Pharmacist prescribing in Northern Ireland: a quantitative assessment
8
RESEARCH ARTICLE Pharmacist prescribing in Northern Ireland: a quantitative assessment Laura McCann • Sharon Haughey • Carole Parsons • Fran Lloyd • Grainne Crealey • Gerard J. Gormley • Carmel M. Hughes Received: 21 April 2011 / Accepted: 25 July 2011 / Published online: 10 August 2011 Ó Springer Science+Business Media B.V. 2011 Abstract Objective Health care in the United Kingdom (UK) has undergone a significant change in terms of the range of professionals who are permitted to prescribe medications. This study aimed to capture information on pharmacist prescribing in Northern Ireland (NI). Setting Primary and secondary care in NI. Method A structured self-administered questionnaire was developed and sent to all pharmacists who were identified as qualified prescribers in NI (n = 105), although only 100 respondents provided details of their prescribing status i.e. currently prescribing, previous prescribers and those who had never prescribed. Three versions of the questionnaire were developed to accommodate each category of prescriber. The question- naire, which sought information on clinical areas/practice settings of prescribers, their working arrangements and barriers to prescribing was distributed by mail on two occasions to maximise response rates. Descriptive analyses were used as appropriate, together with Chi-squared tests or Fisher exact tests to evaluate associations between responses and demographic information, with significance set a priori at P \ 0.05. Qualitative data (from the free text response section) were analysed for recurring themes using content analysis. Results A response rate of 76.0% (n = 76) was achieved. There were more female respon- dents (73.7%) than males (26.3%). Nearly 50% of respondents were currently prescribing (n = 36; 47.4%), 46.1% (n = 35) had never prescribed and 6.6% (n = 5) had prescribed in the past. There were perceived benefits in terms of patient care and perception of the pharmacist within the health care team. A number of barriers to pharmacist prescribing were reported. Independent pre- scribing was viewed as the way forward, although phar- macists expressed reluctance to prescribe without a diagnosis or beyond the team setting. Conclusion Phar- macy prescribing has yet to fully embedded in routine practice. This study has shown that the number of qualified prescribers in NI is relatively small and not all have taken up prescribing responsibilities. Well recognised barriers were reported as reasons as to why qualified prescribers were unable to use their prescribing skills. Further research should provide an in-depth understanding of pharmacy prescribing in NI and examine patients’ experiences of this form of practice. Keywords Independent prescribing Á Non-medical prescribing Á Northern Ireland Á Pharmacist prescribing Á Supplementary prescribing L. McCann Á S. Haughey Á C. Parsons Á C. M. Hughes (&) School of Pharmacy, Queen’s University Belfast, 97 Lisburn Road, Belfast BT9 7BL, Northern Ireland, UK e-mail: [email protected] F. Lloyd Northern Ireland Centre for Pharmacy Learning and Development, Queen’s University Belfast, Belfast, Northern Ireland, UK e-mail: [email protected] G. Crealey Northern Ireland Clinical Research Support Centre, Belfast Health and Social Care Trust, Belfast, Northern Ireland, UK e-mail: [email protected] G. J. Gormley Department of General Practice and Primary Care, School of Medicine, Dentistry and Biomedical Sciences, Queen’s University Belfast, Belfast, Northern Ireland, UK e-mail: [email protected] 123 Int J Clin Pharm (2011) 33:824–831 DOI 10.1007/s11096-011-9545-7
-
Upload
laura-mccann -
Category
Documents
-
view
213 -
download
0
Transcript of Pharmacist prescribing in Northern Ireland: a quantitative assessment

RESEARCH ARTICLE
Pharmacist prescribing in Northern Ireland: a quantitativeassessment
Laura McCann • Sharon Haughey •
Carole Parsons • Fran Lloyd • Grainne Crealey •
Gerard J. Gormley • Carmel M. Hughes
Received: 21 April 2011 / Accepted: 25 July 2011 / Published online: 10 August 2011
� Springer Science+Business Media B.V. 2011
Abstract Objective Health care in the United Kingdom
(UK) has undergone a significant change in terms of the
range of professionals who are permitted to prescribe
medications. This study aimed to capture information on
pharmacist prescribing in Northern Ireland (NI). Setting
Primary and secondary care in NI. Method A structured
self-administered questionnaire was developed and sent to
all pharmacists who were identified as qualified prescribers
in NI (n = 105), although only 100 respondents provided
details of their prescribing status i.e. currently prescribing,
previous prescribers and those who had never prescribed.
Three versions of the questionnaire were developed to
accommodate each category of prescriber. The question-
naire, which sought information on clinical areas/practice
settings of prescribers, their working arrangements and
barriers to prescribing was distributed by mail on two
occasions to maximise response rates. Descriptive analyses
were used as appropriate, together with Chi-squared tests
or Fisher exact tests to evaluate associations between
responses and demographic information, with significance
set a priori at P \ 0.05. Qualitative data (from the free text
response section) were analysed for recurring themes using
content analysis. Results A response rate of 76.0%
(n = 76) was achieved. There were more female respon-
dents (73.7%) than males (26.3%). Nearly 50% of
respondents were currently prescribing (n = 36; 47.4%),
46.1% (n = 35) had never prescribed and 6.6% (n = 5)
had prescribed in the past. There were perceived benefits in
terms of patient care and perception of the pharmacist
within the health care team. A number of barriers to
pharmacist prescribing were reported. Independent pre-
scribing was viewed as the way forward, although phar-
macists expressed reluctance to prescribe without a
diagnosis or beyond the team setting. Conclusion Phar-
macy prescribing has yet to fully embedded in routine
practice. This study has shown that the number of qualified
prescribers in NI is relatively small and not all have taken
up prescribing responsibilities. Well recognised barriers
were reported as reasons as to why qualified prescribers
were unable to use their prescribing skills. Further research
should provide an in-depth understanding of pharmacy
prescribing in NI and examine patients’ experiences of this
form of practice.
Keywords Independent prescribing � Non-medical
prescribing � Northern Ireland � Pharmacist prescribing �Supplementary prescribing
L. McCann � S. Haughey � C. Parsons � C. M. Hughes (&)
School of Pharmacy, Queen’s University Belfast, 97 Lisburn
Road, Belfast BT9 7BL, Northern Ireland, UK
e-mail: [email protected]
F. Lloyd
Northern Ireland Centre for Pharmacy Learning and
Development, Queen’s University Belfast, Belfast, Northern
Ireland, UK
e-mail: [email protected]
G. Crealey
Northern Ireland Clinical Research Support Centre, Belfast
Health and Social Care Trust, Belfast, Northern Ireland, UK
e-mail: [email protected]
G. J. Gormley
Department of General Practice and Primary Care, School
of Medicine, Dentistry and Biomedical Sciences, Queen’s
University Belfast, Belfast, Northern Ireland, UK
e-mail: [email protected]
123
Int J Clin Pharm (2011) 33:824–831
DOI 10.1007/s11096-011-9545-7

Impact statements
• Prescribing by pharmacists in Northern Ireland has yet
to be embedded within primary and secondary care
• Barriers have still to be overcome before the benefits of
pharmacist prescribing can be fully realised
Introduction
Health care in the United Kingdom (UK) has undergone
significant changes in terms of the roles and responsibilities
of the professionals who provide patient services. This has
been notable in relation to prescribing as a result of the
recommendations of the Crown Report, on the prescribing,
supply and administration of medicines [1], published in
1999. This report recommended extending prescribing
authority to non-medical professionals, including nurses
and pharmacists [1, 2]. In the context of this report, these
non-medical prescribers (NMPs) were described as
dependent prescribers (now called supplementary pre-
scribers) [SPs]. Supplementary prescribing is a partnership
between the independent prescriber (IP) and SP, who draw
up, with the patient’s agreement, an individual Clinical
Management Plan (CMP) for the patient’s condition before
supplementary prescribing begins, allowing a SP to man-
age the treatment of individual patients within identified
parameters [3, 4]. A SP may only prescribe medication
within a patient-specific CMP which may include authority
to alter doses or to stop medicines that are no longer needed
[5]. Further policy changes have taken place and NMPs
have gained independent prescribing rights [2]; an IP is
‘responsible for the assessment of patients with undiag-
nosed and diagnosed conditions and for decisions about the
clinical management required, including prescribing [6].
Provided the appropriate training has been successfully
completed and an IP is working within their competency,
an IP may prescribe almost any medicine deemed appro-
priate for a patient. Since 2006, any pharmacist who wishes
to become a prescriber must complete an accredited edu-
cation and training programme, comprising at least 26 days
of teaching, with an additional 12 days of learning in
practice supervised by a medical practitioner (mentor) [7].
A number of studies have evaluated nurse and phar-
macist supplementary prescribing [8–10], however there is
still a paucity of data relating to the impact of such pre-
scribing behaviour on clinical outcomes for patients and
patients’ views of the role of pharmacists in prescribing.
Early findings from a number of reports on pharmacist
prescribing largely mirror what has been reported from
nurse prescribing research. Benefits such as increased job
satisfaction, self-confidence, increased time with patients,
greater recognition of the role of the pharmacist, greater
level of medicines information provided and time-saving
have been reported [8–10], but this has been tempered by
financial and organisational problems, a lack of awareness
of the pharmacists’ prescribing role and restrictions
imposed by the CMP [8]. Research has also shown that
current levels of pharmacist prescribing in primary care
and community practice in England are extremely low,
equating to only 0.004% of all prescribing (in terms of
number of prescribed items) in this sector [11].
Aim of the study
This study aimed to capture information on pharmacist
prescribing in Northern Ireland (NI) [such as clinical areas/
practice settings of prescribers, their working arrangements
and barriers to prescribing] and was part of a larger study
evaluating pharmacist prescribing in NI.
Method
Ethical approval was granted from the Office for Research
Ethics Committee Northern Ireland (reference: 09/NIR03/
54). Governance approval was granted from the relevant
Health authorities. At the time of this study, 105 pharma-
cists had qualified as a SP and/or an IP in NI (representing
approximately 6% of all qualified pharmacists in NI). All
prescribers had been trained in conjunction with the
Northern Ireland Centre for Pharmacy Learning and
Development (NICPLD) and contact with pharmacist pre-
scribers was facilitated through this organisation. Contact
details were retrieved from the NICPLD database and
confirmed with the Pharmaceutical Society of Northern
Ireland (PSNI) which is responsible for maintaining a
register of all pharmacist prescribers. This approach
allowed the identification of other qualified pharmacist
prescribers who may not have trained via NICPLD, but
who now worked as a pharmacist prescriber in NI.
Three versions of a structured self-administered ques-
tionnaire were developed by referring to previous qualita-
tive findings [12, 13], and other relevant literature to
accommodate the current status of prescribing pharmacists:
i.e. those currently prescribing; those who had prescribed
in the past but who are not currently prescribing, and those
who were qualified as prescribers but had never prescribed.
The three questionnaires had common sections on demo-
graphics, clinical area or intended clinical area of practice,
practice setting or intended practice setting, questions on
outcomes for pharmacists, patients and other healthcare
professionals, barriers to prescribing and the future of
pharmacist prescribing. Pharmacists were asked to provide
Int J Clin Pharm (2011) 33:824–831 825
123

any other comments regarding pharmacist prescribing (free
text section). Additional questions were included for cur-
rent prescribers and those who had prescribed in the past
(e.g. prescribing activities, drugs most commonly pre-
scribed (free text) extent of involvement in the multi-dis-
ciplinary team etc.). The questionnaire was piloted (current
prescriber version) with a random sample of prescribing
pharmacists (n = 30) from Scotland, ten of whom pro-
vided feedback on its content and ease of completion; it
was also reviewed by two colleagues in the School of
Pharmacy, Queen’s University Belfast.
Initially an email was drafted and sent to all qualified
pharmacist prescribers to ascertain their prescribing status
(n = 105). Pharmacists were asked to indicate their status
(by selecting one category) as previously outlined and
responding via email to the research fellow (LMC). Phar-
macist prescribers were also asked to provide their current
postal address. A cover letter was sent with the appropriate
questionnaire to explain the nature of the research project
and to reiterate the assurance of confidentiality. The first
mailing took place in October 2009; a second mailing was
carried out in November 2009. All returned questionnaires
were coded and data entered into SPSS� version 18 (SPSS
Inc., Illinois, USA) for analysis. Descriptive analyses were
used as appropriate, together with Chi-squared tests or
Fisher exact tests to test for associations between responses
and demographic information, with significance set a priori
at P \ 0.05. Qualitative data (from free response sections)
were analysed for recurring themes using content analysis.
Results
Of the 105 pharmacist prescribers contacted, 100 replied
(of whom 46 were current prescribers; 47 had never pre-
scribed and 7 had prescribed previously) to the initial email
correspondence providing details on prescribing status,
representing the denominator for the study. Following
distribution of the appropriate questionnaire (two mailings)
a 76.0% response rate (n = 76) was achieved. There were
more female respondents (73.7%) than males (26.3%).
Nearly 50% of respondents were currently prescribing
(47.4%, n = 36), 46.1% (n = 35) had never prescribed
(e.g. due to lack of funding, resources) and 6.6% (n = 5)
had prescribed in the past (e.g. due to a change in job). A
demographic profile of the study respondents is presented
in Table 1.
The dominant clinical areas for current and previous
prescribers were (1) hypercholesterolaemia (hyperlipida-
emia), (2) hypertension, (3) cardiovascular and diabetes
management and (4) anti-coagulation. The clinical areas in
which pharmacists who had never prescribed had intended
to prescribe were (1) respiratory e.g. asthma, chronic
obstructive pulmonary disease (COPD) etc., (2) hyperten-
sion, (3) haematology and (4) pain management. The four
classes of drugs (reported in free text section) most com-
monly prescribed by current and previous pharmacist pre-
scribers were (1) lipid-regulating drugs (13.3%) (2)
angiotensin-converting enzyme inhibitors/angiotensin-II
receptor antagonists (12.2%) (3) anti-coagulants (10%) and
(4) thiazides and diuretics (7.2%).
Barriers to implementing prescribing reported by those
who had never prescribed included inadequate resources to
cover other core services (n = 16; 45.7%); inadequate
funding (n = 10, 28.6%) and onerous paperwork associ-
ated with the CMP (n = 10, 28.6%). The main barriers
experienced by current prescribers when first qualified
included inadequate funding (n = 12; 33.3%); lack of
awareness of pharmacist prescribing by other healthcare
professionals (n = 12; 33.3%); inability of computers to
generate pharmacist prescriptions (n = 10; 27.8%) and
onerous paperwork associated with the CMP (n = 10;
27.8%).
Over 30% of current prescribers felt that they were
‘excellent’ at ‘opening the patient consultation’ (n = 11,
30.6%) and answering patient questions (n = 13; 36.1%).
Nearly 45% (n = 16; 44.4%) of current prescribers felt
they were ‘excellent’ at explaining information to patients
(5 point Likert scale). Over 20% (n = 8; 22.2%) of current
prescribers felt that they were ‘excellent’ at ‘setting aside
time to allow patients to ask any questions they may have’.
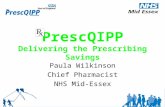
However, only 5% of current prescribers felt they were
‘excellent’ at ‘undertaking physical examination of
patients’ (n = 2; 5.6%) while half (n = 18; 50%) felt
‘adequate’ in undertaking this activity (Fig. 1).
Irrespective of prescribing status, most pharmacists
‘agreed’ or ‘strongly agreed’ that pharmacist prescribing
reduced the time-delay for patients between dose adjust-
ments [63/76 (82.9%)], increased continuity of care [62/76
(81.6%)], increased patient involvement in drug treatment
decisions [61/76 (80.3%)], increased patient compliance/
adherence [63/76 (82.9%)], increased monitoring of
patients’ drug therapy [70/76 (92.2%)], increased appropri-
ateness of drug therapy used [69/76 (90.8%)] and improved
patient safety [64/76 (84.3%)]. Over 70% of respondents
‘agreed’ or ‘strongly agreed’ that prescribing increased the
amount of time spent with patients during consultations
[71.1% (54/76)]. Current/previous prescribers were signifi-
cantly more likely to ‘strongly agree’ or ‘agree’ than those
who had never prescribed with the statement(s) that pre-
scribing had reduced the time-delay for patients between
dose adjustments (P = 0.01); and that prescribing had
increased patient compliance/adherence (P = 0.027).
Irrespective of prescribing status, most pharmacists
‘agreed’ or ‘strongly agreed’ that prescribing elevated the
professional status of the pharmacist [66/76 (86.8%)],
826 Int J Clin Pharm (2011) 33:824–831
123

Table 1 Demographic profile of pharmacist prescribers in NI who responded to the questionnaire (n = 76)
Currently
prescribing
Previously
prescribed
Never
prescribed
47.4% (n = 36) 6.6% (n = 5) 46.1% (n = 35)
Gender
Male 19.4% (n = 7) 20% (n = 1) 34.3% (n = 12)
Female 80.6% (n = 29) 80% (n = 4) 65.7% (n = 23)
Year of pharmacist registration
1979–1989 38.9% (n = 14) 60% (n = 3) 25.7% (n = 9)
1990–1999 50.0% (n = 18) 40% (n = 2) 62.9% (n = 22)
2000–2010 11.1% (n = 4) 0 11.4% (n = 4)
Type of prescribing undertaken
Supplementary prescribing 0 80% (n = 4) N/A
Independent prescribing 88.9% (n = 32) 0 N/A
Both supplementary and independent prescribing 11.1% (n = 4) 20% (n = 1) N/A
Prescribing setting**
Hospital inpatient 5.6% (n = 2) 20% (n = 1) 25.7% (n = 9)
Hospital outpatient 19.4% (n = 7) 20% (n = 1) 14.3% (n = 5)
Hospital inpatient and outpatient 25.0% (n = 9) 20% (n = 1) 20.0% (n = 7)
*GP surgery 47.2% (n = 17) 40% (n = 2) 17.1% (n = 6)
Community pharmacy 0 0 11.4% (n = 4)
GP surgery and community pharmacy 0 0 5.7% (n = 2)
Other (for e.g. private or prison) 0 0 5.7% (n = 2)
*GP general practitioner
**Missing data
Ability in opening the
patient consultation
Ability in explaining information
Ability in setting aside time to
allow patients to ask questions
Ability in answering questions
Ability in undertaking
physical examination
Ability in closing the patient
consultation
2.8% 5.6% 5.6%13.9%
8.3%
16.7%16.7%
50.0%
11.1%
52.8%
44.4%
55.6%
44.4%
25.0%
63.9%
30.6%
44.4%
22.2%
36.1%5.6%
16.7%
Poor Between poor and adequate Adequate Between adequate and excellent Excellent
Fig. 1 Pharmacists’ (current prescribers) abilities in a number of activities related to prescribing
Int J Clin Pharm (2011) 33:824–831 827
123

increased their job satisfaction [69/76 (90.8%)], stream-
lined previous practice [65/76 (85.5%)], increased profes-
sional autonomy [70/76 (92.1%)] and resulted in better
utilisation of pharmacists’ clinical skills [75/76 (98.7%)].
No respondents ‘disagreed’ or ‘strongly disagreed’ with
any of the above statements. Most pharmacists either
‘disagreed’ or ‘strongly disagreed’ with the statement that
pharmacist prescribing increased the responsibility and
accountability of pharmacist prescribers in a negative way
[54/76 (71.1%)]. Current/previous prescribers were sig-
nificantly more likely to ‘strongly agree’ or ‘agree’ with the
statement(s) that prescribing had increased their job satis-
faction (P = 0.026) than those who had never prescribed;
and that pharmacist prescribing had legalised previous
practice e.g. writing prescriptions and getting doctors to
sign them (P= 0.031).
Table 2 indicates that eighty per cent of prescribers
[80.3%, (n = 61)] either ‘strongly agreed’ or ‘agreed’ with
the statement ‘‘I envisage the future as pharmacist Inde-
pendent Prescribing rather than pharmacist Supplementary
Prescribing’. Eighty per cent [80.3%, (n = 61)] of pre-
scribers either ‘strongly agreed’ or ‘agreed’ with the state-
ment ‘‘I would prefer to undertake pharmacist independent
prescribing after a diagnosis has been made by a doctor’’.
Over 50% of prescribers either ‘strongly agreed’ or ‘agreed’
with the statements that pharmacist supplementary pre-
scribing should only be undertaken in a team environment
[56.6%, (n = 43)] and pharmacist independent prescribing
should only be undertaken in a team environment [51.40%,
n = 39)]. Over fifty per cent of pharmacists (n = 41;
53.9%) either ‘disagreed’ or ‘strongly disagreed’ with the
statement ‘‘I am happy to undertake diagnosis in my role as
a pharmacist independent prescriber’’.
A number of recurrent themes were apparent from
the free text responses provided. These were summa-
rised under the themes of: issues relating to information
technology (e.g. need for shared patient records), lack
of funding and lack of awareness of the pharmacists’
role, (Table 3) and largely reinforced the quantitative
findings.
Table 2 Pharmacists’ responses on the development of pharmacist supplementary and independent prescribing
Strongly
agree/agree
Neither agree
or disagree
Disagree/strongly
disagree
Supplementary prescribing has no future as it usually
focuses on one clinical area only
19.7% (n = 15) 22.4% (n = 17) 57.9% (n = 44)
I envisage the future as pharmacist independent
prescribing rather than pharmacist supplementary prescribing
80.3% (n = 61) 13.2% (n = 10) 6.6% (n = 5)
Pharmacist independent prescribing is welcomed by all doctors 13.1% (n = 10) 39.5% (n = 30) 47.3% (n = 36)
Doctors perceive pharmacist independent prescribing
as handing over too much control
18.4% (n = 14) 48.7% (n = 37) 31.5% (n = 24)
I am happy to undertake diagnosis in my role as a
pharmacist independent prescriber
31.6% (n = 24) 14.5% (n = 11) 53.9% (n = 41)
I would prefer to undertake pharmacist independent prescribing
after a diagnosis has been made by a doctor
80.30% (n = 61) 13.20% (n = 10) 6.60% (n = 5)
Doctors with whom I work closely would be happy
for me to make diagnoses
35.2% (n = 26) 40.5% (n = 30) 24.4% (n = 18)
All doctors would be happy for any pharmacist prescriber
to make diagnoses
0 (n = 0) 14.70% (n = 11) 85.30% (n = 64)
All doctors would prefer pharmacist independent prescribing
to take place following a diagnosis made by a doctor
44.7% (n = 34) 42.1% (n = 32) 13.1% (n = 10)
Pharmacist independent prescribing should be limited
to minor ailments and conditions for which treatments
are covered by a protocol
13.1% (n = 10) 7.9% (n = 6) 79.0% (n = 60)
Pharmacist supplementary prescribing should only
be undertaken in a team environment
56.6% (n = 43) 17.1% (n = 13) 26.3% (n = 20)
Pharmacist independent prescribing should only
be undertaken in a team environment
51.4% (n = 39) 11.8% (n = 9) 36.9% (n = 28)
Pharmacist prescribers should be managerially
accountable to a physician e.g. consultant/GP
38.2% (n = 29) 28.9% (n = 22) 32.8% (n = 25)
For pharmacist prescribing to be successful,
prescribing pharmacists must operate a
24 h-a-day, 7 days-a-week service
7.9% (n = 6) 18.4% (n = 14) 73.7% (n = 56)
828 Int J Clin Pharm (2011) 33:824–831
123

Discussion
A 76% response rate was achieved and of those who
responded, over 50% had either never prescribed or pre-
scribed in the past (e.g. no longer prescribing because of a
change in job); just over 50% of respondents are currently
prescribing in NI. This supports earlier work which found
that pharmacist prescribing has been accepted in practice
but is not widely prevalent [14, 15]. There were a higher
number of female respondents than males, reflecting the
overall demographic profile of pharmacists in NI (35.8%
male and 64.2% female) [NICPLD, 2011].
For those who were currently prescribing or had pre-
scribed previously, the dominant clinical areas were hy-
percholesterolaemia (hyperlipidaemia), hypertension,
cardiovascular and diabetes management and anti- coagu-
lation. This is similar to findings from other studies of
pharmacist prescribing. Over 35% of respondents in the
study by George et al. [8] were prescribing in the area of
cardiovascular medicine, and just over 7% were prescrib-
ing in respiratory medicine. The largest number of items
prescribed (according to British National Formulary cate-
gory [BNF]) in the study by Baqir et al. [15] were in the
cardiovascular, central nervous and gastro-intestinal areas.
Findings from this study have been positive in terms of
how pharmacists perceive this new method of practice.
Over 80% of pharmacists ‘agreed’ or ‘strongly agreed’ that
prescribing increased continuity of care and increased
patient compliance/adherence. This has been found previ-
ously in studies of non-medical prescribing [8, 13, 16]. In
this present study most pharmacists ‘disagreed’ or ‘strongly
disagreed’ that pharmacist prescribing increased responsi-
bility and accountability of a pharmacist prescriber in a
negative way; this suggests that pharmacists may be con-
fident in their abilities and eager to take on the extra
responsibility associated with prescribing. This appears to
support findings by Lloyd et al. [13] where it was reported
that pharmacists felt a greater level of responsibility and
accountability but welcomed and accepted this as part of
their professional progression, and there was greater rec-
ognition of their role in the health care team [13]. Phar-
macists already have experience in many aspects of clinical
Table 3 Free text responses reported by responding pharmacists
Themes Pharmacist quotes
Information
technology
‘‘This is an evolving role largely dependent on access to patient records if it is to progress but need also to continue tobuild relationships with medical practitioners’’ (CP, primary care)
‘‘I feel that pharmacy independent prescribing can only take place in a primary care setting, within GP practices. This isbecause we have no access to patient history and notes otherwise. This makes prescribing from elsewhere more difficultand possibly less effective’’ (CP, primary care)
‘‘I have seen no evidence that supplementary or independent prescribing will be implemented in community pharmacy. Ibelieve I will never use my qualification and that it was ‘mis-sold’ to me. I believe it was a waste of time and money. Itmay be useful in hospital or surgery settings but not in community pharmacy’’ (NP, primary care)
Inadequate funding ‘‘Supplementary prescribing was a missed opportunity on the part of the board. A completely unrealistic pay suggestionjust made it impossible for me to leave my business and work in surgeries which until records are shared was the onlysafe method’’ (NP, primary care)
‘‘Hospital pharmacists have not been remunerated for taking on these additional roles and responsibilities. Paid as Band7’s*, same band as many nurses and other pharmacists who have not taken on additional roles’’ (CP, secondary care)
‘‘Although I have qualified as a supplementary prescriber, I have not used this qualification and do not see this changing.Funding and access to clinical notes are the main barriers. With an increasing workload in my dispensary, providingadditional services such as minor ailments, smoking cessation and weight management, it does not pay me to leave mypharmacy to run a clinic in a GP surgery’’ (NP, primary care)
‘‘Funding issues-it is not financially viable to work with independent prescribing qualification’’ (NP, primary care)
Lack of awareness ‘‘I feel that GPs are not ready to hand over any of their prescribing yet to pharmacists. I think GPs are trainingpharmacists as supplementary and independent prescribers but are not fully aware of the role they are training us for.Many GPs feel that the idea of pharmacists prescribing is very contentious and feel there is a conflict of interest betweenpharmacists prescribing and dispensing’’ (NP, primary care)
‘‘Once GPs understand the supplementary prescribing/independent prescribing role they feel more comfortable-
particularly if you can work in an area (such as benzodiazepine reduction) which can involve a lot of time’’ (CP, primary
care)
‘‘I feel that pharmacist prescribing has been hindered by the development of clinical nurse specialists. The nurses are inmore contact with the medical teams and therefore have a greater ability to expand their roles. There are also a greaternumber of nurses and they get more publicity. Pharmacy management not particularly supportive of pharmacistprescribers or clinical pharmacist roles’’ (NP, secondary care)
CP currently prescribing, NP never prescribed
*Pay scale: secondary care setting
Int J Clin Pharm (2011) 33:824–831 829
123

practice [17] therefore taking on responsibilities for pre-
scribing and monitoring therapy can be seen as a natural
extension of a pharmacist’s existing role [17].
In this current study, over 80% of pharmacists ‘agreed’
or ‘strongly agreed’ that prescribing improved patient
safety. This has been found elsewhere [19]; this may be
because pharmacists are particularly well placed to make
an impact on patient safety due to their high risk aversion/
safety focus [17]. Respondents in a study by Weiss and
Sutton [20] felt that the addition of new prescribers would
improve safety and access by ensuring that prescribing
decisions were documented, and taken responsibility for,
by a prescriber who was available in a timely manner. It
has been argued that recognising levels of competency is
crucial in managing prescribing decisions for all health
care professionals (HCPs). HCPs are accountable for their
acts and omissions and must work within their skills,
knowledge and competence [17]. It is particularly impor-
tant that pharmacists develop a culture of safety, do not
prescribe outside their areas of competency and are sup-
ported in their prescribing role, rigorous and robust gov-
ernance procedures should be in place where pharmacist
prescribers operate [18].
A number of barriers to implementing pharmacist pre-
scribing were noted such as inadequate funding, inadequate
resources to cover other core services and onerous paper-
work associated with the Clinical Management Plan
(CMP). Most of those who had never prescribed reported
experiencing such barriers to prescribing which would
suggest that these issues played a significant part in phar-
macists not beginning prescribing practice. Logistical
barriers to implementation identified such as information
technology issues (lack of access to patient notes in pri-
mary care), the CMP, funding and lack of resources have
all been reported previously [8, 13, 15]. It may also be
possible that doctors are not happy with shared access to
patient notes and wish to retain this control. In this present
study, onerous paperwork associated with the CMP was
cited as a barrier when pharmacists first qualified; in the
past CMPs (supplementary prescribing only) were con-
sidered restrictive, time consuming and unsuitable in get-
ting agreement from the IP [8]. This appears to be no
longer an issue as the introduction of independent pre-
scribing rights for pharmacists means generic treatment
plans are now used and CMPs are no longer required. Other
research (mainly UK) has cited similar barriers; financial
pressures, both organisational and personal (e.g. cost of
indemnity insurance) as barriers to expanding the services
offered by prescribing pharmacists [15].
Implicit within a prescribing consultation are history-
taking, clinical examination skills and the diagnostic and
therapeutic decision-making processes [20]. In this present
study there was a general view that pharmacists were least
confident at undertaking physical examination of patients.
Eighty percent of pharmacists preferred to undertake
pharmacist independent prescribing after a diagnosis had
been made by a doctor. It appears that whilst pharmacists
have taken on the role of prescriber, they have less desire to
take on the role of diagnostician and would prefer to pre-
scribe within a team context. Indeed, in most cases, the
initial diagnosis is made by the doctor. This mirrors what
has been reported in earlier studies of pharmacist pre-
scribing; Lloyd et al. [13] reported that there were major
concerns voiced over pharmacist involvement in diagnosis
as doctors considered this their defining role and appreci-
ated that pharmacists themselves would be uncomfortable
with diagnosis. Similarly, were two aspects of the pre-
scribing process where pharmacists felt the least compe-
tent: conducting clinical examinations and making initial
diagnostic decisions [20]. Pharmacists in this study [20]
conveyed that they were not used to carrying out physical
examinations of patients and many had selected pharmacy
as a profession because they did not want ‘to get their
hands dirty’ [20].
A number of recurrent themes were reported by pre-
scribers in the final section for free text responses. Essential
to effective prescribing was the need for shared patient
records. Inadequate funding and lack of support and
awareness of pharmacist prescribing from other HCPs were
cited as significant barriers. Again, these issues have been
reported elsewhere [8, 12]. Some of these barriers may help
explain why community pharmacists as yet cannot pre-
scribe from their own pharmacy.
In this current study, over 80% of respondents either
‘strongly agreed’ or ‘agreed’ with the statement ‘I envisage
the future as pharmacist independent prescribing rather
than pharmacist supplementary prescribing’. This could
potentially be attributed to the onerous paperwork associ-
ated with the CMP and reflects the findings of Lloyd et al.
[13]. Provided pharmacists have successfully completed
the appropriate training and are working within their
competency, independent prescribing allows pharmacists
to prescribe almost any medicine believed to be appropriate
for the patient although there are some limitations [5]. It is
advantageous that a CMP is no longer required to be used
by pharmacist IPs. Independent prescribing is clearly the
future model of practice although pharmacist prescribers
will continue to work under appropriate guidelines, often
using generic treatment plans which indicate the scope and
extent of prescribing practice.
The role of response bias must not be overlooked; the
extent to which non-response bias plays a part in this study
is unknown. The intrinsic motivation of the respondent is
critical to who responded; those pharmacists who were
particularly interested in the area of pharmacist prescribing
may have been most likely to respond.
830 Int J Clin Pharm (2011) 33:824–831
123

Conclusion
This study has shown that the number of qualified pre-
scribers in NI is relatively small (in comparison to the rest
of the UK) and not all have taken up prescribing respon-
sibilities. Well recognised barriers were reported as reasons
as to why qualified prescribers were unable to use their
prescribing skills. Independent prescribing was viewed as
the way forward, however, respondents considered that the
role of diagnostician should remain with a doctor as they
have overall responsibility for a patient’s care. Further
research should provide an in-depth understanding of
pharmacy prescribing in NI and examine patients’ experi-
ences of this form of practice.
Acknowledgments The authors would like to thank all pharmacist
prescribers who completed the questionnaire. A copy of the ques-
tionnaire can be made available to the reader on request.
Funding This work was supported by Health and Social Care
Research and Development (HSC R and D) Northern Ireland.
Conflicts of interest None.
References
1. Crown Report: Review of prescribing, supply and administration
of medicines. 1999; Final report. London: Department of Health.
http://www.dh.gov.uk/dr_consum_dh/groups/dh_digitalassets/
@dh/@en/documents/digitalasset/dh_4077153.pdf. Accessed 10
Jan 2010.
2. Offredy M. Development of non-medical prescribing—Historical
background and competency framework for successful prescrib-
ing. In: Sodha M, Dhillon S, editors. Non-medical prescribing.
London: Pharmaceutical Press; 2009. p. 1–10. ISBN: 97808
53697688.
3. Department of Health. Supplementary prescribing by nurses and
pharmacists with the NHS in England: a guide for implementa-
tion. March 2003. http://www.dh.gov.uk/dr_consum_dh/groups/
dh_digitalassets/@dh/@en/documents/digitalasset/dh_4068431.
pdf. Accessed 10 Jan 2010.
4. Department of Health, Social Services and Public Safety. Sup-
plementary prescribing by nurses and pharmacists within the
HPSS in Northern Ireland: a guide for implementation. April
2004. http://www.dhsspsni.gov.uk/prescribing_nurses_pharmaci
sts_in_hpss_ni.pdf. Accessed 4 Feb 2010.
5. Wingfield J. Legal and ethical aspects of prescribing. In: Sodha
M, Dhillon S, editors. Non-medical prescribing. London: Phar-
maceutical Press; 2009. p. 12–30. ISBN: 9780853697688.
6. Department of Health. Improving patients’ access to medicines: a
guide to implementing nurse and pharmacist independent pre-
scribing within the NHS in England. April 2006 www.dh.gov.uk/
nonmedicalprescribing. Accessed 10 Oct 2010.
7. Royal Pharmaceutical Society of Great Britain. Outline curricu-
lum for training programmes to prepare pharmacist prescribers.
London: Royal Pharmaceutical Society of Great Britain; 2006.
8. George J, McCaig D, Bond CM, Cunningham ITS, Diack HL,
Watson AM, Stewart DC. Supplementary prescribing: early
experiences of pharmacists in Great Britain. Ann Pharmacother.
2006;40:1843–50.
9. Weiss MC, Sutton J, Adams C. Exploring innovation in phar-
macy practice: a qualitative evaluation of supplementary pre-
scribing by pharmacists. 2006; Royal Pharmaceutical Society of
Great Britain. http://www.pprt.org/Documents/Publications/Ex
ploring_innovation_in_pharmacy_practice_supplementary_prescri
bing.pdf. Accessed 3 February 2010.
10. Cooper RJ, Anderson C, Avery T, et al. Nurse and pharmacist
supplementary prescribing in the UK-a thematic review of the
literature. Health Policy. 2008;85:277–92.
11. Guillaume L, Cooper R, Avery A, et al. Supplementary pre-
scribing by community and primary care pharmacists: an analysis
of PACT data 2004–2006. J Clin Pharm Ther. 2008;33:11–6.
12. Lloyd F, Hughes CM. Pharmacists’ and mentors’ views on the
introduction of pharmacist supplementary prescribing-a qualita-
tive evaluation of views and context. Int J Pharm Pract.
2007;15:31–7.
13. Lloyd F, Parsons C, Hughes C. ‘It’s showed me the skills that he
has’: pharmacists’ and mentors’ views on pharmacist supple-
mentary prescribing. Int J Pharm Pract. 2010;18 (1):29–36.
14. Stewart D, George J, Pfleger D, et al. Pharmacist supplementary
prescribing training: a study of pharmacists’ perceptions and
planned participation. Int J Pharm Pract. 2007;15:319–25.
15. Baqir W, Clemerson J, Smith J. Evaluating pharmacist pre-
scribing across the north east of England. Brit J Clin Pharm.
2010;2:147–9.
16. Berry D, Courtenay M, Bersellini E. Attitudes towards, and
information needs in relation to, supplementary nurse prescribing
in the UK: an empirical study. J Clin Nurs. 2006;15:22–8.
17. O’Neill R. Clinical governance and patient safety in prescribing.
In: Sodha M, Dhillon S, editors. Non-medical prescribing. Lon-
don: Pharmaceutical Press; 2009. p. 32–57. ISBN: 9780853697
688.
18. Offredy M. Clinical decision making and evidence-based pre-
scribing. In: Sodha M, Dhillon S, editors. Non-medical pre-
scribing. London: Pharmaceutical Press; 2009. p. 85–97.
19. Stewart D, MacLure K, Bond C, et al. Pharmacist prescribing in
primary care: the views of nominated patients across Great
Britain who had experienced the service. Int J Pharm Pract. 2010;
18 (suppl 2):15–16.
20. Weiss MC, Sutton J. The changing nature of prescribing: phar-
macists as prescribers and challenges to medical dominance.
Sociol Health Ill. 2009;31(3):406–21.
Int J Clin Pharm (2011) 33:824–831 831
123