
Pharmacy Quality Assurance Commission Quality Assurance Commission . ... professional publications...
39
Pharmacy Quality Assurance Commission Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Introduction: (introduction added) • This checklist includes the reported “principal competencies, conditions, practices, and quality assurance that are required” (“shalls”) in U.S. Pharmacopeial (USP) <797>. • This checklist is designed to be a tool to guide and aid you to assess your compliance with USP <797>. • At the end of the checklist, there is a section specifically addresses isolators which includes USP <797> requirements and <800> recommendations. • The language provided in this checklist, at times, does not include all of the specific language communicated in USP <797>, if there is a need for further understanding of requirement language, please refer to USP <797> for additional language. • Department of Health Office of Inspection and Investigations is available to assist you with interpreting these requirements, and assist your understanding the compliance with USP <797>. • The Pharmacy Quality Assurance Commission recognizes that USP <797> and <800> are currently being revised, and recommends your pharmacy to keep abreast of the any developments and proposals with the revision, specifically if remodeling your facility. For this information, please visit the U.S. Pharmacopeial (USP) website- http://www.usp.org/usp-healthcare-professionals/compounding Notes Key: • Identified changes in comparison of template document-Alabama State Board of Pharmacy USP <797> Compliance Self-Assessment Form- (deletions/additions/moved items), research, or questions • Items that need to be reviewed Pharmacy Quality Assurance Commission 1 2/19/2016 (Draft)
Transcript of Pharmacy Quality Assurance Commission Quality Assurance Commission . ... professional publications...

Pharmacy Quality Assurance Commission Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist
Introduction: (introduction added)
• This checklist includes the reported “principal competencies, conditions, practices, and quality assurance that are required” (“shalls”) in U.S. Pharmacopeial (USP) <797>.
• This checklist is designed to be a tool to guide and aid you to assess your compliance with USP <797>.
• At the end of the checklist, there is a section specifically addresses isolators which includes USP <797> requirements and <800> recommendations.
• The language provided in this checklist, at times, does not include all of the specific language communicated in USP <797>, if there is a need for further understanding of requirement language, please refer to USP <797> for additional language.
• Department of Health Office of Inspection and Investigations is available to assist you with interpreting these requirements, and
assist your understanding the compliance with USP <797>.
• The Pharmacy Quality Assurance Commission recognizes that USP <797> and <800> are currently being revised, and recommends your pharmacy to keep abreast of the any developments and proposals with the revision, specifically if remodeling your facility. For this information, please visit the U.S. Pharmacopeial (USP) website- http://www.usp.org/usp-healthcare-professionals/compounding
Notes Key: • Identified changes in comparison of template document-Alabama State Board of Pharmacy USP
<797> Compliance Self-Assessment Form- (deletions/additions/moved items), research, or questions
• Items that need to be reviewed Pharmacy Quality Assurance Commission 1 2/19/2016 (Draft)
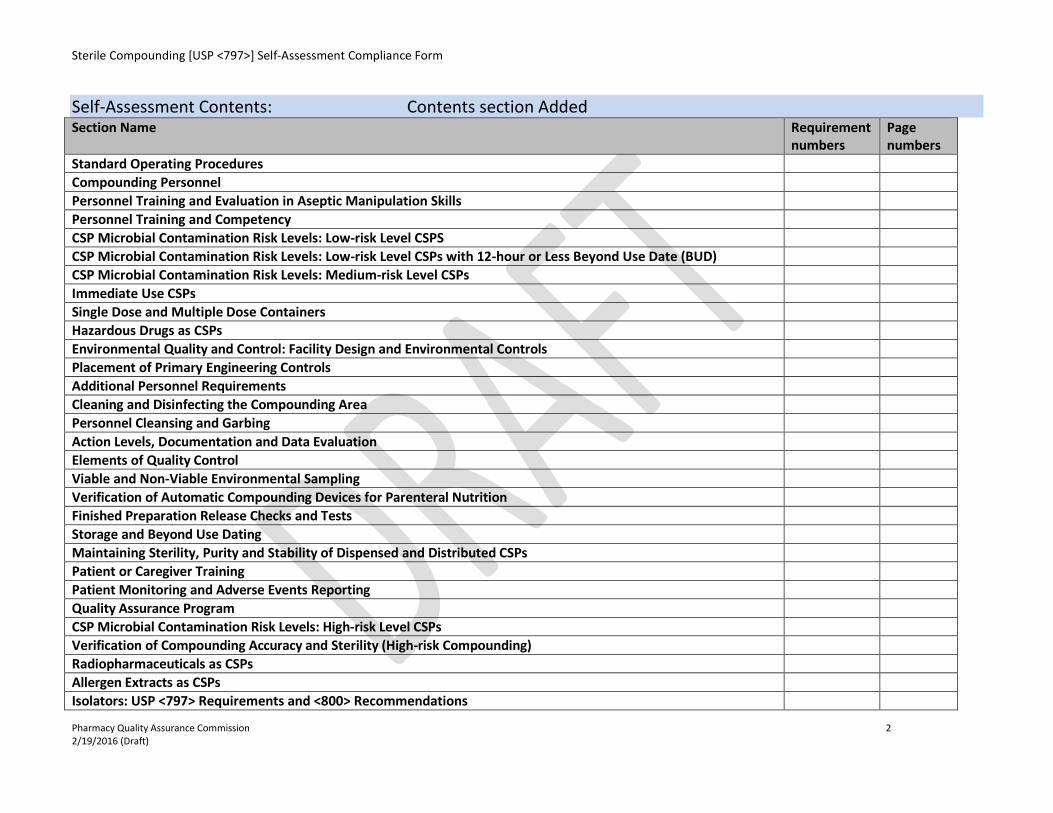
Sterile Compounding [USP <797>] Self-Assessment Compliance Form
Self-Assessment Contents: Contents section Added Section Name Requirement
numbers Page numbers
Standard Operating Procedures Compounding Personnel Personnel Training and Evaluation in Aseptic Manipulation Skills Personnel Training and Competency CSP Microbial Contamination Risk Levels: Low-risk Level CSPS CSP Microbial Contamination Risk Levels: Low-risk Level CSPs with 12-hour or Less Beyond Use Date (BUD) CSP Microbial Contamination Risk Levels: Medium-risk Level CSPs Immediate Use CSPs Single Dose and Multiple Dose Containers Hazardous Drugs as CSPs Environmental Quality and Control: Facility Design and Environmental Controls Placement of Primary Engineering Controls Additional Personnel Requirements Cleaning and Disinfecting the Compounding Area Personnel Cleansing and Garbing Action Levels, Documentation and Data Evaluation Elements of Quality Control Viable and Non-Viable Environmental Sampling Verification of Automatic Compounding Devices for Parenteral Nutrition Finished Preparation Release Checks and Tests Storage and Beyond Use Dating Maintaining Sterility, Purity and Stability of Dispensed and Distributed CSPs Patient or Caregiver Training Patient Monitoring and Adverse Events Reporting Quality Assurance Program CSP Microbial Contamination Risk Levels: High-risk Level CSPs Verification of Compounding Accuracy and Sterility (High-risk Compounding) Radiopharmaceuticals as CSPs Allergen Extracts as CSPs Isolators: USP <797> Requirements and <800> Recommendations
Pharmacy Quality Assurance Commission 2 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist
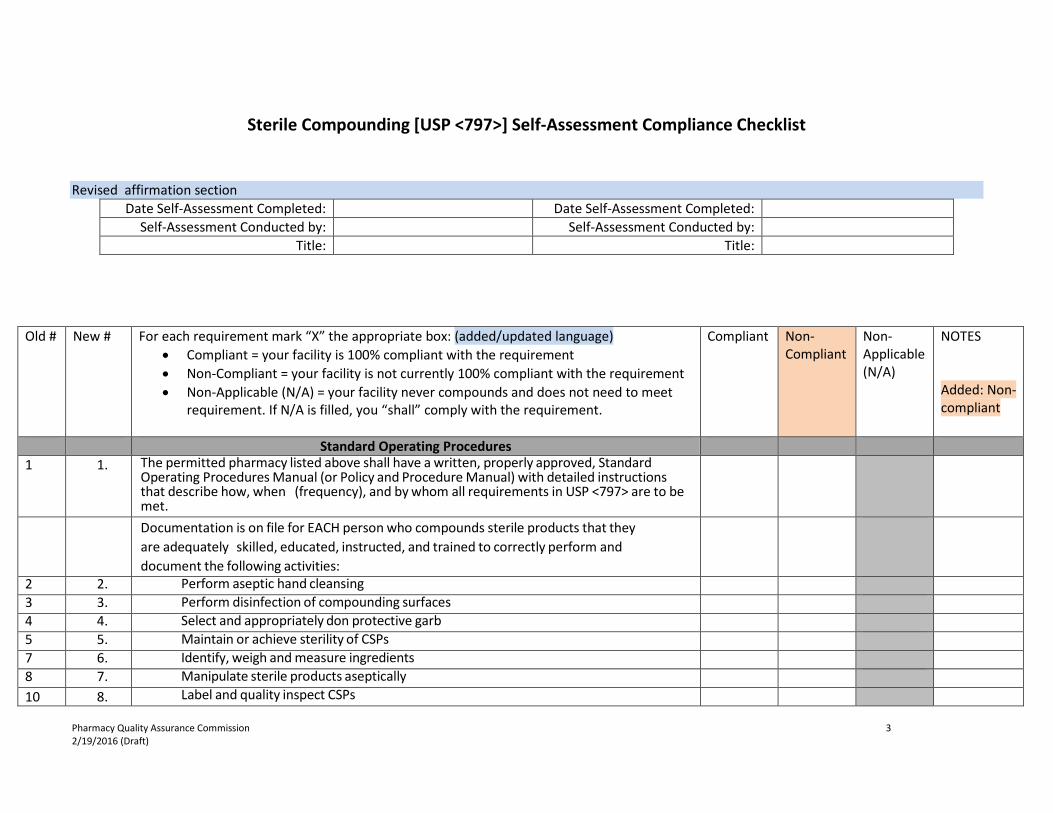
Revised affirmation section Date Self-Assessment Completed: Date Self-Assessment Completed:
Self-Assessment Conducted by: Self-Assessment Conducted by: Title: Title:
Old # New # For each requirement mark “X” the appropriate box: (added/updated language) • Compliant = your facility is 100% compliant with the requirement • Non-Compliant = your facility is not currently 100% compliant with the requirement • Non-Applicable (N/A) = your facility never compounds and does not need to meet
requirement. If N/A is filled, you “shall” comply with the requirement.
Compliant Non-Compliant
Non-Applicable (N/A)
NOTES Added: Non-compliant
Standard Operating Procedures 1 1. The permitted pharmacy listed above shall have a written, properly approved, Standard
Operating Procedures Manual (or Policy and Procedure Manual) with detailed instructions that describe how, when (frequency), and by whom all requirements in USP <797> are to be met.
Documentation is on file for EACH person who compounds sterile products that they are adequately skilled, educated, instructed, and trained to correctly perform and document the following activities:
2 2. Perform aseptic hand cleansing 3 3. Perform disinfection of compounding surfaces 4 4. Select and appropriately don protective garb 5 5. Maintain or achieve sterility of CSPs 7 6. Identify, weigh and measure ingredients 8 7. Manipulate sterile products aseptically 10 8. Label and quality inspect CSPs
Pharmacy Quality Assurance Commission 3 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
Personnel Training and Evaluation in Aseptic Manipulation Skills Moved
section: Personnel related
38 9. Before beginning to prepare CSPs, personnel are trained by expert personnel, audio-video instructional sources, professional publications in the theoretical principles, practical skills of aseptic manipulations and in achieving and maintaining ISO Class 5 environmental conditions
39 10. Personnel perform didactic review and pass written and media-fill testing of aseptic manipulative skills initially, then at least annually thereafter for low- and medium-risk level compounding
40 11. Personnel perform didactic review and pass written and media-fill testing of aseptic manipulative skills initially, and at least semi-annually for high-risk compounding
41 12. Personnel who fail written tests or whose media-fill test vials result in cross microbial colonization are immediately re-instructed and re-evaluated prior to resuming compounding
Personnel Training and Competency Moved section: Personnel related
149 13. Prior to compounding, personnel are trained in garbing procedures, aseptic work practices, achieving and maintaining ISO Class 5 conditions and cleaning and disinfections procedures
Need to review language
150 14. Media-fill testing of aseptic work skills are performed initially before beginning to prepare CSPs and at least annually thereafter for low- and medium-risk level; and semi-annually for high-risk level
Need to review language
151 15. Personnel who fail written tests, observational audits, or whose media-fill test vials have one or more units showing contamination are re-instructed and re-evaluated to ensure correction of all aseptic work practice deficiencies; personnel pass all evaluations prior to resuming compounding
Need to review language
152 16. Personnel demonstrate proficiency of proper hand hygiene, garbing and consistent cleaning procedures in addition to didactic evaluation of aseptic media fill and glove tip testing
Need to review language
153 17. Personnel are visually observed during the process of performing hand hygiene and garbing procedures and appropriately documented and maintained to provide a permanent record
Need to review language
154 18. Personnel successfully complete an initial competency evaluation and gloved fingertip/thumb sampling procedure no less than 3 times before initially being allowed to compound CSPs;
Need to
Pharmacy Quality Assurance Commission 4 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
which must be repeated at least annually for low- and medium-risk, and twice annually for high-risk compounding
review language
155 19. All compounding personnel have technique and competency evaluated initially during the Media-Fill Test Procedure and subsequent annual or semi-annual Media-Fill Test Procedures.
Need to review language
CSP Microbial Contamination : Low-risk Level CSPs 11 20. The CSPs are compounded with aseptic manipulations entirely within ISO Class 5 or better
quality air using only sterile ingredients, products, components and devices
12 21. Compounding involves only transfer, measuring and mixing manipulations using not more than 3 commercially manufactured sterile products and not more than 2 entries into any container
13 22. Manipulations are limited to aseptically opening ampoules, penetrating disinfected stoppers on vials with sterile needles and syringes and transferring sterile liquids in sterile syringes to sterile administration devices, package containers of other sterile products, and containers for storage and dispensing
14 23. In the absence of sterility tests, storage is not more than 48 hours at controlled room temperature, 14 days at cold temperature, and 45 days in a solid frozen state of -25° to -10°
CSP Microbial Contamination: Low-risk Level CSPs with 12-Hour or Less Beyond Use Date (BUD)
16 24. PECs are certified, maintained ISO Class 5 and located in a segregated compounding area restricted to sterile compounding activities
17 25. The segregated compounding area is not in a location that has unsealed windows or doors that connect to the outdoors or high traffic flow, or in a location that is adjacent to construction sites, warehouse or food preparation
18 26. Sinks are not located within one meter of the ISO Class 5 PEC; sinks are separated from the immediate area of the ISO Class 5 PEC device
Added language: “within one meter of”. Language in proposed 797, provides guidance of
Pharmacy Quality Assurance Commission 5 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
distance.
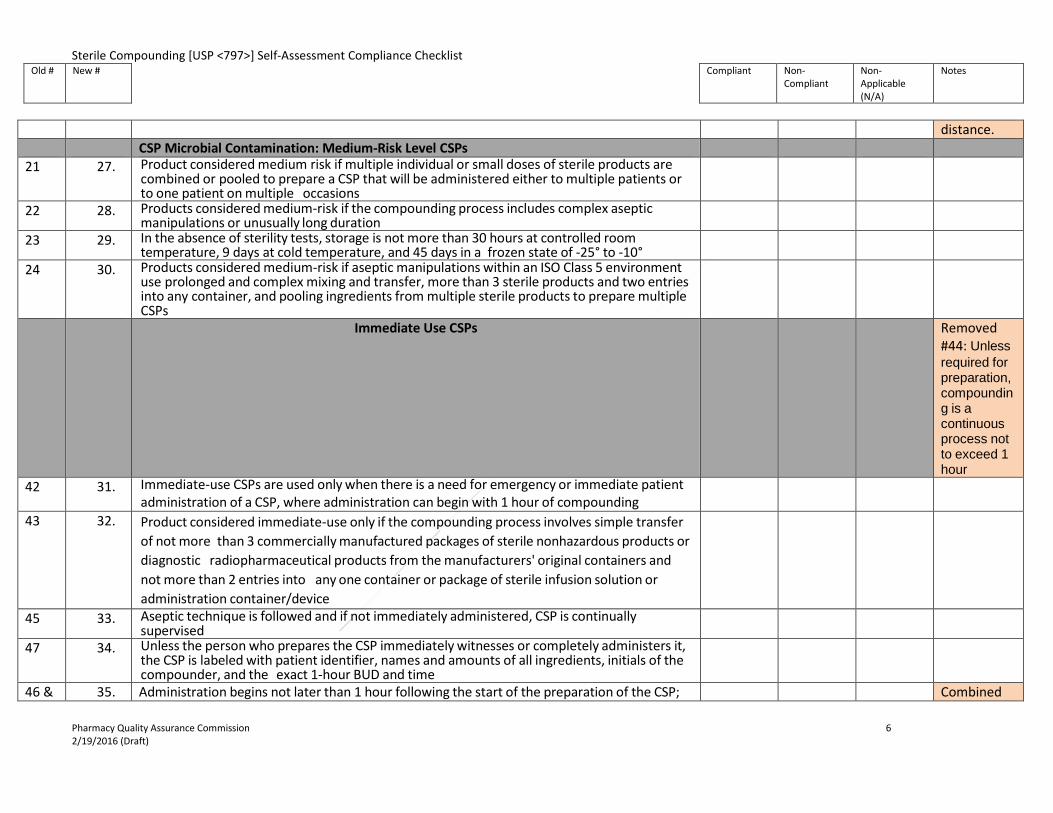
CSP Microbial Contamination: Medium-Risk Level CSPs 21 27. Product considered medium risk if multiple individual or small doses of sterile products are
combined or pooled to prepare a CSP that will be administered either to multiple patients or to one patient on multiple occasions
22 28. Products considered medium-risk if the compounding process includes complex aseptic manipulations or unusually long duration
23 29. In the absence of sterility tests, storage is not more than 30 hours at controlled room temperature, 9 days at cold temperature, and 45 days in a frozen state of -25° to -10°
24 30. Products considered medium-risk if aseptic manipulations within an ISO Class 5 environment use prolonged and complex mixing and transfer, more than 3 sterile products and two entries into any container, and pooling ingredients from multiple sterile products to prepare multiple CSPs
Immediate Use CSPs Removed #44: Unless required for preparation, compounding is a continuous process not to exceed 1 hour
42 31. Immediate-use CSPs are used only when there is a need for emergency or immediate patient administration of a CSP, where administration can begin with 1 hour of compounding
43 32. Product considered immediate-use only if the compounding process involves simple transfer of not more than 3 commercially manufactured packages of sterile nonhazardous products or diagnostic radiopharmaceutical products from the manufacturers' original containers and not more than 2 entries into any one container or package of sterile infusion solution or administration container/device
45 33. Aseptic technique is followed and if not immediately administered, CSP is continually supervised
47 34. Unless the person who prepares the CSP immediately witnesses or completely administers it, the CSP is labeled with patient identifier, names and amounts of all ingredients, initials of the compounder, and the exact 1-hour BUD and time
46 & 35. Administration begins not later than 1 hour following the start of the preparation of the CSP; Combined
Pharmacy Quality Assurance Commission 6 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
48 If administration has not begun within 1 hour of being compounded, CSP is discarded 46 & 48 Single Dose and Multiple Dose Containers 49 36. Single-dose containers entered in worse than ISO Class 5 air quality are used within 1 hour of
entry
50 37. Single-dose containers entered in ISO Class 5 or cleaner air are used within 6 hours of entry Research: vials / syringes
51 38. Opened single-dose ampoules are not stored 52 39. Closure sealed multiple-dose containers are used within 28 days after initial opening or entry,
unless specified otherwise by the manufacturer
Hazardous Drugs as CSPs 6 40. Protect personnel and compounding environment from contamination by hazardous drugs Moved to
Hazardous 53 41. Hazardous drugs are prepared for administration only under conditions that protect the
healthcare workers and other personnel in the preparation and storage areas
54 42. Hazardous drugs are stored separately from other inventory 55 43. Hazardous drugs are handled with caution at all times using appropriate chemotherapy gloves
during receiving, distribution, stocking, inventorying, preparation for administration and disposal
56 44. Hazardous drugs are prepared in an ISO Class 5 environment with protective engineering controls in place and follows aseptic practices specified for the appropriate contamination risk levels
57 45. Access is limited to areas where hazardous drugs are stored and prepared 58 46. All hazardous drugs are prepared in a BSC or a CACI that meets or exceeds standards 59 47. The ISO Class 5 BSC or CACI is placed in an ISO Class 7 area, physically separated and
optimally has not less than 0.01-inch water column negative pressure to adjacent positive pressure ISO Class 7 or better ante-areas. Certain exceptions allowed if CACI meets 797 requirements
List exceptions/ what are the exceptions?
60 48. A pressure indicator is installed that can be readily monitored for correct room pressurization 61 49. If closed-system vial-transfer devices are used, they are used within the ISO Class 5
environment of a BSC or CACI
62 50. Personnel protective equipment is worn when compounding 63 51. Personnel who compound hazardous drugs are trained in storage, handling and disposal of
drugs prior to preparing or handling hazardous CSPs
Pharmacy Quality Assurance Commission 7 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
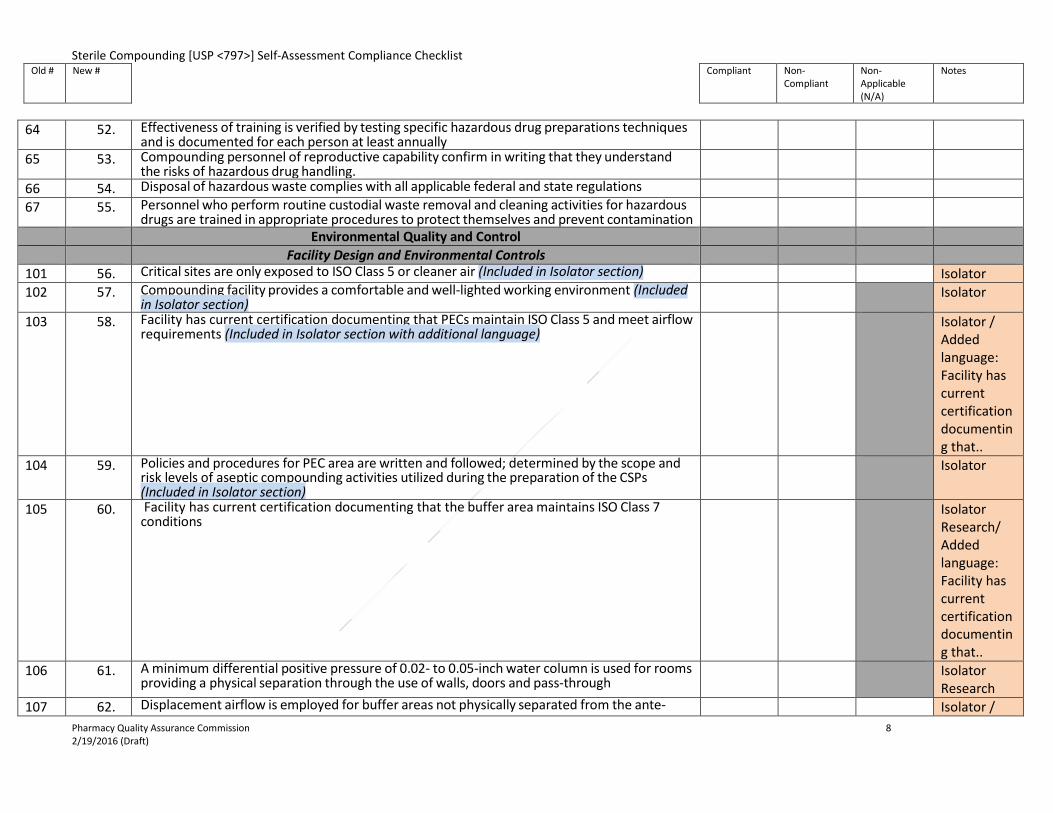
64 52. Effectiveness of training is verified by testing specific hazardous drug preparations techniques
and is documented for each person at least annually
65 53. Compounding personnel of reproductive capability confirm in writing that they understand the risks of hazardous drug handling.
66 54. Disposal of hazardous waste complies with all applicable federal and state regulations 67 55. Personnel who perform routine custodial waste removal and cleaning activities for hazardous
drugs are trained in appropriate procedures to protect themselves and prevent contamination
Environmental Quality and Control Facility Design and Environmental Controls 101 56. Critical sites are only exposed to ISO Class 5 or cleaner air (Included in Isolator section) Isolator 102 57. Compounding facility provides a comfortable and well-lighted working environment (Included
in Isolator section) Isolator
103 58. Facility has current certification documenting that PECs maintain ISO Class 5 and meet airflow requirements (Included in Isolator section with additional language)
Isolator / Added language: Facility has current certification documenting that..
104 59. Policies and procedures for PEC area are written and followed; determined by the scope and risk levels of aseptic compounding activities utilized during the preparation of the CSPs (Included in Isolator section)
Isolator
105 60. Facility has current certification documenting that the buffer area maintains ISO Class 7 conditions
Isolator Research/ Added language: Facility has current certification documenting that..
106 61. A minimum differential positive pressure of 0.02- to 0.05-inch water column is used for rooms providing a physical separation through the use of walls, doors and pass-through
Isolator Research
107 62. Displacement airflow is employed for buffer areas not physically separated from the ante- Isolator / Pharmacy Quality Assurance Commission 8 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
areas Added: able
to select N/A (due to ante room)
108 63. Adequate HEPA-filtered airflow is supplied to the buffer area and ante-area (Included in Isolator section with additional language)
Isolator
109 64. Facility has current certification documenting that ante-area and ISO Class 7 buffer area are supplied with HEPA-filtered air receive an ACPH of not less than 30 (Included in Isolator section with additional language)
Isolator / Added language: Facility has current certification documenting that..
110 65. If the area has an ISO Class 5 recirculating device, a minimum of 15 ACPHs through the area supply HEPA filters is adequate, providing the combined ACPH not less than 30 (Included in Isolator section)
Isolator Research/ Added: able to select N/A (due to ante room)
111 66. Only the furniture, equipment, supplies and other material required for the compounding activities are brought into the area and they are nonpermeable, nonshedding, cleanable, and resistant to disinfectants; before such items are brought into the area, they are cleaned and disinfected (Included in Isolator section)
Isolator
112 67. The surfaces of ceilings, walls, floors, fixtures, shelving, counters and cabinets in the buffer area are smooth, impervious, free from cracks and crevices and nonshedding; the surfaces are resistant to damage by disinfectant agents (Included in Isolator section with additional language)
Isolator
113 68. Junctures of ceilings to walls are coved or caulked (Included in Isolator section) Isolator 114 69. If ceilings consist of inlaid panels, the panels are impregnated with a polymer to render them
impervious and hydrophobic; they are caulked around each perimeter (Included in Isolator section)
Isolator
115 70. The exterior lens surface of the ceiling lighting fixtures are smooth, mounted flush and sealed; any other penetrations through the ceiling or walls are sealed (Included in Isolator section)
Isolator
116 71. The buffer area does not contain sources of water (sinks) or floor drains (Included in Isolator section with additional language)
Isolator
Pharmacy Quality Assurance Commission 9 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
117 72. Works surfaces are constructed of smooth, impervious materials (Included in Isolator section) Isolator 118 73. Carts are stainless steel wire, nonporous plastic or sheet metal with cleanable casters
(Included in Isolator section) Isolator
119 74. Storage shelving, counters and cabinets are smooth, impervious, free from cracks and crevices, nonshedding, cleanable and disinfectable; their number, design and manner of installation promotes effective cleaning and disinfection (Included in Isolator section)
Isolator
Placement of Primary Engineering Controls Deleted #122: Certification that each ISO classified area is within established guidelines is performed no less than every 6 months and each time the LAFW, BSC, CAI or CACI is relocated or the physical structure of the buffer area or anti-area has been altered (covered in viable/non-viable
120 75. PECs are located within a restricted access ISO Class 7 buffer area unless an exception met Exceptions:
Added:
Pharmacy Quality Assurance Commission 10 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
• Only authorized personnel and materials required for compounding and cleaning
shall be permitted in buffer area • Presterilization procedures for high-risk level CSPs, such as weighing and mixing,
shall be completed in no worse than Class 8 environment. • PECS shall be located out of traffic patterns and away from room air currents that
could disrupt the intended airflow patterns.
Exception language from USP797
121 76. When isolators are used for sterile compounding, the recovery time to achieve ISO Class 5 air quality is documented and internal procedures are developed
Isolator
123 77. A pressure gauge or velocity meter is installed to monitor the pressure differential or air-flow between the buffer area and the ante-area and between the ante-area and the general environment outside the compounding area; results are reviewed and documented in a log at least every work shift (minimum daily) or by a continuous recording device (Included in Isolator section)
Isolator
124 78. The pressure between the ISO Class 7 and the general pharmacy area is not less than 5 Pa -0.02 inch water column (Included in Isolator section with additional language)
Isolator
125 79. In facilities where low- and medium-risk level CSPs are prepared, differential airflow is maintained at a minimum velocity of 0.2 meters/second (40 feet per minute) between buffer area and ante-area
Isolator
Additional Personnel Requirements 129 80. Foods, drinks and materials exposed in patient care and treatment areas do not enter ante-
areas, buffer areas or segregated compounding areas
Cleaning and Disinfecting the Compounding Area 130 81. When compounding activities require the manipulation of patient’s blood-derived or other
biological material, the manipulations are clearly separated from routine material-handling procedures and equipment used in CSP preparation and are controlled by specific SOPs to avoid any cross-contamination
N/A? Added: patient’s to language-from USP797.
Able to select N/A? Examples of when to apply: include/exclude?
131 82. When possible, packaged compounding supplies and components are uncartoned and wiped down with a disinfectant that does not leave a residue in an ante-area ISO Class 8 air quality,
Isolator
Pharmacy Quality Assurance Commission 11 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
before being passed into buffer areas; Supplies are allowed to dry before compounding (Included in Isolator section)
133 83. For ISO Class 5, all cleaning and disinfecting practices and policies for the compounding of CSPs are included in written SOPs and are followed by all compounding personnel
Moved from Personnel Cleansing & Garbing
134 84. LAFWs, BSCs, CAIs, and/or CACIs are cleaned and disinfected frequently, including at the beginning of each work shift, before each batch preparation is started, every 30 minutes during continuous compounding periods, when spills occur and when surface contamination is known or suspected
Moved from Personnel Cleansing & Garbing
135 85. Work surfaces in ISO Class 7 buffer areas, ISO Class 8 ante-areas and segregated compounding areas are cleaned and disinfected at least daily, and dust and debris are removed when necessary from storage sites (Included in Isolator section with additional language)
Isolator/ moved from Personnel Cleansing & Garbing
136 86. Floors in ISO Class 7 and 8 areas are cleaned daily when no compounding occurs; mopping is performed by trained personnel using approved agents and written procedures (Included in Isolator section with additional language)
Isolator/ moved from Personnel Cleansing & Garbing
137 87. In the buffer or clean area, ante-area and segregated compounding area, walls, ceilings, and shelving are cleaned and disinfected monthly (Included in Isolator section with additional language)
Isolator/ Moved from Personnel Moved from Cleansing & Garbing
138 88. All cleaning materials are nonshedding and dedicated to use in the buffer or clean area, ante-area, and segregated areas and are not removed from these areas except for disposal
Moved from Cleansing & Garbing
139 89. If cleaning materials are reused, SOPs ensure that the effectiveness of the cleaning device is maintained and repeated use does not add to the bioburden of the area being cleaned
Moved from Cleansing & Garbing
140 90. Sterile 70% IPA swabs do not contact any object before contacting the site to be cleaned Moved from Pharmacy Quality Assurance Commission 12 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
Cleansing & Garbing
141 91. No particle-generating material is used to disinfect the sterile entry points of packages and devices
Moved from Cleansing & Garbing
142 92. No shipping cartons are taken into the buffer area, clean area or segregated compounding area
Moved from Cleansing & Garbing
Personnel Cleansing and Garbing 132 93. Personal hand hygiene and garb procedures are performed in ante-areas 143 94. Personnel with rashes, sunburn, weeping sores, conjunctivitis, active respiratory infection or
cosmetics are prohibited from preparing CSPs
No #, New
95. Don shoe covers one at a time placing covered shoe on clean side line of demarcation
144 & 145
96. PPE is donned in an order that proceeds from activities considered dirtiest to cleanest: Garb and cleansing in ante-area as follows: Dirty garb (shoes or shoe covers, head and facial hair covers, face mask) Hand hygiene (fingernail cleansing, hand and forearm washing and drying), Clean garb nonshedding gown (Included in Isolator section)
Isolator / combined 144 & 145/ organized dirtiest to cleanest
146 97. Cleansing and gloving in buffer room or area as follows: hand cleansing with an alcohol-based product with persistent activity, allow hands to dry, don sterile gloves and apply 70% IPA (Included in Isolator section with additional language)
Isolator / Added language: don sterile gloves and apply 70% IPA
147 98. Gloves are routinely disinfected with sterile 70% IPA after contacting nonsterile objects 148 99. Gloves are inspected for holes and replaced when breaches are detected No #, New
100. Only exterior gown used for non-hazardous compounding maybe removed and redoned in the ante area during the work shift if not visibly soiled. It is suggested that gowns be redones only if they are removed and retained on the clean side of the line of demarcation in the ante area
Added new requirement
Pharmacy Quality Assurance Commission 13 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
Action Levels, Documentation and Data Evaluation 156 101. Surface sampling is performed in all ISO classified areas on a periodic basis Need to
review language
157 102. Microbial sampling data is collected and reviewed routinely Need to review language
158 103. When microbial sampling exceed action levels, procedures and practices are reviewed Need to review language
Elements of Quality Control 159 104. A written description of specific training and performance evaluations for compounding
personnel is developed for each site Need to
review language
160 105. Facility follows procedures for physical inspection of all sterile drugs and devices Need to review language
161 106. If any nonsterile components, including containers and ingredients, are used to make a CSP, such CSPs must be high risk
Need to review language
162 107. Bulk of unformulated drug substances and added substances or excipients are stored in tightly closed containers under temperature, humidity and lighting conditions that are either indicated in the official monographs or approved by suppliers
Need to review language
163 108. The date of receipt of nonsterile components is clearly and indelibly marked on each package Need to review language
164 109. All devices used to compound a CSP operate properly within acceptable tolerance limits, as determined by the device's manufacturer or any regulations that govern the use of that device
Need to review language
165 110. For all equipment, SOPs exist and are followed that state routine maintenance required and frequency of calibration, annual maintenance, monitoring for proper function, and procedures for use
Need to review language
Pharmacy Quality Assurance Commission 14 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
166 111. Personnel are appropriately trained to operate any equipment they use while compounding
and are trained to determine if the device is operating properly or is malfunctioning. Need to
review language
167 112. Results from equipment maintenance and calibration are kept for the lifetime of the equipment
Need to review language
Viable and Non-Viable Environmental Sampling Added Section
127 113. For low-risk level CSPs with 12-hour or less BUD prepared in a PEC that maintains an ISO Class 5 sampling, air sampling is performed at locations inside the ISO Class 5 environment and other areas that are in close proximity to the ISO Class 5
After Class 5….Deleted: during the certification of the PEC
128 114. A sufficient volume of air (400 to 1000 liters) is tested at each location where compounding takes place, performed at least semi-annually
No #, New
115. Engineering control performance verification is performed by a qualified individual no less than every 6 months and whenever the device or room is relocated, altered or major service to the facility is performed. (Nonviable)
Added New requirement
No #, New
116. Total particle counts are performed by a qualified operator using state-of-the-art electronic equipment and are within established guidelines in each ISO classified area no less than every 6 months and whenever the LAFW, BSC, CAI, or CACI is relocated or the physical structure of the buffer area or ante-area has been altered. (Nonviable)
Added New requirement
No #, New
117. An appropriate environmental sampling plan is in place for airborne viable particles, is performed at least every 6 months, and includes locations within each ISO class 5 environments and in the ISO class 7 and 8 areas
Added New requirement
No #, New
118. The sampling plan for airborne particles includes sample location, method of collection, frequency of sampling, volume of air sampled, time of day as related to activity in the compounding area and action levels
Added New requirement
No #, New
119. A general microbiological growth medium supplemented with additives to neutralize the effects of disinfecting agents is used to support the growth of bacteria.
Added New requirement
No #, New
120. Surface sampling is performed in all ISO classified areas on a periodic basis to evaluate cleaning and disinfecting procedures and employee competency in work practices
Added New requirement
No #, New
121. Sampling data is collected and reviewed on a routine basis as a means of evaluating overall control of the compounding environment
Added New requirement
Pharmacy Quality Assurance Commission 15 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
No #, New
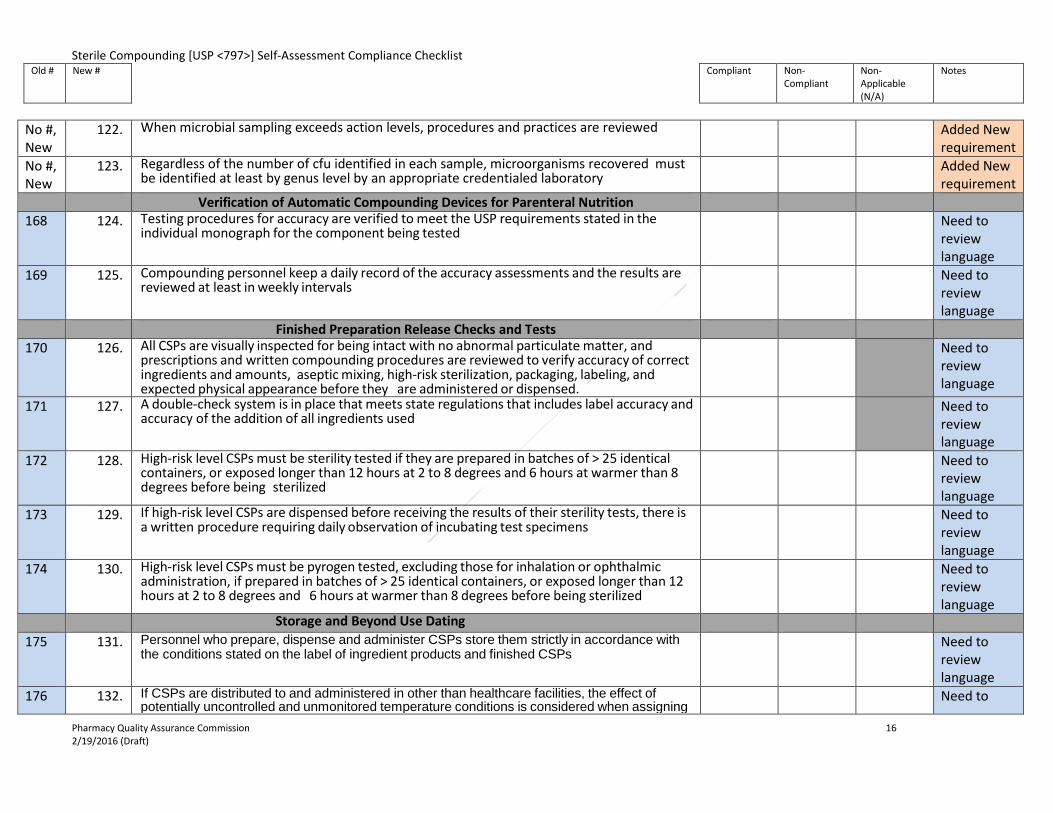
122. When microbial sampling exceeds action levels, procedures and practices are reviewed Added New requirement
No #, New
123. Regardless of the number of cfu identified in each sample, microorganisms recovered must be identified at least by genus level by an appropriate credentialed laboratory
Added New requirement
Verification of Automatic Compounding Devices for Parenteral Nutrition 168 124. Testing procedures for accuracy are verified to meet the USP requirements stated in the
individual monograph for the component being tested Need to
review language
169 125. Compounding personnel keep a daily record of the accuracy assessments and the results are reviewed at least in weekly intervals
Need to review language
Finished Preparation Release Checks and Tests 170 126. All CSPs are visually inspected for being intact with no abnormal particulate matter, and
prescriptions and written compounding procedures are reviewed to verify accuracy of correct ingredients and amounts, aseptic mixing, high-risk sterilization, packaging, labeling, and expected physical appearance before they are administered or dispensed.
Need to review language
171 127. A double-check system is in place that meets state regulations that includes label accuracy and accuracy of the addition of all ingredients used
Need to review language
172 128. High-risk level CSPs must be sterility tested if they are prepared in batches of > 25 identical containers, or exposed longer than 12 hours at 2 to 8 degrees and 6 hours at warmer than 8 degrees before being sterilized
Need to review language
173 129. If high-risk level CSPs are dispensed before receiving the results of their sterility tests, there is a written procedure requiring daily observation of incubating test specimens
Need to review language
174 130. High-risk level CSPs must be pyrogen tested, excluding those for inhalation or ophthalmic administration, if prepared in batches of > 25 identical containers, or exposed longer than 12 hours at 2 to 8 degrees and 6 hours at warmer than 8 degrees before being sterilized
Need to review language
Storage and Beyond Use Dating 175 131. Personnel who prepare, dispense and administer CSPs store them strictly in accordance with
the conditions stated on the label of ingredient products and finished CSPs Need to
review language
176 132. If CSPs are distributed to and administered in other than healthcare facilities, the effect of potentially uncontrolled and unmonitored temperature conditions is considered when assigning
Need to
Pharmacy Quality Assurance Commission 16 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
BUDs review
language 177 133. The controlled temperature areas are monitored at least once daily and results are documented Need to
review language
178 134. Facilities have policies and procedures governing the determination of BUDs Need to review language
179 135. Compounding personnel verify the storage temperature when placing a product into or removing a product from the storage unit
Need to review language
180 136. Temperature-sensitive mechanisms are placed to reflect true temperature in the controlled space and are not subject to significantly prolonged temperature fluctuations
Need to review language
Maintaining Sterility, Purity and Stability of Dispensed and Distributed CSPs 181 137. The facilities have written procedures for proper packaging, storage, and transportation
conditions to maintain sterility, quality, purity and strength of CSPs Need to
review language
182 138. Chemotoxic and other hazardous CSPs have safeguards to maintain the integrity of the CSP and minimize the exposure potential of these products to the environment and personnel
Need to review language
183 139. Delivery and patient-care-setting personnel are properly trained to deliver the CSP to the appropriate storage location
Need to review language
184 140. Outdated and unused CSPs are returned to the compounding facility for disposition as appropriate
Need to review language
185 141. SOPs exist to ensure that the storage conditions in the patient-care setting are suitable for the CSP-specific storage requirements
Need to review language
186 142. Returned CSPs are only redispensed if sterility, acceptable purity, strength and quality can be assured
Need to review
Pharmacy Quality Assurance Commission 17 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
language
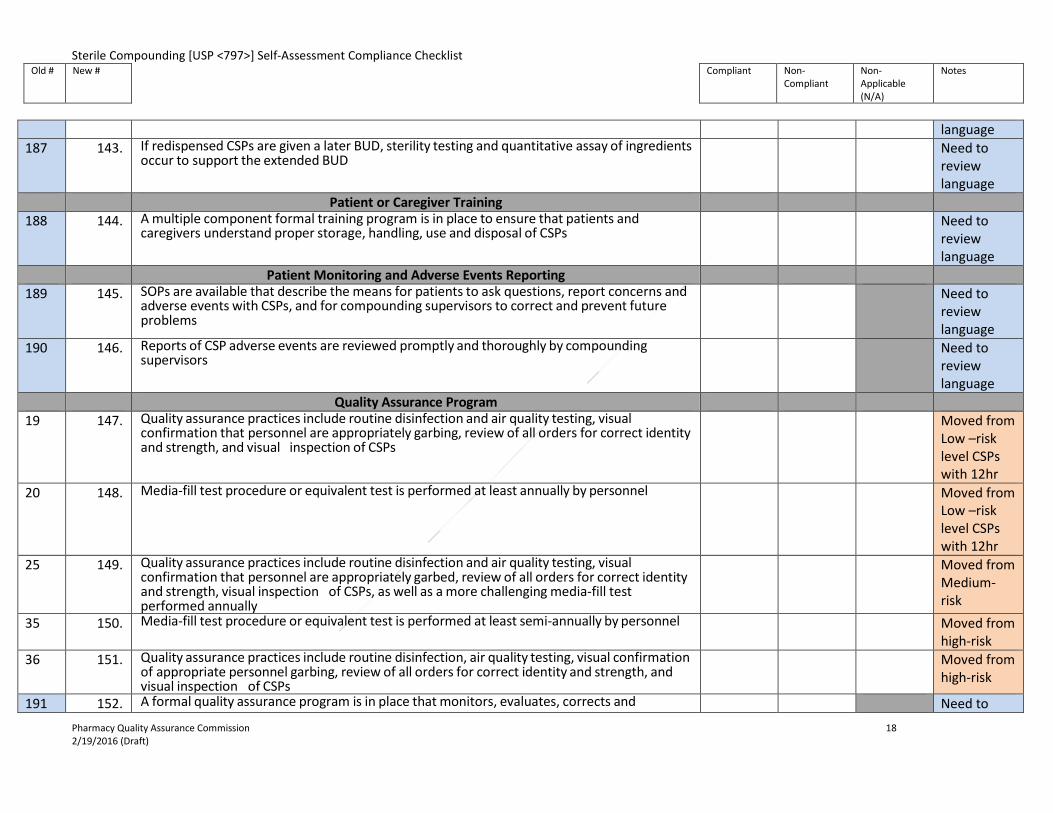
187 143. If redispensed CSPs are given a later BUD, sterility testing and quantitative assay of ingredients occur to support the extended BUD
Need to review language
Patient or Caregiver Training 188 144. A multiple component formal training program is in place to ensure that patients and
caregivers understand proper storage, handling, use and disposal of CSPs Need to
review language
Patient Monitoring and Adverse Events Reporting 189 145. SOPs are available that describe the means for patients to ask questions, report concerns and
adverse events with CSPs, and for compounding supervisors to correct and prevent future problems
Need to review language
190 146. Reports of CSP adverse events are reviewed promptly and thoroughly by compounding supervisors
Need to review language
Quality Assurance Program 19 147. Quality assurance practices include routine disinfection and air quality testing, visual
confirmation that personnel are appropriately garbing, review of all orders for correct identity and strength, and visual inspection of CSPs
Moved from Low –risk level CSPs with 12hr
20 148. Media-fill test procedure or equivalent test is performed at least annually by personnel Moved from Low –risk level CSPs with 12hr
25 149. Quality assurance practices include routine disinfection and air quality testing, visual confirmation that personnel are appropriately garbed, review of all orders for correct identity and strength, visual inspection of CSPs, as well as a more challenging media-fill test performed annually
Moved from Medium-risk
35 150. Media-fill test procedure or equivalent test is performed at least semi-annually by personnel Moved from high-risk
36 151. Quality assurance practices include routine disinfection, air quality testing, visual confirmation of appropriate personnel garbing, review of all orders for correct identity and strength, and visual inspection of CSPs
Moved from high-risk
191 152. A formal quality assurance program is in place that monitors, evaluates, corrects and Need to Pharmacy Quality Assurance Commission 18 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
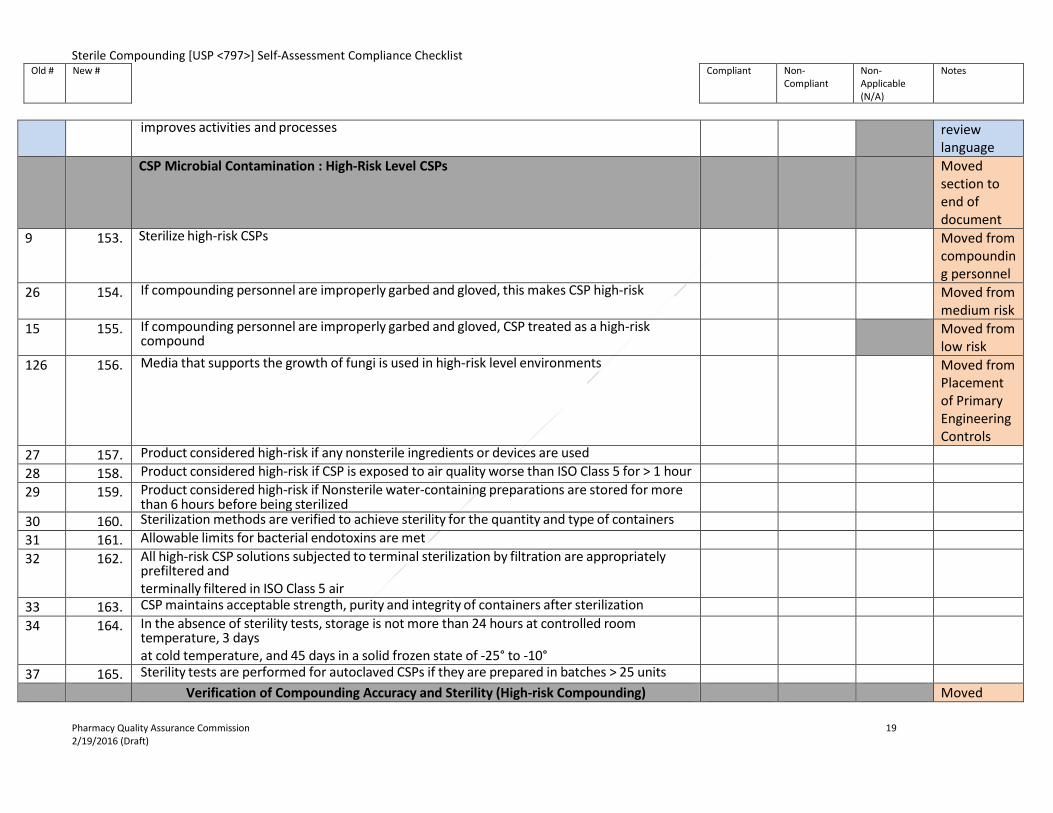
improves activities and processes review
language CSP Microbial Contamination : High-Risk Level CSPs Moved
section to end of document
9 153. Sterilize high-risk CSPs Moved from compounding personnel
26 154. If compounding personnel are improperly garbed and gloved, this makes CSP high-risk Moved from medium risk
15 155. If compounding personnel are improperly garbed and gloved, CSP treated as a high-risk compound
Moved from low risk
126 156. Media that supports the growth of fungi is used in high-risk level environments Moved from Placement of Primary Engineering Controls
27 157. Product considered high-risk if any nonsterile ingredients or devices are used 28 158. Product considered high-risk if CSP is exposed to air quality worse than ISO Class 5 for > 1 hour 29 159. Product considered high-risk if Nonsterile water-containing preparations are stored for more
than 6 hours before being sterilized
30 160. Sterilization methods are verified to achieve sterility for the quantity and type of containers 31 161. Allowable limits for bacterial endotoxins are met 32 162. All high-risk CSP solutions subjected to terminal sterilization by filtration are appropriately
prefiltered and terminally filtered in ISO Class 5 air
33 163. CSP maintains acceptable strength, purity and integrity of containers after sterilization 34 164. In the absence of sterility tests, storage is not more than 24 hours at controlled room
temperature, 3 days at cold temperature, and 45 days in a solid frozen state of -25° to -10°
37 165. Sterility tests are performed for autoclaved CSPs if they are prepared in batches > 25 units Verification of Compounding Accuracy and Sterility (High-risk Compounding) Moved
Pharmacy Quality Assurance Commission 19 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
section to end of document
81 166. Packaged and labeled CSPs are visually inspected for physical integrity and expected appearance
82 167. The accuracy of identities, concentrations, amounts and purities of ingredients in CSPs are confirmed by reviewing labels on packages, observing and documenting correct measurements with approved and correctly standardized devices, and reviewing information in labeling with certificates of analysis provided by suppliers
83 168. The licensed healthcare professional is responsible for determining that the selected sterilization method both sterilizes and maintains the strength, purity, quality and packaging integrity of CSPs.
84 169. Commercially available sterile filters are approved for human-use applications in sterilizing pharmaceutical fluids
85 170. Sterile filters used to sterilize CSPs are pyrogen free with a nominal porosity of 0.2 or 0.22 micrometers
86 171. Sterile filters used are certified by the manufacturer to retain at least 10^7 microorganisms of a strain of Brevundimonas diminuta on each square centimeter of upstream filter surface area
87 172. The compounding supervisor ensures that the filters are chemically and physically stable at the pressure and temperature conditions to be used, that they have enough capacity to filter the required volumes, and that they will achieve sterility and maintain prefiltration pharmaceutical quality
88 173. The filter dimensions and liquid material to be sterile-filtered permit the sterilization process to be completed rapidly, without replacement of the filter during the process
89 174. When CSPs are known to contain excessive particulate matter, a prefilter of larger-porosity membrane is placed upstream from the sterilizing filter to remove gross particulate contaminants.
90 175. Filter units used are subjected to manufacturers' recommended integrity test 91 176. Personnel must know that filters will achieve sterilization of the particular CSPs being
sterilized
92 177. The description of steam sterilization conditions and duration for specific CSPs are included in written documentation in the compounding facility
93 178. The effectiveness of steam sterilization is verified using appropriate Bis of Bacillus stearothermophilus and other confirmation methods
94 179. Heated filtered air is evenly distributed throughout the chamber by a blower device; the oven is equipped with a system for controlling temperature and exposure period
Pharmacy Quality Assurance Commission 20 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
95 180. Dry heat is used only for those materials that cannot be sterilized by steam 96 181. During sterilization, sufficient space is left between materials to allow for good air circulation 97 182. The description of dry heat sterilization conditions and duration for specific CSPs are included
in written documentation in the compounding facility
98 183. The effectiveness of dry heat sterilization is verified using appropriate BIs of Bacillus subtilis and other confirmation methods
99 184. The description of dry heat depyrogenation cycle conditions and duration for specific CSPs are included in written documentation in the compounding facility
100 185. The effectiveness of the dry heat depyrogenation cycle is verified using endotoxin challenge vials (ECVs); the bacterial endotoxin test is performed on the ECVs to verify that the cycle is capable of achieving a 3- log reduction in endotoxin
Radiopharmaceuticals as CSPs Moved section to end
68 186. Radiopharmaceuticals are compounded using appropriately shielded vials and syringes in a properly functioning and certified ISO Class 5 PEC located in the ISO Class 8 or cleaner air environment
69 187. Radiopharmaceutical vials designed for multi-use, compounded with technetium-99m, exposed to ISO Class 5 environment, and punctured by needles with no direct contact contamination are used by the time indicated by the manufacturers' recommendations
70 188. Technetium-99m/molybdenum-99 generator systems are stored and operated under conditions recommended by manufacturers and applicable state and federal regulations; such generator systems are operated in an ISO Class 8 or cleaner air environment
71 189. Direct visual inspection of radiopharmaceutical CSPs containing high concentrations of doses of radioactivity are conducted in accordance with ALARA
72 190. Radiopharmaceuticals prepared as low-risk level CSPs with 12-hour or less BUD are prepared in a segregated compounding area; a line of demarcation is established
73 191. Materials and garb exposed in patient care and treatment do not cross the line of demarcation
Allergen Extracts as CSPs Moved section to end
74 192. Compounding is performed only with simple transfers using sterile ingredients and supplies 75 193. Allergen extracts contain appropriate concentrations of preservatives 76 194. Before compounding, personnel appropriately wash hands with soap and water, apply
alcohol-based scrub with persistent activity, don hair covers, facial hair covers, gowns, face masks and gloves
Pharmacy Quality Assurance Commission 21 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist Old # New # Compliant Non-
Compliant Non-Applicable (N/A)
Notes
77 195. Sterile gloves are intermittently disinfected with sterile 70% IPA 78 196. Vial/ampule critical sites are wet with 70% IPA for 10 seconds and allowed to dry before use 79 197. Compounding manipulations are performed to minimize contact contamination of critical
sites
80 198. Vials are labeled with patient's name, BUD and storage information based on manufacturers' recommendations or peer-reviewed literature
Pharmacy Quality Assurance Commission 22 2/19/2016 (Draft)

Isolators USP <797> Requirements and <800> Recommendations
• The following section focuses on Isolators. The contents include USP<797> requirements (“shalls”) and <800> recommendations. • Isolator USP <797> requirements will be noted in each item with the following: [USP <797> requirement] • Information for <800> was obtained by interpreting the proposed General Chapter <800> Hazardous Drugs-Handling in Healthcare Settings PF
40(3) [May–Jun.2013], (CMP: J. Sun.) Correspondence Number-C139868. Location of document-http://www.usp.org/usp-nf/notices/general-chapter-hazardous-drugs-handling-healthcare-settings
Corresponding number indicates that the item is located in the checklist. The language maybe the same or additional language has been added.
New Isolators Added section
Newor corresponding #
General
Compliant Non-Compliant
Non-Applicable (N/A)
Added section
New A1
Placement in a restricted access ISO Class 7 buffer area required Exceptions where isolators may be placed in an air quality worse than ISO Class 7 (only applies if all of the following conditions are met)
• The isolator shall provide isolation from the room and maintain ISO Class 5 during dynamic operating conditions, including transferring ingredients, components, and devices into and out of the isolator and during preparation of CSP’s
• Particle counts sampled approximately 6 to 12 inches upstream of the critical exposure site shall maintain ISO Class 5 levels during compounding operations
• Not more than 3520 particles (0.5 um and larger) per m3 shall be counted during material transfer, with the particle counter probe located as near to the transfer door as possible without obstructing the transfer
Added recommendation/ Need to review language
Pharmacy Quality Assurance Commission 23 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
New A2 If placement cannot be located in a ISO Class 7 buffer area and all exception conditions cannot
be met, then the PEC (Primary Engineering Control) is considered a PEC located in a segregated compounding area and only low-risk CSP’s with 12-hour or less BUD can be prepared
Added recommendation/ Need to review language
New A3 Sterile gloves are required for sterile compounding and should be replaced regularly. A sterile glove should be placed over the top of the glove mounted to the isolator and should be replaced at the same interval as is appropriate for any other sterile compounding process. The glove mounted to the sleeve (gauntlet) does not need to be sterile and should be replaced daily or between operators.
Added recommendation/ Need to review language
101 A4 Critical sites are only exposed to ISO Class 5 or cleaner air [USP <797> requirement] Same language as <797> Checklist item 101; from Facility Design and Environmental Controls
102 A5 Compounding facility provides a comfortable and well-lighted working environment [USP <797> requirement]
Same language as <797> Checklist item 102; from Facility Design and Environme
Pharmacy Quality Assurance Commission 24 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
ntal Controls
103 A6 Facility has current certification according to the Controlled Environment Testing Association (CETA) Application Guides documenting that PECs maintain ISO Class 5 and meet airflow requirements [USP <797> requirement]
Similar language as <797> Checklist item 103; from Facility Design and Environmental Controls
104 A7 Policies and procedures for PEC area are written and followed; determined by the scope and risk levels of aseptic compounding activities utilized during the preparation of the CSPs [USP <797> requirement]
Same language as <797> Checklist item 104; from Facility Design and Environmental Controls
108 A8 Adequate ceiling delivered HEPA-filtered airflow is supplied to the buffer area and ante-area [USP <797> requirement]
Similar language as <797> Checklist item 108; from Facility Design and
Pharmacy Quality Assurance Commission 25 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
Environmental Controls
109 A9 Facility has current certification according to the CETA Application Guides documenting that the ante-area and ISO Class 7 buffer area are supplied with HEPA-filtered air receive an ACPH of not less than 30 [USP <797> requirement]
Similar language as <797> Checklist item 109; from Facility Design and Environmental Controls
110 A10
If the area has an ISO Class 5 recirculating device, a minimum of 15 ACPHs through the area supply HEPA filters is adequate, providing the combined ACPH not less than 30 [USP <797> requirement]
Same language as <797> Checklist item 110; from Facility Design and Environmental Controls
111 A11 Only the furniture, equipment, supplies and other material required for the compounding activities are brought into the area and are non-permeable, non-shedding, cleanable, and resistant to disinfectants; before such items are brought into the area, they are cleaned and disinfected [USP <797> requirement]
Same language as <797> Checklist item 111; from Facility
Pharmacy Quality Assurance Commission 26 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
Design and Environmental Controls
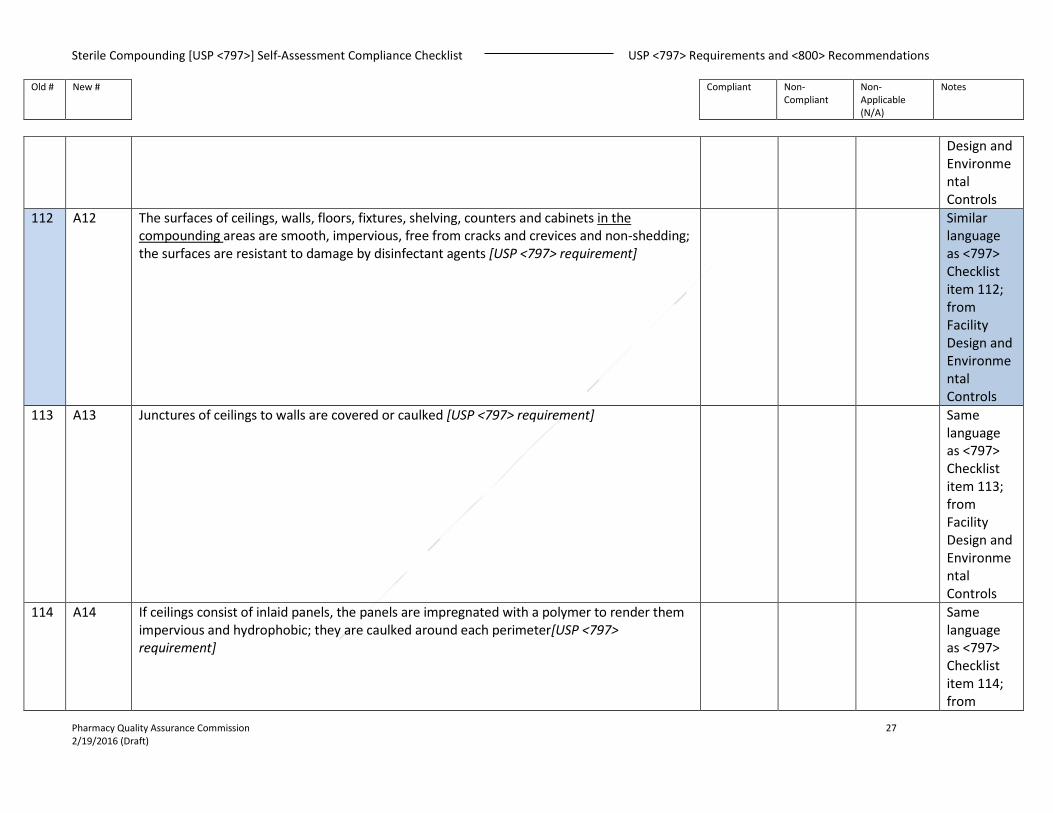
112 A12 The surfaces of ceilings, walls, floors, fixtures, shelving, counters and cabinets in the compounding areas are smooth, impervious, free from cracks and crevices and non-shedding; the surfaces are resistant to damage by disinfectant agents [USP <797> requirement]
Similar language as <797> Checklist item 112; from Facility Design and Environmental Controls
113 A13 Junctures of ceilings to walls are covered or caulked [USP <797> requirement] Same language as <797> Checklist item 113; from Facility Design and Environmental Controls
114 A14 If ceilings consist of inlaid panels, the panels are impregnated with a polymer to render them impervious and hydrophobic; they are caulked around each perimeter[USP <797> requirement]
Same language as <797> Checklist item 114; from
Pharmacy Quality Assurance Commission 27 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
Facility Design and Environmental Controls
115 A15 The exterior lens surface of the ceiling lighting are smooth, mounted flush and sealed; any other penetrations through the ceiling or walls are sealed [USP <797> requirement]
Same language as <797> Checklist item 115; from Facility Design and Environmental Controls
116 A16 The buffer area does not contain sources of water (sinks) or floor drains, but sinks are permitted in a Segregated Compounding Area when located at least 1 meter or 3 feet away from the PEC [USP <797> requirement]
Similar language as <797> Checklist item 116; from Facility Design and Environmental Controls
117 A17 Work surfaces are constructed of smooth, impervious materials [USP <797> requirement] Same language as <797> Checklist item 117;
Pharmacy Quality Assurance Commission 28 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
from Facility Design and Environmental Controls
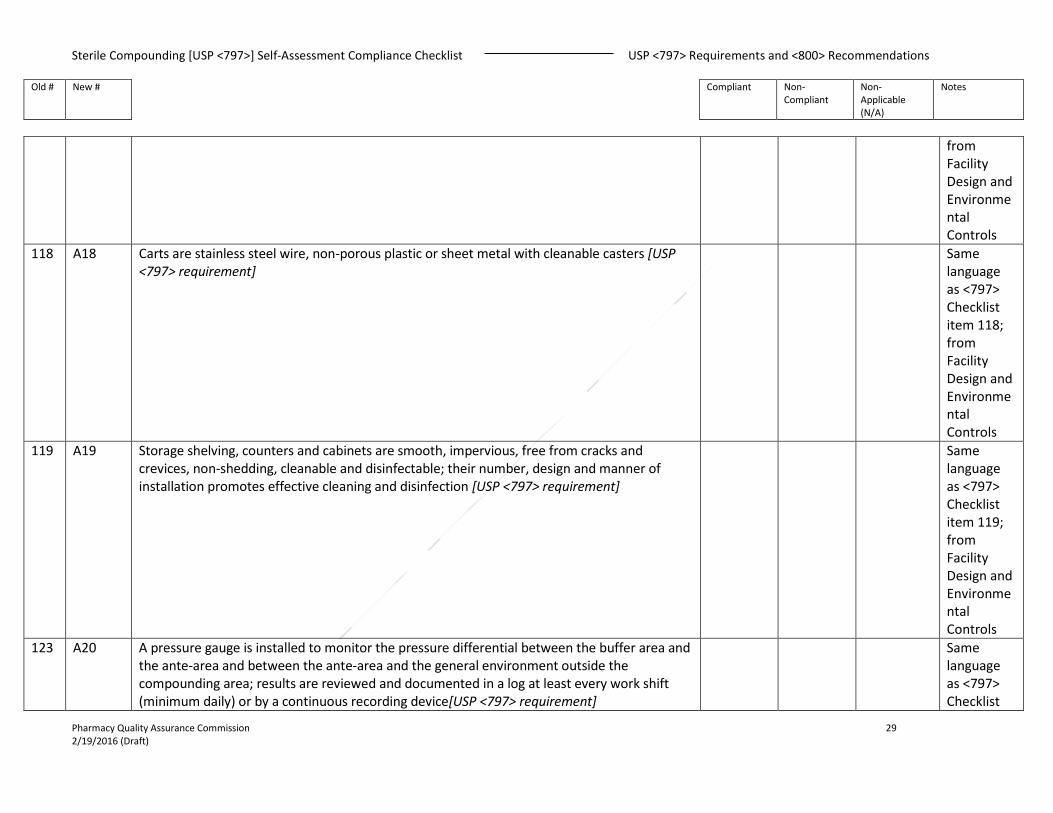
118 A18 Carts are stainless steel wire, non-porous plastic or sheet metal with cleanable casters [USP <797> requirement]
Same language as <797> Checklist item 118; from Facility Design and Environmental Controls
119 A19 Storage shelving, counters and cabinets are smooth, impervious, free from cracks and crevices, non-shedding, cleanable and disinfectable; their number, design and manner of installation promotes effective cleaning and disinfection [USP <797> requirement]
Same language as <797> Checklist item 119; from Facility Design and Environmental Controls
123 A20 A pressure gauge is installed to monitor the pressure differential between the buffer area and the ante-area and between the ante-area and the general environment outside the compounding area; results are reviewed and documented in a log at least every work shift (minimum daily) or by a continuous recording device[USP <797> requirement]
Same language as <797> Checklist
Pharmacy Quality Assurance Commission 29 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
item 123; from Placement of Primary Engineering Controls
124 A21 The pressure between the ISO Class 7 and the general pharmacy area is not less than 5 Pa (0.02 inch water column). If using a cascading pressure differential, this value should be 0.04”. 0.02 from buffer room to anteroom and 0.02” from the anteroom to the general pharmacy [USP <797> requirement]
Similar language as <797> Checklist item 124; from Placement of Primary Engineering Controls
131 A22 All packaged compounding supplies and components are uncartoned and wiped down with a disinfectant that does not leave a residue in an ante-area ISO Class 8 air quality, before being passed into buffer areas; Supplies are allowed to dry before compounding [USP <797> requirement]
Same language as <797> Checklist item 131; from Cleaning and Disinfecting the Compounding Area
135 A23 Work surfaces in ISO Class 7 buffer areas, ISO Class 8 ante-areas and segregated compounding areas are cleaned and disinfected at least daily, and dust and debris are removed when necessary from storage sites. This cleaning is clearly documented (paper or electronically) [USP <797> requirement]
Similar language as <797> Checklist
Pharmacy Quality Assurance Commission 30 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
item 135; from Cleaning and Disinfecting the Compounding Area
136 A24 Floors in ISO Class 7 and 8 areas and segregated compounding areas are cleaned daily with a germicidal detergent and water when no compounding occurs; mopping is performed by trained personnel using approved agents and written procedures [USP <797> requirement]
Similar language as <797> Checklist item 136; from Cleaning and Disinfecting the Compounding Area
137 A25 In the buffer or clean area, ante-area and segregated compounding area, walls, ceilings, and shelving are cleaned and disinfected monthly and cleaning is clearly and properly documented [USP <797> requirement]
Similar language as <797> Checklist item 137; from Cleaning and Disinfecting the Compounding Area
Pharmacy Quality Assurance Commission 31 2/19/2016 (Draft)
Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
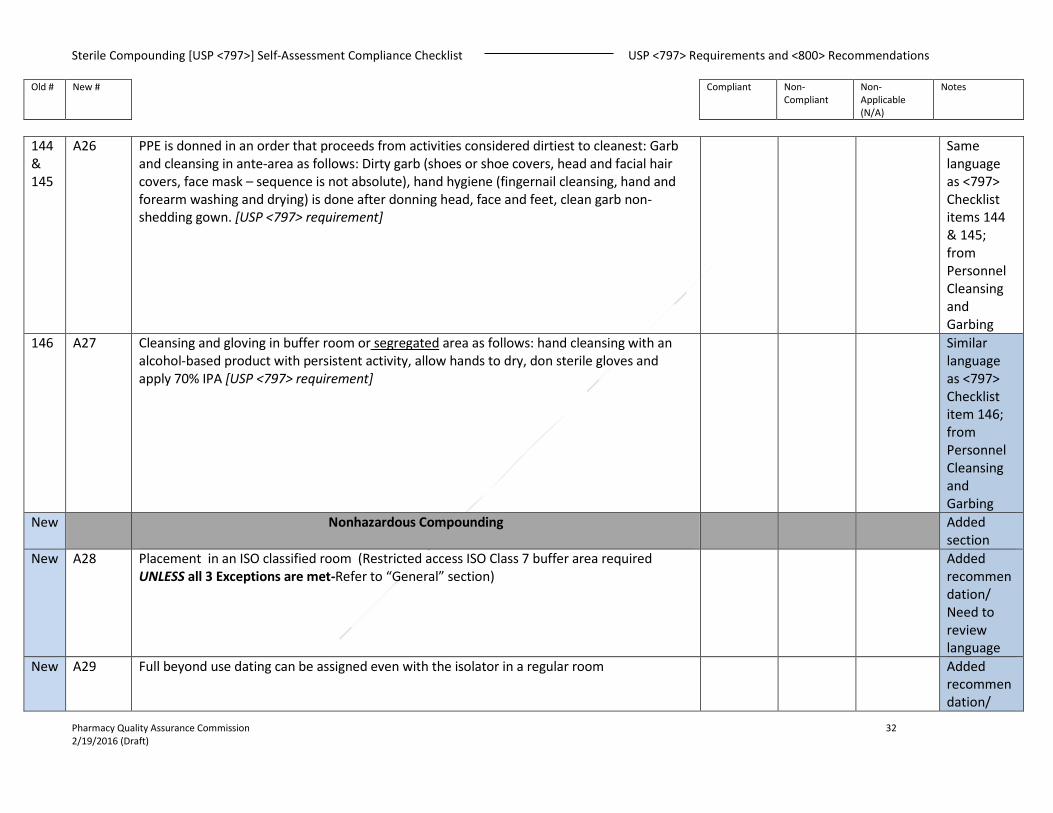
144 & 145
A26 PPE is donned in an order that proceeds from activities considered dirtiest to cleanest: Garb and cleansing in ante-area as follows: Dirty garb (shoes or shoe covers, head and facial hair covers, face mask – sequence is not absolute), hand hygiene (fingernail cleansing, hand and forearm washing and drying) is done after donning head, face and feet, clean garb non-shedding gown. [USP <797> requirement]
Same language as <797> Checklist items 144 & 145; from Personnel Cleansing and Garbing
146 A27 Cleansing and gloving in buffer room or segregated area as follows: hand cleansing with an alcohol-based product with persistent activity, allow hands to dry, don sterile gloves and apply 70% IPA [USP <797> requirement]
Similar language as <797> Checklist item 146; from Personnel Cleansing and Garbing
New Nonhazardous Compounding
Added section
New A28 Placement in an ISO classified room (Restricted access ISO Class 7 buffer area required UNLESS all 3 Exceptions are met-Refer to “General” section)
Added recommendation/ Need to review language
New A29 Full beyond use dating can be assigned even with the isolator in a regular room Added recommendation/
Pharmacy Quality Assurance Commission 32 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
Need to review language
New A30 Room must be cleanable and accommodations for hand washing must be available Added recommendation/ Need to review language
New A31 Must be unidirectional airflow Added recommendation/ Need to review language
New A32 Should be certified in accordance with CETA CAG-002 (as referenced in CAG-003 and <797>) Added recommendation/ Need to review language
110 A33 If the area has an ISO Class 5 recirculating device, a minimum of 15 ACPHs through the area supply HEPA filters is adequate, providing the combined ACPH not less than 30 [USP <797> requirement]
Same language as <797> Checklist item 110; from Facility Design and Environmental Controls.
Pharmacy Quality Assurance Commission 33 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
New A34 Garbing same as those in Personal Cleansing and Garbing , unless manufacturer can provide
written documentation based on validated environmental testing that any component(s) of PPE or personal cleansing is not required
Added recommendation/ Need to review language
New Hazardous Compounding
Added section
New A35 For Nonsterile- Containment Ventilated Enclosure (CVE) or Class I Biological Safety Cabinet (BSC) (**Class II BSCs or Compounding Aseptic Containment Isolators (CACIs) may be used for nonsterile compounding if they are dedicated for nonsterile compounding; if they are used for occasional nonsterile compounding, Class II BSCs or CACIs must undergo thorough cleaning and disinfection before being used for sterile compounding)
Added recommendation/ Need to review language
New A36 For Sterile- Class II BSC or CACI Added recommendation/ Need to review language
New A37 All compounding shall be done in a separate area designated for hazardous drug compounding. A separate, negative pressure room or Containment Segregated Compounding Area (C-SCA) is allowed if it has at least 12 ACPH.
Added recommendation/ Need to review language
New A38 C-SCA must be cleanable (all of the architectural elements of a cleanroom; walls, floors, ceilings) and have accommodations for hand washing
Added recommendation/ Need to review language
Pharmacy Quality Assurance Commission 34 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
New A39 Hazardous drugs (HDs) shall not be stored, unpacked, compounded, or otherwise
manipulated in an area that is positive pressure relative to the surrounding area. Added
recommendation/ Need to review language
New A40 Low- and medium-risk CSPs may be prepared in a BSC located in a C-SCA, provided the beyond-use date of the CSP does not exceed 12 hours
Added recommendation/ Need to review language
New A41 CACI that meets the requirements in <797> may be used for hazardous drug compounding if it is placed in a C-SCA
Added recommendation/ Need to review language
New A42 Access to areas where HDs are stored and prepared shall be restricted to authorized staff Added recommendation/ Need to review language
New A43 Location of the HD compounding area shall be located away from break rooms and refreshment areas. Signage designating the hazard shall be prominently displayed before entry into the HD area
Added recommendation/ Need to review language
New A44 BSC or CACI used for the preparation of HDs shall not be used for the preparation of a non-HD unless the non-HD preparation is placed into a protective outer wrapper before removal from
Added recommen
Pharmacy Quality Assurance Commission 35 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
the Containment Primary Engineering Control (C-PEC) and is labeled to require PPE handling precautions
dation/ Need to review language
New A45 Containment Primary Engineering Controls (C-PECs) – Shall be externally vented and placed in a restricted access segregated room which has a minimum negative pressure of 0.01 inches of water column
Added recommendation/ Need to review language
New A46 Containment Secondary Engineering Controls (C-SECs) – Shall be vented to the outside air through HEPA filtration
Added recommendation/ Need to review language
New A47 For both Sterile and Nonsterile HD compounding, a sink shall be available for hand washing. It shall not be within an ISO Class 7 buffer area.
Added recommendation/ Need to review language
New A48 For Nonsterile Compounding – Shall be performed in a C-PEC that provides personnel and environmental protection (i.e., Class I BSC or CVE). The C-PEC shall be externally vented. (Unidirectional airflow within the C-PEC is not required)
Added recommendation/ Need to review language
New A49 For Nonsterile Compounding – The C-PEC shall be placed in a room that is physically separated (i.e., a different room from other preparation areas) but does not need to be ISO 7 nor have HEPA-filtered air (Minimum of 12 ACPH, maintained at a negative pressure of at least 0.01 inches of water column and all the architectural finish requirements prescribed in
Added recommendation/ Need to
Pharmacy Quality Assurance Commission 36 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
<797> review
language New A50 For Sterile Compounding – Shall be performed in a C-PEC that provides an ISO Class 5 critical
area and shall be used in conjunction with aseptic practices specified for the appropriate risk levels (i.e., Class II and III BSCs and CACIs). The airflow shall be unidirectional (laminar flow) and the “first air” at the face of the filter is free from airborne particulate contamination
Added recommendation/ Need to review language
New A51 For Sterile Compounding – C-PEC placement in a C-SEC that meets ISO Class 7 is preferred, but if a C-PEC is placed in a room with air quality worse than ISO Class 7, the BUD of all CSOs prepared in that area may need to be limited to 12 h, depending on the type of C-PEC used
Added recommendation/ Need to review language
New A52 Garbing and gloving requirements shall be used for compounding and HD (nonsterile and sterile) in any setting and when using any and all C-PECs
Added recommendation/ Need to review language
New A53 Gloves used shall be labeled as ASTM-tested chemotherapy gloves, be power-free and free of physical defects
Added recommendation/ Need to review language
New A54 Wearing two pairs of gloves is required when compounding, administering, managing a spill and disposing of HDs. For sterile preparations, the outer glove shall be sterile. Change gloves every 30 minutes or when torn, punctured or contaminated
Added recommendation/ Need to review language
Pharmacy Quality Assurance Commission 37 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
New A55 When working within a CACI, the outer glove (over the isolator glove) shall be a sterile,
powder free, ASTM-tested chemotherapy glove Added
recommendation/ Need to review language
New A56 Hand hygiene shall be performed before donning gloves and immediately after removal of gloves
Added recommendation/ Need to review language
New A57 Disposable gowns that protect from spills and splashes of HDs and waste material, that have been tested to resist permeability by HDs, shall be worn when handling HDs (Absorbent materials are not appropriate outer wear when handling HDs)
Added recommendation/ Need to review language
New A58 Head, hair and shoe covers shall be worn in HD compounding areas. Shoe covers are not worn outside the HD compounding area in order to avoid spreading drug contamination to other areas
Added recommendation/ Need to review language
New A59 Consider all PPE worn when handling HDs as being contaminated with trace quantities of HDs and worn PPE should not be placed into red bag or red sharps containers, but disposed of accordingly
Added recommendation/ Need to review language
New A60 HDs should be received from the supplier sealed in impervious plastic and should be immediately delivered to the C-SEC. HDs shall only be stored in areas with appropriate
Added / Need to
Pharmacy Quality Assurance Commission 38 2/19/2016 (Draft)

Sterile Compounding [USP <797>] Self-Assessment Compliance Checklist USP <797> Requirements and <800> Recommendations
Old # New # Compliant Non-Compliant
Non-Applicable (N/A)
Notes
ventilation controls and handled with ASTM-tested, powder-free chemotherapy gloves review
language New A61 C-PECs used for compounding HDs shall be disinfected at the beginning of the workday,
between batches of compounding medications, at the beginning of each subsequent shift (if compounding takes place over an extended period of time), routinely during compounding, and after anytime the C-PEC has been powered off
Added recommendation/ Need to review language
New A62 For BSCs and CACIs, the area under the work tray shall be cleaned at least monthly to reduce the contamination level (when cleaning a CACI, donning a respirator when opening the front of the cabinet is necessary)
Added recommendation/ Need to review language
New A63 Each entity shall have a compounding supervisor or designated individual responsible for developing and implementing appropriate procedures, overseeing facility compliance with applicable laws, regulations and standards; ensuring competency of personnel and assuring environmental control of the compounding areas
Added recommendation/ Need to review language
Pharmacy Quality Assurance Commission 39 2/19/2016 (Draft)
![Pharmacy Quality Assurance Commission - Home ... Quality Assurance Commission Sterile Compounding [USP ] Self-Assessment Compliance Checklist Introduction: (introduction](https://static.fdocuments.net/doc/165x107/5ab389b47f8b9aea528e4fe1/pharmacy-quality-assurance-commission-home-quality-assurance-commission-sterile.jpg)

















