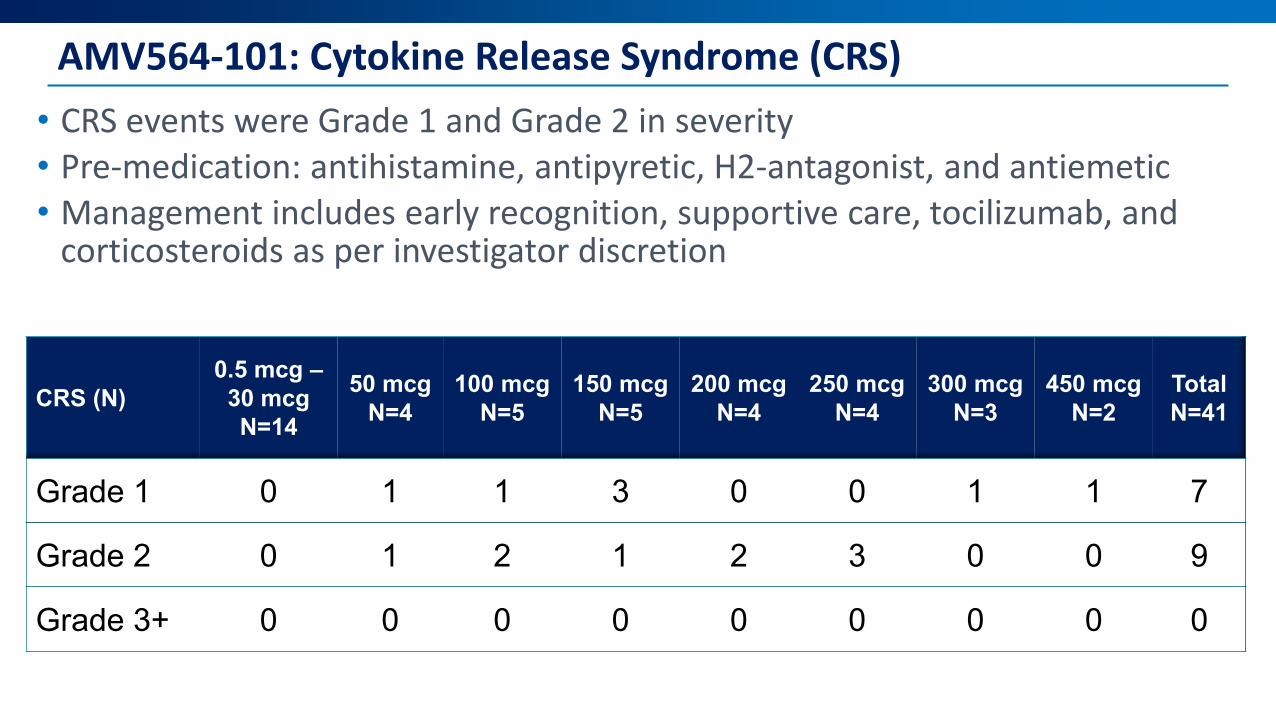
AMV564-101: Cytokine Release Syndrome (CRS)• CRS events were Grade 1 and Grade 2 in severity• Pre-medication: antihistamine, antipyretic, H2-antagonist, and antiemetic• Management includes early recognition, supportive care, tocilizumab, and
corticosteroids as per investigator discretion
CRS (N)0.5 mcg –
30 mcgN=14
50 mcgN=4
100 mcgN=5
150 mcgN=5
200 mcgN=4
250 mcgN=4
300 mcgN=3
450 mcgN=2
TotalN=41
Grade 1 0 1 1 3 0 0 1 1 7
Grade 2 0 1 2 1 2 3 0 0 9
Grade 3+ 0 0 0 0 0 0 0 0 0
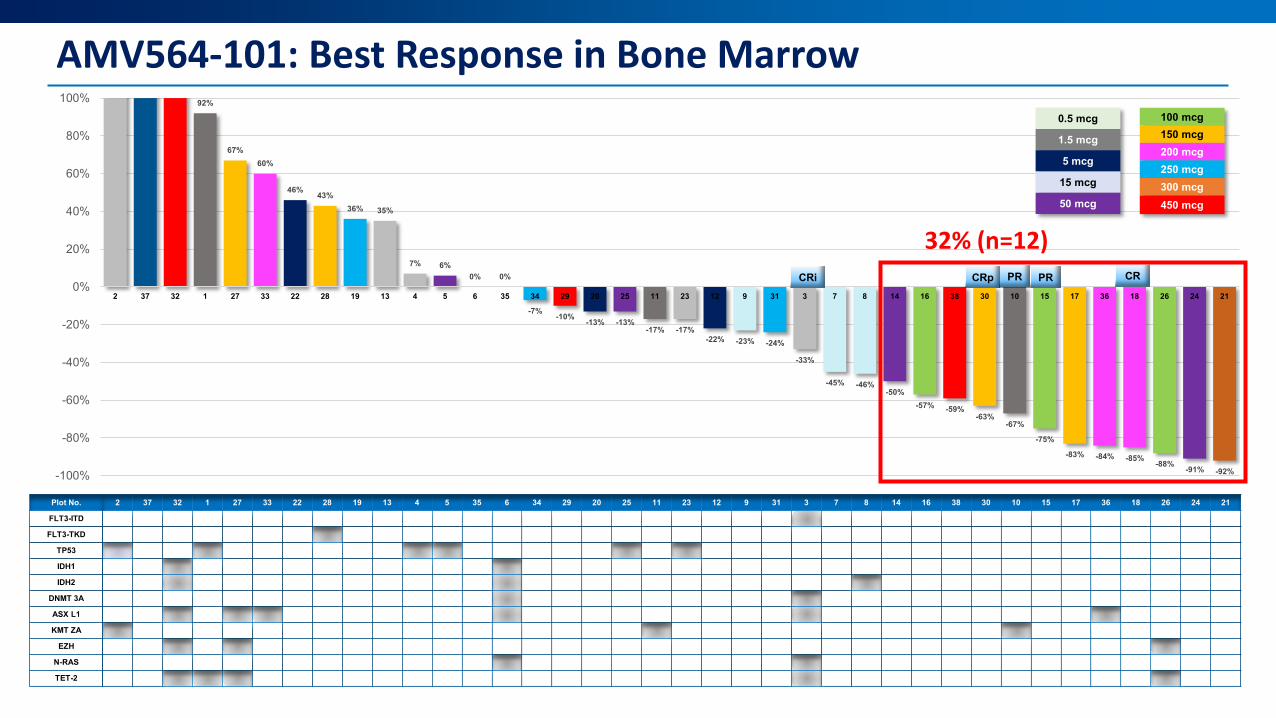
AMV564-101: Best Response in Bone Marrow
2 37 32 1 27 33 22 28 19 13 4 5 35 6 34 29 20 25 11 23 12 9 31 3 7 8 14 16 38 30 10 15 17 36 18 26 24 21
92%
67%60%
46% 43%36% 35%
7% 6%0% 0%
-7% -10% -13% -13%-17% -17%
-22% -23% -24%
-33%
-45% -46%-50%
-57% -59%-63%
-67%
-75%
-83% -84% -85% -88% -91% -92%-100%
-80%
-60%
-40%
-20%
0%
20%
40%
60%
80%
100%
2 37 32 1 27 33 22 28 19 13 4 5 6 35 34 29 20 25 11 23 12 9 31 3 7 8 14 16 38 30 10 15 17 36 18 26 24 21
CRi CRp PR CRPR
0.5 mcg
1.5 mcg
5 mcg
15 mcg
50 mcg
100 mcg150 mcg200 mcg250 mcg300 mcg450 mcg
Plot No.
FLT3-ITD
FLT3-TKD
TP53
IDH1
IDH2
DNMT 3A
ASX L1
KMT ZA
EZH
N-RAS
TET-2
32% (n=12)
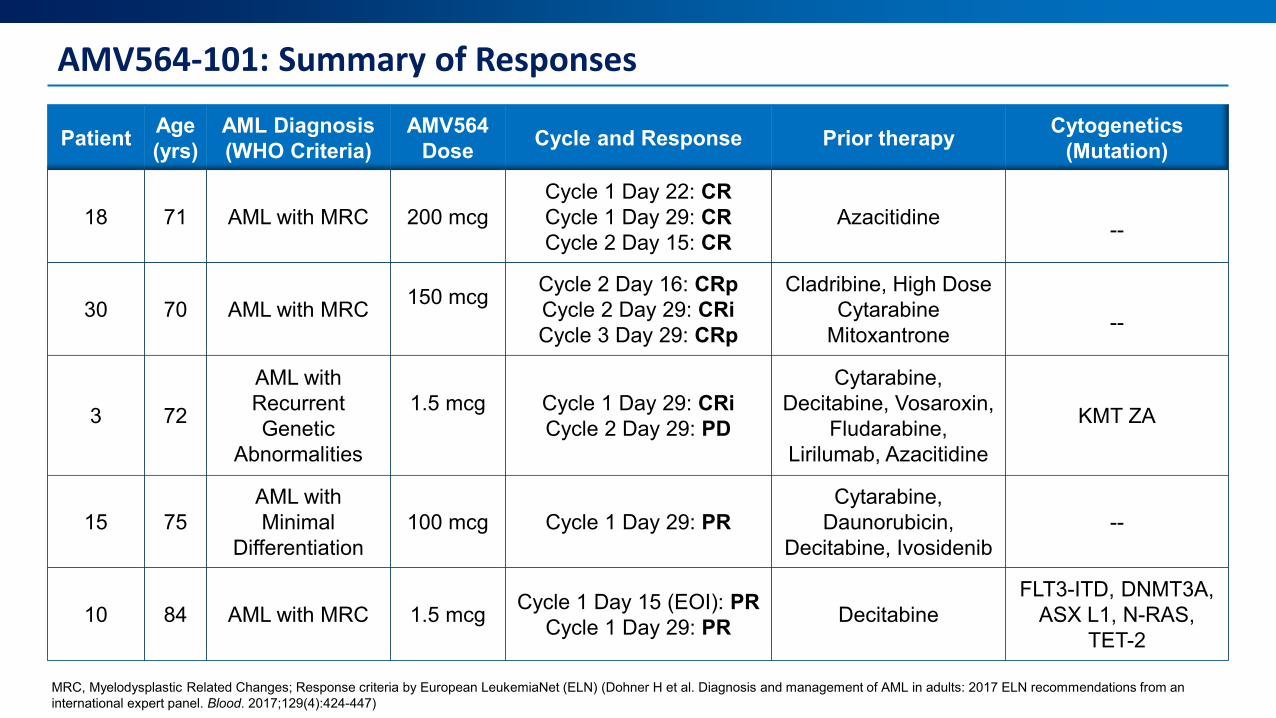
AMV564-101: Summary of Responses
Patient Age (yrs)
AML Diagnosis (WHO Criteria)
AMV564 Dose Cycle and Response Prior therapy Cytogenetics
(Mutation)
18 71 AML with MRC 200 mcgCycle 1 Day 22: CRCycle 1 Day 29: CRCycle 2 Day 15: CR
Azacitidine --
30 70 AML with MRC 150 mcg Cycle 2 Day 16: CRpCycle 2 Day 29: CRiCycle 3 Day 29: CRp
Cladribine, High Dose Cytarabine
Mitoxantrone --
3 72
AML with Recurrent Genetic
Abnormalities
1.5 mcg Cycle 1 Day 29: CRiCycle 2 Day 29: PD
Cytarabine, Decitabine, Vosaroxin,
Fludarabine, Lirilumab, Azacitidine
KMT ZA
15 75AML with Minimal
Differentiation100 mcg Cycle 1 Day 29: PR
Cytarabine, Daunorubicin,
Decitabine, Ivosidenib--
10 84 AML with MRC 1.5 mcg Cycle 1 Day 15 (EOI): PRCycle 1 Day 29: PR Decitabine
FLT3-ITD, DNMT3A, ASX L1, N-RAS,
TET-2
MRC, Myelodysplastic Related Changes; Response criteria by European LeukemiaNet (ELN) (Dohner H et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424-447)
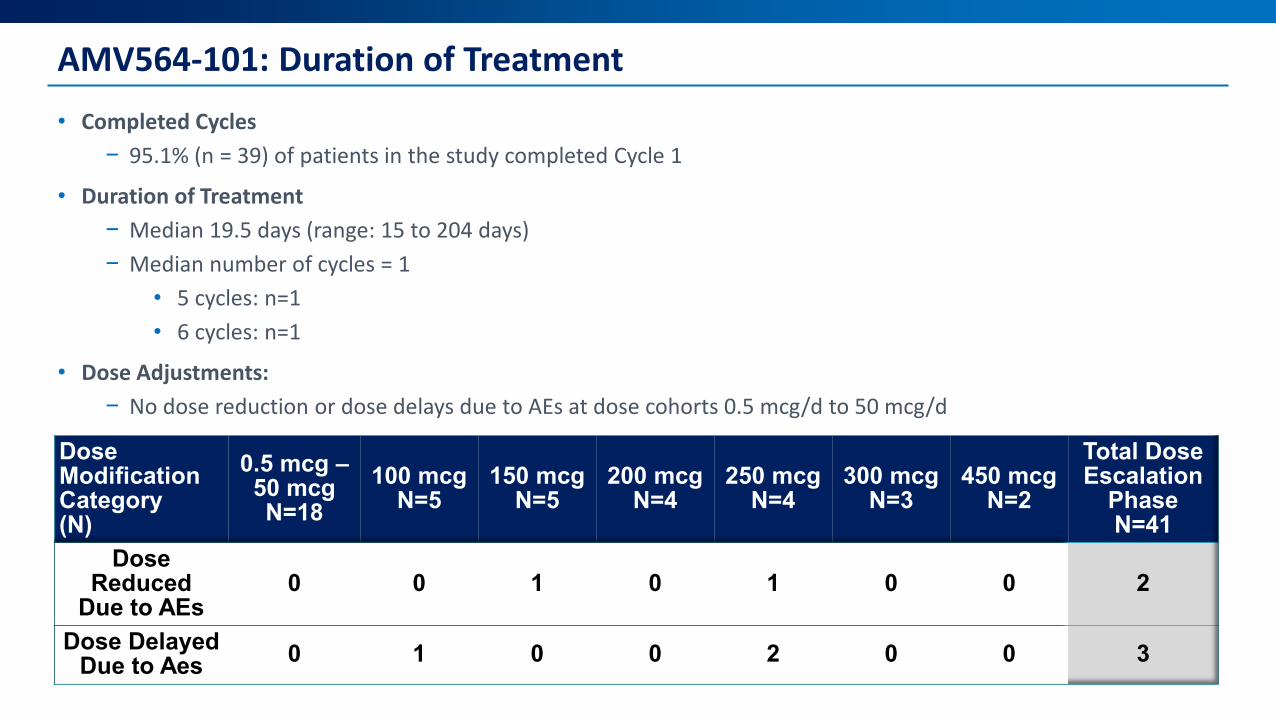
AMV564-101: Duration of Treatment• Completed Cycles
− 95.1% (n = 39) of patients in the study completed Cycle 1
• Duration of Treatment− Median 19.5 days (range: 15 to 204 days)− Median number of cycles = 1
• 5 cycles: n=1 • 6 cycles: n=1
• Dose Adjustments: − No dose reduction or dose delays due to AEs at dose cohorts 0.5 mcg/d to 50 mcg/d
Dose Modification Category(N)
0.5 mcg –50 mcgN=18
100 mcgN=5
150 mcgN=5
200 mcgN=4
250 mcgN=4
300 mcgN=3
450 mcgN=2
Total Dose Escalation
Phase N=41
Dose Reduced
Due to AEs0 0 1 0 1 0 0 2
Dose Delayed Due to Aes 0 1 0 0 2 0 0 3
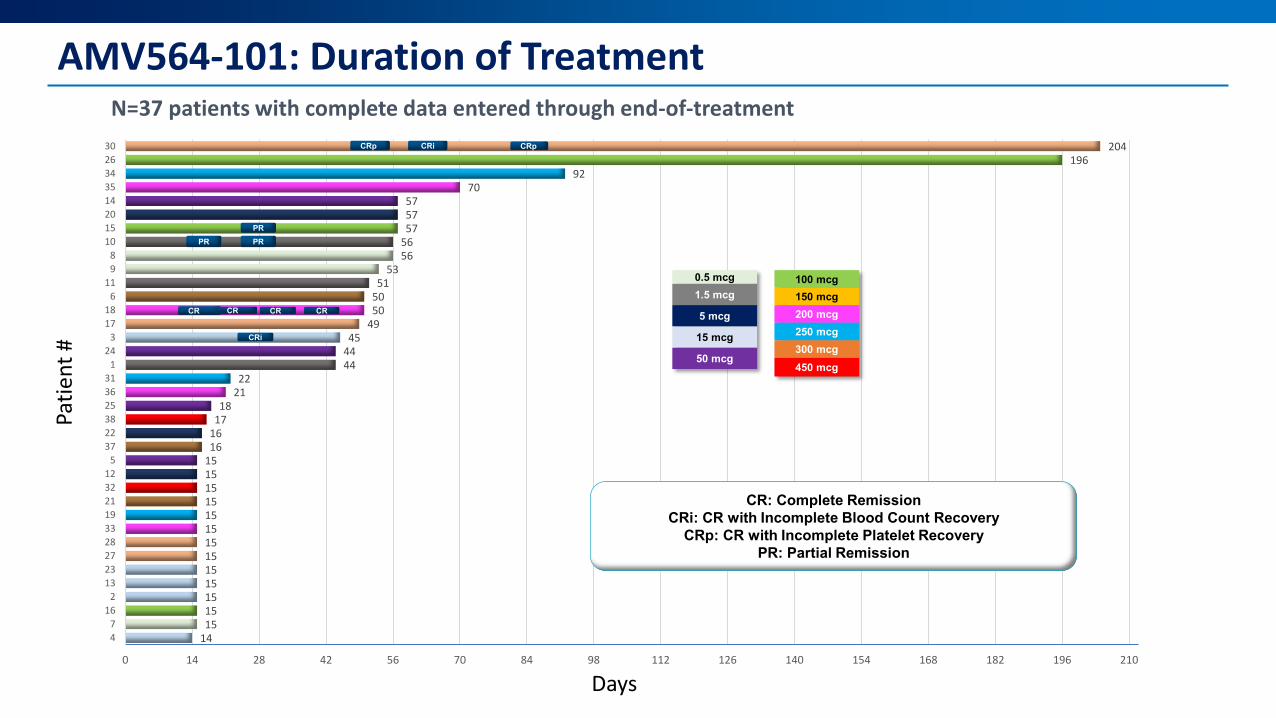
AMV564-101: Duration of Treatment
141515151515151515151515151516161718
2122
444445
49505051
535656575757
7092
196204
0 14 28 42 56 70 84 98 112 126 140 154 168 182 196 210
47
162
132327283319213212
5372238253631
124
31718
611
98
1015201435342630
CR: Complete RemissionCRi: CR with Incomplete Blood Count Recovery
CRp: CR with Incomplete Platelet RecoveryPR: Partial Remission
0.5 mcg1.5 mcg
5 mcg
15 mcg
50 mcg
100 mcg150 mcg200 mcg250 mcg300 mcg450 mcg
CRp CRi CRp
PR PRPR
CR CRCR CR
CRi
N=37 patients with complete data entered through end-of-treatment
Days
Patie
nt #
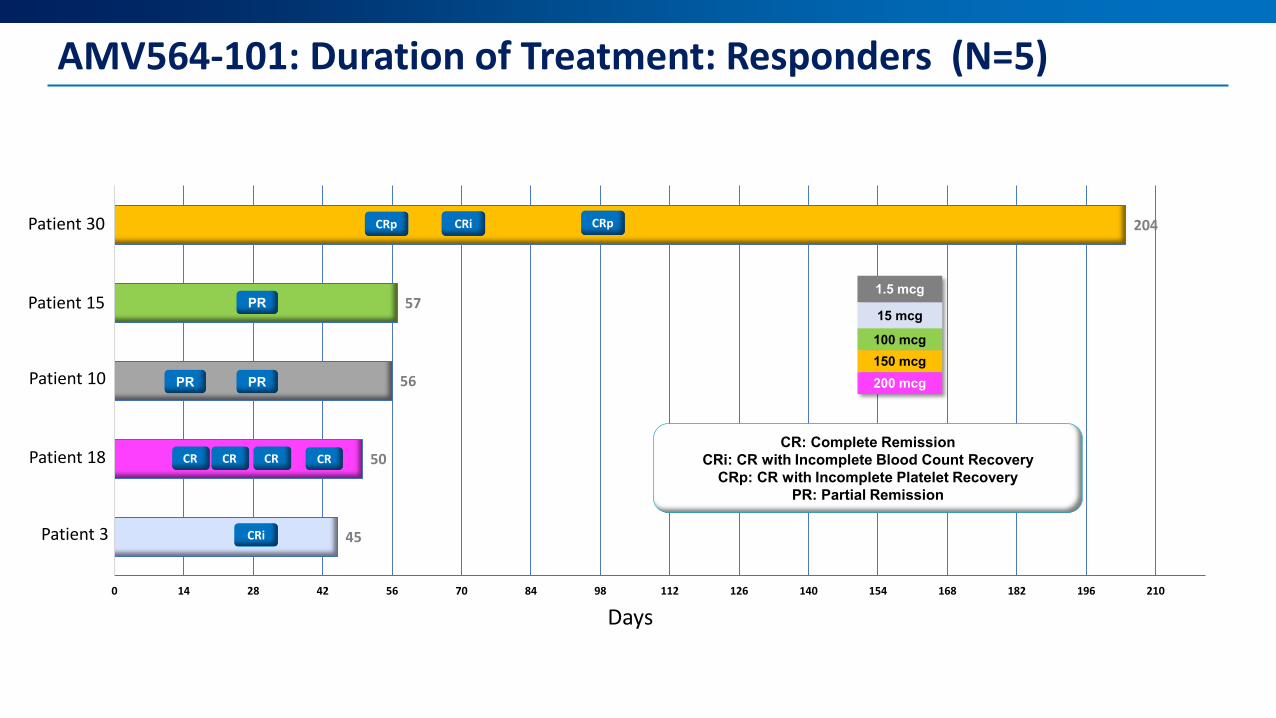
AMV564-101: Duration of Treatment: Responders (N=5)
45
50
56
57
204
0 14 28 42 56 70 84 98 112 126 140 154 168 182 196 210
No. 3
No. 18
No. 10
No. 15
No. 30
CR CRCR CR
CRi
CRp CRi CRp
PR PR
1.5 mcg
15 mcg
100 mcg150 mcg200 mcg
CR: Complete RemissionCRi: CR with Incomplete Blood Count Recovery
CRp: CR with Incomplete Platelet RecoveryPR: Partial Remission
PRPatient 15
Patient 10
Patient 18
Patient 3
Patient 30
Days
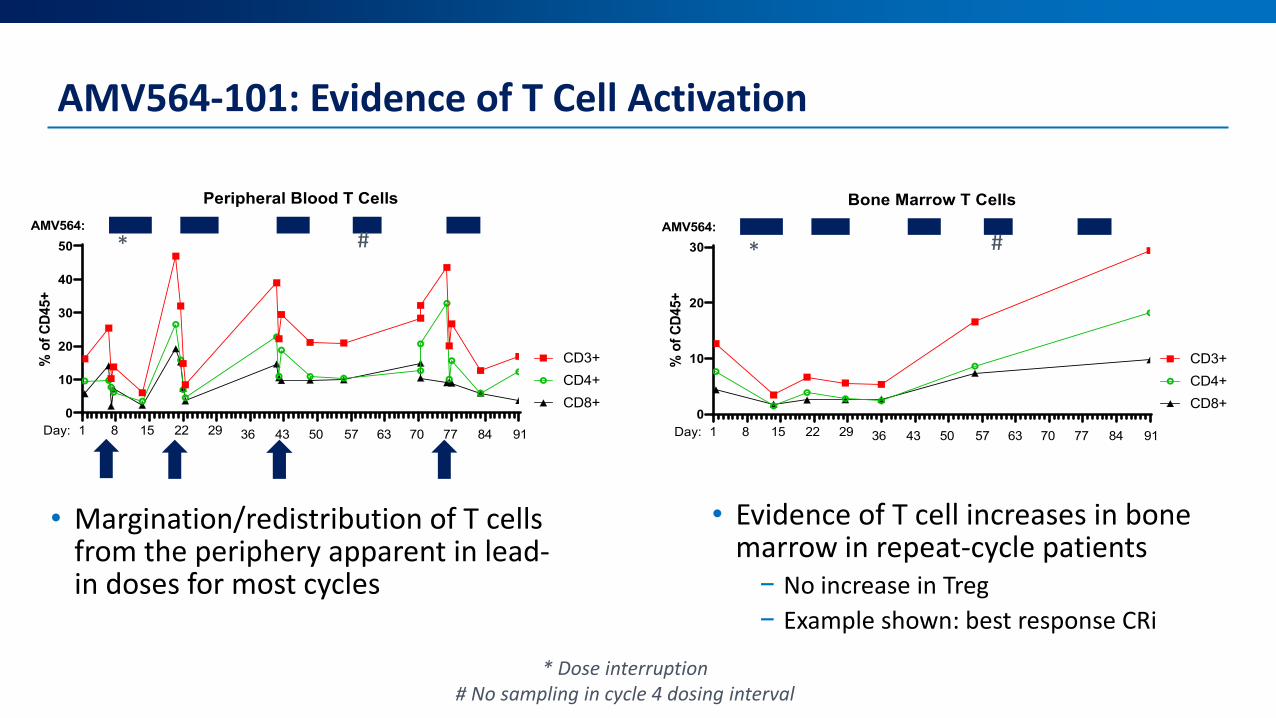
AMV564-101: Evidence of T Cell Activation
• Margination/redistribution of T cells from the periphery apparent in lead-in doses for most cycles
* Dose interruption# No sampling in cycle 4 dosing interval
0
10
20
30
40
50
Peripheral Blood T Cells
% o
f CD4
5+
CD3+CD4+CD8+
AMV564:
Day: 1 8 15 22 29 36 43 50 57 63 70 77 84 91
* #
0
10
20
30
Bone Marrow T Cells
% o
f CD4
5+
CD3+CD4+CD8+
AMV564:
Day: 1 8 15 22 29 36 43 50 57 63 70 77 84 91
* #
• Evidence of T cell increases in bone marrow in repeat-cycle patients
− No increase in Treg− Example shown: best response CRi

AMV564-101: Conclusions and Future Directions
• AMV564 administered as continuous IV infusion is safe and well-tolerated at doses up to 450 mcg/day in heavily pre-treated relapsed/refractory AML patients
• No Dose-Limiting Toxicities • No Grade 3+ CRS• Low incidence of discontinuation due adverse events• Early evidence of clinical activity• AMV564 activates T-cells and shows anti-leukemic blast activity• Subcutaneous and chronic dosing of AMV564 are being explored
in other clinical trials
Acknowledgments
• Patients and their families
• Investigators, study teams, and site personnel