Pharmacology. Pharmacology The study of drugs and their actions.
Upload
carmela-alonzoCategory
view
184download
3
1
GROUP 2
Report
BLOOD DRUGS
Submitted to:
Dr. Sherwin Banan
Submitted by:
Alonzo, Carmela
Pacual, JP Brando
Galang, Roan Eina
Olivas, Nanette
Labbuanan, Kristell Anne
Sanao, Bryan Jay
Domingo, Rafael
Santos, Bryan
Baculi, Daryll

2
NAMES
NO ATTENDANCE
NO CONTRIBUTION
NO REPORT
NO GRADE
Alonzo, Carmela
Pascual, JP Brando,
Galang, Roan
Olivas, Nanette
Santos, Bryan
Domingo, Rafael
Labbuanan, Kristell Ann
Sanao, Bryan
Baculi, Daryll
February 15, 2015

3
BLOOD DRUGS
I. OVERVIEW
The vascular system delivers oxygen and nutrients to all body cells and removes waste
products from tissues. This closed system functions as a pressure system, with blood flowing
continuously from high-pressure to low-pressure areas. Injury of a blood vessel compromises
the closed system, causing blood to flow out of the injured vessel (now a low-pressure area).
With severe injury to a vessel, the entire circulatory system may be compromised and the
patient could die.
Blood vessel injuries are common, occurring, for instance, when someone hits the edge of a
table, coughs too hard, or falls down. They initiate a series of normal reactions that stops blood
flow and maintains balance within the system. The reactions include:
reflex vasoconstriction
platelet aggregation
blood coagulation (clot formation), which causes blood to solidify
clot resolution, which returns blood to the fluid state.
In many clinical situations, drugs are used to slow or stop this process, with the goal of
preventing tissue damage from the decreased blood flow that occurs when the clotting process
cuts off blood supply to an area. The succeeding discussion reviews the processes the body uses

4
to maintain the cardiovascular system and discusses the mechanisms of action, benefits, and
risks of drugs used to alter coagulation.
After an injury to a blood vessel, the vessel constricts. With a small injury, constriction
typically seals the open space, allowing blood to flow and helping the vessel to heal. A larger
injury exposes endothelial cells lining the vessel to blood flowing through it, causing platelets to
adhere to the injured area.
When a platelet adheres, it releases chemicals that attract more platelets, in turn drawing
even more platelets to the area in a process called platelet aggregation. Consequently, a
platelet plug forms. In some cases, this is enough to seal the leak and keep pressures stable

5
while the vessel heals. In more severe injuries, the vessel wall injury activates Hagemann factor,
a clotting factor. Activated Hagemann factor triggers activation of other clotting factors,
initiating the clotting cascade. The cascade ends in conversion of prothrombin to thrombin;
activated thrombin initiates clot formation.
All clotting factors are made in the liver and require vitamin K for their formation. Calcium is
the catalyst that speeds the clotting cascade. Activated thrombin breaks down fibrinogen into
fibrin. An insoluble protein, fibrin forms a clot at the site. The change of blood from fluid to
solid form stops blood flow in the vessel.
In this process, called the intrinsic process, a clot forms within the vessel. A similar process,
the extrinsic process, occurs in blood that has leaked out of the vessel at the injury site. This
process produces a seal within the vessel, along with a seal outside the vessel. While this allows
the vessel wall to seal and heal, it could interrupt blood flow to tissues beyond that point,
causing ischemia or even cell death. When Hagemann factor is activated and triggers the
clotting cascade, it also causes plasminogen conversion to plasmin. Plasmin dissolves fibrin and
returns blood to the fluid state. This is the body’s clot-dissolving mechanism. Plasminogen,
made in the liver, also is activated by such conditions as stress, fever, and various enzymes. This
process protects against the harmful effects of clot formation.
Indications for drugs that alter coagulation
In certain clinical situations for instance, coronary artery disease, immobility, atrial
fibrillation, and joint replacement interfering with coagulation helps prevent clots that could
impede blood flow and cause tissue damage or death. Patients with coronary artery disease, for
example, have narrowed vessels. An immobile patient loses the protective massaging of veins
caused by muscle fiber contractions; also, blood pools and doesn’t return to the heart
efficiently. With atrial fibrillation, blood pools in the heart’s auricles and may clot. The artificial
parts of a hip or knee replacement initially may damage a blood vessel, leading to clotting.
All drugs that alter coagulation interfere with the normal protective reflexes. As a nurse,
you need to be aware of the dangers of eliminating these reflexes, which could include serious
or even fatal bleeding episodes. Drugs that alter coagulation include platelet inhibitors and
anticoagulants
Platelet inhibitors are often the first line of defense in preventing vascular clots; they
don’t affect clots that already have formed. These drugs block platelets’ ability to adhere and

6
aggregate to form the platelet plug, the first step in sealing the vascular system and preventing
blood loss into body tissues.
Current platelet inhibitors include abciximab (ReoPro), anagrelide (Agrylin), aspirin,
cilostazol (Pletal), clopidogrel (Plavix), dipyridamole (Persantine), eptifibatide (Integrilin),
ticlopidine (Ticlid), ticagrelor (Brilinta), and tirofiban (Aggrastat). These drugs are used to treat
cardiovascular diseases in which vessels become occluded, as well as to maintain venous and
arterial grafts and prevent cerebrovascular occlusion. They’re also given as adjuncts to
thrombolytic therapy in treating myocardial infarction (MI) and preventing post-MI reinfarction.
Ticagrelor, released in 2011, is indicated only to prevent thromboembolic events in acute
coronary syndrome. Its black-box warning cites the risk of excessive bleeding and dangers of
sudden withdrawal, which can trigger an acute cardiovascular event.
Most platelet inhibitors block receptors on platelets to prevent adhesion; anagrelide
prevents platelet formation in the bone marrow. Bleeding (including bleeding caused by
toothbrushing and excessive bleeding after injury) is the most common adverse effect. Easy
bruising also may occur.
II. THROMBUS VS. EMBOLUS
Thrombosis is the formation of an unwanted blood clot in the vessel and is the most common
abnormality of homeostasis. Thrombotic disorder treated with drugs such as: anticoagulant and
fibrinolytics.

7
o Acute myocardial infarction- the blood clots blocks the coronary arteries which may
produce a heart attack.
o Deep vein thrombosis-is the formation of a blood clot or thrombus within a deep vein,
predominantly in the legs.
o Pulmonary embolism- is a condition in which a part of a blood clot in a vein breaks away
and travel through the heart and into the pulmonary circulatory system

8
o Acute ischemic stroke- the blood supply to part of the brain is cut off because
atherosclerosis or a blood clot has blocked a blood vessel.
Bleeding disorders involving the failure of homeostasis are less common than
thromboembolic disease:
Hemophillia, the blood does not clot properly and bleeding persists. Blood does not clot
normally because it lacks sufficient blood clotting protein (clotting factor). These are treated
with dietary supplement of vitamin k. Anemia; red blood cell count stays persistently low, or
below 4million. Iron deficiency anemia is a common complication of pregnancy. It is treated
with iron supplement and iron rich foods including egg, cereals, green leafy vegetable and meat
specially the liver.
THROMBUS vs EMBOLUS

9
Thrombus is a clot that adheres to a vessel wall immobile. Embolus is an intravascular
clot that floats in the blood. Mobile, thus a detached thrombus becomes an embolus. Both
thrombi and emboli are dangerous, because they may occlude blood vess els and deprive
tissues of oxygen and nutrients.
Arterial thrombosis most often occurs in medium-size vessels rendered thrombogenic
by surface lesions on endothelial cells caused by atherosclerosis. In contrast, Venous
thrombosis, is triggered by blood stasis or inappropriate activation of the coagulation cascade,
frequently result of a defect in the normal hemostatic defense mechanisms.
III. PLATELET RESPONSE TO VASCULAR INJURY
Physical trauma to the vascular system, such as a puncture or a cut, initiates a complex
series of interactions between platelets, endothelial cells, and the coagulation cascade. These
interactions lead to hemostasis or the cessation of blood loss from a damaged blood vessel.
Platelets are central in this process. Initially there is vasospasm of the damaged blood vessel to
prevent further blood loss. The next step involves the formation of a platelet-fi brin plug (clot)
at the site of the puncture. The creation of an unwanted thrombus involves many of the same
steps as normal clot formation, except that the triggering stimulus is a pathologic condition in
the vascular system rather than an external physical trauma.
A. Resting Platelets
Platelets act as vascular sentries, monitoring the integrity of the endothelium. In the
absence of injury, resting platelets circulate freely, because the balance of chemical signals
indicates that the vascular system is not damaged.

10
B. Platelet Adhesion
When the endothelium is injured, platelets adhere to and virtually cover the exposed
collagen of the subendothelium. This triggers a complex series of chemical reactions, resulting
in platelet activation.
C. Platelet Activation
Receptors on the surface of the adhering platelets are activated by the collagen of the
underlying connective tissue. This causes morphologic changes in platelets and the release of
platelet granules containing chemical mediators, such as adenosine diphosphate (ADP),
thromboxane A2, serotonin, platelet-activation factor, and thrombin. These signaling molecules
bind to receptors in the outer membrane of resting platelets circulating nearby. These
receptors function as sensors that are activated by the signals sent from the adhering platelets.
The previously dormant platelets become activated and start to aggregate. These actions are
mediated by several messenger systems that ultimately result in elevated levels of calcium and
a decreased concentration of cAMP within the platelet.
D. Platelet Aggregation
The increase in cytosolic calcium accompanying activation is due to a release of
sequestered stores within the platelet. This leads to:
1) the release of platelet granules containing mediators, such as ADP and serotonin that
activate other platelets;
2) activation of thromboxane A2 synthesis; and
3) activation of glycoprotein (GP) IIb/IIIa receptors that bind fibrinogen and, ultimately,
regulate platelet-platelet interaction and thrombus formation. Fibrinogen, a soluble plasma GP,
simultaneously binds to GP IIb/IIIa receptors on two separate platelets, resulting in platelet
cross-linking and platelet aggregation.
11
This leads to an avalanche of platelet aggregation, because each activated platelet can
recruit other platelets.
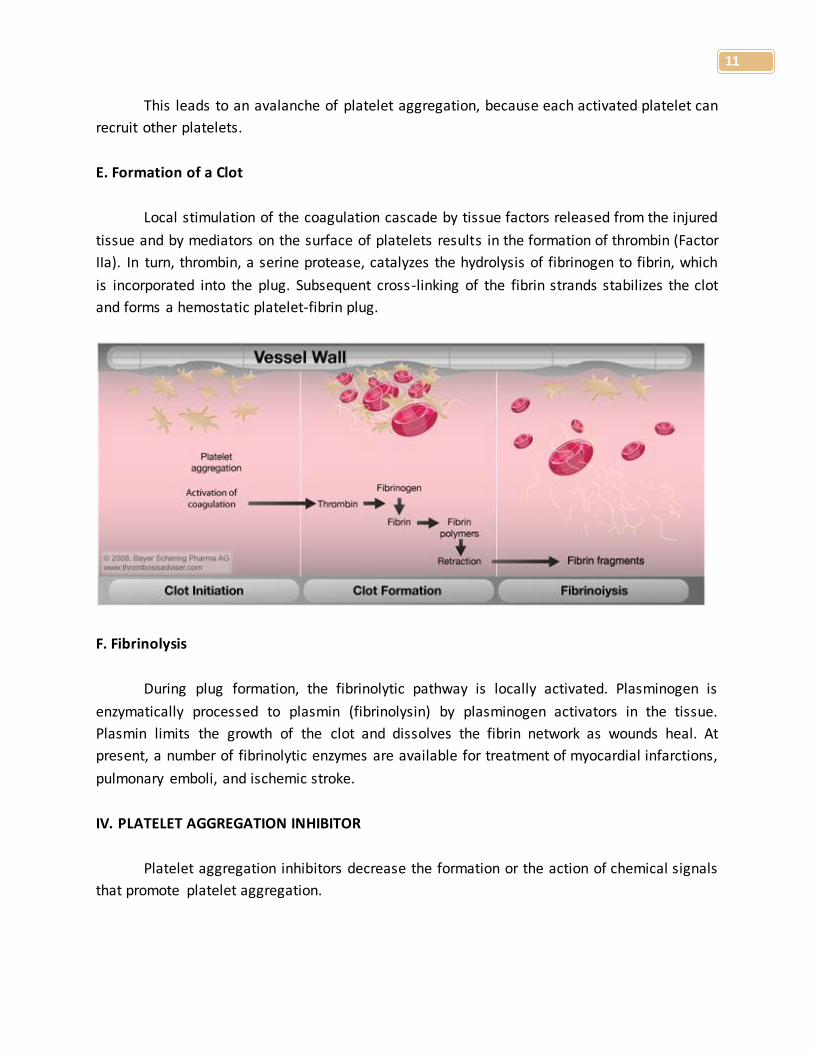
E. Formation of a Clot
Local stimulation of the coagulation cascade by tissue factors released from the injured
tissue and by mediators on the surface of platelets results in the formation of thrombin (Factor
IIa). In turn, thrombin, a serine protease, catalyzes the hydrolysis of fibrinogen to fibrin, which
is incorporated into the plug. Subsequent cross-linking of the fibrin strands stabilizes the clot
and forms a hemostatic platelet-fibrin plug.
F. Fibrinolysis
During plug formation, the fibrinolytic pathway is locally activated. Plasminogen is
enzymatically processed to plasmin (fibrinolysin) by plasminogen activators in the tissue.
Plasmin limits the growth of the clot and dissolves the fibrin network as wounds heal. At
present, a number of fibrinolytic enzymes are available for treatment of myocardial infarctions,
pulmonary emboli, and ischemic stroke.
IV. PLATELET AGGREGATION INHIBITOR
Platelet aggregation inhibitors decrease the formation or the action of chemical signals
that promote platelet aggregation.

12
The platelet aggregation inhibitors inhibit cyclooxygenase-1 (COX-1) or block GP IIb/IIIa
or ADP receptors, thereby interfering in the signals that promote platelet aggregation. Since
these agents have different mechanisms of actions, synergistic or additive effects may be
achieved when agents from different classes are combined.
A. Aspirin
Stimulation of platelets by thrombin, collagen and ADP results in activation of platelet
membrane phospholipases that liberate arachidonic acid from membrane phospholipids.
Arachidonic acid is first converted to prostaglandin H2 by COX-1; prostaglandin H2 is further
metabolized to thromboxane A2, which is released into plasma.
B. Ticlopidine and clopidogrel
These drugs irreversibly inhibit the binding of ADP to its receptors on platelets and, thus,
inhibit the activation of the GP IIb/IIIa receptors required for platelets to bind to fibrinogen and
to each other.
Ticlopidine is approved for the prevention of transient ischemic attacks and strokes for patients
with prior cerebral thrombotic event. Adveres Drug reaction includes:
Neutropenia/Agranulocytosis
Thrombotic Thrombocytopenic Purpura (TTP)
Aplastic anemia
Clopidogrel is used to prevent thrombotic events associated with percutaneous coronary
intervention with or without coronary stent.
C. Abciximab
Stimulating platelet aggregation directed attempts to block this receptor on activated
platelets.
D. Eptifibatide and tirofiban
Similar to Abciximab
E. Dipyridamole

13
Increases intracellular levels of cAMP by inhibiting cyclic nucleotide phosphodiesterase,
resulting in decreased thromboxane A2 synthesis. It may potentiate the effect of prostacyclin to
antagonize platelet stickiness and, therefore, decrease platelet adhesion to thrombogenic
surfaces.
V. BLOOD COAGULATION
The coagulation process that generates thrombin consist of two interrelated pathways,
the extrinsic and intrinsic system.
Extrinsic system more important system in vivo is initiated by the activation of clotting factor
VII by tissue factor or thromboplastin.
Intrinsic system triggered by the activation of clotting factor XII, following its contact in vitro
with glass or highly charged surface.
FORMATION OF FIBRIN
Both the extrinsic and intrinsic system involve in cascade of enzyme reaction that
sequentially transform various plasma factor(proenzyme) to their active (enzymatic) form. If
thrombin is not formed or , coagulation is inhibited. Each step in the activation process is
catalytic,(for example, one unit of activated factor Xa can potentially generate 40units of
thrombin, which will result to the production of large amount of fibrin at the site of injury)
ROLL OF CELL SURFACES

14
Phospholipid-based protein-protein complex-consist of membrane surfaces provided by
phospholipid of activated platelets or activated endothelial cell, an enzyme, a substrate, and a
cofactor.
Calcium is essential to this process, bridging anionic phospholipid and y-carboxyglutamic
acid resisues of the clotting factor.
INHIBITORS OF COAGULATION
It is important that coagulation is restricted to the local site of the vascular injury,
Inhibitors of coagulation factors:
Protein C
Protein S
Antithrombin III
Tissue factor pathway imhibitor
The mechanism of action of several anticoagulant agents, including hrparin and heparin related
products, involves actiovation of these endogenous inhibitor(primarily Antithrombin III)
VI. ANTICOAGULANT
Anticoagulant medicines reduce the ability of the blood to clot (coagulation means
clotting). This is necessary if the blood clots too much, as blood clots can block blood vessels
and lead to conditions such as a stroke or a heart attack.
A. HEPARIN
Heparin injection is an anticoagulant. It is used to decrease the clotting ability of the
blood and help prevent harmful clots from forming in blood vessels. This medicine is sometimes
called a blood thinner, although it does not actually thin the blood. Heparin will not dissolve
blood clots that have already formed, but it may prevent the clots from becoming larger and
causing more serious problems.
Heparin is used to prevent or treat certain blood vessel, heart, and lung conditions.
Heparin is also used to prevent blood clotting during open-heart surgery, bypass surgery,
kidney dialysis, and blood transfusions. It is used in low doses to prevent the formation of blood
clots in certain patients, especially those who must have certain types of surgery or who must
remain in bed for a long time. Heparin may also be used to diagnose and treat a serious blood

15
condition called disseminated intravascular coagulation. This medicine is available only with
your doctor's prescription.
This product is available in the following dosage forms:
Injectable
Solution
B. OTHER PARENTERAL ANTICOAGULANTS
1. LEPIRUDIN
Lepirudin is used in thinning the blood and preventing blood clots in patients with low
blood platelets caused by heparin. It may also be used for other conditions as determined by
your doctor.
Lepirudin is a thrombin inhibitor. It works by blocking the activity of thrombin, which
helps to prevent the formation of blood clots.
2. FONDAPARINUX
Fondaparinux is an anticoagulant medication chemically related to low molecular weight
heparins.
Fondaparinux is similar to enoxaparin in reducing the risk of ischemic events at nine
days, but it substantially reduces major bleeding and improves long-term mortality and
morbidity.
Fondaparinux is given subcutaneously daily. Clinically, it is used for the prevention
of deep vein thrombosis in patients who have had orthopedic surgery as well as for the
treatment of deep vein thrombosis and pulmonary embolism.
C. VITAMIN K ANTAGONIST
Vitamin K antagonists (VKA) are a group of substances that reduce blood clotting by
reducing the action of vitamin K. They are used as rat poisons but also
as anticoagulant medications in the prevention of thrombosis.
Mechanism of Action

16
These drugs deplete the active form of the vitamin by inhibiting the enzyme vitamin K
epoxide reductase and thus the recycling of the inactive vitamin K epoxide back to the active
reduced form of vitamin K. The drugs are structurally similar to vitamin K and act as competitive
inhibitors of the enzyme. The term "vitamin K antagonist" is a misnomer, as the drugs don't
directly antagonise the action of vitamin K in the pharmacological sense, but rather the
recycling of vitamin K.Vitamin K is required for the proper production of certain proteins
involved in the blood clotting process.
The action of this class of anticoagulants may be reversed by administering vitamin K for
the duration of the anticoagulant's residence in the body, and the daily dose needed for
reversal is the same for all drugs in the class. However, in the case of the second generation
"super warfarins" intended to kill warfarin resistant rodents, the time of vitamin K
administration may need to be prolonged to months, in order to combat the long residence
time of the poison. The vitamin K antagonists can cause birth defects (teratogens).
VII. THROMBOLYTIC DRUGS
Acute thromboembolic disease in selected patients may be treated by the
administration of agents that activate the conversion of plasminogen to plasmin-a serine
protease that hydrolyzes fibrin and, thus, dissolves clots. Streptokinase, one of the first such
agents to be approved, causes a systematic fibrinolytic state that can lead to bleeding
problems. Alteplase acts more locally on the thrombotic fibrin to produce fibrinolysis. In the
case of acute myocardial infarction, the thrombolytic drugs are reserved for those instances
when angioplasty is not an option or until the patient can be taken to a facility that performs
percutaneous coronary interventions. Fibrinolytic drugs may lyse both normal and pathologic
thrombi.
Common characteristics of thrombolytic agents
Mechanism of action: All act either directly or indirectly to convert plasminogen to plasmin,
which in turn cleaves fibrin, thus lying thrombi. Clot dissolution and reperfusion occur with a
higher frequency when therapy is initiated early after clot formation, increased local thrombi
may occur as the clot dissolves, leading to enhanced platelet aggregability and thrombosis.
Strategies to prevent this include administration of antiplatelet drugs, such as aspirin, or
antithrombotics, such as, heparin.

17
Therapeutic uses: Originally used for the treatment of deep-vein thrombosis and serious
pulmonary embolism, thrombolytic drugs are now being used less frequently for these
conditions. Their tendency to cause bleeding has also blunted their used in treating acute
myocardial infarction or peripheral arterial thrombosis. However, thrombolytic agents are
helpful in restoring catheter and shunt function, by lying clots causing occlusions. Thrombolytic
agents are also used to dissolve clots that result in strokes.
Pharmacokinetics: For myocardial infarction, intracoronary delivery of the drugs is the most
reliable in terms of achieving recanalization. However, cardiac catheterization may not be
possible in the 2-to-6 hour “therapeutic window”, beyond which significant myocardial salvage
becomes less likely. Thus, thrombolytic agents are usually administered intravenously, because
this route is rapid, is inexpensive, and does not have the risks of catheterization.
Adverse effects: The thrombolytic agents do not distinguish between the fibrin of an unwanted
thrombus and the fibrin of a beneficial hemostatic plug. Thus, hemorrhage is a major side
effect. For example, a previously unsusoected lesion, such as a peptic ulcer, may hemorrhage
following injection of a thrombolytic agent. These drugs are contraindicated in patients with
healing wounds, pregnancy, history of cerebrovascular accident, or metastic cancer. Continued
presence of thrombogenic stimuli may cause rethrombosis after lysis of the initial clot.
1. Alteplase. Alteplase (formerly known as tissue plasminogen activator, or tPA) is a serine
protease originally derived from cultured human melanoma cells. It is now obtained as a
product of recombinant DNA technology.
Mechanism of Action
Alteplase has a low affinity for free plasminogen in the plasma, but it rapidly activates
plasminogen that is bound to fibrin in a thrombus or a hemostatic plug, thus, alteplase is said to
be “fibrin selective,” and at low doses, it has the advantage of lysing only fibrin, without
unwanted degradation of other proteins-notably fibrinogen.
Therapeutic uses
Alteplase is approved for the treatment of myocardial infarction, massive pulmonary
embolism, and acute ischemic stroke. Alteplase seems to be superior to streptokinase in
dissolving older clots and ultimately, may be approved for other applications. Alteplase ,
administered within 3 hours of the onset of ischemic stroke, significantly improves clinical
outcome-that is, the patient’s ability to perform activities of daily living. Reteplase is simila r to
alteplase can be uses as an alternative.

18
Pharmacokinetics: Alteplase has a very short half-life (about 5 minutes) and therefore, is
administered as a total dose equal to 0.9 mg/kg.
Adverse effects: Bleeding complications, including gastrointestinal and cerebral haemorrhages,
may occur.
2. Streptokinase. Streptokinase is an extracellular protein purified from culture broths of
group C β-hemolytic streptococci.
Mechanism of action
Streptokinase has no enzymic activity. Instead, it forms an active one-to-one complex
with plasminogen. This enzymatically active complex coverts uncomplex plasminogen to the
active enzyme plasmin.
Therapeutic uses
Streptokinase is approved for use in acute pulmonary embolism, deep-vein thrombosis,
acute myocardial infarction, arterial thrombosis, and occluded access shunts.
Pharmacokinetics
Streptokinase therapy is instituted within 4 hours of myocardial infarction and is infused
for 1 hour. Its half-life is less than half an hour.
Adverse effects
Bleeding disorders: Activation of circulating plasminogen by streptokinase leads to
elevated levels of plasmin, which may precipitate bleeding by dissolving hemostatic
plugs. In the rare instance of life –threatening hemorrhage, aminocaproic acid may be
administered.
Hypersensitivity: Streptokinase is a foreign protein and is anti-genic. Rashes, fever, and
rarely, anaphylaxis occur. Because most individuals have had a streptococcal infection
sometime in their lives, circulating antibodies against streptokinase are likely to be
present in most patients.
3. Anistreplase ( anisoylated plasminogen streptokinase activator complex. Anistreplase
is a performed complex of streptokinase and plasminogen and it is considered to be a
prodrug. Streptokinase must be released, and only plasminogen to which it was
associated will get converted to plasmin.

19
VIII. DRUG USED TO TREAT BLEEDING
Bleeding problem may have their origin in naturally occurring pathologic conditions such
as hemophilia (a serious disease that causes a person who has been cut or injured bleeding for
a very long period of time) or result of fibrinolytic states (that may rise after GI surgery or
prostatectomy).
The use of anticoagulants may also give rise to hemorrhage.
Certain natural proteins and Vitamin K, as well as synthetic antagonists, are effective
controlling this bleeding. For example, hemophilia is a consequence of a deficiency in plasma
coagulation factors, most frequently Factors VIII and IX.
Blood transfusion is also an option for treating severe hemorrhage.
A. Aminocaproic Acid and Tranexamic Acid. Fibrinolytic states can be controlled by the
administration of aminocaproic acid or tranexaminc acid. These drugs are synthetic,
which they inhibits plasminogen activation, are orally active and excreted in the urine. A
side effect of this treatment is intravascular thrombosis.
B. Protamine sulfate is an agent that antagonizes the anticoagulant effect of heparin. This
protein derived from the fish sperm or testes and is high in arginine content. The
adverse effects of drug administration include hypersensitivity as well as dyspnea,
flushing, bradycardia, and hypotension.
C. Vitamin K or Phytomenadione is a fat-soluble vitamins the human body needs
for complete synthesis of certain proteins that are required for blood coagulation, and
also certain proteins that the body uses to manipulate binding of calcium in bone and
other tissues. The vitamin K-related modification of the proteins allows them to
bind calcium ions, which they cannot do otherwise. Without vitamin K, blood
coagulation is seriously impaired, and uncontrolled bleeding occurs. Low levels of
vitamin K also weaken bones and promote calcification of arteries and other soft tissues.
D. Aprotinin, is a serine protease inhibitor that stops bleeding by blocking plasmin. It can
inhibit streptokinase. This agent may cause renal dysfunction and hypersensitivity
reaction. In addition, this agent should not be administered to patients who have
already been exposed to the drug within the previous 12 months due to the possibility
of anaphylactic reaction.

20
IX. AGENTS USED TO TREAT ANEMIA
Anemia is defined as a below-normal plasma hemoglobin concentration resulting from a
decreased number of circulating red blood cells or an abnormally low total hemoglobin content
per unit of blood volume. In other words anemia is a condition in which your blood has a lower
than normal number of red blood cells.
The following are causes of Anemia:
o Chronic blood loss
o Bone marrow abnormalities
o Increased hemolysis
o Infections
o Malignancy
o Endocrine deficiencies
o Renal failure
Anemia can be at least temporarily corrected by transfusion of whole blood.
Diagnostic procedure: Blood Transfusion
Nutritional anemias are caused by dietary deficiencies of substances such as:
1. Iron. It is stored in intestinal mucosal cells as ferritin until needed by the body. Iron
deficiency results from a negative iron balance due to depletion of iron stores and/ or
inadequate intake, culminating in hypochromic microcytic anemia. The treatment of
deficiency in iron is supplementation of ferrous sulfate. The Adverse Effect is GIT
Disturbances.

21
2. Folic Acid. The primary use of folic acid is in treating deficiency states that arise from
inadequate levels of the vitamin. Folate deficiency may be caused by increased demand,
poor absorption caused by pathology of the small intestines , alcoholism and treatment
with drugs that are dihydrofolate reductase inhibitors. The primary results of deficiency
are megaloblastic anemia and cyanocobalamin (Vitamin B12).
3. Cyanocobalamin. Deficiencies of vitamin B12 can result from either low dietary levels,
poor absorption of the vitamin due to the failure of gastric parietal cells to produce
intrinsic factor, or loss of activity of the receptor needed for intestinal uptake of the
vitamin.
4. Erythropoietin and Darbepoetin. Erythropoietin is a GP, normally made by the kidney,
which regulates red blood cell proliferation and differentiation in bone marrow.
Human erythropoietin is effective in the treatment of anemia caused by end stage renal
disease.
Darbepoetin is a long acting version of erythropoietin that differs from erythropoietin by
the addition of two carbohydrate chains, which improves its biologic activity.
Darbepoetin has no value in acute treatment of anemia due to its delayed onset of
action.
X. AGENTS USED TO TREAT SICKLE CELL DISEASE

22
Sickle cell anemia has no widely available cure. However, treatments can help relieve
symptoms and treat complications. The goals of treating sickle cell anemia are to relieve pain;
prevent infections, organ damage, and strokes; and control complications (if they occur).
Blood and marrow stem cell transplants may offer a cure for a small number of people
who have sickle cell anemia. Researchers continue to look for new treatments for the disease.
Infants who have been diagnosed with sickle cell anemia through newborn screening are
treated with antibiotics to prevent infections and receive needed vaccinations. Their parents
are educated about the disease and how to manage it. These initial treatment steps have
greatly improved the outcome for children who have sickle cell anemia.
Specialists Involved. People who have sickle cell anemia need regular medical care.
Some doctors and clinics specialize in treating people who have the disease. Hematologists
specialize in treating adults and children who have blood diseases or disorders.

23
Treating Pain
Medicines and Fluids
Mild pain often is treated at home with over-the-counter pain medicines, heating pads,
rest, and plenty of fluids. More severe pain may need to be treated in a day clinic, emergency
room, or hospital.
The usual treatments for acute (rapid-onset) pain are fluids, medicines, and oxygen
therapy (if the oxygen level is low). Fluids help prevent dehydration, a condition in which your
body doesn't have enough fluids. Fluids are given either by mouth or through a vein. Your
doctor may prescribe antibiotics if you have an infection.
Treatment for mild-to-moderate pain usually begins with acetaminophen (Tylenol®) or
nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen. If pain continues or becomes
severe, stronger medicines called opioids might be needed. Talk with your doctor about the
possible benefits and risks of taking strong pain medicine, especially if the medicine will be used
for a long period.
Hydroxyurea
Severe sickle cell anemia can be treated with a medicine called hydroxyurea This
medicine prompts your body to make fetal hemoglobin. Fetal hemoglobin, or hemoglobin F, is
the type of hemoglobin that newborns have. In people who have sickle cell anemia, fetal
hemoglobin helps prevent red blood cells from sickling and improves anemia.
It is taken daily by mouth, hydroxyurea reduces how often painful sickle cell crises and
acute chest syndrome occur. Many people taking hydroxyurea also need fewer blood
transfusionsand have fewer hospital visits.
Preventing Complications
Blood transfusions are commonly used to treat worsening anemia and sickle cell
complications. A sudden worsening of anemia due to an infection or enlarged spleen is a
common reason for a blood transfusion. Some, but not all, people who have sickle cell anemia
need regular blood transfusions to prevent life-threatening problems, such as stroke, spleen
problems, or acute chest syndrome.