The Delta Forum 2005 Perspectives on Developing an Aerospace Workforce for 2025
Upload
trinhtuyenCategory
view
215download
2
ADAPTED PHYSICAL ACTIVITY QUARTERLY, 1986, 3,227-235
New Perspectives for Developing Range of Motion and Flexibility
for Special Populations
Paul R. Surburg Indiana University
The purpose of this article was to examine techniques that are available to adapted physical educators and therapeutic recreators to enhance flexibility. Based upon current research and literature in the areas of flexibility and range of motion, this article explored theoretical constructs as well as applications of specific techniques. A two-tier model for flexibility enhancement was gener- ated which served as a basis for the development of this article. One tier in- volved considerations concerning the stretching of collagenous tissue, implications regarding elastic and viscous properties, and new methods for stretching this type of tissue. The other tier incorporated neurophysiological mechanisms, their effect upon agonist and antagonist muscles, and facilita- tion exercises to improve flexibility.
During the Eisenhower administration the President's Council on Physical Fitness was established to foster improvement of physical fitness among Ameri- can youth. Data from a type of adapted fitness test, the Kraus-Weber test, precipi- tated this emphasis upon physical fitness. While the Kraus-Weber test was designed to evaluate components related to low back problems, comparison of data be- tween European and American youth on this one facet of fitness served as the catalyst to usher in the fitness movement.
Today numerous adults are involved in physical fitness programs, but many physical educators and sports medicine personnel are concerned about the fitness level of our youth. At a recent meeting of the U.S. Olympic Committee (Paul, 1985) a common theme was the deplorable level of physical fitness of American youth. A recent article by Legwold (1983), entitled "New Verse, Same Chorus: Children Aren't Fit," reflects this growing awareness that American youth are not fit. Cotton, Blankenbaker, and Harrison (1985), in a paper presented at the 1985 AAHPERD Conference, reported that the present level of youth fitness in this country was only slightly more improved than that of the youth of the 1960s, as evaluated by the Kraus-Weber test. Many individuals who are concerned with the fitness levels of our youth are spearheading another major effort to improve physical h e s s .
Request reprints from Dr. Paul R. Surburg, Dept. of Physical Education, HPER Bldg., Indiana University, Bloomington, IN 47405.

If this resurgence concerning physical fitness does emerge, how will adapted physical education be affected? From one perspective, a renewed emphasis upon physical fitness in physical education will affect many types of special popula- tions, for as the result of mainstreaming practices, a certain number of handicapped students are now found in regular physical education classes. Furthermore, research has shown special populations to be generally underfit.
Some physical educators already have been active in this area of research. Winnick and Short (1982) established fitness norms for certain types of han- dicapped students and have developed materials for improving physical fitness levels of these groups. A component of the definition of physical education as delineated by the regulations of PL 94-142 is physical and motor fitness. If an individualized education program has been designed to fulfill the intent of this law, physical fitness is an integral part of an adapted physical education program.
Certain facets of fitness, such as strength development and cardiovascular efficiency, have received much more attention and media coverage than the de- velopment of flexibility. However, it behooves all adapted physical educators to be conversant with recent trends in flexibility enhancement because some han- dicapping conditions are devoid of needed flexibility or range of motion. Also, the adapted physical educator must provide a continuity of services from hospital and clinic to school setting. In many school systems the adapted physical educa- tor is called upon to provide in-service training to regular physical educators. A greater knowledge of flexibility will help the physical education teacher deal effectively with this facet of fitness for both normal and handicapped students.
Theoretical Model
A clear understanding of the underlying principles or mechanisms for flexibility development is needed before the adapted physical educator may prudently ap- ply flexibility techniques to special populations. Throughout this article both flex- ibility and range of motion (ROM) will be referred to in the same context, for although these terms are not synonymous, they are related. The development of optimal fitness for certain types of handicapping conditions requires attainment of a suitable ROM at a joint before any type of flexibility exercise program can be attempted.
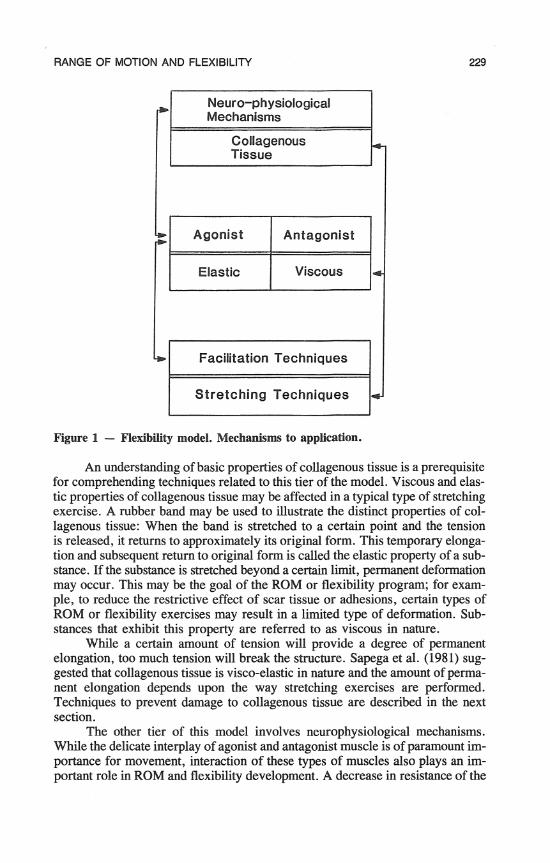
A two-tier model is presented to help understand the mechanisms involved in flexibility development (Figure 1). Many individuals think of flexibility de- velopment in terms of stretching exercises for the elongation of muscle tissue. Sapega, Quedenfeld, Moyer, and Butler (1981) stated "the weight of laboratory evidence indicates that when a relaxed muscle is physically stretched, most-if not all-of the resistance to stretch is derived from the extensive connective tis- sue framework and sheathing within and around the muscle, not from the myo- fibrillar elements" (p. 58). In addition to this type of tissue, ligaments, aponeuroses, fascial bonds, joint capsules, and tendons will be included in the collagenous tissue component. Adhesions, fibrous tissue, and/or scar tissue as-
RANGE OF MOTION AND FLEXIBILITY
Antagonist 1 1 1 *
Stretching Techniques
Figure 1 - Flexibility model. Mechanisms to application.
Neuro-physiological Mechanisms
Collagenous Tissue
An understanding of basic properties of collagenous tissue is a prerequisite for comprehending techniques related to this tier of the model. Viscous and elas- tic properties of collagenous tissue may be affected in a typical type of stretching exercise. A rubber band may be used to illustrate the distinct properties of col- lagenous tissue: When the band is stretched to a certain point and the tension is released, it returns to approximately its original form. This temporary elonga- tion and subsequent return to original form is called the elastic property of a sub- stance. If the substance is stretched beyond a certain limit, permanent deformation may occur. This may be the goal of the ROM or flexibility program; for exam- ple, to reduce the restrictive effect of scar tissue or adhesions, certain types of ROM or flexibility exercises may result in a limited type of deformation. Sub- stances that exhibit this property are referred to as viscous in nature.
While a certain amount of tension will provide a degree of permanent elongation, too much tension will break the structure. Sapega et al. (1981) sug- gested that collagenous tissue is visco-elastic in nature and the amount of perma- nent elongation depends upon the way stretching exercises are performed. Techniques to prevent damage to collagenous tissue are described in the next section.
The other tier of this model involves neurophysiological mechanisms. While the delicate interplay of agonist and antagonist muscle is of paramount im- portance for movement, interaction of these types of muscles also plays an irn- portant role in ROM and flexibility development. A decrease in resistance of the
c

agonistic or target muscle group (Hartley-O'Brien, 1980) is an objective of flexi- bility or ROM exercises. Autogenic inhibition may help to reduce the tension in the agonistic muscle group. Impulses from the Golgi tendon organ override excitatory impulses from muscle spindles (McCough, Deering, & Stewart, 1950). This phenomenon seems to occur when muscles are stretched in a certain manner.
Reciprocal inhibition involves an agonist-antagonist relationship. When excitatory impulses from afferent nerves interact with motor neurons of an agonist muscle, afferent impulses to the motor neurons of the antagonist muscles cause an inhibitory effect and subsequent relaxation of these muscles. The use of in- hibitory mechanisms in the development of flexibility and ROM is a physiologi- cal principle that is the basis for Kabat's proprioceptive neuromuscular facilita- tion (PNF) techniques (Kabat, 1965). In certain instances the use of PNF for flex- ibility development should be called proprioceptive neuromuscular inhibition.
Although the efficacy of PNF techniques for flexibility development has been established (Holt, Travis, & Okita, 1970; Rizk, Christopher, Pinals, Hig- gins, & Fix, 1983; Tanigawa, 1972), Markos (1979) reported that a PNF tech- nique not only improved flexibility of the target hamstring but exhibited a transfer effect in the contralateral limb. This study by Markos not only reinforces the concept of neurophysiological elements operant in flexibility development but also opens a door for expanding the flexibility model. Since the collagenous tissue element of this model was not involved, there may be a learning component to flexibility development. The application of this idea to special populations may be more significant than to nonhandicapped persons. Individuals with certain neu- rologic damage, such as with some types of mental retardation, may not be able to utilize this learning component for flexibility development.
The use of relaxation techniques is another way to reduce target muscle resistance. This approach may be particularly useful when dealing with spastic muscles related to upper motor neuron lesions.
From Theory to Practice: Techniques for Collagenous Tissue
Techniques for the development of ROM and flexibility are often synonymous in nature but there may be a hierarchical sequence concerning their purpose. A person with hip flexion contractions associated with muscular dystrophy, an above- knee amputation (Krusen, Kottke, & Ellwood, 1966) or limited motion because of burns may need to develop ROM before flexibility development may be con- sidered a goal. For other students who are mildly mentally retarded, learning disabled, or obese, improvement of fitness levels including flexibility may be part of their individualized education program.
A word of caution should be interjected as the focus of flexibility develop- ment shifts from theoretical to practical aspects. All flexibility programs for spe- cial population students should be approved by a physician. The level of medical direction or involvement will vary with the student's condition. For the obese erson the physician may recommend an appropriate physical fitness program
uding flexibility development. With the bum victim returning to school, the sician may designate specific types of flexibility or ROM exercises to be done
hysical education class. For the student with an upper motor neuron problem

RANGE OF MOTION AND FLEXIBILITY 231
such as cerebral palsy, the physician or other medical personnel may recommend appropriate procedures and exercises that complement the total rehabilitation pro- gram. A greater emphasis may be placed on relaxing target muscle groups rather than stretching them.
While certain ROM and flexibility exercises seem to be more oriented toward the neurophysiological elements of the flexibility paradigm, other tech- niques are directed toward the collagenous tissue component. Some techniques involve both elements of the model. For purposes of organization, this dichoto- my will be used to discuss the nuances of flexibility development.
Flexibility or ROM exercises that are targeted toward collagenous tissue may be classified as active, passive, or a combination of both. Manipulation of a body part by a teacher or therapist through ROM, with or without prolonged stretch, is an example of a passive exercise. Using the aforementioned hip flex- ion contractures as an example, the adapted physical educator would lift the low- er extremity through hip extension until resistance is encountered. This position is held or additional pressure is applied for a brief period of time. This final posi- tion is established below the pain threshold.
Active exercise for the hip example involves the student's contracting the hip extension muscles until resistance precludes additional motion. The student may hold this elongated position for a brief period and then return the leg to the original or resting position. A variation of this technique is to move the body part several times through the desired motions and, on a designated repetition, hold the limb or body part in the elongated position for up to 6 seconds. A com- bination of active and passive protocols may be used. For example, an adapted physical educator may passively move the body part through the desired ROM and the student will actively hold the elongated position for a desired amount of time.
When connective tissue is stretched or placed in an elongated position, the visco-elastic properties of collagen must be considered. These properties must be taken into account and appropriate techniques used to enhance flexibility and to ensure minimal structural damage. Sapega et al. (1981) contend that minimal damage will occur with low intensity, prolonged stretching at warm tempera- tures and the cooling of tissue before tension is released. Referring to the exam- ple of hip flexion contractures, hot packs could be used to elevate the temperature of the target muscle group, and a low-to-moderate force would be applied to the target muscle group before tension is released. Kottke, Pauley, and Ptak (1966), Rizk et al. (1983), and Bohannon, Chavis, Larkin, Lieber, and Riddick (1985) have used this prolonged loading to help establish ROM in hip flexors, shoulder motions, and knee motions. Light, Nuzik, Personius, and Barstrom (1984) reported a preference for a low-load prolonged stretch for establishing ROM at the knee over a high-load brief stretch approach.
For adapted physical educators, the procedures just described may not be philosophically compatible or pragmatically possible. The basic approach to flex- ibility development espoused by Sapega may be incorporated into an adapted phys- ical education program. He recommended 5 minutes of warmup activities followed by some light stretching exercises. After students have concluded about two-thirds of their activities or the major part of the class period, the flexibility part of each student's fitness program is implemented following sufficient time for the tissues to warm up. This protocol may be used in different contexts for both normal and

232 Surburg
handicapped students. Cognizant of the visco-elastic properties of collagenous tissue, adapted or regular physical educators may incorporate this procedure into their flexibility programs. They may use such sophisticated measures as neuromus- cular facilitation patterns or as simple an approach as encouraging a student to move a joint through a designated number of degrees.
For the elementary school student with rheumatoid arthritis, extension of the fingers may be the movement of choice. Activities and games that incorporate these movements are done toward the end of the class period. With mentally han- dicapped students who lack needed motion at a joint, the following activity may be done toward the end of the class period: A colored dot is placed at the deltoid tuberosity and the student is instructed to move the dot toward the ceiling when shelhe hears music. Because of the dot's location, the student will engage in numer- ous movements that involve abduction and external rotation. These motions are key movements for efficient shoulder movement (Calliet, 1972). Placing the dot near the bicipital groove tends to result in more shoulder flexion at the gleno- humeral joint than other motions. Several dots may be placed on the body, not all of which have the specific goal of flexibility development but whose net effect is a type of dance experience. The adapted physical educator is providing an en- joyable experience for students, yet the goal of flexibility improvement is being attained without damage to collagenous tissue.
Neurophysiological Techniques
The second tier of the flexibility model incorporates neurophysiological mechan- isms to enhance ROM and flexibility. While there are several therapeutic ap- proaches such as Brunnstrom (1970), Bobath and Bobath (1964), and Rood (1962) methods based upon neurologic facilitation and inhibition, a method originated by Kabat (1965) and refined by Knott and Voss (1968) called proprioceptive neu- romuscular facilitation (PNF) is used extensively for flexibility and ROM de- velopment.
Three PNF techniques are used to develop ROM and flexibility. One tech- nique is called rhythmic stabilization and involves alternate isometric contrac- tions of the target and antagonistic muscle groups (Knott & Voss, 1968; Sur- burg, 1981). Using again the example of hip flexion contractures, which are not the result of an upper motor neuron lesion, 10 alternate isometric contractions of hip extensors and flexors would be executed per exercise set. These isometric contractions may be applied in a cardinal plane or in diagonal, spiral patterns. The latter approach is part of the Knott and Voss method (1968) and will not be discussed in this article.
A second technique called "contract-relax" incorporates passive movement of the target muscle group until it is in an elongated position. The student is in- structed to isotonically contract the target muscles as the teacher applies resistance to the movement. This resisted movement returns the body part to the original or resting position. When this position has been attained the student is instructed to relax, and after a 5-second rest period the entire process is repeated. A varia-
is the "hold-relax" technique, in which an isometric contrac- up is substituted for the isotonic contraction. Hardy

RANGE OF MOTION AND FLEXIBILITY 233
(1985) reported that a 6-second isometric contraction was more effective than contractions of shorter duration. This result was found to be operant when the subjects elongated the target muscles through active contraction of the antagonist muscle group rather than passive elongation of the target muscle group.
Efficacy of PNF techniques has been demonstrated in the literature. Holt et al. (1970) and Tanigawa (1972) reported the superiority of the hold-relax tech- nique over the traditional elongated stretch approach. In like fashion, Markos (1979) found contract-relax and hold-relax to be superior to ROM exercises for improving hip movements. More recently, studies by Sady, Wortman, and Blanke (1982) and Prentice (1983) demonstrated the superiority of PNF techniques over traditional stretching exercises.
All the research concerning PNF techniques does not provide evidence of this technique's superiority in establishing flexibility. Hartley-O'Brien (1980), Medeiros, Smidt, Bunneister, and Soderberg (1977) and Moore and Hutton (1980) reported that elongated techniques were as effective as PNF procedures for de- veloping flexibility. A perusal of these studies does reveal some confounding vari- ables such as the control group registering gains in ROM (Hartley-O'Brien, 1980), learning and possible asymmetrical transfer effects (Morris, 1981) in the Moore and Hutton study (1980), and absence of elements associated with PNF techniques (Medeiros et al., 1977).
Roles for Flexibility Development
As indicated in the introductory section, increasing ROM andlor flexibility is an important element of physical fitness enhancement. Students with such condi- tions as cerebral palsy, muscular dystrophy, obesity, rheumatoid arthritis, arn- putations, and excessive lordotic curves may benefit from ROM or flexibility exercises. For example, PNF techniques may reduce tight hip flexors that con- tribute to lordosis; the student with cerebral palsy may be exposed to relaxation techniques to enhance motion of the hip.
An inter-relationship exists between flexibility and motor fitness. For example, the mechanical concept of impulse (FT = mv) exemplifies this rela- tionship. If the time (T) is increased over which a force (F) may be applied, the velocity (V) will be increased provided the mass (M) of an object does not change. Translated to a motor skill, an increase in ROM at a joint should increase the time (T) for application of force. In terms of throwing or kicking skills, a person is able to bring the arm or leg further back in preparation to execute these skills. This increase in distance to apply a force translates into a time increment.
Surburg (1981) investigated the role assigned to PNF techniques in sports medicine. His findings indicated that PNF techniques were used in rehabilitative procedures, as preventive measures and as warmup exercises. While the role of rehabilitation in adapted physical education may not be endorsed by all adapted physical educators, the use of flexibility techniques for preventing injuries and as warmup exercises should have universal acceptance.
A new momentum for physical fitness development of school-age children may not come to fruition, but adapted physical educators must continue to facili- tate the development of physical fitness components. This article has covered tech-

niques of flexibility development that usually are not found in adapted physical education literature. These concepts and techniques may benefit handicapped stu- dents when adapted physical educators incorporate the techniques into fitness programs.
References
Bobath, K., & Bobath, B. (1964). The facilitation of normal postural reactions and move- ments in the treatment of cerebral palsy. Physiotherapy, 50, 246-262.
Bohannon, R.W., Chavis, D., Larkin, P., Lieber, C., & Riddick, L. (1985). Effec- tiveness of repeated prolonged loading for increasing flexion in knees demonstrat- ing postoperative stiffness. Physical Ilzerapy, 65, 494-496.
Brunnstrom, S. (1970). Movement therapy in hemiplegia. New York: Harper & Row. Calliet, R. (1972). Shoulder pain. Philadelphia: F.A. Davis. Cotton, D.J., Blankenbaker, J., & Hamson, R.D. (1985, April). Kraus- Weber test:
Fitness comparisons of American youngsters 30 years later. Paper presented at the AAHPERD Annual Conference, Atlanta.
Hardy, L. (1985). Improving active range of hip flexion. Research Quarterly for Exercise and Sport, 56, 111-114.
Hartley-O'Brien, S.J. (1980). Six mobilization exercises for active range of hip flexion. Research Quarterly for Exercise and Sport, 51, 625-635.
Holt, L.E., Travis, T.M., & Okita, T. (1970). Comparative study of three stretching techniques. Perceptual and Motor Skills, 31 , 61 1-616.
Kabat, H. (1965). Proprioceptive facilitation in therapeutic exercise. In S. Licht (Ed.), Therapeutic exercise @p. 327-343). Baltimore: Waverly Press.
Knott, M., & Voss, D.E. (1968). Proprioceptive neuromusczilar facilitation: Patterns and techniques. New York: Haeber-Harper.
Kottke, F.J., Pauley, D.L., & Ptak, R.H. (1966). The rationale for prolonged stretching for correction of shortening of connective tissue. Archives of Physical Medicine and Rehabilitation, 47, 345-352.
Krusen, F.H., Kottke, F.J., & Ellwood, P.M. (1966). Handbook of physical medicine and rehabilitation. Philadelphia: W.B. Saunders.
Legwold, G. (1983). New verse, same chorus: Children aren't fit. Ilze Physician and Sportsmedicine, 1 1 , 152-155.
Light, K., Nuzik, S., Personius, W., & Bmtrom, A. (1984). Low-load prolonged stretch vs. high-load brief stretch in treating knee contractures. Physical Ilzerapy, 64, 330-333.
Markos, P.D. (1979). Ipsilateral and contralateral effects of proprioceptive neuromuscular facilitation techniques on hip motion and electromyographic activity. Physical Zher- apy, 59, 1366-1373.
McCough, G., Deering, I., & Stewart, W. (1950). Inhibition of knee jerk from tendon spindles and crureus. Jouml of Neurophysiology, 13, 343-350.
Medeiros, J.M., Srnidt, G.L., Burmeister, L.F., & Soderberg, G.L. (1977). The influence of isometric exercise and passive stretch on hip joint. Physical Zherapy, 57,5 18-523.
Moore, M.A., & Hutton, R.S. (1980). Electromyographic investigation of muscle stretching

RANGE OF MOTION AND FLEXIBILITY 235
Morris, H. (1981, April). Experimental considerations in the analysis of repeated measure- ments. Paper presented at the AAHPERD Annual Conference, Boston.
Paul, C.R. (1985, February). Consultation Meeting on Fitness and Ethics. Minutes of the U. S. Olympic Committee Education Council. (Available from C .R. Paul, 1750 E. Boulder St., Colorado Springs, CO 80904-5760.)
Prentice, W. (1983). A comparison of static stretching and PNF stretching for improving hip joint flexibility. Athletic Training, 18, 56-59.
Rizk, T.E., Christopher, R.P., Pinals, R.S., Higgins, A.C., & Fix, R. (1983). Adhesive capsulitis (frozen shoulder): A new approach to its management. Archives of Phys- ical Medicine and Rehabilitation, 64, 29-33.
Rood, M. (1962). The use of sensory receptors to activate, facilitate, and inhibit motor response, autonomic and somatic in development sequence. In C. Sattely (Ed.), Approaches to treatment of patients with neuromuscular dysfunction @p. 26-37). Dubuque: IA: W.C. Brown.
Sady, S.P., Wortman, M.A., & Blanke, D. (1982). Flexibility training: Ballistic, static or proprioceptive neuromuscular facilitation? Archives of Physical Medicine and Rehabilitation, 63, 261 -263.
Sapega, H.A., Quedenfeld, T.C., Moyer, R.A., & Butler, R.A. (1981). Biophysical factors in range-of-motion exercise. The Physician and Sportsmedicine, 9 , 57-65.
Surburg, P.R. (1981). Neuromuscular facilitation techniques in sports medicine. The Physician and Sportsmedicine, 9 , 114-127.
Tanigawa, M. C. (1972). Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Physical Therapy, 52, 725-735.
Winnick, J., & Short, F. (1982). The physical Jimess of sensory and orthopedically impaired youth (Project Unique-Final Report). Brockport: State University of New York, College at Brockport.