Pharmacy Prior Authorization Oncology Detailed … Provider Documents... · Pharmacy Prior...
19
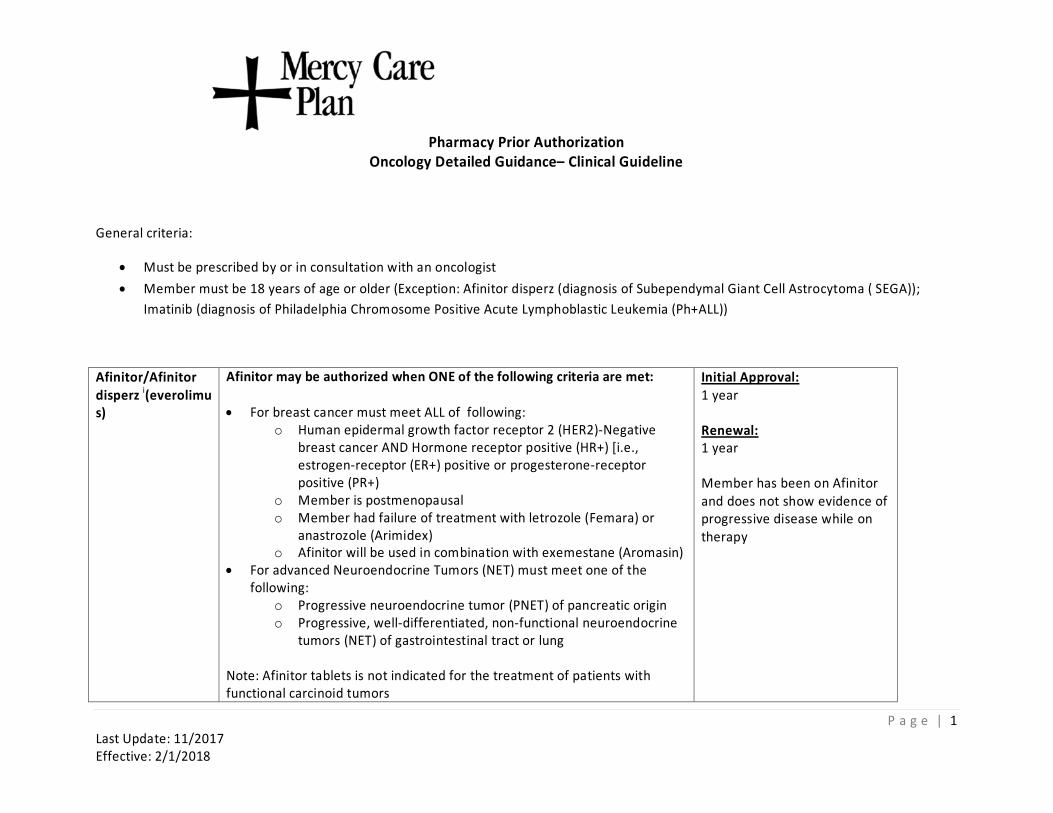
Pharmacy Prior Authorization Oncology Detailed Guidance– Clinical Guideline General criteria: • Must be prescribed by or in consultation with an oncologist • Member must be 18 years of age or older (Exception: Afinitor disperz (diagnosis of Subependymal Giant Cell Astrocytoma ( SEGA)); Imatinib (diagnosis of Philadelphia Chromosome Positive Acute Lymphoblastic Leukemia (Ph+ALL)) Afinitor/Afinitor disperz i (everolimu s) Afinitor may be authorized when ONE of the following criteria are met: • For breast cancer must meet ALL of following: o Human epidermal growth factor receptor 2 (HER2)-Negative breast cancer AND Hormone receptor positive (HR+) [i.e., estrogen-receptor (ER+) positive or progesterone-receptor positive (PR+) o Member is postmenopausal o Member had failure of treatment with letrozole (Femara) or anastrozole (Arimidex) o Afinitor will be used in combination with exemestane (Aromasin) • For advanced Neuroendocrine Tumors (NET) must meet one of the following: o Progressive neuroendocrine tumor (PNET) of pancreatic origin o Progressive, well-differentiated, non-functional neuroendocrine tumors (NET) of gastrointestinal tract or lung Note: Afinitor tablets is not indicated for the treatment of patients with functional carcinoid tumors Initial Approval: 1 year Renewal: 1 year Member has been on Afinitor and does not show evidence of progressive disease while on therapy Page | 1 Last Update: 11/2017 Effective: 2/1/2018
Transcript of Pharmacy Prior Authorization Oncology Detailed … Provider Documents... · Pharmacy Prior...
Pharmacy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
General criteria:
• Must be prescribed by or in consultation with an oncologist • Member must be 18 years of age or older (Exception: Afinitor disperz (diagnosis of Subependymal Giant Cell Astrocytoma ( SEGA));
Imatinib (diagnosis of Philadelphia Chromosome Positive Acute Lymphoblastic Leukemia (Ph+ALL))
Afinitor/Afinitor disperz i(everolimu s)
Afinitor may be authorized when ONE of the following criteria are met:
• For breast cancer must meet ALL of following: o Human epidermal growth factor receptor 2 (HER2)-Negative
breast cancer AND Hormone receptor positive (HR+) [i.e., estrogen-receptor (ER+) positive or progesterone-receptor positive (PR+)
o Member is postmenopausal o Member had failure of treatment with letrozole (Femara) or
anastrozole (Arimidex) o Afinitor will be used in combination with exemestane (Aromasin)
• For advanced Neuroendocrine Tumors (NET) must meet one of the following:
o Progressive neuroendocrine tumor (PNET) of pancreatic origin o Progressive, well-differentiated, non-functional neuroendocrine
tumors (NET) of gastrointestinal tract or lung
Note: Afinitor tablets is not indicated for the treatment of patients with functional carcinoid tumors
Initial Approval: 1 year
Renewal: 1 year
Member has been on Afinitor and does not show evidence of progressive disease while on therapy
P a g e | 1 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy P
rior Authorization Oncology Detailed Guidance– Clinical Guideline
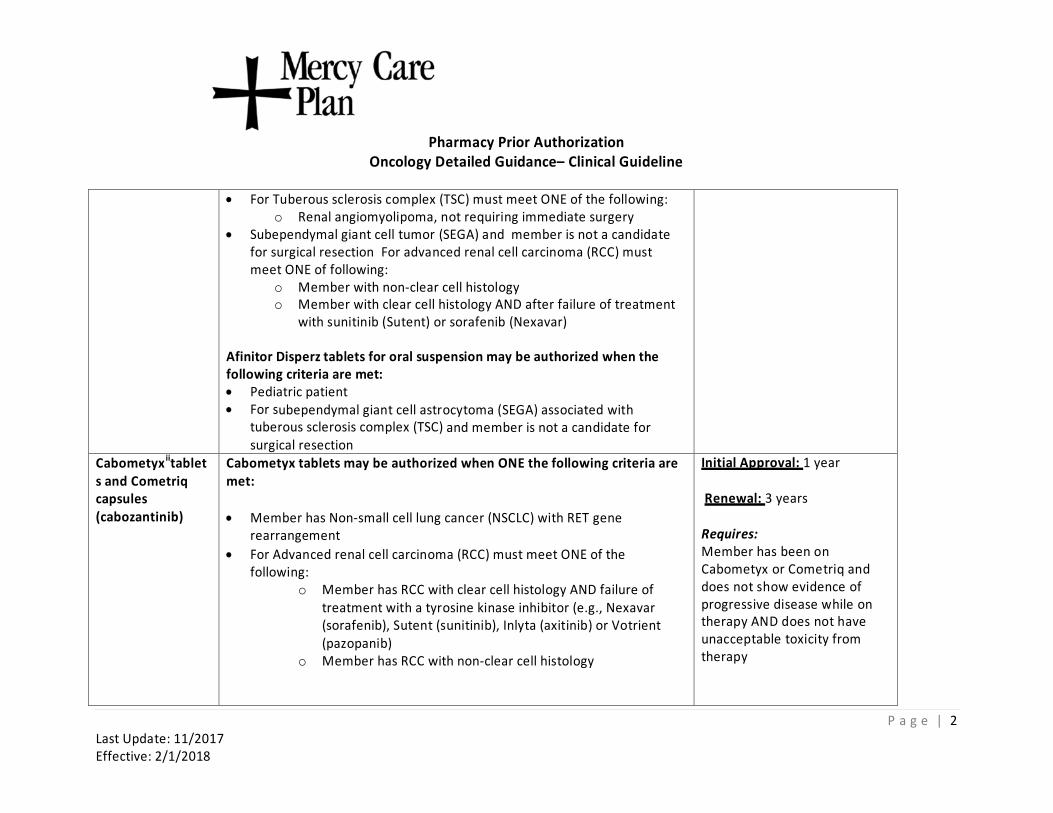
• For Tuberous sclerosis complex (TSC) must meet ONE of the following: o Renal angiomyolipoma, not requiring immediate surgery
• Subependymal giant cell tumor (SEGA) and member is not a candidate for surgical resection For advanced renal cell carcinoma (RCC) must meet ONE of following:
o Member with non-clear cell histology o Member with clear cell histology AND after failure of treatment
with sunitinib (Sutent) or sorafenib (Nexavar)
Afinitor Disperz tablets for oral suspension may be authorized when the following criteria are met: • Pediatric patient • For subependymal giant cell astrocytoma (SEGA) associated with
tuberous sclerosis complex (TSC) and member is not a candidate for surgical resection
Cabometyxiitablet s and Cometriq capsules (cabozantinib)
Cabometyx tablets may be authorized when ONE the following criteria are met:
• Member has Non-small cell lung cancer (NSCLC) with RET gene rearrangement
• For Advanced renal cell carcinoma (RCC) must meet ONE of the following:
o Member has RCC with clear cell histology AND failure of treatment with a tyrosine kinase inhibitor (e.g., Nexavar (sorafenib), Sutent (sunitinib), Inlyta (axitinib) or Votrient (pazopanib)
o Member has RCC with non-clear cell histology
Initial Approval: 1 year
Renewal: 3 years
Requires: Member has been on Cabometyx or Cometriq and does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
P a g e | 2 Last Update: 11/2017 Effective: 2/1/2018
Pharma
cy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
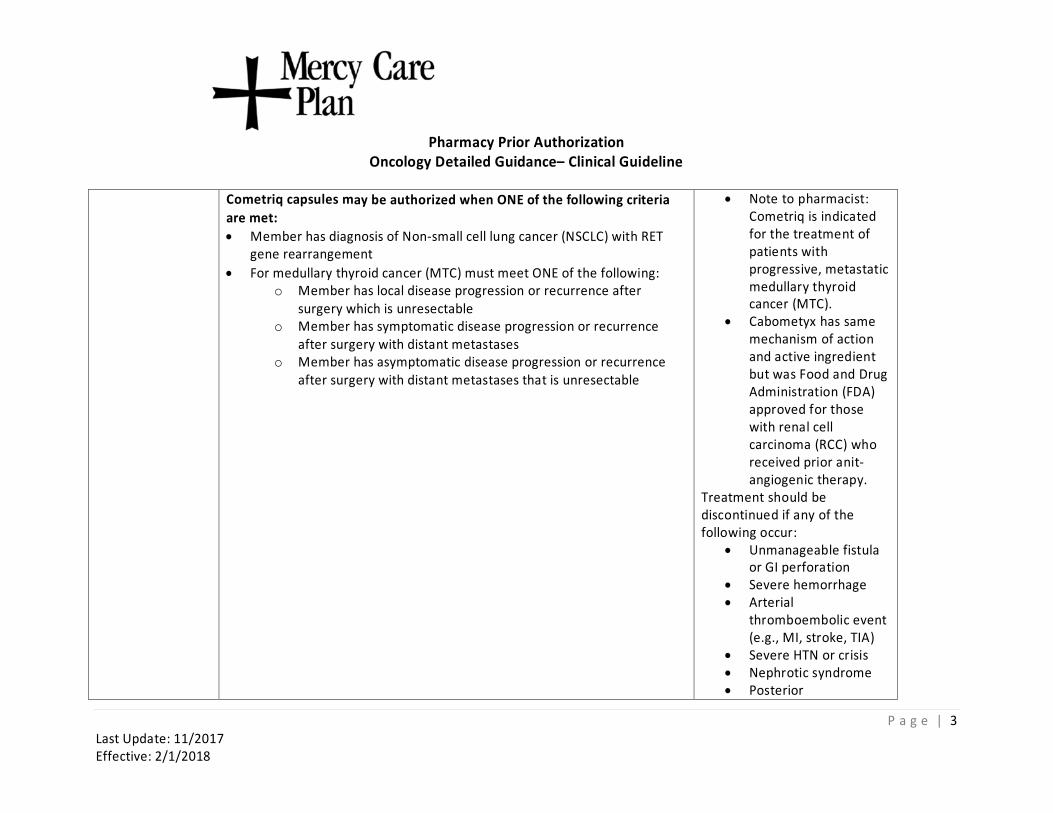
Cometriq capsules may be authorized when ONE of the following criteria are met: • Member has diagnosis of Non-small cell lung cancer (NSCLC) with RET
gene rearrangement • For medullary thyroid cancer (MTC) must meet ONE of the following:
o Member has local disease progression or recurrence after surgery which is unresectable
o Member has symptomatic disease progression or recurrence after surgery with distant metastases
o Member has asymptomatic disease progression or recurrence after surgery with distant metastases that is unresectable
• Note to pharmacist: Cometriq is indicated for the treatment of patients with progressive, metastatic medullary thyroid cancer (MTC).
• Cabometyx has same mechanism of action and active ingredient but was Food and Drug Administration (FDA) approved for those with renal cell carcinoma (RCC) who received prior anitangiogenic therapy.
Treatment should be discontinued if any of the following occur: • Unmanageable fistula
or GI perforation • Severe hemorrhage • Arterial
thromboembolic event (e.g., MI, stroke, TIA)
• Severe HTN or crisis • Nephrotic syndrome • Posterior
P a g e | 3 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy Prior Aut
horization Oncology Detailed Guidance– Clinical Guideline
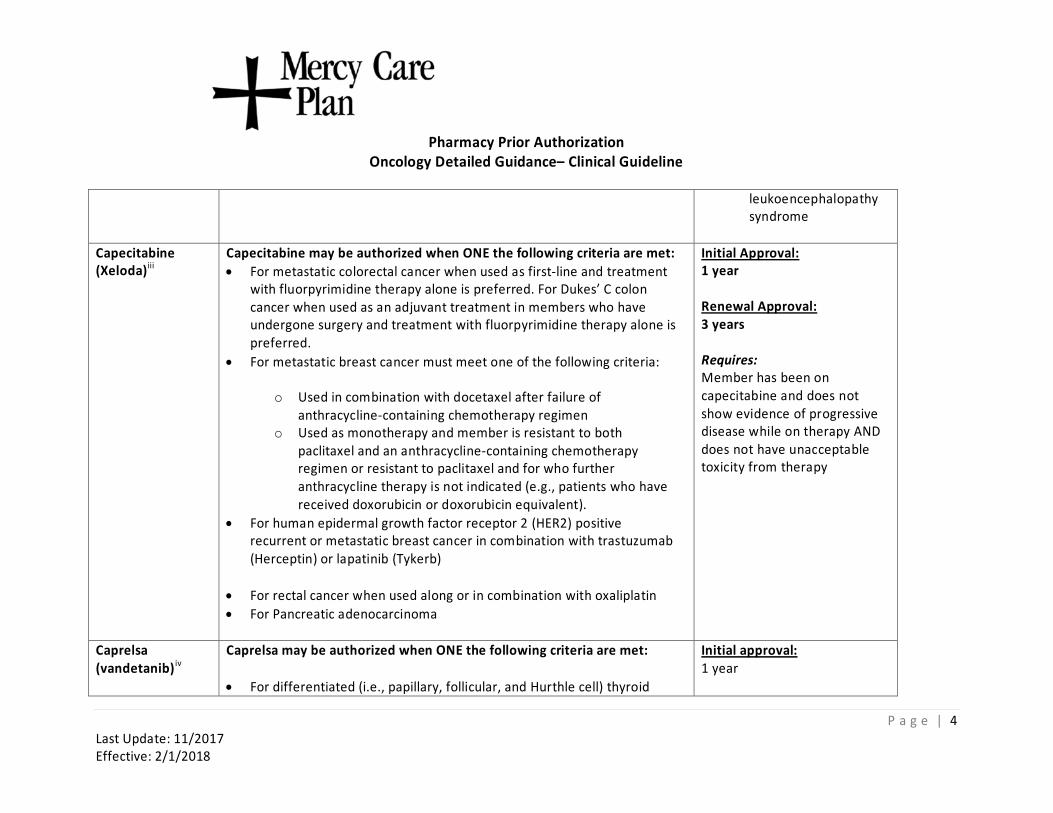
leukoencephalopathy syndrome
Capecitabine (Xeloda)iii
Capecitabine may be authorized when ONE the following criteria are met:• For metastatic colorectal cancer when used as first-line and treatment
with fluorpyrimidine therapy alone is preferred. For Dukes’ C colon cancer when used as an adjuvant treatment in members who have undergone surgery and treatment with fluorpyrimidine therapy alone is preferred.
• For metastatic breast cancer must meet one of the following criteria:
o Used in combination with docetaxel after failure of anthracycline-containing chemotherapy regimen
o Used as monotherapy and member is resistant to both paclitaxel and an anthracycline-containing chemotherapy regimen or resistant to paclitaxel and for who further anthracycline therapy is not indicated (e.g., patients who have received doxorubicin or doxorubicin equivalent).
• For human epidermal growth factor receptor 2 (HER2) positive recurrent or metastatic breast cancer in combination with trastuzumab (Herceptin) or lapatinib (Tykerb)
• For rectal cancer when used along or in combination with oxaliplatin • For Pancreatic adenocarcinoma
Initial Approval: 1 year
Renewal Approval: 3 years
Requires: Member has been on capecitabine and does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
Caprelsa (vandetanib) iv
Caprelsa may be authorized when ONE the following criteria are met:
• For differentiated (i.e., papillary, follicular, and Hurthle cell) thyroid
Initial approval: 1 year
P a g e | 4 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy Pri
or Authorization Oncology Detailed Guidance– Clinical Guideline
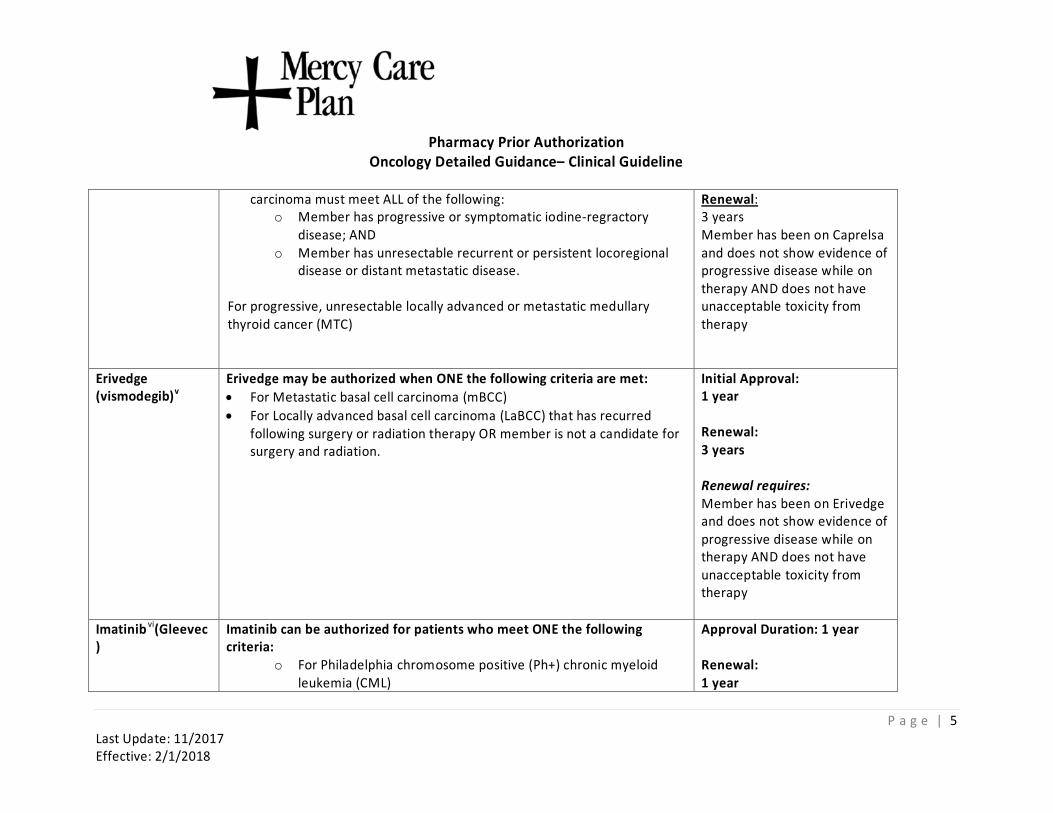
carcinoma must meet ALL of the following: o Member has progressive or symptomatic iodine-regractory
disease; AND o Member has unresectable recurrent or persistent locoregional
disease or distant metastatic disease.
For progressive, unresectable locally advanced or metastatic medullary thyroid cancer (MTC)
Renewal: 3 years Member has been on Caprelsa and does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
Erivedge (vismodegib)v
Erivedge may be authorized when ONE the following criteria are met: • For Metastatic basal cell carcinoma (mBCC) • For Locally advanced basal cell carcinoma (LaBCC) that has recurred
following surgery or radiation therapy OR member is not a candidate for surgery and radiation.
Initial Approval: 1 year
Renewal: 3 years
Renewal requires: Member has been on Erivedge and does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
Imatinib vi(Gleevec )
Imatinib can be authorized for patients who meet ONE the following criteria:
o For Philadelphia chromosome positive (Ph+) chronic myeloid leukemia (CML)
Approval Duration: 1 year Renewal: 1 year
P a g e | 5 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy Pri
or Authorization Oncology Detailed Guidance– Clinical Guideline
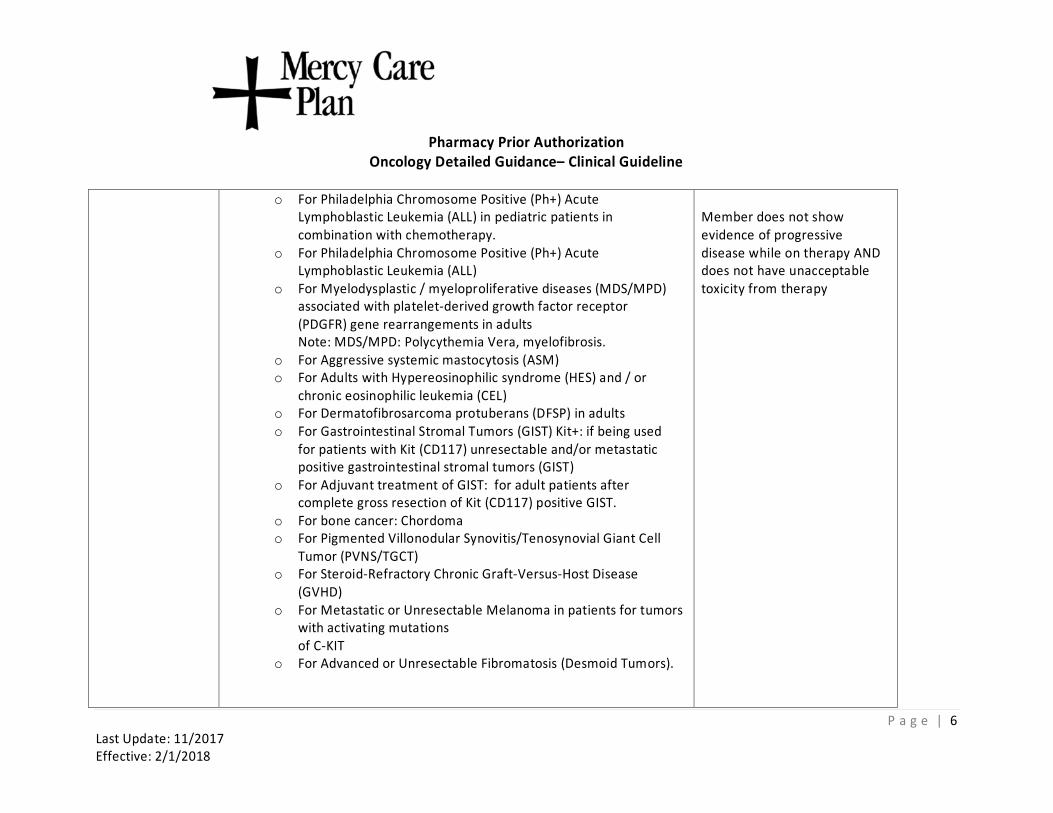
o For Philadelphia Chromosome Positive (Ph+) Acute Lymphoblastic Leukemia (ALL) in pediatric patients in combination with chemotherapy.
o For Philadelphia Chromosome Positive (Ph+) Acute Lymphoblastic Leukemia (ALL)
o For Myelodysplastic / myeloproliferative diseases (MDS/MPD) associated with platelet-derived growth factor receptor (PDGFR) gene rearrangements in adults Note: MDS/MPD: Polycythemia Vera, myelofibrosis.
o For Aggressive systemic mastocytosis (ASM) o For Adults with Hypereosinophilic syndrome (HES) and / or
chronic eosinophilic leukemia (CEL) o For Dermatofibrosarcoma protuberans (DFSP) in adults o For Gastrointestinal Stromal Tumors (GIST) Kit+: if being used
for patients with Kit (CD117) unresectable and/or metastatic positive gastrointestinal stromal tumors (GIST)
o For Adjuvant treatment of GIST: for adult patients after complete gross resection of Kit (CD117) positive GIST.
o For bone cancer: Chordoma o For Pigmented Villonodular Synovitis/Tenosynovial Giant Cell
Tumor (PVNS/TGCT) o For Steroid-Refractory Chronic Graft-Versus-Host Disease
(GVHD) o For Metastatic or Unresectable Melanoma in patients for tumors
with activating mutations of C-KIT
o For Advanced or Unresectable Fibromatosis (Desmoid Tumors).
Member does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
P a g e | 6 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy P
rior Authorization Oncology Detailed Guidance– Clinical Guideline
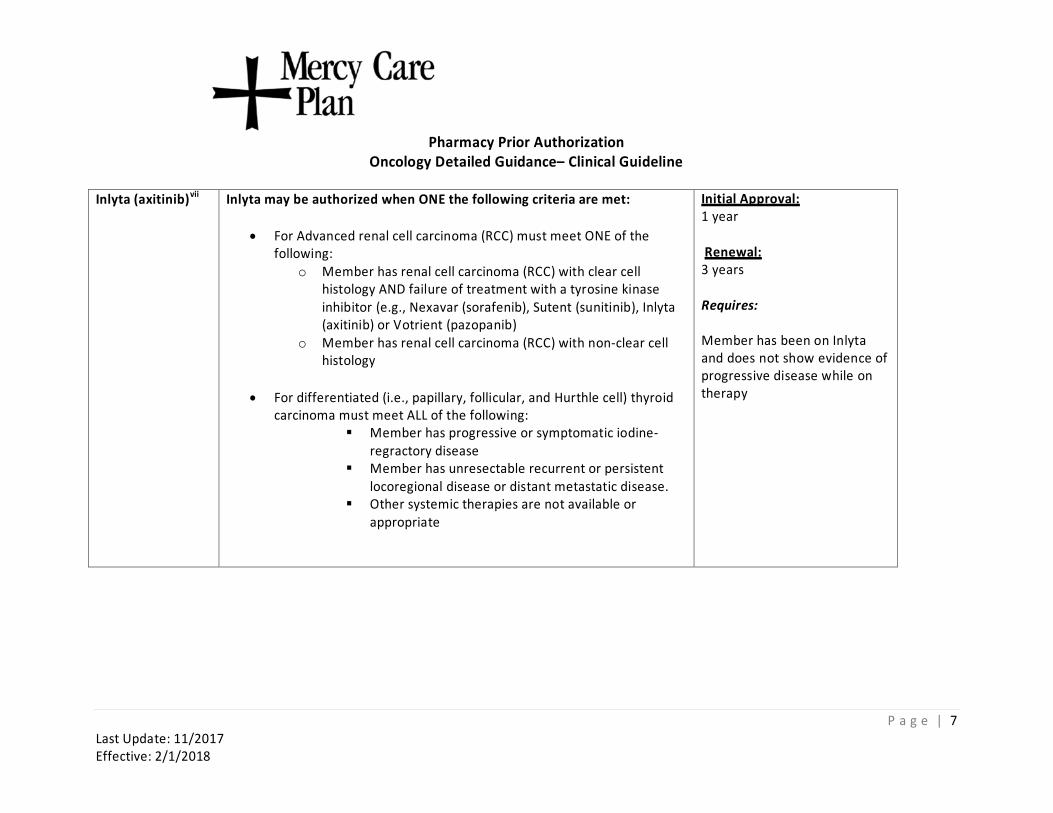
Inlyta (axitinib)vii Inlyta may be authorized when ONE the following criteria are met:
• For Advanced renal cell carcinoma (RCC) must meet ONE of the following:
o Member has renal cell carcinoma (RCC) with clear cell histology AND failure of treatment with a tyrosine kinase inhibitor (e.g., Nexavar (sorafenib), Sutent (sunitinib), Inlyta (axitinib) or Votrient (pazopanib)
o Member has renal cell carcinoma (RCC) with non-clear cell histology
• For differentiated (i.e., papillary, follicular, and Hurthle cell) thyroid carcinoma must meet ALL of the following:
Member has progressive or symptomatic iodineregractory disease
Member has unresectable recurrent or persistent locoregional disease or distant metastatic disease.
Other systemic therapies are not available or appropriate
Initial Approval: 1 year
Renewal: 3 years
Requires:
Member has been on Inlyta and does not show evidence of progressive disease while on therapy
P a g e | 7 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
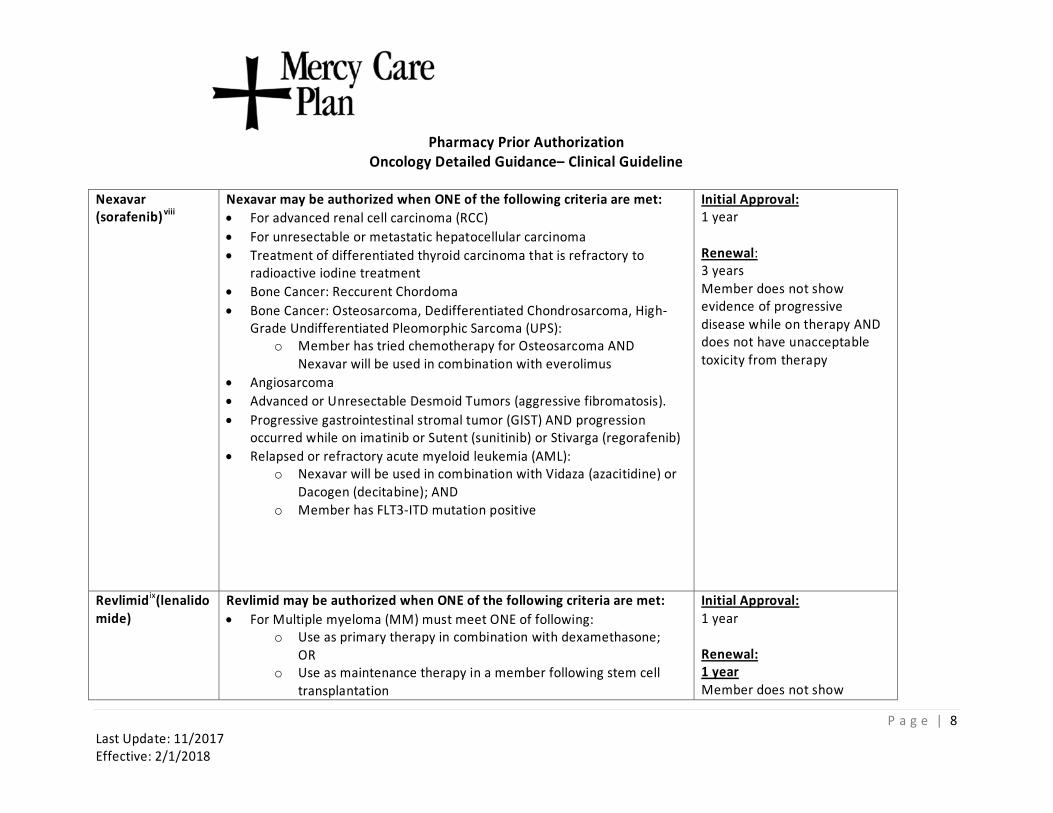
Nexavar (sorafenib)viii
Nexavar may be authorized when ONE of the following criteria are met: • For advanced renal cell carcinoma (RCC) • For unresectable or metastatic hepatocellular carcinoma • Treatment of differentiated thyroid carcinoma that is refractory to
radioactive iodine treatment • Bone Cancer: Reccurent Chordoma • Bone Cancer: Osteosarcoma, Dedifferentiated Chondrosarcoma, High-
Grade Undifferentiated Pleomorphic Sarcoma (UPS): o Member has tried chemotherapy for Osteosarcoma AND
Nexavar will be used in combination with everolimus • Angiosarcoma • Advanced or Unresectable Desmoid Tumors (aggressive fibromatosis). • Progressive gastrointestinal stromal tumor (GIST) AND progression
occurred while on imatinib or Sutent (sunitinib) or Stivarga (regorafenib) • Relapsed or refractory acute myeloid leukemia (AML):
o Nexavar will be used in combination with Vidaza (azacitidine) or Dacogen (decitabine); AND
o Member has FLT3-ITD mutation positive
Initial Approval: 1 year
Renewal: 3 years Member does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
Revlimidix(lenalido mide)
Revlimid may be authorized when ONE of the following criteria are met: •
For Multiple myeloma (MM) must meet ONE of following: o Use as primary therapy in combination with dexamethasone;
OR o Use as maintenance therapy in a member following stem cell
transplantation
Initial Approval: 1 year
Renewal: 1 year Member does not show
P a g e | 8 Last Update: 11/2017 Effective: 2/1/2018
Pharmac
•
y Prior Authorization Oncology Detailed Guidance– Clinical Guideline
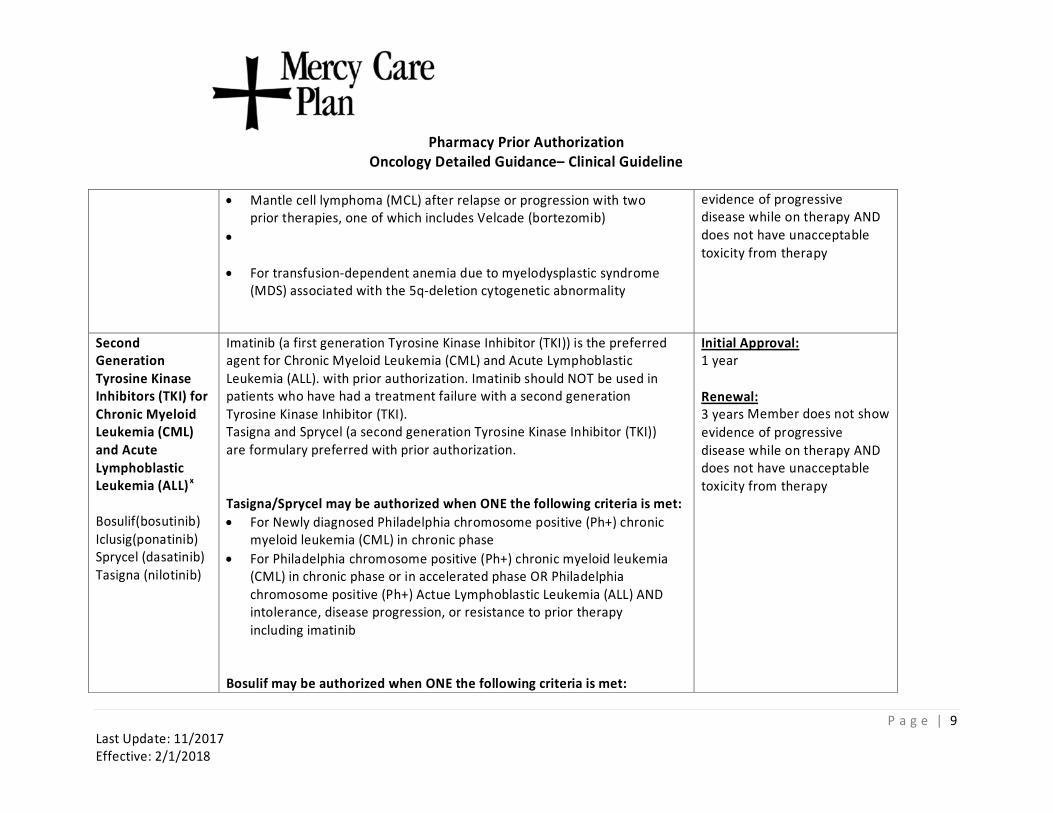
• Mantle cell lymphoma (MCL) after relapse or progression with two prior therapies, one of which includes Velcade (bortezomib)
• For transfusion-dependent anemia due to myelodysplastic syndrome (MDS) associated with the 5q-deletion cytogenetic abnormality
evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
Second Generation Tyrosine Kinase Inhibitors (TKI) forChronic Myeloid Leukemia (CML) and Acute Lymphoblastic Leukemia (ALL)x Bosulif(bosutinib) Iclusig(ponatinib) Sprycel (dasatinib) Tasigna (nilotinib)
Imatinib (a first generation Tyrosine Kinase Inhibitor (TKI)) is the preferred agent for Chronic Myeloid Leukemia (CML) and Acute Lymphoblastic Leukemia (ALL). with prior authorization. Imatinib should NOT be used in patients who have had a treatment failure with a second generation Tyrosine Kinase Inhibitor (TKI). Tasigna and Sprycel (a second generation Tyrosine Kinase Inhibitor (TKI)) are formulary preferred with prior authorization.
Tasigna/Sprycel may be authorized when ONE the following criteria is met: •
For Newly diagnosed Philadelphia chromosome positive (Ph+) chronic myeloid leukemia (CML) in chronic phase
• For Philadelphia chromosome positive (Ph+) chronic myeloid leukemia (CML) in chronic phase or in accelerated phase OR Philadelphia chromosome positive (Ph+) Actue Lymphoblastic Leukemia (ALL) AND intolerance, disease progression, or resistance to prior therapy including imatinib
Bosulif may be authorized when ONE the following criteria is met:
Initial Approval: 1 year Renewal: 3 years Member does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
P a g e | 9 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy
Prior Authorization Oncology Detailed Guidance– Clinical Guideline
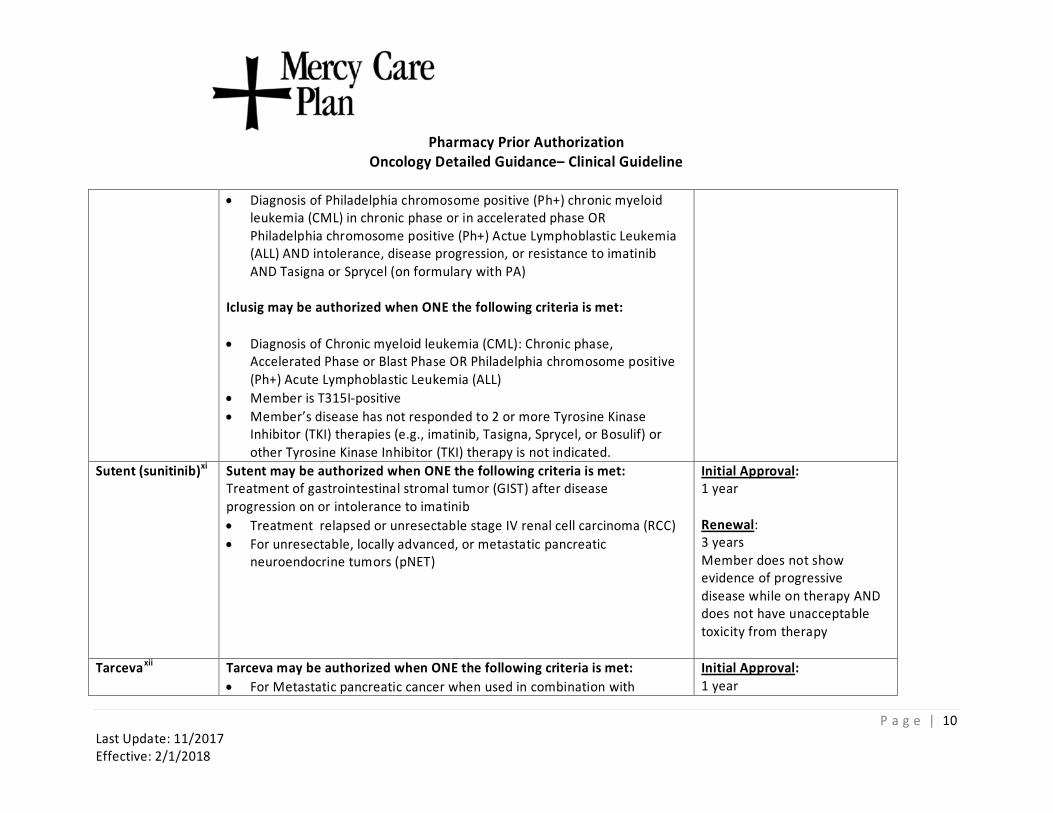
• Diagnosis of Philadelphia chromosome positive (Ph+) chronic myeloid leukemia (CML) in chronic phase or in accelerated phase OR Philadelphia chromosome positive (Ph+) Actue Lymphoblastic Leukemia (ALL) AND intolerance, disease progression, or resistance to imatinib AND Tasigna or Sprycel (on formulary with PA)
Iclusig may be authorized when ONE the following criteria is met: • Diagnosis of Chronic myeloid leukemia (CML): Chronic phase,
Accelerated Phase or Blast Phase OR Philadelphia chromosome positive (Ph+) Acute Lymphoblastic Leukemia (ALL)
• Member is T315I-positive • Member’s disease has not responded to 2 or more Tyrosine Kinase
Inhibitor (TKI) therapies (e.g., imatinib, Tasigna, Sprycel, or Bosulif) or other Tyrosine Kinase Inhibitor (TKI) therapy is not indicated.
Sutent (sunitinib)xi Sutent may be authorized when ONE the following criteria is met: Treatment of gastrointestinal stromal tumor (GIST) after disease progression on or intolerance to imatinib •
Treatment relapsed or unresectable stage IV renal cell carcinoma (RCC) • For unresectable, locally advanced, or metastatic pancreatic
neuroendocrine tumors (pNET)
Initial Approval: 1 year
Renewal: 3 years Member does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
Tarcevaxii Tarceva may be authorized when ONE the following criteria is met: • For Metastatic pancreatic cancer when used in combination with
Initial Approval: 1 year
P a g e | 10 Last Update: 11/2017 Effective: 2/1/2018
Pharma
cy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
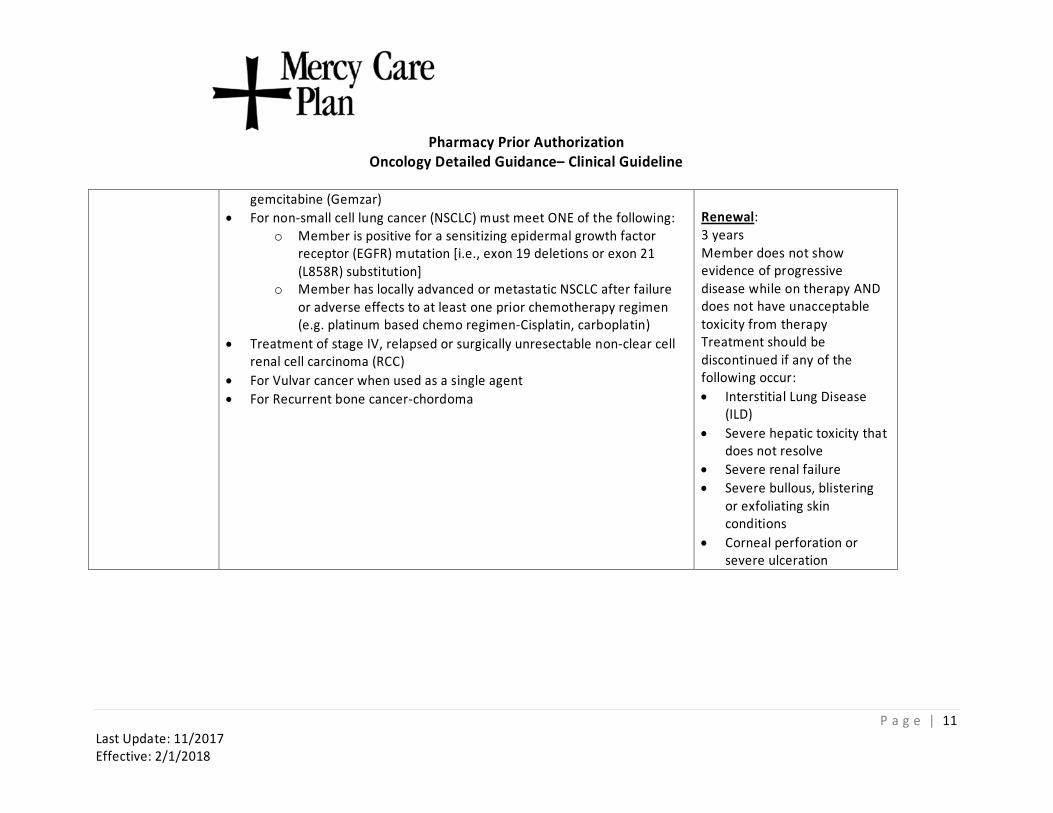
gemcitabine (Gemzar) •
For non-small cell lung cancer (NSCLC) must meet ONE of the following: o Member is positive for a sensitizing epidermal growth factor
receptor (EGFR) mutation [i.e., exon 19 deletions or exon 21 (L858R) substitution]
o Member has locally advanced or metastatic NSCLC after failure or adverse effects to at least one prior chemotherapy regimen (e.g. platinum based chemo regimen-Cisplatin, carboplatin)
• Treatment of stage IV, relapsed or surgically unresectable non-clear cell renal cell carcinoma (RCC)
• For Vulvar cancer when used as a single agent • For Recurrent bone cancer-chordoma
Renewal: 3 years Member does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy Treatment should be discontinued if any of the following occur: •
Interstitial Lung Disease (ILD)
• Severe hepatic toxicity that does not resolve
• Severe renal failure • Severe bullous, blistering
or exfoliating skin conditions
• Corneal perforation or severe ulceration
P a g e | 11 Last Update: 11/2017 Effective: 2/1/2018
Phar
macy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
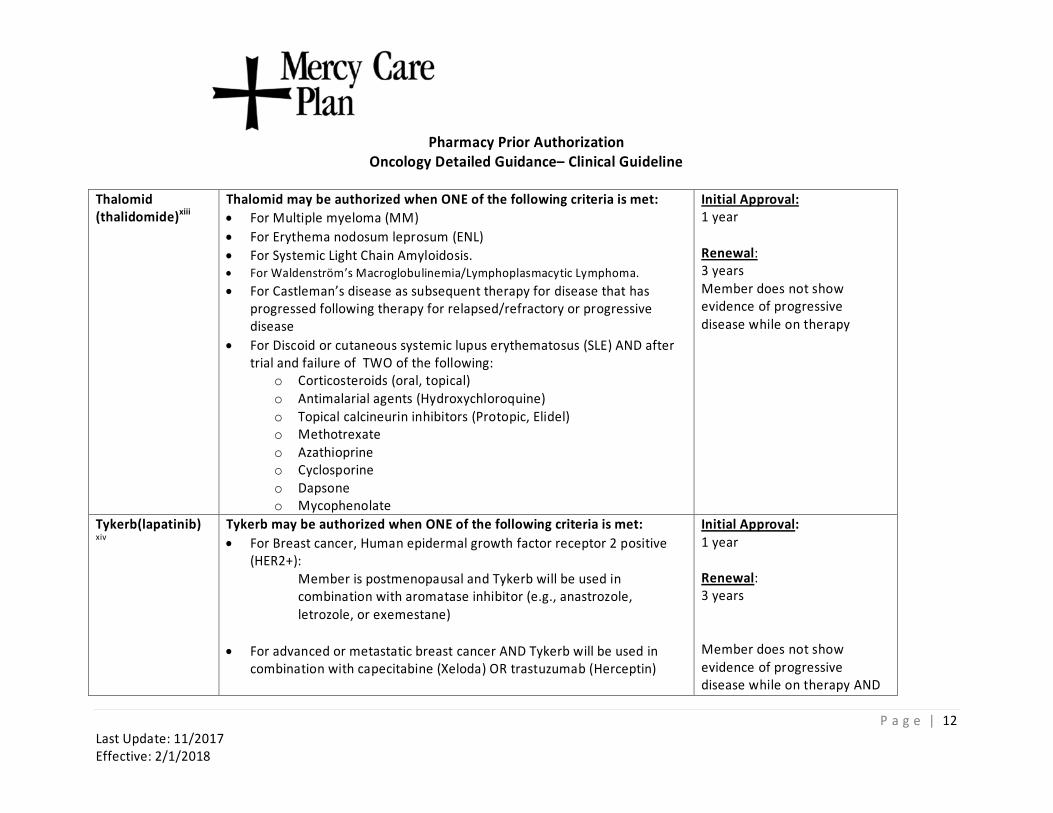
Thalomid (thalidomide)xiii
Thalomid may be authorized when ONE of the following criteria is met: • For Multiple myeloma (MM) • For Erythema nodosum leprosum (ENL) • For Systemic Light Chain Amyloidosis. • For Waldenström’s Macroglobulinemia/Lymphoplasmacytic Lymphoma. • For Castleman’s disease as subsequent therapy for disease that has
progressed following therapy for relapsed/refractory or progressive disease
• For Discoid or cutaneous systemic lupus erythematosus (SLE) AND after trial and failure of TWO of the following:
o Corticosteroids (oral, topical) o Antimalarial agents (Hydroxychloroquine) o Topical calcineurin inhibitors (Protopic, Elidel) o Methotrexate o Azathioprine o Cyclosporine o Dapsone o Mycophenolate
Initial Approval: 1 year Renewal: 3 years Member does not show evidence of progressive disease while on therapy
Tykerb(lapatinib) xiv
Tykerb may be authorized when ONE of the following criteria is met: •
For Breast cancer, Human epidermal growth factor receptor 2 positive (HER2+):
Member is postmenopausal and Tykerb will be used in combination with aromatase inhibitor (e.g., anastrozole, letrozole, or exemestane)
• For advanced or metastatic breast cancer AND Tykerb will be used in combination with capecitabine (Xeloda) OR trastuzumab (Herceptin)
Initial Approval: 1 year
Renewal: 3 years
Member does not show evidence of progressive disease while on therapy AND
P a g e | 12 Last Update: 11/2017 Effective: 2/1/2018
Pharmac
y Prior Authorization Oncology Detailed Guidance– Clinical Guideline
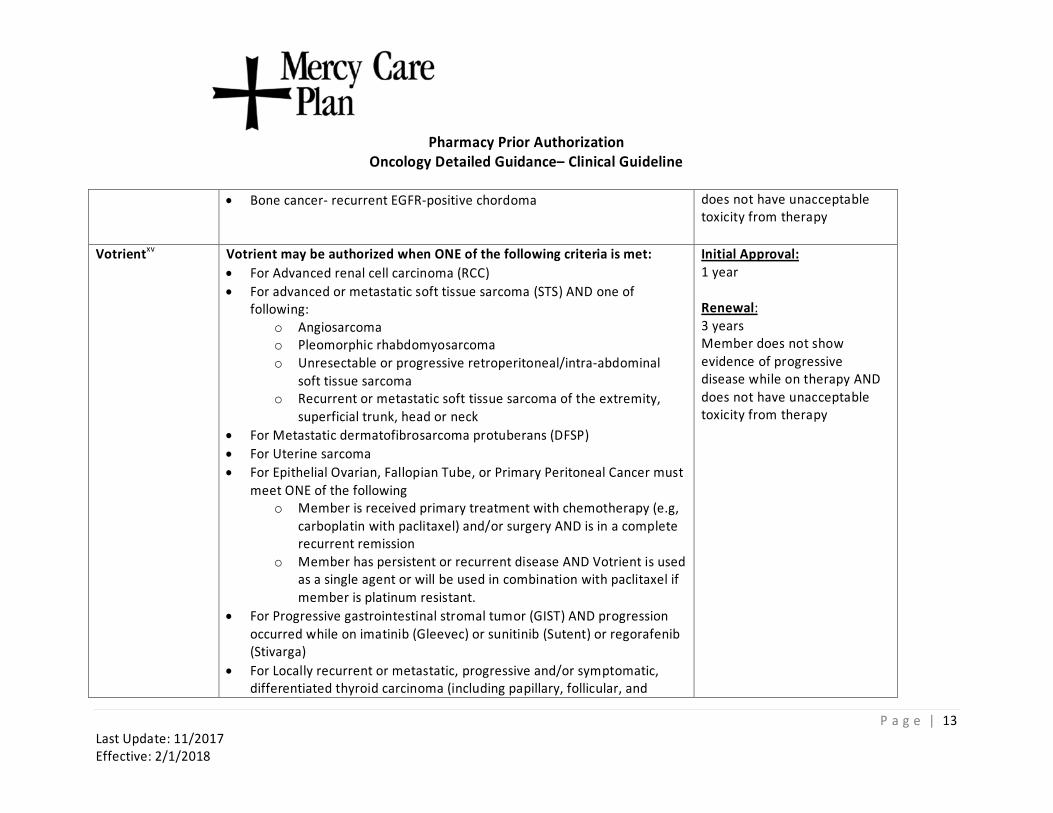
• Bone cancer- recurrent EGFR-positive chordoma does not have unacceptable toxicity from therapy
Votrientxv Votrient may be authorized when ONE of the following criteria is met: • For Advanced renal cell carcinoma (RCC) • For advanced or metastatic soft tissue sarcoma (STS) AND one of
following: o Angiosarcoma o Pleomorphic rhabdomyosarcoma o Unresectable or progressive retroperitoneal/intra-abdominal
soft tissue sarcoma o Recurrent or metastatic soft tissue sarcoma of the extremity,
superficial trunk, head or neck • For Metastatic dermatofibrosarcoma protuberans (DFSP) • For Uterine sarcoma • For Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer must
meet ONE of the following o Member is received primary treatment with chemotherapy (e.g,
carboplatin with paclitaxel) and/or surgery AND is in a complete recurrent remission
o Member has persistent or recurrent disease AND Votrient is used as a single agent or will be used in combination with paclitaxel if member is platinum resistant.
• For Progressive gastrointestinal stromal tumor (GIST) AND progression occurred while on imatinib (Gleevec) or sunitinib (Sutent) or regorafenib (Stivarga)
• For Locally recurrent or metastatic, progressive and/or symptomatic, differentiated thyroid carcinoma (including papillary, follicular, and
Initial Approval: 1 year
Renewal: 3 years Member does not show evidence of progressive disease while on therapy AND does not have unacceptable toxicity from therapy
P a g e | 13 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy P
rior Authorization Oncology Detailed Guidance– Clinical Guideline
Hurthle cell) refractory to radioactive iodine treatment, AND other systemic therapies are not available or are inappropriate
i Afinitor References: 1. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomized placebo-controlled phase III trial. The Lancet. 2008 2. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Kidney Cancer. http://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf Version 3.2015. Accessed September 12, 2017. 3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Breast Cancer. http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Version 3.2015. Accessed September 8, 2015. 4. Besalga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012 Feb 9;366(6):520-9. 5. National Guideline Clearinghouse (NGC). Guideline summary: Guidelines on renal cell carcinoma. In: National Guideline Clearinghouse (NGC).
http://www.guideline.gov/content.aspx?id=45321&search=advanced+renal+cell+carcinoma#Section420. Rockville (MD): Agency for Healthcare Research and Quality (AHRQ); cited 2015 August 10. Available: http://www.guideline.gov.
6. Owens, James. Tuberous sclerosis complex: Management. In UpToDate, Post TW (Ed.), Waltham, MA, (accessed on August 10,2015). 7. Torres, Vicente. Renal angiomyolipomas. In UpToDate, Post TW (Ed.), Waltham, MA, (accessed on August 10, 2015). 8. Chan Ang, Jennifer. Metastatic pancreatic neuroendocrine tumors and poorly differentiated gastroenteropancreatic neuroendocrine carcinomas: Systemic therapy
options to control tumor growth and symptoms of hormone hypersecretion. In UpToDate, Post TW (Ed.), Waltham, MA, (accessed August 10, 2015). 9. Ellis, Matthew. Treatment approach to metastatic hormone receptor-positive breast cancer: Endocrine therapy. In UpToDate, Post TW (Ed.), Waltham, MA, (accessed
August 10, 2015). 10. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Neuroendocrine Tumors. http://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf. Version 1.2015. Accessed September 8, 2015.
11. Afinitor (everolimus) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; February 2016. 12. Afinitor. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017.
ii Cabometyx References: 1. Cabometyx (cabozantinib) [package insert]. South San Francisco, CA; Exelixis, Inc: Revised May 2016. 2. Cometriq™ [prescribing information]. San Francisco, CA: Exelixis Inc; May 2016. 3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. http://www.nccn.org. Cabometyx/Cometriq.. Accessed September 2017.
iii Xeloda References
P a g e | 14 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
1. Xeloda [capecitabine] prescribing information. South San Francisco, CA: Genentech, inc. Updated: March, 2015. 2. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Colon Cancer. http://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Version 2.2016. Accessed December 17, 2015. 3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Anal Carcinoma. http://www.nccn.org/professionals/physician_gls/pdf/anal.pdf. Version 2.2015. Accessed November 4, 2015. 4. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Brest Cancer. http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Version 1.2016. Accessed December 17, 2015. 5. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Capetabine. http://www.nccn.org. Accessed September 11, 2017. iv Caprelsa References
1. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Caprelsa. http://www.nccn.org. Accessed September 11, 2017.
2. Aetna CPB: Antineoplastics Accessed August 2015 3. Vandetanib. In: Clinical Pharmacology Online. Atlanta, GA: Elsevier / Gold Standard; [Updated 7/30/2014;Accessed August 2015] http://clinicalpharmacology
ip.com/Forms/Monograph/monograph.aspx?cpnum=3722&sec=monindi&t=0 v Erivedge References
1. Erivedge® (vismodegib) full prescribing information. Genentech, Inc., South San Francisco, CA. Jan 2012. 2. Erivedge® medical letter. Genentech, Inc. Feb 6, 2012. 3. Basal Cell and Squamous Cell Skin Cancers. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology (National Comprehensive
Cancer Network (NCCN) Guidelines). Version 1.2012. National Comprehensive Cancer Network (NCCN) Website. 4. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: http://www.nccn.org. Erivedge. Accessed September, 11, 2017. 5. Sekulic A, Et al. A pivotal study evaluating efficacy and safety of the hedgehog pathway inhibitor (HPI) vismodegib (GDC-0449) in patients with locally advanced (la)
or metastatic (m) basal cell carcinoma (BCC). European Association of Dermato-Oncology (EADO) Abstract. 2011 vi Gleevec References
1. Gleevec [full prescribing information]. East Hanover, NJ: Novartis U.S.; Revised 02/2013 2. Gleevec. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 3. National Comprehensive Cancer Network (NCCN) Drugs and Biologics Compendium
http://www.nccn.org/professionals/drug_compendium/MatrixGenerator/Matrix.aspx?AID=18 accessed 3/18/2010, 3/24/11, 3/27/12 4. National Comprehensive Cancer Network. Practice Guidelines in Oncology – Chronic Myelogenous Leukemia, Version I.2014 09/09/13. 5. National Comprehensive Cancer Network. Practice Guidelines in Oncology – Acute Lymphoblastic Leukemia, Version I.2013 03/25/13. 6. Alvarado Y, Apostolidou E, Swords R, Giles FJ. Emerging therapeutic options for Philadelphia-positive acute lymphocytic leukemia. Expert Opin Emerg Drugs. 2007
Mar;12(1):165-79
P a g e | 15 Last Update: 11/2017 Effective: 2/1/2018
Pharm
acy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
7. National Institute for Clinical Excellence (NICE). Imatinib for the treatment of unresectable and/or metastatic gastro-intestinal stromal tumours. London (UK): National Institute for Clinical Excellence (NICE); 2004 Oct. 38 p.
8. Pardanani A, Ketterling RP, Brockman SR, et al: CHIC2 deletion, a surrogate for FIP1L1-PDGFRA fusion, occurs in systemic mastocytosis associated with eosinophilia and predicts response to imatinib mesylate therapy. Blood 2003 Nov 1; 102(9): 3093-6
9. McArthur G. Dermatofibrosarcoma Protuberans: Recent Clinical Progress. Ann Surg Oncol. 2007 Jul 24 10. Fletcher S, Bain B. Diagnosis and treatment of hypereosinophilic syndromes. Curr Opin Hematol. 2007 Jan;14(1):37-42
vii Inlyta References: 1. Inlyta (axitinib) [package insert]. NY, NY; Pfizer: Revised January 2012. 2. Rini BI, Escudier B, Tomczak P, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomized phase 3 trial. Lancet
2011;378:1931-39. 3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Kidney Cancer. http://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf Version 3.2015. Accessed September 8, 2015. 4. Inlyta. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017.
viii Nexavar References 1. Nexavar prescribing information. Bayer Healthcare Pharmaceuticals Inc.; Wayne, NJ: December 2012. 2. Nexavar. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 3. Bukowski R, Cella D, Gondek K, et al. Effects of sorafenib on symptoms and quality of life: results from a large randomized placebo-controlled study in renal cancer. Am
J Clin Oncol. 2007 Jun;30(3):220-7 4. Sorafenib, National Comprehensive Cancer Network (NCCN) Drugs and Biologics Compendium. [cited 3/25/2010]. Available from: URL:
http://www.nccn.org/professionals/ drug_compendium/MatrixGenerator/Matrix.aspx?AID=134. 5. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Kidney Cancer. Fort Washington, PA: National Comprehensive Cancer
Network, 2013. (Accessed March 4, 2013, at http://www.nccn.org/ professionals/ physician_gls/ PDF/kidney.pdf ) 6. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Hepatobiliary Cancer. Fort Washington, PA: National Comprehensive Cancer
Network, 2012. (Accessed March 4, 2013, at http://www.nccn.org/professionals/ physician_gls/pdf/hepatobiliary.pdf)) ix Revlimid References
1. Revlimid® (lenalidomide) prescribing information. Celgene Corp., June 2013. 2. Revlimid. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017.
3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Multiple Myeloma. http://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf. Version 2.2016. Accessed December 10, 2015.
4. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Myelodysplastic Syndrome. http://www.nccn.org/professionals/physician_gls/pdf/mds.pdf. Version 1.2016. Accessed December 10, 2015.
x Second Generation TKI References 1. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Chronic Myelogenous Leukemia. http://www.nccn.org/professionals/physician_gls/pdf/cml.pdf. Version 1.2015. Accessed September 8, 2015.
P a g e | 16 Last Update: 11/2017 Effective: 2/1/2018

Pharma
cy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
2. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Acute Lymphoblastic Leukemia. http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Version 1.2015. Accessed September 8, 2015.
3. Bosulif [full prescribing information]. New York, NY: Pfizer U.S.; Revised 09/2013. 4. Bosulif. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 5. Gleevec. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 6. Gleevec [full prescribing information]. East Hanover, NJ: Novartis U.S.; Revised 02/2013. 7. Sprycel. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 8. Tasigna. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 9. Cortes JE, et al, Bosutinib Versus Imatinib in Newly Diagnosed Chronic-Phase Chronic Myeloid Leukemia: Results From the BELA Trial. J Clin Oncol, 2012;30(28):3486
3492. 10. Cortes JE, et al, Safety and efficacy of bosutinib (SKI-606) in chronic phase Philadelphia chromosome-positive chronic myeloid leukemia patients with resistance or
intolerance to imatinib. Blood. 2011;118(17): 4567-4576. 11. Khoury HJ, et al, Bosutinib is active in chronic phase chronic myeloid leukemia after imatinib and dasatinib and/or nilotinib therapy failure. Blood, 2012;119(15)3403
3412. 12. Shieh MP, Mitsuhashi M, LillyM. Moving on up: Second-Line Agents as Initial Treatment for Newly-Diagnosed Patients with Chronic Phase CML. Clin Med Insights Oncol,
2011;5:185-199. 13. Antineoplastics - Pharmacy Clinical Policy Bulletins Aetna Non-Medicare Prescription Drug Plan. Aetna Clinical Pharmacy Bulletins
xi Sutent References 1. Sutent prescribing information. Pfizer Inc.;New York, NY; Updated 5/2015. 2. Sutent. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017.
3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Kidney Cancer. http://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf. Version 1.2016. Accessed October 30, 2015.
4. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Neuroendocrine Tumors. http://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf. Version 1.2015. Accessed October 30, 2015.
5. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Soft Tissue Sarcoma. http://www.nccn.org/professionals/physician_gls/pdf/sarcoma.pdf. Version 1.2015. Accessed October 30, 2015.
xii Tarceva References 1. Tarceva® (erlotinib) prescribing information. Genentech, Inc.: South San Francisco, CA. Updated: May, 2015. 2. Tarceva. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice
Guideline in Oncology: Kidney Cancer. http://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf. Version 1.2016. Accessed October 30, 2015.
P a g e | 17 Last Update: 11/2017 Effective: 2/1/2018
Pharmacy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
4. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Pancreatic Adenocarcinoma. http://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf. Version 2.2015. Accessed December 15, 2015.
5. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical Practice Guideline in Oncology: Non-Small Cell Lung Cancer. http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Version 2.2016. Accessed December 15, 2015.
xiii Thalomid References 1. Thalomid. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 2. Thalomid® (thalidomide) prescribing information. Celgene Corp., Updated 8/2015. 3. National Comprehensive Cancer Network (NCCN): National Comprehensive Cancer Network. National Comprehensive Cancer Network (NCCN) Clinical
Practice Guideline in Oncology: Multiple Myeloma. http://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf. Version 2.2016. Accessed December 10, 2015.
4. Clarke J. Management of refractory discoid lupus and subacute cutaneous lupus. Waltham, MA: UptoDate; Last modified October 22, 2015. http://www.uptodate.com/contents/management-of-refractory-discoid-lupus-and-subacute-cutaneouslupus?source=search_result&search=thalidomide&selectedTitle=15%7E150#H1088110. Accessed December 15, 2015.
5. Schur PH, Moschella SL. Mucocutaneous manifestations of systemic lupus erythematosus. Waltham, MA: UptoDate; Last modified April 16, 2014. http://www.uptodate.com/contents/mucocutaneous-manifestations-of-systemic-lupuserythematosus?source=search_result&search=sle&selectedTitle=5%7E150#H18. Accessed December 15, 2015.
6. Scollard D, Stryjewska B. Treatment and prevention of leprosy. Waltham, MA: UptoDate; Last modified December 7, 2015. http://www.uptodate.com/contents/treatment-and-prevention-ofleprosy?source=search_result&search=erythema+nodosum+leprosum&selectedTitle=2%7E11#H89888451. Accessed December 15, 2015.
xiv Tykerb References 1. Tykerb Prescribing Information. GlaxoSmithKline. December. 2012. 2. National Comprehensive Cancer Network. Breast Cancer Treatment Guidelines for Patients – Version 1.2013, 3/5/13.
http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf 3. Wolff AC, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2
testing in breast cancer. J Clin Oncol. Jan 2007; 25(1): 118-145. 4. Geyer CE, et al. Lapatinib plus Capecitabine for HER2-Positive Advanced Breast Cancer. N Engl J Med 2006;355:2733-43. 5. Xeloda® (capecitabine) prescribing information. Roche Pharmaceuticals, Inc., 2/2011. http://www.rocheusa.com/products/xeloda/pi.pdf 6. Tykerb. DrugDex. Micromedex website. www.thomsonhc.com. Accessed 4/12/12. 7. Tykerb. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017. 8. Revlimid. AHFS Drug Information. Ovid website. http://ovidsp.tx.ovid.com. Accessed. 4/12/12
xv Votrient References 1. Votrient prescribing information. GlaxoSmithKline; Research Triangle Park, NC; August 2013. 2. Votrient. Clinical Pharmacology. Clinical Pharmacology Website. www.clinicalpharmacology.com. Accessed September 13, 2017.
P a g e | 18 Last Update: 11/2017 Effective: 2/1/2018
Pharma
cy Prior Authorization Oncology Detailed Guidance– Clinical Guideline
3. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Kidney Cancer. Fort Washington, PA: National Comprehensive Cancer Network, Inc. 2013. (Accessed Feb. 26, 2013, at http://www.nccn.org/professionals/physician_gls/ PDF/kidney.pdf )
4. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Soft Tissue Sarcoma. Fort Washington, PA: National Comprehensive Cancer Network, Inc. 2013 (Accessed September 13, 2013, at http://www.nccn.org/professionals/physician_gls/pdf/sarcoma.pdf)
P a g e | 19 Last Update: 11/2017 Effective: 2/1/2018