
Pharmacotherapy for the Continence Nurse
30
4/13/2017 1 Urinary Tract Infection Across the Lifespan: Latest Developments in Assessment, Prevention & Management Mikel, PhD, PNP, FNP, CUNP, CCCN, FAANP, FAAN Department of Urology, School of Medicine Department of Acute & Specialty Care, School of Nursing University of Virginia Charlottesville, VA Objectives Define urinary tract infection, its epidemiology and pathophysiology Outline prevention strategies, focusing on underlying evidence and investigational techniques Discuss evaluation of domiciliary and febrile UTI Review management of UTI including pharmacologic and behavioral interventions UTI: Global Definitions Urinary Tract Infection (UTI) – Inflammatory response of urothelium to bacterial invasion; usually associated with bacteriuria & pyuria 1 – Definitions in general dictionaries Bacterial infection of urethra, bladder, ureters, kidneys 2 Infection of any part of the urinary tract, especially the urethra or bladder 3 1. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al ( eds ). Campbell - Walsh Urology, 11 th ed. Elsevier, 2016, pp. 237 - 303. 2. Online Medical Dictionary. http://cancerweb.ncl.ac.uk/cgi - bin/omd?query=urinary+tract+infection . 3. Online Oxford English Dictionary. http://dictionary.reference.com/browse/urinary%20tract%20infection
Transcript of Pharmacotherapy for the Continence Nurse

4/13/2017
1
Urinary Tract Infection Across the Lifespan: Latest Developments in
Assessment, Prevention & Management
Mikel, PhD, PNP, FNP, CUNP, CCCN, FAANP, FAAN
Department of Urology, School of Medicine
Department of Acute & Specialty Care, School of Nursing
University of Virginia
Charlottesville, VA
Objectives
Define urinary tract infection, its epidemiology and pathophysiology
Outline prevention strategies, focusing on underlying evidence and investigational techniques
Discuss evaluation of domiciliary and febrile UTI
Review management of UTI including pharmacologic and behavioral interventions
UTI: Global Definitions
Urinary Tract Infection (UTI)
– Inflammatory response of urothelium to bacterial invasion; usually associated with bacteriuria & pyuria1
– Definitions in general dictionaries
Bacterial infection of urethra, bladder, ureters, kidneys2
Infection of any part of the urinary tract, especially the urethra or bladder3
1. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. Elsevier,
2016, pp. 237-303.
2. Online Medical Dictionary. http://cancerweb.ncl.ac.uk/cgi-bin/omd?query=urinary+tract+infection.
3. Online Oxford English Dictionary. http://dictionary.reference.com/browse/urinary%20tract%20infection

4/13/2017
2
UTI: Laboratory BasedClassifications
Bacteriuria: bacteria in urine; may be symptomatic or asymptomatic; CFU > 105 considered clinically relevant but correlation with clinical symptoms is weak1
Pyuria: white blood cells (pus) in the urine, indicates inflammatory response to something, but not necessarily bacteria2
Asymptomatic bacteriuria: sometimes called screening bacteriuria2; resist intervention without indication
Acute Pyelonephritis: chills, fever and flank pain along with bacteriuria and pyuria2
1. Fall M et al. Lakartidningen 1993; 90: 1036.
2. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016,
pp. 237-303.
UTI: Classification based on Environment
Community Acquired (Domiciliary) UTI (formerly classified as uncomplicated): – Symptomatic UTI in otherwise healthy patient; is
not associated with fever or history of urinary tract defects (majority of UTI from epidemiologic perspective); originally limited to women
– Pathogen usually multidrug sensitive coliform bacterial species; most common is E coli
Nosocomial/ facility/ healthcare acquired UTI– Historically this was one criterion of complicated
UTI (others were gender and presenting symptoms)– Pathogens often differ from domiciliary; pathogens
more likely to be resistant to multiple antimicrobialsSchaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed.
2016, pp. 237-303.
vs
UTI: Classification Based on Natural History
First time/ isolated infection: initial infection or more than 1 year from prior UTI
Recurrent UTI: patient was infected, became well (infection free) and is infected again
Unrsesolved UTI: bacteriuria persists despite antibiotic Rx
Chronic UTI: little meaning or clinical relevance
Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016, pp. 237-
303.

4/13/2017
3
Epidemiology
UTI: Prevalence in Infancy & Childhood
Among female infants with fever (overall 7.0%, 95%CI 5.5-8.4%)– 0-3 mos 7.5%
– 3-6 5.7%
– 6-12 mos 8.3%
– >12 mos 2.1%
Among male infants with fever:– <3 mos 2.4% circumcised
20.1% uncircumcised (highest of any group)
Whites infants 8%; black infants 4.7%
Among older children (<19 yrs) pooled prevalence of febrile and non-febrile UTI - 7.8%
Shaikh N et al. Pediatric Infectious Disease Journal 2008; 27(4): 302-8.
UTI: Prevalence in Community Dwelling Women
Epidemiology1,2
– 3.5% of adult, community dwelling women have bacteriuria, most are asymptomatic
– Cumulative risk for women; 30% by age 24 yrs; lifetime risk approximately 50%, most common reason adult woman seeks care for illness
– UTI account for 7 million new clinic/ office visits per year
1 million visits to ED
100,000 admissions to hospital 1. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016, pp.
237-303.
2. Butler CC et al. British Journal of General Practice 2015; 65(639): e702-e707.

4/13/2017
4
UTI: Prevalence & Incidence: Community Dwelling Men
Occurrences in domiciliary men less frequent than women; account for approximately 20% of UTI prevalence in adults
Annual incidence of UTI in men approximately 1318/ 100,000 (1.3%)
Men with UTI more likely to have fever and more likely to require hospital admission
– 424,000 ED visits by men found to be UTI related (majority were > 65 years of age)2
– 100,000 hospital admissions
Greibling TL Journal of Urology 2005; 173: 1288-94.
Healthcare (Facility) Acquired UTI
1. Figure: APIC Guide 2008: Guide to Elimination of Catheter-Associated Urinary Tract Infections.2. Klevens RM, et al. 2002. Public Health Rep. 2007; 122:160-167.
80% of all UTIs are catheter
related
Healthcare Acquired UTI
Less well studied on a national or global basis that domiciliary UTI; resistance to almost all antimicrobials among these infection approaches 20%1
Approximately 139,000 documented CAUTI occurred in 20072
Prevalence of any healthcare-Associated infections from 2010-2011 in US was 4% (95% CI: 3.7– 4.4%)3
1. Tandogdu A, Wagenlehner FME. Current Opinion in Infectious Disease 2016; 29: 73-9. 2. Wise M. Abstract 3703. Society of Healthcare Epidemiology of America, April 2, 2011; Dallas TX. 2. Magill SS et al. New England Journal of Medicine 2014; 370: 1198-1208.

4/13/2017
5
Epidemiology of UTI: Population-Based Risk Factors
Adults1
– Gender: 30% risk of UTI by the time a woman reaches 24th
year of life, 50% lifetime risk
– Age: prevalence ranges from 3.5% to 20%in elder women; prevalence increases from 0.6% to 10% as men reach age 65 years or older1
– History of UTI: probably linked to host immune defenses
Recurrent UTI occurs in 46% of women within 1 year
– Most reinfections occur within 4-5 months1,2
– Many are infected with different organism2
1. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016,
pp. 237-303.
2. Mabeck CE. Postgraduate Medical Journal 1972; 48(566): 69.
UTI: A Note of Caution
Suspect Interstitial Cystitis when…– UTI like symptoms (frequent urination, LUT
pressure/ pain), occur but U/A is negative
– Multiple UTI have been treated without relief from bothersome LUTS
– Patient complains of “chronic UTI” & has seen multiple providers without relief
– Empiric treatment of repeated UTI complaints with “partial response” after 2-4 weeks
Savaris RF, Teixara LM, Torres TG. International Journal of Gynecology and Obstetrics 2006; 93: 256-7.
UTI:Etiology &
Pathophysiology

4/13/2017
6
Etiology & Pathophysiology
General Principles1. UTI represents temporary loss in an ongoing
skirmish between pathogens & host (patient), resulting colonization and overgrowth of pathogen to detriment of host
2. Most pathogens are bacterial, fungal or tubercular; viral pathogens exits but are much less common
3. Differences in anatomy of urinary tract in male and female results in differences in clinical manifestations and progression of infection left untreated
UTI: Etiology & Pathophysiology
Pathogens usually enter urinary tract via urethra, rarer alternatives included – Hematogenous: critically ill, septic patient
– Lymphatogenous: seen with retroperitoneal abscess or severe bowel infection
Bacterial Reservoirs – Gastrointestinal Tract*
– Vaginal vault
– Skin
– Foreign objectFigure: http://www.lifespan.org/adam/graphics/images/en/19094.jpg
UTI: Etiology & Pathophysiology
4/13/2017
7
Multiple Contributing Factors
Multitude of Associated/Risk Factors, these are especially prevalent
– Sexual activity (↑ inoculation)
– Spermicide (↑ binding)
– Reduced estrogens (alters vaginal flora; ↑ binding)
– Antimicrobial therapy (↓ normal flora)
– Urinary stasis (↓ antegrade flow)
– Inadequate fluid intake
– Urinary or fecal incontinence
– Incomplete bladder emptying
– Foreign body in urinary tract
Schaeffer AJ, Mateulewicz RS, Klumpp
DJ. In Wein AJ et al (eds). Campbell-
Walsh Urology, 11th ed. 2016, pp. 237-303.
Health Care Associated UTI:Etiology & Pathophysiology
Risk of CAUTI proportionally related to duration of catheterization1
Bacterial species swarm catheter from urethral meatus toward vesicle; laboratory studies show proteus and pseudomonas species swarm in as little as 24 - 48 hours2
Planktonic bacteria up-regulate specific genes to form biofilm; rendering them up to 1,000 fold more resistant to antimicrobial Rx3
1. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th
ed. 2016, pp. 237-303.2. Williams GJ, Stickler DJ. Infection Control & Hospital Epidemiology 2008; 29(5): 443. 3. Ferrieres L et al. FEMS Immunological Med Microbiology 2007; 51: 212.
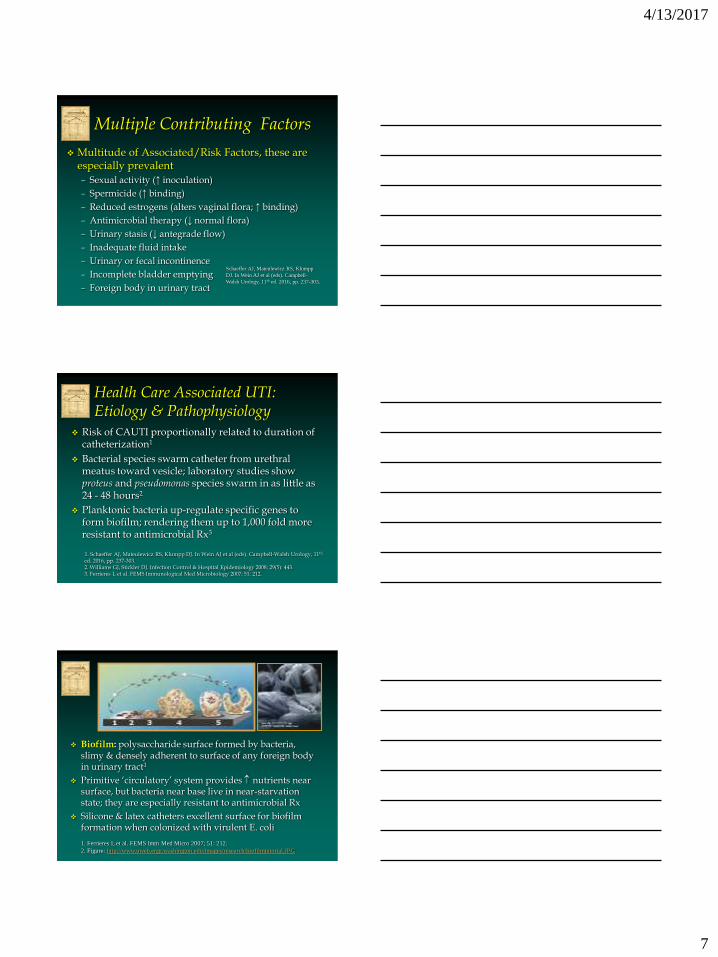
Biofilm: polysaccharide surface formed by bacteria, slimy & densely adherent to surface of any foreign body in urinary tract1
Primitive ‘circulatory’ system provides nutrients near surface, but bacteria near base live in near-starvation state; they are especially resistant to antimicrobial Rx
Silicone & latex catheters excellent surface for biofilm formation when colonized with virulent E. coli
1. Ferrieres L et al. FEMS Imm Med Micro 2007; 51: 212.
2. Figure: http://www.uweb.engr.washington.edu/images/research/biofilmtutorial.JPG

4/13/2017
8
Most UTI in Adults are Bacterial: N = 22,830 domiciliary patients
Foxman B. Nature Reviews: Urology 2010; 7: 653-70.
Most UTI in Adults are Bacterial:N = 5,563 hospitalized adults
Foxman B. Nature Reviews: Urology 2010; 7: 653-70.
Most UTI in Adults are Bacterial: N = 2,777 elders in LTCF
Foxman B. Nature Reviews: Urology 2010; 7: 653-70.

4/13/2017
9
Bacterial Virulence: The Enemy’s Weapons
Host Defenses
Figures on next 2 slides are integrative review on immune defenses in human urinary tract:
– Abraham SN, Miao Y. Nature Reviews Immunology 2015; 15:655-63.
Epithelial cells in the nephron secrete numerous substances that protect host against UTI and bacteria including• Uromodulin/ Tamm-Horsfall glycoprotein: binds to fimbriae
stopping bacteria from adhering to urinary tract• Multiple interleukins (IL-1, IL-6, IL-8): recruit macrophages to
area• Other molecules remove essential nutrients from urine; for
example, NGAL & siderophores remove or bind iron that is essential to bacterial growth and reproduction

4/13/2017
10
Urothelium of Bladder
Bladder defenses• After invading epithelium, urothelium ↑ cyclic AMP literally kicking bacterium back
out into urine• Urothelium secretes antimicrobial proteins, peptides and chemokines• It all this is insufficient, the bladder will exfoliate/shed its superficial layer with
bacterial content• All of this ultimately supported by local immune cells; mostly mast cells and Ly6C-
macrophages
Diseases & Disorders that Compromise Host Defenses
P1/P2 blood group phenotype (non secretors of P1/P2): ↑ likelihood of bacteriuria, symptomatic UTI and febrile UTI1,2
Diabetes mellitus: predisposes to more severe infections, combined effect of glucosuria plus compromised immune response3
HIV: immunocompromised and higher prevalence of virulent bacteria when UTI occurs
Neurologic disease: results in neurogenic bladder, obstruction, sphincter dyssynergia, greater likelihood of use of indwelling or intermittent catheterization
1. Lichodziejewska-Niemierko M et al. Clinical Nephrology 1995; 44(6): 376-9.
2. Ishitoya S et al. BJU International 2002; 89(9): 851-4.
3. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016, pp.
237-303.
Viral Urinary Tract Infections
Rare in patients with competent immune system function; most commonly seen after organ transplantation1
Asymptomatic viruria does occur; most common is BK virus
Most commonly associated with hemorrhagic UTI
Principal pathogens are cytomegalovirus, adenovirus and BK virus
Paduch DA. Current Urology Reports 2007; 8: 324.

4/13/2017
11
Fungal Urinary Tract Infections
Most common in critically ill patients with ongoing or recent exposure to broad spectrum antibiotics
Risk Factors include:– Immunocompromised immune function, renal
transplantation
– Diabetes mellitus
– Older
– Renal failure, hemodialysis
Candidiasis most common, Blastoschizomyces also occurs
Krcmery S, Dubrava M, Krcmery Jr, V. International J Antimicrobial Agents 1999; 11: 289.
Parasitic Urinary Tract Infections
From public health perspective schistosomiasis is the most significant parasitic infection of lower UTI in men (and women)
– Parasite enters human host while bathing waters in tropical areas (Africa, Pacific rim)
– Urothelium reacts to deposition of eggs with inflammation and secondary bacterial UTI
– Reinfection, inadequate treatment result in progressive disorder with scarring, uropathy and high risk of urinary tract cancers
Ghoneim MA. BJU International 2002; 89 (Supplement 1): 22.
Evaluation &
Diagnosis

4/13/2017
12
Clinical Manifestations: Neonates & Infants
Fever 67%
Irritability 55%
Poor Feeding 38%
Vomiting 36%
Diarrhea 36%
Abdominal distension <10%
Jaundice < 10%
Shortliffe LMD. Infection & Inflammation of Pediatric GU Tract. Campbell-Walsh Urology, 9th ed, 2007, p. 3232.
Clinical Manifestations:Older Children
Dysuria in 15%-30%
Vague lower abdominal pain, not well localized to flanks or suprapubic area
Sudden change in LUTS
Enuresis, urge UI
Cloudy & malodorous urine (most common cause of cloudy urine: phosphaturia)
Cooper CS, Storm DW. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th edition. 2016, pp. 2926-48.
Classic Clinical Manifestations
Dysuria (burning, “voiding barbed wire”1) tends to occurs during and after void
Suprapubic or lower back pain
Voiding frequency
Urgency
Malaise
Malterud K, Baerheim A. Scandinavian Journal of Primary Health Care 1999; 17(1);49-53.

4/13/2017
13
Clinical Manifestations: Older Adults >75 years)
Lower urinary tract symptoms (LUTS) tend to be less “focused” than younger adults1
Greatest differences in very old ( 80 yrs) and very frail elders
Retrospective review of 104 patients 70 yrs revealed confusion (30%), cough (27%), dyspnea (28%) with no reported LUTS despite bacteriuria, pyuria and fever – in absence of radiographic evidence of chest infection2
1. Malterud K, Baerheim A. Scandinavian J Primary Health Care 1999; 17(1): 49.
2. Barkham T et al. Age & Ageing 1996; 25(2): 130.
Diagnosis
Urine collection: Voided Specimen
– Retract foreskin and cleanse in uncircumcised male and female
– Collection bag or cloth diaper in infant
Catheterization or suprapubic aspiration – Selected cases when voided specimen
cannot be obtained
Indwelling catheter– Consider changing long-term catheter that
has been in for more than 3-5 days
Assessment: Routine Studies
Urinalysis
Dipstick:– UTI (nitrites & leukocytes)
– Diabetes mellitus (glucose)
– Diabetes insipidus/ water intoxication (specific gravity)
– LUT tumor (blood, RBC)
Microscopic examination– UTI (WBC & bacteria)
– LUT (red blood cells)

4/13/2017
14
UTI: Interpreting the U/A
Bacteriuria: bacteria in urine; CFU > 105
considered clinically relevant but this criterion correlates poorly with clinical symptoms1
Pyuria: white blood cells (pus in the urine), indicates inflammatory response to something (like an indwelling
catheter) but not necessarily bacteria
1. Fall M et al. Lakartidningen 1993; 90: 1036.
2. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology,
11th ed. 2016, pp. 237-303.
Urinalysis: How Accurate?
Dipstick testing1
– Nitrite testing very specific (97%) but less sensitive (43%) when CFU <105
– Leukocyte esterase specificity is 59% and its sensitivity is 84%
– When combined…specificity is 98% and sensitivity is 84%
Take home message: use a back up screening test whenever possible (microscopy)
Semeniuk H, Church D. Journal Clinical Microbiology 1999; 37(9): 3051.
Urinalysis: Microscopy
Preparation of sample
– 10-15 ml into test tube
– Centrifuge at 5 minutes at 2000rpm or 2 minutes with high speed models
– Pour off all but sludge in bottom
– Agitate the sludge, place drop in center of slide
– Cover with slip cover
4/13/2017
15
Urinalysis: Microscopy
Examine with both eyes open, leave glasses on
Use moderate light setting, most use too much
Start with low setting 100x), then move to high (400x)
Look around, concentrate on edges of slip cover as well as center
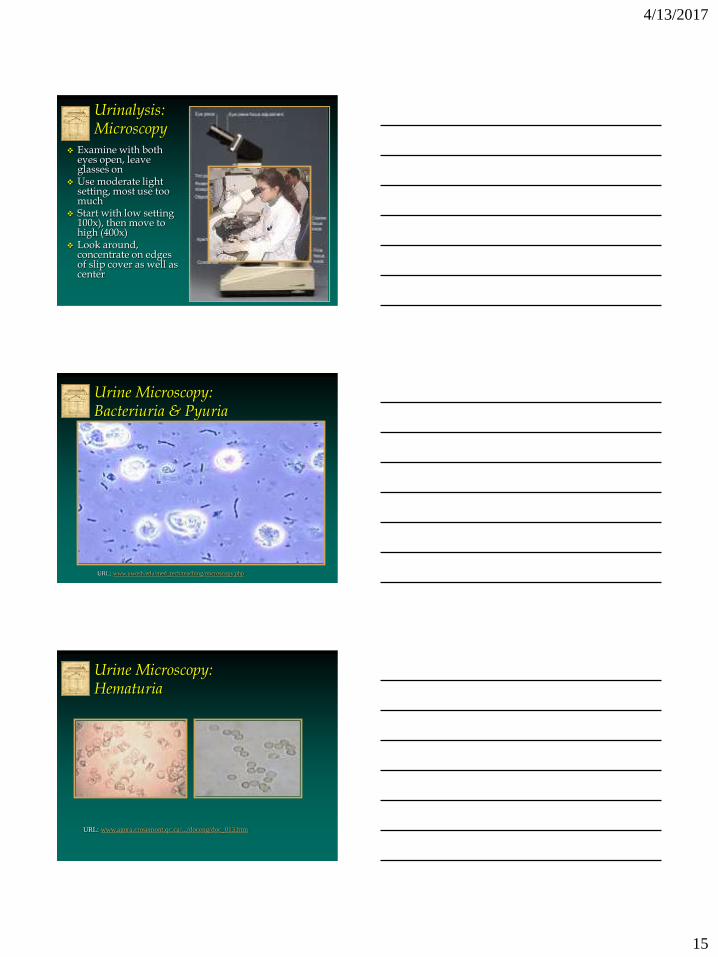
Urine Microscopy: Bacteriuria & Pyuria
URL: www.uwosh.edu/med_tech/teaching/microscopy.php
Urine Microscopy: Hematuria
URL: www.agora.crosemont.qc.ca/.../doceng/doc_013.htm

4/13/2017
16
Urine Microscopy: Skin Cells
Fogazzi GB URL: www.ndt-educational.org/fogazzislidepart6.asp
Urine Culture
Cultures can be obtained via direct surface plating or dip slides
Slides are easier but less accurate
Sensitivity testing usually recommended
Can be done at point of care or professional laboratory (latter more common with existing CLIA regulations)
Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-
Walsh Urology, 11th ed. 2016, pp. 237-303.
UTI Diagnosis: Colony Counts
Emerging evidence suggests that current clinical standard for urine cultures (>105 CFU/ml may not be best across bacterial species (suggested based on optimal NPV/PPV)
– E coli (most prevalent) may be clinically relevant at 103
CFU/ml
– Enterococci species: 103 – 104 CFU/ml
– Group B streptococci:104 – 105 CFU/ml
Results also suggest limited value of midstream clean urine specimen vs catheterized
Hooton TM et al. New England Journal of Medicine 2013; 369(20): 1883-91.

4/13/2017
17
Prevention &
Management
UTI Prevention:Behavioral Interventions
Sexual activity (intercourse) well established risk factor for women, possible risk factor in men
Very weak to moderate evidence supports the following interventions1,2
– Less frequent intercourse (<3 times weekly)
– Limiting partners
– Washing hands and genital area before and after intercourse
– Voiding within 30 minutes of intercourse
– Switching to different birth control method (diaphragm, spermicidal foam, even BCP have been connected; sexual activity is powerful confounding factor in these studies)
1. NIDDK. UTI in adults: http://www.niddk.nih.gov/health-information/health-topics/urologic-disease/urinary-tract-
infections-in-adults/Pages/facts.aspx , accessed 2/16/2016.
2. Amiri FN et al. La Revie de Sante Mediterranee orientale 2009; 15(1): 104-10.
UTI Prevention: Behavioral Interventions
Wide variety of hygienic measures have been recommended; supporting evidence often weak or absent
– Indirect but robust support for hand hygiene when in contact with fecal matter (recc. adapted from HAI literature), also adapted to advice about wiping from font to back following micturition or defecation1
– Weaker evidence for additives to bath water (“bubble baths” or “perfumed baths”, “scented soaps”), associated ↑risk for UTI, evidence traces its roots to very old case studies and multiple case series describing vulvovaginitis and LUTS in women and children rather than UTI occurrences2,3
1. Schuman EK, Chenoweth CE. Critical Care Medicine 2010; 31 (8 Supplement): S373-9.
2. Simmons RJ Obstetrics & Gynecology 1955; 6: 447-8.
3. Marshall S. Journal of Urology 1965; 93(1): 112.

4/13/2017
18
UTI Prevention: Behavioral Interventions
Multiple other hygienic measures have been advocated that have no known evidence to support or refute…
– Avoid tight fitting clothing
– Breathable vs non-breathable undergarments
– Shower versus tub bath
– Tampons versus pads for containing menstrual flow
– Voiding every __ hours, whether the individual desires to urinate or not, postponing urination, etc.
– Void before or following physical activities
Preventing UTI & Recurrences
Fluid Intake– Avoid extremes (consumption of high volumes of
fluid or fluid restriction)
– US Food & Science Board RDA for fluids: 30ml/kg/24 hr or ½ oz/lb/day (ambulatory person, moderate climate)
Approximately 1.5-2.2 liters in adult women, 1.5-2.3 in adult men; 1.2-2.3 in adults > 70 years of age
Children aged 1 to 3 years 1.0 to 1.5 liters; increase to 1.2 to 1.9 liters in older children
1. IOM/ US Food & Science Board: Dietary Reference Intake for Water & Sodium. URL: http://www.iom.edu/Global/News%20Announcements/~/media/442A08B899F44DF9AAD083D86164C75B.ashx
Preventing UTI & Recurrences
American cranberry (Vaccinium macrocarpon)
– Principal antimicrobial action is not its ability to acidify urine; it is the concentration of Type a Pro-anthocyanins (PAC)
– Effective dose hypothesized to be >30mg administered twice daily; equals 2 8 ounce servings or juice or 2 capsules containing 36 mg PAC*
– Red cranberries have highest PAC concentration; avoid white cranberry juice
1. Strothers L. Personal communication. 2. Gurley BJ. Archives of Internal Medicine 2011; 171(14): 1279-80. * = TheraCran (Theralogix, Rockville MD)

4/13/2017
19
Preventing UTI & Recurrences
Mixed evidence suggests consuming probiotics (lactobacillus) via dietary sources (yogurt, etc.) might reduce UTI risk1,2
Particularly sparse evidence suggests that consumption of certain fruits & berries or juices from these may reduce risk of UTI3
Sparse evidence also suggest acupuncture may help (mechanism unclear, amy reduce residual urine in some)1
1. Hanson L et al. Journal of Midwifery & Women’s Health 2016; 61(3): 339-55.
2. Schwenger EM, Tejani AM, Loewen PS. Cochrane Database of Systematic Review.
DOI: 10.1002/14651858.CD008772.pub2, 2015.
3. Kontiokari T et al. American Journal of Nutrition 2003; 77 (3): 600.
Prevention of UTI or Recurrence:Angocin Anti-Infekt N
Herbal produce containing Tropaeoli majoris and Armoraciae rusticanae radix (horse radish) for recurring UTI
In vitro study demonstrated antimicrobial activity against E. coli, Pseudomonas aeruginosa, MRSA, Staphylococcus Pyogenes species1
Clinical study of 219 adults (women & men), aged 18-75 years with recurring UTI had fewer UTI over 90 day period2
2 serious AE in treatment group not associated with herbal preparation
1. Conrad A et al. Arzneimittelforschung. 2006;56(12):842.
2. Albrecht U, Goos KH, Schnieder B. Current Medical Research & opinion 2007; 23(10): 2415.
Circumcision for Prevention of UTI
Is circumcision protective against UTI?
– Circumcision reduces UTI risk approximately 10-fold over first 6 months of life and demonstrable benefit up to 12 months, colonization of bacteria declines by age 5 years as foreskin grows and retraction is easier1
– Controversy over whether benefit extends beyond extends beyond 1st year of life, cohort analysis needed
– Evidence supports reduced transmission rates of HIV & syphilis, mixed evidence concerning relative risk for transmission of chancroid, HSV-22
1. Cooper CS, Storm DW. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016, pp. 2926-48.
2. Morris BJ. BioEssasy 2007; 29: 1147.

4/13/2017
20
Future of UTI Prevention: Vaccines?
E coli associated with 75% or more of UTIs in community dwelling women, various vaccine targets
– Vaccine for FimH protein has shown promise in blocking adherence of E coli to bladder wall
– Vaccine for D-galactopyranoside receptors in vaginal wall and epithelial cells in kidney may protect against development of pyelonephritis
– Vaccine for UpaG a auto-transporter may block E coli’s ability to bind to bladder wall and from biofilm
Moriel DG, Schembri MA. Current Pharmaceutical Biotechnology 2013; 14: 967-74.
Future of UTIPrevention: Vaccines?
2 RCT of vaccine, E coli extract (unable to adhere to wall of bladder, activates innate antibodies against E coli colonization)
– Both tested in women with recurrent UTI (3 in 1 year); one was a capsule administered daily for 90 days, off for 60 days, then daily for first 10 days of months 7-9; the other was a weekly vaginal suppository for 90 days, then weekly suppository for additional 90 days
– Both groups achieved significantly fewer recurrences than placebo group; neither are commercially available in US
Bauer HW et al. European Urology 2005; 47: 542-8.
Russo TA et al. Vaccine 2007; 25(19): 3859-70.
Preventing CAUTI Intervention Bundle: no single intervention
sufficient to reduce CAUTI incidence; evidence based winning strategies include – Reduce indwelling catheter days by implementing
system for monitoring catheter insertion and removal1,2
– Use bladder scanners to aid in timely catheter removal2
– Evaluate all aspects of existing indwelling catheter policies3
– Enhance use of alternative means for urinary drainage: intermittent catheterization and external collection devices1-3
1. Saint S, Chenowith CE. Infectious Disease Clinics of North America 2003; 17: 411.
2. Saint S et al. Clinical Infectious Disease 2008; 46: 43.
3. Gray M. Journal of Wound, Ostomy & Continence Nursing 2004; 31(1): 3

4/13/2017
21
Pharmacotherapy for Management of UTI and
Prevention of Recurrences
Management of Community Acquired UTI
Goals of treatment
– Eradicate bacteriuria
– Alleviate symptoms
– Prevent recurrence
Empiric therapy may be administered in otherwise healthy younger adults, culture & sensitivity recommended in adults with comorbid conditions, febrile or recurring UTI
UTI: Empiric Treatment
Empiric treatment recommended for nonfebrile UTI in community dwelling women (IDSA 2010 CPG)
– First Line Therapy
Nitrofurantoin ER 100 mg twice daily for 5 days
Trimethoprim/ Sulfamethoxazole DS 1 tablet twice daily for 3 days
– Second Line Therapy
Ciprofloxacin 250 mg twice daily or 500 mg daily for 3 days
Gupta K et al. Clinical Infectious Disease 2011; 52:e103-e120.

4/13/2017
22
Pharmacotherapy for UTI: Empiric Antimicrobial Therapy
Infectious Disease Society of America initially recommended empiric therapy for women with uncomplicated UTI in 1999; guidelines updated in 2010/111; principal recommendations include:– Consider nitrofurantoin as first line agent (A-I)* – Add fosfomycin to your first line choices (A-I)*– Penicillamines should not be used alone for empiric therapy
owing to high resistance throughout US (A-III)**– Penicillamine plus -lactam should be considered when
above agents cannot be used (B-I)^– Use the fluoroquinolones as second line treatments for
empiric therapy (A-III)**
1. Gupta K et al. Clinical Infectious Disease 2011;52:e103-e120.
* A-I: strong recommendation based on good evidence ** A-III: strong rec based on expert opinion/ consensus ^ B-I: moderate recommendation based on good evidence
Gu
pta
K et a
l. Clin
ical In
fectiou
s Disea
se 20
11
; 52
:e10
3-e1
20
UTI: Empiric Treatment:Antibiotic Options for Pregnant Women
Multiple β-lactams may be considered in pregnant women
Pantori, A. Urinary Tract Infection. Urology Core Curriculum for Residents URL:
https://www.auanet.org/university/core_topic.cfm?coreid=92, downloaded 2/16/2016.

4/13/2017
23
Pharmacotherapy for UTI
Trimethoprim-Sulfamethoxazole1 (Bactrim DS, Septra DS)
– IDSA recommends 160/800mg (double strength tablet) administered twice daily for 3 days
– Adverse SE include significant hyperkalemia in patients with renal insufficiency, diabetes mellitus, older age or use of angiotensin-converting enzyme (ACE) inhibitor; study published in 2011 found incidence was 51.4 per 100,00; no association seen with fluoroquinolones or nitrofurantoin2
– Linked to bloody, antibiotic-associated diarrhea in children3
1. Gupta K et al. Clinical Infectious Disease 2011;52:e103-e120 2. Lam M et al. American Journal of Kidney Diseases 2011; 57(3): 521-5. 3. Barakat M et al. J Pediatric Gastroenterology & Nutrition 2011; 52(1): 60-4.
Pharmacotherapy for UTI
Nitrofurantoin (Macrodantin, Macrobid)1,2
– Administer as 100 mg twice daily for 5 days
– Achieves high urinary levels effective for E. coli and many other common domiciliary pathogens; less penetration in serum – do not use if evolving pyelonephritis suspected
– Typically offers limited activity against Proteus, Pseudomonas, Serratia (~3-4% sensitivity)
– Recent RCT found equivalent or superior efficacy to 3 day course of TMP/SMZ3
– Linked to risk of C. Difficile associated diarrhea2
1. Gupta K et al. Clinical Infectious Disease 2011;52:e103-e120. 2. Schultz HJ. Mayo Clinic Proceedings 2011; 86(6): 477-9. 3. Gupta K et al. Archives of Internal Medicine 2007; 167(20): 2207-12.
Pharmacotherapy for UTI
Fosfomycin (Monurol)1,2
– Administer as 3 gram sachet in single dose in 90-120 ml of water; drug is not bound to plasma proteins, reaches high urinary levels in 2-2.5 hours and persisting for 36-48 hours; primarily excreted in urine
– Efficacy shown non-inferior to norfloxacin, ofloxacin, ceftriaxone in several RCT
– Carries risk for C. Difficile associated diarrhea, other SE include diarrhea, nausea, headache
– IND and primary clinical experiences in women
1. Gupta K et al. Clinical Infectious Disease 2011;52:e103-e120.
2. Shrestra, NK, Tomford JW. Infectious Diseases in Clinical Practice 2001; 10(5): 255-60.
3. Usta TA et al. International Journal of Obstetrics & Gynecology 2011; 114:229-33.

4/13/2017
24
Pharmacotherapy for UTI
Fluoroquinolones (Cipro, Levaquin)1
– Second line agents, administer ciprofloxacin as 500 mg twice daily or levofloxacin as 500 mg once daily
– Levofloxacin offers broader coverage for gram positive organisms; some prefer ciprofloxacin for empiric
– Linked to C difficile associated diarrhea
– In vitro study finding suggests that ciprofloxacin activity may be augmented by Pelargonium graveolens, an essential oil2
1. Gupta K et al. Clinical Infectious Disease 2011;52:e103-e120. 2. Malik T et al. Phytotherapy Research 2011; 25: 1225-8.
Pharmacotherapy for LUT Pain/Discomfort
Consider short-term urinary analgesic– Phenazopyridine (Pyridium, 200mg three times daily):
reduces burning and alleviates dysuria1
– MOA unknown, turns urine deep orange capable of staining clothing, some patients mistakenly identify color as indicating hematuria
– Adverse side effects include fever, confusion, uncommon to rare SE impaired renal or liver function, hemolytic anemia (anemia risk rises with prolonged use)1,2
1. Gaines KK. Urologic Nursing 2004; 24(3): 207-9.
2. Singh M et al. Journal of Renal Failure 2014; 36(5): 804-7.
Pharmacotherapy: Special Considerations in Children
Diagnosis requires urinalysis plus culture in all infants and children with febrile UTI, microscopy strongly recommended – look for ≥ 10 WBC/hpf
– Lower threshold for hospital admission, especially in infants & young children (↑ likelihood of sepsis)
– 7-14 days of antibiotic therapy for all febrile UTIs; 2-4 days for afebrile episodes – begin with empiric selection and confirm
– Look for antimicrobials available as liquid or suspension
– Nitrofurantoin and cephalosporin often used as first line (greater likelihood of Enterococcus species); penicillamine use limited by E coli resistance
Cooper CS, Storm DW. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016, pp. 2926-48.

4/13/2017
25
Pharmacotherapy for LUT Pain/Discomfort
Combination agents for short-term analgesia contain one or more of the following agents
– Pharmacologic actions of individual agents
Hyoscyamine (atropine): anticholinergic
Methanemine: urinary antiseptic, antimicrobial agent that acts by concentrating formaldehyde in low concentrations
Methylene blue: mild antiseptic effect
Sodium biphosphate: mild antiseptic effect
Phenyl salicylate: ASA with typical analgesic response
Pharmacotherapy for LUT Pain/Discomfort
4 agent formulations contain Hyoscyamine sulfate 0.06 - 0.12 mg, a few (Urised, Prosed)
also list low dose atropine but this is a bit unclear on more recent diosing, appears to have changed to hyoscyamine
Methenamine 81.2 – 118 mg
Methylene blue 10 - 10.8 mg
Sodium biphosphate 40.8 mg
Phenyl salicylate 36-40 mg
– Typically prescribed as 1 tablet up to 4 times daily
– Multiple branded names (Uribel, Prosed, Urised, Urogesic blue); contain similar active agents, doses vary slighty (check with local pharmacy)
Pharmacologic Strategies for Preventing Recurrent UTI
Consider ongoing course of suppressive antibiotic course for adults with recurrent UTI
– Daily dose; usually treat with a first line drug for empiric UTI treatment (nitrofurantoin, trimethoprim/sulfamethoxazole)
– Consider baseline liver function panel and possibly chest X-ray if contemplating long-term suppression with nitrofurantoin
– I recommend 6 month trial; some extend to 1 year trial
Pantori, A. Urinary Tract Infection. Urology Core Curriculum for Residents URL:
https://www.auanet.org/university/core_topic.cfm?coreid=92, downloaded 2/16/2016.

4/13/2017
26
Pharmacologic Strategies for Preventing Recurrent UTI
Consider self start antibiotic therapy
– 3 day course of antibiotic prescribed that patient stores in home
– Provide specimen cup for urinalysis ± urine culture with standing order with local laboratory
– Teach patient to monitor for symptoms
Consider post-coital antibiotic therapy
– Prescribe antibiotic as above and instruct patient to take single dose following intercourse
Pantori, A. Urinary Tract Infection. Urology Core Curriculum for Residents URL:
https://www.auanet.org/university/core_topic.cfm?coreid=92, downloaded 2/16/2016.
Preventing Recurrent UTI:Methenamine
Methenamine (Hiprex, Mandelamine, Urex)
– Extensively excreted in urine, converting hexamine to formaldehyde, ↓ urinary pH exert antiseptic activity
– Magnitude of effect (and clinical effectiveness) remains controversial
– Cochrane Review indented 13 studies (2013 subjects); Overall study quality rated as low and heterogeneity too great for meta-analysis
– Methenamine more effective than placebo in reduction of bacteriuria (RR 0.56, 95% CI 0.37-0.83) and symptomatic UTI (RR 0.24, 95% CI 0.07-0.89); sued short term (1 week or less); no differences when used in patients with urinary tract abnormalities (e.g. NGB) or indwelling catheters
Lee BSB et al. Cochrane Database 2012, Issue 10. Art. No.: CD003265. DOI: 10.1002/14651858.CD003265.pub3.
Preventing UTI Recurrence in Postmenopausal Women
Sparse evidence suggests benefit from intravaginal estrogen in women with urogentialatrophy
– Systematic review pooled data from 4 studies (2798 women) found that oral estrogens did not reduce risk fro recurring UTI, RR 1.08, 95%CI: 0.89-1.33
– Non-pooled results from 2 studies suggest that intravaginal estrogens (cream or ring device) mayreduce risk for recurrence RR 0.25, 95% CI: 0.13 - 0.50 and RR 0.64, 95% CI: 0.47-0.86
Perrotta C et al. Cochrane Database of Systematic Reviews. (2)CD005131, 2008.

4/13/2017
27
Preventing UTI Recurrence
Recurrent UTI defined as 3 occurrences in 12 months or 2 in 6 months
All primary preventive strategies should be considered for preventing recurrence
Consider obtaining urine culture for recurrent UTI to exclude possibility of persistent bacteriuria
Consider referral or imaging of urinary tract for urinary stone, anatomic defect of urinary tract, obstructive uropathy, etc.
Pantori, A. Urinary Tract Infection. Urology Core Curriculum for Residents URL:
https://www.auanet.org/university/core_topic.cfm?coreid=92, downloaded 2/16/2016.
Management of Febrile and Healthcare Acquired UTI
Febrile UTI:Principles of Management
Determine need for hospitalization
– Evidence of sepsis
– High fever
– High WBC
– Vomiting and dehydration precluding ability to take oral medications or fluid/electrolyte balance
– Lack of resources in home
Schaeffer AJ, Schaeffer EM. In: Campbell-Walsh Urology, 10th ed. Philadelphia: Elsevier, 2012, pp. 257-326.

4/13/2017
28
Pharmacotherapy for Febrile UTI
Begin with empiric therapy; IDSA/EMSID guidelines recommend ciprofloxacin twice daily*1
– Consider single parenteral dose of antimicrobial agent before starting empiric oral therapy; often aminoglycoside, ceftriaxone, or fluoroquinolone2
– Tailor antibiotic selection based on sensitivity panel
– If hospital admission required, start with aminoglycoside ± aminopenicillin, fluoroquinolone, extended spectrum (3rd or 4th generation) cephalosporin (example is ceftazadime)
1. Gupta K et al. Clinical Infectious Disease 2011; 52:e103-e120. 2. Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al (eds). Campbell-Walsh Urology, 11th ed. 2016,
pp. 237-303.
* Level of Recommendation = A-III
Pharmacotherapy for Febrile UTI
Antibiotic options for febrile UTI1
– Fluoroquinolone: ciprofloxacin 500 mg twice daily for 7 days or levofloxacin once daily for 5 days (B-II)*
– Trimethoprim-sulfamethoxazole (160/800 mg, DS) for 14 days (A-I)*
– -lactams less effective than these suggestions, recommend initial parenteral dose or beginning with initial dose of aminoglycoside (B-II, B-III)*; optimal duration of therapy is unknown – possibly 10-14 days
1. Gupta K et al. Clinical Infectious Disease 2011; 52:e103-e120.
*= Level of Recommendation
Community-BasedManagement
7-14 day course of ciprofloxacin (more effective than 14 days of TMP-SMX: 96% vs. 83%)1
Oral ciprofloxacin taken as directed provides serum levels comparable to parenteral administration
Repeat culture 5-7 days if response questioned
Repeat culture 14 days after treatment completed; 10%-16% will recur
Extend treatment to 6 weeks if necessary and exclude abscess or complicating condition
1. Schaeffer AJ, Schaeffer EM. Campbell-Walsh Urology, 10th ed. Elsevier, 2012.

4/13/2017
29
Extended Evaluation in Infants, Children & Adults
Infants & Children
Febrile UTI in child associated with ↑ risk of vesicoureteral
reflux and renal damage (big bang hypothesis)
– Controversy exists as to proper evaluation of infants and children who experience first (or 2nd) febrile UTI
– Extended evaluation usually involves one or more of the following Ultrasonography
Voiding urethrogram
Radionuclide cystogram or imaging of upper urinary tracts
Gadolinium MRI
– Extend evaluation after 1st or 2nd UTI?
– Is VCUG necessary? Cooper CS, Storm DW. In Wein AJ et al (eds). Campbell-
Walsh Urology, 11th ed. 2016, pp. 2926-48.
American Academy of Pediatrics Revised their Guidelines for Infants 3 months to 2 years
Diagnosis should include urinalysis and positive urine culture
Infants with proven febrile infants should undergo renal and bladder ultrasonography
VCUG routinely only when:
– Ultrsound reveals hydronephrosis, scarring, or other findings that would suggest high-grade VUR or obstructive uropathy
*VCUG indicated after 2nd febrile UTI
Revised AAP Guidelines on UTI in Febrile Infants and Young Children:
http://www.aafp.org/afp/2012/1115/p940.html

4/13/2017
30
Top Down AlgorithmFebrile UTI
DMSA scan
Cortical defect Normal Central photopenia
(Pyelonephritis) (Hydronephrosis)
No further W/U*
VCUG Ultrasound
*Recurrent febrile UTI
VCUG (*AAP Guideline)
Algorithm courtesy H Gil
Rushton, MD
Additional Diagnostic Studies for Febrile of Healthcare Acquired UTI
Upper tract imaging: ultrasound or spiral CT when renal colic present or urinary calculi suspected
Abdominal CT for unresolved (persistent) UTI to exclude abscess or anatomic abnormality
Doppler enhanced ultrasound when epididymitis suspected
Referral and cystourethroscopy in selected cases
URL: www.medscape.com/viewarticle/466477Schaeffer AJ, Mateulewicz RS, Klumpp DJ. In Wein AJ et al
(eds). Campbell-Walsh Urology, 11th ed. 2016, pp. 237-303.
Conclusions
UTI prevalent in both genders
Lifetime risk greatest for women vs men
Classification of UTI, diagnosis and treatment based on where UTI was acquired (community vs healthcare setting)
Management must go beyond short course antimicrobials to include multiple non-[pharmacologic interventions to prevent or limit recurrences

















